

PURPOSE
Immunotherapy has revolutionized the treatment of advanced non–small-cell lung cancer (NSCLC). In two phase III trials (CheckMate 017 and CheckMate 057), nivolumab showed an improvement in overall survival (OS) and favorable safety versus docetaxel in patients with previously treated, advanced squamous and nonsquamous NSCLC, respectively. We report 5-year pooled efficacy and safety from these trials.
METHODS
Patients (N = 854; CheckMate 017/057 pooled) with advanced NSCLC, ECOG PS ≤ 1, and progression during or after first-line platinum-based chemotherapy were randomly assigned 1:1 to nivolumab (3 mg/kg once every 2 weeks) or docetaxel (75 mg/m2 once every 3 weeks) until progression or unacceptable toxicity. The primary end point for both trials was OS; secondary end points included progression-free survival (PFS) and safety. Exploratory landmark analyses were investigated.
RESULTS
After the minimum follow-up of 64.2 and 64.5 months for CheckMate 017 and 057, respectively, 50 nivolumab-treated patients and nine docetaxel-treated patients were alive. Five-year pooled OS rates were 13.4% versus 2.6%, respectively; 5-year PFS rates were 8.0% versus 0%, respectively. Nivolumab-treated patients without disease progression at 2 and 3 years had an 82.0% and 93.0% chance of survival, respectively, and a 59.6% and 78.3% chance of remaining progression-free at 5 years, respectively. Treatment-related adverse events (TRAEs) were reported in 8 of 31 (25.8%) nivolumab-treated patients between 3–5 years of follow-up, seven of whom experienced new events; one (3.2%) TRAE was grade 3, and there were no grade 4 TRAEs.
CONCLUSION
At 5 years, nivolumab continued to demonstrate a survival benefit versus docetaxel, exhibiting a five-fold increase in OS rate, with no new safety signals. These data represent the first report of 5-year outcomes from randomized phase III trials of a programmed death-1 inhibitor in previously treated, advanced NSCLC.
INTRODUCTION
Historically, 5-year survival rates of patients with advanced non–small-cell lung cancer (NSCLC) who received chemotherapy were < 5%.1 Effective treatment options for patients without targetable molecular alterations, particularly for those who progressed after first-line chemotherapy, were limited until recently. With clinically meaningful survival benefits, durable responses, and favorable safety profiles versus chemotherapy, immune checkpoint inhibitors have become the standard of care for patients who progressed on or after platinum-based chemotherapy.2-7 Immune checkpoint inhibitors are also effective as first-line treatment and are recommended, with or without chemotherapy, as the standard of care for treatment-naive patients with advanced NSCLC.8-14
CONTEXT
Key Objective
Immune checkpoint inhibitors have improved patient survival versus chemotherapy in previously treated, advanced non–small-cell lung cancer (NSCLC). However, data on long-term outcomes are limited. Using pooled data from two randomized phase III clinical trials (CheckMate 017 and CheckMate 057), we assessed 5-year efficacy and safety outcomes with nivolumab versus chemotherapy in this setting.
Knowledge Generated
Based on these first 5-year results of programmed death-1 inhibitors from phase III clinical trials in the previously treated, advanced NSCLC setting, patients derived long-term survival benefit and durable responses with nivolumab versus chemotherapy, regardless of histology and PD-L1 expression. Nivolumab maintained a favorable safety profile in this patient population; no new safety signals were identified. Furthermore, some patients experienced prolonged disease control even after stopping nivolumab.
Relevance
With the longest follow-up to date for randomized phase III trials of programmed death-1 inhibitors in previously treated, advanced NSCLC, these results represent an important advancement in the treatment of lung cancer and help inform clinical decisions.
Nivolumab, a fully human, monoclonal, antiprogrammed death-1 (PD-1) antibody, was the first PD-1 inhibitor to demonstrate clinically meaningful activity in NSCLC.15 Nivolumab is approved in the United States, the European Union, and other countries for second-line treatment of advanced NSCLC, based on improved overall survival (OS) and a favorable safety profile versus docetaxel in two randomized, open-label, phase III trials in advanced squamous (CheckMate 017; NCT01642004) and nonsquamous (CheckMate 057; NCT01673867) NSCLC with disease progression following platinum-based chemotherapy.4,5,16,17
At 2-, 3-, and 4-year follow-ups, OS rate and progression-free survival (PFS) rate from these trials continued to favor nivolumab over docetaxel, with no new safety signals identified for nivolumab.18-20 Here, we present the pooled 5-year survival and safety data from CheckMate 017 and 057, representing the longest follow-up to date for randomized phase III trials of an immune checkpoint inhibitor in previously treated, advanced NSCLC.
METHODS
Patients
Eligibility criteria for both trials have been previously described.4,5
Study Design
CheckMate 017 (previously treated squamous NSCLC) and CheckMate 057 (previously treated nonsquamous NSCLC) were international, randomized, open-label, phase III trials. Patients were randomly assigned 1:1 to receive nivolumab (3 mg/kg once every 2 weeks) or docetaxel (75 mg/m2 once every 3 weeks) in both trials (Appendix Fig A1, online only). Random assignment was stratified by prior paclitaxel use and geographical location in CheckMate 017 and by prior maintenance treatment and line of therapy (second v third) in CheckMate 057.
Treatment continued until disease progression, unacceptable toxicity, or other protocol-specified reasons. Further details on treatment beyond progression in the nivolumab group and crossover in the docetaxel group are given in the Appendix (online only).
Both trials were conducted in accordance with the International Conference on Harmonisation Good Clinical Practice Guidelines and the Declaration of Helsinki. An institutional review board or independent ethics committee at each site approved the trial Protocols (online only). All patients provided written informed consent.
Assessments
Tumor assessments were performed by investigators according to RECIST v1.1 at baseline, at 9 weeks, every 6 weeks thereafter during the first year of treatment, and then every 12 weeks until disease progression or discontinuation of therapy in patients receiving nivolumab beyond progression. Patients were followed continuously for survival while receiving treatment and every 3 months after discontinuation.
Safety was assessed throughout the treatment period and at two follow-up visits, which occurred within 100 days of last dose or before the start of crossover treatment. Beyond 100 days from the last dose of treatment, patients with ongoing treatment-related adverse events (TRAEs) were followed until the TRAE resolved, returned to baseline, or was deemed irreversible. The severity of adverse events (AEs) was graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events (version 4.0). Select AEs were defined as having a potential immunologic cause that may require management through immune-modulating medication.
Archival or recent pretreatment tumor biopsy specimens were assessed for expression of PD-1 ligand 1 (PD-L1) protein at a central laboratory using a validated automated immunohistochemical assay (PD-L1 IHC 28-8 pharmDx; Dako, Carpinteria, CA) as previously described.4,5
Statistical Analyses
Efficacy and safety were assessed in all randomly assigned patients and in all patients who received at least one dose of the trial drug, respectively, using pooled data from CheckMate 017 and 057 studies. The primary end point was OS for both studies; secondary end points included objective response rate (ORR), PFS, and efficacy by tumor PD-L1 expression. Data for these end points have been previously reported.4,5 To investigate the impact of progression-free status on long-term survival, an exploratory landmark analysis of OS at 5 years based on progression-free status at 2, 3, and 4 years was performed. The probability of patients remaining progression-free at later timepoints based on their progression-free status at 2, 3, and 4 years was also assessed.
Survival curves and rates, landmark analyses, and duration of response (DOR) were estimated using the Kaplan-Meier method. Hazard ratios (HRs) and CIs were estimated using a Cox proportional hazard model.
RESULTS
At the database locks (May 8, 2019, for CheckMate 017 and May 16, 2019, for CheckMate 057) for this analysis, the minimum follow-up was 64.2 months and 64.5 months, respectively; the corresponding median follow-up was 69.5 months and 69.4 months.
Patients and Treatment
Baseline characteristics of patients randomly assigned to nivolumab (CheckMate 017: n = 135; CheckMate 057: n = 292) and docetaxel (CheckMate 017: n = 137; CheckMate 057: n = 290) were generally well balanced (Appendix Table A1, online only).4,5,18-20
Patient disposition is summarized in the Appendix Figure A2, online only. Following a protocol amendment, 23 nivolumab-treated patients transitioned to nivolumab 480 mg once every 4 weeks.20 Of 427 docetaxel-treated patients, 23 crossed over to receive nivolumab 3 mg/kg once every 2 weeks. Two of these patients subsequently received nivolumab 480 mg once every 4 weeks per protocol amendments. At 5 years, 50 of 427 patients randomly assigned to nivolumab and 9 of 427 patients randomly assigned to docetaxel were still alive; 18 of 418 (4.3%) nivolumab-treated patients remained on treatment for ≥ 5 years; no patients remained on docetaxel. The median (range) number of nivolumab (3 mg/kg) and docetaxel doses in CheckMate 017 was 8.0 (1-151) and 3.0 (1-29), respectively, and in CheckMate 057, the median (range) was 6.0 (1-139) and 4.0 (1-23), respectively.
OS
In the pooled CheckMate 017/057 population, OS remained longer with nivolumab versus docetaxel (HR: 0.68; 95% CI, 0.59 to 0.78). Pooled 5-year OS rates were 13.4% (95% CI, 10.4 to 16.9) with nivolumab versus 2.6% (95% CI, 1.4 to 4.5) with docetaxel (Fig 1A). Consistent with previous reports, most deaths between 3 and 5 years with nivolumab (12 of 14 deaths) and docetaxel (20 of 23 deaths) were due to disease.18,19
FIG 1.
