

ABSTRACT
Depression is a mental illness affecting more than 260 million people worldwide. In Greenland, the prevalence of patients treated with antidepressant medicine (antidepressants) has not previously been investigated. The aim of this study was to estimate and compare the age- and gender-specific prevalence of patients treated with antidepressants in Greenland and Denmark. The study was a cross-sectional register study using data from population and medical registers in Greenland and Denmark. Included was 1,573 Greenlandic patients and 419,151 Danish patients treated with antidepressants, respectively. The overall prevalence of patients aged 10–89 years treated with antidepressants was 3.5% in Greenland, and 8.1% in Denmark, being significantly lower in Greenland compared to Denmark (p < 0.001). The age- and gender-specific prevalence was significantly lower for patients from Greenland compared to from Denmark. In both Greenland and Denmark, the prevalence of women receiving antidepressants was significantly higher than for men. Finally, there was regional differences in the prevalence of usage of antidepressants in Greenland. Undiagnosed depression might contribute to the lower prevalence in Greenland as well as limited access to primary healthcare.
KEYWORDS: Antidepressant medicine, depression, prevalence, Denmark, Greenland
Introduction
Depression is one of the most common mental illnesses worldwide among adults [1]. It is becoming increasingly frequent in the general population, and has therefore become an important public health problem. The number of incident cases of depression worldwide increased with almost 50% within the last few decades from 1990 to 2017 [2]. The latest numbers from WHO furthermore show that more than 264 million people worldwide suffer from depression [3]. A systematic review of mental disorders in Europe [4] found the prevalence of depression in the population to be 8%, and that the risk of suffering from depression during a lifetime is between 17–18%. WHO ranked depression as the third cause of burden of disease worldwide and projected that the disease will rank first by 2030 [5].
Depression is a serious illness that has a profound effect on health, as it reduces functioning and quality of life. Depression is accompanied by high mortality [6], severe morbidity [7] and high socioeconomic costs [8] relative to sick days, hospitalisations, and early retirement. Correct diagnosis, sufficient assessment of the duration of the depression, degree of illness and depression subtype, presence of any comorbidity and current psychosocial strains are the prerequisite for choosing the right treatment. This applies to both the choice of medicine and psychotherapeutic treatment. Treatment of depression involves both the treatment of the depression itself as well as prevention of possible future depressions. Antidepressant medicine, i.e. antidepressants, constitutes a group of drugs used to treat moderate to severe depression, is among the most prescribed drugs in Europe [9]. Besides depression, antidepressants are also used for a wide range of other conditions such as anxiety disorders, panic disorders, phobia, posttraumatic stress disorder and chronic pain condition. In addition, antidepressants are also used in clinical practice for other indications, e.g. eating disorders, dysthymia and for the treatment of adverse symptoms in patients with schizophrenia. According to the Danish Board of Health, 414,521 people received antidepressants in 2016, corresponding to approximately 7% of Denmark’s population [10]. However, the prevalence of people receiving antidepressants in Denmark has not been investigated since 2016, and it has never before been investigated in Greenland.
In Greenland, the healthcare system is challenged by lack of qualified health care providers, financial constraints, and having to deliver high quality treatments in a very large and sparsely populated country. Thus, ensuring diagnosis and treatment of depression can be challenging as the disease often progresses chronically, and as it takes weeks for the antidepressants to work, while the side effects come immediately. A systematic review and network meta-analysis of 195 countries [2] identified Greenland as the country with the third highest age-standardised incidence rate of major depression (6.26 per 1000) in 2017. A number of studies furthermore indicate a high degree of mental vulnerability in Greenland [11,12], including a high suicide rate [13] and many medication overdoses [14]. In Greenland, the prevalence of patients treated with antidepressants is unknown. Therefore, the primary aim of this study was to estimate the age- and gender-specific prevalence of depression in Greenland, using treatment with antidepressant as a proxy,, and to compare the prevalence with the Danish data.
Material and methods
Study design
The study was performed as a cross-sectional study, using data from population and medical registers in Greenland [15,16] and Denmark [17,18].
Setting
Greenland is the world’s largest island, with a population of 55,992 people (in 2019) located in 17 towns and approximately 60 settlements along the coast. Almost the entire population of Greenland live in South and West Greenland, while only approximately 10% live in East and North Greenland. The majority of Greenland’s population are urban dwellers. About 60% of Greenland’s population live in the five largest cities (Nuuk, Sisimiut, Ilulissat, Aasiaat and Qaqortoq). Most inhabitants are born in Greenland. In Nuuk, newcomers from Denmark and the rest of the world constitute approximately 11%. Greenland was previously a Danish colony, and is now a self-governed country under the Danish kingdom.
