

PURPOSE
Patients with cancer living in socioeconomically disadvantaged areas have worse cancer outcomes. The association between socioeconomic deprivation and outcomes among patients with cancer participating in clinical trials has not been systematically examined.
METHODS
We examined survival outcomes for patients enrolled in phase III and large phase II clinical trials for major cancers conducted by the SWOG Cancer Research Network from 1985 to 2012. Socioeconomic deprivation was measured using trial participants' residential zip codes linked to the Area Deprivation Index (ADI). Five-year overall survival, progression-free survival, and cancer-specific survival were examined using Cox regression frailty models, adjusting for age, sex, and race, and separately for insurance status, prognostic risk, and rural or urban residency.
RESULTS
We examined 41,109 patients from 55 trials comprising 24 cancer histology and stage-specific cohorts. Compared with trial participants in the most affluent areas (ADI, 0%-20%), trial participants from areas with the highest socioeconomic deprivation (ADI, 80%-100%) had worse overall (hazard ratio [HR] = 1.28, 95% CI, 1.20 to 1.37, P < .001), progression-free (HR = 1.20, 95% CI, 1.13 to 1.28, P < .001), and cancer-specific survival (HR = 1.27, 95% CI, 1.18 to 1.37, P < .001). The results were similar after adjusting for insurance status, prognostic risk, and rural or urban residency. There was a continuous increase in risk of all outcomes as the ADI quintile increased.
CONCLUSION
In patients with cancer with access to protocol-directed care in clinical trials, high area-level socioeconomic deprivation was associated with worse survival. Future research should examine whether the etiology of this residual disparity is related to reduced access to supportive care or postprotocol therapy and/or to differences in health status not reflected by protocol selection criteria.
INTRODUCTION
Poverty is detrimental to health. A key underlying reason is that individuals from socioeconomically disadvantaged areas have limited access to vital healthcare resources, which may become a chronic risk factor for worse disease outcomes.1,2 Indeed, the association between low socioeconomic status and poor health outcomes has been well-documented in the literature for many diseases.3,4
CONTEXT
Key Objective
Poverty is detrimental to health. A key underlying reason is that individuals from socioeconomically deprived areas have limited access to healthcare resources. In cancer, an unresolved question is whether socioeconomic disparities in outcomes remain after accounting for access to quality cancer care. We examined the relationship between socioeconomic deprivation and outcomes for 41,109 patients enrolled in clinical trials, who have uniform access to protocol-directed treatment.
Knowledge Generated
Compared with trial patients in the most affluent areas, patients from the highest socioeconomically deprived areas had a 28% increased risk of death (P < .001). The findings were consistently observed within major patient groups.
Relevance
These findings suggest that initial access to quality cancer care as represented by treatment in a clinical trial is insufficient to eliminate the disparate outcomes related to socioeconomic deprivation. Policies to mitigate socioeconomic differences in cancer outcomes should emphasize access to cancer care services beyond initial therapy.
Patients with cancer from socioeconomically deprived areas have limited access to screening and treatment services and tend to have more advanced disease at presentation.5-8 Studies using cancer population data have shown that these patients have worse cancer outcomes.9-11 Evidence suggests that these disparities persist even after accounting for individual-level socioeconomic variables such as insurance status.12,13 An important and unresolved question is whether these disparate outcomes remain after accounting for access to quality cancer care.
We used data from patients participating in cancer treatment clinical trials to systematically examine whether patients from poor areas experienced worse outcomes. Patients in trials have uniform access to protocol-guided care and are uniformly staged to limit potential differences in underlying health status. These advantages enable investigators to account for the confounding influences of inconsistent pretreatment evaluation, care, and post-treatment surveillance. A better understanding of whether patients from socioeconomically deprived areas experience worse cancer outcomes can provide valuable insight into whether policies to improve outcomes should address not just individuals but also communities.
METHODS
Patients
In this retrospective observational study of pooled clinical trial participants, we used data from the SWOG Cancer Research Network, a member of the National Cancer Institute's funded National Clinical Trials Network and Community Oncology Research Program. We systematically reviewed the SWOG trial database to identify phase III trials or large phase II trials completed beginning in 1985 (when zip code data began to be routinely collected) for which the primary analysis was previously published. Data were pooled across trials of similar histology and stage to increase power to identify potential differences in outcomes between patients from areas with different levels of socioeconomic deprivation. A cancer-specific cohort was included in the analysis if—based on the observed sample size and number of events—the power to detect a hazard ratio (HR) of 1.5 or greater between groups was 80% or greater (Data Supplement, online only).14
Each trial included in this analysis was previously approved by an institutional review board; informed consent was previously obtained from all patients for each study included. This research was approved by the Fred Hutchinson Cancer Research Center's Institutional Review Board.
