

Abstract
Objectives:
To evaluate the efficacy of double-filtration plasmapheresis (DFPP) treatment of myasthenia gravis (MG) through a systematic review and meta-analysis.
Methods:
PubMed, Cochrane Library, Embase, China National Knowledge Infrastructure (CNKI), Chinese Scientific Journals Database (VIP), and Wanfang databases were searched for randomized controlled trials (RCTs) and clinical controlled trials (CCTs) on DFPP for MG from database establishment to June 2019. Two researchers independently screened the articles, extracted the data, and cross checked the results. RevMan 5.3 was used for statistical analyses.
Results:
Seven RCTs and 2 CCTs were found comprising 329 patients. The results showed that clinical MG remission rate after DFPP treatment was significantly higher (OR = 4.33; 95% confidence interval [CI], 1.97–9.53; P < .001) and the serum levels of antititin antibody was significantly decreased (standardized mean difference [SMD] = 9.30; 95% CI, 7.51–11.08; P < .001). In addition, the quantitative MG (QMG) score, hospital stay and time to remission of MG symptoms, and acetylcholine receptor antibody (AchRAb) decreased in the DFPP treatment group; however, these outcomes had high heterogeneity among the studies. Only one study has reported on the adverse effects, including hypotension and hematoma.
Conclusion:
This meta-analysis suggests that DFPP can be recommended for the short-term mitigation of MG. Because our review was limited by the quantity and quality of the included studies, the above conclusions should be verified by additional high-quality studies.
Keywords: double-filtration plasmapheresis, myasthenia gravis, plasma exchange
1. Introduction
Myasthenia gravis (MG) is an autoimmune disease in which antibodies bind to acetylcholine receptor (AchR) or to functionally related molecules in the postsynaptic membrane at the neuromuscular junction.[1] The disease is characterized by fluctuating muscle weakness and abnormal fatigability.[2] Current therapeutic options for MG are acetylcholinesterase inhibitors; glucocorticoids (GC); intravenous immunoglobulin (IVIg); plasma exchange (PE); thymectomy; monoclonal antibodies; and immunosuppressive agents.[3]
PE is appropriately used as a short-term treatment for MG patients who have life-threatening signs, such as respiratory insufficiency or dysphagia.[4] The PE procedure consists of filtering venous blood and removing plasma constituents, including normal and pathogenic immunoglobulins, after which the removed plasma is usually replaced with fresh-frozen plasma or albumin.[5] PE has been shown to induce a rapid recovery, corresponding to the decline in acetylcholine receptor antibody (AchRAb)[6]; however, this treatment comes with many complications,[7–9] such as allergic reactions, sepsis, and affecting the blood's ability to coagulate. In recent years, newly developed techniques for plasmapheresis, including double-filtration plasmapheresis (DFPP)[10] and immunoadsorption (IA),[11] have provided more selective removal of pathogenic substances without the need for plasma supplementation. DFPP consists of a first filter to separate plasma from blood (a plasma separator) and a second filter to separate albumin from larger molecules, such as immunoglobulins, immune complexes, and lipoproteins, in the plasma (a plasma fractionator).[12]
The systematic review and meta-analysis of DFPP treatment for MG is lacking; therefore, the purpose of this study was to systematically and objectively evaluate the efficacy and safety of DFPP in the treatment of MG using evidence-based medicine to provide a reference for clinical decision making.
2. Methods
2.1. Search strategy
A computer search of PubMed, Cochrane Library, Embase, CNKI, Vip, and Wanfang databases was conducted to locate all clinical research articles on DFPP treatment of MG from the time of database establishment to June 2019. In the database search, the following subject words and free words were combined for full text retrieval: (myasthenia gravis) or (myasthenia gravis, ocular) or (ocular myasthenia gravis) or (myasthenia gravis, generalized) or (generalized myasthenia gravis) and (double filtration plasmapheresis) or DFPP.
2.2. Selection criteria
2.2.1. Types of studies
We searched for randomized controlled trials (RCTs) and quasi-randomized trials (clinical controlled trial [CCTs]) on DFPP treatment of MG, which involved clinical studies on groups of patients divided according to the type of intervention in any form in Chinese or English.
2.2.2. Participants
Patients with MG that was confirmed by clinical manifestations, a neostigmine test, neuroelectrophysiological examination, and detection of AChRAb were included in the studies.
2.2.3. Interventions
Patients who had been treated with DFPP.