The Greenlandic healthcare system is organised in five regions (Kujataa, Sermersooq, Qeqqa, Disko, Avannaa) (see Figure 1) covering a number of towns and settlements. In each region, there are the following treatment sites; one regional hospital, health centres, nursing stands and settlement consultations. The regional hospital is located in the largest city in the region (Kujataa: Qaqortoq, Sermersooq: Nuuk, Qeqqa: Sisimiut, Disko: Aasiaat, Avannaa: Ilulissat) (see Figure 1). Each region is managed by a regional management consisting of a Leading Regional Doctor and a Leading Regional Nurse. Each town has a primary health care centre, whereas minor health care units exist in the settlements. In most towns in Greenland, physicians are working for short-term periods. The National Hospital (Queen Ingrids Hospital, DIH) is located in the capital, Nuuk, which provides secondary specialised health care for the entire country. Depression is treated at local health centres and regional hospitals, while serious cases and suicidal people are referred to the psychiatric ward at DIH Nuuk.
Figure 1.

Illustration of the Greenlandic health system’s organisation in five regions (Kujataa, Sermersooq, Qeqqa, Disko, Avannaa). The regional hospital is located in the largest city in the region (Kujataa: Qaqortoq, Sermersooq: Nuuk, Qeqqa: Sisimiut, Disko: Aasiaat, Avannaa: Ilulissat)
The following cities in the five regions are included in this study:Kujataa: Qaqortoq*, Narsaq, Nanortalik and settlements.Sermersooq: Nuuk*, Paamiut, Ittoqqortoormiut and settlements.Qeqqa: Sisimiut*, Maniitsoq and settlements.Disko: Aasiaat*, Qeqertarsuaq, Qasigiannguit and settlements.Avannaa: Ilulissat*, Uummannaq, Upernavik, Qaanaaq and settlements.*Localisation of the regional hospital.The population number in each region are marked on the figure.https://commons.wikimedia.org/wiki/File:Greenland-Icecap-contours-map.svg
In Greenland, health care is free for the inhabitants. All medicine with prescription is free of charge and is handed out at the pharmacies, which are located as a part of the primary health care centres. In Denmark, the health care system consists of a primary and a secondary sector. The primary sector consists of the general physicians, who have the authority to refer patients to the secondary sector, consisting of the hospitals and other specialised medical units. These health care services are also free in Denmark. On the other hand, all prescribed medicine are available at pharmacies, against payment, but there is some coverage of the expenditures from the health care system.
Study population
The study included patients aged 10–89 years residing in Greenland or Denmark. In Greenland, medical data was extracted from the electronic medical record (EMR) system from 16 towns (all of Greenland except Tasiilaq, which has a different journal system). Patients, who in 2019 had received a prescription for antidepressants, were identified using the anatomic classification code N06A (sertralin, citalopram, mirtazapine and venlafaxine), and included in the analysis. As background population, the population number (age group 10–89 years) in Greenland (in the abovementioned 16 towns except for Tasiilaq) as of 1 January 2019 was found from Greenland online statistics bank. This population accounted for 81.32% of the entire Greenlandic population [15].
In Denmark, medical data was available in an online medical register system containing age- and gender-specific data for > 99% of all sold antidepressants [18]. Data from 2019 was used in the analyses. The population (age group 10–89 years) from the 1st quarter of 2019 from Denmark’s online statistics bank was used as background population [17].
Statistical analyses
Estimates were calculated with 95% confidence intervals. The prevalence was calculated for each age group with the background population (the population of Greenland expect for Tasiilaq) as the denominator. Variables were described using means and standard deviation (SD). QQ-plots were used to check for normality. Chi-square tests were used to compare frequencies. Normally distributes variables were compared using two-tailed t-test. P-values below 0.05 were considered significant. Statistical analyses were performed using IBM SPSS Statistics 27.
The study was approved by The Ethics Committee for Medical Research in Greenland and by The Agency for Health and Prevention in Greenland.
Results
A total of 1,573 Greenlandic patients and 419,151 Danish patients treated with antidepressants were included in the study. The study population consisted of 506 (32.2%) men and 1,067 (67.8%) women in Greenland and 151,064 (36.0%) men and 268,087 (64.0%) women in Denmark.
Table 1 show the prevalence of patients treated with antidepressants in Greenland compared to Denmark according to gender and age. In Greenland, the total prevalence for men and women aged 10–89 years was significantly lower (p < 0.001) than in Denmark (3.5% compared to 8.1%). Furthermore, except for the age group 10–19 years, the total prevalence of men and women within each age group was significantly lower in Greenland (p < 0.001) compared to Denmark. For both countries, the total prevalence was positively correlated with age.
Table 1.