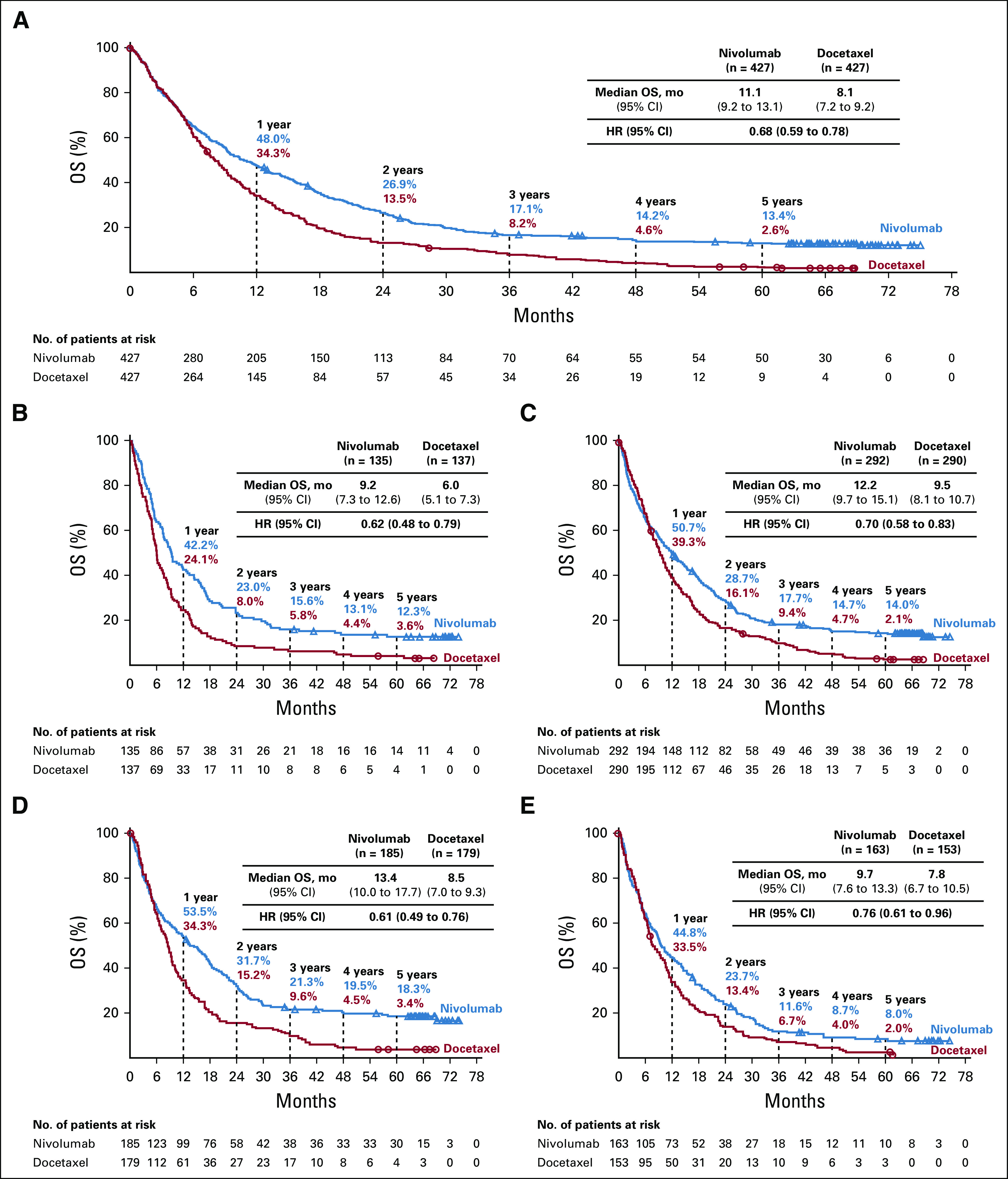
OS of all treated patients: (A) overall, (B) by SQ tumor histology, (C) by NSQ tumor histology, (D) by ≥ 1% PD-L1 expression, and (E) by < 1% PD-L1 expression. Minimum follow-up: CheckMate 017: 64.2 months; CheckMate 057: 64.5 months. HR, hazard ratio; mo, months; No., number; NSQ, nonsquamous; OS, overall survival; PD-L1, programmed death ligand 1; SQ, squamous.
Pooled OS rates at 5 years were similar with squamous and nonsquamous histology: 12.3% (95% CI, 7.4 to 18.5) and 14.0% (95% CI, 10.2 to 18.3) with nivolumab and 3.6% (95% CI, 1.4 to 7.8) and 2.1% (95% CI, 0.9 to 4.4) with docetaxel, respectively (Figs 1B and 1C). OS benefit continued to be observed with nivolumab versus docetaxel regardless of tumor PD-L1 expression (Figs 1D and 1E); 5-year OS rates were 18.3% (95% CI, 13.0 to 24.2) versus 3.4% (95% CI, 1.4 to 6.8) in patients with PD-L1 expression ≥ 1% and 8.0% (95% CI, 4.4 to 13.0) versus 2.0% (95% CI, 0.5 to 5.3) in those with PD-L1 expression < 1%.
OS benefit was observed with nivolumab across several subgroups, including patients with baseline liver metastases (HR, 0.67 [95% CI, 0.50 to 0.89]), adrenal metastases (HR, 0.41 [95% CI, 0.27 to 0.60]), neutrophil-to-lymphocyte ratio < median (HR, 0.63 [95% CI, 0.51 to 0.77]), lactate dehydrogenase ≥ upper limit of normal (HR, 0.74 [95% CI, 0.59 to 0.93]), and those with no baseline proton pump inhibitor use (HR, 0.61 [95% CI, 0.51 to 0.72]; Appendix Fig A3, online only).
PFS
PFS rates consistently favored nivolumab versus docetaxel over time (Fig 2A). Pooled 5-year PFS rates were 8.0% (95% CI, 5.4 to 11.2) with nivolumab and 0% with docetaxel. PFS rates by histology and for patients with PD-L1 expression ≥ 1% and < 1% are shown in the Appendix Figure A4, online only.
FIG 2.
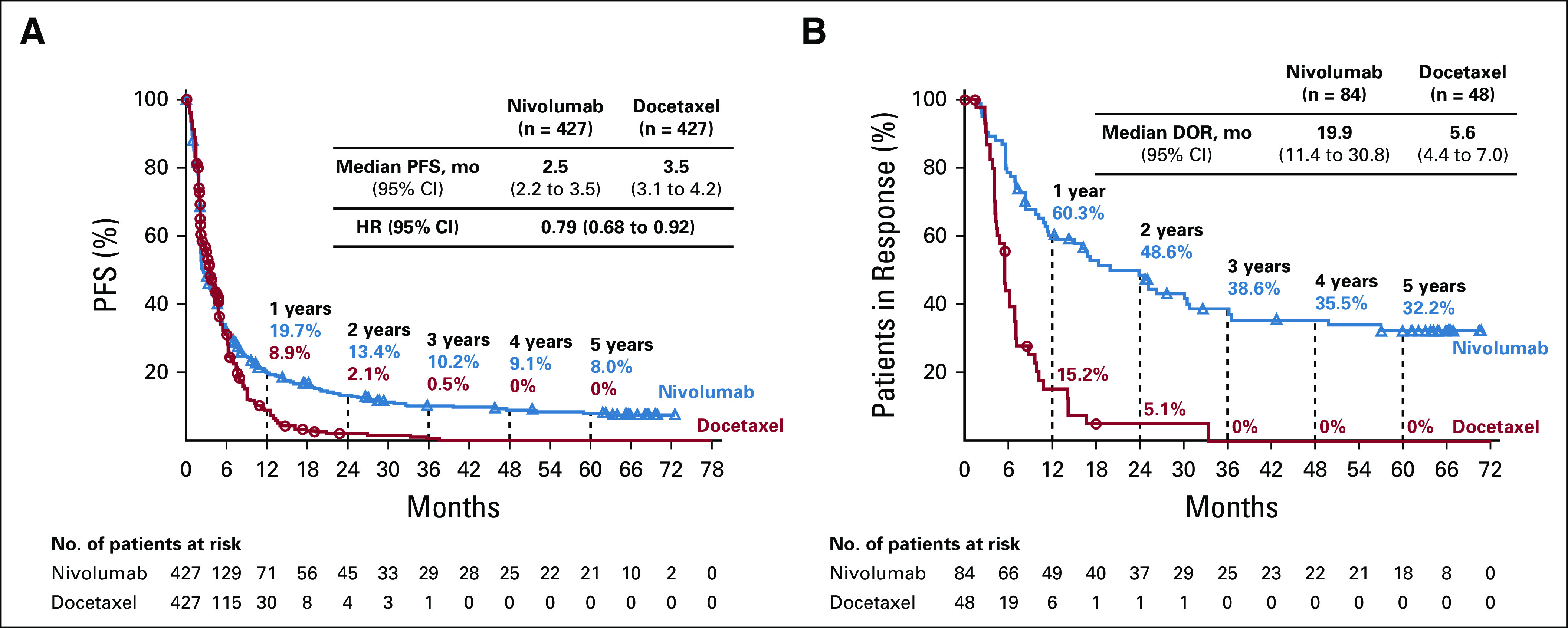
(A) PFSa and (B) DORa among all treated patients. aPer local investigator; minimum follow-up: CheckMate 017: 64.2 months; CheckMate 057: 64.5 months. Since the primary analysis of the CheckMate 057 trial, one patient's response changed from SD to PR and one from PR to CR. DOR for these two patients was determined according to their latest response category. DOR, duration of response; HR, hazard ratio; mo, months; No., number; PFS, progression-free survival.
Landmark Survival Analyses
Landmark analysis of PFS and OS by progression-free status at 2, 3, and 4 years showed that a high proportion of nivolumab-treated patients remained progression-free during subsequent years and had long-term OS benefits (Fig 3). Patients who were progression-free at 2 years (n = 45), 3 years (n = 29), and 4 years (n = 25) had a 59.6%, 78.3%, and 87.5% chance of being progression-free at 5 years, respectively, and an 82.0%, 93.0%, and 100.0% chance of survival at 5 years, respectively. In the docetaxel arm, patients who were progression-free at 2 years (n = 4) and 3 years (n = 1) had a 0% chance of being progression-free at 5 years and a 0% chance of survival at 5 years; no patients were progression-free at 4 years.
FIG 3.
