

Abstract
Background
Over recent decades, there has been a dramatic transformation in mechanization reaching all aspects of people's lives in Saudi Arabia. In the light of this, there was a significant change in physical behavior in the community. The aim of the current study was to investigate the national and regional distribution of physical activity practice among adults aged ≥15 y across Saudi Arabia.
Methods
Data from the Bulletin of Household Sports Practice National Survey were used to determine the physical activity practice distribution. A total of 26 000 families from 13 administrative regions across Saudi Arabia were surveyed.
Results
The proportion of the total Saudi population who were practitioners of physical activity (i.e. ≥150 min per week) among Saudi adults aged ≥15 y was 17.40%, while the proportion of non-practitioners was 82.60%.
Conclusion
This study found a low level of physical activity among Saudi adults who meet physical activity guidelines. These findings suggest that interventions and promotional programs should be developed to increase physical activity among the Saudi population.
Keywords: physical activity, Saudi Arabia, sedentary behavior, sport
Introduction
The term ‘physical activity’ refers to any bodily movements produced by skeletal muscles that require energy expenditure higher than the basal level.1 Increasing evidence in the literature has indicated the importance of regular engagement in physical activity to an individual's health and well-being.2,3 Also, several governmental reports and consensus statements have further emphasized the essential role of physical activity at both individual and community levels.4–6 Physical inactivity and sedentary behavior, on the other hand, have been identified among the major detrimental factors for a number of chronic non-communicable diseases such as diabetes mellitus, obesity, cardiovascular disorders, certain types of cancer, osteoporosis and mental impairments.7,8 Furthermore, a lack of physical activity has been linked to premature mortality.9 Consequently, surveillance of physical activity practice in countries has increasingly become a public health priority.
Low physical activity is a global phenomenon. The WHO reported reduced physical activity levels and showed that about 27.5% of the global population are insufficiently physically active. Regionally, the average prevalence rate among countries of the Gulf Cooperation Council is 46.24%. Statistics from other countries showed that 40% of the population in the USA, 35.9% in the UK and 29.4% in Europe are physically inactive. The WHO report added that the physical activity level declines with increasing age and that females have lower rates of physical activity than males.10
Until recently, the physical demands of daily living activities might have been enough to maintain a reasonable level of physical fitness in Saudi Arabia. But, over the past few decades, there has been a rapid development in living standards and an increase in the use of largely automatic equipment, which has reached all aspects of the population in Saudi Arabia. With regard to this dramatic transformation in lifestyles, there was a significant change in physical behavior in the community, and that shift towards sedentary lifestyles and low levels of physical activity increased the burden on society by reducing individual productivity and increasing the cost of healthcare.11
Previous studies of physical activity in Saudi Arabia indicated that people are not physically active enough to achieve health benefits from physical activity.12,13 In an observational study including a proportionate sample of 2176 Saudi adults, Amin et al. demonstrated that 80% of the population did not achieve an adequate level of physical activity with beneficial health effects. They also reported an association of chronic disease with physical inactivity.14 A population-based study by Al-Nozha et al. assessed the physical activity profile among Saudi adults and showed that the prevalence of inactivity was very high, accounting for 96.1% of the Saudi population.12 A brief review by Al-Hazzaa suggested that the prevalence of physical inactivity reached as high as 43.3–99.5% among Saudi children and adults, and that the proportion of Saudis who are at risk due to physical inactivity was higher for coronary heart disease than for any other factor.13 Al-Nuaim et al. assessed the prevalence rate of physical activity in relation to obesity among Saudi adolescents. The study revealed a significant correlation between physical activity level and body mass index, and overweight and obese subjects showed a significantly lower level of physical activity compared with those whose weight was normal.15
Although the results of these studies cannot be disregarded, they were limited to samples from certain geographical areas in Saudi Arabia. This sheds light on the importance of this study, which focuses on studying the situation at a regional level to provide more comprehensive results. Additionally, most of the aforementioned studies included specific age groups and gender but none of them paid attention to the educational status of participants. Thus, there is still a need for more studies to provide physical activity data representing the Saudi population by age, gender and educational status.
Despite the health benefits of physical activity having been well established, the level of physical activity did not increase among the Saudi population.12,14,15 Increasing physical activity requires a whole-of-society and culturally relevant approach and therefore demands a collective effort across different sectors and disciplines.
