

Abstract
Coronavirus disease 2019 (COVID-19) is the respiratory disease caused by the novel severe acute respiratory syndrome-coronavirus-2 and is characterized by clinical manifestations ranging from mild, flu-like symptoms to severe respiratory insufficiency and multi-organ failure. Patients with more severe symptoms may require intensive care treatments and face a high mortality risk. Also, thrombotic complications such as pulmonary embolisms and disseminated intravascular coagulation are frequent in these patients. Indeed, COVID-19 is characterized by an abnormal inflammatory response resembling a cytokine storm, which is associated to endothelial dysfunction and microvascular complications. To date, no specific treatments are available for COVID-19 and its life-threatening complication. Immunomodulatory drugs, such as hydroxychloroquine and interleukin-6 inhibitors, as well as antithrombotic drugs such as heparin and low molecular weight heparin, are currently being administered with some benefit. Ozone therapy consists in the administration of a mixture of ozone and oxygen, called medical ozone, which has been used for over a century as an unconventional medicine practice for several diseases. Medical ozone rationale in COVID-19 is the possibility of contrasting endothelial dysfunction, modulating the immune response and acting as a virustatic agent. Thus, medical ozone could help to decrease lung inflammation, slow down viral growth, regulate lung circulation and oxygenation and prevent microvascular thrombosis. Ozone-therapy could be considered a feasible, cost-effective and easy to administer adjuvant therapy while waiting for the synthesis of a therapy or the development of the vaccine.
Keywords: COVID-19, cytokine storm, endothelial dysfunction, immunomodulation, medical ozone, ozone therapy, ozone, SARS-COV-2, virustatic
INTRODUCTION
Coronavirus disease 2019 (COVID-19) is a disease caused by the novel severe acute respiratory syndrome (SARS)-coronavirus-2 (SARS-CoV-2), a virus belonging to the same family of the viruses causing SARS and middle-eastern respiratory syndrome (MERS), which was first reported in Wuhan in December 2019, in the province of Hubei, China.1 COVID-19 shows a wide spectrum of clinical manifestations, ranging from mild, flu-like symptoms to severe interstitial pneumonia.
Patients with more severe symptoms may require intensive care treatment due to acute respiratory failure, needing mechanical ventilation and high positive end-expiratory pressure, and face high mortality risk.2 COVID-19 can cause an abnormal inflammatory response, which indeed resembles a “cytokine storm” characterized by increased plasma concentrations of C-reactive proteins, ferritin, pro-inflammatory cytokines (interleukin (IL)-1β, IL-6, IL-12, tumor necrosis factor, interferon-γ) and decreased numbers of CD16+ and CD56+ lymphocytes.3 This inflammatory pattern is different from that of severe SARS patients4 and it is similar to that at the basis of adaptive immunity.5 Immunomodulatory agents such as anti-rheumatoid arthritis drugs (chloroquine, hydroxychloroquine and tocilizumab, a humanized monoclonal antibody targeting IL-6) are currently prescribed as an adjuvant treatment of COVID-19, in addition to antiviral drugs.6 Immune activation is associated to endothelial dysfunction and microvascular complications,7 with significant septal capillary injury, characterized by mural and luminal fibrin deposition, permeation of the interalveolar septa by neutrophils and significant deposits of terminal complement components consistent with sustained, systemic activation of the alternative and lectin-based complement pathways, associated with procoagulant state.8 COVID-19 can also determine thrombotic complications: 1.4% of dead patients meet the International Society on Thrombosis and Haemostasis criteria for disseminated intravascular coagulation, as proven by the increased levels of D-dimer and fibrinogen, with lower anti-thrombin levels and spontaneous increase of the length of international normalized ratio,9 while only 0.6% of patients who survive meet these criteria10; pulmonary congestion with microvascular thrombosis and occlusion is the most relevant aspect on pathology.3 Pathological findings include “spotty lungs,” where hyperemic/hemorrhagic areas co-exist with areas of normal lung. There is also vascular hypertrophy, with enlarged (up to 20 times) and tubular pulmonary vessels, with microthrombi, followed by reduction of caliber. In the alveoli, there are typical findings of diffuse alveolar damage, with desquamation of pneumocytes, formation of hyaline membranes and fibrotic exudate.11 To suggest the systemic origin of the coagulative disorder, there is increasing evidence of central line thrombosis and vascular occlusive events (e.g., ischemic limbs).12 Moreover, there is increasing evidence of other SARS-CoV2-related vasculitis such as skin purpura8 and cerebrovascular accidents.13
The use of heparin has, indeed, proven useful in these patients: high-dose heparin is being used with success in patients who develop moderate to severe forms of COVID-19.14 Other treatments being investigated include defibrotide, a mixture of single-stranded oligonucleotides showing anti-clotting properties and used to treat veno-occlusive disease (NCT04335201), and tissue-plasminogen activators.15 Yet, even though these approaches seem to work, they are symptomatic treatments and do not act on the causes of the endothelial dysfunction.
