

Abstract
Objectives:
The purpose of this study is to investigate the effect of the comprehensive oral care program on oral health status and symptoms in head and neck cancer (HNC) patients undergoing radiotherapy.
Methods:
This was a quasi-experimental study using a non-equivalent control group in non-synchronized design. All participants including control and experimental group were asked for the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire H&N35 (EORTC QLQ-H&N35) and given an oral health education 4 times at baseline, immediate postradiotherapy, 3 months after radiotherapy, and 6 months after radiotherapy. In each visit except for final, the experimental group was given fluoride varnish application and fluoride mouth rinsing solution for daily use. Oral health examination for dental caries, plaque score (PS), bleeding on probing (BOP), and salivary flow rate was performed in baseline and 6 months after radiotherapy. Statistical analyses were done by paired t-tests and mixed ANCOVA repeated-measures analysis.
Results:
From November 1, 2013 to October 31, 2015, a total 61 patients undergoing radiotherapy for HNC cancer were enrolled (30 in control and 31 in experimental groups). Decrease in salivary flow rate was comparable between 2 groups. Dental caries increased in control group (P = .006); PS and BOP were decreased in experimental group (P < .001 and .004, respectively). Experimental group showed lower swallowing, speech problems, and less sexuality scores in EORTC QLQ-H&N35 than control group.
Conclusion:
We found improvement in oral health and the quality of life in HNC patients with comprehensive oral care intervention by dental professionals. Communicating and cooperating between the healthcare and dental professionals is needed to raise the quality of health care services for HNC patients receiving radiotherapy.
Keywords: fluoride, head and neck cancer, oral health, quality of life, radiotherapy
1. Introduction
Head and neck cancer (HNC), an umbrella term for malignancies of larynx and hypopharynx, nasal cavity, paranasal sinuses, nasopharynx, oropharynx, oral cavity, and salivary gland, accounts for about half a million cases annually, ranking it as the sixth most common cancer globally.[1] About 90% of HNCs are squamous cell carcinomas arising from the epithelium in the region of head and neck.[2] Smoking, alcohol use, dietary micronutrient deficiency, solar irradiation and infection with human papilloma virus are important risk factors.[3,4]
Radiotherapy which is the most commonly used method for the treatment of HNC, uses high-energy radiation to shrink tumors and kill cancer cells, thus preventing the cells from growing, dividing, and spreading. However, when using radiotherapy, irradiation of normal tissue, in particular tissue close to the tumor, is unavoidable. Thus, this therapy often complex and frequently associated with significant short-and long-term complications including mucositis, dysgeusia, dysphagia, weight loss, malnutrition, hypo-salivation, increased risk of dental caries, increased risk of progression of periodontal disease, dental hypersensitivity, infections, mucosal atrophy, trismus, neuropathic pain and osteoradionecrosis (ORN).[5] A reduction in salivary function is a common side-effect of radiotherapy to the head and neck region.[6] When major salivary glands are subject to high radiotherapy doses, hypo-salivation becomes a problem and the resulting dry mouth environment makes retention of intact dentition a significant challenge.[5,7] Limited and often poor dietary choices compound the risk of dental breakdown in these patients.[5,7,8] Dental extractions as a result of dental caries place post-radiotherapy patients at risk of ORN with potentially serious consequences.[7,9] These side effects may delay and interfere with cancer treatment and may result in increased treatment costs and reduced quality of life (QoL).[10] Preservation of intact dentition is, therefore, paramount in safeguarding the HNC patient's life quality.
There were several studies on the application of oral preventive programs for HNC patients undergoing radiotherapy.[11–16] It is now well-established that prevention of dental caries for HNC patients with radiotherapy is multifaceted, involving regular dental care, maintenance of meticulous oral hygiene, fluoride use and dietary modification, minimizing consumption of cariogenic and acidic foods.[7,17–19] Above mentioned preventive tools could reduce demineralization and enhance remineralization of dental hard tissue. Moreover, recent systematic review stated that professionally applied fluoride products effectively remineralise early dental caries.[20] Therefore, fluoride application, dietary counseling, and oral health education including tooth brushing instruction are the methods of choice in combating dental diseases in HNC as in all patients.[21,22] However, few studies have examined the impact of a comprehensive oral care program on oral health status and QoL for patients with HNC who received radiotherapy. The current study aims to evaluate the impact of oral care program on the oral health and QoL in patients undergoing radiotherapy for HNC.
2. Materials and methods
2.1. Study design
A quasi-experimental, non-equivalent control group, non-synchronized design was used. We examined the effects of a comprehensive oral care intervention on the oral health and quality of life outcomes of HNC undergoing radiotherapy. Ethical approval of the study was granted by the Institutional Review Board (IRB No: 1402–078–558) of Seoul National University Hospital; voluntary participation, anonymity, and confidentiality were ensured throughout the study.