Age- and gender-specific prevalence of patients treated with antidepressants in Greenland and Denmark
| Prevalence (%) in age groups | Total (men and women), % (95% CI) (n/N) |
Men, % (95% CI) (n/N) |
Women, % (95% CI) (n/N) |
Men vs women |
|||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Greenland |
Denmark |
||||||||||
| Greenland | Denmark | P-value RR (95% CI) |
Greenland | Denmark | P-value RR (95% CI) |
Greenland | Denmark | P-value RR (95% CI) |
P-value RR (95% CI) |
P-value RR (95% CI) |
|
| 10–19 years | 1.1 (0.8–1.3) (73/6.846) |
1.2 (1.1–1.2) (7.945/683.669) |
0.462 0.92 (0.73–1.15) |
0.5 (0.3–0.8) (19/3.501) |
0.8 (0.8–0.8) (2.820/350.177) |
0.083 0.67 (0.43–1.06) |
1.6 (1.2–2.0) (54/3.345) |
1.5 (1.5–1.6) (5.125/333.492) |
0.717 1.05 (0.81–1.37) |
<0.001 0.34 (0.30–0.57) |
<0.001 0.16 (0.15–0.17) |
| 20–29 years | 2.6 (2.2–2.9) (216/8.421) |
4.8 (4.7–4.8) (37.492/783.879) |
<0.001 0.54 (0.47–0.61) |
1.5 (1.1–1.9) (65/4.341) |
3.5 (3.4–3.5) (13.938/400.078) |
<0.001 0.43 (0.34–0.55) |
3.7 (3.1–4.3) (151/4.080) |
6.1 (6.1–6.2) (23.554/383.801) |
<0.001 0.60 (0.52–0.71) |
<0.001 0.40 (0.30–0.54) |
<0.001 0.57 (0.56–0.58) |
| 30–39 years | 2.8 (2.4–3.2) (215/7.636) |
6.8 (6.7–6.8) (46.043/681.161) |
<0.001 0.42 (0.37–0.48) |
1.8 (1.4–2.2) (71/3.936) |
5.1 (5.0–5.1) (17.482/345.904) |
<0.001 0.36 (0.28–0.45) |
3.9 (3.3–4.5) (144/3.700) |
8.5 (8.4–8.6) (28.561/335.257) |
<0.001 0.46 (0.39–0.54) |
<0.001 0.46 (0.35–0.61) |
<0.001 0.59 (0.58–0.60) |
| 40–49 years | 4.3 (3.8–4.9) (257/5.922) |
8.7 (8.6–8.8) (66.284/762.648) |
<0.001 0.5 (0.44–0.56) |
2.6 (2.1–3.2) (85/3.230) |
6.4 (6.3–6.5) (24.386/382.551) |
<0.001 0.41 (0.33–0.51) |
6.4 (5.5–7.3) (172/2.692) |
11.0 (10.9–11.1) (41.898/380.097) |
<0.001 0.58 (0.50–0.67) |
<0.001 0.41 (0.32–0.53) |
<0.001 0.58 (0.57–0.59) |
| 50–59 years | 4.0 (3.6–4.4) (359/9.077) |
9.6 (9.6–9.7) (76.951/797.775) |
<0.001 0.41 (0.36–0.44) |
2.3 (1.9–2.7) (112/4.920) |
7.2 (7.1–7.3) (28.820/400.964) |
<0.001 0.32 (0.26–0.38) |
5.9 (5.2–6.7) (247/4.157) |
12.1 (12.0–12.2) (48.131/396.811) |
<0.001 0.49 (0.43–0.55) |
<0.001 0.38 (0.31–0.48) |
<0.001 0.59 (0.58–0.60) |
| 60–69 years | 4.4 (3.8–5.0) (221/5.004) |
10.5 (10.4–10.6) (69.603/662.929) |
<0.001 0.42 (0.37–0.48) |
3.0 (2.4–3.6) (84/2.819) |
8.1 (8.0–8.1) (26.254/325.943) |
<0.001 0.37 (0.30–0.46) |
6.3 (5.3–7.3) (137/2.185) |
12.9 (12.8–13.0) (43.349/336.986) |
<0.001 0.49 (0.43–0.57) |
<0.001 0.48 (0.36–0.62) |
<0.001 0.63 (0.62–0.64) |
| 70–79 years | 7.9 (6.8–9.1) (167/2.104) |
12.1 (12.0–12.2) (66.693/552.058) |
<0.001 0.66 (0.57–0.76) |
4.6 (3.4–5.8) (53/1.161) |
9.4 (9.3–9.5) (24.622/262.429) |
<0.001 0.49 (0.37–0.63) |
12.1 (10.0–14.2) (114/943) |
14.5 (14.4–14.7) (42.071/289.629) |
0.034 0.83 (0.70–0.99) |
<0.001 0.38 (0.28–0.52) |
<0.001 0.65 (0.64–0.66) |
| 80–89 years | 12.4 (9.6–15.2) (65/525) |
18.3 (18.2–18.5) (40.152/219.003) |
<0.001 0.68 (0.54–0.85) |
7.8 (4.3–11.4) (17/217) |
14.0 (13.7–14.2) (12.742/91.188) |
0.009 0.56 (0.36–0.89) |
15.6 (11.5–19.6) (48/308) |
21.4 (21.2–21.7) (27.410/127.815) |
0.012 0.73 (0.56–0.94) |
0.008 0.50 (0.30–0.85) |
<0.001 0.65 (0.64–0.66) |
| Total (10–89 years) | 3.5 (3.3–3.6) (1.573/45.535) |
8.1 (8.1–8.2) (419.151/ 5.143.122) |
<0.001 0.42 (0.40–0.45) |
2.1 (1.9–2.3) (506/24.125) |
5.9 (5.9–5.9) (151.064/ 2.559.234) |
<0.001 0.36 (0.33–0.39) |
5.0 (4.7–5.3) (1.067/ 21.410) |
10.4 (10.3–10.4) (268.087/ 2.583.888) |
<0.001 0.48 (0.45–0.51) |
<0.001 0.42 (0.38–0.47) |
<0.001 0.57 (0.57–0.57) |
95% CI: Confidence interval, n: Number of patients treated with antidepressants, N: Number of people in the background population.