In this scenario, it is imperative to find new therapeutic options. An interesting option could be ozone therapy. In the present short review, we describe potential benefits of ozone therapy in COVID-19. A literature search was conducted on PubMed and Embase including “ozone,” “medical ozone,” “endothelial dysfunction,” “cytokine storm,” “shock,” and “ARDS” as search terms. An additional search was conducted on ClinicalTrial.gov including “ozone,” “COVID-19,” “SARS-CoV-2” and “oxygen therapy.”
WHAT IS OZONE THERAPY?
Ozone is an allotropic form of oxygen, with a molecule made up by three oxygen atoms. Ozone is a powerful oxidant, directly acting on the cells through lipidic peroxidation, amino acids oxidations and DNA irreversible damage, leading to cell death.16 Being one of the strongest oxidants, it is extremely toxic. Ozone therapy consists in the preparation of an extemporary mixture of ozone (5% maximum concentration) and oxygen (95% minimum concentration), so-called medical ozone (MO). MO has several actions and has been applied on a wide range of pathologies as an unconventional medicine practice.17 MO can be administered systemically by adding it to a sample of patient's blood which is then reinfused (auto-hemo-infusion) or by adding it to saline solution. It can also be administered locally, by subcutaneous/intramuscular injection, by inhalation or by exposing the skin or other bodily cavities (i.e., rectal, nasal) to an air mixture containing MO.18 The biological effects of ozone are mainly mediated by antioxidant systems.19 The anti-inflammatory, immuno-modulator and virustatic effects of ozone as well as its direct effect on coagulation and microcirculation improvement are particularly important.
MECHANISMS OF ACTION
Biochemical reactions
MO reacts within biological liquids – especially in the blood – with a wide range of substrates, involved in several metabolic pathways. These complex reactions occur very quickly, and MO's half-life lasts only milliseconds. MO mainly reacts with polyunsaturated fatty acids, bound to albumin and present in most lipids and phospholipids, as well as with antioxidants, proteins and carbohydrates.20 Most of MO is involved in the reaction of “addition of polyunsaturated fatty acids to double carbon bonds,” known as “Criegée reaction.”20 This reaction involves the formation of a primary ozonide, which splits into a lipid peroxidation product whose structure is α-hydroxy-hydroperoxide and its aldehyde. Lipid peroxidation products oxidizing power is lower than other peroxides and in an aqueous solution it is degraded into hydrogen peroxide, a reactive oxygen species. Among the aldehydes that are formed in this process, the most active is the 4-hydroxy-2,3 trans-nonenal, fundamental in cellular signal-transduction, by upregulating the antioxidant system in a controlled way on numerous cells of the organism.21 This cascade of reactions ends with the exhaustion of MO. In other words, ozone is an unstable molecule and causes oxidative reactions but, if administered properly (i.e., MO), it generates a “controlled and transient oxidative stress,” which stimulates the cell's antioxidant system. This is the paradox that a molecule having oxidizing activity can be the basis of a complex antioxidant mechanism with several metabolic effects, as summarized in Figure 1.22
Figure 1.
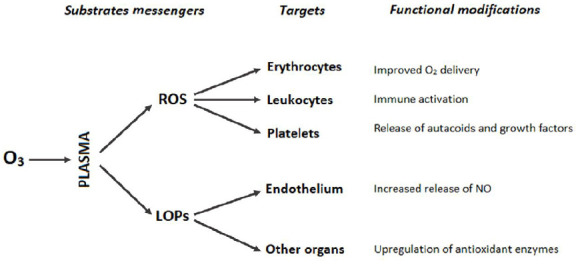
Biological effects of oxygen-ozone.
