

Abstract
Objective
To evaluate the stability after orthodontic treatment between two types of lower fixed retainers: those bonded onto all anterior teeth or those bonded only onto the canines.
Materials and Methods
The following electronic databases were consulted: PubMed, Scopus, Web of Science, Cochrane Library, Lilacs, OpenGrey, ClinicalTrials, and Google Scholar. No restriction of language or year were applied. After selection of studies, risk-of-bias evaluation and qualitative synthesis of the included studies were performed using The Cochrane Collaboration's tool for randomized studies and the “Risk of Bias in Non-randomized Studies of Interventions” (ROBINS-I) tool for nonrandomized studies, and a summary of the overall strength of evidence was presented using the “Grading of recommendations, assessment, development and evaluation” tool.
Results
Among the 180 studies retrieved from the searches, five were included in this review. Three of them showed a low risk of bias, while two presented a high risk of bias. With regard to stability, two studies reported better stability for retainers bonded to all six teeth, while the other three showed no difference. The retainer bonded to all teeth presented a higher breakage rate in one study.
Conclusions
Stability seems better with lower fixed retainers bonded on all anterior teeth. The breakage rate may not change according to the bonding. However, studies with greater methodological soundness are necessary to reach a more reliable conclusion.
Keywords: Orthodontic retainers, Long-term effects, Orthodontic appliances
INTRODUCTION
After orthodontic movement, teeth tend to return to the direction from which they were originally moved1 as a result of traction of the elastic fibers of the gingiva and the imbalance among forces between the lips and tongue.2 After finishing treatment, time is needed for the reorganization of alveolar bone and periodontium.3 Orthodontic retainers are ideally suited to maintain tooth alignment after treatment.4
In the lower arch, fixed retainers in the anterior segment are a valid option for managing the significant relapse rate in this area.5 Recent evidence6,7 indicated that retainers are essential for long-term stability. However, there are still questions regarding the efficacy of the different types of retainers available.8
The 3 × 3 fixed retainer, bonded using the direct technique, is a commonly used type of retainer in the lower arch. This is likely attributable to the accessibility and cost-effectiveness of the technique.9 This type of retainer can be bonded either to the lingual surface of the lower canines only or to all six of the lower teeth, on the lingual surface of the incisors and canines.4,9 In addition to stability, another concern associated with fixed retainers has been the possibility of increased levels of dental plaque and calculus as a result of poor dental hygiene due to the difficulty of brushing and flossing the area around the retainer.10
Several systematic reviews11–14 and original studies15,16 investigated the benefits and damage associated with fixed and removable retainers. Those studies focused on stability and clinical performance of both types of retainers, considering the different materials and design of the appliances.11–16
Despite the fact that the influence of design and bonding technique for lower fixed retainers was discussed in original studies,15,16 no systematic review has addressed this question. A previous systematic review11 evaluated the difference between fixed orthodontic retainers bonded to all teeth and those bonded only to the canines, but only the periodontal condition and bonding failures were presented; results regarding the stability of dental alignment were not reported. This systematic review aimed to evaluate the difference in stability between lower fixed retainers bonded on all six anterior teeth (lower incisors and canines) and those bonded only to the canines. Additionally, breakage rates were also evaluated.
MATERIALS AND METHODS
Protocol and Registration
The protocol of this systematic review was registered in the PROSPERO database (International Prospective Register of Systematic Reviews–PROSPERO; http://www.crd.york.ac.uk/PROSPERO) under the code CRD42016050719. The Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA)17 guidelines were followed in this review.
Eligibility Criteria
The PICO/PECO strategy was applied. Prospective and retrospective studies performed in adults and adolescents (P), using lower fixed retainers bonded only on canines (I/E) compared to retainers bonded to all anterior teeth (lower incisors and canines), were evaluated with regard to stability (O). Animal studies, technical articles, case reports, literature reviews, and noncontrolled studies were excluded.
Search Strategy and Study Selection
Searches in the following databases were performed through June 2019: PubMed, Scopus, Web of Science, The Cochrane Library, LILACS, and ClinicalTrials. The gray literature was consulted through OpenGrey and Google Scholar. No language or year restriction was applied. The predefined search strategies presented a combination of Mesh and free terms related to orthodontic retainers and were adapted to each database (Appendix 1).
After searches were conducted, the results were imported into a reference manager software (EndNote web, Clarivate Analytics, Philadelphia, Pa). Duplicated results were excluded by automatic and manual assessment.
The selection process was performed in two phases. In the first phase, the title and abstracts that did not follow the established eligibility criteria were excluded. In the second phase, articles remaining from phase I were assessed by full text. Among the selected studies resulting from this process, reference lists were also evaluated to retrieve new articles following the eligibility criteria. All steps of the selection process were conducted independently by two reviewers (ALCSB and LBM) and checked by a third reviewer (SMAM) in case of disagreement.
Data Extraction and Risk of Bias
The results extracted from included articles were evaluated qualitatively. The country, year of publication, study design, sample characteristics, methods of evaluation, results, and statistical analysis were obtained from the included studies. In the event of an absence of information among the articles, the authors were contacted by e-mail. In an attempt to contact authors, one e-mail was sent once every week for five consecutive weeks for each study.
The risk of bias was assessed through two tools: The Cochrane Collaboration's tool for assessing the risk of bias18 applied in randomized controlled studies and the “Risk of Bias in Non-randomized Studies of Interventions” (ROBINS-I) tool19 in nonrandomized studies. In The Cochrane Collaboration's tool for assessing risk of bias18 tool, seven domains were included: random sequence generation (selection bias), allocation concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias), selective reporting (reporting bias), and other bias. The performance bias and the detection bias were not considered in this evaluation. For each domain, the risk of bias was judged as “low risk,” “high risk,” or “unclear risk.”
The ROBINS-I tool19 was used in nonrandomized studies. This checklist presents three main evaluation domains: preintervention, during intervention, and postintervention. After the individualization of the main criteria, the risk of bias was assessed for each domain and classified as “low,” “moderate,” “serious,” “critical,” or “no information.”
Level of Evidence
A summary of the overall strength of evidence was presented using the “Grading of recommendations, assessment, development and evaluation” (GRADE) tool.20 Included studies were evaluated according to their design, study quality, consistency, and directness. Evaluation of stability and frequency of breakage were performed.
