

Abstract
Our objective was to inform state and community interventions focused on increasing household preparedness by examining the association between self-reported possession of household disaster preparedness items (ie, a 3-day supply of food and water, a written evacuation plan, and a working radio and flashlight) and perceptions of household preparedness on a 3-point scale from “well prepared” to “not at all prepared.” Data were analyzed from 14 states participating in a large state-based telephone survey: the 2006–2010 Behavioral Risk Factor Surveillance System (BRFSS) (n = 104,654). Only 25.3% of the population felt they were well prepared, and only 12.3% had all 5 of the recommended items. Fewer than half the households surveyed had 4 or more of the recommended preparedness items (34.1%). Respondents were more likely to report their households were well prepared as the number of preparedness items possessed by their household increased. Risk factors for having no preparedness items were: younger age, being female, lower levels of education, and requesting the survey to be conducted in Spanish. To increase household disaster preparedness, more community-based preparedness education campaigns targeting vulnerable populations, such as those with limited English abilities and lower reading levels, are needed.
Vulnerable households are more likely to experience negative consequences in disasters.1–6 Vulnerability is defined as an inability to cope with and recover from the impact of disasters due to physical, psychological, social, or economic susceptibility.3,7–9 Socioeconomic differences, such as low income, little education, and language barriers, as well as preferences for sources of preparedness information (eg, in-person communication rather than internet searches) have been noted as significant risk factors that contribute to increased vulnerability in certain populations during and after disasters.6–11 When individuals adopt the protective behaviors associated with preparing for disasters, they increase their ability to be self-sufficient and decrease their vulnerability to adverse conditions for the duration of the disaster.10,12,13
Communities that are affected by disasters often experience a disruption of essential services such as public health, medical, and transportation.3–5 Frequently, due to the disruption of these services, people are required to be self-sufficient for at least 3 days after the initial impact of a disaster.6,10 Individual or household preparedness measures—including having a 3-day supply of food and water, a battery-powered radio, and a flashlight and having a household emergency plan—are behaviors that are thought to improve an affected population’s ability to cope with the disruption of services and mitigate the number of people who might overwhelm emergency and healthcare systems.6,10,13–16 People who are prepared decrease the burden on the emergency response system, allowing first responders and medical professionals to provide services to the more vulnerable and less resilient populations,6 thus adding to the overall resilience of communities.6,17
Individual or household preparedness behaviors are thought to be influenced by many factors, such as prior disaster experience and risk perception, economic and demographic characteristics, social cohesion, and health conditions, although results have not been consistent across studies.6,10,18–20 For example, some preparedness behaviors have been found to increase in certain populations after they experience disasters21,22 but not in others.21,23,24 In some studies, Hispanic people have been found to be more prepared than non-Hispanic people,25 while other studies have found them to be less prepared.19,20 Potential causes of the study variations could be the use of different metrics to assess preparedness behaviors, the different types of disasters experienced, and the different populations affected.6,10,16 Conversely, other characteristics, such as age, sex, race, income, and education, tend to consistently emerge as predictors of individual or household preparedness.2,6,19,20,22,25–27 Un-fortunately, current information on the predictors of individual preparedness behaviors is limited and centers mostly on basic demographics and risk perception.6,8,10,16,28,29
While easily conflated, preparedness perception is different from risk perception.10,20,22,24,30 Risk perception refers to an individual’s evaluation of his or her vulnerability to a risk,31 whereas preparedness perception refers to an individual’s judgment about his or her readiness to withstand or respond to a potential risk.10,20,22 In general, the study of risk perception explores a range of constructs from cognitive to affective, their relationship between demographic and social characteristics, and behavior associated with various risks.32–34 Preparedness perception often focuses on an appraisal of one’s resources in relation to one’s susceptibility to a risk.6,10,22,24,35
To help inform state and community interventions focused on increasing household preparedness, we estimated recent household preparedness levels of 5 preparedness items—3-day supply of food and water, written evacuation plan, and a working radio and flashlight—and examined the association between the self-reported household possession of preparedness items, the individual’s preparedness perception on a 3-point scale from “well prepared” to “not at all prepared,” and sociodemographic characteristics using data collected from select states from 2006 to 2010 in the Behavioral Risk Factor Surveillance Survey (BRFSS) (available at http://www.cdc.gov/brfss/annual_data/annual_data.htm).
Methods
The BRFSS is a state-based surveillance system, operated by state health departments in collaboration with the Centers for Disease Control and Prevention (CDC). The objective of the BRFSS is to collect uniform, state-specific data on preventive health practices and risk behaviors that are linked to chronic diseases, injuries, and preventable infectious diseases in the adult population.36 Trained interviewers collect data from a standardized questionnaire on a monthly basis using an independent probability sample of households with landline telephones in the noninstitutionalized US adult population. Potential study participants are informed prior to the interview that the survey is being conducted by the health department, with the purpose of the study being to “gather information about the health of the state’s residents.” The BRFSS questionnaire consists of 3 parts: (1) core questions asked in all 50 states, the District of Columbia, Puerto Rico, Guam, and the US Virgin Islands; (2) supplemental modules, which are a series of questions on specific topics (eg, adult asthma history, intimate partner violence, mental health) that a state can choose to include in their survey; and (3) questions added by the states individually. All BRFSS questionnaires, data, and reports are available at http://www.cdc.gov/brfss/.
General Preparedness Module Questions
The General Preparedness module was included in the BRFSS in select states from 2006 to 2010. Preparedness data were available for Connecticut, Montana, Nevada, and Tennessee in 2006; Delaware, Louisiana, Maryland, Nebraska, and New Hampshire in 2007; Georgia, Montana, Nebraska, New York, and Pennsylvania in 2008; Mississippi in 2009; and Montana and North Carolina in 2010 (n = 104,654). The General Preparedness module begins by stating to respondents:
The next series of questions asks about how prepared you are for a large-scale disaster or emergency. By large-scale disaster or emergency, we mean any event that leaves you isolated in your home or displaces you from your home for at least 3 days. This might include natural disasters such as hurricanes, tornados, floods, and ice storms, or man-made disasters such as explosions, terrorist events, or blackouts.