The main purpose of the present study was to estimate the national and regional prevalence rates of physical activity in Saudi Arabia. This study sought to provide an overview of the prevalence rate of physical activity, which will help to guide plans towards increasing population awareness, providing infrastructure to increase exposure to physical activity practice and developing public policy to prevent physical comorbidities, thus reducing the financial burden of chronic health problems.
Materials and methods
The selection process of sample units from the statistical frameworks designed to include the target population was conducted over two steps. In the first step, the primary sampling units were selected. These units were the enumeration areas, as part of the coding and enumeration phase of the buildings and residential real estate units. A total of 1334 enumeration areas were selected from all the administrative regions of Saudi Arabia by using a proportional size method and weighting the total number of Saudi households. In the second step, the final sampling units were randomly drawn from the statistical areas; these units were the households in the enumeration areas that were chosen in the first step through using the regular random sample. Twenty households were chosen from each area, which resulted in a total of 26 000 households across Saudi Arabia, as shown in Figure 1. Trained field researchers from the General Authority for Statistics (GSTAT) interviewed each head of household and recorded all data in an electronic form using an iPad device.
Figure 1.

Flowchart of the survey sample selection.
The term physical activity was defined in this study as any voluntary body movement produced by skeletal muscles resulting in an increase in breathing rate and heart rate, for example, running, brisk walking, cycling, swimming and traditional sports such as football, handball and basketball. The survey was prepared and designed by professionals and experts in the field of physical activity. In developing the survey, international standards and concepts were taken into consideration. The form consists of six sections that addresses matters (in Arabic) such as if the individual currently practices a sports activity at least once a week, the duration of an individual's sporting activity per week (in min), the place where the individual engages in sporting activity, the number of times an individual practices their sport each week, if an individual has ever been involved in a sports activity, the reason(s) for an individual's discontinuation of sporting activity (if applicable) and the reason(s) why an individual does not engage in physical activity (if applicable). All of the analyses were conducted using Microsoft Excel 2016 (Microsoft Corp., Redmond, WA, USA).
Results
A total of 26 000 families from 13 administrative regions across Saudi Arabia were surveyed. The proportion of total Saudi adult males aged ≥15 y who were practitioners of physical activity (i.e. ≥150 min per week) was 17.40%, while the proportion of non-practitioners was 82.60%. Of the total number of Saudi males, the percentage who practiced a physical activity was 28.30% whereas the percentage who did not was 71.70%. Of the total number of Saudi females, the percentage who practiced a physical activity was 8.90% whereas the percentage who did not was 91.10%. With regard to non-Saudis, the overall percentage who practiced a physical activity was 13.88% whereas the percentage who did not was 86.12%. Of these, 16.12% of non-Saudi males practiced a physical activity while 83.88% did not; 8.04% of non-Saudi females practiced a physical activity while 91.96% did not (Figure 2). Details regarding practitioners of physical activity categorized by the type of activity are shown in Table 1. The physical activity practiced most by individuals was walking, which accounted for 56.05%, followed by playing football (25.68%); swimming was the least practiced physical activity (2.34%; Figure 3).
Figure 2.

Percentages of physical activity practice in Saudi Arabia.
Table 1.
Percentage distribution of individuals who practice physical activity by activity type in Saudi Arabia
| Saudi | Non-Saudi | Total | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | Type of physical activity practice | Male | Female | Total | Male | Female | Total | Male | Female | Total |
| 1 | Walking | 25.58 | 14.76 | 40.34 | 12.13 | 3.58 | 15.71 | 37.71 | 18.34 | 56.05 |
| 2 | Swimming | 1.76 | 0.18 | 1.94 | 0.38 | 0.02 | 0.40 | 2.14 | 0.20 | 2.34 |
| 3 | Running | 1.99 | 0.28 | 2.27 | 0.42 | 0.02 | 0.45 | 2.41 | 0.31 | 2.72 |
| 4 | Playing football | 21.92 | 0.09 | 22.00 | 3.68 | 0.01 | 3.68 | 25.59 | 0.09 | 25.69 |
| 5 | Body-building | 4.31 | 0.07 | 4.38 | 1.41 | 0.02 | 1.42 | 5.72 | 0.09 | 5.80 |
| 6 | Other | 4.02 | 1.84 | 5.86 | 2.24 | 0.36 | 2.60 | 6.26 | 2.20 | 8.46 |
Figure 3.
