

Abstract
Secretory carcinoma of the breast is a rare subtype of breast cancer. It can occur at any age but is usually diagnosed in patients under 30 years. It is the most common subtype of breast malignancy in the pediatric population and has a favorable outcome. Surgical excision is the best treatment and adjuvant therapies are still under debate. We present the case report of a 26-year-old patient with secretory carcinoma of the breast, including imaging, histologic findings, and clinical outcome.
Keywords: Breast cancer, breast, secretory carcinoma of the breast, triple-negative breast cancer
INTRODUCTION
Secretory carcinoma of the breast is an uncommon variant of breast cancer. McDivitt and Stewart first termed “juvenile breast carcinoma” by presenting a case series of seven pediatric patients in 1966.[1] The name was later replaced with “secretory carcinoma of the breast” since this disease occurs in all age groups.[2] A few male cases have also been reported in the literature (2%).[3] We present a case of a young female patient with secretory breast carcinoma.
CASE REPORT
A 26-year-old Taiwanese woman visited our hospital complaining of a palpable but painless lump in her right breast for 1 week. She had no significant medical history or family history of breast cancer. On physical examination, a 1.5 cm mass was noted at the lower inner quadrant of her right breast without nipple retraction or nipple discharge and fibroadenoma was suspected. Greyscale ultrasound revealed a heterogeneous hypoechoic mass with irregular shape and spiculated margin [Figure 1]. Color Doppler ultrasound showed internal vascularity[figure not shown]. No axillary lymphadenopathy was detected. Full-field digital mammography [Figure 2] and breast tomosynthesis showed an isodensity irregular mass with an obscured margin. The lesion was classified as BI-RADS 4B, and percutaneous core-needle biopsy confirmed that the mass was a secretory carcinoma.
Figure 1.
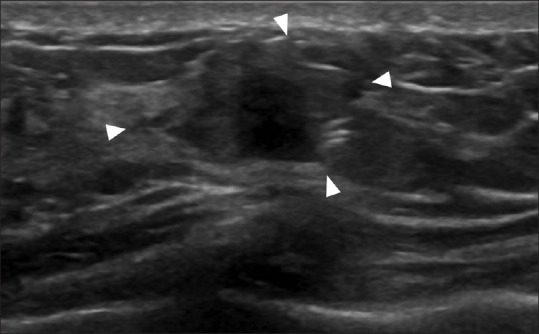
Grayscale ultrasound shows a heterogeneous irregular mass with spiculated margin (arrowheads)
Figure 2.

On craniocaudal view of full-field digital mammography, a 1.5 cm irregular isodensity mass with obscured margin is noted at the posterior lower inner region of the right breast (arrowheads)
Microscopic findings revealed tumor glands with band-looking nuclei and secretory material. There was no evidence of lymphovascular invasion, tumor necrosis, or microcalcification. No in situ component was present. On immunohistochemical staining, the tumor cells were diffusely positive for S100 protein, absence of myoepithelial cells in p40, and were negative for estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor 2 (HER2) (triple negative). The Ki67 proliferation index was low (6%) [Figure 3a and b]. The patient underwent surgical excision and remains disease-free after 1 year.
Figure 3.
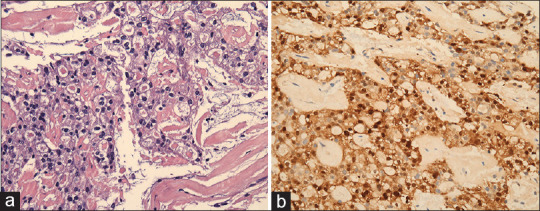
(a) High-power picture shows low-grade tumor glands with eosinophilic secretory material. (b) Tumor cells are diffusely immunoreactive for S100 protein
DISCUSSION
Secretory carcinoma of the breast is a rare type of invasive carcinoma, typically seen in children and young adults, and has a favorable prognosis. Although this is the most common breast cancer in the pediatric population,[4] only about 120 cases have been reported, so this disease is not well known in daily practice.
Secretory carcinoma of the breast mimics common benign breast lesions such as fibroadenoma on physical examination. Discrete nodular densities with irregular margins are frequently reported (if visible on mammography).[5] Ultrasound plays an important role compared to mammography and typically reveals a circumscribed, isoechoic, to hypoechoic mass with occasional heterogeneous internal echoes and lobulated margin. The imaging findings of secretory carcinoma are nonspecific. The differential diagnosis includes benign entities such as fibroadenoma and well-differentiated malignant carcinomas such as medullary, papillary, or mucinous subtypes.[5,6] A diagnosis depends on pathologic results, and the clinician should consider biopsy when there are suspicious features on BI-RADS such as irregular shape and non-circumscribed margins.