2.2. Participants
Study participants were enrolled from November 1, 2013 to October 31, 2015 among patients undergoing radiotherapy for non-metastatic and measurable HNC at the Department of Radiation Oncology in Seoul National University Hospital. All the recruited patients signed an informed consent. The subjects enrolled during the first 12 months of the first year (November 1, 2013 to October 31, 2014) were assigned to the control group, and those from the second year (November 1, 2014 to October 31, 2015) to the experimental group. The participants were blinded after assignment to interventions. The flow diagram of this study was shown in Figure 1. During the period of enrollment, there was no change of radiotherapy schema. Patients who were mentally incapacitated, with secondary or recurrent HNC, distant metastasis, skin cancer, congenital anomaly of the head and neck, chronic illness, or any previous or current psychiatric illness were excluded from the study. Those who had less than 20 teeth were also excluded. Those who were unable to answer the questionnaire due to senile dementia or severe intercurrent disease were also excluded. The hospitals staff who were not examiners, generated the allocation sequence, enrolled participants and assigned participants to experimental and control group.
Figure 1.
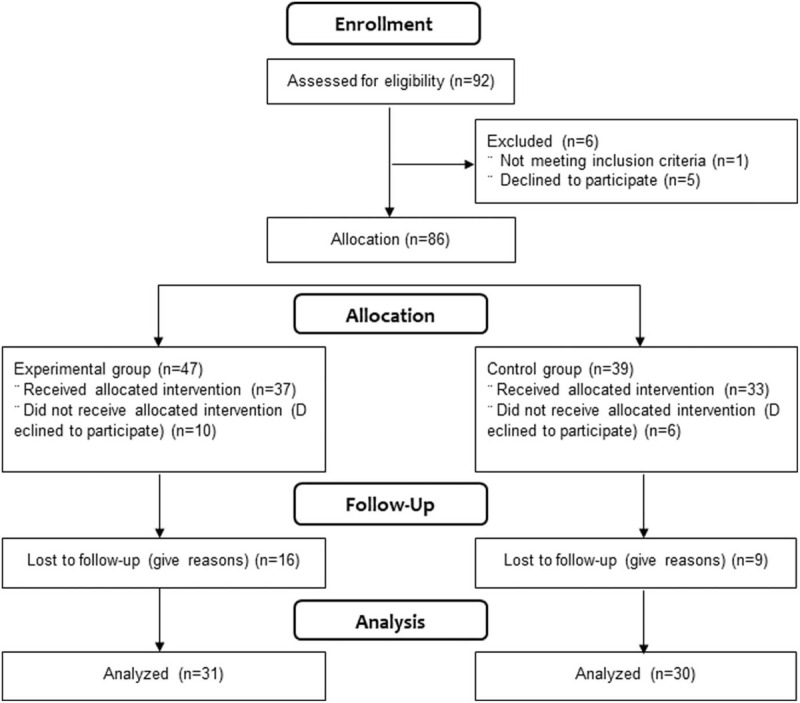
Flow diagram of study.
2.3. Training of the research assistant
The correspondence author oriented the first author as a research assistant regarding the study processes prior to the commencement of this study. The research assistant worked as a registered dental hygienist for 5 years in a dental clinic, was a doctoral candidate, and was blinded to the participants’ assignment to groups. The training lasted 3 hours daily over 5 days—and included the oral health education and measurement of variables related to this study. In addition, the correspondence author observed the research assistant periodically to ensure that education and measurement was performed correctly throughout the study.
2.4. Comprehensive oral care program
The experimental arm underwent 4 sessions of comprehensive oral care program before, immediately after, 3 months after, and 6 months after radiotherapy. The program consisted of oral health education, fluoride varnish application, and fluoride mouth rinsing. Oral health education was conducted by a dental hygienist and educated the patients and their caregivers about the oral care method to reduce the side effects caused by the radiotherapy. The contents of the education consisted of the reasons why oral care is important for HNC patients, definition and side effects of radiotherapy, toothbrush selection and tooth-brushing method, fluoride mouth-rinsing solution usage, diet, and denture cleaning and storing method. Separate educational booklets were provided after the training. The control group received only oral health education.
Five percent topical fluoride varnish application was done using CavityShield (CS, 3 M ESPE, St. Paul, MN, USA). It was applied to only the experimental group 3 times (before radiotherapy, immediate after radiotherapy, 3 months after radiotherapy). After the application, the patient was informed of the precautions and the effect was maintained.
Patients in the experimental group were given a 0.05% sodium fluoride solution, which was given before radiotherapy and up to 6 months after treatment. The method of use was to rinse the mouth with 10 to 15 ml of the solution once a day for 1 minute and to prevent rinsing the mouth for 30 minutes after brushing.