Area Deprivation Index and Covariates
We measured socioeconomic deprivation using trial participants' residence zip codes linked to the Area Deprivation Index (ADI) (ADI; University of Wisconsin School of Medicine and Public Health, 2019; 2013 version). The ADI is a comprehensive index composed of 17 indicators reflecting a diverse set of socioeconomic variables including neighborhood-level measures of education (two variables), employment (two), housing quality (five), and poverty (eight; Data Supplement).15 The ADI has been rigorously tested, is inclusive of all US neighborhoods, and is regularly updated. The ADI measure is scored from 0 to 100, with higher scores indicating greater socioeconomic deprivation. Based on recent studies, we split the ADI measure into quintiles; thus, for analysis purposes, the most deprived patients were defined as those in the highest ADI quintile (81%-100%) and the most affluent were patients in the lowest ADI quintile (0%-20%).16-19
Adjustment covariates included the following demographic variables: age (< 30, 30-34, …, 75-79, ≥ 80), race (Black v Others, by self-report), and sex. Patient-level insurance status was available for a subset of patients, categorized as using Medicaid, Medicare plus Medicaid, or self-pay versus using private insurance, Medicare, or military and/or Veteran's Administration insurance. To account for potential differences in clinical risk, for each cancer cohort, we identified key clinical risk factors, typically reflected by their inclusion as stratification variables in the trials (Data Supplement). For each patient, we summed the number of adverse clinical risk factors, creating a composite prognostic score, standardized to a 0-100 scale.14 Additionally, rural or urban residency was coded according to the US Department of Agriculture rural-urban continuum codes (1-3 = urban; 4-9 = rural).20
Outcomes
The primary end point was overall survival, measured as days from study registration to death by any cause or, for patients still alive, as days to last contact (censored). Secondarily, we examined progression-free survival, defined as time from trial registration to the date of death by any cause, evidence of protocol-defined relapse or progressive disease, or date of last contact for those alive and progression free at last contact (censored). We also examined cancer-specific survival, defined as time from study registration to date of cancer-specific death, death by another cause (censored), or last contact for those alive at last contact (censored). Detailed cause-of-death information was available for 28% of patient deaths; for remaining patients, we considered any death preceded by documented relapse or progression a cancer-specific death.
Statistical Analysis
We evaluated outcomes by quintile of the ADI score from highest quintile (most deprived) to lowest quintile (most affluent). We limited analyses to the first 5 years after registration to focus on cancer-related and treatment-related survival. Patients with last contact date or death date > 5 years postregistration were censored at 5 years of follow-up. For each cancer-specific cohort, we used multivariable Cox regression to assess the association of ADI quintile score and survival outcomes, with covariate adjustment.21 We used multivariable Cox regression frailty models to generate overall estimates of the association of ADI quintile score and survival outcomes aggregated across cancer cohorts, including each cancer cohort as a random effect to account for differences in period of enrollment, cancer-specific staging, and prognosis.21,22 Multiple models were conducted using a nested approach, to evaluate the extent to which additional adjustment for important covariates potentially modified the results. The primary model included covariate adjustments for age, sex, and race. Subsequent models also adjusted, separately, for insurance status (including an indicator variable for whether insurance status was available, yes v no), the prognostic score, rural or urban residency, and all three covariates.
We used Wald chi-square statistics derived from multivariable Cox regression models for statistical testing. Tests for statistical significance were two-sided, α = .05. We examined data through April 24, 2020.
Additional Analyses
Analyses were also conducted in the subsets of patients defined by age (< 65 v ≥ 65 years), sex, race (White v non-White), insurance status (Medicaid or no insurance v Medicare or private), disease stage (advanced v not advanced), time period of enrollment in approximate 10-year intervals (1985-1994 v 1995-2004 v 2005-2012), and geographic location (rural v urban). Furthermore, for each outcome, we examined whether the findings were sensitive to the influence of individual cancer cohorts by iteratively excluding each individual cohort and regenerating the aggregate frailty model regression estimates.
RESULTS
In total, 41,109 patients from 55 trials comprising 24 cancer-specific cohorts were examined (Table 1; Data Supplement). Overall, 29.0% of patients were ≥ 65 years, 61.5% were female, 10.3% were Black, and 10.4% (among those with known data) had no insurance or were enrolled in Medicaid. The four most common cancers (breast, colorectal, lung, and prostate) comprised 71.8% of the sample, and 36.8% had advanced-stage disease. There were clear trends toward higher rates of older patients, males, Black patients, and patients with Medicaid or no insurance as the level of deprivation increased (Table 1). One third (32.8%) of patients from the most deprived areas were Black.
TABLE 1.
Patient Characteristics by ADI Quintile

Association of Socioeconomic Deprivation and Survival Outcomes
Despite cohort-level heterogeneity, a trend toward worse overall survival for patients from the most deprived areas was apparent, even after accounting for the demographic covariates (Data Supplement). Among the 24 cancer cohorts we analyzed, the risk of a poorer outcome was statistically significantly greater for patients in the most deprived quintiles in eight instances for overall survival, in seven instances for progression-free survival, and in eight instances for cancer-specific survival. In contrast, in no instance was the risk of a poorer outcome statistically significantly greater for patients in the most affluent group.
These trends are reflected in aggregate models. In a multivariate Cox regression frailty model with the cancer cohorts treated as random effects, trial participants from the highest deprivation areas had worse overall survival on average (HR = 1.28, 95% CI, 1.20 to 1.37, P < .001) compared with patients from the most affluent areas (Fig 1; Table 2). The findings were of similar magnitude and direction for both progression-free survival and cancer-specific survival.
FIG 1.

Forest plot of hazard ratio comparing highest deprivation quintile versus lowest deprivation quintile. The results are from primary modeling approach, adjusting for age, race, and sex in frailty model with cancer type as random effect. The boxes in the forest plot represent the hazard ratios, and the horizontal lines are the 95% CIs; the vertical line is the line of equal hazard. HR, hazard ratio.
TABLE 2.
Changes in HR Comparing Lowest Versus Highest Area Deprivation Index Quintiles

The addition of other socioeconomic, clinical, and geographic variables to the regression models only modestly attenuated the association (Table 2). For instance, the aggregate estimate of the increased risk of death comparing patients in the most deprived versus the most affluent areas of 28% (HR = 1.28, 95% CI, 1.20 to 1.37, P < .001) was reduced to 22% (HR = 1.22, 95% CI, 1.14 to 1.31, P < .001) when insurance status, baseline clinical risk, and rural or urban residency were included in the model.
There was a clear trend toward consistently increasing risk of death as the level of deprivation increased (Fig 2). This trend was also apparent for progression-free and cancer-specific survival and for both the primary and secondary models.
