

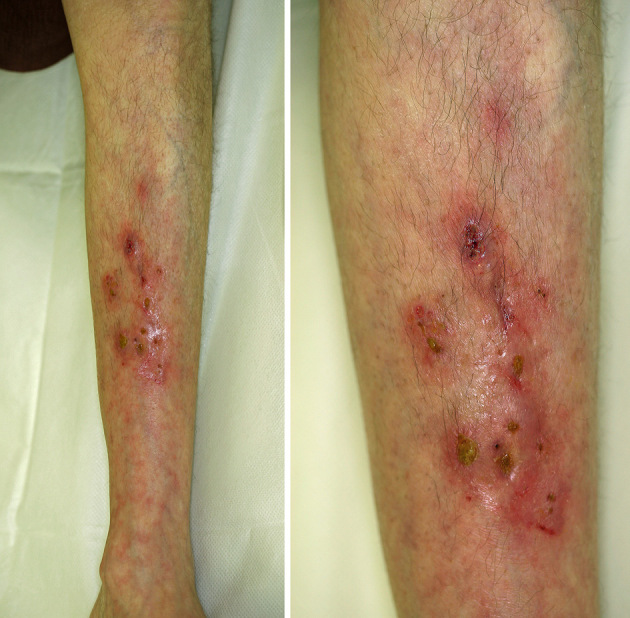
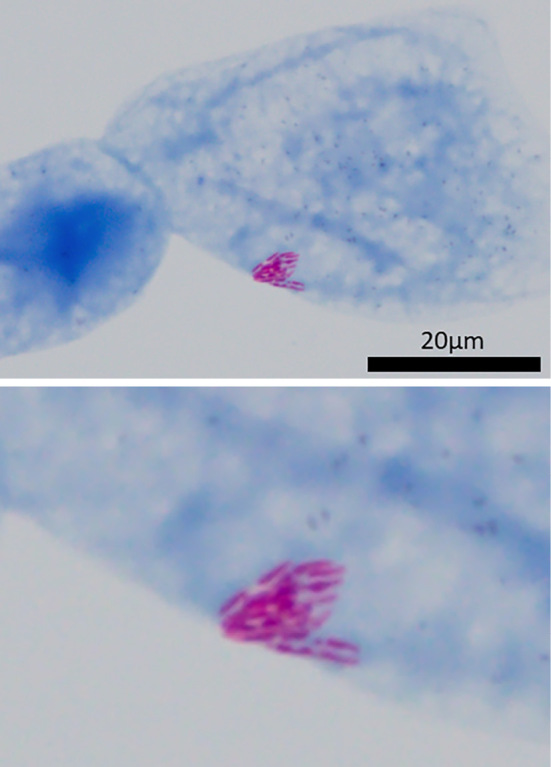
A 55-year-old woman presented with a 3-month history of progressively worsening, intractable, ulcerated papules on her left lower leg (Picture 1). She had a history of rheumatoid arthritis and was treated with 4 mg/day of prednisolone, 8 mg/week of methotrexate, and 4 mg/day of baricitinib (Janus kinase inhibitor) for 1 year. Bacterial culture revealed no bacterial growth. However, acid-fast staining of the purulent discharge demonstrated acid-fast bacilli (Picture 2). Eventually, Mycobacteroides chelonae was identified from pus and biopsied tissues. The patient was treated with oral clarithromycin and sitafloxacin for three months with improvement. M. chelonae is a rapidly growing mycobacterium belonging to the Runyon classification group IV and is a causative bacteria associated with intractable skin lesions (1). Acid-fast staining and mycobacterial culture are important for the diagnosis. M. chelonae infection should be considered in cases of long-term intractable skin lesions, such as in this patient with immunodeficiency (2).
Picture 1.
Picture 2.
The authors state that they have no Conflict of Interest (COI).
Acknowledgement
We thank Dr. Atsushi Yoshida at the Department of Infectious Diseases, Tokyo Women's Medical University, Tokyo, Japan for the culture and drug-susceptibility testing of M. chelonae.
References
- 1. Griffith DE, Aksamit T, Brown-Elliott BA, et al. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med 175: 367-416, 2007. [DOI] [PubMed] [Google Scholar]
- 2. Uslan DZ, Kowalski TJ, Wengenack NL, Virk A, Wilson JW. Skin and soft tissue infections due to rapidly growing mycobacteria: comparison of clinical features, treatment, and susceptibility. Arch Dermatol 142: 1287-1292, 2006. [DOI] [PubMed] [Google Scholar]