All the interventions were delivered when the participants visited a radiotherapy clinic for radiation treatment and follow-up and were conducted in a separate and independent room within the radiotherapy clinic. To increase compliance or participants, the participants were called to confirm before the date of the clinic visit.
2.5. Questionnaires
QoL was evaluated using questionnaires prepared by European Organization for Research and Treatment of Cancer Quality of Life Questionnaire H&N35 (EORTC QLQ-H&N35).[23] These questionnaires were completed during follow-up appointments in person. The results of the QoL questionnaires were analyzed according to the specific scoring manual provided by the EORTC,[24] all scores were expressed on a scale ranging between 0 to 100. The EORTC QLQ-H&N35 questionnaire consists of 7 multi-item symptom scales (pain, sensory problems, social contact problems, swallowing, social eating problems, speech problems, and reduced sexuality) and 11 single-item symptom scales (nutritional supplement use, mouth opening problems, teeth problems, coughing, painkiller use, weight loss, weight gain, sticky saliva, feeding tube, dry mouth, and feeling ill). Most items were rated on a 4-point scale ranging from 1 (“not at all”) to 4 (“very much”); 5 components used a binary response set (“yes” or “no”). Higher scores in the symptom scale amount to a higher level of symptomatology and a poor QoL.
2.6. Oral health examination
The oral examination was assessed at baseline and 6 months after radiotherapy with disposable plane mirror and World Health Organization (WHO) probe (Hu-Friedy, Chicago, IL). Dental caries experience, plaque score (PS), bleeding on probing (BOP), and salivary flow rate were evaluated by an experienced dentist. Dental caries was defined by WHO criteria.[25] The mean number of caries experience (decayed, missing due to caries, and filled due to caries) were calculated. O’Leary indices were examined to assess quantity of plaque. This index was calculated by dividing the number of plaque tooth surfaces by the total number of available tooth surfaces and multiplying by 100. BOP was measured at 6 sites (mesio-buccal, mid-buccal, disto-buccal, mesio-lingual/palatal, mid-lingual/palatal, and disto-lingual/palatal) per tooth for all teeth, excluding third molars. The percentage of BOP was calculated by dividing the number of sites with bleeding on probing by the number of sites explored and multiplying this value by 100. The stimulated whole saliva samples were obtained by chewing on wax blocks (Dentocult SM kits, Orion Diagnostica Co. Ltd, Epsom, Finland) for 5 minutes. Salivary flow rate was measured in ml/minutes.
2.7. Sociodemographic, Health behavior, and tumor site factors
We interviewed each participant about age, gender, education level (less than high school, high school, or more than college), occupation (white collar, blue collar, or unemployment), health behavior including smoking and drinking (never, former, or current). Tumor site was obtained from clinical chart.
2.8. Statistical analysis
Using G∗Power 3.0.10,[26] 27 participants were required for each group so that a medium effect size of 1.0 could be achieved. A two-sample t-test was performed at a 95% confidence interval and a significance level of 0.05. In consideration of the dropout rate, we included 46 participants in each group.
Data was entered and analyzed using the Statistical Package for the Social Sciences (SPSS) v23.0 (IBM SPSS Statistics, Armonk, NY). All statistical tests achieved a significance level of P < .05 for a bilateral significance. The baseline characteristics of groups were compared using independent t-test for continuous variable and Chi-Squared test for categorical variables. The effect of the oral health promotional intervention was assessed using paired t-tests with oral health (Dental caries, PS, BOP, and salivary flow rate). The mixed ANCOVA repeated-measures analysis to compare the QoL (EORTC QLQ-H&N35) between experimental and control group was performed. Age, gender, education, occupation, smoking, drinking, and tumor site were adjusted as covariates.
3. Results
3.1. Patients characteristics
During the course of the study, 15 patients in the experimental group withdrew from the study (5 were inappropriate for inclusion and 10 refused to participate further). Sixteen participants in the control group withdrew (9 were inappropriate for inclusion and 7 refused to participate further). Finally, there were a total of 61 participants in the study, with 31 in the experimental group and 30 in the control group; thus, the sample size was acceptable (Fig. 1). The age ranged between 33 to 81 years old at the time of inclusion. Among the 61 participants, the majority was male (n = 36; 59.0%). Three fourths received more than high school education (n = 46; 75.4%) and more than 4 fifths were blue collar or unemployed (n = 50; 82.0%). More than half were former or current smoker (n = 31; 50.8%) and former or current drinker (n = 36; 59.0%). The most prevalent primary tumor site was the oral cavity or oropharynx (n = 20; 32.8%). There were no statistical significances between experimental and control group among age, gender, education, occupation, smoking, drinking, and tumor site. The characteristics of the patients are summarized in Table 1.
Table 1.