FIG 2.
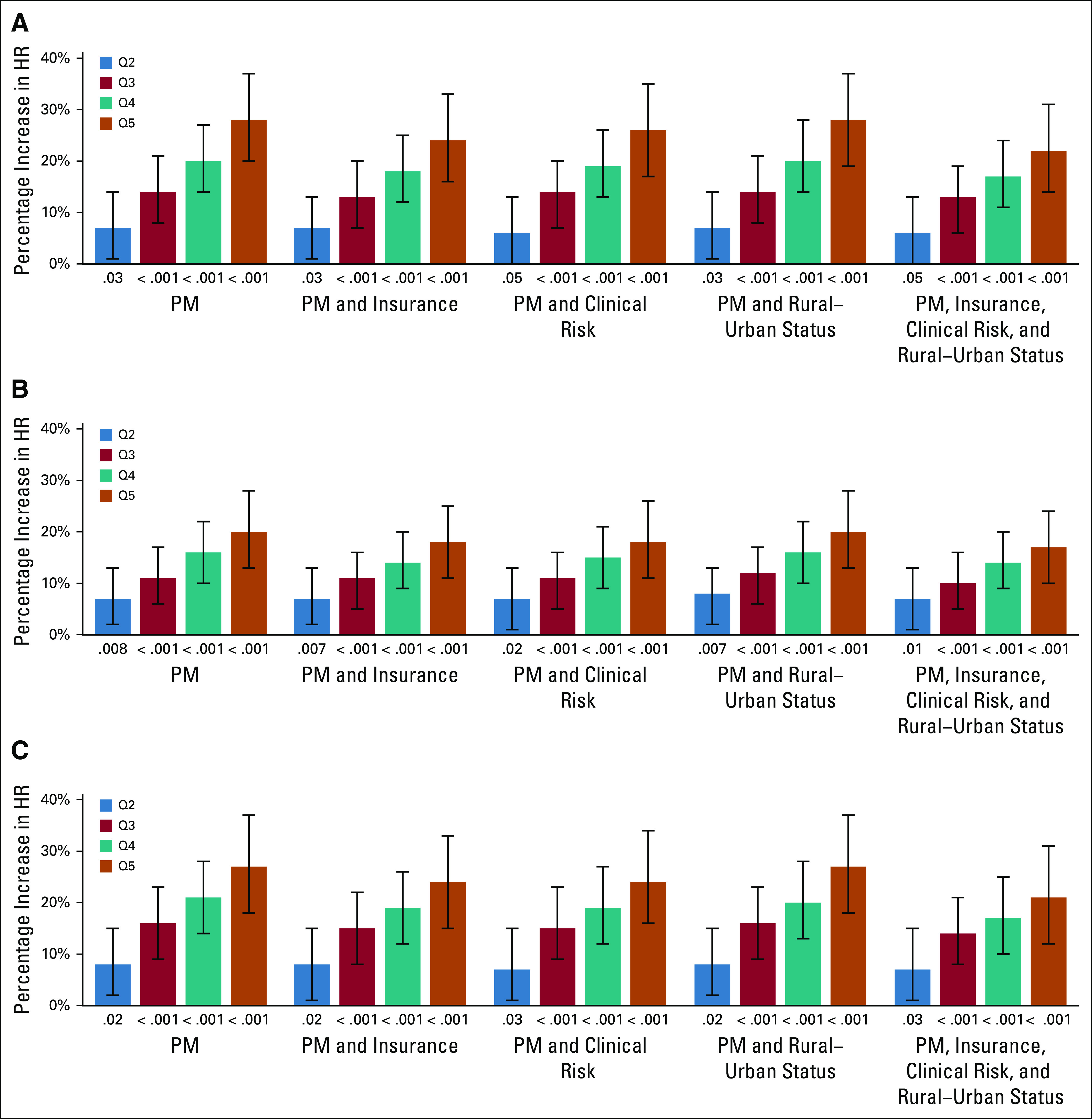
Percentage increase in HR by end point, model, and ADI quintile. (A) Overall survival, (B) progression-free survival, and (C) cancer-specific survival. The results are shown by quintile, defined as Q2, ADI 21%-40%; Q3, ADI 41%-60%; Q4, ADI 61%-80%; and Q5, ADI-81%-100%, most disadvantaged. The P value below each bar represents the comparison for the given quintile of area level deprivation with the lowest area-level deprivation quintile (Q1, ADI 0%-20%, most affluent). Analyses were conducted using Cox regression frailty models; in each model, the cancer type (Data Supplement) was considered a random effect. The vertical lines indicate the 95% CIs. ADI, Area Deprivation Index; HR, hazard ratio; PM, Primary Model.
Additional Analyses
Compared with patients in the most affluent areas, patients in the most deprived areas had statistically significantly greater risk of overall, progression-free, and cancer-specific survival among those who were < 65 years, ≥ 65 years, female, male, White, and non-White, using Medicare or private insurance, with adjuvant disease, with advanced disease, enrolled from 1985 to 1994, 1995 to 2004, or 2005 to 2012, and in rural or urban areas (Fig 3). In contrast, in the small set (10.4%) of patients with Medicaid or no insurance, there was no observed difference in risk of outcomes between patients from the most deprived compared with the most affluent areas.
FIG 3.