2.2.4. Comparator
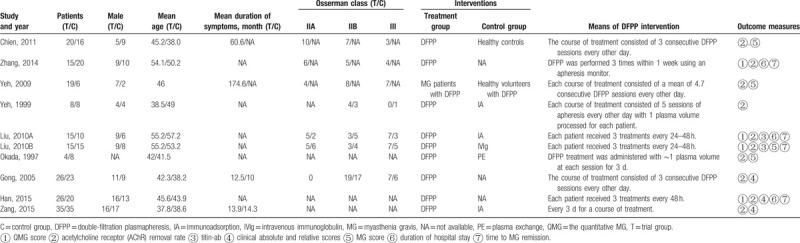
The control groups were healthy volunteers treated with DFPP or MG patients treated with IVIG, PE, or IA, as shown in Table 1.
Table 1.
Demographic and clinical characteristics of the myasthenia gravis patients included in the study.
2.2.5. Outcomes
The primary outcome was clinical efficacy rate during the treatment period.
The secondary outcomes were reduced quantitative MG (QMG) score, rate of adverse reactions and number of respiratory supports, duration of hospital stay, time to MG remission, serum antibody levels.
2.3. Exclusion criteria
The exclusion criteria were as follows: animal experiments or in vitro studies, the original data could be extracted, and the effective data could not be obtained by contacting the author, case reports, reviews, or meta-analyses; or repeated publication of the articles.
2.4. Data extraction and quality assessment
Two researchers (PL and MM) independently screened the articles, extracted the data, and cross checked the information. When there was disagreement, a third researcher was used to help resolve the issue. Any lack of data was supplemented as much as possible by contacting the author. Standardized data extraction tables were adopted to extract information from eligible articles. The extracted data included the following information: basic: the first author and the year of publication; basic subject characteristics: sample size, age, course of disease, MG severity (Osserman classification); intervention content: intervention measures and DFPP implementation time; and outcome measurement.
The evaluation of the methodological quality of the studies included random sequence generation, allocation concealment, patient blinding, observer blinding, incomplete outcome data, selective reporting, and other bias.[13]
2.5. Statistical analyses
Review Manager (RevMan 5.3) provided by Cochrane Collaboration Network (https://us.cochrane.org/) was used for statistical analyses. Measurement data were evaluated using the weighted mean difference (WMD) or SMD. The heterogeneity among the studies was tested using the Q value and I2 value.
If P ≥ .1 and I2 ≤ 50%, there was no heterogeneity among the studies and the fixed effects model was used for analyses; if P < .1 or I2 > 50%, there was heterogeneity among the studies and the random effects model was used for analyses. If the data from each study could not be analyzed by meta-analysis, descriptive analyses were used. The data for continuous variables were summarized by the mean ± standard deviation, and dichotomous outcomes were calculated using the risk ratio (RR). The results were expressed as the 95% confidence interval (95% CI). Subgroup analyses were used to find the source of heterogeneity, and sensitivity analyses were used to evaluate whether the results of the meta-analysis were stable and reliable, if appropriate. P < .05 was considered a significant difference.
2.6. Ethical approval
This study did not involve ethical approval or informed consent of patients because we did not recruit patients. We integrated and analyzed the data from research papers.
3. Results
3.1. Study selection and characteristics
Using the above retrieval strategies, 585 papers were found, with 571 remaining after removing duplicates. Of these, 539 were excluded after reading the title and abstract. Of the remaining 32 papers, 9 (7 RCTs and 2 CCTs)[12,14–20,22] were included after reading the full text. The screening process for this meta-analysis is provided in Fig. 1. The 9 studies comprised 329 patients. The basic features of the included papers are provided in Table 1.
Figure 1.