P-values below 0.05 are in bold. RR = Risk Ratio.
For men aged 10–89 years, the total prevalence was significantly lower (p < 0.001) in Greenland compared to Denmark (2.1% compared to 5.9%). The prevalence for men aged 20–89 years was significantly lower in Greenland compared to Denmark (p < 0.001 for age group 20–79 years, and p = 0.009 for age group 80–89 years). In accordance, calculation of risk ratios based on the prevalence estimated in Table 1 showed that Greenlandic men of all ages had a lower risk (0.45 times on average) of using antidepressants compared to Danish men (Figure 2).
Figure 2.
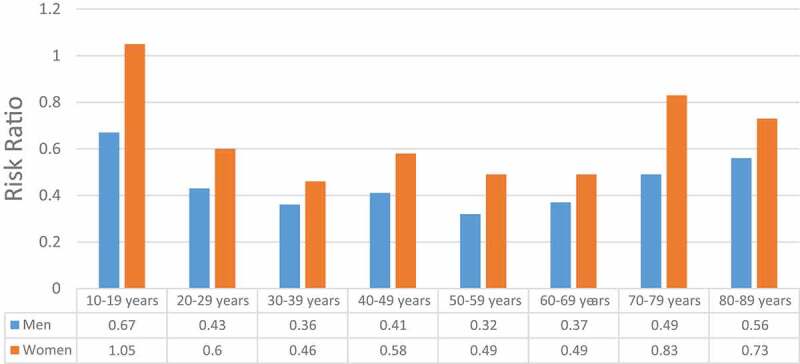
Risk ratios of age- and gender-specific prevalence in Greenland compared to Denmark
Risk ratios based on calculated prevalence from Table 1. The risk ratios describe the risk of Greenlandic men and women of different ages receiving antidepressants compared to Danish men and women of similar age groups.
For women aged 10–89 years, the total prevalence was significantly lower in Greenland (p < 0.001) compared to Denmark (5.0% compared to 10.4%). There was no difference in prevalence of usage of antidepressants in the age group 10–19 years between Denmark and Greenland. The prevalence for women aged 20–89 years was significantly lower in Greenland compared to Denmark (p < 0.001 for age groups 20–69 years, and p < 0.05 for age groups 70–89 years). Calculation of risk ratios supported this trend (Figure 2), as Greenlandic women aged 10–19 years had a similar risk as Danish women aged 10–19 years of using antidepressants (i.e. a risk ratio ~1), while Greenlandic women of the remaining age groups had a lower risk of using antidepressant than Danish women (0.60 times on average).
For both men and women in Greenland and Denmark, the prevalence increased with age (from age 10–89 years), except for Greenlandic men and women aged 50–59 years, where a slight decrease was observed compared to the age group 40–49 years of age. However, the slight decrease is associated with uncertainty, as the confidence intervals between the two age groups overlap, and an actual decrease might thus not exist.
In both Greenland and Denmark, the prevalence was significantly higher among women within each listed age group (Denmark ages 10–89 years: p < 0.001; Greenland ages 10–79 years: p < 0.001 and 80–89 years: p < 0.01) compared to men. Consequently, the total prevalence among women was significantly higher (p < 0.001) than among men in both Greenland and Denmark: Greenland; 5.0% compared to 2.1% and Denmark; 10.4% compared to 5.9%, respectively (only p-value and risk ratio shown in Table 1).
The overall prevalence of patients aged 10–89 years treated with antidepressants for each region in Greenland is illustrated in Table 2. A significant difference between the regions was observed (p < 0.001). The highest prevalence was observed in region Sermersooq (4.9%) followed by Qeqqa (3.0%), Avannaa (2.7%), Disko (2.2%) and Kujataa (2.2%). For all regions, the total prevalence of patients aged 10–89 years treated with antidepressants increased with age, except for the age-group 50–59 years (Figure 3). The prevalence in Nuuk was significantly higher (p = 0.003) than the rest of region Sermersooq (5.0% compared to 3.3%), and also significantly higher (p < 0.001) than in the rest of Greenland which was found to be 2.6% (data not shown).
Table 2.