To assess the presence of preparedness items in the household, respondents were asked the following 5 questions:
“Does your household have a 3-day supply of nonperishable food for everyone who lives there? By nonperishable we mean food that does not require refrigeration or cooking.”
“Does your household have a 3-day supply of water for everyone who lives there? A 3-day supply of water is 1 gallon of water per person per day.”
“Does your household have a written evacuation plan for how you will leave your home in case of a large-scale disaster or emergency that requires evacuation?”
“Does your household have a working battery-operated radio and working batteries for use if the electricity is out?”
“Does your household have a working flashlight and working batteries for use if the electricity is out?”
Perceived household preparedness was assessed by asking the respondent, “How well prepared do you feel your household is to handle a large-scale disaster or emergency? Would you say, well prepared, somewhat prepared, not prepared at all?”
Statistical Analysis
We first examined individual items, total number of items, and perceived level of preparedness by selected sociodemographic characteristics. Then we conducted logistic regression analysis to examine the relationship between perception of household preparedness and each of the individual household preparedness items. Finally, we examined perception of preparedness by total number of items possessed.
Sociodemographic characteristics of interest included age in years (18–24, 25–44, 45–54, 55+), gender, race/ethnicity (white non-Hispanic [W-NH], black non-Hispanic [B-NH], Hispanic, other non-Hispanic [O-NH]), education (less than high school, high school graduate, some college, college or more), and language used to conduct the survey (English, Spanish). All analyses were weighted to account for the complex survey design, resulting in weighted percentages, confidence intervals, and adjusted odds ratios (AOR). Significance was assessed using an alpha level of 0.05. All analyses were conducted using SAS-callable SUDAAN (Research Triangle, release 9.2, Research Triangle Park, NC; 2008).
Results
Study Characteristics
Among the 104,654 (weighted sample size: 64,244,421) participants aged 18 years or older in the 14 states completing the General Preparedness module, the largest proportion of respondents in each demographic characteristic were white (74.3%), aged 25 years or older (90.1%), had at least a high school education (90.7%), and responded to the survey in English (98.3%) (Table 1).
Table 1.
Prevalence Estimates of Household Preparedness Item by Sociodemographic Characteristic, Behavioral Risk Factor Surveillance Survey, 2006–2010
| Demographic Characteristic | Study Characteristics | 3-Day Supply of Food | 3-Day Supply of Water | Evacuation Plan | Working Radio | Working Flashlight | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| % (95% CI) | % (95% CI) | Chi2 p-Value | % (95%) CI | Chi2 p-Value | % (95% CI) | Chi2 p-Value | % (95% CI) | Chi2 p-Value | % (95% CI) | Chi2 p-Value | |
| Overall | 104,654 (weighted: 64,244,421) | 82.9 (82.4–83.5) | 53.6 (52.9–54.3) | 21.1 (20.6–21.7) | 77.7 (77.2–78.3) | 94.8 (94.4–95.1) | |||||
| Sex | |||||||||||
| Men | 48.2 (47.5–48.8) | 84.2 (83.3–85.0) | <0.0001 | 57.2 (56.1–58.3) | <0.0001 | 21.0 (20.2–21.9) | 0.6631 | 79.6 (78.6–80.5) | <0.0001 | 95.6 (95.1–96.1) | <0.0001 |
| Women | 51.8 (51.2–52.5) | 81.8 (81.1–82.5) | 50.3 (49.4–51.1) | 21.3 (20.6–21.9) | 76.1 (75.3–76.8) | 94.0 (93.6–94.4) | |||||
| Race | |||||||||||
| White non-Hispanic | 74.3 (73.7–75.0) | 84.8 (84.2–85.4) | <0.0001 | 52.1 (51.3–52.9) | <0.0001 | 19.6 (19.0–20.2) | <0.0001 | 80.4 (79.8–81.0) | <0.0001 | 97.0 (96.7–97.2) | <0.0001 |
| Black non-Hispanic | 14.0 (13.5–14.4) | 77.9 (76.1–79.5) | 58.2 (56.3–60.2) | 26.2 (24.7–27.9) | 72.4 (70.5–74.1) | 89.1 (87.8–90.2) | |||||
| Hispanic | 6.5 (6.1–6.9) | 75.0 (71.6–78.1) | 55.0 (51.4–58.7) | 26.8 (23.9–29.9) | 67.1 (63.5–70.4) | 84.4 (81.5–86.9) | |||||
| Other non-Hispanica | 5.2 (4.9–5.5) | 78.7 (75.5–81.6) | 60.4 (57.0–63.7) | 23.9 (21.3–26.7) | 67.3 (63.7–70.8) | 90.8 (88.4–92.8) | |||||
| Age | |||||||||||
| 18–24 | 9.9 (9.4–10.5) | 79.7 (77.1–82.1) | <0.0001 | 53.1 (50.0–56.3) | <0.0001 | 17.9 (15.9–20.1) | <0.0001 | 75.6 (72.8–78.2) | 0.0001 | 92.0 (90.2–93.5) | <0.0001 |
| 25–44 | 39.2 (38.5–39.9) | 79.5 (78.4–80.5) | 48.5 (47.3–49.8) | 19.8 (18.8–20.7) | 76.5 (75.4–77.6) | 93.6 (92.9–94.2) | |||||
| 45–54 | 19.2 (18.8–19.7) | 83.5 (82.5–84.5) | 52.9 (51.6–54.3) | 21.5 (20.5–22.6) | 79.5 (78.4–80.5) | 95.8 (95.2–96.3) | |||||
| 55+ | 31.7 (31.2–32.2) | 87.9 (87.4–88.5) | 60.2 (59.4–61.1) | 23.5 (22.8–24.2) | 78.8 (78.1–79.5) | 96.5 (96.1–96.8) | |||||
| Education | |||||||||||
| <High school | 9.3 (8.9–9.7) | 80.0 (78.0–81.8) | 0.0001 | 59.7 (57.4–61.9) | <0.0001 | 26.7 (24.8–28.6) | <0.0001 | 67.8 (65.6–70.0) | <0.0001 | 88.3 (86.6–89.8) | <0.0001 |
| High school | 30.1 (29.5–30.7) | 83.8 (82.8–84.7) | 57.0 (55.7–58.2) | 24.8 (23.8–25.8) | 78.6 (77.5–79.6) | 94.5 (94.0–95.1) | |||||
| Some college | 25.4 (24.8–26.0) | 84.3 (83.3–85.3) | 53.5 (52.1–54.8) | 22.0 (21.0–23.1) | 79.7 (78.6–80.7) | 95.1 (94.4–95.7) | |||||
| College or more | 35.2 (34.6–35.9) | 82.0 (81.0–83.0) | 49.3 (48.1–50.4) | 16.1 (15.3–16.9) | 78.2 (77.2–79.1) | 96.4 (95.8–96.8) | |||||
| Survey language | |||||||||||
| English | 98.3 (98.1–98.5) | 83.2 (82.7–83.8) | <0.0001 | 53.6 (52.9–54.3) | 0.0008 | 20.6 (20.1–21.2) | 0.0661 | 78.1 (77.5–78.7) | <0.0001 | 95.2 (94.8–95.5) | <0.0001 |
| Spanish | 1.7 (1.5–1.9) | 68.2 (62.1–73.7) | 64.5 (58.2–70.2) | 25.6 (20.7–31.2) | 56.5 (50.0–62.7) | 74.7 (68.7–79.9) | |||||
Asian, non-Hispanic; Native Hawaiian/Pacific Islander, non-Hispanic; American Indian/Alaska Native, non-Hispanic; other race, non-Hispanic; multirace, non-Hispanic.