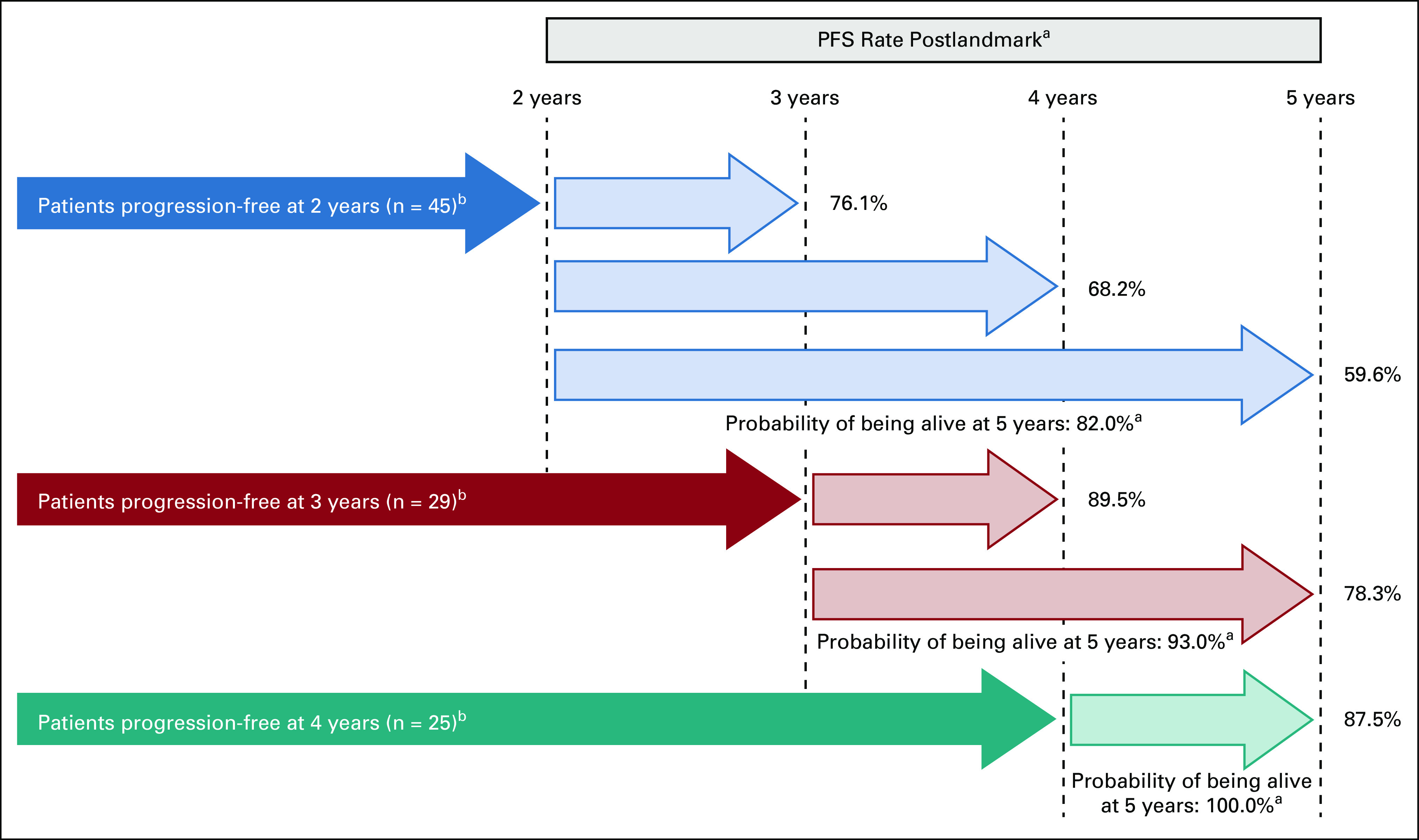
PFS and OS landmark analyses by PFS at 2, 3, and 4 years. aBased on Kaplan-Meier estimates; bNumber of patients at risk. OS, overall survival; PFS, progression-free survival.
Tumor Response
Consistent with previous reports,4,5,18,19 the pooled ORR was higher with nivolumab (19.7% [95% CI, 16.0 to 23.8]) than docetaxel (11.2% [95% CI, 8.4 to 14.6]; Appendix Table A2, online only). Since the primary analysis of CheckMate 057, one patient treated with nivolumab improved from stable disease to partial response (PR) and another, also treated with nivolumab, improved from PR to complete response (CR). No patients from CheckMate 017 experienced a change in the response since the primary analysis.
Median DOR was longer with nivolumab (19.9 months [95% CI, 11.4 to 30.8]) versus docetaxel (5.6 months [95% CI, 4.4 to 7.0]) in the pooled population. Longer DOR with nivolumab was observed regardless of histology or tumor PD-L1 expression (Appendix Fig A5, online only). The pooled 5-year DOR rate with nivolumab was 32.2% (95% CI, 21.9 to 43.0); no patients in the docetaxel arm had ongoing responses at 5 years (Fig 2B).
5-Year Survivors
Baseline characteristics of patients who survived ≥ 5 years in the nivolumab arm (n = 50) and docetaxel arm (n = 9) were generally similar to the overall population and those who survived < 1 year (n = 222 and n = 282, respectively), despite numerical differences in ECOG PS 0 (in both arms), PD-L1 expression ≥ 1% (nivolumab arm), and stage IIIB NSCLC (docetaxel arm; Appendix Fig A3).
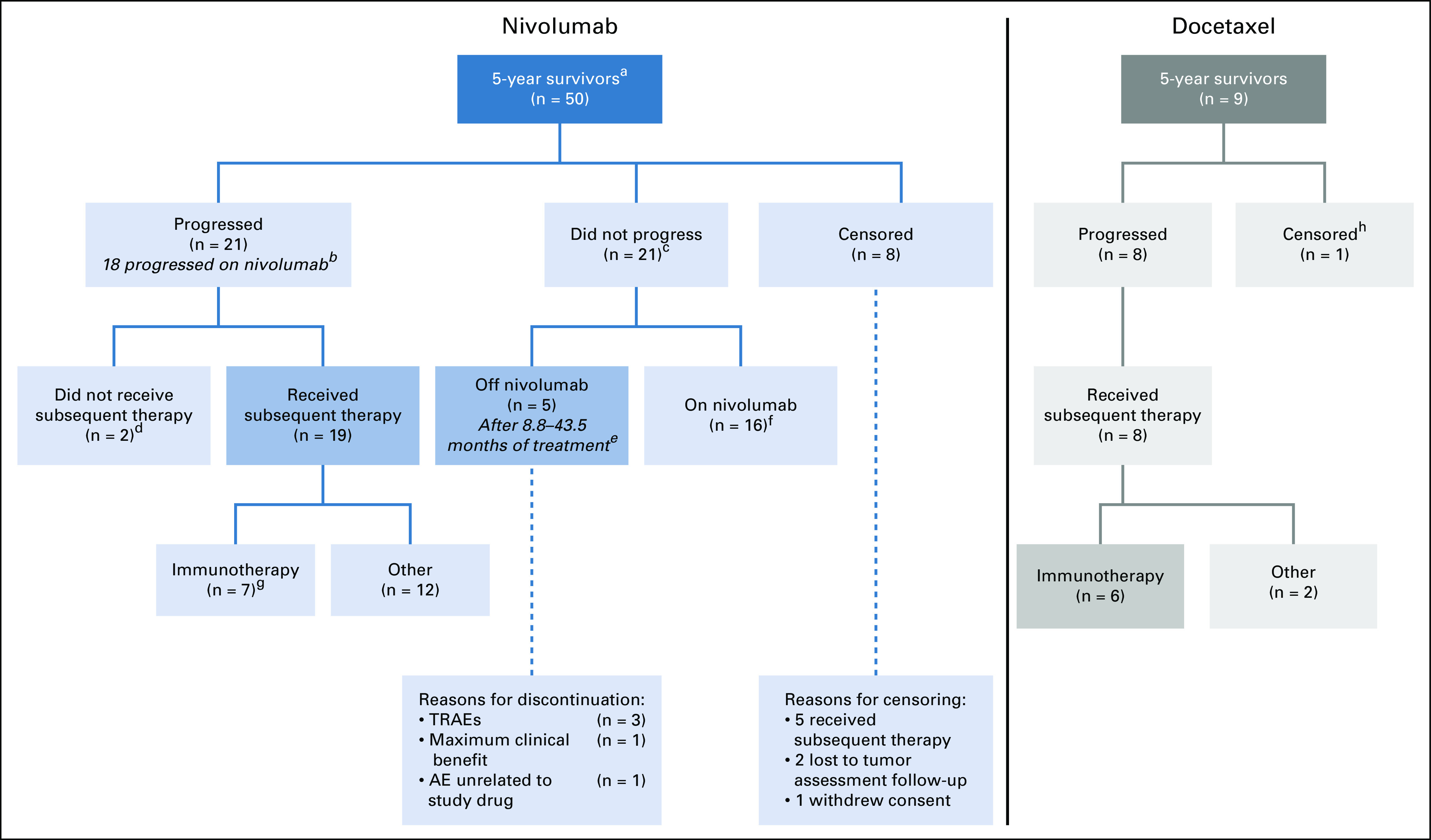
Among the 50 patients who survived ≥ 5 years in the nivolumab arm (including 18 who had switched to nivolumab 480 mg once every 4 weeks), 21 (42.0%) had not progressed by 5 years and 21 (42.0%) had progressed (Fig 5A; Appendix Fig A6, online only), and eight (16.0%) had been censored for PFS. The median (range) duration of treatment for nivolumab and docetaxel in 5-year survivors was 36.9 months (1.8-76.2+ months) and 3.5 months (0.7-20.0 months), respectively; 35 patients received nivolumab treatment for ≥ 2 years and 18 remained on nivolumab at 5 years. Of the 32 patients who had discontinued nivolumab, the median duration of treatment was 27.7 months. Aside from disease progression, reasons for discontinuation included TRAEs, AEs unrelated to the study drug, or maximum clinical benefit.
FIG 5.
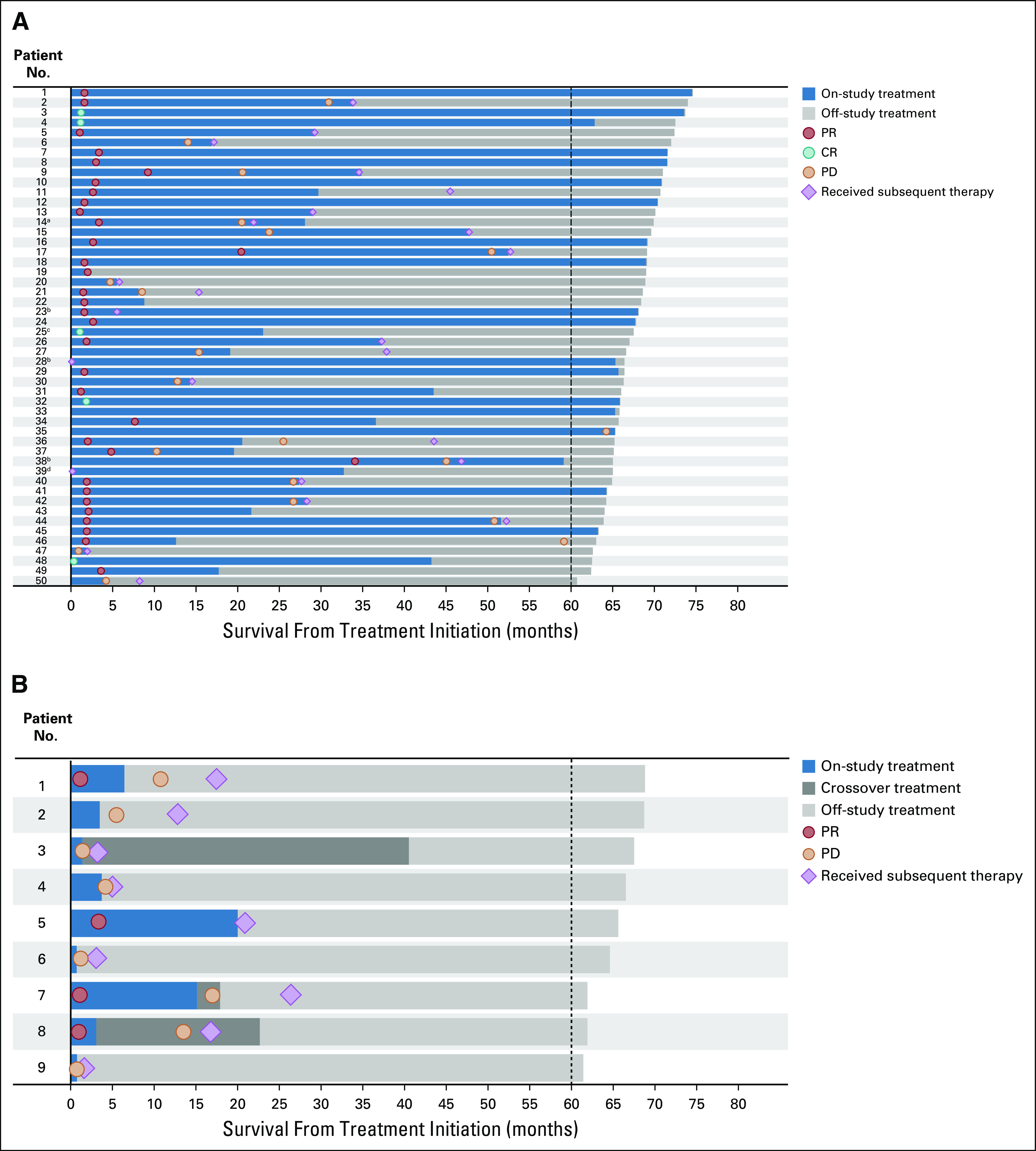
Treatment status of ≥ 5-year survivors treated with (A) nivolumab and (B) docetaxel. Timing of only the first administered subsequent therapy is noted, patients may have received ≥ 1 subsequent treatment. aPatient received radiotherapy prior to discontinuation of nivolumab; bPatient received radiotherapy in addition to nivolumab; cPatient withdrew consent, and so subsequent treatment status is unknown. dPatient response note reported. CR, complete response; No., number; PD, progressive disease; PR, partial response.