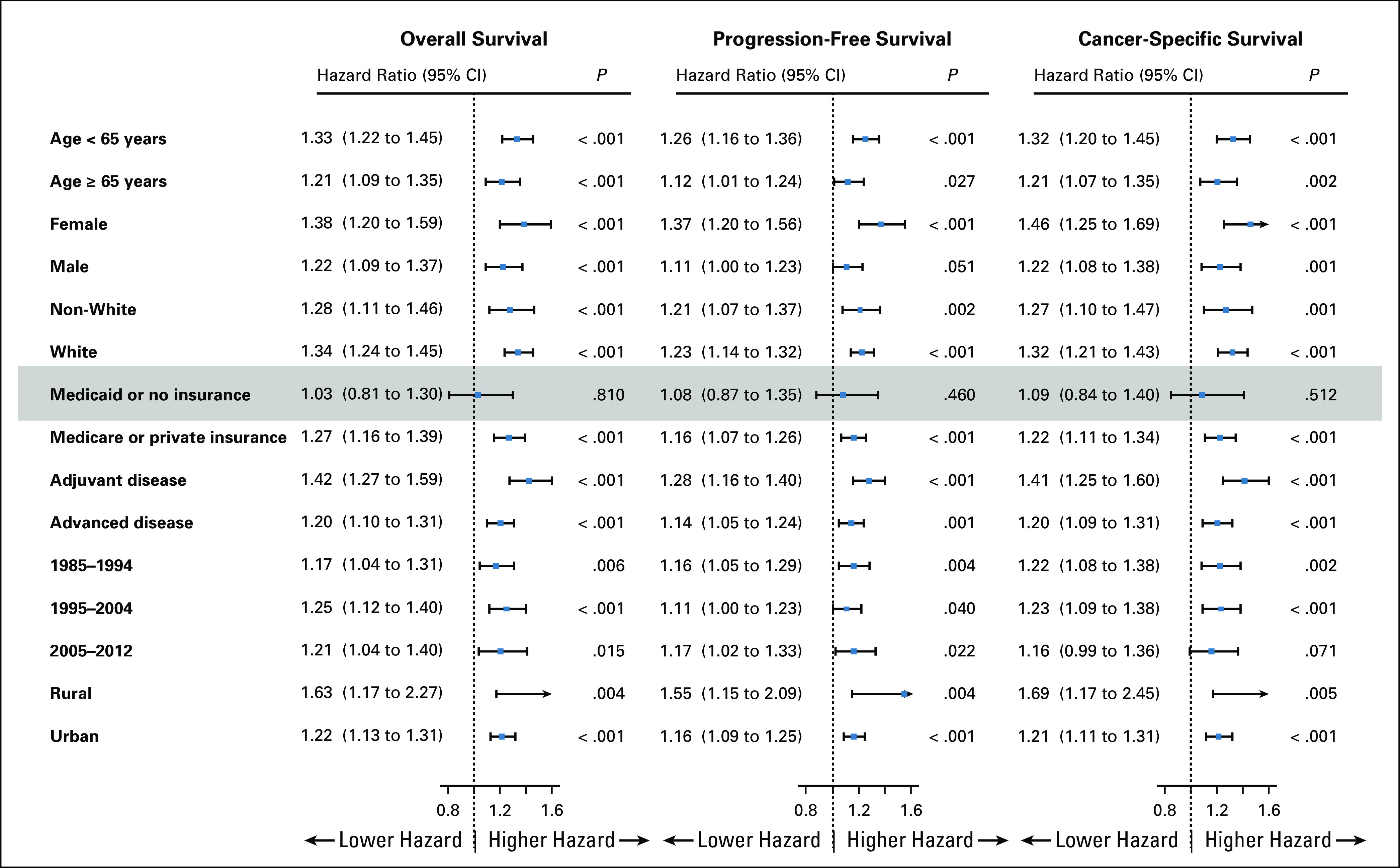
Forest plot of hazard ratio comparing highest deprivation quintile versus lowest deprivation quintile within patient groups. The results are from primary modeling approach, adjusting for age, race, and sex in frailty model with cancer type as random effect. The boxes in the forest plot represent the hazard ratios, and the horizontal lines are the 95% CIs; the vertical line is the line of equal hazard. Findings are statistically significant for all groups except patients with Medicaid or no insurance.
The exclusion of individual cancer cohorts changed the overall hazard ratio from 1.260 (−7.1% change) to 1.311 (+11.1% change; Fig 4). Similarly, only modest changes were also observed for progression-free and cancer-specific survival. The findings were also largely insensitive to the exclusion of individual studies (Data Supplement).
FIG 4.
