

Abstract
Background: Renal cyst is a common benign disease which is rare to progress from simple renal cyst to renal cell carcinoma. Case presentation: A 62-year-old woman who suffered a simple renal cyst for over 20 years complained intermittent lumbar in recent 2 years. At her latest admission, the cyst lesion displayed enhancement in the cystic wall by CT scan and cystic to partially solid change by ultrasound, so we did a partial nephrectomy and found that the cystic lesion had become a cyst-solid transition. The pathology turned out to be renal clear cell carcinoma. Conclusions: Although the canceration of a renal cyst is a small probability event, patients with a long history of a cyst, especially those with symptoms, need to seek for medical treatment in time, and if necessary, lesion biopsy or resection may be under consideration.
Keywords: Renal cyst, renal cancer, evolution, case report
Introduction
The kidney is a frequent site of cysts, and about 40% of patients who have an imaging examination are diagnosed with renal cyst [1]. There are many reasons for the formation of a renal cyst. At present, the main recognized factors are: congenital dysplasia, gene mutation, various infections, and toxin damage [1,2]. Renal cyst can express differently in numbers and volume. According to the features of cysts, they can be divided into simple cysts, multilocular cysts, and multiple cysts. Among them, simple renal cyst is the most common renal cystic disease. In most cases, renal cysts are asymptomatic and rarely malignant. Under some conditions, the growth pattern of renal cysts becomes more aggressive over time.
Cyst aggressiveness generally does not involve malignancy; they are mostly benign growths, showing changes in quantity and volume rather than malignant lesions [2]. In rare conditions, such as intracapsular hemorrhage or infection [3], they become more challenging and complex in the content of cysts. Cancer is then 3x more likely [4,5]. In this condition, some patients or doctors generally let down their vigilance so progression is easy, evento the late stage of renal carcinoma. Therefore, we hope that we draw some attention to the patients with symptomatic simple cysts or benign cystic lesions by this case report, so as to avoid or reduce the chance of malignant progression.
Case presentation
A 62-year-old woman with intermittent lumbago for 10 days visited our outpatient department. Positive physical examination showed percussion pain in the left renal area. The patient had a renal-cyst history for over 20 years. Two years ago, the patient was hospitalized in the local hospital and complained with intermittent lumbago. The admission examination with ultrasound showed a renal cyst with intracapsular hemorrhage (33*26 mm) (April, 2018; Figure 1A). The symptom was reduced by some painkillers under medical advice and regular follow-up was suggested. Three months later, the patient with no symptoms went for a return visit and CT scan showed the cystic lesion was smaller than before (21*18 mm) (July, 2018; Figure 1B); kidney function tests and tumor biomarkers were within the normal range. One year ago, the patient went for another return visit and the ultrasound showed that the size of the cyst was 11*14 mm (April, 2019; Figure 2A). Considering the long history of renal cystic lesion and the altered clinical features within the recent two years, the possibility of malignant transformation couldn’t be ruled out and the patient was admitted to our department.
Figure 1.
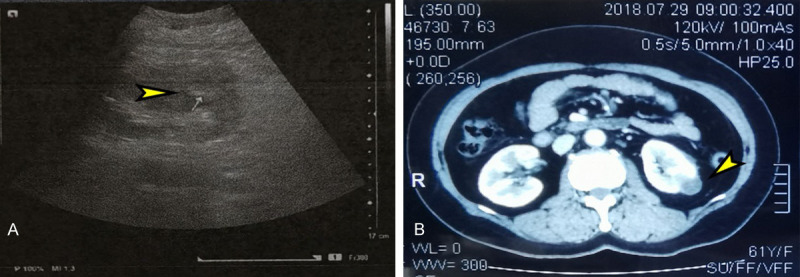
Imaging results showed benign cystic changes. A. Ultrasound: Renal cyst of left kidney: intra-cystic hemorrhage. B. CT scan (enhanced): Cystic lesion of left kidney.
Figure 2.