Of the patients who survived ≥ 5 years in the nivolumab arm (n = 50), 5 patients had CRs and 34 patients had PRs. A total of eight and three patients had stable and progressive disease, respectively. In the docetaxel arm, four of the 5-year survivors (n = 9) had a PR, two patients had stable disease, and three patients had progressive disease. No docetaxel-treated survivors had a CR.
A total of 24 nivolumab-treated patients were known to receive subsequent therapy, of whom 10 had subsequent immunotherapy (Appendix Tables A4 and A5, online only). At 5 years, 5 of 50 nivolumab-treated patients were progression-free and did not require subsequent therapy (Appendix Fig A6); reasons for discontinuing nivolumab (after 8.8-43.5 months of treatment) were TRAEs (n = 3), maximum clinical benefit (n = 1), and AE unrelated to study drug (n = 1). Among the 9 patients who survived ≥ 5 years in the docetaxel arm (including two patients who crossed over to receive nivolumab 3 mg/kg once every 2 weeks and one who received 3 mg/kg and 480 mg once every 4 weeks), eight had progressed and one was censored for PFS. All nine patients received subsequent therapy; four had subsequent immunotherapy (excluding patients who crossed over to nivolumab; Appendix Table A4; Fig 5B).
Safety
No patients received treatment with docetaxel for more than 2 years; therefore, updated safety data as of the 5-year follow-up are presented only for patients who received nivolumab. At 5 years, 284 of 418 patients (67.9%) treated with nivolumab experienced TRAEs; 45 patients (10.8%) had grade 3-4 events. No new safety signals were observed. Between 3- and 5-year minimum follow-ups, eight of 31 patients (25.8%) still receiving nivolumab had TRAEs (Table 1), of whom one patient (3.2%) had a grade 3 event (increased lipase); there were no grade 4 events. A total of 13 different events were reported in these 8 patients between 3 and 5 years of treatment, of which three events were recurrent (nummular eczema, pruritus, and rash occurring in one patient each).
TABLE 1.
Treatment-Related Adverse Events With Nivolumab (Overall and at 3-5 Years' Follow-Up)

Overall, 27 (6.5%) nivolumab-treated patients experienced TRAEs of any grade leading to discontinuation; the most common (in ≥ 2 patients) were pneumonitis (n = 6; 1.4%) and interstitial lung disease (n = 3; 0.7%), and colitis, increased alanine aminotransferase, increased AST, and rash (n = 2; 0.5%). Since the 3-year follow-up, one patient in the nivolumab arm experienced a TRAE, leading to discontinuation (grade 2 nummular eczema).19 At the time of database lock, no new treatment-related deaths had occurred since the primary analyses (n = 1 in the nivolumab arm and n = 4 in the docetaxel arm).4,5
Consistent with previous reports, few treatment-related select AEs occurred after the 3-year minimum follow-up (Fig 4).18,19 Of the 31 patients who remained on treatment with nivolumab between 3 and 5 years of follow-up, five patients (16.1%) experienced treatment-related select AEs: four patients (12.9%) with skin or subcutaneous tissue disorders (one each of grade 1-2 erythema, pruritus, rash, and skin exfoliation) and two patients (6.5%) with a GI disorder (grade 1-2 diarrhea). A total of eight different events were reported in these five patients between 3 and 5 years of treatment, of which two events were recurrent (pruritus and rash occurring in one patient each).
FIG 4.

Patients on treatment with first treatment-related select AE by yeara,b. Median (range) nivolumab treatment duration: 2.8 (0-76.2 +) months. aIncludes events of any grade reported between the first dose and 30 days after the last dose of trial therapy; bSelect AEs were events with a potential immunological cause. AE, adverse event; No., number.
DISCUSSION
This is the longest follow-up to date for randomized phase III trials of a PD-1 inhibitor in previously treated, advanced NSCLC. After a 5-year minimum follow-up in the CheckMate 017 and 057 studies, nivolumab continued to demonstrate clinically meaningful OS, PFS, and DOR benefits versus docetaxel and maintained a favorable safety profile. The pooled 5-year OS rate was 13.4% with nivolumab, representing a five-fold increase over docetaxel (2.6%). These findings are consistent with previously reported 5-year and 6-year OS rates with nivolumab among patients with previously treated, advanced NSCLC in CheckMate 003 trial (15.6% and 14.7%, respectively).21 The OS rates detailed here are also similar to the five-year OS rates observed in the single-arm, phase I trial of pembrolizumab in patients with previously treated NSCLC (15.5%).22 OS benefit with nivolumab versus docetaxel was observed regardless of tumor histology. Notably, OS benefit (HR < 1) was observed with nivolumab versus docetaxel in patients with tumor PD-L1 expression ≥ 1% (5-year OS rates, 18.3% v 3.4%) or < 1% (8.0% v 2.0%) and across a variety of patient subgroups, demonstrating the potential for nivolumab to improve outcomes in a diverse patient population. In this analysis, no baseline clinical or tumor characteristics were identified to clearly distinguish long-term or short-term survivors in either treatment arm and, because of the disparity in sample sizes across treatment arms, multivariate analysis was not considered appropriate; only nine patients were alive in the docetaxel group at 5 years, making subgroup analysis unfeasible.
The pooled 5-year PFS rate with nivolumab versus docetaxel (8.0% and 0%, respectively) was consistent with previous analyses.20 Notably, the majority of patients without disease progression at 2, 3, and 4 years after treatment with nivolumab remained progression-free at 5 years and survived ≥ 5 years. Although exploratory, these findings provide new information about the probability of remaining progression-free at subsequent timepoints and alive at 5 years, by progression-free status at 2, 3, and 4 years. This analysis provides insight into long-term efficacy outcomes and management of previously treated, advanced NSCLC following treatment with nivolumab. Consistent with the 2- and 3-year follow-ups, responses achieved with nivolumab were durable;18,19 nearly one-third of patients who achieved an objective response had ongoing responses at 5 years versus none with docetaxel. The 5-year timepoint is considered a clinical landmark to evaluate long-term survival, and data beyond 5 years are scarce; a longer follow-up may be required to assess the outcomes of these patients.23
In both this analysis and a pooled analysis across four nivolumab trials in previously treated NSCLC, the proportion of nivolumab-treated patients who remained alive appeared to stabilize at approximately 3 years and plateau thereafter.20 A similar observation was noted in a pooled analysis of ipilimumab in patients with unresectable or advanced melanoma, where the survival curve extended beyond 5 years.24 This suggests that long-term survival beyond 5 years may also be possible in NSCLC; however, this remains to be addressed in future analyses. Indeed, patients with previously treated NSCLC who received nivolumab in CheckMate 003, which has the longest survival follow-up to date among trials of PD-1 inhibitors in previously treated, advanced NSCLC, exhibited similar OS rates at 4, 5, and 6 years (15.6%, 15.6%, and 14.7%, respectively).20 Importantly, no new safety signals were observed with a 5-year follow-up; nivolumab maintained a favorable safety profile versus docetaxel, without long-term toxicity. No evidence of late-onset grade 3-4 treatment-related select AEs was observed.
Among ≥ 5-year survivors in the nivolumab arm (n = 50), the median duration of therapy was 36.9 months and 18 of 50 remained on nivolumab at 5 years, suggesting that some patients may achieve long-term survival with continuous nivolumab treatment. In contrast, median duration off-treatment among the 5-year survivors who had discontinued nivolumab was 41.9 months, and 10.0% (n = 5) of 5-year survivors in the nivolumab arm were off treatment, without subsequent therapy, and had not progressed, suggesting benefit even for patients who stopped nivolumab treatment. Meanwhile, exploratory data from CheckMate 153 suggested a survival benefit with continuous nivolumab treatment beyond 1 year versus stopping treatment at 1 year.25 The optimal treatment duration of nivolumab and PD-1 inhibitors in general for patients with advanced NSCLC remains to be fully elucidated.
In conclusion, 5-year outcomes from the randomized phase III CheckMate 017 and 057 trials demonstrate that nivolumab can provide long-term survival benefit with durable responses and a tolerable safety profile in patients with previously treated, advanced NSCLC. Furthermore, some patients appear to maintain prolonged disease control even after stopping systemic therapy. These findings represent an important advancement in the treatment of lung cancer.
ACKNOWLEDGMENT
We thank the patients and their families, as well as the participating trial teams, for making this trial possible; Jamie Yingst of Bristol Myers Squibb for contributing as protocol manager of this trial; and the staff of Dako, an Agilent Technologies, Inc, company, for collaborative development of the PD-L1 IHC 28-8 pharmDx assay. This study was sponsored by Bristol Myers Squibb and Ono Pharmaceutical Company Ltd. Medical writing and editorial assistance were provided by Amy Horne, MSc, of Caudex and was funded by Bristol Myers Squibb.