RESULTS
Selection and Characteristics of Included Studies
A total of 180 citations were retrieved from databases. After exclusion of 63 duplicated results, 117 title/abstracts were evaluated. Among those, 111 studies were excluded: two were opinion articles, two were systematic reviews that did not assess the bonding of retainers, 12 studies did not evaluate stability of retainers, 32 did not compare the two types of bonding among retainers, and 63 studies did not assess orthodontic lower retainers (Appendix 2). Six studies were reviewed by full text,21–26 and one was excluded because of the absence of stability evaluation.26 Five studies were included in this review21–25 and subjected to qualitative and risk-of-bias assessment (Figure 1; Table 1). Among the included articles, two were randomized trials21,22 and three were nonrandomized clinical trials23–25 (Table 2).
Figure 1.

Flowchart with the number of records identified and removed at each stage of the review according to the PRISMA statement.
Table 1.
Risk of Bias (RoB) of the Included Studies, According to the ROBINS-I Tool19
| Author |
Domains |
|||||||
| Preintervention |
At Intervention |
Postintervention |
||||||
| Bias Due to Confounding |
Bias in Selecting Participants for the Study |
Bias in Classifying Interventions |
Bias Due to Deviations From Intended Intervention |
Bias Due to Missing Data |
Bias in Measuring Outcomes |
Bias in Selecting Reported Result |
Overall RoB Judgment |
|
| Al-Nimri et al.23 | Low | Low | Low | Low | Low | Low | Low | Low |
| Steinnes et al.24 | Low | Low | Low | Low | Low | Low | Low | Low |
| Schutz-Frazon et al.25 | Low | Low | Critical | Moderate | Low | Low | Low | Serious |
Table 2.
Summary of Characteristics and Results of the Included Studiesa
| Author/Country/ Year/Study Design |
Artun et al.21/United States/1997/RCT |
Stormann and Ehmer22/Germany/2002/RCT |
Al-Nimri et al.23/Jordan/2009/Non-RCT |
Steinnes et al.24/Norway/2017/ Non-RCT |
Schutz-Frazon et al.25/Sweden /2017/ Non-RCT |
|
| Sample | Source | Department of Orthodontics, University of Washington, Seattle, Wash | Department of Orthodontics, University of Münster, Germany | Department of Orthodontics, Jordan University of Science and Technology, Jordan | Public Dental Service Competence Centre of Northern Norway, Tromsø, Norway | Department of Orthodontics, Institute for Postgraduate Dental Education, Jonkoping, Sweden |
| n | 49 n = 11: thick plain wire (0.032 inch) bonded only to the canines n = 13: thick spiral wire (0.032 inch) bonded only to the canines n = 11: thin (0.205-inch) flexible spiral wire bonded to each tooth in the segment n = 14: removable retainers | 98 n = 36: twisted wire (0.0215 inch) bonded to each tooth in the segment n = 30: twisted wire (0.0195 inch) bonded to each tooth in the segment n = 32: canine-and-canine prefabricated retainer | 62 n = 31: multistrand lower retainers bonded to all six teeth n = 31 plain wire retainers bonded only in canines | 60 lower fixed retainers: bonded to all six teeth or only canines | 64 n = 28: plain wire (0.028 inch) retainers bonded only in canines n = 36: multistrand (0.0195 inch) lower retainers bonded in all six teeth | |
| Age | Adults and adolescents | 13–17 y | 19.97–20.23 y | 25 y | 12. –13.2 y | |
| Follow-up, y | 3 | 2 | 1 | 8 | 9 | |
| Assessment | Stability | Irregularity Index | Irregularity Index | Irregularity Index | Irregularity Index and PAR index | Irregularity Index |
| Results | Stability | No difference between groups on the alignment of incisors (P = .18) | The relapse rate was higher among retainers bonded only in canines (P < .001) | The retainers bonded only to canines presented a higher than those bonded in all six teeth (P = .002) | No difference among groups (P = .62) | No difference among groups (P = .05) |
| Breakages | 27.3% of retainers bonded to all teeth 20.4% of retainers bonded only in canines: 30.4% in twisted archwire and 9.1% in plain archwire | The retainers bonded in all six teeth (0.0215) presented a higher rate of breakages (53%), followed by the 0.0195 retainers (29%). The retainers bonded only to the canines presented a rate of 18%; P < .001 | No difference among groups (P > .05) | — | No difference among groups (P > .05) | |
RCT indicates randomized controlled trial; Non-RCT, non–randomized controlled trial.
A meta-analysis was not possible to achieve as part of this systematic review as a result of methodological heterogeneity. The included studies used a different wire thickness, so comparisons among them were not feasible.
Results from Individual Studies
Stormann and Ehmer22 and Al-Nimri et al.23 reported better stability for the retainer bonded on all lower anterior teeth. The other three studies21,24,25 showed no differences between the two types of retainers in the frequency of breakage or in the stability of treatment.
Two of the studies included21,22 were randomized clinical trials with a follow-up period ranging from 222 to 321 years. The sample sizes ranged from 4921 to 9822 patients, and only adolescents and young adults were included. The other articles included in this review23–25 were nonrandomized studies. The sample size varied from 62 to 69 patients, and the follow-up time was between 1 and 9 years. The average patient age was from 12 to 25 years among the studies.23–25
The method used to compare the two types of retainers was the Irregularity Index proposed by Little.27 One of the studies24 also used the PAR index.28 To evaluate breakage, the mean number of broken appliances was compared among groups descriptively21,25 or by statistical analysis22,23 (Table 2).
Risk of Bias
For the Artun et al.21 study, there was an unclear risk of bias on the domains random sequence generation (selection bias) and allocation concealment (selection bias). The authors were contacted to clarify the randomization process but they were unable to provide further information (Appendix 3). For the domains of incomplete outcome data (attrition bias) and other bias there was a high risk due to a reported dropout of patients during follow up and the absence of the primary evaluator during follow up. The domains blinding of participants and personnel (performance bias) and blinding of outcome assessment (detection bias) were not evaluated because of the nature of the intervention (Figure 2).
Figure 2.