Preparedness Items and Demographics
Food
Most respondents (82.9%) reported that their household had a 3-day supply of food (Table 1), with women (81.8%), Hispanics (75.0%), people aged 25–44 years (79.5%), individuals with less than a high school education (80.0%), and those receiving the survey in Spanish (68.2%) being the least likely to report having a 3-day supply of food. White non-Hispanic people (84.8%), people aged 55 years or older (87.9%), and individuals with some college education (84.3%) were most likely to have a 3-day supply of food.
Water
Overall, 53.6% of respondents reported having a 3-day supply of water (Table 1). Women (50.3%), white non-Hispanic people (52.1%), people aged 25–44 years (48.5%), individuals with at least a college education (49.3%), and people responding to the survey in English (53.6%) were the least likely to report having a 3-day supply of water. Other non-Hispanic people (60.4%), people aged 55 years and older (60.2%), and individuals with less than a high school education (59.7%) were most likely to have a 3-day supply of water.
Plan
Approximately one-fifth (21.1%) of respondents reported that they have a written evacuation plan (Table 1), with men (21.0%), white non-Hispanic people (19.6%), people aged 18–24 (17.9%), individuals with college education or higher (16.1%), and those receiving the survey in the English language (20.6%) being the least likely to report having a written plan. Hispanic people (26.8%), people aged 55 years or older (23.5%), and individuals with less than a high school education (26.7%) were most likely to have a written evacuation plan.
Radio
More than three-fourths (77.7%) of respondents reported that they have a working radio (Table 1), with women (76.1%), Hispanic people (67.1%), people aged 18–24 years (75.6%), individuals with less than a high school education (67.8%), and people receiving the survey in Spanish (56.5%) being the least likely to report having a working radio. White non-Hispanic people (80.4%), people aged 45–54 years (79.5%), and individuals with some college education (79.7%) were most likely to have a working battery-powered radio.
Flashlight
The majority of respondents (94.8%) reported having a working flashlight (Table 1), with women (94.0%), Hispanic people (84.4%), people aged 18–24 years (92.0%), individuals with less than a high school education (88.3%), and people receiving the survey in the Spanish language (74.7%) being the least likely to report having a flashlight. White non-Hispanic people (97.0%), people aged 55 years or older (96.5%), and individuals with at least a college education (96.4) were most likely to have having a working flashlight.
Number of Preparedness Items and Demographics
Overall, fewer than half the people surveyed had 4 or more of the recommended preparedness items in their households (34.1% had 4, and 12.3% had 5) (Table 2). Approximately one-third (32.9%) reported having 3 items, 14.6% reported having 2 items, 4.8% reported having 1 item, and 1.3% of the population reported having none of the preparedness items.
Table 2.
Prevalence Estimates of Number of Preparedness Items by Sociodemographic Characteristics, Behavioral Risk Factor Surveillance Survey, 2006–2010
| Demographic Characteristic | 0 Items % (95% CI) | 1 Item % (95% CI) | 2 Items % (95% CI) | 3 Items % (95% CI) | 4 Items % (95% I | 5 Items % (95% CI) | Chi2 p-Value |
|---|---|---|---|---|---|---|---|
| Overall | 1.3 (1.1–1.5) | 4.8 (4.5–5.1) | 14.6 (14.1–15.2) | 32.9 (32.3–33.6) | 34.1 (33.4–34.8) | 12.3 (11.9–12.7) | |
| Sex | |||||||
| Men | 1.1 (0.8–1.3) | 4.0 (3.5–4.5) | 13.4 (12.7–14.3) | 31.9 (30.8–33.0) | 36.7 (35.7–37.8) | 12.9 (12.3–13.6) | <0.0001 |
| Women | 1.5 (1.3–1.8) | 5.5 (5.2–6.0) | 15.7 (15.1–16.4) | 33.9 (33.1–34.7) | 31.7 (30.9–32.4) | 11.6 (11.2–12.1) | |
| Race | |||||||
| White non-Hispanic | 0.8 (0.7–1.0) | 3.9 (3.7–4.2) | 13.9 (13.3–14.4) | 34.6 (33.8–35.3) | 35.5 (34.8–36.3) | 11.3 (10.9–11.8) | <0.0001 |
| Black non-Hispanic | 2.7 (2.1–3.4) | 7.0 (6.0–8.2) | 15.9 (14.5–17.3) | 28.6 (26.7–30.5) | 30.2 (28.4–32.1) | 15.6 (14.4–17.0) | |
| Hispanic | 3.2 (2.2–4.5) | 8.8 (6.7–11.5) | 19.6 (16.7–22.9) | 27.0 (23.9–30.4) | 27.3 (24.2–30.6) | 14.2 (11.9–16.8) | |
| Other non-Hispanica | 2.5 (1.6–4.0) | 6.4 (4.9–8.5) | 16.0 (13.4–18.9) | 29.0 (25.8–32.6) | 31.6 (28.4–35.0) | 14.4 (12.4–16.6) | |
| Age | |||||||
| 18–24 | 2.2 (1.4–3.4) | 5.6 (4.5–7.1) | 15.8 (13.5–18.4) | 34.5–31.5–37.6) | 32.3 (29.3–25.4) | 9.6 (8.2–11.3) | <0.0001 |