Baseline (before radiotherapy) characteristics of participants, frequency (%).
| Characteristics | Experimental (n = 31) | Control (n = 30) | P |
| Age (yr), mean (standard deviation, SD) | 56.13 (12.84) | 59.30 (12.09) | .325∗ |
| Gender | |||
| Male | 19 (61.3) | 17 (56.7) | .714 |
| Female | 12 (38.7) | 13 (43.3) | |
| Education | |||
| ≤ middle school | 6 (19.4) | 9 (30.0) | .194 |
| High school | 11 (35.5) | 14 (46.7) | |
| ≥ College | 14 (45.2) | 7 (23.3) | |
| Occupation | |||
| White collar | 6 (19.4) | 5 (16.7) | .925 |
| Blue collar | 11 (35.5) | 10 (33.3) | |
| Unemployed | 14 (45.2) | 15 (50.0) | |
| Smoking | |||
| Never | 15 (48.4) | 15 (50.0) | .990 |
| Former | 14 (45.2) | 13 (43.3) | |
| Current | 2 (6.5) | 2 (6.7) | |
| Drinking | |||
| Never | 12 (38.7) | 13 (43.3) | .467 |
| Former | 18 (58.1) | 14 (46.7) | |
| Current | 1 (3.2) | 3 (10.0) | |
| Tumor site | |||
| Nasopharynx | 6 (19.4) | 5 (16.7) | .894 |
| Larynx | 6 (19.4) | 8 (26.7) | |
| Oral cavity+Oropharynx | 10 (32.3) | 10 (33.3) | |
| Others | 9 (29.0) | 7 (23.3) | |
3.2. Oral health status comparisons
In Table 2, caries experience showed a significant increase in control group (P = .006 by paired t-test) but non-significant in experimental group. PS and BOP showed significant decreases in experimental group (P < .001 for PS and P = .004 for BOP by paired t-test) but non-significant in control group. Salivary flow rate showed significant decreases in both experimental (P = .027 by paired t-test) and control group (P < .001).
Table 2.
Changes of oral health status.
| Experimental group (n = 31) | P | Control group (n = 30) | P | |||||
| Before | After 6 months | Δ (95% CI) | Before | After 6 months | Δ (95% CI) | |||
| Dental caries experience | 5.45 (5.64) | 5.45 (5.77) | 0.00 (−1.19, 1.19) | 1.000 | 6.37 (8.12) | 8.40 (8.27) | −2.03 (−3.44, −0.63) | .006 |
| Plaque score | 24.70 (22.23) | 5.90 (5.00) | 18.80 (11.02, 26.58) | <.001 | 15.74 (12.25) | 21.52 (20.61) | −5.78 (−13.01, 1.45) | .113 |
| Bleeding on probing | 8.41 (12.32) | 2.83 (6.64) | 5.58 (1.89, 9.26) | .004 | 8.85 (10.56) | 10.41 (13.25) | −1.56 (−5.19, 2.08) | .388 |
| Salivary flowrate | 1.18 (0.56) | 0.88 (0.41) | 0.30 (0.04, 0.57) | .027 | 1.29 (0.72) | 0.66 (0.42) | 0.63 (0.29, 0.98) | .001 |
3.3. EORTC QLQ-H&N35 score comparisons
Mean EORTC QLQ-H&N35 symptom scale scores are shown in Table 3. There were no significant QoL differences between the experimental and control groups except for swallowing (P = .035), speech problems (P = .034), and less sexuality (P = .005). While almost all symptoms in experimental group were the highest immediate post radiotherapy but gradually decreased after radiotherapy, symptoms such as less sexuality, teeth, and opening mouth in control group were increased gradually after radiotherapy.
Table 3.
Changes of EORTC QLQ-H&N35 scores, mean (SE).