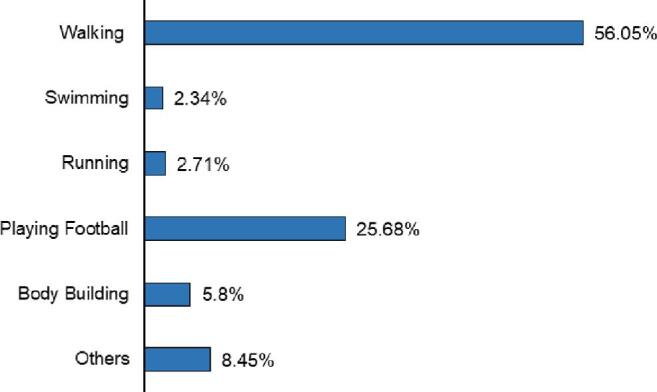
Percentages of individuals who practice physical activity by type of activity in Saudi Arabia.
Details regarding practitioners of physical activity categorized by administrative region are listed in Table 2. The highest rate was in the Mekkah region, where 23.27% of individuals (14.51% Saudis and 8.76% non-Saudis) practiced a physical activity. The lowest rate was in the Al-Baha region, where only 3.05% of Saudis and 0.31% of non-Saudis practiced a physical activity. Details regarding practitioners of physical activity categorized by age group are presented in Table 3. Saudi males in the 15–19 y age group was the highest at 35.86% followed by the 20–24 y age group (34.53%); the age group of ≥65 y was the lowest (10.96%). Saudi females in the 20–24 y age group was the highest at 10.73%, followed by the 25–29 y age group (10.18%); once again, the age group of ≥65 y was the lowest (2.80%).
Table 2.
Percentage distribution of individuals who practice physical activities by administrative region in Saudi Arabia
| Saudi | Non-Saudi | Total | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | Administrative area | Male | Female | Total | Male | Female | Total | Male | Female | Total |
| 1 | Riyadh | 7.36 | 1.93 | 9.29 | 2.69 | 0.70 | 3.38 | 10.04 | 2.63 | 12.67 |
| 2 | Mekkah | 10.55 | 3.96 | 14.51 | 7.17 | 1.59 | 8.76 | 17.72 | 5.54 | 23.27 |
| 3 | Madinah | 4.15 | 1.14 | 5.29 | 0.95 | 0.14 | 1.09 | 5.10 | 1.28 | 6.38 |
| 4 | Qassim | 2.30 | 1.08 | 3.38 | 1.23 | 0.11 | 1.34 | 3.53 | 1.19 | 4.72 |
| 5 | Eastern region | 7.57 | 2.47 | 10.04 | 2.65 | 0.38 | 3.04 | 10.22 | 2.86 | 13.08 |
| 6 | Asir | 3.79 | 1.43 | 5.21 | 0.94 | 0.15 | 1.09 | 4.73 | 1.58 | 6.31 |
| 7 | Tabuk | 3.69 | 0.74 | 4.43 | 0.37 | 0.08 | 0.45 | 4.06 | 0.82 | 4.88 |
| 8 | Hail | 3.72 | 0.75 | 4.47 | 1.10 | 0.08 | 1.18 | 4.82 | 0.82 | 5.65 |
| 9 | Northern borders | 2.91 | 0.93 | 3.84 | 0.67 | 0.21 | 0.88 | 3.58 | 1.14 | 4.72 |
| 10 | Jazan | 3.87 | 0.53 | 4.40 | 0.56 | 0.10 | 0.66 | 4.43 | 0.63 | 5.06 |
| 11 | Najran | 3.18 | 0.86 | 4.04 | 1.28 | 0.27 | 1.55 | 4.46 | 1.13 | 5.59 |
| 12 | Al-Baha | 2.49 | 0.56 | 3.05 | 0.28 | 0.03 | 0.31 | 2.77 | 0.59 | 3.36 |
| 13 | Al-Jouf | 2.68 | 0.55 | 3.23 | 0.94 | 0.14 | 1.08 | 3.62 | 0.69 | 4.31 |
Table 3.