Note: LOP: Lipid peroxidation product; NO: nitric oxide; O3: ozone; ROS: reactive oxygen species. Adapted from Bocci et al.22
Anti-inflammatory and immunomodulatory effects
The anti-inflammatory and immunomodulatory effect of MO is expressed through the activation or inhibition of different molecular pathways, involved in systemic inflammation. For instance, MO inhibits the nuclear factor-kappaB (NF-κB) pathway, whose activation promotes the transcription of proinflammatory cytokine genes such as tumor necrosis factor-α, IL-1β, IL-8.23 The underlying reasons for the anti-inflammatory efficacy of MO therapy can therefore be found in a systemic reduction of inflammatory parameters such as IL-1.24 On the other hand, MO stimulates the activation of the nuclear factor erythroid 2-related factor 2 pathway,25 an intracellular transcription factor, binding to the anti-oxidant response elements nuclear regions encoding for antioxidants enzymes such as superoxide dismutase, catalase and heme oxygenase-1. Heme oxygenase-1 is a microsomal enzyme that catalyzes the degradation of haeme and produces carbon monoxide, which is another inhibitor of the NF-κB pathway.26 Moreover, heme oxygenase-1 directly activates anti-inflammatory cytokines,25 and increases the number of progenitor cells of the endothelium.27,28 Given the above-mentioned reasons, one might wonder if ozone can have an immunosuppressant effect. On the contrary, ozone application in addition to antibiotic therapy can have protective effects on septic injuries of lungs, by lowering the lipopolysaccharide-induced NF-κB hyperexpression.16,29 Yet, even though a few studies have been carried out to evaluate effects of ozone on sepsis, no clear benefits have been found.30,31,32
Effects on microcirculation
MO is mostly applied where microcirculation is impaired, as in peripheral arteriopathies (i.e., diabetic foot or systemic sclerosis).33 Ozone therapy improves blood flow in poorly perfused territories, promoting revascularization, vascular compliance, rheology and blood-tissues gas exchanges. Revascularization can be assessed by video capillaroscopy with optical probe, with the restoration of the three-dimensional capillary bed framework,28 if the capillary damage has not already caused a severe capillary loss.32 Revascularization depends on a non-chaotic neo-angiogenesis, favored by an appropriate synthesis of vascular endothelial growth factor, due to an increased production of hydrogen peroxide.34 In addition, MO induces nitric oxide synthase with the consequent formation of nitric oxide and other reactive nitrogen species. Reactive nitrogen species play a central role as modulators of the physiological signals of the cardiovascular system and in particular of vasodilator mechanisms; nitric oxide also acts as a neuromodulator, and inhibitor of platelet aggregation, vascular adhesion of leukocytes and the proliferation of smooth muscle cells.35 At an erythrocyte level, the molecular pathways determined by MO lead to an increase in the concentration of 2,3-diphosphoglicerate, which determines a right shift in the dissociation curve of oxyhemoglobin and, therefore, an increased exchange of oxygen to the peripheral tissues. In addition, the temporary lipid peroxidation action makes the red blood cell membrane more deformable. Thus, in the smaller capillaries, the red cells, instead of moving in disorder, align themselves and proceed along the axis of the vessel, arranging in a pile (Fahraeus-Lindquist effect) and facilitating metabolic exchanges.36 MO has a beneficial action in the granulation and healing processes through lowering production of tissue plasminogen activation factor and inducing greater quantities of its inhibitors, favoring the processes of fibrinolysis to those of deposition of fibrin.37
The net result of MO in the damage of microcirculation is to favor the regeneration of the microcirculation and the gaseous exchanges (through the increase of the blood flow, decrease of the blood viscosity and of the platelet aggregation, of the erythrocyte deformability and of the release of oxygen) and, at the same time, to reduce thrombotic and fibrotic processes.
Virustatic effects
Ozone directly inactivates some viruses. To successfully penetrate cells, various viruses (e.g., hepatitis A, human immunodeficiency virus, Ebola) require that membrane glycoproteins have sulfhydryl groups in the reduced form. The Ebola virus has regions on the envelope rich in cysteine, whose alteration blocks the growth properties of the virus.38 Ozone can permanently oxidize the thiol residues of cysteine in vitro.39 Virustatic ozone against Ebola has also been tested in vivo, with encouraging results but on a limited sample.40
OZONE IN COVID-19
MO could play a beneficial role in the patient suffering from COVID-19 on various levels. To foster the use of ozone therapy in COVID-19 there is the similarity between the microvascular damage in the peripheral arterial diseases41 and in the diabetic retinopathy42 with the microvascular (arterioles, precapillary arterioles, capillaries, postcapillary venules, and venules) damage at lung level in COVID-19. The latter is evidenced by CT imaging of tubular and enlarged pulmonary vessels followed by a sudden reduction of their caliber43 and by pathological findings of microthrombi and capillary aneurisms. All these diseases share vascular features of microhemorrhages, microthrombi, microaneurysms, pericapillary and tissue edema, as demonstrated both by video capillaroscopy with optical probe and by autopsy findings. The action of MO on microcirculation in terms of organized neo-angiogenesis, increase in blood flow, decrease in blood viscosity and platelet aggregation, and increase in red blood cells deformability and gas exchanges was previously discussed. Overall, MO therapy has given excellent benefits in diabetic foot, trophic or pressure ulcers, systemic sclerosis.17,33,34 Positive responses in terms of reduction of ischemic-hemorrhagic damage of the microcirculation could be obtained in COVID-19 pneumonia and on other parenchyma by an early MO auto-hemo-infusion. These positive responses could be mediated both by increasing the production of surfactant and the elasticity