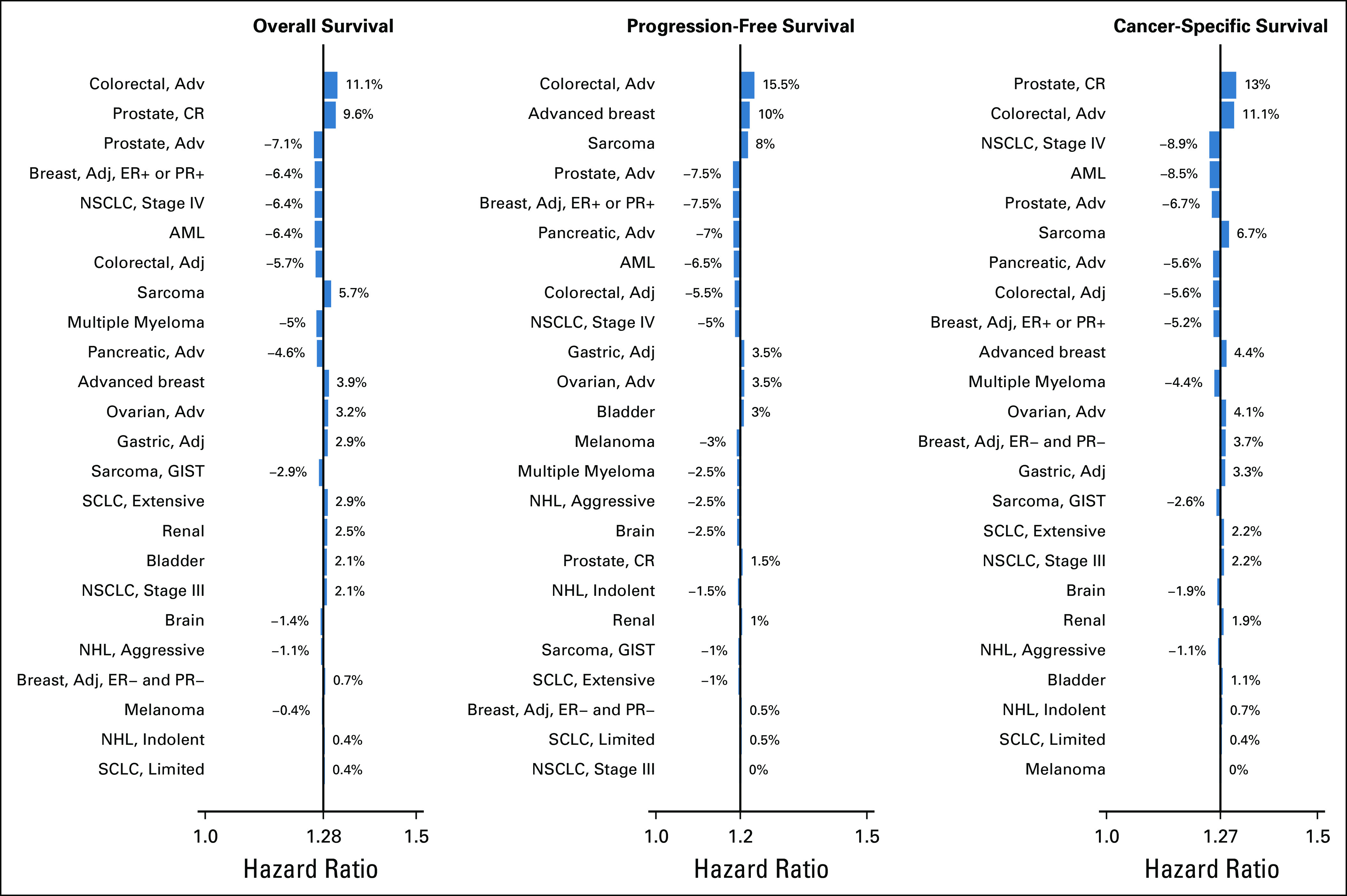
Change in overall frailty regression model results due to excluding individual cancer cohorts (eg, leave one out analysis). For overall survival, progression-free survival, and cancer-specific survival, the difference between the primary model adjusted hazard ratio and the adjusted hazard ratio excluding the specified cancer cohort is shown by the bars. The percentage difference is also shown. Adj, adjuvant; Adv, advanced; AML, acute myeloid leukemia; CR, castration-resistant; ER, estrogen-receptor; GIST, GI stromal tumor; NHL, non-Hodgkin's lymphoma; NSCLC, non–small-cell lung cancer; PR, progesterone receptor; SCLC, small-cell lung cancer.
DISCUSSION
The examination of the relationship between socioeconomic deprivation and cancer outcomes in clinical trial patients with cancer is crucial for understanding whether socioeconomic disparities persist even after accounting for access to quality cancer care. This comprehensive study combined data from more than 40,000 clinical trial patients. Participants were from a wide variety of cancer types and stages, were uniformly staged, prospectively treated, and followed under protocol-directed care. Patients from the most socioeconomically deprived areas were older and more likely to be male, Black, and to have Medicaid or no insurance. Even after accounting for these factors, patients from the most deprived areas had a greater risk of death. The findings were consistent for progression-free and cancer-specific survival, suggesting an association with both cancer and noncancer outcomes. Moreover, the risk of death increased consistently as the level of deprivation increased, irrespective of the strategy for covariate adjustment, representing a dose response to the increasing burden of deprivation. The findings were uniformly observed for all subgroups of patients, with the exception of those with Medicaid or no insurance. Thus, socioeconomic disparities in cancer outcomes persist for almost all patients after accounting for initial access to protocol-directed, quality cancer care in clinical trials.
This study complements and extends previous research linking area-level attributes and outcomes among patients with cancer.11,13,23-27 First, studies using cancer population data cannot account for access to care, an essential consideration when examining cancer health disparities. By using trial data, we implicitly accounted for initial access to uniform, high quality care in the design. Second, we relied on the recently developed ADI, a comprehensive socioeconomic deprivation index.15 One common limitation of clinical trial data is lack of patient-level socioeconomic information. Instead, the ADI is an area- or community-level attribute, although it likely correlates with individual-level measures, so is useful in discriminating outcomes between different individuals in numerous settings.28-30 Third, detailed trial records allowed us to account for uniformly collected clinical risk variables that were unavailable in previous studies. Finally, we included a broad range of different cancers, reinforcing the generalizability of the results.
Previous studies have used census-based area-level poverty or education measures and showed highly variable increases (18%-164%) in risk of mortality for patients in the lowest socioeconomic categories.23,25,26 Only a few studies have applied a multiattribute index to examine this relationship. Singh and Jemal categorized counties according to 11 US Census–based indicators using registry data from the 1990s.11 They found that patients with cancer from the most deprived areas had a 56% increased mortality risk. Hastert et al13 applied a socioeconomic index based on six indicators to a cohort of patients of age 50 to 76 years recruited from 2000 to 2002 and showed a 68% increased mortality risk for those in the most deprived areas. Taken together, these studies showed about a 60% increased risk of mortality, notably greater than the 28% increased risk in our study. If these studies accurately reflect the outsized risk of poor outcomes for patients with cancer living in the most socioeconomically deprived areas, the comparison suggests that access to protocol-guided care may mitigate half of the negative effects of living in socioeconomically deprived areas.