Percentage distribution of individuals who practice physical activities by age group in Saudi Arabia
| Saudi | Non-Saudi | Total | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | Age groups, y | Male | Female | Total | Male | Female | Total | Male | Female | Total |
| 1 | 15–19 | 12.77 | 2.29 | 15.05 | 2.63 | 0.39 | 3.02 | 15.40 | 2.68 | 18.08 |
| 2 | 20–24 | 11.62 | 3.20 | 14.82 | 2.19 | 0.60 | 2.79 | 13.81 | 3.79 | 17.61 |
| 3 | 25–29 | 9.06 | 2.80 | 11.87 | 3.36 | 0.60 | 3.96 | 12.42 | 3.40 | 15.82 |
| 4 | 30–34 | 6.86 | 2.16 | 9.02 | 3.24 | 0.75 | 4.00 | 10.10 | 2.91 | 13.01 |
| 5 | 35–39 | 5.00 | 2.02 | 7.02 | 2.83 | 0.60 | 3.42 | 7.83 | 2.62 | 10.44 |
| 6 | 40–44 | 3.29 | 1.35 | 4.64 | 2.19 | 0.35 | 2.54 | 5.48 | 1.70 | 7.19 |
| 7 | 45–49 | 2.61 | 1.09 | 3.70 | 1.70 | 0.24 | 1.93 | 4.30 | 1.33 | 5.63 |
| 8 | 50–54 | 2.28 | 0.77 | 3.05 | 1.15 | 0.27 | 1.43 | 3.43 | 1.04 | 4.48 |
| 9 | 55–59 | 1.68 | 0.70 | 2.38 | 0.84 | 0.10 | 0.94 | 2.52 | 0.80 | 3.32 |
| 10 | 60–64 | 1.62 | 0.27 | 1.89 | 0.42 | 0.05 | 0.47 | 2.03 | 0.33 | 2.36 |
| 11 | ≥65 | 1.48 | 0.27 | 1.75 | 0.28 | 0.02 | 0.31 | 1.77 | 0.29 | 2.06 |
Non-Saudi males aged 15–19 y had the highest engagement in physical activities (38.33%) followed by the 20–24 y age group (20.14%); the 40–44 y age group had the lowest engagement (12.99%). Non-Saudi females aged 20–24 y had the highest engagement in physical activities (10.60%) followed by the 50–54 y age group (10.48%); the age group of ≥65 y had the lowest engagement (2.73%).
Details regarding practitioners of physical activity categorized by educational status are shown in Table 4. For Saudi males, the group with an educational status of secondary or equivalent was the highest at 23.23%, followed by the graduate group (13.94%), while the high diploma group was the lowest (0.06%). Saudi females in the graduate group engaged in a physical activity was the highest (6.24%), followed by the secondary or equivalent group (5.14%); the PhD group was the lowest (0.06%). Regarding non-Saudis males, the secondary or equivalent group was the highest (5.58%), followed by the intermediate education group (4.91%); the high diploma group was the lowest (0.11%). For non-Saudi females, the secondary or equivalent group engaged in physical activities was the highest (1.15%), followed by the graduate group (1.03%); the high diploma group was the lowest (0.02%).
Table 4.
Percentage distribution of individuals who practice physical activity by educational status in Saudi Arabia
| Saudi | Non-Saudi | Total | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Educational status | Male | Female | Total | Male | Female | Total | Male | Female | Total | |
| 1 | Illiterate | 0.24 | 0.40 | 0.64 | 0.24 | 0.09 | 0.34 | 0.49 | 0.49 | 0.98 |
| 2 | Literate | 0.93 | 0.95 | 1.88 | 2.05 | 0.38 | 2.43 | 2.98 | 1.34 | 4.31 |
| 3 | Primary education | 3.69 | 0.95 | 4.64 | 2.08 | 0.26 | 2.34 | 5.77 | 1.21 | 6.98 |
| 4 | Intermediate education | 10.69 | 2.28 | 12.97 | 4.91 | 0.61 | 5.52 | 15.60 | 2.89 | 18.49 |
| 5 | Secondary or equivalent | 23.23 | 5.14 | 28.37 | 5.58 | 1.15 | 6.74 | 28.81 | 6.30 | 35.11 |
| 6 | Under-university diploma | 4.64 | 0.69 | 5.33 | 1.56 | 0.27 | 1.84 | 6.20 | 0.97 | 7.17 |
| 7 | Graduate | 13.94 | 6.24 | 20.18 | 3.83 | 1.03 | 4.86 | 17.77 | 7.27 | 25.04 |
| 8 | High diploma | 0.06 | 0.03 | 0.09 | 0.11 | 0.02 | 0.13 | 0.17 | 0.05 | 0.23 |
| 9 | Master's degree | 0.63 | 0.16 | 0.79 | 0.27 | 0.09 | 0.35 | 0.90 | 0.25 | 1.15 |
| 10 | PhD degree | 0.22 | 0.06 | 0.28 | 0.20 | 0.06 | 0.26 | 0.42 | 0.13 | 0.54 |
The reasons why individuals do not practice physical activity are listed in Table 5. For Saudis, the most common reason for not practicing physical activity was lack of desire (33.50%). Other reasons included an absence of adapted facilities in the neighborhood (11.72%), lack of time (10.10%) and injury or disability (9.81%). The percentage of Saudi individuals who do not practice physical activity due to other reasons was 1.09%. For non-Saudis, lack of time was the most common reason for not practicing physical activity (19.65%) followed by lack of desire (11.23%), lack of facilities in the district (1.33%) and injury or impairment (1.01%). The percentage of non-Saudis who do not practice physical activity due to other reasons was 1.64%.