of the alveoli and by a reduction of endothelial damage, through platelet adhesion reduction and through blockage of the coagulation cascade preventing microthrombi formation.44 In addition, this effect would also occur at a peripheral level, by reducing formation of deep venous thrombi and consequent pulmonary embolism. Both micro and macrothrombi lead to the formation of pulmonary shunt and pulmonary hypertension, that are typical features of hypoxemia refractory to ventilatory therapy.45 To our knowledge, no studies have been published regarding the development of pulmonary hypertension in COVID-19 or its severity in those with a history of pulmonary hypertension. In the authors’ opinion, MO should not be administered in a context of advanced microvascular lung damage with massive capillary loss, similar to what occurs in systemic sclerosis with pulmonary hypertension46; in this context ozone could determine a worsening of lung damage, inflammation and edema in patients with pulmonary hypertension,47 or it could have no effect due to the capillary loss. Yet, an anti-hypoxemic action was observed by the MO auto-hemo-infusion in patients suffering from chronic obstructive bronchitis.48 Furthermore, in an animal model with a healthy lung, ozone seems to have a protective action on the genesis of pulmonary edema, thanks to the ability to stimulate the pulmonary sympathetic nervous system, and block microvascular responses to acetylcholine and substance P at a lung level.49 Interestingly, when applied to the patient with severe respiratory insufficiency, requiring mechanical ventilation with long-term elevated positive end-expiratory pressure (as in severe COVID-19 pneumonia), inhaled ozone improved gas exchanges in the lung, increased surfactant production and lung compliance in a small sample of patients.44
Another potential benefit of MO auto-hemo-infusion could be on the “cytokine storm” in the pathogenesis of respiratory failure, disseminated intravascular coagulation and multi-organ failure in COVID-19. The protective immunomodulatory effects of ozone in septic lung injury have already been discussed previously. “Cytokine storm” hemodynamic consequences are similar to those of toxic shock.50 In toxic shock, as in septic shock, microcirculatory abnormalities are cardinal features, being dissociated from that of systemic hemodynamic and more severe among non-survivors.51 Therefore, microcirculatory alterations may persist despite correction of systemic hemodynamic variables with vasopressors drugs.52 Ozone preconditioning has been demonstrated to be as potent as dexamethasone in reducing tumor necrosis factor-α level during lipopolysaccharide-induced endotoxic shock and oxidative stress in a murine model.31 In addition to primary “cytokine storm,” a superinfection and a secondary septic shock are prevalent among patients with COVID-19.31,53 Ozone has both a direct bactericidal action, through lipid peroxidation product and reactive oxygen species,54 and an indirect one, through an increase in neutrophilic chemotaxis and myeloperoxidase activity.55 Thus, MO could both reduce the microcirculatory alterations induced by the “cytokine storm” and the occurrence of bacterial superinfections and septic shock.
Like in the case of Ebola virus, another potential action of ozone is the inactivation of the spike protein that coronaviruses need to infect guest cells. The spike protein is rich in cysteine residues, permanently oxidized by ozone, and these residues are preserved during the evolution of the viral strains.56 Therefore, SARS-CoV-2 could potentially be inactivated by ozone-mediated oxidation during the viremic phase (if administered early via auto-hemo-infusion) and at the level of the colonized nasopharyngeal mucosa of healthy carriers through topic formulations.57
Only one clinical trial about ozone therapy in patients affected by severe COVID-19 related pneumonia has been conducted to date (NCT04370223). Preliminary data showed that the patients treated with MO presented both shorter time to clinical improvement and a significantly higher proportion of patients achieving 14-day clinical improvement compared to those receiving supportive care.58 Yet, it was a single-center study enrolling few patients and larger randomized clinical trials are needed. On the other hand, three trials about hyperbaric oxygen therapy have already been conducted (NCT04370223, NCT04343183, and NCT04332081). This preliminary data suggest potential benefit of hyperbaric oxygen therapy in COVID-19.59 This finding is also of interests because, in a murine model of pulmonary damage, a combination of hyperbaric oxygen therapy and MO was demonstrated to be more effective than hyperbaric oxygen therapy regarding serum IL-1β, lung glutathione storages and histologic outcome.29
CONTRAINDICATIONS FOR OZONE THERAPY
Regarding MO systemic therapy, there are some contraindications and warnings. First, MO should not be administered directly in the blood and should not be mixed in solution with other drugs but saline solution, because of its oxidizing effect. Second, there are no studies about ozone-therapy and pregnancy; hence it should be avoided in this case. Another absolute contraindication is glucose-6-phosphate dehydrogenase deficiency in systemic administration,60 the same warning concerning antimalarials.61 Potentially, MO administration in patients suffering from hyperthyroidism could be harmful for the lungs, as shown in murine models.62
CONCLUSIONS
The adjuvant use of ozone-therapy in COVID-19 through auto-hemo-infusion could better oxygenate the tissues, decrease lung inflammation and regulate the immune response, avoiding the “cytokine storm,” slow down viral growth, regulate lung microcirculation and avoid or slow down vascular hypertrophy and the consequent hyperemia, especially in the initial stages, by contrasting endothelial damage, in analogy with what happens in peripheral arterial pathologies. An association with other currently available treatments is mandatory, to avoid or limit the use of intubation and, ultimately, allowing a shortening of healing times with the possibility of greater replacement in the intensive care, to date the real limiting factor.