| 25–44 | 1.6 (1.4–2.0) | 6.0 (5.4–6.7) | 16.6 (15.6–17.5) | 34.6 (33.4–35.9) | 30.5 (29.3–31.6) | 10.7 (10.0–11.4) | |
| 45–54 | 1.1 (0.9–1.4) | 4.4 (3.9–5.0) | 14.5 (13.6–15.5) | 32.7 (31.5–34.0) | 34.2 (32.9–35.5) | 13.0 (12.2–14.0) | |
| 55+ | 0.7 (0.5–0.9) | 3.2 (2.9–3.5) | 12.0 (11.5–12.6) | 30.7 (29.9–31.5) | 39.0 (38.2–39.9) | 14.4 (13.8–15.0) | |
| Education | |||||||
| < High school | 2.8 (2.1–3.8) | 6.9 (5.8–8.3) | 16.8 (15.0–18.7) | 27.3 (25.2–29.5) | 30.4 (28.3–32.5) | 15.8 (14.3–17.4) | <0.0001 |
| High school | 1.3 (3.8–4.9) | 4.3 (3.8–4.9) | 13.6 (12.7–14.5) | 30.6 (29.4–31.8) | 35.5 (34.3–36.7) | 14.7 (13.9–15.6) | |
| Some college | 1.1 (0.8–1.4) | 4.5 (3.9–5.1) | 13.7 (12.8–14.7) | 33.0 (31.7–34.3) | 35.0 (33.7–36.3) | 12.8 (12.0–13.7) | |
| College or more | 1.0 (0.8–1.4) | 4.9 (4.4–5.5) | 15.7 (14.8–16.6) | 36.3 (25.1–37.4) | 33.2 (32.1–34.3) | 8.9 (8.3–9.5) | |
| Survey language | |||||||
| English | 1.2 (1.0–1.4) | 4.7 (4.4–5.1) | 14.5 (14.0–15.1) | 33.1 (32.4–33.8) | 34.3 (33.7–35.0) | 12.1 (11.7–12.5) | 0.0002 |
| Spanish | 6.3 (3.7–10.3) | 10.1 (6.9–14.5) | 18.5 (14.1–23.8) | 28.0 (22.2–34.6) | 25.9 (20.7–32.0) | 11.3 (7.9–15.8) | |
Asian, non-Hispanic; Native Hawaiian/Pacific Islander, non-Hispanic; American Indian/Alaska Native, non-Hispanic; other race, non-Hispanic; multirace, non-Hispanic.
Perception and Demographics
Overall, only 25.3% of the population felt that their households were well prepared, with most respondents reporting that their households were somewhat prepared (55.5%) (Table 3). Men responding to the survey were significantly more likely than women to report feeling that their households were well prepared (29.3% versus 21.7%), and women were significantly more likely than men to report feeling their households were not prepared at all (21.4% versus 16.7%). People aged 55 years and older were significantly more likely than younger people to report feeling their households were well prepared. People with at least a college education were significantly less likely than those with less education to report feeling their households were well prepared. Those with less than a high school education were significantly more likely than those with a higher educational attainment to report feeling their households were not prepared at all (28.0% versus 18.8%, 18.4% and 17.8%). Notably, people requesting the survey to be conducted in Spanish were significantly more likely than those requesting that the survey be conducted in English to report feeling that their households were not prepared at all (41.9% versus 18.7%).
Table 3.
Level of Perceived Preparedness by Sociodemographic Characteristic, Behavioral Risk Factor Surveillance Survey, 2006–2010
| Characteristic | Level of Perceived Preparedness | Chi-square | ||
|---|---|---|---|---|
| Well-Prepared | Somewhat Prepared | Not Prepared at All | ||
| Overall | 25.3 (24.8–25.9) | 55.5 (54.9–56.2) | 19.1 (18.6–19.7) | |
| Sex | ||||
| Men | 29.3 (28.3–30.3) | 54.0 (52.9–55.2) | 16.7 (15.8–17.6) | <0.0001 |
| Women | 21.7 (21.0–22.3) | 56.9 (56.1–57.8) | 21.4 (20.7–22.1) | |
| Race | ||||
| White non-Hispanic | 26.2 (25.6–26.9) | 56.9 (56.2–57.7) | 16.9 (16.3–17.5) | <0.0001 |
| Black non-Hispanic | 23.0 (21.4–24.7) | 52.8 (50.8–54.7) | 24.2 (22.6–25.9) | |
| Hispanic | 21.0 (18.0–24.3) | 48.7 (45.0–52.3) | 30.3 (27.2–33.7) | |
| Other non-Hispanica | 23.4 (20.9–26.2) | 51.0 (47.5–54.5) | 25.6 (22.5–28.9) | |
| Age | ||||
| 18–24 | 26.5 (23.8–29.4) | 52.7 (49.5–55.8) | 20.9 (18.5–23.5) | <0.0001 |
| 25–44 | 20.3 (19.3–21.3) | 56.9 (55.7–58.2) | 22.8 (21.8–23.9) | |
| 45–54 | 23.8 (22.7–25.0) | 56.4 (55.0–57.7) | 19.9 (18.8–21.0) | |
| 55+ | 32.2 (31.4–33.0) | 54.2 (53.3–55.0) | 13.6 (13.0–14.3) | |
| Education | ||||
| Less than high school | 26.8 (24.8–28.8) | 45.2 (42.9–47.5) | 28.0 (25.9–30.2) | <0.0001 |
| High school diploma | 26.8 (25.7–27.9) | 54.5 (53.2–55.7) | 18.8 (17.8–19.8) | |
| Some college | 26.3 (25.1–27.5) | 55.3 (53.9–56.6) | 18.4 (17.4–19.6) | |
| College or more | 23.1 (22.1–24.0) | 59.2 (58.0–60.3) | 17.8 (16.8–18.7) | |
| Survey language | ||||
| English | 25.5 (24.9–26.1) | 55.8 (55.1–56.5) | 18.7 (18.2–19.3) | <0.0001 |
| Spanish | 11.8 (7.3–18.7) | 46.3 (39.8–52.9) | 41.9 (35.7–48.4) | |
Asian, non-Hispanic; Native Hawaiian/Pacific Islander, non-Hispanic; American Indian/Alaska Native, non-Hispanic; other race, non-Hispanic; multirace, non-Hispanic.