Table 5.
Reasons for not practicing physical activity for individuals in Saudi Arabia
| Saudi | Non-Saudi | Total | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | Reasons for not practicing physical activity | Male | Female | Total | Male | Female | Total | Male | Female | Total |
| 1 | Unwillingness to practice physical activity | 10.95 | 22.55 | 33.50 | 5.95 | 5.28 | 11.23 | 16.90 | 27.83 | 44.73 |
| 2 | Lack of enough time | 3.76 | 6.33 | 10.10 | 15.56 | 4.09 | 19.65 | 19.32 | 10.42 | 29.74 |
| 3 | Lack of enough facilities in the district | 2.08 | 9.65 | 11.72 | 0.36 | 0.97 | 1.33 | 2.43 | 10.62 | 13.06 |
| 4 | Injury or impairment | 4.62 | 5.19 | 9.81 | 0.59 | 0.42 | 1.01 | 5.21 | 5.61 | 10.83 |
| 5 | Other | 0.28 | 0.81 | 1.09 | 0.29 | 0.26 | 0.55 | 0.57 | 1.07 | 1.64 |
Discussion
The purpose of this study was to describe the prevalence of physical activity among adults in Saudi Arabia using a representative national survey. The study found that the prevalence of physical activity was 17.40% among Saudi adults, which was below that in some populations in Europe and the USA. Previous research showed that the prevalence of moderate to vigorous physical activity in Portuguese adults was 30% and 27%, respectively, which is almost double the prevalence of physical activity in the Saudi population.16 Another report from the USA found that 48% of adults were meeting physical activity guidelines (i.e. performing at least 150 min per week of moderate to vigorous activity).17 The low prevalence of physical activity in Saudi Arabia is still below Asian countries such as China and Nibal. In China, the prevalence of physical activity in rural and urban areas was 78.1% and 21.8%, respectively, which is higher than for Saudi adults.18 In Nibal, the prevalence of physical activity was very high, exceeding 95% of the general population.19 This huge difference in physical activity level in Saudi Arabia compared with other countries requires further investigation to identify the reasons for the low physical activity level.
The prevalence of physical activity among Saudi adult males (28.30%) compared with females (8.90%) indicated a significant difference. One reason behind this disparity could be the non-availability of specialized gyms for females. Also, the practicing of sporting and other physical activities may be restricted because of cultural reasons pertaining to modest clothing for females in Saudi Arabia. The low level of physical activity was highlighted in the study by Al-Eisa and Al-Sobayel,20 which investigated the level of physical activity in 161 Saudi women. The reasons underlying the low level of physical activity in Saudi females merits further qualitative research. Although the difference between males and females involved in physical activity has conflicting findings in previous reports, its magnitude is substantial in the Saudi population. For example, a previous report showed that physical activity level was 68% in males compared with 60% in females in the USA. Furthermore, males showed a higher physical activity level (69.6%) compared with females (63.2%) in China. However, between males and females, our study population showed a greater than threefold difference in meeting physical activity guidelines compared with the aforementioned studies. Unlike our study, previous evidence showed that females had a higher physical activity level (62.1%) compared with males (60.7%) in Europe.21 These differences between males and females and between studies could be attributed to the perception of the importance of physical activity for health reasons, prioritizing of physical activity, barriers to physical activity, as well as to the intensity of different types of physical activity. Finally, the season and weather could be important barriers to physical activity in Saudi Arabia that should be addressed in future research.22,23
Physical activity level decreased with increasing age in our study, which is consistent with previous research. Aging has a biological basis with a decline in physical activity.24 This could be attributed to physiological changes in different systems and organs due to cellular function decline.25–27 In addition, comorbidities such as arthritis and diabetes have a strong link to aging and a declining physical activity level.28–30 Therefore, it is important for future researchers and policymakers to identify the barriers to older adults engaging in physical activities.