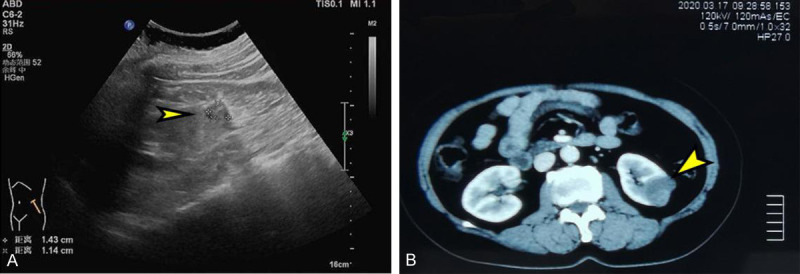
Imaging results showed non-benign features. A. Ultrasound: Cystic lesion of left kidney. B. CT scan (enhanced): Cystic lesion of left kidney.
Admission medical imaging examination: CT scan showed a left renal cystic lesion was detected (35*30 mm) (March, 2020; Figure 2B); CT displayed that the density of cysts was not uniform and a partially enhanced lesion was observed within the cyst. Ultrasound examination showed some part of a cystic lesion (33*28 mm) (March, 2020; Figure 3A) was undergoing cystic-solid transition. By admission laboratory examination kidney function tests and tumor biomarkers were within the normal range.
Figure 3.

Cystic degeneration is characterized by malignancy. A. Ultrasound: cystic-solid lesion of left kidney. B. Postoperative gross specimen: Pathologic changes of cystic-solid features.
Considering that the patient’s cyst lesion was at least classified as Bosniak IIF, there is a high risk of canceration, so we adopted surgical treatment for this patient. Laparoscopic partial nephrectomy was performed for the patient and the size of mass located in the middle and lower part of the left kidney, which is obviously adherent to the surrounding renal tissue. Postoperative gross specimen showed: The size of the mass was 4.5*2.3*2.3 cm and the thickness of the wall was 0.1-0.2 cm (Figure 3B). The excised tumor was sent for pathologic examination. The pathology report showed: The cancer cells with small and round nuclei are round and transparent and there was cytoplasmic red staining of some cancer cells. The cancer cells were arranged in papillary formations, nests, and tubular glands (H&E staining ×100). Immunohistochemisty: CK (pan) (+), CD10 (partially+), Ksp-Cadherin (+), CK7 (-) , P504s (+), Ki-67 (10% +), P53 (-), Vimentin (+). This was consistent with the diagnostic characteristics of renal clear cell carcinoma (Figure 4). The patient recovered completely in 7 days after operation and was discharged. The patient was followed up for half a year, and there was no obvious recurrence indication. As of September, the lab examinations and physical signs of the patient had no obvious abnormality.
Figure 4.
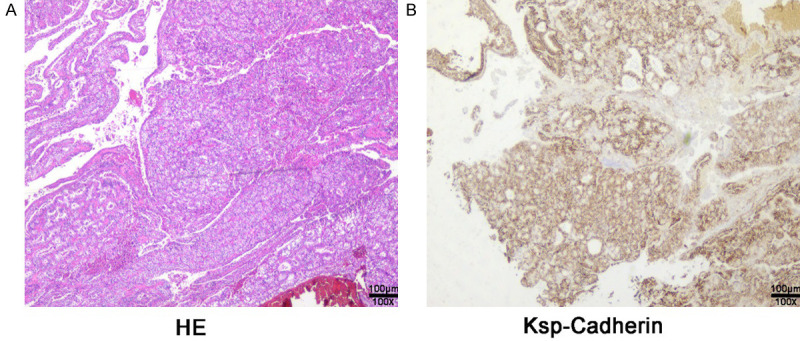
Pathology report: clear renal cell carcinoma. A. Hemotoxylin and eosin (H&E) stain of the renal lesions showed cells with small and round nuclei with cytoplasm that was round and transparent (100×). B. Ksp-cadherin Immunohistochemisty of the renal lesions tested positive (100×).
Discussion and conclusion
Renal cyst seems to be a common benign disease but it is closely related to renal malignant disease. In different pathologic types of renal cancer, we can find cystic pathologic changes [6,7]. Papillary renal cell carcinoma may present as a large cyst, which may contain hemorrhagic fluid or a necrotic substance and its pseudocapsule may consist of the surrounding mesenchyme [8-10]. In clear cell renal cell carcinoma, dense consolidation is the main manifestation in renal lesion tissues [9]. However, we can also see that some clear cell carcinoma lesions are cystic or cystic solid [9,11,12], just like this clinicopathologic report we reported. Also, multilocular cystic renal cell carcinoma consists only of cysts [13,14]. In addition to these findings, there are rare renal tumors characterized by no cysts on gross examination.