Overall prevalence of patients treated with antidepressants (N06A) for each region in Greenland
| Prevalence (%) in age groups | Kujataa |
Sermersooq |
Qeqqa |
Disko |
Avannaa |
Total |
P |
|---|---|---|---|---|---|---|---|
| % (95% CI) (n/N) | |||||||
| 10–19 years | 0.1 (−0.1–0.4) (1/825) |
1.6 (1.1–2.2) (40/2.432) |
1.3 (0.7–2.0) (17/1.271) |
0.4 (0.0–0.9) (4/925) |
0.8 (0.3–1.3) (11/1.393) |
1.1 (0.8–1.3) (73/6.846) |
0.001 |
| 20–29 years | 0.9 (0.3–1.5) (9/964) |
4.2 (3.5–4.9) (138/3.288) |
1.8 (1.1–2.4) (26/1.479) |
0.6 (0.1–1.0) (6/1.036) |
2.2 (1.5–2.9) (37/1.654) |
2.6 (2.2–2.9) (216/8.421) |
<0.001 |
| 30–39 years | 1.9 (0.9–2.8) (15/794) |
3.6 (3.0–4.2) (120/3.329) |
2.8 (1.9–3.7) (35/1.259) |
1.1 (0.4–1.8) (9/821) |
2.5 (1.7–3.3) (36/1.433) |
2.8 (2.4–3.2) (215/7.636) |
0.001 |
| 40–49 years | 3.6 (2.1–5.1) (21/588) |
5.4 (4.5–6.3) (131/2.422) |
4.5 (3.2–5.8) (46/1.023) |
2.6 (1.4–3.8) (17/656) |
3.4 (2.4–4.4) (42/1.233) |
4.3 (3.8–4.9) (257/5.922) |
0.005 |
| 50–59 years | 3.1 (2.1–4.1) (36/1.174) |
5.7 (5.0–6.5) (193/3.361) |
3.0 (2.1–3.8) (48/1.622) |
2.8 (1.8–3.8) (31/1.112) |
2.8 (2.1–3.6) (51/1.808) |
4.0 (3.6–4.4) (359/9.077) |
<0.001 |
| 60–69 years | 3.0 (1.8–4.1) (23/779) |
6.2 (5.1–7.3) (111/1.788) |
3.9 (2.6–5.1) (35/904) |
3.2 (1.8–4.5) (20/630) |
3.5 (2.3–4.7) (32/903) |
4.4 (3.8–5.0) (221/5.004) |
<0.001 |
| 70–79 years | 2.8 (1.2–4.4) (11/395) |
15.2 (12.2–18.2) (83/547) |
4.8 (2.7–7.0) (19/393) |
7.6 (4.8–10.4) (26/341) |
6.5 (4.2–8.9) (28/428) |
7.9 (6.8–9.1) (167/2.104) |
<0.001 |
| 80–89 years | 9.2 (2.2–16.3) (6/65) |
24.3 (16.3–32.3) (27/111) |
9.6 (4.7–14.6) (13/135) |
13.8 (6.9–20.8) (13/94) |
5.0 (1.1–8.9) (6/120) |
12.4 (9.6–15.2) (65/525) |
<0.001 |
| Total (10–89 years) | 2.2 (1.8–2.6) (122/5.584) |
4.9 (4.6–5.2) (843/17.278) |
3.0 (2.6–3.3) (239/8.086) |
2.2 (1.9–2.6) (126/5.615) |
2.7 (2.4–3.0) (243/8.972) |
3.5 (3.3–3.6) (1.573/45.535) |
<0.001 |
95% CI: Confidence interval.
n: Number of patients treated with antidepressants.
N: Number of people in the background population.
P-values below 0.05 (p < 0.05) are in bold.
Figure 3.
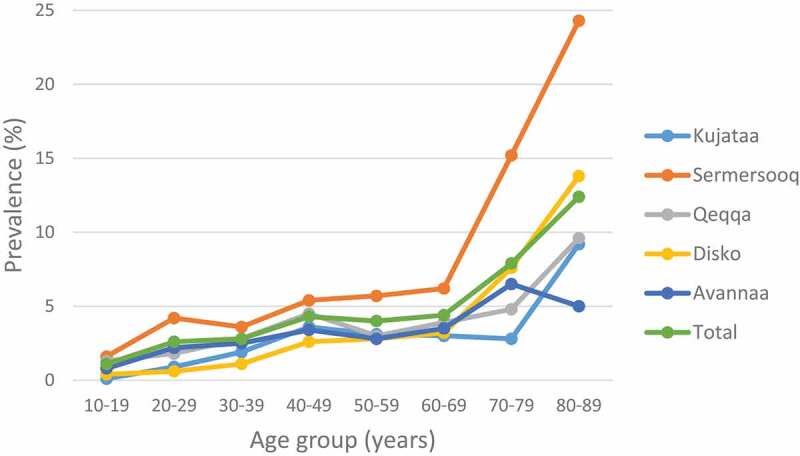
Regional prevalence in Greenland according to age
Prevalence (%) of patients receiving antidepressants in the five regions of Greenland, according to age.
Discussion
The prevalence of patients treated with antidepressants in Greenland was 3.5% and much lower compared to the 8.1% observed in Denmark. The lower prevalence in Greenland compared to Denmark was observed for both genders of all age groups. In both countries, the prevalence was higher among women than for men of all age groups. In Greenland, a regional difference was observed, with the highest prevalence observed in the capital, Nuuk, in region Sermersooq.