Of the participants, >50% regularly participate in physical activity with the goal of either enhancing health or improving their general fitness; this suggests that more than half the sample are aware of the importance of physical activity. This finding suggests that people aware of the associated health benefits of physical activity might be more active. This is consistent with the health belief model,31 which highlighted that the more individuals know about the health benefits of being active then the more probable it is that they adhere to a physical exercise regime. The value of knowledge and awareness about the health-related benefits of exercise was reported in different countries and this should be reflected in any physical activity promotional campaigns seeking to emphasize the health value of physical activity.32,33
The lack of a physical activity environment as an external barrier to participation in physical activity (e.g. the gym, walking trails) was indisputable with regard to females. This may be due to a limited number of specialized female-focused gyms, which nowadays are increasing in number. However, female participants’ responses also demonstrated a notable perceived unwillingness to participate in physical activity, which suggests that factors other than the physical activity environment are impacting upon their participation in physical activity; in which case, increasing the number of specialized female gyms might not help raise overall public activity levels. In a cross-sectional study of Chinese women (n = 360) about barriers to participation in physical activity,34 one of the main internal barriers was the lack of support from family and friends. Consistently, Iranian women reported a similar barrier, stating that they would rather spend time with their family members than participating in physical activity,35 which suggests that a family-friendly physical activity environment would be important for the community. Other factors consistently reported from different countries included a lack of energy for physical activity and insufficient annual income.34–36 Notably, it is important to study the Saudi population barrier, especially for women, before implementing any action plan.
Aerobic exercise (e.g. walking and swimming) was the predominant means of practicing physical activity in Saudi Arabia. These forms of exercise have proven to be a cost-effective method for preventing multiple medical and psychological illnesses.37,38 With the Saudi population aging,39,40 it is important to implement community-based projects that aim to enhance adherence to physical activity, specifically aerobic exercise. Urban design and transportation have been found to contribute to community engagement in physical activity.41,42 Moreover, the availability and accessibility of walking trails were associated with better adherence to physical activity.42,43 Therefore, there is a need to evaluate the number of walking trails and their accessibility to non-disabled and disabled individuals in Saudi Arabia.
This study has some limitations that need to be considered. A cross-sectional design is one of the limitations as it cannot determine causality. Another limitation is using self-reported outcome measures for the key variable (physical activity) as this is subject to recall and social desirability biases. Further, self-reported measures could cause over-reporting of physical activity level and this must be considered when interpreting the results of our study. The validity and reliability of using this questionnaire is another limitation, which must be considered in future research. Studies are needed to further examine the possible risk factors associated with physical inactivity in Saudi Arabia. Finally, using objective measures such as accelerometers are needed to accurately assess the prevalence of physical activity.
Conclusion
This study found a low physical activity level among Saudi adults meeting physical activity guidelines (17.40%). Males had a threefold higher physical activity level than females. Among the types of physical activity, walking was the most common type of activity in this population, which more than half of participants practiced. Physical activity level decreased with increasing age in Saudi adults and this trend was consistent in both genders.
Acknowledgements
The authors would like to thank the Prince Sattam bin Abdulaziz University for their support throughout this project.
Contributor Information
Bader A Alqahtani, Department of Health and Rehabilitation Sciences, Prince Sattam Bin Abdulaziz University, Alkharj, Saudi Arabia.
Aqeel M Alenazi, Department of Health and Rehabilitation Sciences, Prince Sattam Bin Abdulaziz University, Alkharj, Saudi Arabia.
Ahmed S Alhowimel, Department of Health and Rehabilitation Sciences, Prince Sattam Bin Abdulaziz University, Alkharj, Saudi Arabia.
Ragab K Elnaggar, Department of Health and Rehabilitation Sciences, Prince Sattam Bin Abdulaziz University, Alkharj, Saudi Arabia; Department of Physical Therapy for Pediatrics, Faculty of Physical Therapy, Cairo University, Giza, Egypt.
Authors’ contributions
BA conceived and designed the study. BA, and RE helped with data interpretation. BA, AMA, ASA, RE draft writing, read and approved the final version of the manuscript.
Funding
Prince Sattam bin Abdulaziz University (# 2019/03/10805).
Competing interests
None declared.
Ethical approval
Not required.