Appendix 1. Supplementary methods
Patients
Patients were ≥ 18 years of age and had an Eastern Cooperative Oncology Group performance status (ECOG PS) of 0 or 1, measurable disease according to Response Evaluation Criteria in Solid Tumors version 1.1 (RECIST v1.1),26 and disease recurrence or progression during or after one prior platinum-based chemotherapy regimen. In CheckMate 057, an additional line of prior therapy with a tyrosine kinase inhibitor was permitted in patients with known epidermal growth factor receptor mutations or anaplastic lymphoma kinase rearrangements.
Study design
Patients in the nivolumab arm were permitted to continue treatment after initial disease progression if they met protocol-defined criteria, including if the trial drug was tolerated and patients were obtaining clinical benefit as determined by the investigator. Those in the docetaxel group who no longer derived benefit were eligible to receive nivolumab in the crossover and/or extension phases of the trials following a 3-week washout period.
After the readout of the primary end point, the protocol was amended such that nivolumab-treated patients were allowed to transition to nivolumab 480 mg every 4 weeks;27 docetaxel-treated patients who ended treatment at any time during the trials could cross over to nivolumab, either 3 mg/kg every 2 weeks or 480 mg every 4 weeks.
FIG A1.
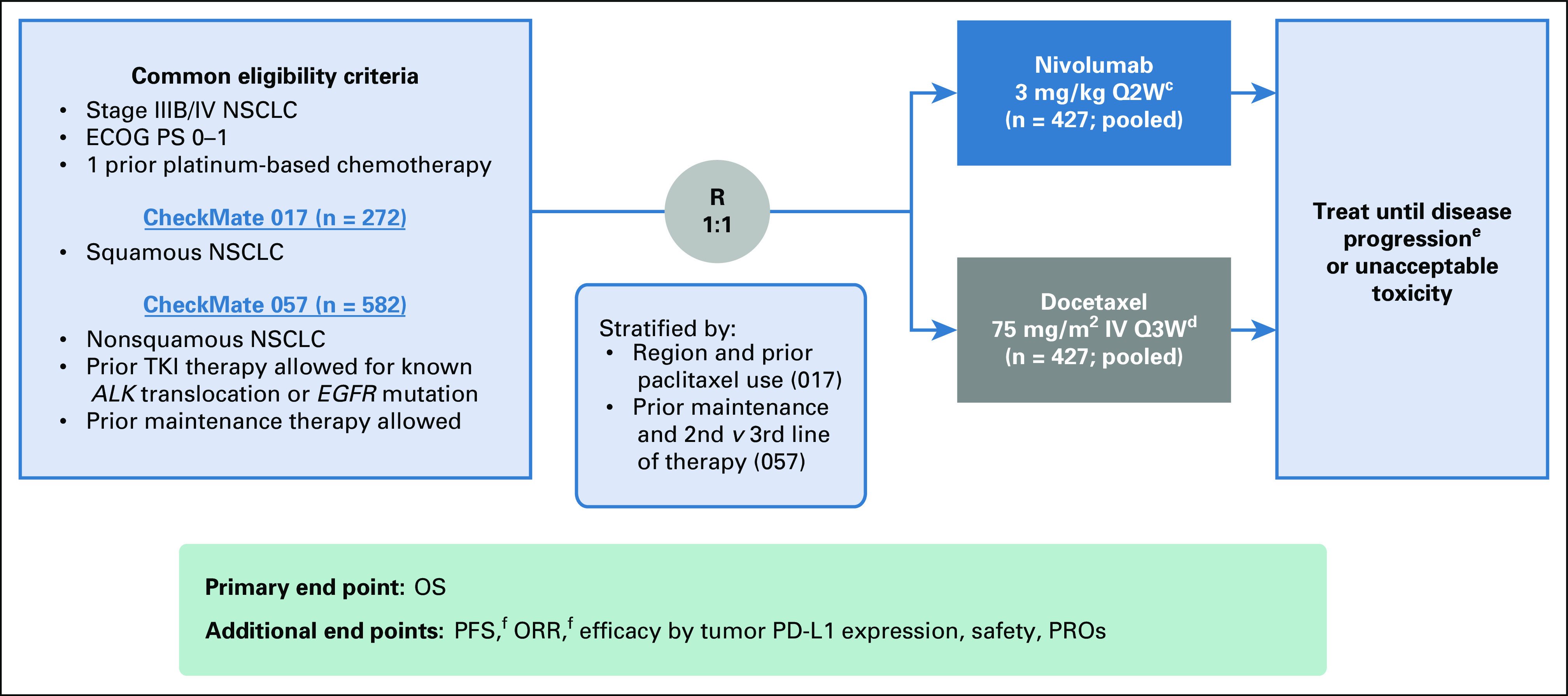
Study design.a,b aNCT01642004; database lock: May 8, 2019; minimum follow-up for OS, 64.2 months; bNCT01673867; database lock: May 16, 2019; minimum follow-up for OS, 64.5 months; cOptional switch to nivolumab 480 mg every 4 weeks allowed as per the protocol amendment in September 2016; dAfter completion of the primary analyses, patients in the docetaxel arms who ended treatment at any time during the trials were allowed to cross over to nivolumab; eDefined by RECIST 1.1; patients receiving nivolumab may be treated beyond progression under protocol-defined circumstances; fAs assessed by investigator. ALK, anaplastic lymphoma kinase; ECOG PS, Eastern Cooperative Oncology Group performance status; EGFR, epidermal growth factor receptor; IV, intravenous; NSCLC; non–small-cell lung cancer; NSQ, nonsquamous; ORR, objective response rate; OS, overall survival; PD-L1, programmed death ligand 1; PFS, progression-free survival; PROs, patient-reported outcomes; Q2W, every 2 weeks; Q3W, every 3 weeks; R, randomized; SQ, squamous; TKI, tyrosine kinase inhibitor. Reprinted from Annals of Oncology, 29(4), Waterhouse M, Domine M, Garassino LQM, et al, “Nivolumab Versus Docetaxel in Previously Treated Advanced Nonsmall-Cell Lung Cancer (CheckMate 017 and CheckMate 057): 3-Year Update and Outcomes in Patients With Liver Metastases,” 959-965, 2018, with permission from Elsevier.
FIG A2.

CONSORT diagram of patient disposition for (A) CheckMate 017 and (B) CheckMate 057. AE, adverse event.
FIG A3.
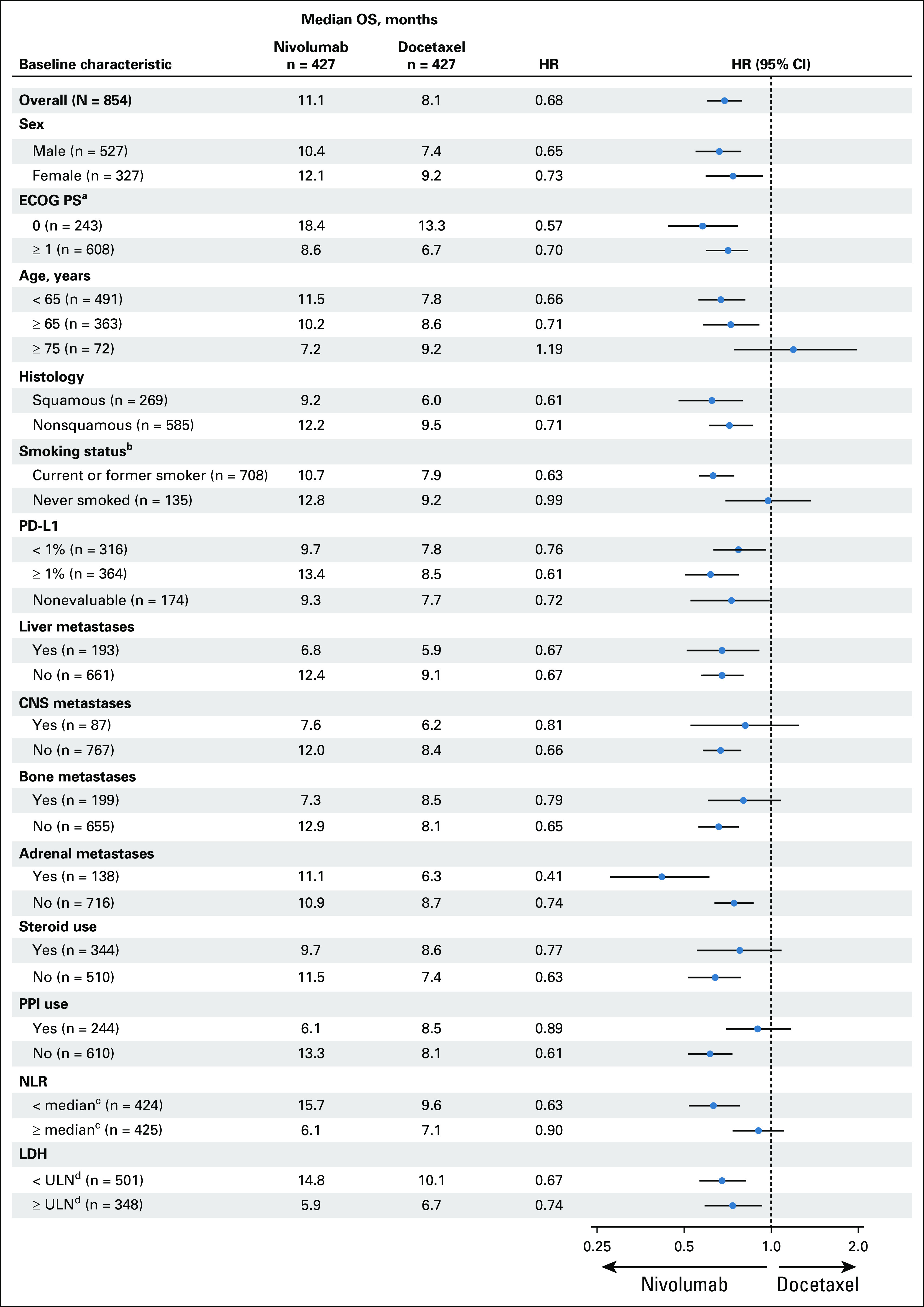
Forest plot of OS in predefined subgroups. Hazard ratios were not reported for subgroups with fewer than 10 patients per treatment group. aNot reported in two and one patients with nivolumab and docetaxel, respectively. bUnknown in seven and four patients with nivolumab and docetaxel, respectively. cMedian NLR was 4.80. NLR was not reported in two patients each in nivolumab and docetaxel arms. dNot reported in three and two patients with nivolumab and docetaxel, respectively. ECOG PS, Eastern Cooperative Oncology Group performance status; HR, hazard ratio; LDH, lactate dehydrogenase; NLR, neutrophil-to-lymphocyte ratio; OS, overall survival; PD-L1, programmed death ligand 1; PPI, proton pump inhibitor; ULN, upper limit of normal.