The histologic diagnosis is based on features, a mixture of well-circumscribed borders and pushing borders, with a variable combination of solid, tubular, and microcystic patterns. A sclerotic center may be present. These low-grade tumor cells contain eosinophilic granular to foamy or vacuolated cytoplasm and characteristic intracellular and extracellular secretory material. On immunohistochemical staining, the tumor is more commonly negative for ER, PR, and HER2. Some tumors, usually in adult male patients, may be positive for ER and PR.[7] In recent years, studies have shown that secretory carcinoma of the breast is associated with the balanced translocation t (12;15) (p13;q25), producing an ETV6–NTRK gene fusion, which can help pathologists distinguish this disease from ductal carcinoma.[8] Future developments in targeted therapy for secretory carcinoma are possible with this evidence.
The small number of cases hinders the establishment of standard treatment guidelines. Complete surgical excision is widely accepted as best practice, with breast bud preservation in pediatric cases.[3,6] Since axillary lymph node metastasis can occur in relatively small tumors (2.0 cm), sentinel lymph node dissection is generally indicated for larger tumors and may provide survival benefits.[7,9] Adjuvant chemotherapy is used if there is axillary lymph node metastasis. Radiation therapy is being used more often in recent years[3] and shows improved locoregional control. Local recurrence can occur 20 years after initial surgery;[10] hence, a 20-year follow up period is recommended.
In conclusion, secretory carcinoma of the breast is a rare breast cancer that is primarily seen in young people and has a good prognosis. Although there is no diagnostic imaging feature, clinicians should keep this differential diagnosis in mind in young patients with breast lesions. More clinical research is needed to better understand this disease.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understands that her name and initials will not be published and due efforts will be made to conceal her identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
Dr. Hong-Jen Chiou, a Deputy Editor-in-Chief at Journal of Medical Ultrasound, had no role in the peer review process of or decision to publish this article.
REFERENCES
- 1.McDivitt RW, Stewart FW. Breast carcinoma in children. JAMA. 1966;195:388–90. [PubMed] [Google Scholar]
- 2.d'Amore ES, Maisto L, Gatteschi MB, Toma S, Canavese G. Secretory carcinoma of the breast. Report of a case with fine needle aspiration biopsy. Acta Cytol. 1986;30:309–12. [PubMed] [Google Scholar]
- 3.Horowitz DP, Sharma CS, Connolly E, Gidea-Addeo D, Deutsch I. Secretory carcinoma of the breast: Results from the survival, epidemiology and end results database. Breast. 2012;21:350–3. doi: 10.1016/j.breast.2012.02.013. [DOI] [PubMed] [Google Scholar]
- 4.Chung EM, Cube R, Hall GJ, González C, Stocker JT, Glassman LM. From the archives of the AFIP: Breast masses in children and adolescents: Radiologic-pathologic correlation. Radiographics. 2009;29:907–31. doi: 10.1148/rg.293095010. [DOI] [PubMed] [Google Scholar]
- 5.Montalvo N, Posso V, Redrobán L. Secretory carcinoma in a 79-year-old woman: An exceptionally rare type of breast carcinoma. Rare Tumors. 2016;8:6650. doi: 10.4081/rt.2016.6650. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Paeng MH, Choi HY, Sung SH, Moon BI, Shim SS. Secretory carcinoma of the breast. J Clin Ultrasound. 2003;31:425–9. doi: 10.1002/jcu.10198. [DOI] [PubMed] [Google Scholar]
- 7.Hoda RS, Brogi E, Pareja F, Nanjangud G, Murray MP, Weigelt B, et al. Secretory carcinoma of the breast: Clinicopathologic profile of 14 cases emphasising distant metastatic potential. Histopathology. 2019;75:213–24. doi: 10.1111/his.13879. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Tognon C, Knezevich SR, Huntsman D, Roskelley CD, Melnyk N, Mathers JA, et al. Expression of the ETV6-NTRK3 gene fusion as a primary event in human secretory breast carcinoma. Cancer Cell. 2002;2:367–76. doi: 10.1016/s1535-6108(02)00180-0. [DOI] [PubMed] [Google Scholar]
- 9.Aktepe F, Sarsenov D, Özmen V. Secretory carcinoma of the breast. J Breast Health. 2016;12:174–6. doi: 10.5152/bs.2016.3249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Krausz T, Jenkins D, Grontoft O, Pollock DJ, Azzopardi JG. Secretory carcinoma of the breast in adults: Emphasis on late recurrence and metastasis. Histopathology. 1989;14:25–36. doi: 10.1111/j.1365-2559.1989.tb02111.x. [DOI] [PubMed] [Google Scholar]