References
- 1. Caspersen CJ, Powell KE, Christenson GM. Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public Health Rep. 100(2):126–31. [PMC free article] [PubMed] [Google Scholar]
- 2. Das P, Horton R. Physical activity—time to take it seriously and regularly. Lancet. 2016;388(10051):1254–55. [DOI] [PubMed] [Google Scholar]
- 3. Hills AP, Street SJ, Byrne NM. Physical activity and health: ``what is old is new again''. Adv Food Nutr Res. 2015;75:77–95. [DOI] [PubMed] [Google Scholar]
- 4. Haskell WL, Lee IM, Pate RRet al. Physical activity and public health: updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Circulation. 2007;116(9):1081–93. [DOI] [PubMed] [Google Scholar]
- 5. Physical activity and cardiovascular health: NIH consensus development panel on physical activity and cardiovascular health . JAMA. 1996;276(3):241–6. [PubMed] [Google Scholar]
- 6. Downs AM. Physical activity and cardiovascular health: a national consensus. Cardiopulm Phys Ther J. 1999;10(4):157. [Google Scholar]
- 7. Carter MI, Hinton PS. Physical activity and bone health. Mo Med. 2014;111(1):59–64. [PMC free article] [PubMed] [Google Scholar]
- 8. World Cancer Research Fund/American Institute for Cancer Research . Physical activity and the risk of cancer. Continous Updat Proj. 2018;(18):12–4. [Google Scholar]
- 9. Mok A, Khaw KT, Luben Ret al. Physical activity trajectories and mortality: population based cohort study. BMJ. 2019;365:l2323. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. World Health Organization (WHO) . Prevalence of insufficient physical activity among adults Data by WHO region 2016. Available from https://apps.who.int/gho/data/view.main.2482?lang=en [accessed February 17 2020]. [Google Scholar]
- 11. Al-Hazzaa HM. The public health burden of physical inactivity in saudi arabia. J Family Community Med. 2004;11(2):45–51. [PMC free article] [PubMed] [Google Scholar]
- 12. Al-Nozha MM, Al-Hazzaa HM, Arafah MRet al. Prevalence of physical activity and inactivity among Saudis aged 30–70 years. Saudi Med J. 2007;28(4):559–68. [PubMed] [Google Scholar]
- 13. Al-Hazzaa HM. Prevalence of physical inactivity in Saudi Arabia: a brief review. East Mediterr Health J. 2004;10(4-5):663–70. [PubMed] [Google Scholar]
- 14. Amin TT, Khoudair AS Al, Harbi MA Alet al. Leisure time physical activity in Saudi Arabia: prevalence, pattern and determining factors. Asian Pacific J Cancer Prev. 2012;13(1):351–60. [DOI] [PubMed] [Google Scholar]
- 15. Al-Nuaim AA, Al-Nakeeb Y, Lyons Met al. The prevalence of physical activity and sedentary behaviours relative to obesity among adolescents from Al-ahsa, Saudi Arabia: Rural versus urban variations. J Nutr Metab. 2012;2012:417589. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Teixeira PJ, Marques A, Lopes Cet al. Prevalence and preferences of self-reported physical activity and nonsedentary behaviors in Portuguese adults. J Phys Act Health. 2019;16(4):251–8. [DOI] [PubMed] [Google Scholar]
- 17. Prevalence of self-reported physically active adults-United States, 2007 . MMWR morbidity and mortality weekly report. Available from https://www.cdc.gov/mmwr/preview/mmwrhtml/mm5748a1.htm [accessed January 26 2020]. [PubMed] [Google Scholar]
- 18. Muntner P, Gu D, Wildman RPet al. Prevalence of physical activity among Chinese adults: results from the International Collaborative Study of Cardiovascular Disease in Asia. Am J Public Health. 2005;95(9):1631–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Pedisic Z, Shrestha N, Loprinzi PDet al. Prevalence, patterns, and correlates of physical activity in Nepal: Findings from a nationally representative study using the Global Physical Activity Questionnaire (GPAQ). BMC Public Health. 2019;19(1):864. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Al-Eisa ES, Al-Sobayel HI.. Physical activity and health beliefs among Saudi women. J Nutr Metab. 2012;2012:642187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Marques A, Sarmento H, Martins Jet al. Prevalence of physical activity in European adults - compliance with the World Health Organization's physical activity guidelines. Prev Med. 2015;81:333–38. [DOI] [PubMed] [Google Scholar]