If auto-hemo-infusion is not administrable, MO could be delivered through dilution in saline solution or rectal infusion. Endonasal application could be administered to inactivate colonizing SARS-CoV2 in the asymptomatic carriers. Furthermore, since there are no major side effects and it can be synergistic with other therapies, it is a candidate to be an essential therapy in home care, given its easy execution and low cost. Ozone-therapy could be considered a feasible, cost-effective and easy to administer adjuvant therapy while waiting for the synthesis of a therapy or the development of the vaccine.
Footnotes
Conflicts of interest
The authors declare no conflicts of interest.
Financial support
The authors declare they did not receive financial support for the present review.
Copyright license agreement
The Copyright License Agreement has been signed by all authors before publication.
Plagiarism check:
Checked twice by iThenticate.
Peer review:
Externally peer reviewed.
REFERENCES
- 1.Li Q, Guan X, Wu P, et al. Early transmission dynamics in Wuhan, China, of Novel Coronavirus-Infected Pneumonia. N Engl J Med. 2020;382:1199–1207. doi: 10.1056/NEJMoa2001316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Grasselli G, Zangrillo A, Zanella A, et al. Baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy Region, Italy. JAMA. 2020;323:1574–1581. doi: 10.1001/jama.2020.5394. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Li G, Fan Y, Lai Y, et al. Coronavirus infections and immune responses. J Med Virol. 2020;92:424–432. doi: 10.1002/jmv.25685. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Channappanavar R, Perlman S. Pathogenic human coronavirus infections: causes and consequences of cytokine storm and immunopathology. Semin Immunopathol. 2017;39:529–539. doi: 10.1007/s00281-017-0629-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Franza L, Carusi V, Altamura S, et al. Interrelationship between inflammatory cytokines (IL-1, IL-6, IL-33, IL-37) and acquired immunity. J Biol Regul Homeost Agents. 2019;33:1321–1326. doi: 10.23812/Editorial. [DOI] [PubMed] [Google Scholar]
- 6.Stebbing J, Phelan A, Griffin I, et al. COVID-19: combining antiviral and anti-inflammatory treatments. Lancet Infect Dis. 2020;20:400–402. doi: 10.1016/S1473-3099(20)30132-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Zelic M, Roderick JE, O’Donnell JA, et al. RIP kinase 1-dependent endothelial necroptosis underlies systemic inflammatory response syndrome. J Clin Invest. 2018;128:2064–2075. doi: 10.1172/JCI96147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Magro C, Mulvey JJ, Berlin D, et al. Complement associated microvascular injury and thrombosis in the pathogenesis of severe COVID-19 infection: A report of five cases. Transl Res. 2020;220:1–13. doi: 10.1016/j.trsl.2020.04.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Zhang Y, Zheng L, Liu L, Zhao M, Xiao J, Zhao Q. Liver impairment in COVID-19 patients: A retrospective analysis of 115 cases from a single centre in Wuhan city, China. Liver Int. 2020 doi: 10.1111/liv.14455. doi:10.1111/liv.14455. [DOI] [PubMed] [Google Scholar]
- 10.Tang N, Li D, Wang X, Sun Z. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J Thromb Haemost. 2020;18:844–847. doi: 10.1111/jth.14768. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Xu Z, Shi L, Wang Y, et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir Med. 2020;8:420–422. doi: 10.1016/S2213-2600(20)30076-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Mao L, Jin H, Wang M, et al. Neurologic manifestations of hospitalized patients with coronavirus disease 2019 in Wuhan, China. JAMA Neurol. 2020;77:1–9. doi: 10.1001/jamaneurol.2020.1127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Wu Y, Xu X, Chen Z, et al. Nervous system involvement after infection with COVID-19 and other coronaviruses. Brain Behav Immun. 