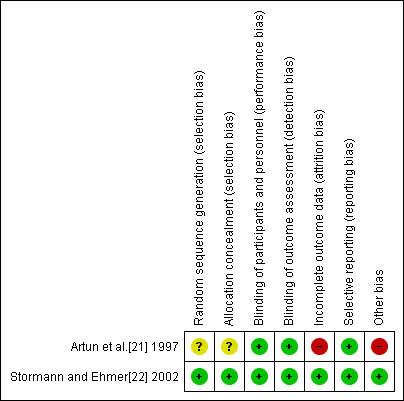
Risk of bias of the randomized studies according to The Cochrane Collaboration's tool.
The study from Stormann and Ehmer22 presented a low risk of bias for all domains considered. The article thoroughly described the randomization process, reported all the results, and seemed to be free from other sources of bias (Figure 2).
Among the nonrandomized studies, two23,24 of them presented a low risk of bias in all domains. The other study25 was classified as having a moderate risk of bias, due to the retrospective definition of some aspects of the assignments of intervention.
Level of Evidence
The GRADE evaluation highlights the results reported by the included studies, suggesting that there was better stability when lower retainers bonded on all anterior teeth were used compared to retainers bonded only to canines. A higher rate of breakage was reported for retainers bonded on all teeth; however, the strength of these results should be carefully considered because of the risk of bias and type of the included studies (Table 3).
Table 3.
Grading of Recommendation, Assessment, Development, and Evaluation (GRADE) instrument20
| Certainty Assessment |
Summary of Findings |
||||||||||
| No. of Participants (Studies) FollowUp |
Risk of Bias |
Inconsistency |
Indirectness |
Imprecision |
Publication Bias |
Overall Certainty of Evidence |
Study Event Rates, No. (%)% |
Relative Effect (95% CI) |
Anticipated Absolute Effects |
||
| With Bonded Only in Canines |
With Lower Fixed Retainers Bonded in All Teeth |
Risk with Bonded Only in Canines |
Risk Difference with Lower Fixed Retainers Bonded in All Teeth |
||||||||
| Absence of relapse on stability (follow up: range 2–3 y) | |||||||||||
| 133 (2 RCTs) | Seriousa | Not serious | Not serious | Not serious | None | ⊕⊕⊕ ○ Moderate | 70/77 (90.9) | 48/56 (85.7) | Not estimable | Not pooled | Not pooled |
| Absence of relapse on stability (follow up: range 1–9 y) | |||||||||||
| 186 (3 observational studies) | Seriousb | Not serious | Seriousc | Not serious | None | ⊕⊕ ○○ Low | 47/78 (60.3) | 77/108 (71.3) | Not estimable | Not pooled | Not pooled |
| No. of breakages (follow up: range 1–9 y) | |||||||||||
| 259 (4 observational studies) | Seriousa,b | Not serious | Not serious | Not serious | None | ⊕⊕⊕ ○ Moderate | 30/115 (26.1) | 58/144 (40.3) | Not estimable | Not pooled | Not pooled |
Artun et al. reported an unclear risk of Bias on the domains Random sequence generation (selection bias) and Allocation concealment (selection bias)
Schutz-Frasson et al. was classified as a moderae risk of bias, due to the retrospective definition of some aspects of the assignments of intervention
Al-Nimri et al. presents the stability as a secondary outcome
CI indicates confidence interval; RCT, randomized controlled trial.
DISCUSSION
Summary of Evidence
Among the five studies included in this review, differences were found between the performance of lower fixed retainers bonded to all lower anterior teeth and those bonded to canines only. Stormann and Ehmer22 and Al-Nimri et al.23 reported lower relapse rates when lower retainers were bonded to all teeth (canines and incisors). Artun et al.,21 Steinnes et al.,24 and Schutz-Frazon et al.25 reported no difference between the two types of retainers evaluated. Regarding the risk of bias, two studies were classified as high risk21,25 and the other studies as low risk.22–24
The better results that were reported for retainers bonded to all lower anterior teeth may be attributed to the reduced protrusive forces produced by the tongue during the retention phase. The lower retainers bonded only on the canines could result in protrusion of the incisors that were not bonded.29
The stability of tooth position during fixed orthodontic retention can also be influenced by other factors, such as breakage of the retainer,26,30 tooth rotation,31,32 increased intercanine distance,32 the diameter of retainer wire,26,32 and the follow-up duration.6,7 The occurrence of breakage during follow up between the two retainer designs was found to be different in only one study.22 That study reported a high rate of breakage for retainers bonded on all anterior teeth.22 Even though the breakage of fixed retainers was previously associated with poor stability,26,30 in this specific study,22 no relapse on orthodontic treatment was reported.
Another factor previously shown to influence the stability of orthodontic treatment was the presence of tooth rotations corrected during treatment.31,32 A high Irregularity Index (80%) was associated with relapse of tooth rotations in two included studies.22,23 The return of rotations seemed to be related to the amount of rotation before treatment.31,32 An increase in intercanine distance during treatment has also been shown to be a cause of relapse of the crowding of anterior lower teeth.32 In this review, no changes in intercanine distance were detected in the studies.22,23
The wire thickness of the retainers used was different in the various studies included in this review.21–25 Canine-to-canine retainers can be made with stainless-steel twisted archwires or plain stainless-steel archwires.9 The twisted archwires have been described as very elastic and highly resilient,33 allowing for physiological movement of the teeth, in addition to having a design that offers great mechanical retention of the material.5 One study21 included in this review suggested that twisted archwires were more effective in tooth alignment maintenance. This result was in agreement with the findings of another study,31 which reported less adverse effects31 as compared to those associated with retainers made of plain stainless-steel bonded only on canines.34 It is suggested that the use of twisted archwires is a safer alternative to prevent unexpected movements during the retention phase.34
Limitations
The variation in follow-up time may have been a factor contributing to the differences found between the studies. Artun et al.,21 Steinnes et al.,24 and Schutz-Frazon et al.25 observed that there was no difference in stability between the two types of retainers, those bonded to all teeth or those bonded only to canines, at 3, 8, and 9 years of follow up, respectively. However, all of the included studies21–25 identified that the retainers bonded to all teeth resulted in adequate stability, comparing for 3, 2, 1, 8, or 9 years, respectively. In the long term, this stability seemed to remain regardless of the type of retainer. There was evidence that restraint stability was effective in the long term6,7 and that the highest relapse rate occurred during the first 2 years.6
Regarding the sample size, none of the studies21–25 performed a power calculation to determine the appropriate sample size. The absence of sample calculations was previously reported as a common characteristic in orthodontic journals.35 The use of nonstatistical factors to assess sample size may compromise the validity of the results and the conclusions found.36 However, in the studies included, the samples used appeared to be large enough.