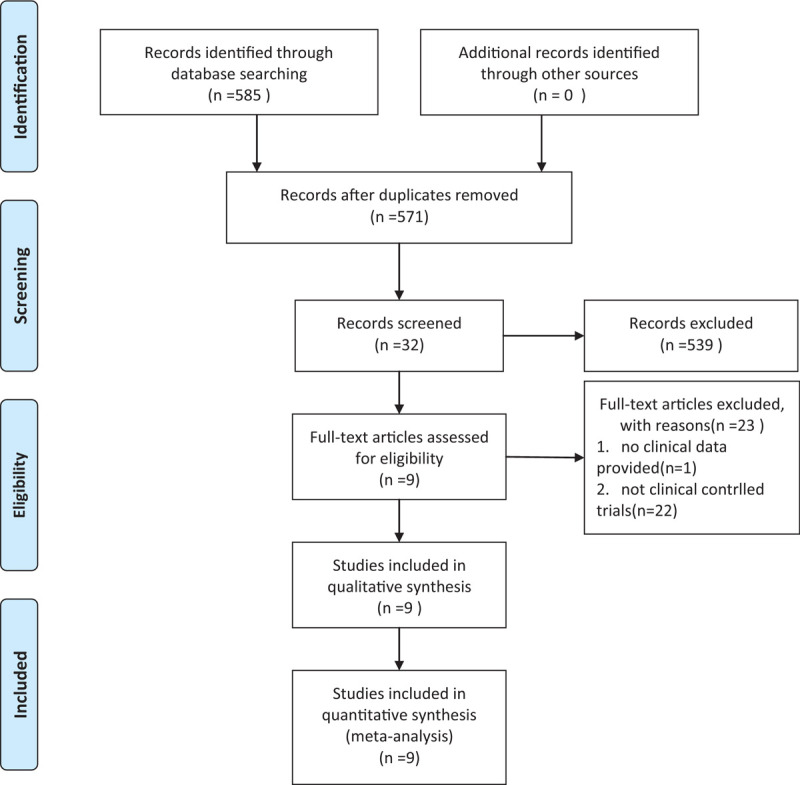
Screening process for this meta-analysis.
3.2. Risk of bias and study quality
The quality of the studies was assessed using the Cochrane recommended tool for assessing the risk of bias (Fig. 2).
Figure 2.
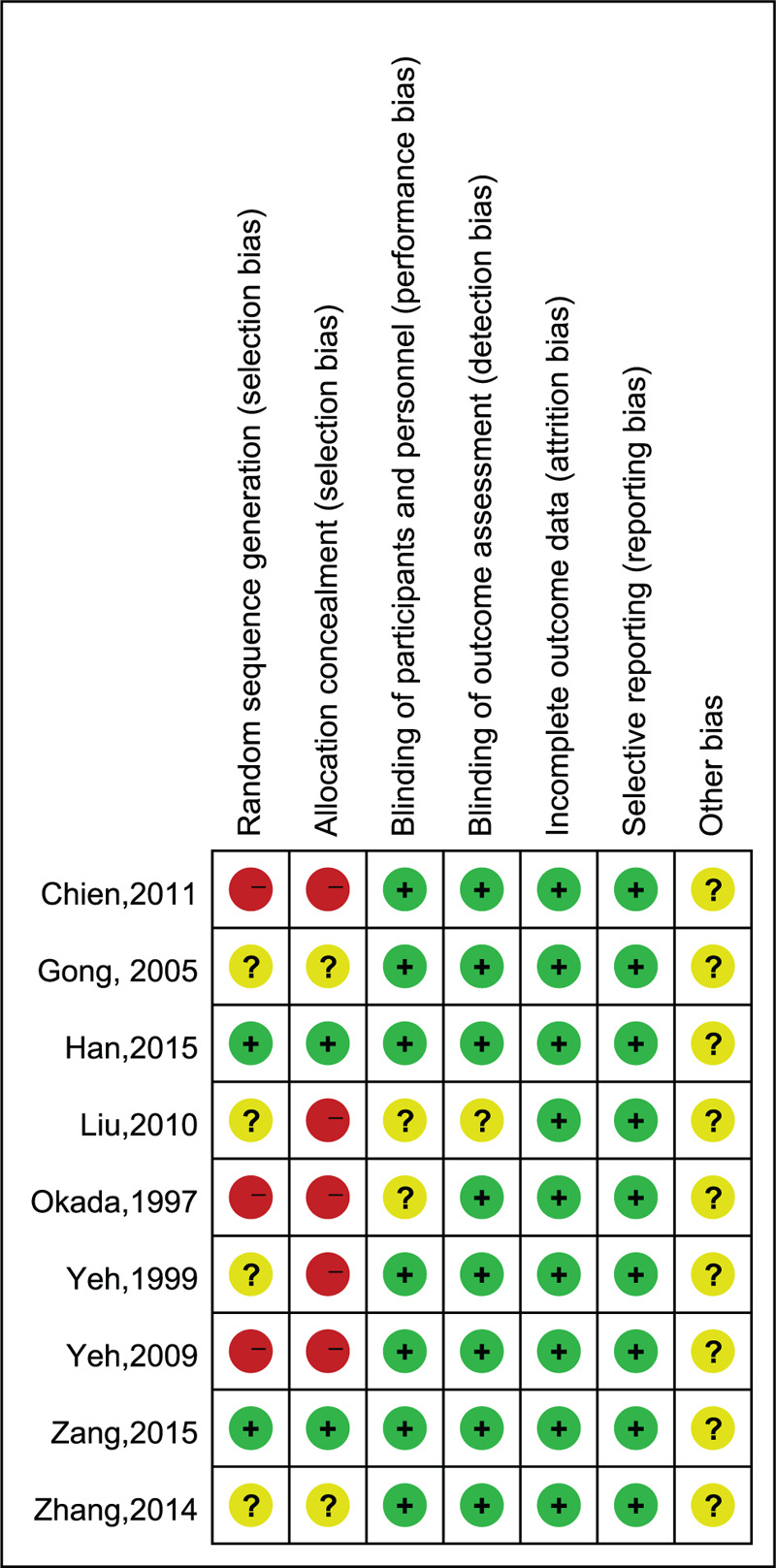
Risk of bias summary based on the review authors’ judgement for each included study.