Preparedness Item and Perception
Respondents who reported feeling their households were well prepared were 4.2 times more likely to report having a 3-day supply of food compared to those who did not report feeling well prepared (adjusted for sociodemographic covariates: sex, age group, race/ethnicity, survey language, and education) (Table 4). A similar pattern was found for a 3-day supply of water (AOR = 4.0), a written evacuation plan (AOR = 3.1), a working battery-operated radio (AOR = 2.6), and a flashlight (AOR = 2.3). Overall, as the number of preparedness items increased, respondents were more likely to report feeling their households were well prepared (0 items, 4.2%; 1 item, 4.2%; 2 items, 8.2%; 3 items, 15.4%; 4 items, 35.1%; 5 items, 56.5%) and less likely to report that their households were not prepared at all (0 items, 79.0%; 1 item, 63.9%; 2 items, 39.0%; 3 items, 19.1%; 4 items, 7.4%; 5 items, 3.7%) (Figure 1).
Table 4.
Adjusted Odds Ratios of Being Well Prepared by Preparedness Item, Behavioral Risk Factor Surveillance Survey, 2006–2010
| Item | Well Prepared AORa (95% CI) | Not Well Prepared AORa (95% CI) |
|---|---|---|
| 3-day supply of food | 4.2 (3.7–4.8) | Referent |
| 3-day supply of water | 4.0 (3.7–4.3) | Referent |
| Evacuation plan | 3.1 (2.8–3.3) | Referent |
| Radio | 2.6 (2.4–2.9) | Referent |
| Flashlight | 2.3 (1.9–2.9) | Referent |
Adjusted odds ratio by age, sex, race/ethnicity, survey language, and education.
Figure 1.
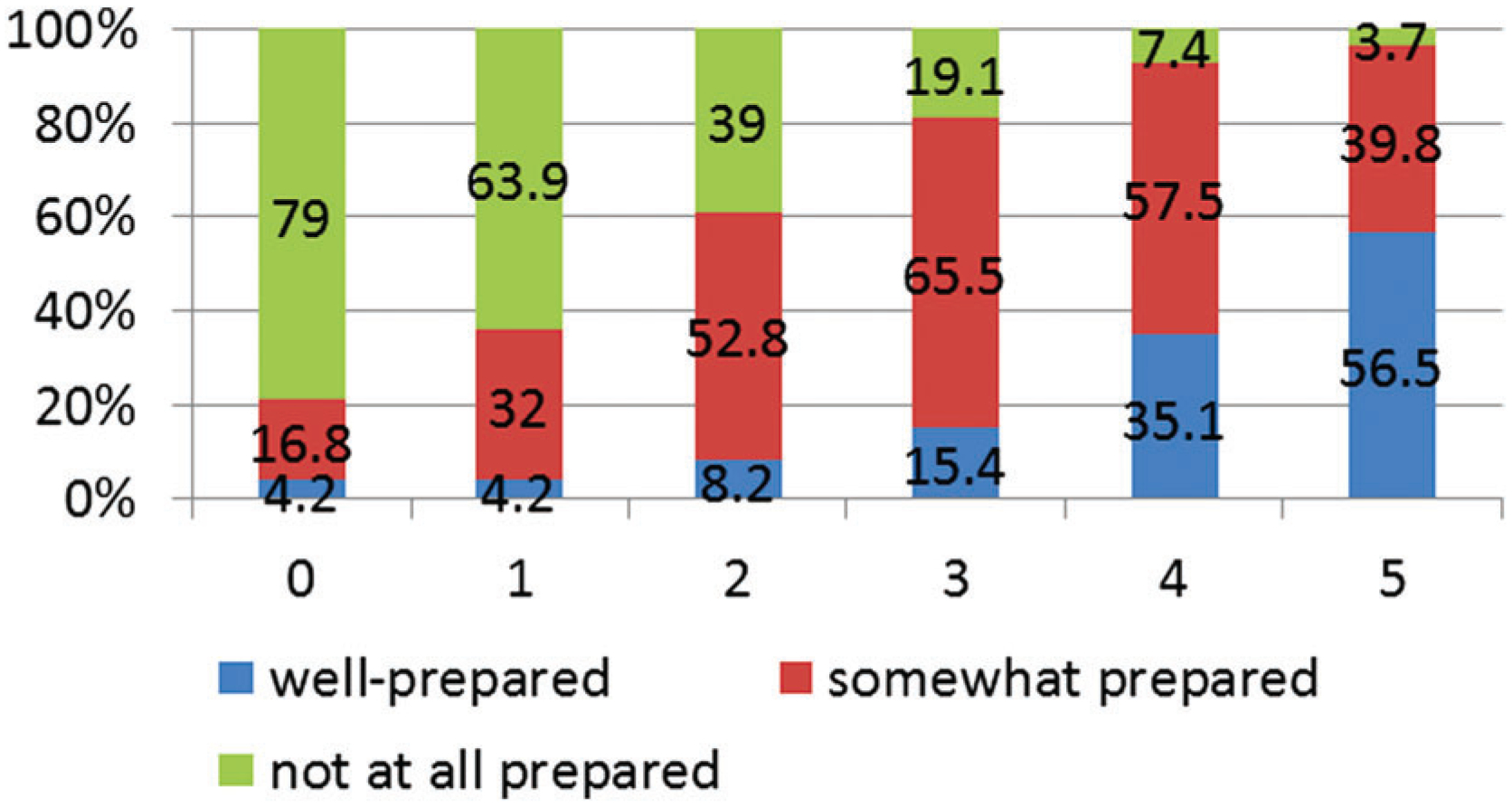
Perception of Preparedness by Number of Items, BRFSS, 2006–2010
Discussion
Analysis of the 2006–2010 BRFSS data for 14 states revealed that only a quarter of the respondents felt their households were well prepared. Fewer than half of the respondents surveyed indicated that their household had 4 or more of the recommended preparedness items, and only 12.3% of the respondents reported having all 5 of the recommended household preparedness items. Despite the low prevalence of prepared items, households reporting a preparedness perception of being well prepared were more likely to report having more preparedness items. The items most likely to be associated with respondents perceiving their households to be well prepared was a 3-day supply of food, followed by a 3-day supply of water, a written preparedness plan, a working battery-operated radio, and, lastly, a working flashlight.