Among the randomized trials included in this review, a high risk of bias was detected in one study21 and a low risk was found22 in another study. Among the three nonrandomized studies, two were classified as low risk23,24 and one25 as high risk.
Randomization in controlled clinical studies is an essential step ensuring reliability of the sample allocation and, consequently, influencing the validity of the results.37 Thus, even with a low risk of bias from the evaluation of a suitable tool for nonrandomized studies,19 two studies included in this review23,25 were still less robust due to the absence of a randomized design.
In the fields of random sequence generation and allocation concealment, an uncertain risk was identified in one study21 due to the absence of precise information regarding the method of randomization. An attempt to contact the authors was conducted, but the author was not able to clarify the method used. It is essential to perform adequate allocation concealment to reduce selection bias for confounding factors and to improve the internal validity of the study and influence the clinical outcome.37
Regarding the field of incomplete outcome data, the study by Artun et al.21 was classified as high risk of bias since patients were abandoned as a result of bonding failure, causing an uneven distribution among genders, age, and gingival state. The loss of these patients may have impaired evaluation of the final results since it can generate failures in the homogeneity of the evaluated groups. In the other risks of bias domain in the same study it was identified that the principal investigator was not available for all contention maintenance and routine clinical practice and that absence of the primary evaluator may have represented a systematic error within the sample.21 A failure of the executed measurements assessment may have implications in the dimensioning of the size of the sample examined, generating a lack of reliability of the obtained data.35
Overall, the studies have suggested there was better stability and a higher rate of breakage in lower retainers bonded on all anterior teeth, with a certainty varying from very low to moderate. Even though the results suggested better outcomes from retainers bonded to all lower anterior teeth, the clinical decision made for individual patients may involve subjective factors, such as the professional training of the provider and the patient's compliance/acceptance. Inclusion of these variables in further studies may help in developing a more reliable conclusion.
CONCLUSIONS
The current evidence may point to better stability of dental alignment when lower fixed orthodontic retainers are bonded to all anterior teeth.
However, as uncertainty is moderate, more reliable research on the topic is needed to clarify some of the contradictions among the studies included.
APPENDIX 1.
Database and Search Strategies
| Database |
Search Strategy |
| PubMed | #1 (((((((((((((((((Orthodontic Patients[Title/Abstract]) OR Patients with bonded retainer [Title/Abstract]) OR Patients with orthodontic retainers [Title/Abstract]) OR Patients after orthodontic treatment [Title/Abstract]) OR Patients of the finishing phase of orthodontic treatment [Title/Abstract]) OR Patients adults [Title/Abstract]) OR Young patients [Title/Abstract]) OR Orthodontic appliance [MeSH Terms]) OR Orthodontic appliance [Title/Abstract]) OR Appliance, Orthodontic [Title/Abstract]) OR Appliances, Orthodontic [Title/Abstract]) OR Orthodontic, Appliances [Title/Abstract]) OR Fixed orthodontic appliance [Title/Abstract]) OR Fixed appliance [Title/Abstract]) OR Orthodontic treatment [Title/Abstract])) AND #2 (((((((((((((((((((((((((((((((Canine to canine retainer [Title/Abstract]) OR Bonded only to the canines [Title/Abstract]) OR Bonded to the canines only [Title/Abstract]) OR Bonded orthodontic canine to canine retainers [Title/Abstract]) OR Bonded orthodontic canine to canine retainer [Title/Abstract]) OR Bonded to two teeth [Title/Abstract]) OR Bonded from canine to canine [Title/Abstract]) OR (Canine [Title/Abstract] AND canine retainer [Title/Abstract])) OR (Canine [Title/Abstract] AND canine retainers [Title/Abstract])) OR Canine-and-canine retainer [Title/Abstract]) OR Canine-and-canine retainers [Title/Abstract]) OR Canine-to-canine retainers [Title/Abstract]) OR Canine-to-canine retainer [Title/Abstract]) OR Canine to canine retainers [Title/Abstract]) OR Canine to canine lingual retainer [Title/Abstract]) OR Canine to canine lingual retainers [Title/Abstract]) OR Canine-to-canine lingual retainers [Title/Abstract]) OR Canine-to-canine lingual retainer [Title/Abstract]) OR Canine-to-canine lingual retainers bonded to two [Title/Abstract]) OR Canine-to-canine lingual retainer bonded to two [Title/Abstract]) OR Lower canine-to-canine retainer [Title/Abstract]) OR Lower canine-to-canine retainers [Title/Abstract]) OR Lower canine to canine retainer [Title/Abstract]) OR Lower canine to canine retainers [Title/Abstract]) OR Orthodontic mandibular canine-to-canine retainers [Title/Abstract]) OR Orthodontic mandibular canine-to-canine retainer [Title/Abstract]) OR Retainers canine-to-canine [Title/Abstract]) OR Retainer canine-to-canine [Title/Abstract]) OR Retainer canine-and-canine [Title/Abstract]) OR Retainers canine-and-canine [Title/Abstract]) OR Types of mandibular canine-to-canine retainers [Title/Abstract])) AND #3 ((((((((((((((((((((((((((((((((((((((((((((Orthodontic Retainers [MeSH Terms]) OR Orthodontic Retainers [Title/Abstract]) OR Retainers, Orthodontic [Title/Abstract]) OR Orthodontic, Retainer [Title/Abstract]) OR Retainer, Orthodontic [Title/Abstract]) OR Bonded to all mandibular anterior teeth [Title/Abstract]) OR Bonded to six teeth [Title/Abstract]) OR Bonded to each tooth [Title/Abstract]) OR (Bonded to incisors [Title/Abstract] AND canines [Title/Abstract])) OR Bonded retainers [Title/Abstract]) OR Bonded retainer [Title/Abstract]) OR Bonded lingual retainers [Title/Abstract]) OR Bonded lingual retainer [Title/Abstract]) OR Bonded mandibular retainers [Title/Abstract]) OR Bonded mandibular retainer [Title/Abstract]) OR Bonding a retainer [Title/Abstract]) OR Bonding a retainers [Title/Abstract]) OR Bonded to all six anterior teeth [Title/Abstract]) OR Direct bonded lingual retainers [Title/Abstract]) OR Direct bonded lingual retainer [Title/Abstract]) OR Direct bonded lingual retainers [Title/Abstract]) OR Direct bonding of retainer [Title/Abstract]) OR Direct bonding of retainers [Title/Abstract]) OR Fixed retainers [Title/Abstract]) OR Fixed retainer [Title/Abstract]) OR Fixed lingual retainers [Title/Abstract]) OR Fixed lingual retainer [Title/Abstract]) OR Fixed lingual retention [Title/Abstract]) OR Fixed mandibular retainer [Title/Abstract]) OR Fixed mandibular retainers [Title/Abstract]) OR Lingual retainers [Title/Abstract]) OR Lingual retainer [Title/Abstract]) OR Lingual retainers bonded to six teeth [Title/Abstract]) OR Lingual retainer bonded to six teeth [Title/Abstract]) OR Mandibular bonded retainers [Title/Abstract]) OR Mandibular bonded retainer [Title/Abstract]) OR Mandibular retainers [Title/Abstract]) OR Mandibular retainer [Title/Abstract]) OR Mandibular anterior teeth retained [Title/Abstract]) OR Orthodontic fixed retainer [Title/Abstract]) OR Orthodontic fixed retainers [Title/Abstract]) OR Orthodontic retainer [Title/Abstract]) OR Retainer bonded to six teeth [Title/Abstract]) OR Retainers bonded to six teeth [Title/Abstract]) Final search: #1 AND #2 AND #3 |
| Scopus | ((TITLE-ABS-KEY (“Orthodontic Patients”) OR TITLE-ABS-KEY (“Patients with bonded retainer”) OR TITLE-ABS-KEY (“Patients with orthodontic retainers”) OR TITLE-ABS-KEY (“Patients after orthodontic treatment”) OR TITLE-ABS-KEY (“Patients of the finishing phase of orthodontic treatment”) OR TITLE-ABS-KEY (“Patients adults”) OR TITLE-ABS-KEY (“Young patients”) OR TITLE-ABS-KEY (“Orthodontic appliance”) OR TITLE-ABS-KEY (“Fixed orthodontic appliance”) OR TITLE-ABS-KEY (“Fixed appliance”) OR TITLE-ABS-KEY (“Orthodontic treatment”))) AND (((TITLE-ABS-KEY (“Canine to canine retainer”) OR TITLE-ABS-KEY (“Bonded only to the canines”) OR TITLE-ABS-KEY (“Bonded to the canines only”) OR TITLE-ABS-KEY (“Bonded orthodontic canine to canine retainers”) OR TITLE-ABS-KEY (“Bonded orthodontic canine to canine retainer”) OR TITLE-ABS-KEY (“Bonded to two teeth”) OR TITLE-ABS-KEY (“Bonded from canine to canine”) OR TITLE-ABS-KEY (“Canine and canine retainer”) OR TITLE-ABS-KEY (“Canine and canine retainers”) OR TITLE-ABS-KEY (“Canine-and-canine retainer”) OR TITLE-ABS-KEY (“Canine-and-canine retainers”) OR TITLE-ABS-KEY (“Canine-to-canine retainers”) OR TITLE-ABS-KEY (“Canine-to-canine retainer”) OR TITLE-ABS-KEY (“Canine to canine retainers”) OR TITLE-ABS-KEY (“Canine to canine lingual retainer”) OR TITLE-ABS-KEY (“Canine to canine lingual retainers”))))) OR (( TITLE-ABS-KEY (“Canine-to-canine lingual retainers”) OR TITLE-ABS-KEY (“Canine-to-canine lingual retainer”) OR TITLE-ABS-KEY (“Canine-to-canine lingual retainers bonded to two”) OR TITLE-ABS-KEY (“Canine-to-canine lingual retainer bonded to two”) OR TITLE-ABS-KEY (“Lower canine-to-canine retainer”) OR TITLE-ABS-KEY (“Lower canine-to-canine retainers”) OR TITLE-ABS-KEY (“Lower canine to canine retainer”) OR TITLE-ABS-KEY (“Lower canine to canine retainers”) OR TITLE-ABS-KEY (“Orthodontic mandibular canine-to-canine retainers”) OR TITLE-ABS-KEY (“Orthodontic mandibular canine-to-canine retainer”) OR TITLE-ABS-KEY (“Retainers canine-to-canine”) OR TITLE-ABS-KEY (“Retainer canine-to-canine”) OR TITLE-ABS-KEY (“Retainer canine-and-canine”) OR TITLE-ABS-KEY (“Retainers canine-and-canine”) OR TITLE-ABS-KEY (“Types of mandibular canine-to-canine retainers”)))))) AND (((((((( TITLE-ABS-KEY (“Orthodontic Retainers”) OR TITLE-ABS-KEY (“Bonded to all mandibular anterior teeth”) OR TITLE-ABS-KEY (“Bonded to six teeth”) OR TITLE-ABS-KEY (“Bonded to each tooth”) OR TITLE-ABS-KEY (“Bonded to incisors and canines”) OR TITLE-ABS-KEY (“Bonded retainers”) OR TITLE-ABS-KEY (“Bonded retainer”) OR TITLE-ABS-KEY (“Bonded lingual retainers”) OR