The magnitude of the socioeconomic disparity observed in our study is equivalent to the treatment effect for contemporary large treatment trials.31,32 Our finding is consistent with a previous study demonstrating the enormous potential reductions in cancer-related mortality because of the elimination of socioeconomic disparities.25 The observation that socioeconomic disparities in cancer outcomes persist despite access to treatment is consistent with the idea that low socioeconomic status represents a risk factor for poor health outcomes because of poor access to resources (including medical, technical, and financial resources).1 In this setting, the receipt of protocol-guided therapy may provide beneficial initial access to guideline-based cancer care, but will not otherwise materially alter the tendency toward poor access to healthcare resources over the long term. Other research has suggested the potential effects of chronic stress exposure on health outcomes through mechanisms of altered immunological and neuroendocrine function, mechanisms which would endure despite access to guideline-based care.33,34 Additionally, living in a lower socioeconomic area is associated with more risky health behaviors, including smoking, obesity, physical inactivity, alcohol use, and poor diet.35,36 For vulnerable populations, a diagnosis of cancer may amplify high-risk behaviors.37 Finally, although trial patients are uniformly staged and treated, residual differences in prognosis between patients from socioeconomically deprived and affluent areas may be associated with differences in clinical outcomes.
These findings have policy implications for patients with cancer both in trials and outside trials. Oncology care resources are sparse in certain areas, which will adversely affect those lacking the financial resources to travel for care.38 Thus, even patients able to access initial guideline-based care might not have access to follow-up care, including supportive care and postprogression care. Telehealth models may be vital in such situations, providing the convenience that allows patients to more easily overcome the economic constraints of travel, having to take time off work, or childcare—issues that may be particularly burdensome for individuals in more deprived areas that lack an adequate oncology clinical care infrastructure.39 One notable consequence of the recent COVID-19 pandemic has been the accelerated adoption of telehealth by many oncology care centers.40 This development—if sustained—is likely to benefit both patients and physicians over the long term, especially those living and working in more deprived areas.
More generally, these findings suggest that mechanisms that enable patients with cancer to maintain access to quality care—such as adequate health insurance—are required. Of note, we observed no gradient in clinical outcomes among patients with Medicaid or no insurance, suggesting that residence in affluent areas provides no added benefit for these patients. State-level Medicaid programs provide needed access to healthcare services for socioeconomically deprived individuals, but have historically varied widely in eligibility and the provision of services, with reduced and interrupted access related to adverse cancer outcomes.41 The Affordable Care Act not only provided more ready access to health insurance for all individuals but also strengthened cancer coverage for states adopting the Medicaid expansion,42 with subsequent improvements in coverage for cancer survivors.43 But not all states have participated in the Medicaid expansion, and this legislation is yet to be modified or discontinued. Additionally, Congress recently passed legislation to require state Medicaid programs to cover routine patient costs for cancer clinical trial participation.44 This legislation could provide coverage for routine supportive care that patients with Medicaid may be lacking.
There are limitations to the current study. Although the trials included in the analysis routinely capture protocol treatment data, other data on supportive care administered during therapy, the management of acute complications, and treatments administered after progression are lacking. Details about the types of resources relevant to cancer survivorship were also not available. Additionally, the findings relate to enrollments from a single National Cancer Institute network group, so the results may not be generalizable to other groups. The absence of an observed ADI gradient among patients with Medicaid or no insurance is limited by the relatively few patients in this subgroup, potentially limiting power to identify trends over ADI quartiles. Also, the quality of care for patients enrolled over multiple decades to multiple trials may vary, although since treatment was guided by protocol, the risk of poor quality care was likely minimized. Finally, since the individual cohort–specific effects were considered random, the interpretation about which cancers are primarily subject to socioeconomic adversity is limited.
Our findings suggest that initial access to protocol-guided therapy in a clinical trial is not—by itself—sufficient to eliminate the disparate outcomes related to deprivation. Future research should examine whether the etiology of this residual disparity is related to reduced access to supportive care or postprotocol therapy and/or to differences in health status—determined using linked data sources such as Medicare claims—not reflected by protocol staging criteria. Policies to mitigate socioeconomic differences in cancer outcomes should emphasize access to cancer care services beyond initial therapy. Moreover, understanding whether there are differences in outcomes for patients from poor areas receiving clinical trial care is important for researchers designing and interpreting clinical trials. This is especially true given the increasingly recognized importance of ensuring that trial cohorts adequately represent the cancer population for which the experimental therapy is targeted.
Raymond U. Osarogiagbon
Stock and Other Ownership Interests: Lilly, Pfizer, Gilead Sciences
Honoraria: Biodes
Consulting or Advisory Role: Association of Community Cancer Centers (ACCC), AstraZeneca, American Cancer Society, Triptych Health Partners
Patents, Royalties, Other Intellectual Property: 2 US and 1 China patents for lymph node specimen collection kit and method of pathologic evaluation
Other Relationship: Oncobox
Scott D. Ramsey
Employment: Flatiron Health
Consulting or Advisory Role: Bayer, Genentech, Bristol-Myers Squibb, AstraZeneca, Merck, GRAIL, Pfizer, Seattle Genetics, Biovica
Research Funding: Bayer, Bristol-Myers Squibb, Microsoft
Travel, Accommodations, Expenses: Bayer Schering Pharma, Bristol-Myers Squibb, Flatiron Health, Bayer, GRAIL
Dawn L. Hershman
Consulting or Advisory Role: AIM Specialty Health
No other potential conflicts of interest were reported.
DISCLAIMER
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or The Hope Foundation for Cancer Research.
PRIOR PRESENTATION
Presented in part at the ASCO Quality Care Symposium, San Diego, CA, September 6-7, 2019.