FIG A4.
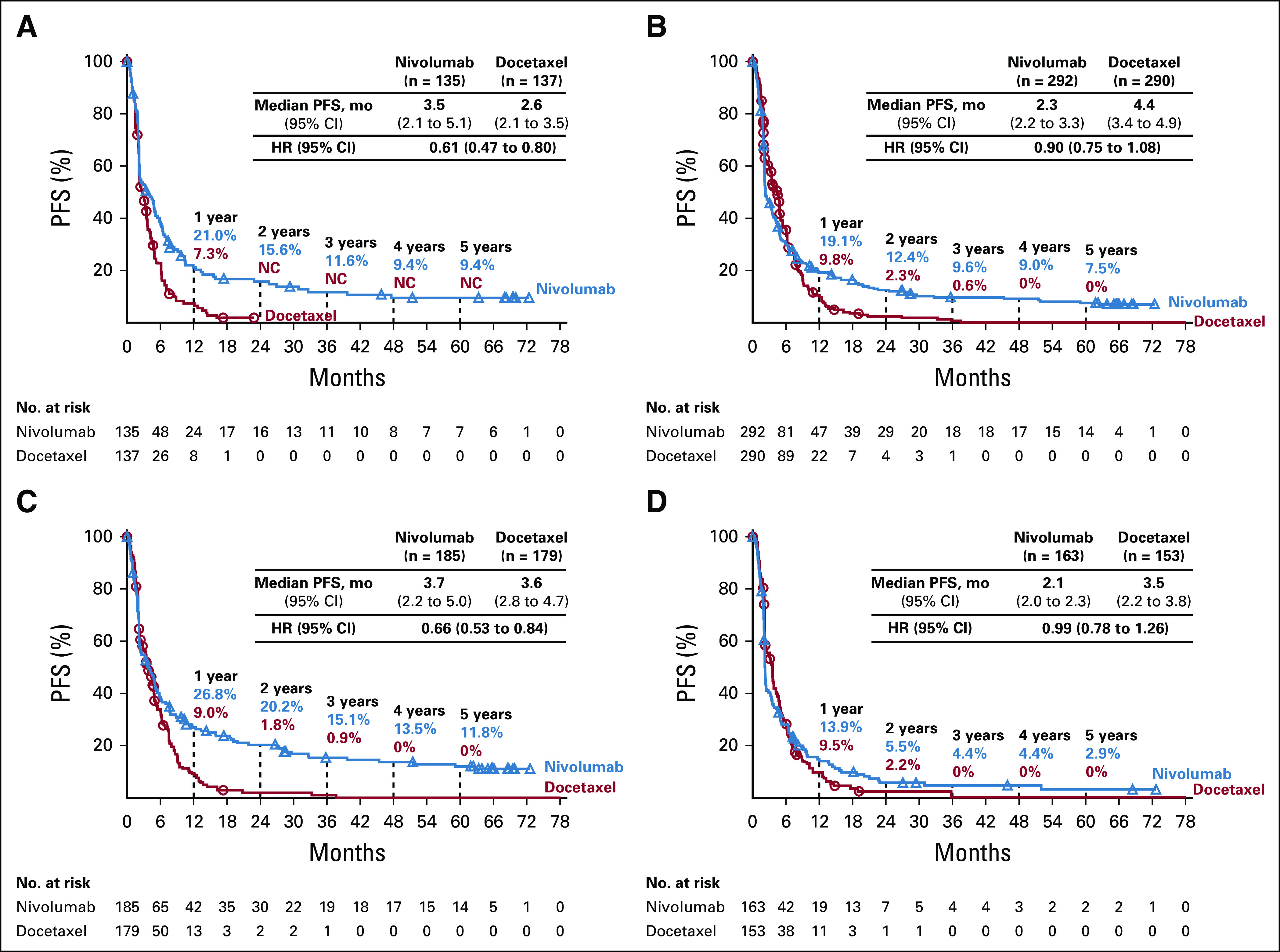
PFS in patients with (A) SQ tumor histology, (B) NSQ tumor histology, (C) ≥ 1% PD-L1 expression, and (D) < 1% PD-L1 expression. aPer local investigator; minimum follow-up: CheckMate 017: 64.2 months and CheckMate 057: 64.5 months. HR, hazard ratio; NC, not calculable; No., number; NSQ, nonsquamous; PD-L1, programmed death ligand 1; PFS, progression-free survival; SQ, squamous.
FIG A5.
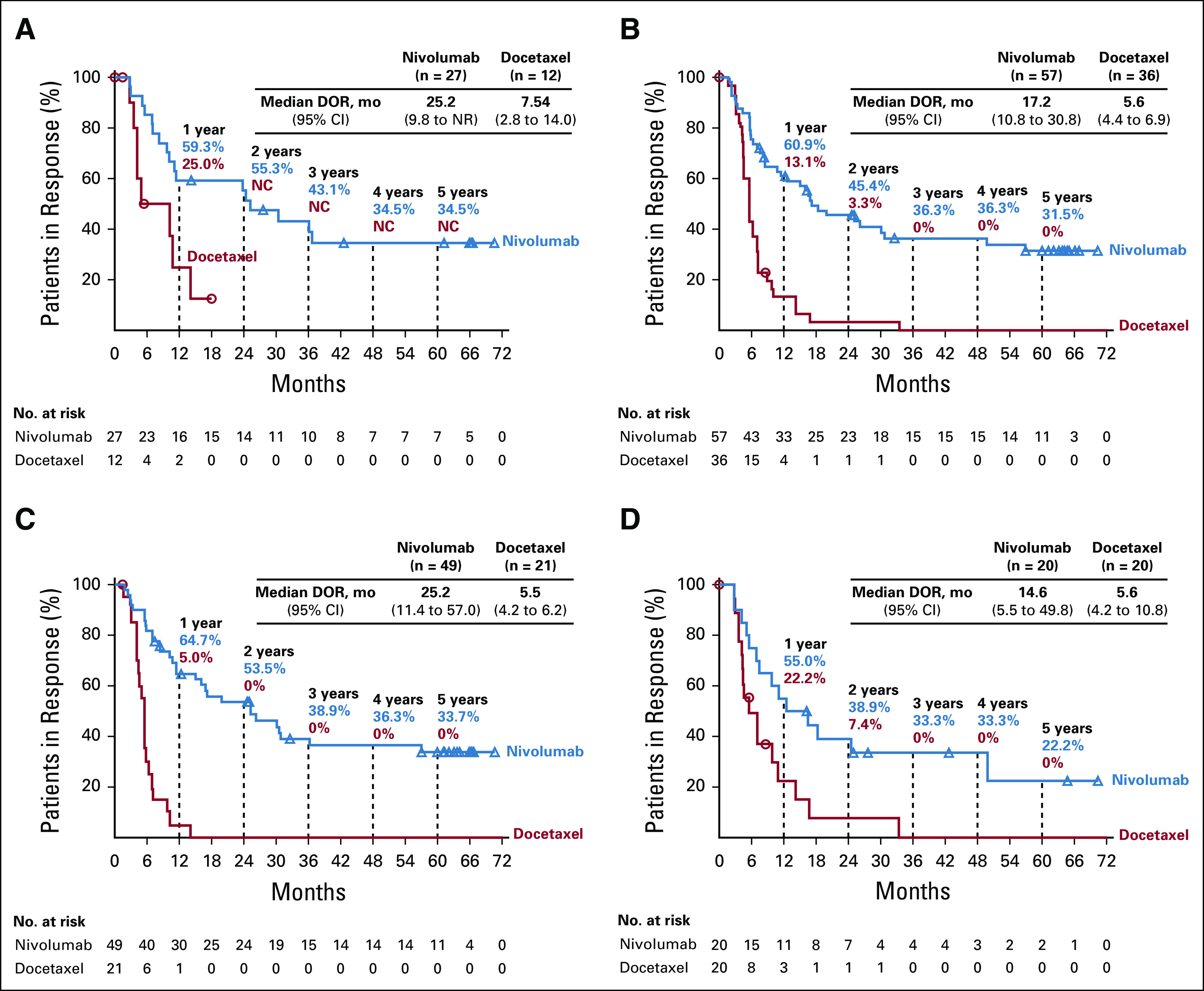
DORa in all treated patients with (A) SQ tumor histology, (B) NSQ tumor histology, (C) ≥ 1% PD-L1 expression, and (D) < 1% PD-L1 expression. aPer local investigator. DOR, duration of response; NC, not calculable. No., number; NSQ, nonsquamous; PD-L1, programmed death ligand 1; SQ, squamous.
FIG A6.
Treatment status of survivors at 5 years. aMedian (range) nivolumab treatment duration: 36.9 (1.8-76.2 +) months. bThe other 3 patients progressed (1.8, 4.5, and 44.2 months, respectively) after discontinuing nivolumab treatment. cAfter nivolumab treatment. dInformation on subsequent therapy was not available as of database lock. eNivolumab treatment durations for individual patients: 8.8, 21.7, 36.6, 43.3, and 43.5 months. fMedian (range) nivolumab treatment duration: 68.4 (62.9-76.2 +) months. gIncludes two patients treated with nivolumab as first subsequent therapy. hBecause of the receipt of subsequent therapy. AE, adverse event; TRAEs, treatment-related adverse events.
TABLE A1.
Baseline Characteristics in the Pooled CheckMate 017 and 057 Population and by Trial

TABLE A2.
Tumor Response in All Randomly Assigned Patients and by Trial

TABLE A3.
Baseline Characteristics of < 1-Year and ≥ 5-Year Survivors on Nivolumab and Docetaxel in the Pooled CheckMate 017 and 057 Population

TABLE A4.
Subsequent Therapies Received by 5-Year Survivors

TABLE A5.
CheckMate 017 Investigators

TABLE A6.
CheckMate 057 Investigators

PRIOR PRESENTATION
Presented at the IASLC 2019 World Conference on Lung Cancer, Barcelona, September 7-10, 2019, Spain; 2019 Fall Meeting of the Florida Society of Clinical Oncology, Orlando, FL, November 8−9, 2019; and the British Thoracic Oncology Group Annual Conference 2020, Dublin, Ireland, January 29-31, 2020.
SUPPORT
Supported by Bristol Myers Squibb.
CLINICAL TRIAL INFORMATION
DATA SHARING STATEMENT
Bristol Myers Squibb policy on data sharing may be found at https://www.bms.com/researchers-and-partners/clinical-trials-and-research/disclosure-commitment.html.