| Experimental group (n = 31) | Control group (n = 30) | P | |||||||
| Before radiotherapy | Immediate after radiotherapy | 3 months after radiotherapy | 6 months after radiotherapy | Before radiotherapy | Immediate after radiotherapy | 3 months after radiotherapy | 6 months after radiotherapy | ||
| Pain | 19.57 (18.35) | 49.24 (26.09) | 24.88 (21.33) | 16.67 (8.74) | 18.52 (13.82) | 46.82 (32.77) | 21.62 (18.91) | 26.23 (28.65) | .328 |
| Swallowing | 19.05 (23.10) | 47.34 (27.07) | 18.11 (21.53) | 13.23 (12.88) | 12.04 (15.80) | 34.12 (32.96) | 21.62 (16.15) | 22.43 (26.80) | .035 |
| Senses problems | 14.28 (23.15) | 46.97 (21.60) | 27.53 (17.84) | 16.67 (16.67) | 13.89 (24.07) | 59.52 (30.46) | 32.61 (23.29) | 29.01 (29.45) | .251 |
| Speech problems | 17.57 (21.58) | 36.36 (26.15) | 14.49 (20.50) | 12.70 (15.43) | 18.83 (20.71) | 27.78 (31.04) | 27.02 (24.98) | 29.22 (29.09) | .034 |
| Social eating | 23.90 (28.03) | 39.01 (17.51) | 15.15 (14.69) | 20.24 (21.34) | 19.44 (25.59) | 42.26 (35.27) | 29.71 (21.44) | 37.03 (34.15) | .064 |
| Social contact | 15.66 (20.63) | 27.27 (26.50) | 8.55 (12.34) | 13.65 (19.26) | 19.63 (23.25) | 23.33 (31.78) | 19.70 (22.30) | 26.17 (31.64) | .470 |
| Less sexuality | 20.24 (32.20) | 38.59 (31.94) | 12.32 (16.06) | 15.87 (17.85) | 12.38 (17.78) | 27.38 (35.57) | 23.48 (27.53) | 29.48 (34.09) | .005 |
| Teeth | 27.90 (31.64) | 30.16 (29.63) | 26.08 (28.35) | 23.81 (30.08) | 37.14 (36.84) | 30.95 (27.62) | 39.39 (40.67) | 38.46 (34.88) | .672 |
| Opening mouth | 24.03 (33.59) | 43.94 (40.35) | 23.19 (32.46) | 25.39 (31.45) | 25.92 (32.96) | 33.33 (32.02) | 34.85 (34.85) | 48.71 (35.56) | .062 |
| Dry mouth | 31.74 (30.31) | 57.57 (31.17) | 49.27 (24.35) | 53.96 (28.82) | 33.33 (29.81) | 59.52 (32.50) | 65.21 (29.26) | 51.85 (31.12) | .347 |
| Sticky saliva | 23.01 (29.89) | 61.90 (26.42) | 43.47 (23.43) | 44.44 (33.88) | 22.22 (26.42) | 45.23 (42.58) | 49.27 (29.93) | 39.50 (30.71) | .217 |
| Coughing | 20.15 (23.16) | 37.88 (29.63) | 20.29 (24.07) | 25.39 (29.63) | 19.44 (18.47) | 43.59 (39.40) | 20.29 (19.43) | 18.52 (26.69) | .683 |
| Weight loss | 51.16 (50.58) | 54.55 (50.96) | 30.43 (47.05) | 33.33 (48.30) | 41.18 (49.96) | 50.00 (51.89) | 50.00 (51.18) | 44.44 (50.64) | .384 |
| Weight gain | 13.95 (35.06) | 23.81 (43.64) | 42.86 (50.71) | 28.57 (46.29) | 14.29 (35.50) | 21.43 (42.58) | 19.05 (40.24) | 22.22 (42.37) | .462 |
| Nutritional supplements | 34.88 (48.22) | 22.73 (42.89) | 47.83 (51.08) | 52.38 (51.18) | 34.29 (48.16) | 35.71 (49.72) | 27.27 (45.58) | 29.63 (46.53) | .332 |
| Feeding tube | 16.28 (37.35) | 9.52 (30.08) | 8.70 (28.81) | 4.76 (21.82) | 17.14 (38.24) | 15.38 (37.55) | 4.55 (21.32) | 14.81 (36.20) | .734 |
| Pain killers | 55.81 (50.25) | 54.55 (50.96) | 26.09 (44.90) | 9.52 (30.08) | 60.00 (49.71) | 50.00 (51.89) | 27.27 (45.58) | 44.44 (50.64) | .060 |
| Felt ill | 21.43 (30.19) | 33.33 (32.53) | 17.39 (22.18) | 12.70 (16.59) | 16.67 (23.23) | 38.46 (35.60) | 19.70 (24.47) | 25.92 (33.75) | .302 |
There was no adverse events reported as judged by the investigators in the experimental and control group.
4. Discussion
Our results suggest that preventive fluoride application protocols showed positive change in oral health status such as dental caries, dental plaque score, and gingival inflammation using paired t-test. The current standard protocol using topical fluoride, which is based on the study by Dreizen et al[27] has become a mainstay of preventive dental care in the HNC population. Fluoride may be administered in a number of ways such as fluoride custom tray,[28] brush on fluoride-containing toothpastes,[29] and fluoride varnish.[30] Compliance to oral preventive protocols is crucial to maintaining oral health. However, compliance with fluoride application in carriers by the population of patients with HNC is generally thought to be poor and may be due to the inconvenient method of application.[7] Therefore, the efficacy of fluoride may be limited in the HNC population due to the lack of calcium and phosphate secondary to hyposalivation,[31] patient adherence,[7] and poor health behavior.[32]
Previous study showed that oral hygiene alone is totally inadequate as a safeguard against radiotherapy-associated dental caries and addition of the fluoride gel to the caries preventive regimen was notably successful in stopping ongoing caries and in preventing new caries. The preventive effects of fluoride gel were through an increase in the caries resistance of the surface enamel or also included a fluoride-provoked change in the metabolic patterns of the plaque.[27]
Only 1 previous study[30] assessed the caries prevention effect of fluoride varnish in irradiated HNC patients. They found that with the three-month interval fluoride varnish application, the caries incremental rate was found to be 1.6/month for 15 months. However, it was seen that the rate of caries progression was slower initially, till first 6 months, that is, 1.3/month. The caries incremental rate increased after 6 months to 1.7/month, indicating that the progression of radiation caries is a late effect of radiotherapy. These findings support that the efficacy of fluoride might be limited in long-term oral care protocols. However, no control group for comparison was an important weakness of previous study. Our research may be the first clinical trial to assess the efficacy of fluoride varnish.