SUPPORT
Supported by the National Cancer Institute of the National Institutes of Health under Award Numbers UG1CA189974, U10CA180888, and U10CA180819; by an American Cancer Society Research Scholar Grant (Unger; Award Number: 134589-RSGI-20-027-01-CPHPS); and in part by The Hope Foundation for Cancer Research (Unger).
AUTHOR CONTRIBUTIONS
Conception and design: Joseph M. Unger, Anna B. Moseley, Christabel K. Cheung, Dawn L. Hershman
Financial support: Joseph M. Unger
Collection and assembly of data: Joseph M. Unger, Anna B. Moseley, Dawn L. Hershman
Data analysis and interpretation: Joseph M. Unger, Anna B. Moseley, Raymond U. Osarogiagbon, Banu Symington, Scott D. Ramsey, Dawn L. Hershman
Manuscript writing: All authors
Final approval of manuscript: All authors
Accountable for all aspects of the work: All authors
AUTHORS' DISCLOSURES OF POTENTIAL CONFLICTS OF INTEREST
Persistent Disparity: Socioeconomic Deprivation and Cancer Outcomes in Patients Treated in Clinical Trials
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to www.asco.org/rwc or ascopubs.org/jco/authors/author-center.
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (Open Payments).
Raymond U. Osarogiagbon
Stock and Other Ownership Interests: Lilly, Pfizer, Gilead Sciences
Honoraria: Biodes
Consulting or Advisory Role: Association of Community Cancer Centers (ACCC), AstraZeneca, American Cancer Society, Triptych Health Partners
Patents, Royalties, Other Intellectual Property: 2 US and 1 China patents for lymph node specimen collection kit and method of pathologic evaluation
Other Relationship: Oncobox
Scott D. Ramsey
Employment: Flatiron Health
Consulting or Advisory Role: Bayer, Genentech, Bristol-Myers Squibb, AstraZeneca, Merck, GRAIL, Pfizer, Seattle Genetics, Biovica
Research Funding: Bayer, Bristol-Myers Squibb, Microsoft
Travel, Accommodations, Expenses: Bayer Schering Pharma, Bristol-Myers Squibb, Flatiron Health, Bayer, GRAIL
Dawn L. Hershman
Consulting or Advisory Role: AIM Specialty Health
No other potential conflicts of interest were reported.
REFERENCES
- 1.Link BG, Phelan J: Social conditions as fundamental causes of disease. J Health Soc Behav 80-94, 1995 [PubMed] [Google Scholar]
- 2.Butler DC Petterson S Phillips RL, et al. : Measures of social deprivation that predict health care access and need within a rational area of primary care service delivery. Health Serv Res 48:539-559, 2013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Chen E, Miller GE: Socioeconomic status and health: Mediating and moderating factors. Annu Rev Clin Psychol 9:723-749, 2013 [DOI] [PubMed] [Google Scholar]
- 4.Cutler DM, Lleras-Muney A, Vogl T: Socioeconomic status and health: Dimensions and mechanisms. NBER Working Paper No. 14333. 2008. [Google Scholar]
- 5.Hines R Markossian T Johnson A, et al. : Geographic residency status and census tract socioeconomic status as determinants of colorectal cancer outcomes. Am J Public Health 104:e63-71, 2014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Johnson AM Hines RB Johnson JA III, et al. : Treatment and survival disparities in lung cancer: The effect of social environment and place of residence. Lung Cancer 83:401-407, 2014 [DOI] [PubMed] [Google Scholar]
- 7.Lin Y, Wimberly MC: Geographic variations of colorectal and breast cancer late-stage diagnosis and the effects of neighborhood-level factors. J Rural Health 33:146-157, 2017 [DOI] [PubMed] [Google Scholar]
- 8.Towne SD, Jr, Smith ML, Ory MG: Geographic variations in access and utilization of cancer screening services: Examining disparities among American Indian and Alaska native elders. Int J Health Geogr 13:18, 2014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.DeRouen MC Parsons HM Kent EE, et al. : Sociodemographic disparities in survival for adolescents and young adults with cancer differ by health insurance status. Cancer Causes Control 28:841-851, 2017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Singer S Bartels M Briest S, et al. : Socio-economic disparities in long-term cancer survival-10 year follow-up with individual patient data. Support Care Cancer 25:1391-1399, 2017 [DOI] [PubMed] [Google Scholar]
- 11.Singh GK, Jemal A: Socioeconomic and racial/ethnic disparities in cancer mortality, incidence, and survival in the United States, 1950-2014: Over six decades of changing patterns and widening inequalities. J Environ Public Health 2017:2819372, 2017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Silber JH Rosenbaum PR Ross RN, et al. : Disparities in breast cancer survival by socioeconomic status despite Medicare and Medicaid insurance. Milbank Q 96:706-754, 2018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Hastert TA Beresford SA Sheppard L, et al. : Disparities in cancer incidence and mortality by area-level socioeconomic status: A multilevel analysis. J Epidemiol Community Health 69:168-176, 2015 [DOI] [PubMed] [Google Scholar]