Strengths and limitations
A major strength of this study is that the entire population of Denmark and the majority of the population in Greenland was included. Another strength is that the Greenlandic data was extracted from the EMR. Additionally, this was the first study to investigate prevalence of patients receiving antidepressants in Greenland, and to compare it to the prevalence in Denmark.
One of the main limitations of this study is that the reason why a patient has been prescribed antidepressants as well as the duration of the treatment are not included. As mentioned previously, antidepressants are not used exclusively for depression, but also for other disorders. It is thus difficult to know the exact extent of depression. However, a systematic review and network meta-analysis [19] has reported that antidepressants are widely and routinely used in the treatment of major depressive disorders worldwide. Considering duration of the treatment, it is important that treatment is taken continuously to elicit therapeutic effects. It was not possible to investigate potential important clinical modifiers of treatment response at the individual patient level – for example the reason for the treatment, severity of symptoms and duration of treatment. For this reason, the results should be assessed with caution. Notwithstanding these limitations, the findings from this study represent the prevalence of the patients treated with antidepressants during 2019.
Another limitation of the study is the selection of the Greenlandic study population, which included the population (aged 10–89 years) of the 16 previously mentioned towns (Figure 1) with associated settlements and sheep farms, accounting for 81.32% of the totally Greenlandic population. In this study, Tasiilaq, on the East coast, and the associated settlements were not included because of the use of a different journal system. Tasiilaq is known for social hardship, lack of jobs and leisure activities. From this background, the prevalence of patients treated with antidepressants in Greenland can possibly be underestimated. However, since only about 5% of the entire Greenland’s population lives in Tasiilaq, the size of the underestimation is expected to be of less significance. We should however interpret this limitation with caution, because the sample of participants in the included 16 towns may not fully represent the diverse characteristics found in Tasiilaq.
Furthermore, the comparison of the Greenlandic and the Danish population must be made with some reservations, since the patients in Greenland were identified through the medical register as all patients who were prescribed antidepressants, while in Denmark the number of patients was identified through individual purchases of antidepressants. This information may not reflect actual use. Overall, the use of antidepressants is less in Greenland compared to Denmark.
In summary, there is a risk of underestimating the number of patients with depression in both Greenland and Denmark, when carrying out studies based on antidepressants prescriptions. Still, the age- and gender-specific comparison of prevalence of patients treated with antidepressants can provide some valuable information about depression management in Greenland.
Prevalence
Contradictory to a study from 2017 ranking Greenland as the country with the third-highest age-standardised incidence rate of major depression [2], we found the prevalence of patients treated with antidepressants in Greenland to be relatively low. The lower prevalence in Greenland compared to Denmark may reflect some differences in the healthcare systems of Greenland and Denmark, and between the populations in general.
Firstly, awareness of depression and access to healthcare may be the different in the two healthcare systems of Greenland and Denmark. In Denmark, depression care is provided by private practitioners (primary sector). If the depression is severe, patients are referred to a psychiatric ward in a secondary sector – consisting of specialists, often those with a long-term relation to patient. In addition, there is a broad collaboration between various clinics specialising in depression. In contrast, most towns in Greenland are staffed with physicians working only for a short time in Greenland. Thus, obviously, acute conditions will be more of their focus than the long-term managing of chronic conditions and preventive medicine, including screening for undetected depression. In addition, the medical staff might not have received proper training allowing them to recognise the disease. This may partly explain the lower use of antidepressants in Greenland – possibly an under-prioritisation of depression treatment.
Secondly, although depression is a public disease, there is ignorance and many prejudices about depression in the society in Greenland, which can lead to societal stigmatisation. This, in combination with possible cultural differences in the perception of depression, might contribute to underdiagnoses of depression, underestimation of patients in need of antidepressants, and finally a lower use of antidepressants in Greenland.
Thirdly, the observed difference in prevalence of patients treated with antidepressants may partly be explained by a higher prevalence of depression in Denmark compared with Greenland. Several studies have shown that psychiatric disorders are more common among people living in urban cities compared to living in rural areas [20,21]. Such an urban-rural difference in occurrence of depression and other mental disorders might help explain the overall discrepancy in prevalence between Greenland and Denmark, as Greenland might be considered rural overall when compared to Denmark.
Our finding of a higher prevalence of women treated with antidepressants is in line with several studies [19,22,23]. In this study, women constitute more than half of the participants (67.8% in Greenland and 64.0% in Denmark). A similar overrepresentation of women is found in a systematic review and network meta-analysis [19], where 62.3% of the sample population were women. Research has shown that gender and age is linked to depression, so that women are more likely to suffer from depression than men [24], and older people more likely to suffer from depression [25] as a result of more underlying illnesses [26]. Increasing prevalence of patients treated with antidepressants is also found in this study for both genders, except for Greenlandic population aged 50–59 years, where a slight decrease was observed. Meta-analysis of published literature of age and risk for depression among the elderly [27], have found out that older age appears to be an important risk factor for depression in the general population. In accordance, we found the use of antidepressants to increase with age, so that the highest prevalence was seen in among the eldest (age group 80–89 years). One possible explanation may be the increasing incidence of comorbidity among the elderly. In addition, a study [28] highlights the impact of genetic predisposition, as the risk of depression is significantly higher among relatives to depressed people, especially their first-degree relatives, compared to the general population. In Sermersooq, almost 25% of the 80–89 year old patients receive antidepressants. Contributing to such a high prevalence might also be an issue with phasing out medication resulting from the lack of long-term working physicians in Greenland.
