

Abstract
There are multiple lesions in the jawbones with a common histological character of the presence of osteoclast-like giant cells under one category – giant cell lesions. The central giant cell granuloma (CGCG) is the most common of all and is found to be more prevalent in the Indian population. The pathogenicity still remains an enigma and needs to be differentiated from other look-alike lesions in order to have proper treatment planning. Furthermore, CGCG specifically needs to be differentiated from central giant cell tumor to avoid mutilating surgeries. This article is an attempt to give an outline of the CGCG with updating of the latest information on the perception of this lesion.
Keywords: Giant cells, granuloma, osteolytic lesion
INTRODUCTION
Giant cell granuloma and its related lesions in the jaw are grouped under single umbrella but with varied clinical behavior ranging from simple reactive to neoplasm sometimes even manifesting as aggressive malignant neoplasm. The ubiquitous presence of giant cells in many unrelated bone lesions further complicates differential diagnosis. The reactive secondary changes in the lesion, many a times give a pseudo picture of malignancy and it needs a great deal of expertise to recognize the basic nature of the lesion. That is why clinicopathological correlation taking into consideration of radiological findings and sometimes, the serumal evaluation is of utmost importance before reaching the final diagnosis, especially into diverse group of histologically overlapping giant cell entities.
The central giant cell granuloma (CGCG) was once thought to represent reactive lesion, however the unpredictable and sometimes occasionally aggressive behavior and because of its possible relationship to tumors of long bone and some syndromes, it is best classified as benign neoplasm.
CLINICAL FEATURES
The CGCG has a wide age range in its manifestations; however, two-thirds of the cases occur below the age of 30 years with a predilection for females atleast twice as common than the males. Both the jaws are affected and 80% are involving the region anterior to the first premolar and rarely noticed in the posterior segment. In general, CGCG is asymptomatic in the beginning but later becomes expansile. Multiple cases of CGCG have been reported in patients with mutations of the RAS/MAPK pathway, especially in syndromal cases.
RADIOGRAPHIC FEATURES
Sharply demarcated radiolucency sometimes extends between the displaced tooth roots. Few cases exhibit sclerotic margin denoting the slow expansile nature. Sometimes, faint calcifications are noticed depicting the poorly mineralized osteoid trabeculae within the lesion and this helps to differentiate from giant cell tumors. The roots are not resorbed, but the tooth may be lost due to lack of bony support. Larger lesions may exhibit multilocularity. The cortex generally is intact, but in more aggressive lesions, it may be breached.
HISTOPATHOLOGY
CGCG is a benign proliferation of fibroblasts and multinucleated giant cells that occur most exclusively in the jaws. The primary tumor cells of CGCG are fibroblasts. The secondary cells which are microscopically the most prominent are the multinucleated giant cells. Other accessory cells seen considerably smaller numbers are macrophages, dendrocytes and endothelial cells.
The fibroblasts make up the proliferative component of CGCG since they express the proliferative protein marker Ki67 which are indicative of the cells in the cell cycle.[1] The tumor fibroblasts are also believed to be responsible for the recruitment and retention of monocytes which subsequently transform to multinucleated giant cells.[1]
The key feature of the lesion is the presence of multinucleated giant cells that are unevenly distributed and form clearly recognizable clusters separated by scar-like stromal tissue. The giant cell and their clustering are particularly evident in areas of hemorrhage. There may be trabeculae of newly formed reactive bone on the periphery of the lesion. Sometimes, the bone formation may be extensive and obscure other elements of the lesion [Figure 1].
Figure 1.
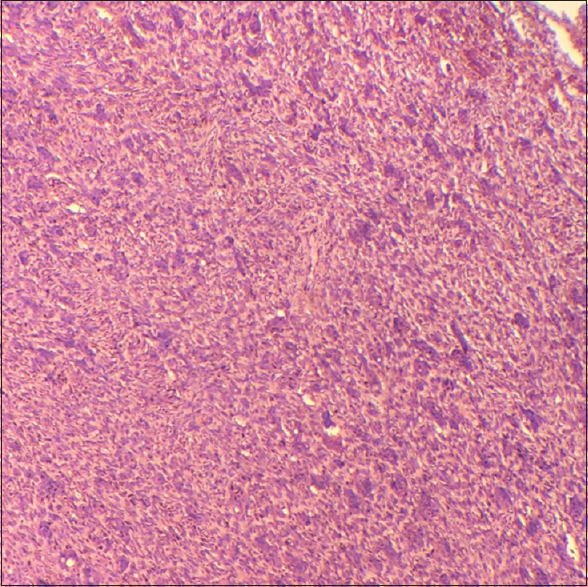
The histopathology showing irregularly distributed giant cells (H&E, ×10)
ULTRASTRUCTURAL FEATURES
Structurally, the giant cells that are present in the CGCG are very similar to giant cells in the giant cell tumor. However, the surrounding spindle-shaped stromal cells of CGCG are typically monofibroblastic differentiation, while in the tumor, the normal nuclear stromal cells show macrophage-like picture.[2] Since the stromal proliferative cells of CGCG show myofibroblastic differentiation, it is more appropriate to call this lesion as myofibroblastoma which will give the clarity of origin of the cell as well as benign behavior of the cell.