A “quasi-experimental case-control study design” is a between-subjects design in which participants have not been randomly assigned to conditions. If at the end of the study there was a difference in the 2 groups’ oral health outcome, it might be strong evidence for the efficacy of the intervention. However, providing treatment intervention to the experimental group, while providing control intervention to the control group at the same time, may not be blinded to both the patients and the investigators. Moreover, giving different intervention to the patients undergoing cancer therapy may affect the patients’ psychological state and this could be an important confounding of the study results. Therefore, the first year participants of our study were assigned to control group, and the next year were assigned to experimental group. This type of allocation made sure that the experimental and control groups did not overlap each other during study period, and at least, the participants were able to be blinded to the test.
In our data, salivary flow rate was decreased in both experimental and control group. According to the literature, xerostomia is prevalent condition in patients with cancer, related to both the disease and the oncologic treatment, not presenting any significant impact by the dental care provided.[33]
Although the preventive oral health effects of fluoride varnish were not evident in our study, we also examined whether the comprehensive oral care program may influence the EORTC QLQ-H&N35 score or not. According to our study, QoL-scores on all scales deteriorated during treatment, reaching the worst scores around end of radiotherapy and started to improve within 3 months later. Especially, swallowing, speech, and sexuality parameters of the EORTC QLQ-H&N35 module worsened at immediate after radiotherapy in both experimental and control group probably because of acute toxicities of treatment but recovered significantly over 6 months only in experimental group. Previous study showed that statistically significant and clinically relevant deteriorations were found on QLQ-H&N35 dry mouth and sticky saliva scales.[34] Another study found that a linear improvement over time was seen for social eating and social contacts and non-linear changes were seen for oral pain with improvement after treatment and deterioration afterwards and for senses with deterioration after treatment and improvement afterwards.[35] Patients with oral or oropharynx cancer had more sexual problems compared to patients with hypopharynx or larynx cancer,[35] while patients with hypopharynx or larynx cancer had more swallowing and speech problems.[36] In our study, the significant improvements in swallowing, speech, and sexuality parameters in experimental group might suggest that the implementation of comprehensive oral care program may contribute to improving QoL of HNC patients by reducing the negative impact of oral complications.
There are limitations inherent to this study. Small sample size, non-randomized clinical trial, short follow-up period (6 months), no information about diet consumption, and poor standardization of oral care protocol are limitations that may negatively affect the validity of clinical data. Additionally, there was no oral prophylaxis procedure before the commencement of the study which could interrupt the randomization. Hence, further well-designed randomized controlled trials are needed to reduce biases and identify the most effective approaches to prevent and manage oral complications and QoL in HNC patients.
5. Conclusion
In our study, comprehensive oral care intervention could prevent dental caries and increased quality of life in HNC patients. Radiation induced oral side effects are frequent complications and may generate significant impact on HNC patients’ long-term and overall QoL. To enable optimal dental care for HNC patients before, during and after radiotherapy, close interdisciplinary communication and cooperation among radiation oncologists, dentists, medical oncologists, and oral surgeons is absolutely essential. Clinicians should be equipped with knowledge about signs and symptoms of oral cavity so that appropriate clinical assessment and timely treatment referral can be made. Clinicians need to inform and educate HNC patients about
-
1.
potential risk of oral side effects after radiation-based therapy; and
-
2.
preventative strategies, for example, treatment of xerostomia-related complaints, meticulous oral hygiene, diet adaptation, control of cariogenic flora, and use of prescription-strength fluoride.
Compliance with preventative strategies must be reinforced by the health care team.
Author contributions
Conceptualization: Dong-Hun Han, Jin-Ho Kim, Hong-Gyun Wu.
Data curation: Hye-Ju Lee, Dong-Hun Han.
Formal analysis: Hye-Ju Lee, Dong-Hun Han.
Investigation: Hye-Ju Lee, Dong-Hun Han.
Methodology: Dong-Hun Han, Jin-Ho Kim.
Project administration: Dong-Hun Han, Jin-Ho Kim, Hong-Gyun Wu.
Supervision: Dong-Hun Han.
Validation: Dong-Hun Han.
Writing – original draft: Hye-Ju Lee.
Writing – review & editing: Dong-Hun Han, Jin-Ho Kim.