3.3. Primary outcome measures
3.3.1. Clinical efficacy rate
The relative score, calculated as follows:
was used to evaluate the therapeutic efficacy. A relative score of ≥95% was considered to be full recovery, 80% to 95% partial recovery, 50% to 80% partially effective, 25% to 50% improved, and ≤25% ineffective. Clinically effective was defined as relative scores above 25%. Clinically effective was defined as relative scores above 25%.[21] Five studies[22,15–18] comprising 192 patients reported the clinical efficacy rate of DFPP treatment for MG. The clinical MG remission rate after DFPP treatment was not heterogeneous among the study groups (P = .59, I2 = 0%). Analyses using the fixed effects model showed that the clinical MG remission rate after DFPP treatment was significantly higher than that in the control group (OR = 4.33; 95% CI, 1.97–9.53; P = .0003), as shown in Fig. 3.
Figure 3.
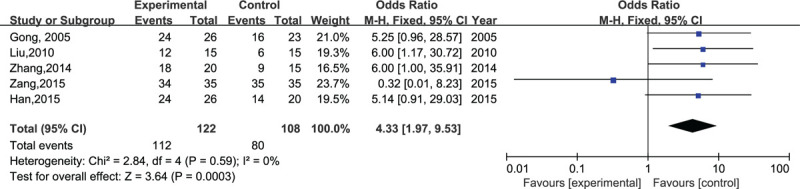
Clinical efficacy rate after double-filtration plasmapheresis treatment.
3.4. Secondary outcome measures
3.4.1. QMG score descent range
Three studies[14,16,22] comprising 136 patients reported the QMG score descent range in MG. The QMG score descent range after DFPP treatment was heterogeneous among each study group (P < .01, I2 = 99%). Analyses using the random-effects model showed that this score was significantly higher than that of the control group (MD = 37.64; 95% CI, 36.33, 38.95; P < .01), as shown in Fig. 4.
Figure 4.

Descent range of the quantitative myasthenia gravis score after double-filtration plasmapheresis treatment.
3.4.2. Serum antibody removal rate
Serum antibody removal rate was calculated as follows:
The AChRAb removal rate was evaluated in 7 studies[12,14–18,22] comprising 275 patients. After the heterogeneity test, the random effects model was used to analyze the results (P < .01, I2 = 100%). The combined MD was 18.86 (95% CI, 1.17–36.55; P = .04), as shown in Fig. 5.
Figure 5.
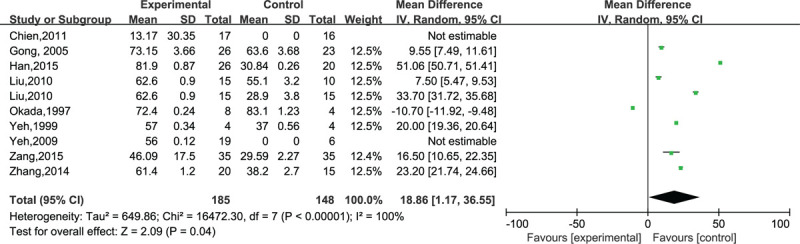
Acetylcholine receptor antibody levels after double-filtration plasmapheresis treatment.