The higher prevalence of patients treated with antidepressants in Nuuk indicates a systematic difference in the delivery of healthcare between Nuuk and the remaining 16 towns in Greenland. This may be due to more permanent doctors, e.g. in the psychiatric ward in Nuuk, enabling more focus and longer-term follow-up on patients. This indicates higher attention on depression. Furthermore, depression may also occur more frequently in the big city compared to the rural areas, as supported by studies showing that life in an urban environment is associated with increased risk for mental illness in general and a broad range of psychiatric disorders [20,21]. Further surveys are needed to identify the underlying reason for significantly higher prevalence of patients receiving antidepressants in Nuuk compared to the rest of the country.
In conclusion, we found the prevalence of patients aged 10–89 years treated with antidepressant medicine to be 3.5% in Greenland and 8.1% in Denmark. We furthermore observed both age-, gender- and regional differences in the prevalence of Greenlandic patients treated with antidepressants. The low prevalence in Greenland may be affected by a higher number of undiagnosed patients, as well as differences in awareness of depression and access to healthcare. Based on the presented prevalence of the use of antidepressant medication, we cannot conclude that the depression is a public disease in Greenland, and further attention and research is needed to better understand the reasons for using antidepressant medication in Greenland.
Funding Statement
The authors have not received any funding or benefits from industry or elsewhere to conduct this study.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- [1].Kassebaum NJ, Arora M, Barber RM, Bhutta ZA, Carter A, Casey DC, Charlson FJ, Coates MM, Coggeshall M, Cornaby L, Dandona L. Global, regional, and national disability-adjusted life-years (DALYs) for 315 diseases and injuries and healthy life expectancy (HALE), 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388(10053):1603-1658. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Liu Q, He H, Yang J, et al. Changes in the global burden of depression from 1990 to 2017: findings from the global burden of disease study. J Psychiatr Res. 2019;126:134–140. [DOI] [PubMed] [Google Scholar]
- [3].Smith K. Mental health: a world of depression. Nature. 2014;515(7526):181. [DOI] [PubMed] [Google Scholar]
- [4].Wittchen HU, Jacobi F. Size and burden of mental disorders in Europe–a critical review and appraisal of 27 studies. Eur Neuropsychopharmacol. 2005;15(4):357–9. [DOI] [PubMed] [Google Scholar]
- [5].Malhi GS, Mann JJ. Depression. Lancet. 2018;392(10161):2299–2312. [DOI] [PubMed] [Google Scholar]
- [6].Gilman SE, Sucha E, Kingsbury M, et al. Depression and mortality in a longitudinal study: 19522011. Cmaj. 2017;189(42):E1304–e10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Zhang Y, Chen Y, Ma L. Depression and cardiovascular disease in elderly: current understanding. J Clin Neurosci. 2018;47:1–5. [DOI] [PubMed] [Google Scholar]
- [8].Greenberg PE, Fournier AA, Sisitsky T, et al. The economic burden of adults with major depressive disorder in the USA (2005 and 2010). J Clin Psychiatry. 2015;76(2):155–162. [DOI] [PubMed] [Google Scholar]
- [9].Forns J, Pottegård A, Reinders T, et al. Antidepressant use in Denmark, Germany, Spain, and Sweden between 2009 and 2014: incidence and comorbidities of antidepressant initiators. J Affect Disord. 2019;249:242–252. [DOI] [PubMed] [Google Scholar]
- [10].Sundhedsdatastyrelsen . Laveste antal brugere af antidepressiv medicin de seneste 10 år; 2017. Available from: https://sundhedsdatastyrelsen.dk/da/tal-og-analyser/analyser-og-rapporter/laegemidler/emnespecifikke-analyser/analyser-om–antidepressiva.
- [11].Lynge I, Munk-Jorgensen P, Pedersen AL, et al. Common mental disorders among patients in primary health care in Greenland. Int J Circumpolar Health. 2004;63(Suppl 2):377–383. [DOI] [PubMed] [Google Scholar]
- [12].Curtis T, Larsen FB, Helweg-Larsen K, et al. Violence, sexual abuse and health in Greenland. Int J Circumpolar Health. 2002;61(2):110–122. [DOI] [PubMed] [Google Scholar]
- [13].Sargeant H, Forsyth R, Pitman A. The epidemiology of suicide in young men in Greenland: a systematic review. Int J Environ Res Public Health. 2018;15:11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Bloch LH, Drachmann GH, Pedersen ML. High prevalence of medicine-induced attempted suicides among females in Nuuk, Greenland, 2008-2009. Int J Circumpolar Health. 2013;72:72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Greenland S Population in localities in age-group 10-98 within 10 years interval; 2019. Available from: http://bank.stat.gl/pxweb/da/Greenland/Greenland__BE__BE01__BE0120/BEXST3.PX/table/tableViewLayout1/?rxid=7c28234a-9358-471d-a798-b45d340a6327.