Footnotes
Abbreviations: BOP = bleeding on probing, EORTC QLQ-H&N35 = European Organization for Research and Treatment of Cancer Quality of Life Questionnaire H&N35, HNC = head and neck cancer, ORN = osteoradionecrosis, PS = plaque score, QoL = quality of life, SPSS = Statistical Package for the Social Sciences, WHO = World Health Organization.
How to cite this article: Lee HJ, Han DH, Kim JH, Wu HG. The effect of comprehensive oral care program on oral health and quality of life in patients undergoing radiotherapy for head and neck cancer: a quasi-experimental case-control study. Medicine. 2021;100:16(e25540).
D-HH and H-GW contributed equally to this work.
This work was supported by the Seoul National University Hospital (SNUH) Research Fund (No. 24-20130030) and the National Research Foundation of Korea (NRF) Grant funded by the Korean Government (MOE) (No. 2015R1D1A1A01061392).
The authors have no conflicts of interests to disclose.
The datasets generated during and/or analyzed during the current study are not publicly available, but are available from the corresponding author on reasonable request.
Obtained by independent t-test.
P values were obtained by Chi-Squared test.
P values were obtained by paired t-test.
Bold denotes statistical significance at P < .05
P values were obtained by mixed ANCOVA repeated-measures analysis adjusting for age, gender, education, occupation, smoking, drinking, and tumor site.
Bold denotes statistical significance at P < .05.
References
- [1].Jemal A, Bray F, Center MM, et al. Global cancer statistics. CA Cancer J Clin 2011;61:69–90. [DOI] [PubMed] [Google Scholar]
- [2].Brunotto M, Zarate AM, Bono A, et al. Risk genes in head and neck cancer: a systematic review and meta-analysis of last 5 years. Oral Oncol 2014;50:178–88. [DOI] [PubMed] [Google Scholar]
- [3].Johnson NW, Jayasekara P, Amarasinghe AA. Squamous cell carcinoma and precursor lesions of the oral cavity: epidemiology and aetiology. Periodontal 2000 2011;57:19–37. [DOI] [PubMed] [Google Scholar]
- [4].Mirghani H, Amen F, Moreau F, et al. Do high-risk human papillomaviruses cause oral cavity squamous cell carcinoma? Oral Oncol 2015;51:229–36. [DOI] [PubMed] [Google Scholar]
- [5].Epstein JB, Thariat J, Bensadoun RJ, et al. Oral complications of cancer and cancer therapy: from cancer treatment to survivorship. CA Cancer J Clin 2012;62:400–22. [DOI] [PubMed] [Google Scholar]
- [6].Deasy JO, Moiseenko V, Marks L, et al. Radiotherapy dose-volume effects on salivary gland function. Int J Radiat Oncol Biol Phys 2010;76:S58–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Deng J, Jackson L, Epstein JB, et al. Dental demineralization and caries in patients with head and neck cancer. Oral Oncol 2015;51:824–31. [DOI] [PubMed] [Google Scholar]
- [8].Benn AM, Thomson WM. Saliva: an overview. N Z Dent J 2014;110:92–6. [PubMed] [Google Scholar]
- [9].Nabil S, Samman N. Incidence and prevention of osteoradionecrosis after dental extraction in irradiated patients: a systematic review. Int J Oral Maxillofac Surg 2011;40:229–43. [DOI] [PubMed] [Google Scholar]
- [10].Langendijk JA, Doornaert P, Verdonck-de Leeuw IM, et al. Impact of late treatment-related toxicity on quality of life among patients with head and neck cancer treated with radiotherapy. J Clin Oncol 2008;26:3770–6. [DOI] [PubMed] [Google Scholar]
- [11].Oton-Leite AF, Elias LS, Morais MO, et al. Effect of low level laser therapy in the reduction of oral complications in patients with cancer of the head and neck submitted to radiotherapy. Spec Care Dentist 2013;33:294–300. [DOI] [PubMed] [Google Scholar]
- [12].Cheng KK, Molassiotis A, Chang AM, et al. Evaluation of an oral care protocol intervention in the prevention of chemotherapy-induced oral mucositis in paediatric cancer patients. Eur J Cancer 2001;37:2056–63. [DOI] [PubMed] [Google Scholar]
- [13].Cheng KK, Molassiotis A, Chang AM. An oral care protocol intervention to prevent chemotherapy-induced oral mucositis in paediatric cancer patients: a pilot study. Eur J Oncol Nurs 2002;6:66–73. [DOI] [PubMed] [Google Scholar]
- [14].Lalla RV, Bowen J, Barasch A, et al. MASCC/ISOO clinical practice guidelines for the management of mucositis secondary to cancer therapy. Cancer 2014;120:1453–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Eduardo Fde P, Bezinelli LM, de Carvalho DL. Oral mucositis in pediatric patients undergoing hematopoietic stem cell transplantation: clinical outcomes in a context of specialized oral care using low-level laser therapy. Pediatr Transplant 2015;19:316–25. [DOI] [PubMed] [Google Scholar]