Two studies[16,22] comprising 65 patients evaluated the serum levels of the removal rate of antititin antibody. After the heterogeneity test, the random effects model was used to analyze the results (P = .20, I2 = 39%). The combined SMD was 9.30 (95% CI, 7.51–11.08; P < .01). The results showed that the serum levels of anti-AChR-ab and anti-titin antibody significantly decreased after DFPP treatment (P < .05), as shown in Fig. 6.
Figure 6.

Serum levels of anti-titin antibody after double-filtration plasmapheresis treatment.
3.4.3. Duration of hospital stay (day)
Three studies[16,17,22] comprising 136 patients were evaluated for the duration of hospital stay. Random effects model analyses (P < .01, I2 = 99%) showed that the duration of hospital stay for MG patients after DFPP treatment was significantly decreased (MD = –5.71; 95% CI, –8.30 to –3.12; P < .01), as shown in Fig. 7.
Figure 7.

Duration of hospital stay for myasthenia gravis patients after double-filtration plasmapheresis treatment.
3.4.4. Time to MG remission (day)
Three studies[16,17,22] comprising 136 patients evaluated the time to MG remission. Random effects model analyses (P < .001, I2 = 100%) showed that the time to MG remission after DFPP treatment was significantly decreased (MD = –3.50; 95% CI, –7.62–0.61; P < .01), as shown in Fig. 8.
Figure 8.

Time to myasthenia gravis remission after double-filtration plasmapheresis treatment.
3.5. Safety evaluation
Only one study[22] has reported any adverse effects. In 15 patients with MG, 3 had adverse reactions during DFPP treatment that comprised hypotension (2), and hematoma (1).
4. Discussion
4.1. Summary of main results
In this study, the efficacy and safety of DFPP treatment for MG from 7 RCTs and 2 CCTs comprising 329 patients were evaluated by meta-analysis. The results showed that the clinical MG remission rate after DFPP treatment was significantly higher and the serum levels of antititin antibody significantly lower. In addition, the results showed that compared with the control group, the QMG score in the DFPP treatment group significantly decreased, hospitalization time and time to remission of MG symptoms decreased, anti-AChR antibody levels decreased; however, these outcomes had high heterogeneity among the studies. Only one study reported adverse events, which were fewer than those in the control group and the symptoms were mild. A possible mechanism underlying the effect of DFPP on MG is the alleviation of symptoms by reducing the pathogenic antibodies to MG; therefore, current research results support the recommendation of DFPP as a routine treatment option for short-term mitigation of MG.
4.2. Interpretation of the results
Treatment paradigms for MG include therapies such as intravenous immunoglobulin and therapeutic plasma exchange.[23,24] The administration of IVIg is convenient and safe, with few complications, but the price is very high.[25]
PE is an accepted, effective therapy for some patients with MG[14]; however, the major drawbacks of plasma exchange are the need for plasma supplements and the possible risk of allergic reactions and transfusion-related infection.[26]
New techniques for PE include IA and DFPP. IA uses an affinity adsorbent of tryptophan-linked polyvinyl alcohol gel that selectively adsorbs most large proteins, including most AchRAb, through hydrophobic interactions.
DFPP is a relatively selective plasma-separation method that transfers the blood through 2 filtration membranes of different pore sizes, and separates and discards pathogenic high molecular-weight substances, plasma albumin, and other physiological substances to selectively remove or reduce pathogenic substances in the patient's blood. In recent years, several of the complications of DFPP have been overcome, and this method has been widely used in clinics to treat autoimmune diseases. Because of the need for indwelling central venous catheters during DFPP treatment and anticoagulant therapy, it is also possible to increase the associated wind risk, such as infection, thrombus, and bleeding.[27]
In this study, the efficacy and safety of DFPP treatment of MG were evaluated by meta-analysis. The results showed that DFPP treatment of MG is 91% effective, which confirms the rationale of DFPP treatment for this disease. As for the mechanism by which DFPP treatment affects MG, the current research results focus mostly on its clearance of the pathogenic autoantibodies in circulating blood to correct immune disorders, alleviate MG symptoms. In view of the advantages of the short-term clinical efficacy of DFPP treatment, this choice of treatment is important for patients, especially for severe or critical MG, for which the clinical symptoms must be alleviated. The results showed that compared with the control group, the QMG score of the DFPP treatment group significantly decreased, and that hospitalization time and the time for remission of MG symptoms also decreased.