AUTHOR CONTRIBUTIONS
Conception and design: Scott Gettinger, Javier de Castro Carpeno, Neal Ready, Enriqueta Felip, David R. Spigel, Wilfried Enst Erich Eberhardt, Ang Li, Julie Brahmer
Financial support: Enriqueta Felip
Administrative support: Enriqueta Felip
Provision of study materials or patients: Everett E. Vokes, Laura Q. M. Chow, Marco Angelo Burgio, Javier de Castro Carpeno, Oscar Arrieta, Osvaldo Arén Frontera, Charles Butts, Bruno Coudert, Neal Ready, Enriqueta Felip, David Waterhouse, Fabrice Barlesi, Markus Wohlleber, David E. Gerber, David R. Spigel, Lucio Crino, Wilfried Enst Erich Eberhardt, Julie Brahmer
Collection and assembly of data: Hossein Borghaei, Scott Gettinger, Laura Q. M. Chow, Marco Angelo Burgio, Javier de Castro Carpeno, Adam Pluzanski, Oscar Arrieta, Osvaldo Arén Frontera, Joanna Wójcik-Tomaszewska, Bruno Coudert, Neal Ready, Enriqueta Felip, Miriam Alonso García, David Waterhouse, Manuel Domine, Fabrice Barlesi, Scott Antonia, Markus Wohlleber, David E. Gerber, Grzegorz Czyzewicz, Lucio Crino, Wilfried Enst Erich Eberhardt, Ang Li, Sathiya Marimuthu, Julie Brahmer
Data analysis and interpretation: Hossein Borghaei, Scott Gettinger, Everett E. Vokes, Laura Q. M. Chow, Javier de Castro Carpeno, Adam Pluzanski, Rita Chiari, Charles Butts, Bruno Coudert, Marina Chiara Garassino, Neal Ready, Enriqueta Felip, David Waterhouse, Manuel Domine, Fabrice Barlesi, Scott Antonia, Markus Wohlleber, David R. Spigel, Lucio Crino, Wilfried Enst Erich Eberhardt, Ang Li, Sathiya Marimuthu, Julie Brahmer
Manuscript writing: All authors
Final approval of manuscript: All authors
Accountable for all aspects of the work: All authors
AUTHORS' DISCLOSURES OF POTENTIAL CONFLICTS OF INTEREST
Five-Year Outcomes From the Randomized, Phase III Trials CheckMate 017 and 057: Nivolumab Versus Docetaxel in Previously Treated Non–Small-Cell Lung Cancer
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I =Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO’s conflict of interest policy, please refer to www.asco.org/rwc or ascopubs.org/jco/authors/author-center.
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (Open Payments).
Hossein Borghaei
Honoraria: Bristol Myers Squibb, Celgene, Axiom Biotechnologies, Pfizer,
Consulting or Advisory Role: Bristol Myers Squibb, Lilly, Celgene, Genentech, Pfizer, Boehringer Ingelheim, EMD Serono, Trovagene, Novartis, Merck, AstraZeneca, Genmab, Regeneron, Cantargia AB, BioNTech AG, Abbvie, PharmaMar, Takeda, Amgen, HUYA Bioscience International, Sonnetbio, Rgenix
Research Funding: Millennium, Merck, Celgene, Bristol Myers Squibb, Lilly
Travel, Accommodations, Expenses: Bristol Myers Squibb, Lilly, Clovis Oncology, Celgene, Genentech, Novartis, Merck, Amgen
Other Relationship: University of Pennsylvania, Takeda, Incyte
Scott Gettinger
Consulting or Advisory Role: Bristol Myers Squibb, NEKTAR
Research Funding: Bristol Myers Squibb, Genentech, ARIAD/TAKEDA, Iovance Biotherapeutics
Everett E. Vokes
Stock and Other Ownership Interests: Coordination Pharmaceuticals
Honoraria: Abbvie, Amgen, AstraZeneca, Bristol Myers Squibb, Celgene, Lilly, EMD Serono, Genentech, GlaxoSmithKline, Merck, Novartis, Regeneron, Takeda, Radius Health, Ascendis Pharma
Consulting or Advisory Role: Abbvie, Amgen, AstraZeneca, Bristol Myers Squibb, Celgene, Lilly, Merck, Regeneron, Novartis, EMD Serono, Genentech, GlaxoSmithKline, Takeda, Radius Health, Ascendis Pharma
Research Funding: Abbvie, Bristol Myers Squibb, Celgene, Novartis, Lilly
Travel, Accommodations, Expenses: Abbvie, Amgen, Bristol Myers Squibb, Celgene, Lilly, EMD Serono, Genentech, GlaxoSmithKline, Merck, Novartis, Regeneron
(OPTIONAL) Open Payments Link: https://openpaymentsdata.cms.gov/physician/930740
Laura Q. M. Chow
Consulting or Advisory Role: Merck, Dynavax, Alkermes, Novartis, Pfizer, Cullinan Management Inc, Elicio, Daiichi Sankyo
Research Funding: Pfizer, Genentech, Novartis, Lilly/ImClone, Merck, AstraZeneca/MedImmune, Bristol Myers Squibb, Incyte, Seattle Genetics, Dynavax, ALX Oncology, Alkermes
Javier de Castro Carpeno
Consulting or Advisory Role: AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Merck Sharp & Dohme, Roche, Pfizer, Pierre Fabre, Takeda, Tesaro, Teva
Research Funding: Roche
Travel, Accommodations, Expenses: AstraZeneca Spain, Merck Sharp & Dohme, Roche
Adam Pluzanski
Honoraria: Roche, Bristol Myers Squibb, AstraZeneca, MSD, Pfizer, Takeda
Consulting or Advisory Role: Boehringer Ingelheim
Travel, Accommodations, Expenses: Pfizer, Bristol Myers Squibb, AstraZeneca
Oscar Arrieta
Honoraria: Pfizer, AstraZeneca, Boehringer Ingelheim, Roche
Consulting or Advisory Role: AstraZeneca, Roche, Lilly, Merck, Bristol Myers Squibb
Research Funding: Roche, Bristol Myers Squibb, Merck, AstraZeneca
Travel, Accommodations, Expenses: Lilly
Osvaldo Arén Frontera
Employment: Pfizer
Stock and Other Ownership Interests: Pfizer
Honoraria: Pfizer
Consulting or Advisory Role: Bristol Myers Squibb, BMS COLOMBIA
Rita Chiari
Speakers' Bureau: Takeda
Charles Butts
Research Funding: Bristol Myers Squibb, AstraZeneca, Merck (per-patient funding for clinical trials; paid to institution, not investigator)
Joanna Wójcik-Tomaszewska
Research Funding: Bristol Myers Squibb, MSD Oncology, Roche, Lilly, AVEO, ICON Clinical Research
Bruno Coudert
Honoraria: Roche Laboratories France, AstraZeneca, Bristol Myers Squibb
Consulting or Advisory Role: Roche Laboratories France
Marina Chiara Garassino
Honoraria: MSD Oncology, AstraZeneca/MedImmune, GlaxoSmithKline, Takeda, Roche, Bristol Myers Squibb
Consulting or Advisory Role: Bristol Myers Squibb, MSD, AstraZeneca, Novartis, Takeda, Roche, Tiziana Life Sciences, Sanofi, Celgene, Daiiki Sankyo, Inivata, Incyte, Pfizer, Seattle Genetics, Lilly, GlaxoSmithKline, Bayer, Blueprint Medicines, Janssen
Speakers' Bureau: Janssen, Takeda, MSD Oncology, Celgene, Incyte, Roche, Bristol Myers Squibb, Otsuka, Lilly
Research Funding: Bristol Myers Squibb, MSD, Roche/Genentech, AstraZeneca/MedImmune, AstraZeneca, Pfizer, GlaxoSmithKline, Novartis, Merck, Incyte, Takeda, Spectrum Pharmaceuticals, Blueprint Medicines, Lilly, AstraZeneca, Ipsen, Turning Point Therapeutics, Janssen, Exelixis, MedImmune, Array BioPharma, Sanofi
Travel, Accommodations, Expenses: Pfizer, Roche, AstraZeneca
Neal Ready
Consulting or Advisory Role: Bristol Myers Squibb, Novartis, Merck, Abbvie, Celgene, Merck Serono, AstraZeneca, G1 Therapeutics, Jazz Pharmaceuticals
Speakers' Bureau: Bristol Myers Squibb
Research Funding: Bristol Myers Squibb, Merck
Enriqueta Felip
Consulting or Advisory Role:Consulting or Advisory Role: Roche, Boehringer Ingelheim, AstraZeneca, Bristol Myers Squibb, Guardant Health, Novartis, Takeda, Abbvie, Blueprint Medicines, Lilly, Merck KGaA, Merck Sharp & Dohme, Springer, GlaxoSmithKline, JANSSEN, MEDSCAPE, Merck KGaA, Bayer, Amgen, Pfizer, Puma Biotechnology, Genzyme
Speakers' Bureau: AstraZeneca, Bristol Myers Squibb, Novartis, Boehringer Ingelheim, Merck Sharp & Dohme, Roche, Pfizer, Lilly, Takeda, medscape, Prime Oncology, Touchime, PEER VOICE, Springer
Research Funding: FUNDACIÓN MERCK SALUD, EMD Serono
Other Relationship: GRÍFOLS
David Waterhouse
Consulting or Advisory Role: Bristol Myers Squibb, AZTherapies, Abbvie, Amgen, Celgene, MCGivenny Global, CTI, Janssen Oncology, Seattle Genetics, Jazz Pharmaceuticals, Exelixis
Speakers' Bureau: Bristol Myers Squibb, Janssen Oncology
Travel, Accommodations, Expenses: Bristol Myers Squibb
Manuel Domine
Consulting or Advisory Role: AstraZeneca, Bristol Myers Squibb, Boehringer Ingelheim, MSD Oncology, Pfizer, Roche
Travel, Accommodations, Expenses: AstraZeneca, Boehringer Ingelheim, Lilly, Pfizer, Roche
Fabrice Barlesi
Honoraria: Genentech/Roche, Pfizer, Pierre Fabre, AstraZeneca, Bristol Myers Squibb, Boehringer Ingelheim, Lilly, Novartis, Pierre Fabre, Merck Serono, MSD Oncology, Takeda, Bayer
Consulting or Advisory Role: Roche/Genentech, Pfizer, Novartis, Pierre Fabre, Bristol Myers Squibb, AstraZeneca/MedImmune, Boehringer Ingelheim, Lilly, Merck Serono, MSD Oncology, Takeda, Bayer
Research Funding: Roche/Genentech, AstraZeneca/MedImmune, Bristol Myers Squibb, Pierre Fabre, Pierre Fabre, Amgen, Bayer, Boehringer Ingelheim, Eisai, Lilly, Ipsen, Innate Pharma, Novartis, Merck Serono, MSD Oncology, Pfizer, Sanofi/Aventis, Takeda
Travel, Accommodations, Expenses: Roche/Genentech, Bristol Myers Squibb, AstraZeneca/MedImmune, MSD Oncology
Scott Antonia
Stock and Other Ownership Interests: Cellular Biomedicine Group
Honoraria: AstraZeneca, Bristol Myers Squibb, Merck, Boehringer Ingelheim, Novartis, CBMG, Memgen
Consulting or Advisory Role: Bristol Myers Squibb, AstraZeneca, Merck, Boehringer Ingelheim, Novartis, Memgen, FLX Bio
Travel, Accommodations, Expenses: Bristol Myers Squibb, AstraZeneca, Merck, Boehringer Ingelheim, FLX Bio, Novartis
Markus Wohlleber
Consulting or Advisory Role: Bristol Myers Squibb