- [16].Kubota K, Kobayashi W, Sakaki H. Professional oral health care reduces oral mucositis pain in patients treated by superselective intra-arterial chemotherapy concurrent with radiotherapy for oral cancer. Support Care Cancer 2015;23:3323–9. [DOI] [PubMed] [Google Scholar]
- [17].Sbaraini A, Evans RW. Caries risk reduction in patients attending a caries management clinic. Aust Dent J 2008;53:340–8. [DOI] [PubMed] [Google Scholar]
- [18].Evans RW, Pakdaman A, Dennison PJ, et al. The caries management system: an evidence-based preventive strategy for dental practitioners. Application for adults. Aust Dent J 2008;53:83–92. [DOI] [PubMed] [Google Scholar]
- [19].Sheiham A, James WP. A new understanding of the relationship between sugars, dental caries and fluoride use: implications for limits on sugars consumption. Public Health Nutr 2014;17:2176–84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Gao SS, Zhang S, Mei ML, et al. Caries remineralisation and arresting effect in children by professionally applied fluoride treatment - a systematic review. BMC Oral Health 2016;16:12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Tolentino Ede S, Centurion BS, Ferreira LH, et al. Oral adverse effects of head and neck radiotherapy: literature review and suggestion of a clinical oral care guideline for irradiated patients. J Appl Oral Sci 2011;19:448–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Hancock PJ, Epstein JB, Sadler GR. Oral and dental management related to radiation therapy for head and neck cancer. J Can Dent Assoc 2003;69:585–90. [PubMed] [Google Scholar]
- [23].EORTC. Head & Neck Cancer (Update of QLQ-H&N35). Available at: https://qol.eortc.org/questionnaire/qlq-hn43/. [Google Scholar]
- [24].Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for research and treatment of cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst 1993;85:365–76. [DOI] [PubMed] [Google Scholar]
- [25].WHO. Oral health surveys. Basic methods. 4th Edition. World Health Organization, 1997. pp. 36–44. [Google Scholar]
- [26].Faul F, Erdfelder E, Lang AG, et al. G∗Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods 2007;39:175–91. [DOI] [PubMed] [Google Scholar]
- [27].Dreizen S, Brown LR, Daly TE, et al. Prevention of xerostomia-related dental caries in irradiated cancer patients. J Dent Res 1977;56:99–104. [DOI] [PubMed] [Google Scholar]
- [28].Frydrych AM, Slack-Smith LM, Parsons R. Compliance of post-radiation therapy head and neck cancer patients with caries preventive protocols. Aust Dent J 2017;62:192–9. [DOI] [PubMed] [Google Scholar]
- [29].Thariat J, Ramus L, Darcourt V, et al. Compliance with fluoride custom trays in irradiated head and neck cancer patients. Support Care Cancer 2012;20:1811–4. [DOI] [PubMed] [Google Scholar]
- [30].Dholam KP, Somani PP, Prabhu SD, et al. Effectiveness of fluoride varnish application as cariostatic and desensitizing agent in irradiated head and neck cancer patients. Int J Dent 2013;2013:824982. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [31].Cochrane NJ, Cai F, Huq NL, et al. New approaches to enhanced remineralization of tooth enamel. J Dent Res 2010;89:1187–97. [DOI] [PubMed] [Google Scholar]
- [32].Lockhart PB, Clark J. Pretherapy dental status of patients with malignant conditions of the head and neck. Oral Surg Oral Med Oral Pathol 1994;77:236–41. [DOI] [PubMed] [Google Scholar]
- [33].Funk CS, Warmling CM, Baldisserotto J. A randomized clinical trial to evaluate the impact of a dental care program in the quality of life of head and neck cancer patients. Clin Oral Invest 2014;18:1213–9. [DOI] [PubMed] [Google Scholar]
- [34].Al-Mamgani A, van Rooij P, Tans L, et al. A prospective evaluation of patient-reported quality-of-life after (chemo) radiation for oropharyngeal cancer: which patients are at risk of significant quality-of-life deterioration? Radiother Oncol 2013;106:359–63. [DOI] [PubMed] [Google Scholar]
- [35].Verdonck-de Leeuw IM, Buffart LM, Heymans MW, et al. The course of health-related quality of life in head and neck cancer patients treated with chemoradiation: a prospective cohort study. Radiother Oncol 2014;110:422–8. [DOI] [PubMed] [Google Scholar]
- [36].Rinkel RN, Verdonck-de Leeuw IM, van den Brakel N. Patient-reported symptom questionnaires in laryngeal cancer: voice, speech and swallowing. Oral Oncol 2014;50:759–64. [DOI] [PubMed] [Google Scholar]