- 14.Hershman DL Till C Wright JD, et al. : Healthcare utilization and cost of care in elderly breast cancer patients enrolled in SWOG clinical trials. Breast Cancer Res Treat 181:455-463, 2020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Kind AJH, Buckingham WR: Making neighborhood-disadvantage metrics accessible—the neighborhood atlas. N Engl J Med 378:2456-2458, 2018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Durfey SNM Kind AJH Buckingham WR, et al. : Neighborhood disadvantage and chronic disease management. Health Serv Res 54:206-216, 2019. (suppl 1) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Gordon SH Lee Y Ndumele CD, et al. : The impact of Medicaid managed care plan type on continuous Medicaid enrollment: A natural experiment. Health Serv Res 53:3770-3789, 2018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Joynt Maddox KE Reidhead M Hu J, et al. : Adjusting for social risk factors impacts performance and penalties in the hospital readmissions reduction program. Health Serv Res 54:327-336, 2019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Sheets L Petroski GF Jaddoo J, et al. : The effect of neighborhood disadvantage on diabetes prevalence. AMIA Annu Symp Proc 2017:1547-1553, 2017 [PMC free article] [PubMed] [Google Scholar]
- 20.US Department of Agriculture . Rural-Urban Continuum Codes. https://www.ers.usda.gov/data-products/ruralurban-continuum-codes/.aspx [Google Scholar]
- 21.Cox DR: Regression models and life tables. J R Stat Soc Ser B 1972;342:187-220. [Google Scholar]
- 22.Kalbfleish JD, Prentice RP: The Statistical Analysis of Failure Time Data. Hoboken, NJ, John Wiley, 1980 [Google Scholar]
- 23.Boscoe FP Johnson CJ Sherman RL, et al. : The relationship between area poverty rate and site-specific cancer incidence in the United States. Cancer 120:2191-2198, 2014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Moy E Garcia MC Bastian B, et al. : Leading causes of death in nonmetropolitan and metropolitan areas—United States, 1999-2014. MMWR Surveill Summ 66:1-8, 2017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Siegel R Ward E Brawley O, et al. : Cancer statistics, 2011: The impact of eliminating socioeconomic and racial disparities on premature cancer deaths. CA Cancer J Clin 61:212-236, 2011 [DOI] [PubMed] [Google Scholar]
- 26.Siegel RL, Miller KD, Jemal A: Cancer statistics, 2019. CA Cancer J Clin 69:7-34, 2019 [DOI] [PubMed] [Google Scholar]
- 27.Singh GK Williams SD Siahpush M, et al. : Socioeconomic, rural-urban, and racial inequalities in US cancer mortality: Part I-all cancers and lung cancer and part II-colorectal, prostate, breast, and cervical cancers. J Cancer Epidemiol 2011:107497, 2011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Hu J, Kind AJH, Nerenz D: Area deprivation index predicts readmission risk at an urban teaching hospital. Am J Med Qual 33:493-501, 2018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kind AJ Jencks S Brock J, et al. : Neighborhood socioeconomic disadvantage and 30-day rehospitalization: A retrospective cohort study. Ann Intern Med 161:765-774, 2014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Powell WR Buckingham WR Larson JL, et al. : Association of neighborhood-level disadvantage with Alzheimer disease neuropathology. JAMA Netw Open 3:e207559, 2020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Mayer RJ Van Cutsem E Falcone A, et al. : Randomized trial of TAS-102 for refractory metastatic colorectal cancer. N Engl J Med 372:1909-1919, 2015 [DOI] [PubMed] [Google Scholar]
- 32.Stupp R Taillibert S Kanner AA, et al. : Maintenance therapy with tumor-treating fields plus temozolomide vs temozolomide alone for glioblastoma: A randomized clinical trial. JAMA 314:2535-2543, 2015 [DOI] [PubMed] [Google Scholar]
- 33.Cole SW: Human social genomics. PLoS Genet 10:e1004601, 2014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Thaker PH Han LY Kamat AA, et al. : Chronic stress promotes tumor growth and angiogenesis in a mouse model of ovarian carcinoma. Nat Med 12:939-944, 2006 [DOI] [PubMed] [Google Scholar]
- 35.Heymach J Krilov L Alberg A, et al. : Clinical cancer advances 2018: Annual report on progress against cancer from the American Society of Clinical Oncology. J Clin Oncol 36:1020-1044, 2018 [DOI] [PubMed] [Google Scholar]
- 36.Blackwell DL, Lucas JW, Clarke TC: Summary health statistics for U.S. Adults: National Health Interview Survey, 2012. Vital Health Stat 10:1-161, 2014 [PubMed] [Google Scholar]
- 37.Tucker-Seeley RD, Thorpe RJ: Material-psychosocial-behavioral aspects of financial hardship: A conceptual model for cancer prevention. Gerontologist 59:S88-s93, 2019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Kirkwood MK Bruinooge SS Goldstein MA, et al. : Enhancing the American Society of Clinical Oncology workforce information system with geographic distribution of oncologists and comparison of data sources for the number of practicing oncologists. J Oncol Pract 10:32-38, 2014 [DOI] [PubMed] [Google Scholar]
- 39.Cox A Lucas G Marcu A, et al. : Cancer survivors' experience with telehealth: A systematic review and thematic synthesis. J Med Internet Res 19:e11, 2017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Schrag D, Hershman DL, Basch E: Oncology practice during the COVID-19 pandemic. JAMA 323:2005-2006, 2020 [DOI] [PubMed] [Google Scholar]
- 41.Bradley CJ Gardiner J Given CW, et al. : Cancer, Medicaid enrollment, and survival disparities. Cancer 103:1712-1718, 2005 [DOI] [PubMed] [Google Scholar]
- 42.Umutyan A Chiechi C Beckett LA, et al. : Overcoming barriers to cancer clinical trial accrual: Impact of a mass media campaign. Cancer 112:212-219, 2008 [DOI] [PubMed] [Google Scholar]
- 43.Nikpay SS, Tebbs MG, Castellanos EH: Patient protection and affordable care act Medicaid expansion and gains in health insurance coverage and access among cancer survivors. Cancer 124:2645-2652, 2018 [DOI] [PubMed] [Google Scholar]
- 44.H.R.6836—Clinical Treatment Act. 115th Congress (ed 2). https://www.congress.gov/bill/115th-congress/house-bill/6836/text, 2018 [Google Scholar]