Travel, Accommodations, Expenses: Bristol Myers Squibb, AstraZeneca
David E. Gerber
Stock and Other Ownership Interests: Gilead Sciences
Consulting or Advisory Role: Samsung Bioepis, Catalyst Pharmaceuticals
Research Funding: BerGenBio, Karyopharm Therapeutics, AstraZeneca
Patents, Royalties, Other Intellectual Property: Royalties from Oxford University Press from two books, Royalties from Decision Support in Medicine from the Clinical Decision Support--Oncology on-line program, Patent pending: “Prediction and Treatment of Immunotherapeutic Toxicity” (provisional, application number 62/461,455)
Uncompensated Relationships: Bristol Myers Squibb
David R. Spigel
Leadership: ASCO Adjuvant Lung Cancer Guideline Committee
Consulting or Advisory Role: Genentech/Roche, Novartis, Celgene, Bristol Myers Squibb, AstraZeneca, Pfizer, GlaxoSmithKline, Merck, Nektar, Takeda, TRM Oncology, Evelo Therapeutics, Illumina, PharmaMar, Aptitude Health, Aptitude Health, Dracen Pharmaceuticals, EMD Serono, Iksuda Therapeutics, Molecular Templates, Seattle Genetics, TRIPTYCH Health Partners, Amgen, Curio Sciences, Intellisphere, Ipsen, Jazz Pharmaceuticals, Mirati Therapeutics, Puma Biotechnology, Sanofi/Aventis
Research Funding: Genentech/Roche, Novartis, Celgene, Bristol Myers Squibb, Lilly, AstraZeneca, University of Texas Southwestern Medical Center - Simmons Cancer Center, Merck, G1 Therapeutics, Neon Therapeutics, Takeda, Nektar, Celldex, Clovis Oncology, Daiichi Sankyo, EMD Serono, Astellas Pharma, GRAIL, Transgene, Aeglea Biotherapeutics, Ipsen, BIND Therapeutics, Eisai, ImClone Systems, ImClone Systems, Janssen Oncology, MedImmune, Molecular Partners, Agios, GlaxoSmithKline, Tesaro, Cyteir Therapeutics, Apollomics
Travel, Accommodations, Expenses: AstraZeneca, Genentech, Novartis
Wilfried Enst Erich Eberhardt
Honoraria: AstraZeneca, Roche Pharma AG, Bristol Myers Squibb, MSD Oncology, Boehringer Ingelheim, Lilly, Takeda, Pfizer, Amgen, Novartis, Abbvie
Consulting or Advisory Role: AstraZeneca, Roche, Bristol Myers Squibb, MSD Oncology, Bayer Health, Lilly, Boehringer Ingelheim, Takeda, Pfizer
Research Funding: AstraZeneca, Lilly, Bristol Myers Squibb
Sathiya Marimuthu
Employment: Bristol Myers Squibb
Stock and Other Ownership Interests: Bristol Myers Squibb
Travel, Accommodations, Expenses: Bristol Myers Squibb
Julie Brahmer
Honoraria: Roche/Genentech
Consulting or Advisory Role: Bristol Myers Squibb, Lilly, Celgene, Syndax, Janssen Oncology, Merck, Amgen, Genentech
Research Funding: Bristol Myers Squibb, AstraZeneca, Incyte, Spectrum Pharmaceuticals, Revolution
Travel, Accommodations, Expenses: Bristol Myers Squibb, Roche/Genentech
Other Relationship: Bristol Myers Squibb, Merck, Janssen Oncology
No other potential conflicts of interest were reported.
REFERENCES
- 1.Noone AM Howlader N Krapcho M, et al. : SEER Cancer Statistics Review, 1975–2015, National Cancer Institute, 1975-2015. https://seer.cancer.gov/csr/1975_2015/ [Google Scholar]
- 2.Assi HI Kamphorst AO Moukalled NM, et al. : Immune checkpoint inhibitors in advanced non-small cell lung cancer. Cancer 124:248-261, 2018 [DOI] [PubMed] [Google Scholar]
- 3.Rittmeyer A Barlesi F Waterkamp D, et al. : Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (OAK): A phase 3, open-label, multicentre randomised controlled trial. Lancet 389:255-265, 2017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Brahmer J Reckamp KL Baas P, et al. : Nivolumab versus docetaxel in advanced squamous-cell non-small-cell lung cancer. N Engl J Med 373:123-135, 2015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Borghaei H Paz-Ares L Horn L, et al. : Nivolumab versus docetaxel in advanced nonsquamous non-small-cell lung cancer. N Engl J Med 373:1627-1639, 2015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.National Comprehensive Cancer Network : Non-Small Cell Lung Cancer v5.2019. 2019. https://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf [Google Scholar]
- 7.Herbst RS Garon EB Kim BC, et al. : LBA4 long-term follow-up in the KEYNOTE-010 study of pembrolizumab (pembro) for advanced NSCLC, including in patients (pts) who completed 2 years of pembro and pts who received a second course of pembro. Ann Oncol 29:x39-x43, 2018(suppl 10) [Google Scholar]
- 8.Reck M Rodriguez-Abreu D Robinson AG, et al. : Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N Engl J Med 375:1823-1833, 2016 [DOI] [PubMed] [Google Scholar]
- 9.Gandhi L Rodriguez-Abreu D Gadgeel S, et al. : Pembrolizumab plus chemotherapy in metastatic non-small-cell lung cancer. N Engl J Med 378:2078-2092, 2018 [DOI] [PubMed] [Google Scholar]
- 10.Paz-Ares L Luft A Vicente D, et al. : Pembrolizumab plus chemotherapy for squamous non-small-cell lung cancer. N Engl J Med 379:2040-2051, 2018 [DOI] [PubMed] [Google Scholar]
- 11.Mok TSK Wu YL Kudaba I, et al. : Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): A randomised, open-label, controlled, phase 3 trial. Lancet 393:1819-1830, 2019 [DOI] [PubMed] [Google Scholar]
- 12.Socinski MA Jotte RM Cappuzzo F, et al. : Atezolizumab for first-line treatment of metastatic nonsquamous NSCLC. N Engl J Med 378:2288-2301, 2018 [DOI] [PubMed] [Google Scholar]
- 13.Hellmann MD Paz-Ares L Bernabe Caro R, et al. : Nivolumab plus ipilimumab in advanced non-small-cell lung cancer. N Engl J Med 381:2020-2031, 2019 [DOI] [PubMed] [Google Scholar]
- 14.Ettinger DS Wood DE Aggarwal C, et al. : Non-small cell lung cancer: NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw 2, 2019 [Google Scholar]
- 15.Topalian SL Hodi FS Brahmer JR, et al. : Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N Engl J Med 366:2443-2454, 2012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bristol-Myers Squibb : Opdivo® (nivolumab) prescribing information, March 2019. 2019. http://packageinserts.bms.com/pi/pi_opdivo.pdf
- 17.European Medicines Agency : OpdivoTM (nivolumab) Summary of Product Characteristics. 2019. https://www.ema.europa.eu/en/documents/product-information/opdivo-epar-product-information_en.pdf [Google Scholar]
- 18.Horn L Spigel DR Vokes EE, et al. : Nivolumab versus docetaxel in previously treated patients with advanced non-small-cell lung cancer: Two-year outcomes from two randomized, open-label, phase III trials (CheckMate 017 and CheckMate 057). J Clin Oncol 35:3924-3933, 2017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Vokes EE Ready N Felip E, et al. : Nivolumab versus docetaxel in previously treated advanced non-small-cell lung cancer (CheckMate 017 and CheckMate 057): 3-year update and outcomes in patients with liver metastases. Ann Oncol 29:959-965, 2018 [DOI] [PubMed] [Google Scholar]
- 20.Antonia SJ Borghaei H Ramalingam SS, et al. : Four-year survival with nivolumab in patients with previously treated advanced non-small-cell lung cancer: A pooled analysis. Lancet Oncol 20:1395-1408, 2019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Antonia SJ Borghaei H Ramalingam SS, et al. : Four-year survival with nivolumab in patients with previously treated advanced non-small-cell lung cancer: A pooled analysis. Lancet Oncol 20:1395-140, 2019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Garon EB Hellmann MD Rizvi NA, et al. : Five-year overall survival for patients with advanced nonsmall-cell lung cancer treated with pembrolizumab: Results from the phase I KEYNOTE-001 study. J Clin Oncol 37:2518-2527, 2019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Hubbard MO Fu P Margevicius S, et al. : Five-year survival does not equal cure in non-small cell lung cancer: A surveillance, epidemiology, and end results-based analysis of variables affecting 10- to 18-year survival. J Thorac Cardiovasc Surg 143:1307-1313, 2012 [DOI] [PubMed] [Google Scholar]
- 24.Schadendorf D Hodi FS Robert C, et al. : Pooled analysis of long-term survival data from phase II and phase III trials of ipilimumab in unresectable or metastatic melanoma. J Clin Oncol 33:1889-1894, 2015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Spigel D McCleod M Hussein M, et al. : CheckMate 153: Randomized results of continuous vs 1-year fixed-duration nivolumab in patients with advanced non-small cell lung cancer, in European Society for Medical Oncology ,Volume 12970. Madrid, Spain, 2017 [Google Scholar]
- 26.Eisenhauer EA Therasse P Bogaerts J, et al. : New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur J Cancer 45:228-247, 2009 [DOI] [PubMed] [Google Scholar]
- 27.Garon EB Reinmuth N Falchero L, et al. : CheckMate 384: Phase IIIb/IV trial of nivolumab (nivo) 480 mg Q4W versus 240 mg Q2W after ≤ 12 months of nivo in previously treated advanced NSCLC. J Clin Oncol 37:100, 2019(suppl 8) [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Bristol Myers Squibb policy on data sharing may be found at https://www.bms.com/researchers-and-partners/clinical-trials-and-research/disclosure-commitment.html.