TITLE-ABS-KEY (“Bonded lingual retainer”) OR TITLE-ABS-KEY (“Bonded mandibular retainers”) OR TITLE-ABS-KEY (“Bonded mandibular retainer”) OR TITLE-ABS-KEY (“Bonding a retainer”) OR TITLE-ABS-KEY (“Bonding a retainers”) OR TITLE-ABS-KEY (“Bonded to all six anterior teeth”) OR TITLE-ABS-KEY (“Direct bonded lingual retainers”) OR TITLE-ABS-KEY (“Direct bonded lingual retainer”) OR TITLE-ABS-KEY (“Direct bonding of retainer”) OR TITLE-ABS-KEY (“Direct bonding of retainers”) OR TITLE-ABS-KEY (“Fixed retainers”) OR TITLE-ABS-KEY (“Fixed retainer”))))) OR (( TITLE-ABS-KEY (“Fixed lingual retainers”) OR TITLE-ABS-KEY (“Fixed lingual retainer”) OR TITLE-ABS-KEY (“Fixed lingual retention”) OR TITLE-ABS-KEY (“Fixed mandibular retainer”) OR TITLE-ABS-KEY (“Fixed mandibular retainers”) OR TITLE-ABS-KEY (“Lingual retainers”) OR TITLE-ABS-KEY (“Lingual retainer”) OR TITLE-ABS-KEY (“Lingual retainers bonded to six teeth”) OR TITLE-ABS-KEY (“Lingual retainer bonded to six teeth”) OR TITLE-ABS-KEY (“Mandibular bonded retainers”) OR TITLE-ABS-KEY (“Mandibular bonded retainer”) OR TITLE-ABS-KEY (“Mandibular retainers”) OR TITLE-ABS-KEY (“Mandibular retainer”) OR TITLE-ABS-KEY (“Mandibular anterior teeth retained”) OR TITLE-ABS-KEY (“Orthodontic fixed retainer”) OR TITLE-ABS-KEY (“Orthodontic fixed retainers”) OR TITLE-ABS-KEY (“Orthodontic retainer”) OR TITLE-ABS-KEY (“Retainer bonded to six teeth”) OR TITLE-ABS-KEY (“Retainers bonded to six teeth”)))))) |
| Web of Science | #1 Tópico: (“Orthodontic Patients”) OR Tópico: (“Patients with bonded retainer”) OR Tópico: (“Patients with orthodontic retainers”) OR Tópico: (“Patients after orthodontic treatment”) OR Tópico: (“Patients of the finishing phase of orthodontic treatment”) OR Tópico: (“Patients adults”) OR Tópico: (“Young patients”) OR Tópico: (“Orthodontic appliance”) OR Tópico: (“Fixed orthodontic appliance”) OR Tópico: (“Fixed appliance”) OR Tópico: (“Orthodontic treatment”) #2 Tópico: (“Canine to canine retainer”) OR Tópico: (“Bonded only to the canines”) OR Tópico: (“Bonded to the canines only”) OR Tópico: (“Bonded orthodontic canine to canine retainers”) OR Tópico: (“Bonded orthodontic canine to canine retainer”) OR Tópico: (“Bonded to two teeth”) OR Tópico: (“Bonded from canine to canine”) OR Tópico: (“Canine and canine retainer”) OR Tópico: (“Canine and canine retainers”) OR Tópico: (“Canine-and-canine retainer”) OR Tópico: (“Canine-and-canine retainers”) OR Tópico: (“Canine-to-canine retainers”) OR Tópico: (“Canine-to-canine retainer”) OR Tópico: (“Canine to canine retainers”) OR Tópico: (“Canine to canine lingual retainer”) OR Tópico: (“Canine to canine lingual retainers”) Tópico: (“Canine-to-canine lingual retainers”) OR Tópico: (“Canine-to-canine lingual retainer”) OR Tópico: (“Canine-to-canine lingual retainers bonded to two”) OR Tópico: (“Canine-to-canine lingual retainer bonded to two”) OR Tópico: (“Lower canine-to-canine retainer”) OR Tópico: (“Lower canine-to-canine retainers”) OR Tópico: (“Lower canine to canine retainer”) OR Tópico: (“Lower canine to canine retainers”) OR Tópico: (“Orthodontic mandibular canine-to-canine retainers”) OR Tópico: (“Orthodontic mandibular canine-to-canine retainer”) OR Tópico: (“Retainers canine-to-canine”) OR Tópico: (“Retainer canine-to-canine”) OR Tópico: (“Retainer canine-and-canine”) OR Tópico: (“Retainers canine-and-canine”) OR Tópico: (“Types of mandibular canine-to-canine retainers”) #3 Tópico: (“Orthodontic Retainers”) OR Tópico: (“Bonded to all mandibular anterior teeth”) OR Tópico: (“Bonded to six teeth”) OR Tópico: (“Bonded to each tooth”) OR Tópico: (“Bonded to incisors and canines”) OR Tópico: (“Bonded retainers”) OR Tópico: (“Bonded retainer”) OR Tópico: (“Bonded lingual retainers”) OR Tópico: (“Bonded lingual retainer”) OR Tópico: (“Bonded mandibular retainers”) OR Tópico: (“Bonded mandibular retainer”) OR Tópico: (“Bonding a retainer”) OR Tópico: (“Bonding a retainers”) OR Tópico: (“Bonded to all six anterior teeth”) OR Tópico:(“Direct bonded lingual retainers”) OR Tópico: (“Direct bonded lingual retainer”) OR Tópico: (“Direct bonding of retainer”) OR Tópico: (“Direct bonding of retainers”) OR Tópico: (“Fixed retainers”) OR Tópico: (“Fixed retainer”) Tópico: (“Fixed lingual retainers”) OR Tópico: (“Fixed lingual retainer”) OR Tópico: (“Fixed lingual retention”) OR Tópico: (“Fixed mandibular retainer”) OR Tópico: (“Fixed mandibular retainers”) OR Tópico: (“Lingual retainers”) OR Tópico: (“Lingual retainer”) OR Tópico: (“Lingual retainers bonded to six teeth”) OR Tópico: (“Lingual retainer bonded to six teeth”) OR Tópico: (“Mandibular bonded retainers”) OR Tópico: (“Mandibular bonded retainer”) OR Tópico: (“Mandibular retainers”) OR Tópico: (“Mandibular retainer”) OR Tópico: (“Mandibular anterior teeth retained”) OR Tópico: (“Orthodontic fixed retainer”) OR Tópico: (“Orthodontic fixed retainers”) OR Tópico: (“Orthodontic retainer”) OR Tópico: (“Retainer bonded to six teeth”) OR Tópico: (“Retainers bonded to six teeth”) Final search: #1 AND #2 AND #3 |