The QMG scores[28] are used mainly to assess the extent of MG and muscle weakness. Several studies[14,16,22] have shown that DFPP treatment could significantly improve the endpoints, including the QMG scores. Yeh et al[29,30] have reported that a better response in patients with an age at onset <40 years was associated with a higher QMG score and that the QMG score decreased in all courses in ≤3 months after DFPP. Chien et al[31] have reported that after 1 course of DFPP treatment, the reduced clinical QMG score was correlated with a decrease in the percentage of T-cells. In this study, the QMG score descent range after DFPP treatment of MG significantly increased over that in the control group. MG symptoms were significantly relieved, and MG remission time and hospital stay were significantly reduced.
Anti-AChRAb is a classic autoantibody for MG. The binding of antibodies to the postsynaptic membrane at the neuromuscular junction accelerates antigen regulation by internalization, destroys postsynaptic membrane by activating complements, or blocks the binding to ACHR. This affects the normal conduction of neuromuscular signals, resulting in trigger symptoms such as skeletal muscle weakness and muscle paralysis. In addition, autoimmune antibodies against presynaptic membrane (PrsmR) and titin reportedly compromise neuromuscular transmission, which leads to skeletal muscle weakness.[32,33]
Titin is a major antigenic determinant for cross-striational antibodies. Titin antibodies are found in the sera of 85.7% of MG patients with thymoma (all age groups) and in 58% of nonthymomatous MG with late-onset and detectable AChR-ab.[34] Recent studies have shown that AChR-ab titers are not associated with the clinical manifestations of late-onset MG, but that anti-titin antibodies is associated with the severity of the disease.[35] Romi et al[36] have shown that titin antibodies occurred only in the IgG 1 and IgG 4 subclasses and mean total IgG and IgG 1 titin antibody titers decreased during long-time patient observation together with improvement in the MG symptoms. The results showed that AChR-ab and titin-ab in MG patients significantly decreased after DFPP treatment. The results are highly heterogeneous, which might be the result of the small sample sizes of the including studies, the different proportions of autoantibody-positive samples in the baseline data, or the nonuniform methods of antibody detection. Limited by the quantity and quality of the included studies, the above conclusions need to be verified by more high-quality studies.
5. Conclusions
The meta-analysis and systematic review supply evidence that DFPP treatment can effectively eliminate autoantibodies and has a definite clinical effect on MG patients. It may also significantly reduce AChRAb levels, QMGS, duration of hospital stay, and time to MG remission. DFPP treatment may be a beneficial option for treating MG.
5.1. Implications for practice
The use of DFPP to treat MG has increased over the past few decades; however, the choice of DFPP use is empirical and lacks consensus among doctors. This study found that DFPP can effectively improve MG symptoms within a short period of time.
5.2. Implications for research
In future randomized or nonrandomized prospective studies, a stratified design study will be conducted for the different positive conditions of autoantibodies. There is no international consensus and no implementation criteria; therefore, the treatment methods implemented by each institute were slightly different. We recommend that large-scale, in-depth RCTs be conducted on the different plasma volume, treatment times, treatment intervals, and the safety of different sites of intravascular catheterization by central venous puncture for DFPP in critically ill patients.
5.3. Study limitations
There were several limitations to our study as follows:
-
(1)
Most of the included studies did not describe specific stochastic methods, allocation hiding, and blinding methods; therefore, there could be bias in implementation and measurements.
-
(2)
Only Chinese and English studies were included, and no other languages and gray studies were included; therefore, there could be publication bias.
-
(3)
Outcome indicators were scattered, and each outcome indicator involved few studies, which could have affected the accuracy of the results.
-
(4)
In the DFPP treatment of MG, the effects of different courses of treatment and blood filtration volume need to be more fully analyzed.
-
(5)
None of the 9 studies included in this study mentioned whether patients were tested for Musk antibodies. In the future, randomized controlled trials will be needed to prove the efficacy of DFPP treatment in Musk-positive patients need.
-
(6)
Only one study reported the side effects of DFPP and there was insufficient evidence for a meta-analysis.
Author contributions
Data curation: Peng Liu, Mei Ma.
Formal analysis: Hongxia Yang.
Methodology: Hongxia Yang.
Project administration: Guoyan Qi.
Validation: Guoyan Qi.
Writing – original draft: Chaoying Liu.
Writing – review & editing: Chaoying Liu.
Footnotes
Abbreviations: AchRAb = acetylcholine receptor antibody, CCT = clinical controlled trial, DFPP = double-filtration plasmapheresis, MG = myasthenia gravis, OR = odds ratio, QMG = quantitative MG, RCT = randomized controlled trial, SMD = standardized mean difference.