Therefore, it is of great significance to identify the nature of cysts. According to the Bosniak renal cyst classification system, the cysts in clinical cases can be divided into five types [15]. There is no risk of malignant transformation for typeIand type II non-risk cysts. Type IV has been considered as malignant cystic degeneration without special identification. The walls of type IIF and type III cysts have imaging enhancement and fibrous separation in the cysts, which may turn into malignancy under certain conditions [16]. Therefore, the differentiation identification and follow-up of these two types of cysts are very important, requiring imaging follow-up such as CT or ultrasound. If there are morphologic changes or changes in the clinic symptoms of cystic patients, the existence of malignant changes should be considered. As we reported, the cyst of the patient changed suddenly within 2 years, accompanied by a transformation from benign to malignant. Therefore, it is very necessary to do cyst identification and follow-up.
At present, some studies have also reported clinical cases of simple renal cyst canceration [17,18], but the number of cases is small and scattered [19-23]. According to Bosniak classification, the risk of type IIF is about 5%, but that of type 3 is 50% [15,16]. The choice of treatment plan is also very different between the two groups. Type IIF is mainly for observation and follow-up, while type III is mainly for surgical treatment. In a prospective study, 61 patients with simple renal cyst were followed up for 14 years, only 2 patients developed from renal cyst to renal cancer [24]. It also shows that Bosniak classification is of great value in the identification and treatment of renal cysts.
The total number of patients included in recent reports is small and the real risk of malignancy in simple renal cysts is actually much lower and rare [25]. After reviewing relevant reports of the past five years, we found 6 cases [20,21,23,26-28] of the transformation of a SRC into RCC (Table 1). These studies indicated that neither the actual size nor size changes were specific for the development of a renal neoplasm. The rate of increase in cyst size in patients with renal cancer was similar to that in other patients with normal cysts. Based on these data, it is extremely difficult to clarify whether regular follow-up of the renal cysts is beneficial in the detection of early stage malignancy. The prognosis of renal cancer patients mainly depends on the degree of malignancy, surrounding invasion, and distant metastasis. However, regular imaging examination is still necessary for patients with renal cysts over a long period of time. In this way, the changes of the cyst can be found earlier. In the early stage of malignant tumor, it can be solved by operation and greatly improve the survival and prognosis of patients.
Table 1.
Reported cases of RCC arising from cysts in recent 5 years
| Author | Case | Age | Kidney | Location | Size (cm) | Histology | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| years | number | sex |
|
|
|
|
||||
| side | Bosniak | cyst | tumor | Cyst | tumor | type | Follow-up | |||
| Serrano Á et al [20] | 1 | 44, M | Right | IV | Lower | Intracapsular | 10×11 | 2×1.5 | CRCC | Fine, 6 m |
| Lai S et al [21] | 1 | 75, F | Right | II | Middle | Intracapsular | 4×5 | NM | CRCC | Fine, 3 y |
| 1 | 75, M | Right | I | upper | 7.8×5.1 | NM | CRCC | Fine, 3 y | ||
| Rana C et al [28] | 1 | 40, M | Left | II | Lower | Intracapsular | 4.3×3.9 | NM | PRCC | NM |
| Peng Jiang et al [27] | 1 | 51, M | Left | IV | upper | Intracapsular | NM | NM | SCC | Die, 6 m |
| Bonnevie F et al [26] | 1 | 15, F | Right | IV | Middle | Intracapsular | 10×10 | 10×6.5×5 | Cystic nephroma | NM |
| Yu et al [23] | 1 | 39, F | Left | I | upper | Intracapsular | 7×7 | NM | CRCC | Fine, 1 y |
In conclusion, for renal cyst patients with a long-term history, even benign renal cysts graded as Bosniak typeIand type II, imaging follow-up is necessary. For symptomatic cysts, patients should be considered for surgical treatment rather than conservative treatment, which is more beneficial in the long run.
Acknowledgements
This work was supported by the Wuxi Health Committee Foundation of China (Q201909) and Nanjing Medical University Fund (NMUB2019300). These projects are funded to corresponding author and first author (luyulong).
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Disclosure of conflict of interest
None.