| The Cochrane Library | '"Orthodontic Patients” OR “Patients with bonded retainer” OR “Patients with orthodontic retainers” OR “Patients after orthodontic treatment” OR “Patients of the finishing phase of orthodontic treatment” OR “Patients adults” OR “Young patients” OR “Orthodontic appliance” OR “Fixed orthodontic appliance” OR “Fixed appliance” OR “Orthodontic treatment” in Title, Abstract, Keywords and “Canine to canine retainer” OR “Bonded only to the canines” OR “Bonded to the canines only” OR “Bonded orthodontic canine to canine retainers” OR “Bonded orthodontic canine to canine retainer” OR “Bonded to two teeth” OR “Bonded from canine to canine” OR “Canine and canine retainer” OR “Canine and canine retainers” OR “Canine-and-canine retainer” OR “Canine-and-canine retainers” OR “Canine-to-canine retainers” OR “Canine-to-canine retainer” OR “Canine to canine retainers” OR “Canine to canine lingual retainer” OR “Canine to canine lingual retainers” OR “Canine-to-canine lingual retainers” OR “Canine-to-canine lingual retainer” OR “Canine-to-canine lingual retainers bonded to two” OR “Canine-to-canine lingual retainer bonded to two” OR “Lower canine-to-canine retainer” OR “Lower canine-to-canine retainers” OR “Lower canine to canine retainer” OR “Lower canine to canine retainers” OR “Orthodontic mandibular canine-to-canine retainers” OR “Orthodontic mandibular canine-to-canine retainer” OR “Retainers canine-to-canine” OR “Retainer canine-to-canine” OR “Retainer canine-and-canine” OR “Retainers canine-and-canine” “Types of mandibular canine-to-canine retainers” in Title, Abstract, Keywords and “Orthodontic Retainers” OR “Bonded to all mandibular anterior teeth” OR “Bonded to six teeth” OR “Bonded to each tooth” OR “Bonded to incisors and canines” OR “Bonded retainers” OR “Bonded retainer” OR “Bonded lingual retainers” OR “Bonded lingual retainer” OR “Bonded mandibular retainers” OR “Bonded mandibular retainer” OR “Bonding a retainer” OR “Bonding a retainers” OR “Bonded to all six anterior teeth” OR “Direct bonded lingual retainers” OR “Direct bonded lingual retainer” OR “Direct bonding of retainer” OR “Direct bonding of retainers” OR “Fixed retainers” OR “Fixed retainer” OR “Fixed lingual retainers” OR “Fixed lingual retainer” OR “Fixed lingual retention” OR “Fixed mandibular retainer” OR “Fixed mandibular retainers” OR “Lingual retainers” OR “Lingual retainer” OR “Lingual retainers bonded to six teeth” OR “Lingual retainer bonded to six teeth” OR “Mandibular bonded retainers” OR “Mandibular bonded retainer” OR “Mandibular retainers” OR “Mandibular retainer” OR “Mandibular anterior teeth retained” OR “Orthodontic fixed retainer” OR “Orthodontic fixed retainers” OR “Orthodontic retainer” OR “Retainer bonded to six teeth” OR “Retainers bonded to six teeth” in Title, Abstract, Keywords in Trials' |
| Lilacs | (tw:(“Orthodontic Patients” OR “Patients with bonded retainer” OR “Patients with orthodontic retainers” OR “Patients after orthodontic treatment” OR “Patients of the finishing phase of orthodontic treatment” OR “Patients adults” OR “Young patients” OR “Orthodontic appliance” OR “Fixed orthodontic appliance” OR “Fixed appliance” OR “Orthodontic treatment”)) AND (tw:(“Canine to canine retainer” OR “Bonded only to the canines” OR “Bonded to the canines only” OR “Bonded orthodontic canine to canine retainers” OR “Bonded to two teeth” OR “Bonded from canine to canine” OR “Canine-and-canine retainer” OR “Canine-and-canine retainers” OR “Canine-to-canine retainers” OR “Canine to canine lingual retainer” OR “Canine-to-canine lingual retainers” OR “Canine-to-canine lingual retainers bonded to two” OR “Lower canine-to-canine retainer” OR “Orthodontic mandibular canine-to-canine retainers” OR “Retainers canine-to-canine” OR “Retainers canine-and-canine” OR “Types of mandibular canine-to-canine retainers”)) AND (tw:(“Orthodontic Retainers” OR “Orthodontic Retainer” OR “Bonded to all mandibular anterior teeth” OR “Bonded to six teeth” OR “Bonded to each tooth” OR “Bonded to incisors and canines” OR “Bonded retainers” OR “Bonded lingual retainers” OR “Bonded mandibular retainers” OR “Bonding a retainer” OR “Bonded to all six anterior teeth” OR “Direct bonded lingual retainers” OR “Direct bonding of retainer” OR “Fixed retainers” OR “Fixed lingual retainers” OR “Fixed lingual retention” OR “Fixed mandibular retainer” OR “Lingual retainers” OR “Lingual retainers bonded to six teeth” OR “Mandibular bonded retainers” OR “Mandibular retainers” OR “Mandibular anterior teeth retained” OR “Orthodontic fixed retainer” OR “Retainer bonded to six teeth”)) |
| Clinical Trials | #1: “Orthodontic patient” AND “Canine to canine retainer” AND “Orthodontic Retainers" #2: “Orthodontic patients” AND “Canine to canine retainer” AND “Bonded to six teeth" |
| OpenGrey | #1: “Orthodontic patients” AND “Canine to canine retainer” AND “Bonded to six teeth" #2: “Orthodontic patients” AND “Canine to canine retainer” AND “Orthodontic Retainers" |
| Google Scholar | #1: “Orthodontic patients” AND “Canine to canine retainer” AND “Orthodontic retainers” |
APPENDIX 2.