MOLECULAR ASPECTS
The mutation of H3F3A specifically PG34W or sometimes PG34L was shown to define giant cell tumor of bone and this mutation is not noticed in CGCG of the jaws. This factor can be used to differentiate between these two lesions which are always a point of confusion and controversy of these two lesions in the jaws. However, the whole-exon sequencing study done by Gomes et al. in 2020[1] showed mutation in KRAS, TRPV4 and FGFRI of CGCG which is histologically similar to the nonossifying fibroma of long bones. Similar mutations were also noticed in nonossifying fibroma. Hence, from the molecular point of view, CGCG seems to be more intimately related to nonossifying fibroma than to giant cell tumor of long bones.[1]
CYTOKINES AND OSTEOCLAST
The common finding of all the central giant cell lesions is that there is an osteoclastic overactivity, but the precise predisposing factor is yet unidentified, possibly the microenvironment of bone is altered so that outright development of giant cell lesion occurs.
There are many cytokines involved in affecting bone resorption.[3,4,5] Some may be stimulator, initiator, inhibitors or differentiation of the osteoclast-the bone-resorbing cell. The cytokines that stimulate the osteoclast are colony-stimulating factor, interleukin-1 (mediated by prostaglandin), tumor necrosis factor, transforming growth factor and interleukin-6 and the cytokines that inhibit osteoclast functions are lymphotoxins, interleukin-4 and interferons. These cytokines are produced by macrophages, stromal cells, endothelial cells or T lymphocytes, tumor cells, myeloma cells and sometimes even by the osteoblast themselves. In fact, there is evidence in plenty that indicated local factors generated in the microenvironment of bone-resorbing cells are much more powerful regulators of osteoclast function than by the hormones like parathyroid hormone, calcitonin secreted and sent in the blood circulation.[6]
As we expand our knowledge in understanding the role of these cytokines and the hormones in the pathologies that are related to bone-resorbing diseases be it local or systemic may help us to have better approach in the therapeutic value of these bone diseases. Hence, we need to work out to understand the role of cytokines, purifying the cloning factors produced by the osteoclast and to see how these cytokines interact with each other. Further, this can be tested in the laboratory by developing osteoclast and osteoblast cell lines.
DIFFERENTIAL DIAGNOSIS
CGCG should be differentiated from the brown tumor of hyperparathyroidism, giant cell tumor, nonossifying fibroma and other osteolytic lesions of the jawbones associated with giant cells histologically like cherubism, aneurysmal bone cyst and so on.
The hyperparathyroidism can be differentiated on the basis of biochemical tests, where hypercalcemia, hypophosphatasia and increased PTH will point toward hyperparathyroidism.
The giant cell tumor of long bones virtually will be difficult to differentiate, especially when the CGCG is of the aggressive type. The giant cell tumor shows larger giant cells, more in number of nuclei and generalized distribution of giant cells and absence of osteoid formation. But for all practical purpose, the occurrence of giant cell tumor in the jawbones is very rare and cases have been reported where patients are already suffering from Paget's disease.[2]
The nonossifying fibroma characteristically will show fibrohistiocytic stroma with storiform pattern and prominent xanthogranulomatous reaction. Other giant cells containing look alikes include aneurysmal bone cyst and cherubism, the former exhibit sinusoidal blood spaces within the tumor mass, while the cherubism is diagnosed on clinical grounds of bilateral involvement of the jaws with a family history and noticed in children.
TREATMENT
The first line of choice in treating CGCG is curettage and it is almost always curative. However, in large and aggressive lesions, especially in the growing facial skeleton where curettage is relatively mutilating in such cases, medical treatment with calcitonin and intralesional injection of steroids have been attempted.[7] It has been reported that the size and number of giant cells are reduced and the stroma becomes collagenous to be replaced gradually by lamellar bone. Interferon-alpha-2A has been suggested as additional treatment of CGCG on the basis of anti-angiogenic action.[7]
CONCLUSION
There is a significant advancement in the quest of understanding this enigmatic group of lesions. However, the pathogenesis is yet to be defined with authenticity also therapeutic trials has to be worked out especially, the inhibitors of osteoclastic activity.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
I acknowledge the 3rd year postgraduate students Dr. Jayarathi Ishwarya K S, Dr. Sruthi Chandra V and Dr. Sushmitha S for the literature search and clerical help.
REFERENCES
- 1.Gomes CC, Diniz MG, Bastos VC, Bernardes VF, Gomez RS. Making sense of giant cell lesions of the jaws (GCLJ): Lessons learned from next-generation sequencing. J Pathol. 2020;250:126–33. doi: 10.1002/path.5365. [DOI] [PubMed] [Google Scholar]
- 2.Rosenberg AE. Bone tumors. In: Howard D, editor. Dorfman and Bogdan Czerniak. St. Louis: Mosby; 1998. [Google Scholar]
- 3.Mundy GR. Role of cytokines in bone resorption. J Cell Biochem. 1993;53:296–300. doi: 10.1002/jcb.240530405. [DOI] [PubMed] [Google Scholar]
- 4.Roodman GD. Role of cytokines in the regulation of bone resorption. Calcif Tissue Int. 1993;53:S94–8. doi: 10.1007/BF01673412. [DOI] [PubMed] [Google Scholar]
- 5.Shrestha A, Marla V, Shrestha S, Neupane M. Giant cells and giant cell lesions of oral cavity – A review. Cumhuriyet Dent J. 2014;17:192–204. [Google Scholar]
- 6.Edwards PC. Insight into the pathogenesis and nature of central giant cell lesions of the jaws. Med Oral Patol Oral Cir Bucal. 2015;20:e196–8. doi: 10.4317/medoral.20499. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Regezi J, Sciubba J, Jordan R. Oral Pathology: Clinical-Pathologic Correlations. 4th ed. St Louis: WB Saunders; 2003. [Google Scholar]