Results of the preparedness items by state have been previously published.5 Although these data were gathered in different states during various years (2006: Connecticut, Montana, Nevada, and Tennessee; 2007: Delaware, Louisiana, Maryland, Nebraska, and New Hampshire; 2008: Georgia, Montana, Nebraska, New York, and Pennsylvania; 2009: Mississippi; and 2010: Montana and North Carolina), there were no significant differences found overall between the prevalence of each respective preparedness item when compared to other states, apart from the notable exception of Louisiana, which had experienced the devastating Hurricane Katrina 2 years prior to the data collection. Louisiana reported significantly more working battery-operated radios and significantly more written evacuation plans among survey respondents compared to the rest of the states.5
Generally, as age increased, so did the likelihood of respondents indicating that their household had each preparedness item. Within the existing literature, some studies have found increased age among adults to be correlated with better preparedness,19,20,25 while others have not.6,26 Since disasters are known to disproportionately affect the frail elderly,37–39 perhaps focusing on the correlations between health conditions and preparedness, rather than age alone, would provide more consistent results.40
Our results show that respondents who are traditionally considered the most vulnerable were the least likely to be prepared. Previous studies have shown that individuals with low socioeconomic status, such as those with little education, as well as minorities and individuals with language barriers, such as recent immigrants, are less likely to have the ability to acquire disaster preparedness items and obtain access to preparedness information.3,6–10 Most national, state, and county disaster preparedness information and warnings are often available only in English, are written at reading levels above 9th grade, and are difficult to obtain without internet access,41–45 thus creating an access barrier for populations with low literacy levels, limited English language abilities, and a lack of financial resources.
Further, although national, state, and nonprofit websites are including more translated material,45 individuals must have the ability and motivation to look for preparedness material in this manner.46 It has also been noted that many public health and safety organizations frequently provide literal translations of English-language materials, which often vary from what is culturally acceptable; literal translations of preparedness messages could be difficult for some immigrant populations to understand.41,45
To increase preparedness behaviors, one must first understand the barriers and motivators associated with adopting the behavior.47 Although not the only contributing factor, several theories and models support the need for an individual to be knowledgeable of options and their associated benefits as an important first step toward behavior change.48–50 Studies have shown that many ethnic minorities acquire information through religious and social groups, not through internet resources.41–44 Specifically, Hispanic people have been found to use social networks to share disaster-related information more than non-Hispanic white or non-Hispanic black people.51,52 Preparedness messages need to be delivered through alternative methods that reach beyond the internet and into the community, such as through mass media campaigns and community-based and school-based interventions that involve a family educational component.10,41–44,51,52
National, state, and local agencies that encourage household preparedness behaviors sometimes promote the adoption of such protective behaviors through inconsistent recommendations.10,16,18,53 This has led to variability between agencies as to how many and which supplies to stockpile and in the definition of a family communication plan.10,16,18,54,55 For example, agencies often recommend some of the following components of a family communication plan: (1) a prearranged meeting place for family members after a disaster; (2) a list of important phone numbers and a plan for contacting each family member after a disaster; (3) an evacuation route for a family during a disaster; and (4) a phone number of an out-of-state relative or contact to call.10,12,16,54,55 Recommendations about what the plan should include and whether the plan should be written, verbally discussed, or both also vary across agencies.10,16,41,52,55 Additionally, the lists of recommended preparedness supplies are often different.10,16,53,54 While many campaigns consistently encourage households to acquire basic items such as water, food, and a flashlight to prepared for all hazards, the lists vary concerning the quantities of items to stock as well as other stockpiled items, such as pet supplies, batteries, types of radios, masks, and medications.10,16,20,54 Some households may appreciate that different lists have different suggestions, but others may find the lack of standardization confusing and question the usefulness of the behavior.
As found in other studies, respondents were most likely to have basic nonperishable household items, such as a flashlight, and less likely to have supplies that need to be replenished, such as water.19,20 Although having a written disaster communication plan was the least common preparedness item attained by respondents, it was more highly correlated with the respondents’ perception of being prepared than having a radio and flashlight. Notably, the questions related to having a radio and flashlight as well as the questions related to having a 3-day supply of water and food did not specifically ask if the items were acquired and stored for use specifically during a disaster. As previously discussed, the possession of these items does not imply that they are intended or available for use during a disaster, or that they rely on resources that could not be readily available during a disaster.6,19,20 Given this, refinements of the metrics used to assess preparedness items for future disasters are needed.6,10,20,55
This study has several limitations. First, the study is cross-sectional and self-reported. The self-reporting nature of the data may increase the likelihood of social desirability and self-selection bias. Moreover, acknowledgment of preparedness items was dependent on the participant’s knowledge of the items in the household. Second, BRFSS data likely underrepresent some minority groups and people with limited English since the survey is offered only in English and Spanish. During the timeframe of the study, the BRFSS survey queried only households with landline telephone access, thus excluding households with cell phones only, people who were homeless, people residing in group homes or institutions, and individuals without the capacity to complete a telephone interview. These issues are mitigated by the large sample size and poststratification weights available in BRFSS. Third, the response rates were low: Approximately 1 of every 2 people contacted agreed to participate in the survey. Finally, the respondents from the 14 surveyed states may not necessarily represent perceptions in nonsurveyed states or surrounding states/regions.
Although other studies have noted a gap between actual and perceived preparedness, our results suggest an association between preparedness perception and number of preparedness items in the household. To increase the perception of a prepared household, members need to be knowledgeable about the protective behaviors associated with being well prepared.6,10,48,56 Given this, it could be beneficial to increase state and community-based outreach programs promoting the actions and associated benefits of household preparedness activities. Moreover, additional work should be done to increase knowledge among vulnerable populations, such as the development of culturally appropriate messaging that is easily accessible through religious, social, and education institutions, at an 8th-grade reading level or lower.