Abbreviations
- CT
Computed tomography
- F
female
- M
male
- m
month
- y
year
- NM
not mentioned
- RCC
renal cell carcinoma
- CRCC
clear renal cell carcinoma
- PRCC
papillary renal cell carcinoma
- SRC
simple renal cyst
- SCC
squamous cell carcinoma
- CN
cystic nephroma
References
- 1.Garfield K, Leslie SW. Simple renal cyst. Treasure Island (FL): StatPearls; 2020. [PubMed] [Google Scholar]
- 2.Sigmon DF, Shikhman R, Nielson J. Renal Cyst. Treasure Island (FL): StatPearls; 2020. [PubMed] [Google Scholar]
- 3.Kamboj M, Zeng X, Koratala A. Renal cyst infection: a diagnostic dilemma. Clin Case Rep. 2018;6:762–763. doi: 10.1002/ccr3.1441. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Truong LD, Choi YJ, Shen SS, Ayala G, Amato R, Krishnan B. Renal cystic neoplasms and renal neoplasms associated with cystic renal diseases: pathogenetic and molecular links. Adv Anat Pathol. 2003;10:135–159. doi: 10.1097/00125480-200305000-00003. [DOI] [PubMed] [Google Scholar]
- 5.Reichard EA, Roubidoux MA, Dunnick NR. Renal neoplasms in patients with renal cystic diseases. Abdom Imaging. 1998;23:237–248. doi: 10.1007/s002619900334. [DOI] [PubMed] [Google Scholar]
- 6.Bonsib SM. Renal cystic diseases and renal neoplasms: a mini-review. Clin J Am Soc Nephrol. 2009;4:1998–2007. doi: 10.2215/CJN.02020309. [DOI] [PubMed] [Google Scholar]
- 7.Katabathina VS, Garg D, Prasad SR, Vikram R. Cystic renal neoplasms and renal neoplasms associated with cystic renal diseases in adults: cross-sectional imaging findings. J Comput Assist Tomogr. 2012;36:659–668. doi: 10.1097/RCT.0b013e31826dba18. [DOI] [PubMed] [Google Scholar]
- 8.Courthod G, Tucci M, Di Maio M, Scagliotti GV. Papillary renal cell carcinoma: a review of the current therapeutic landscape. Crit Rev Oncol Hematol. 2015;96:100–112. doi: 10.1016/j.critrevonc.2015.05.008. [DOI] [PubMed] [Google Scholar]
- 9.Kuroda N, Ohe C, Kawakami F, Mikami S, Furuya M, Matsuura K, Moriyama M, Nagashima Y, Zhou M, Petersson F, Lopez JI, Hes O, Michal M, Amin MB. Clear cell papillary renal cell carcinoma: a review. Int J Clin Exp Pathol. 2014;7:7312–7318. [PMC free article] [PubMed] [Google Scholar]
- 10.Kuroda N, Toi M, Hiroi M, Enzan H. Review of papillary renal cell carcinoma with focus on clinical and pathobiological aspects. Histol Histopathol. 2003;18:487–494. doi: 10.14670/HH-18.487. [DOI] [PubMed] [Google Scholar]
- 11.Bokhari A, Tiscornia-Wasserman PG. Cytology diagnosis of metastatic clear cell renal cell carcinoma, synchronous to pancreas, and metachronous to thyroid and contralateral adrenal: report of a case and literature review. Diagn Cytopathol. 2017;45:161–167. doi: 10.1002/dc.23619. [DOI] [PubMed] [Google Scholar]
- 12.Shao T, Yousef P, Shipilova I, Saleeb R, Lee JY, Krizova A. Clear cell papillary renal cell carcinoma as part of histologically discordant multifocal renal cell carcinoma: a case report and review of literature. Pathol Res Pract. 2016;212:229–233. doi: 10.1016/j.prp.2015.12.007. [DOI] [PubMed] [Google Scholar]
- 13.Hu J, Jin L, Li Y, He T, Liu J, Shi B, Yang S, Gui Y, Mao X, Lai Y, Ni L. Multilocular cystic renal cell carcinoma: a case report and review of the literature. Mol Clin Oncol. 2018;8:326–329. doi: 10.3892/mco.2017.1526. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Nassir A, Jollimore J, Gupta R, Bell D, Norman R. Multilocular cystic renal cell carcinoma: a series of 12 cases and review of the literature. Urology. 2002;60:421–427. doi: 10.1016/s0090-4295(02)01742-9. [DOI] [PubMed] [Google Scholar]