- [16].Pedersen ML. Diabetes care in the dispersed population of Greenland. A new model based on continued monitoring, analysis and adjustment of initiatives taken. Int J Circumpolar Health. 2019;78(sup1):1709257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Statistik D Folketal den 1. i kvartalet efter område, tid, alder og køn; 2019. Available from: https://www.statistikbanken.dk/statbank5a/selectvarval/saveselections.asp.
- [18].Medstat.dk . ATC kode: N06A (Antidepressive midler). Andel af salget i primærsektor, der er personhenførtbart; 2019. Available from: https://medstat.dk/da/viewDataTables/medicineAndMedicalGroups/%7B%22year%22:[%222019%22],%22region%22:[%220%22],%22gender%22:[%221%22,%222%22],%22ageGroup%22:[%22A%22,%22000%22,%22001%22,%22002%22,%22003%22,%22004%22,%22005%22,%22006%22,%22007%22,%22008%22,%22009%22,%22010%22,%22011%22,%22012%22,%22013%22,%22014%22,%22015%22,%22016%22,%22017%22,%22018%22,%22019%22,%22020%22,%22021%22,%22022%22,%22023%22,%22024%22,%22025%22,%22026%22,%22027%22,%22028%22,%22029%22,%22030%22,%22031%22,%22032%22,%22033%22,%22034%22,%22035%22,%22036%22,%22037%22,%22038%22,%22039%22,%22040%22,%22041%22,%22042%22,%22043%22,%22044%22,%22045%22,%22046%22,%22047%22,%22048%22,%22049%22,%22050%22,%22051%22,%22052%22,%22053%22,%22054%22,%22055%22,%22056%22,%22057%22,%22058%22,%22059%22,%22060%22,%22061%22,%22062%22,%22063%22,%22064%22,%22065%22,%22066%22,%22067%22,%22068%22,%22069%22,%22070%22,%22071%22,%22072%22,%22073%22,%22074%22,%22075%22,%22076%22,%22077%22,%22078%22,%22079%22,%22080%22,%22081%22,%22082%22,%22083%22,%22084%22,%22085%22,%22086%22,%22087%22,%22088%22,%22089%22,%22090%22,%22091%22,%22092%22,%22093%22,%22094%22,%2295-%22],%22searchVariable%22:[%22people_count%22],%22errorMessages%22:[],%22atcCode%22:[%22N06A%22],%22sector%22:[%220%22]%7D.
- [19].Cipriani A, Furukawa TA, Salanti G, et al. Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: a systematic review and network meta-analysis. Lancet. 2018;391(10128):1357–1366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Romans S, Cohen M, Forte T. Rates of depression and anxiety in urban and rural Canada. Soc Psychiatry Psychiatr Epidemiol. 2011;46(7):567–575. [DOI] [PubMed] [Google Scholar]
- [21].Vassos E, Agerbo E, Mors O, et al. Urban-rural differences in incidence rates of psychiatric disorders in Denmark. Br J Psychiatry. 2016;208(5):435–440. [DOI] [PubMed] [Google Scholar]
- [22].Noordam R, Aarts N, Verhamme KM, et al. Prescription and indication trends of antidepressant drugs in the Netherlands between 1996 and 2012: a dynamic population-based study. Eur J Clin Pharmacol. 2015;71(3):369–375. [DOI] [PubMed] [Google Scholar]
- [23].Bourne C, Kenkel L. Treatment of depression in women. Handb Exp Pharmacol. 2019;250:371–387. [DOI] [PubMed] [Google Scholar]
- [24].Parker G, Brotchie H. Gender differences in depression. Int Rev Psychiatry. 2010;22(5):429–436. [DOI] [PubMed] [Google Scholar]
- [25].Leng Y, Diem SJ, Stone KL, et al. Cognitive outcomes in very old women. J Gerontol A Biol Sci Med Sci. 2018;73(10):1390–1395. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Faravelli C, Alessandra Scarpato M, Castellini G, et al. Gender differences in depression and anxiety: the role of age. Psychiatry Res. 2013;210(3):1301–1303. [DOI] [PubMed] [Google Scholar]
- [27].Zhao KX, Huang CQ, Xiao Q, et al. Age and risk for depression among the elderly: a meta-analysis of the published literature. CNS Spectr. 2012;17(3):142–154. [DOI] [PubMed] [Google Scholar]
- [28].Mullins N, Lewis CM. Genetics of depression: progress at last. Curr Psychiatry Rep. 2017;19(8):43. [DOI] [PMC free article] [PubMed] [Google Scholar]