2020;87:18–22. doi: 10.1016/j.bbi.2020.03.031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Thachil J. The versatile heparin in COVID-19. J Thromb Haemost. 2020;18:1020–1022. doi: 10.1111/jth.14821. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Wang J, Hajizadeh N, Moore EE, et al. Tissue plasminogen activator (tPA) treatment for COVID-19 associated acute respiratory distress syndrome (ARDS): A case series. J Thromb Haemost. 2020 doi: 10.1111/jth.14828. doi:10.1111/jth.14828. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ding W, Jin W, Cao S, et al. Ozone disinfection of chlorine-resistant bacteria in drinking water. Water Res. 2019;160:339–349. doi: 10.1016/j.watres.2019.05.014. [DOI] [PubMed] [Google Scholar]
- 17.Smith NL, Wilson AL, Gandhi J, Vatsia S, Khan SA. Ozone therapy: an overview of pharmacodynamics, current research, and clinical utility. Med Gas Res. 2017;7:212–219. doi: 10.4103/2045-9912.215752. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Bocci V. Autohaemotherapy after treatment of blood with ozone. A reappraisal. J Int Med Res. 1994;22:131–144. doi: 10.1177/030006059402200301. [DOI] [PubMed] [Google Scholar]
- 19.Bocci V, Valacchi G, Corradeschi F, Fanetti G. Studies on the biological effects of ozone: 8. Effects on the total antioxidant status and on interleukin-8 production. Mediators Inflamm. 1998;7:313–317. doi: 10.1080/09629359890820. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Srisankar EV, Patterson LK. Reactions of ozone with fatty acid monolayers: a model system for disruption of lipid molecular assemblies by ozone. Arch Environ Health. 1979;34:346–349. doi: 10.1080/00039896.1979.10667429. [DOI] [PubMed] [Google Scholar]
- 21.Esterbauer H, Schaur RJ, Zollner H. Chemistry and biochemistry of 4-hydroxynonenal, malonaldehyde and related aldehydes. Free Radic Biol Med. 1991;11:81–128. doi: 10.1016/0891-5849(91)90192-6. [DOI] [PubMed] [Google Scholar]
- 22.Bocci V, Borrelli E, Travagli V, Zanardi I. The ozone paradox: ozone is a strong oxidant as well as a medical drug. Med Res Rev. 2009;29:646–682. doi: 10.1002/med.20150. [DOI] [PubMed] [Google Scholar]
- 23.Huth KC, Saugel B, Jakob FM, et al. Effect of aqueous ozone on the NF-kappaB system. J Dent Res. 2007;86:451–456. doi: 10.1177/154405910708600512. [DOI] [PubMed] [Google Scholar]
- 24.Cooke ED, Pockley AG, Tucker AT, Kirby JD, Bolton AE. Treatment of severe Raynaud's syndrome by injection of autologous blood pretreated by heating, ozonation and exposure to ultraviolet light (H-O-U) therapy. Int Angiol. 1997;16:250–254. [PubMed] [Google Scholar]
- 25.Re L, Martínez-Sánchez G, Bordicchia M, et al. Is ozone pre-conditioning effect linked to Nrf2/EpRE activation pathway in vivo? A preliminary result. Eur J Pharmacol. 2014;742:158–162. doi: 10.1016/j.ejphar.2014.08.029. [DOI] [PubMed] [Google Scholar]
- 26.Wei Y, Chen P, de Bruyn M, Zhang W, Bremer E, Helfrich W. Carbon monoxide-releasing molecule-2 (CORM-2) attenuates acute hepatic ischemia reperfusion injury in rats. BMC Gastroenterol. 2010;10:42. doi: 10.1186/1471-230X-10-42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Wu BJ, Midwinter RG, Cassano C, et al. Heme oxygenase-1 increases endothelial progenitor cells. Arterioscler Thromb Vasc Biol. 2009;29:1537–1542. doi: 10.1161/ATVBAHA.109.184713. [DOI] [PubMed] [Google Scholar]
- 28.Cao Y, Wang H, Wang Q, Han X, Zeng W. Three-dimensional volume fluorescence-imaging of vascular plasticity in adipose tissues. Molecular metabolism. 2018;14:71–81. doi: 10.1016/j.molmet.2018.06.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Yamanel L, Kaldirim U, Oztas Y, et al. Ozone therapy and hyperbaric oxygen treatment in lung injury in septic rats. Int J Med Sci. 2011;8:48–55. doi: 10.7150/ijms.8.48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Uludag MO, Ozdemir ED, Bal NB, et al. Effects of ozone treatment in endotoxin induced shock model in rats. Int J Pharmacol. 2017;13:166–174. [Google Scholar]