How to cite this article: Liu C, Liu P, Ma M, Yang H, Qi G. Efficacy and safety of double-filtration plasmapheresis treatment of myasthenia gravis: a systematic review and meta-analysis. Medicine. 2021;100:17(e25622).
This work was supported by financial grants from the Shijiazhuang Science and Technology Bureau Foundation (Grant no. 171461553/151461303) and Key Research of Medical Science Research of Hebei Province, China (Grant no. 20170981).
The authors have no conflicts of interest to disclose.
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
- [1].Gilhus NE. Myasthenia gravis. N Engl J Med 2016;375:2570–81. [DOI] [PubMed] [Google Scholar]
- [2].Wang WW, Hao HJ, Gao F. Detection of multiple antibodies in myasthenia gravis and its clinical significance. Chin Med J (Engl) 2010;123:2555–8. [PubMed] [Google Scholar]
- [3].García-Carrasco M, Escárcega RO, Fuentes-Alexandro S, et al. Therapeutic options in autoimmune myasthenia gravis. Autoimmun Rev 2007;6:373–8. [DOI] [PubMed] [Google Scholar]
- [4].Sanders DB, Wolfe GI, Benatar M, et al. International consensus guidance for management of myasthenia gravis. Neurology 2016;87:419–25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Guptill JT, Juel VC, Massey JM, et al. Effect of therapeutic plasma exchange on immunoglobulins in myasthenia gravis. Autoimmunity 2016;49:472–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Kuks JB, Das PC. Plasma exchange in myasthenia gravis. Int J Artif Organs 1998;21:188–91. [PubMed] [Google Scholar]
- [7].Liew WKM, Powell CA, Sloan SR, et al. Comparison of plasmapheresis and intravenous immunoglobulin as maintenance therapies for juvenile myasthenia gravis. JAMA Neurol 2014;71:575–80. [DOI] [PubMed] [Google Scholar]
- [8].Alipourfaz A, Shojaei M, Peyvandi H, et al. A comparison between IVIG and plasma exchange as preparations before thymectomy in myasthenia gravis patients. Acta Neurologica Belgica 2016;117:01–5. [DOI] [PubMed] [Google Scholar]
- [9].Mandawat A, Kaminski HJ, Cutter G, et al. Comparative analysis of therapeutic options used for myasthenia gravis. Ann Neurol 2010;68:797–805. [DOI] [PubMed] [Google Scholar]
- [10].Agishi T, Kaneko I, Hasuo Y, et al. Double filtration plasmapheresis. Trans Am Soc Artif Intern Organs 1980;26:406–11. [PubMed] [Google Scholar]
- [11].Yamazaki Z, Fujimori Y, Takahama T, et al. Efficiency and biocompatibility of a new immunosorbent. Trans Am Soc Artif Intern Organs 1982;28:318–23. [PubMed] [Google Scholar]
- [12].Yeh JH, Chiu HC. Optimal volume of processed plasma and total number of selective plasmapheresis sessions in the treatment of patients with severe generalized myasthenia gravis. J Clin Apher 1999;14:177–80. [DOI] [PubMed] [Google Scholar]
- [13].The Cochrane Collaboration, Higgins JPT, Altman DG. Higgins JPT, Green S. Chapter 8: assessing risk of bias in included studies. Cochrane Handbook for Systematic Reviews of Interventions Version 5. 1. 0 [Updated March 2011] 2011. [Google Scholar]
- [14].Okada H, Moriwaki K, Sugahara S, et al. Comparative study of clinical effects between plasma adsorption and double filtration plasmapheresis in patients with myasthenia gravis. Ther Apher 1997;1:343–7. [DOI] [PubMed] [Google Scholar]
- [15].Gong J, Wang L. Clinical observation of 26 cases of myasthenia gravis treated by DFPP combined with methylprednisolone. Shandong Med J 2005;45:40. [Google Scholar]
- [16].Zhang L, Liu J, Wang H, et al. Double filtration plasmapheresis benefits myasthenia gravis patients through an immunomodulatory action. J Clin Neurosci 2014;21:1570–4. [DOI] [PubMed] [Google Scholar]