Footnotes
The findings and conclusions in this article are those of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention.
References
- 1.Van Zandt S, Peacock WG, Henry DW, Grover H, High-field WE, Brody SD. Mapping social vulnerability to enhance housing and neighborhood resilience. Housing Policy Debate 2012;22(1):29–55. [Google Scholar]
- 2.Baker EJ. Household preparedness for the aftermath of hurricanes in Florida. Appl Geogr 2011;31(1):46–52. [Google Scholar]
- 3.Lindell MK. Disaster studies. Curr Sociol 2013;61(5–6): 797–825. [Google Scholar]
- 4.Strine TW, Neff LJ, Crawford S. Health-related quality of life domains and household preparedness for public health emergencies: Behavioral Risk Factor Surveillance System, 2006–2010. Disaster Med Public Health Prep 2013;7(2):191–200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.DeBastiani SD, Strine TW. Household preparedness for public health emergencies—14 states, 2006–2010 (reprinted from MMWR 2012; 36:713–719). JAMA 2013;39:21–24. [Google Scholar]
- 6.Levac J, Toal-Sullivan D, O’Sullivan TL. Household emergency preparedness: a literature review. J Community Health 2012;37(3):725–733. [DOI] [PubMed] [Google Scholar]
- 7.Fothergill A, Maestas EG, Darlington JD. Race, ethnicity and disasters in the United States: a review of the literature. Disasters 1999;23(2):156–173. [DOI] [PubMed] [Google Scholar]
- 8.Peguero AA. Latino disaster vulnerability: the dissemination of hurricane mitigation information among Florida’s homeowners. Hisp J Behav Sci 2006;28(1):5–22. [Google Scholar]
- 9.Bourque LB, Regan R, Kelley MM, Wood MM, Kano M, Mileti DS. An examination of the effect of perceived risk on preparedness behavior. Environ Behav 2013;45(5):615–649. [Google Scholar]
- 10.Kohn S, Eaton JL, Feroz S, Bainbridge AA, Hoolachan J, Barnett DJ. Personal disaster preparedness: an integrative review of the literature. Disaster Med Public Health Prep 2012;6(3):217–231. [DOI] [PubMed] [Google Scholar]
- 11.Fothergill A, Peek LA. Poverty and disasters in the United States: a review of recent sociological findings. Nat Hazards 2004;32(1):89–110. [Google Scholar]
- 12.Donahue AK, Eckel CC, Wilson RK. Ready or not? How citizens and public officials perceive risk and preparedness. Public Adm Rev 2014;44(7):89S–111S. [Google Scholar]
- 13.Hick JL, Hanfling D, Burstein JL, et al. Health care facility and community strategies for patient care surge capacity. Ann Emerg Med 2004;44(3):253–261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.The White House. National Security Strategy. 2010. www.whitehouse.gov/sites/default/files/rss_viewer/national_security_strategy.pdf. Accessed July 29, 2015.
- 15.Lindell MK, Prater CS. Assessing community impacts of natural disasters. Nat Hazards Rev 2003;4(4):176–185. [Google Scholar]
- 16.Uscher-Pines L, Chandra A, Acosta J. Household preparedness is not enough: the challenges and opportunities in assessing community readiness for disasters. J Public Health Manag Pract 2013;19:S70–S76. [DOI] [PubMed] [Google Scholar]
- 17.Schoch-Spana M The people’s role in US national health security: past, present, and future. Biosecur Bioterror 2012; 10(1):77–88. [DOI] [PubMed] [Google Scholar]
- 18.Tierney KJ, Lindell MK, Perry RW. Facing the Unexpected: Disaster Preparedness and Response in the United States. Washington, DC: Joseph Henry Press; 2001. [Google Scholar]
- 19.Murphy ST, Cody M, Frank LB, Glik D, Ang A. Predictors of emergency preparedness and compliance. Disaster Med Public Health Prep 2009;3(2):1–10. [DOI] [PubMed] [Google Scholar]
- 20.Ablah E, Konda K, Kelley CL. Factors predicting individual emergency preparedness: a multi-state analysis of 2006 BRFSS data. Biosecur Bioterror 2009;7(3):317–330. [DOI] [PubMed] [Google Scholar]
- 21.Sattler DN, Kaiser CF, Hittner JB. Disaster preparedness: relationships among prior experience, personal characteristics, and distress. J Appl Soc Psychol 2000;30(7):1396–1420. [Google Scholar]
- 22.Russell LA, Goltz JD, Bourque LB. Preparedness and hazard mitigation actions before and after two earthquakes. Environ Behav 1995;27(6):744–770. [Google Scholar]
- 23.Faupel CE, Kelley SP, Petee T. The impact of disaster education on household preparedness for Hurricane Hugo. Int J Mass Emerg Disasters 1992;10(1):5–24. [Google Scholar]
- 24.Paton D, Smith LM, Johnston D. Volcanic hazards: risk perception and preparedness. NZ J Psychol 2000; 29(2): 86–91. [Google Scholar]
- 25.Eisenman DP, Wold C, Fielding J, et al. Differences in individual-level terrorism preparedness in Los Angeles County. Am J Prev Med 2006;30(1):1–6. [DOI] [PubMed] [Google Scholar]
- 26.McCormick LC, Pevear III J, Xie R. Measuring levels of citizen public health emergency preparedness, Jefferson County, Alabama. J Public Health Manag Pract 2013;19(3):266–273. [DOI] [PubMed] [Google Scholar]
- 27.Chen V, Banerjee D, Liu L. Do people become better prepared in the aftermath of a natural disaster? The Hurricane Ike experience in Houston, Texas. J Public Health Manag Pract 2012;18(3):241–249. [DOI] [PubMed] [Google Scholar]
- 28.Personal Preparedness in America: Findings from the 2009 Citizen Corps National Survey. Washington, DC: FEMA; 2009. https://s3-us-gov-west-1.amazonaws.com/dam-production/uploads/20130726-1859-25045-2081/2009_citizen_corps_national_survey_findings___full_report.pdf. Accessed July 29, 2015. [Google Scholar]