- 15.Schoots IG, Zaccai K, Hunink MG, Verhagen P. Bosniak classification for complex renal cysts reevaluated: a systematic review. J Urol. 2017;198:12–21. doi: 10.1016/j.juro.2016.09.160. [DOI] [PubMed] [Google Scholar]
- 16.Sevcenco S, Spick C, Helbich TH, Heinz G, Shariat SF, Klingler HC, Rauchenwald M, Baltzer PA. Malignancy rates and diagnostic performance of the Bosniak classification for the diagnosis of cystic renal lesions in computed tomography - a systematic review and meta-analysis. Eur Radiol. 2017;27:2239–2247. doi: 10.1007/s00330-016-4631-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Campenni A, Ruggeri RM, Giovinazzo S, Sindoni A, Santoro D, Baldari S. Radioiodine uptake in a renal cyst mimicking a metastasis in a patient affected by differentiated thyroid cancer: case report and review of the literature. Ann Nucl Med. 2014;28:472–476. doi: 10.1007/s12149-014-0816-y. [DOI] [PubMed] [Google Scholar]
- 18.Schlittler LA, Dallagasperina VW, Carlotto JR, Vilarroel RU, Lazaretti NS. True adrenal cyst mimicking renal cancer in a young woman: a case report. Cases J. 2009;2:7351. doi: 10.4076/1757-1626-2-7351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Salvatori F, Macchini M, Misericordia M, Paci E, Giovagnoni A, Candelari R. A simple cyst is not always simply a cyst: a case of cystic recurrence after nephrectomy for tubulocystic renal cell carcinoma and literature review. Urologia. 2020;87:119–124. doi: 10.1177/0391560319870091. [DOI] [PubMed] [Google Scholar]
- 20.Serrano A, Sanchez M, Ciappara M, Lopez E, Laso S, Jerez T, Barrera J, Cortes JA, Gonzalez-Peramato P, Blazquez J, Moreno J. Laparoscopic renal cyst excision: large simple renal cyst treatment with renal cell carcinoma cells in its wall. Histogenetic considerations and bibliographic review. Arch Esp Urol. 2019;72:422–428. [PubMed] [Google Scholar]
- 21.Lai S, Jiao B, Wang X, Xu X, Zhang M, Diao T, Zhang G. Renal cell carcinoma originating in the free wall of simple renal cyst: two unusual case reports with literature review. Medicine (Baltimore) 2019;98:e15249. doi: 10.1097/MD.0000000000015249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Boaz RJ, Vig T, Tirkey AJ, John NT, Kumar RM, Kekre N. Cutaneous metastasis of renal cell carcinoma masquerading as an infected sebaceous cyst. J Stomatol Oral Maxillofac Surg. 2018;119:145–147. doi: 10.1016/j.jormas.2017.11.002. [DOI] [PubMed] [Google Scholar]
- 23.Yu Y, Ma L, Wang Z, Zhang Z. Renal cell carcinoma presenting as a simple renal cyst: a case report. Mol Clin Oncol. 2017;6:550–552. doi: 10.3892/mco.2017.1173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Terada N, Arai Y, Kinukawa N, Terai A. The 10-year natural history of simple renal cysts. Urology. 2008;71:7–11. doi: 10.1016/j.urology.2007.07.075. discussion 11-12. [DOI] [PubMed] [Google Scholar]
- 25.Park H, Kim CS. Natural 10-year history of simple renal cysts. Korean J Urol. 2015;56:351–356. doi: 10.4111/kju.2015.56.5.351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Bonnevie F, Meunier P, Andrianne R. Cystic nephroma: a rare kidney neoplasm. Rev Med Liege. 2019;74:125–128. [PubMed] [Google Scholar]
- 27.Jiang P, Wang C, Chen S, Li J, Xiang J, Xie L. Primary renal squamous cell carcinoma mimicking the renal cyst: a case report and review of the recent literature. BMC Urol. 2015;15:69. doi: 10.1186/s12894-015-0064-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Rana C, Kumar M, Babu S, Singhai A, Agarwal H. Type 1 Papillary renal cell carcinoma presenting as an infected benign renal cyst: an uncommon presentation. Indian J Surg Oncol. 2018;9:265–267. doi: 10.1007/s13193-018-0757-3. [DOI] [PMC free article] [PubMed] [Google Scholar]