- 31.Zamora ZB, Borrego A, López OY, et al. Effects of ozone oxidative preconditioning on TNF-alpha release and antioxidant-prooxidant intracellular balance in mice during endotoxic shock. Mediators Inflamm. 2005;2005:16–22. doi: 10.1155/MI.2005.16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Ranaldi GT. Ossigeno-Ozonoterapia nelle patologie arteriose degli arti inferiori. Int J Ozone Ther. 2007;2:131–132. [Google Scholar]
- 33.Liu J, Zhang P, Tian J, et al. Ozone therapy for treating foot ulcers in people with diabetes. Cochrane Database Syst Rev. 2015:CD008474. doi: 10.1002/14651858.CD008474.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Hassanien M, Rashad S, Mohamed N, Elawamy A, Ghaly MS. Non-invasive oxygen-ozone therapy in treating digital ulcers of patients with systemic sclerosis. Acta Reumatol Port. 2018;43:210–216. [PubMed] [Google Scholar]
- 35.Picca A, Sirago G, Pesce V, et al. Administration of enalapril started late in life attenuates hypertrophy and oxidative stress burden, increases mitochondrial mass, and modulates mitochondrial quality control signaling in the rat heart. Biomolecules. 2018;8:177. doi: 10.3390/biom8040177. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Travagli V, Zanardi I, Bocci V. A realistic evaluation of the action of ozone on whole human blood. Int J Biol Macromol. 2006;39:317–320. doi: 10.1016/j.ijbiomac.2006.03.024. [DOI] [PubMed] [Google Scholar]
- 37.Balmes JR, Arjomandi M, Bromberg PA, et al. Ozone effects on blood biomarkers of systemic inflammation, oxidative stress, endothelial function, and thrombosis: The Multicenter Ozone Study in oldEr Subjects (MOSES) PLoS One. 2019;14:e0222601. doi: 10.1371/journal.pone.0222601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Li Y, Perry T, Kindy MS, et al. GLP-1 receptor stimulation preserves primary cortical and dopaminergic neurons in cellular and rodent models of stroke and Parkinsonism. Proc Natl Acad Sci U S A. 2009;106:1285–1290. doi: 10.1073/pnas.0806720106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Dussault PH, George AD, Trullinger TK. Peroxides as oxidative enzyme inhibitors: mechanism-based inhibition of a cysteine protease by an amino acid ozonide. Bioorg Med Chem Lett. 1999;9:3255–3258. doi: 10.1016/s0960-894x(99)00563-6. [DOI] [PubMed] [Google Scholar]
- 40.Rowen RJ, Robins H, Carew K, Kamara MM, Jalloh MI. Rapid resolution of hemorrhagic fever (Ebola) in sierra leone with ozone therapy. Afr J Infect Dis. 2015;10:49–54. [Google Scholar]
- 41.Forsythe RO, Brownrigg J, Hinchliffe RJ. Peripheral arterial disease and revascularization of the diabetic foot. Diabetes Obes Metab. 2015;17:435–444. doi: 10.1111/dom.12422. [DOI] [PubMed] [Google Scholar]
- 42.Murugesan N, Üstunkaya T, Feener EP. Thrombosis and hemorrhage in diabetic retinopathy: a perspective from an inflammatory standpoint. Semin Thromb Hemost. 2015;41:659–664. doi: 10.1055/s-0035-1556731. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Salehi S, Abedi A, Balakrishnan S, Gholamrezanezhad A. Coronavirus Disease 2019 (COVID-19): A Systematic Review of Imaging Findings in 919 Patients. AJR Am J Roentgenol. 2020;doi:10. doi: 10.2214/AJR.20.23034. 2214/AJR.20.23034. [DOI] [PubMed] [Google Scholar]
- 44.Antoszewski Z, Czyz-Grabińska E, Gołofit Z. Ozone therapy in the management of respiratory failure after long term mechanical respiration. Pol Merkur Lekarski. 2001;11:180–181. [PubMed] [Google Scholar]