- 29.Paek HJ, Hilyard K, Freimuth V, Barge JK, Mindlin M. Theory-based approaches to understanding public emergency preparedness: implications for effective health and risk communication. J Health Commun 2010;15(4): 428–444. [DOI] [PubMed] [Google Scholar]
- 30.Miceli R, Sotgiu I, Settanni M. Disaster preparedness and perception of flood risk: a study in an alpine valley in Italy. J Environ Psychol 2008;28(2):164–173. [Google Scholar]
- 31.Slovic P Perception of risk. Science 1987;236(4799):280–285. [DOI] [PubMed] [Google Scholar]
- 32.Sjöberg L Factors in risk perception. Risk Anal 2000; 20(1):1–12. [PubMed] [Google Scholar]
- 33.Loewenstein GF, Weber EU, Hsee CK, Welch N. Risk as feelings. Psychol Bull 2001;127(2):267–286. [DOI] [PubMed] [Google Scholar]
- 34.Ho MC, Shaw D, Lin S, Chiu YC. How do disaster characteristics influence risk perception? Risk Anal 2008;28(3): 635–643. [DOI] [PubMed] [Google Scholar]
- 35.Basolo V, Steinberg LJ, Burby RJ, Levine J, Cruz AM, Huang C. The effects of confidence in government and information on perceived and actual preparedness for disasters. Environ Behav 2008;41(3):338–364. [Google Scholar]
- 36.CDC. Methodologic changes in the Behavioral Risk Factor Surveillance System in 2011 and potential effects on prevalence estimates. MMWR Surveil Summ 2012;61(22): 410. [PubMed] [Google Scholar]
- 37.Fernandez LS, Byard D, Lin CC, Benson S, Barbera JA. Frail elderly as disaster victims: emergency management strategies. Prehosp Disaster Med 2002;17(2):67–74. [DOI] [PubMed] [Google Scholar]
- 38.Aldrich N, Benson WF. Disaster preparedness and the chronic disease needs of vulnerable older adults. Prev Chronic Dis 2008;5(1):A27. [PMC free article] [PubMed] [Google Scholar]
- 39.The White House. The Federal Response to Hurricane Katrina: Lessons Learned. 2006. http://www.floods.org/PDF/Katrina_Lessons_Learned_0206.pdf. Accessed July 29, 2015.
- 40.Ko JY, Strine TW, Allweiss P. Chronic conditions and household preparedness for public health emergencies: Behavioral Risk Factor Surveillance System, 2006–2010. Prehosp Disaster Med 2014;29(1):13–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Nunez-Alvarez A, Martinez K, Ramos A, Gastelum F. San Diego Firestorm 2007 Report: Fire Impact on Farm Workers and Migrant Communities in North County. San Marcos, CA: National Latino Research Center, California State University; 2007. [Google Scholar]
- 42.Wang T, Yasui L. Integrating immigrant families in emergency response, relief and rebuilding efforts. GCIR website. 2008. https://www.gcir.org/publications/gcirpubs/emergency. Accessed July 29, 2015.
- 43.James X, Hawkins A, Rowel R. An assessment of the cultural appropriateness of emergency preparedness communication for low income minorities. Journal of Homeland Security and Emergency Management 2007;4(3). [Google Scholar]
- 44.Andrulis DP, Siddiqui NJ, Gantner JL. Preparing racially and ethnically diverse communities for public health emergencies. Health Aff (Millwood) 2007;26(5):1269–1279. [DOI] [PubMed] [Google Scholar]
- 45.Bott C, Gupta V, Jones K, Karr A, Lark R, McGee S. Public Role and Engagement in Counterterrorism Efforts: Implications of Israeli Practices for the U.S. Arlington, VA: Homeland Security Institute; 2009. http://www.hstoday.us/images/public_role_in_ct_israeli_practices_task_08-22.pdf. Accessed July 29, 2015. [Google Scholar]
- 46.Friedman DB, Tanwar M, Richter JV. Evaluation of online disaster and emergency preparedness resources. Prehosp Disaster Med 2008;23(5):438–446. [DOI] [PubMed] [Google Scholar]
- 47.Prochaska JO, Norcross JC. Stages of change. Psychotherapy 2001;38(4):443–448. [Google Scholar]
- 48.Bandura A Social Learning Theory. Englewood Cliffs, NJ: Prentice-Hall; 1977:305–316. [Google Scholar]
- 49.Ajzen I, Heilbroner RL, Fishbein M, Thurow LC. Understanding Attitudes and Predicting Social Behavior. Englewood Cliffs, NJ: Prentice-Hall; 1980. [Google Scholar]
- 50.Becker MH. The Health Belief Model and Personal Health Behavior. Thorofare, NJ: CB Slack; 1974. [Google Scholar]
- 51.Fothergill A, Maestas EG, Darlington JD. Race, ethnicity and disasters in the United States: a review of the literature. Disasters 1999;23(2):156–173. [DOI] [PubMed] [Google Scholar]
- 52.Glik DC, Eisenman DP, Zhou Q, Tseng CH, Asch SM. Using the Precaution Adoption Process model to describe a disaster preparedness intervention among low-income Latinos. Health Educ Res 2014;29(2):272–283. [DOI] [PubMed] [Google Scholar]
- 53.Glik D, Blevins J, Drury A, Blevins J, Tan P, Shoaf K. Formative research for multi-cultural disaster supply kit campaign in Los Angeles County. Presented at: APHA Annual Meeting; 2006. [Google Scholar]
- 54.Wood MM, Kano M, Mileti DS, Bourque LB. Re-conceptualizing household disaster readiness: the “Get Ready” pyramid. J Emerg Manag 2009;7(1):25–37. [Google Scholar]
- 55.Uscher-Pines L, Chandra A, Acosta J, Kellermann A. Citizen preparedness for disasters: are current assumptions valid? Disaster Med Public Health Prep 2012;6(2):170–173. [DOI] [PubMed] [Google Scholar]
- 56.Wood MM, Mileti DS, Kano M, Kelley MM, Regan R, Bourque LB. Communicating actionable risk for terrorism and other hazards. Risk Anal 2012;32(4):601–615. [DOI] [PubMed] [Google Scholar]