- [17].Han Q, Sha P, Wang YF. Double filtration plasmapheresis combined with glucocorticoid treatment for myasthenia gravis: symptom remission and variation of immune antibodies. Chin J Tissue Eng Res 2015;19:1228–32. [Google Scholar]
- [18].Zang WJ. Clinical study of ia in the treatment of generalized myasthenia gravis. China Foreign Med Treat 2015;29:07–8. [Google Scholar]
- [19].Chien PJ, Yeh JH, Chiu HC, et al. Inhibition of peripheral blood natural killer cell cytotoxicity in patients with myasthenia gravis treated with plasmapheresis. Eur J Neurol 2011;18:1350–7. [DOI] [PubMed] [Google Scholar]
- [20].Yeh JH, Wang SH, Chien PJ, et al. Changes in serum cytokine levels during plasmapheresis in patients with mg. Eur J Neurol 2009;16:1318–22. [DOI] [PubMed] [Google Scholar]
- [21].Xiuyun W, Xianhao X, Hong S. A clinical absolute and relative score system for myasthenia gravis. Chin J Neurol 1997;30:87–90. [Google Scholar]
- [22].Liu JF, Wang WX, Xue J. Comparing the autoantibody levels and clinical efficacy of double filtration plasmapheresis, immunoadsorption, and intravenous immunoglobulin for the treatment of late-onset myasthenia gravis. Ther Apher Dial 2010;14:153–60. [DOI] [PubMed] [Google Scholar]
- [23].Sanders DB, Guptill JT. Myasthenia gravis and Lambert-Eaton myasthenic syndrome. Continuum (Minneap Minn) 2014;20:1413–25. [DOI] [PubMed] [Google Scholar]
- [24].Lagoumintzis G, Zisimopoulou P, Kordas G, et al. Recent approaches to the development of antigen-specific immunotherapies for myasthenia gravis. Autoimmunity 2010;43:436–45. [DOI] [PubMed] [Google Scholar]
- [25].Cojocaru M, Cojocaru IM, Negres S, et al. Intravenous immunoglobulin therapy in neurological disease. Farmacia 2011;59:737–41. [Google Scholar]
- [26].Dodd RY. The risk of transfusion-transmitted infection. N Engl J Med 1992;327:419–21. [DOI] [PubMed] [Google Scholar]
- [27].Yeh JH, Chiu HC. Coagulation abnormalities in serial double-filtration plasmapheresis. J Clin Apher 2010;16:139–42. [DOI] [PubMed] [Google Scholar]
- [28].Barohn RJ, McIntire D, Herbelin L, et al. Reliability testing of the quantitative myasthenia gravis score. Ann N Y Acad Sci 1998;13:769–72. [DOI] [PubMed] [Google Scholar]
- [29].Yeh JH, Chiu HC. Double filtration plasmapheresis in myasthenia gravis - analysis of clinical efficacy and prognostic parameters. Acta Neurol Scand 1999;100:305–9. [DOI] [PubMed] [Google Scholar]
- [30].Yeh JH, Chen WH, Chiu HC. Predicting the course of myasthenic weakness following double filtration plasmapheresis. Acta Neurol Scand 2003;108:174–8. [DOI] [PubMed] [Google Scholar]
- [31].Chien PJ, Yeh JH, Shih CM, et al. A decrease in the percentage of cd3+ cells is correlated with clinical improvement during plasmapheresis in patients with myasthenia gravis. Artif Organs 2013;37:211–6. [DOI] [PubMed] [Google Scholar]
- [32].Vincent A, Bowen J, Newsom-Davis J, et al. Seronegative generalised myasthenia gravis: clinical features, antibodies, and their targets. Lancet Neurol 2003;2:99–106. [DOI] [PubMed] [Google Scholar]
- [33].Romi F, Gilhus NE, Aarli JA. Myasthenia gravis: clinical, immunological, and therapeutic advances. Acta Neurol Scand 2005;111:134–41. [DOI] [PubMed] [Google Scholar]
- [34].Aarli JA, Romi F, Skeie GO, et al. Myasthenia gravis in individuals over 40. Ann N Y Acad Sci 2003;998:424–31. [DOI] [PubMed] [Google Scholar]
- [35].Skeie GO, Aarli JA, Gilhus NE. Titin and ryanodine receptor antibodies in myasthenia gravis. Acta Neurol Scand Suppl 2006;183:19–23. [DOI] [PubMed] [Google Scholar]
- [36].Romi F, Skeie GO, Vedeler C, et al. Complement activation by titin and ryanodine receptor autoantibodies in myasthenia gravis. A study of IgG subclasses and clinical correlations. J Neuroimmunol 2000;111:169–76. [DOI] [PubMed] [Google Scholar]