- 22. Chan CB, Ryan DA.. Assessing the effects of weather conditions on physical activity participation using objective measures. Int J Environ Res Public Health. 2009;6(10):2639–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Aspvik NP, Viken H, Ingebrigtsen JEet al. Do weather changes influence physical activity level among older adults? The Generation 100 study. PLoS One. 2018;13(7):e0199463. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Ingram DK. Age-related decline in physical activity: Generalization to nonhumans. Med Sci Sports Exerc. 2000;32(9):1623–9. [DOI] [PubMed] [Google Scholar]
- 25. Harman D. Aging: a theory based on free radical and radiation chemistry. J Gerontol. 1956;11(3):298–300. [DOI] [PubMed] [Google Scholar]
- 26. Harman D. The biologic clock: the mitochondria? J Am Geriatr Soc. 1972;20(4):145–7. [DOI] [PubMed] [Google Scholar]
- 27. Trounce I, Byrne E, Marzuki S. Decline in skeletal muscle mitochondrial respiratory chain function: possible factor in ageing. Lancet. 1989;333(8639):637–39. [DOI] [PubMed] [Google Scholar]
- 28. Cnop M, Igoillo-Esteve M, Hughes SJet al. Longevity of human islet α- and β-cells. Diabetes Obes Metab. 2011;13(suppl 1):39–46. [DOI] [PubMed] [Google Scholar]
- 29. Berenbaum F. Republished viewpoint: Diabetes-induced osteoarthritis: From a new paradigm to a new phenotype. Postgrad Med J. 2011;88(1038):240–2. [DOI] [PubMed] [Google Scholar]
- 30. Prieto-Alhambra D, Judge A, Javaid MKet al. Incidence and risk factors for clinically diagnosed knee, hip and hand osteoarthritis: Influences of age, gender and osteoarthritis affecting other joints. Ann Rheum Dis. 2014;73(9):1659–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Rosenstock IM. The health belief model and preventive health behavior. Health Educ Monogr. 1974;2(4):354–86. [DOI] [PubMed] [Google Scholar]
- 32. Fredriksson SV, Alley SJ, Rebar ALet al. How are different levels of knowledge about physical activity associated with physical activity behaviour in Australian adults? PLoS One. 2018;13(11):e0207003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Veluswamy SK, Maiya AG, Nair Set al. Awareness of chronic disease related health benefits of physical activity among residents of a rural South Indian region: a cross-sectional study. Int J Behav Nutr Phys Act. 2014;11(1):27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Sit CHP, Kerr JH, Wong ITF. Motives for and barriers to physical activity participation in middle-aged Chinese women. Psychol Sport Exerc. 2008;9(3):266–83. [Google Scholar]
- 35. Dashti S, Joseph HL, Esfehani AJet al. Perceived barriers to physical activity among Iranian women. World Appl Sci J. 2014;32(3):422–8. [Google Scholar]
- 36. Osuji T, Lovegreen S, Elliott M, Brownson RC. Barriers to physical activity among women in the rural Midwest. Women Health. 2006;44(1):41–55. [DOI] [PubMed] [Google Scholar]
- 37. Gaziano TA, Galea G, Reddy KS. Scaling up interventions for chronic disease prevention: the evidence. Lancet. 2007;370(9603):1939–46 [DOI] [PubMed] [Google Scholar]
- 38. Chodzko-Zajko WJ, Proctor DN, Fiatarone Singh MAet al. Exercise and physical activity for older adults. Med Sci Sport Exerc. 2009;41(7):1510–30. [DOI] [PubMed] [Google Scholar]
- 39. Karlin NJ, Weil J, Felmban W. Aging in Saudi Arabia: an exploratory study of contemporary older persons’ views about daily life, health, and the experience of aging. Gerontol Geriatr Med. 2016;2:2333721415623911. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Alqahtani BA, Alshehri MM, Hoover JCet al. Prevalence of falls among older adults in the Gulf Cooperation Council countries: a systematic review and meta-analysis. Arch Gerontol Geriatr. 2019;83:169–74. [DOI] [PubMed] [Google Scholar]
- 41. Saelens BE, Sallis JF, Frank LD. Environmental correlates of walking and cycling: Findings from the transportation, urban design, and planning literatures. Ann Behav Med. 2003;25(2):80–91. [DOI] [PubMed] [Google Scholar]
- 42. Brownson RC, Baker EA, Housemann RAet al. Environmental and policy determinants of physical activity in the United States. Am J Public Health. 2001;91(12):1995–2003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Brownson RC, Housemann RA, Brown DRet al. Promoting physical activity in rural communities. Am J Prev Med. 2000;18(3):235–41. [DOI] [PubMed] [Google Scholar]