- 45.Bendjelid K, Giraud R. Treating hypoxemic patients with SARS-COV-2 pneumonia: Back to applied physiology. Anaesth Crit Care Pain Med. 2020 doi: 10.1016/j.accpm.2020.04.003. doi:10.1016/j.accpm.2020.04.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Ruaro B, Smith V, Sulli A, Decuman S, Pizzorni C, Cutolo M. Methods for the morphological and functional evaluation of microvascular damage in systemic sclerosis. Korean J Intern Med. 2015;30:1–5. doi: 10.3904/kjim.2015.30.1.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Zychowski KE, Lucas SN, Sanchez B, Herbert G, Campen MJ. Hypoxia-induced pulmonary arterial hypertension augments lung injury and airway reactivity caused by ozone exposure. Toxicol Appl Pharmacol. 2016;305:40–45. doi: 10.1016/j.taap.2016.06.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Borrelli E. An integrative approach in the treatment of chronic obstructive pulmonary disease: The role of the ozone therapy. Eur J Integr Med. 2015;7:31. [Google Scholar]
- 49.Delaunois A, Segura P, Dessy-Doizé C, et al. Ozone-induced stimulation of pulmonary sympathetic fibers: a protective mechanism against edema. Toxicol Appl Pharmacol. 1997;147:71–82. doi: 10.1006/taap.1997.8266. [DOI] [PubMed] [Google Scholar]
- 50.Lin L, Xu L, Lv W, et al. An NLRP3 inflammasome-triggered cytokine storm contributes to Streptococcal toxic shock-like syndrome (STSLS) PLoS Pathog. 2019;15:e1007795. doi: 10.1371/journal.ppat.1007795. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Trzeciak S, Dellinger RP, Parrillo JE, et al. Early microcirculatory perfusion derangements in patients with severe sepsis and septic shock: relationship to hemodynamics, oxygen transport, and survival. Ann Emerg Med. 2007;49:88–98, 98.e1-2. doi: 10.1016/j.annemergmed.2006.08.021. [DOI] [PubMed] [Google Scholar]
- 52.Lipinska-Gediga M. Sepsis and septic shock-is a microcirculation a main player. Anaesthesiol Intensive Ther. 2016;48:261–265. doi: 10.5603/AIT.a2016.0037. [DOI] [PubMed] [Google Scholar]
- 53.Wujtewicz M, Dylczyk-Sommer A, Aszkiełowicz A, Zdanowski S, Piwowarczyk S, Owczuk R. COVID-19 - what should anaethesiologists and intensivists know about it. Anaesthesiol Intensive Ther. 2020;52:34–41. doi: 10.5114/ait.2020.93756. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Park JS, Sung BJ, Yoon KS, Jeong CS. The bactericidal effect of an ionizer under low concentration of ozone. BMC Microbiol. 2016;16:173. doi: 10.1186/s12866-016-0785-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Klebanoff SJ. Myeloperoxidase: friend and foe. J Leukoc Biol. 2005;77:598–625. doi: 10.1189/jlb.1204697. [DOI] [PubMed] [Google Scholar]
- 56.Li F. Structure, function, and evolution of coronavirus spike proteins. Annu Rev Virol. 2016;3:237–261. doi: 10.1146/annurev-virology-110615-042301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Ranaldi GT, Villani ER, Franza L. Ozonetherapy: a multirole weapon, rational of the use of the topical pathway against SARS-COV-2. 2020. [Assessed by May 6, 2020]. https://frenxiv.org/n2dup/
- 58.Hernandez A, Vinals M, Pablos A, et al. Ozone therapy for patients with SARS-COV-2 pneumonia: a single-center prospective cohort study. 2020. [Assessed by June 12, 2020]. https://www.medrxiv.org/content/10.1101/2020.1106.1103.20117994v20117992.full.pdf .
- 59.Harch PG. Hyperbaric oxygen treatment of novel coronavirus (COVID-19) respiratory failure. Med Gas Res. 2020;10:61–62. doi: 10.4103/2045-9912.282177. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Nkhoma ET, Poole C, Vannappagari V, Hall SA, Beutler E. The global prevalence of glucose-6-phosphate dehydrogenase deficiency: a systematic review and meta-analysis. Blood Cells Mol Dis. 2009;42:267–278. doi: 10.1016/j.bcmd.2008.12.005. [DOI] [PubMed] [Google Scholar]
- 61.Yazdany J, Kim AHJ. Use of hydroxychloroquine and chloroquine during the COVID-19 pandemic: what every clinician should know. Ann Intern Med. 2020;172:754–755. doi: 10.7326/M20-1334. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Huffman LJ, Judy DJ, Brumbaugh K, et al. Hyperthyroidism increases the risk of ozone-induced lung toxicity in rats. Toxicol Appl Pharmacol. 2001;173:18–26. doi: 10.1006/taap.2001.9174. [DOI] [PubMed] [Google Scholar]