References Excluded from Title-Abstract Evaluation
| Reasons |
Reference |
| Have not evaluated stability | Artun J, Spadafora A, Shapiro P, McNeill R, Chapko M. Hygiene status associated with different types of bonded, orthodontic canine-to-canine retainers. A clinical trial. J Clinical Periodontol. 1987;14:89–94. (Ausência estabilidade) Neto JBC, Régio MRS, Martos J, Spautz F, Moraes GB. Analysis of the periodontal status of patients with mandibular-bonded retainers. Rev Odonto Ciênc. 2010;25:132–136. Hohoff A, Stamm T, Goder G, Sauerland C, Ehmer U, Seifert E. Comparison of 3 bonded lingual appliances by auditive analysis and subjective assessment. Am J Orthod Dentofacial Orthop. 2003;124:737–745. Rody WJ, Elmaraghy S, McNeight AM, et al. Effects of different orthodontic retention protocols on the periodontal health of mandibular incisors. Orthod Craniofac Res. 2016;19:198–208. Owens MJ. Efficacy of Tmporary Fixed Retention Following Comprehensive Orthodontic Treatment [thesis]. Nashville, Tenn: University of Tennessee; 2011. Sawhney B. Orthodontic Retainers: A Survey of Patient Compliance and Satisfaction [thesis]. Ontário, Canada): University of Western Ontario; 2013. |
| Have not compared the two types of bonding among retainers | Bjering R, Sandvik L, Midtb M, Vandevska-Radunovic V. Stability of anterior tooth alignment 10 years out of retention. J Orofac Orthop. 2017;78:275–283. Dyer KC, Vaden JL, Harris EF. Relapse revisited—again. Am J Orthod Dentofacial Orthop. 2012;142:221–227. Tynelius GE , Bondemark L, Lilja-Karlander E. Evaluation of orthodontic treatment after 1 year of retention—a randomized controlled Trial. Eur J Orthod. 2010;32:542–547. Tynelius GE, Bondemark L, Lilja-Karlander E. A randomized controlled trial of three orthodontic retention methods in Class I four premolar extraction cases—stability after 2 years in retention. Orthod Craniofac Res. 2013;16:105-15. Tynelius GE, Petren S, Bondemark L, Lilja-Karlander E. Five-year postretention outcomes of three retention methods—a randomized controlled Trial. Eur J Orthod. 2015;37:345–353. Tynelius GE. Orthodontic retention. Studies of retention capacity, cost-effectiveness and long-term stability. Swed Dent J Suppl. 2014;236:9–65. Kalha AS. Orthodontic retention to have and to hold. Evidence-Based Dent. 2016;17:105–106. Salehi P, Zarif Najafi H, Roeinpeikar SM. Comparison of survival time between two types of orthodontic fixed retainer: a prospective randomized clinical trial. Prog Orthod. 2013;14:25. Ferguson DJ, Makki L, Wilcko MT, Wilcko WM. Instability of the mandibular dental arch? Look again! Semin Orthod. 2017;232:178–196. Juloski J, Glisic B, Vandevska-Radunovic V. Long-term influence of fixed lingual retainers on the development of gingival recession: a retrospective, longitudinal cohort study. Angle Orthod. 2017;87:658–664. Kaji A, Sekino S, Ito H, Numabe Y. Influence of a mandibular fixed orthodontic retainer on periodontal health. Aust Orthod J. 2013;29:76–85. Lie Sam Foek DJ, Ozcan M, Verkerke GJ, Sandham A, Dijkstra PU. Survival of flexible, braided, bonded stainless steel lingual retainers: a historic cohort study. Eur J Orthod. 2008;30:199–204. Maddalone M, Rota E, Mirabelli L, Venino P, Porcaro G. Clinical evaluation of bond failures and survival of mandibular canine-to-canine bonded retainers during a 12-year time span. Int J Clin Pediatr Dent. 2017;10:330–334. Renkema AM, Al-Assad S, Bronkhorst E, et al. Effectiveness of lingual retainers bonded to the canines in preventing mandibular incisor relapse. Am J Orthod Dentofacial Orthop. 2008;134:179–180. Renkema AM, Navratilova Z, Mazurova K, Katsaros C, Fudalej PS. Gingival labial recessions and the post-treatment proclination of mandibular incisors. Eur J Orthod. 2015;37:508–513. Titón C, Rubio E. Contención y estabilidad. Rev. Odontol. Interdisc. 2002;3:40–45. |
| Systematic reviews | Littlewood SJ, Millett DT, Doubleday B, Bearn DR, Worthington HV. Retention procedures for stabilising tooth position after treatment with orthodontic braces. Cochrane Database Syst Rev. Jan 29;(1):CD002283. Madurantakam P, Kumar S. Fixed and removable orthodontic retainers and periodontal health. Evidence-Based Dent. 2017;18:103–104. |
| Opinion article | Vignesh PK, Sumathi Felicita A. Long term effectiveness of various orthodontic retention—a review. 2015;14:56–59. |
| Have not assessed orthodontic lower retainers | Arnold SN, Pandis N, Patcas R, Factors influencing fixed retention practices in German-speaking Switzerland. A survey. J Orofacial Orthop. 2014;75(6):446–458. Akkaya S, Alaçam A. The occurrence of cavitation after orthodontic bonding. A case report. Turk Ortod Derg. 1990;3:123–128. (Relato de caso) Al-Moghrabi D, Pandis N, Fleming PS. The effects of fixed and removable orthodontic retainers: a systematic review. Prog Orthod. 2016;17:24. Ardissono E, El Macdissi N, Adriana G, Peluffo P, Pérez R, Sito P. Reporte de cuatro casos clínicos. Rev Odontol Interdisc. 2000;1:41–46. Assumpção WK, Ota GKB, Ferreira RI, Cotrim-Ferreira FA. Orthodontic retainers: analysis of prescriptions sent to laboratories. Dental Press J Orthod. 2012;17:36.e1–36.e6. Bock NC, Saffar M, Hudel H, et al. Long-term effects of Class II orthodontic treatment on oral health. J Orofacial Orthop. 2018;79:96–108. Firoozmand LM, Brandão JVP, Fialho MPN. Influence of microhybrid resin and etching times on bleached enamel for the bonding of ceramic brackets. Braz Oral Res. 2013;27(2):142–148. De Goes MF, Giannini M, Di Hipólito V, et al. Microtensile bond strength of adhesive systems to dentin with or without application of an intermediate flowable resin layer. Braz Dent J. 2008;19:51–56. Egli F, Bovali E, Kiliaridis S, Conrnellis MA. Indirect vs direct bonding of mandibular fixed retainers in orthodontic patients: comparison of retainer failures and posttreatment stability. A 2-year follow-up of a single-center randomized controlled trial. Am J Orthod Dentofacial Orthop. 2017;151:15–27. Esperança TCD, Martins LP, Gandini LG Jr, Martins RP, Lomardi R. Posttreatment stability – Cases reports description. J Bras Ortodon Ortop Facial. 2005;10:409–419. Gallardo M. Tres casos de Classe II div. 1 severa tratados sin extracciones. Rev Ecua-Ortod. 1997;2:9–17. Gerami A, Dadgar S, Rakhshan V, Jannati P, Sobouti F. Displacement and force distribution of splinted and tilted mandibular anterior teeth under occlusal loads: an in silico 3D finite elements analysis. Prog Orthod. 2016;17(1):16. Goméz Goméz SL, Jaramilo Vallejos PM. Manejo ortodôntico de caninos maxilares retenidos. Rev Fac Odontol Univ Antioq. 2002;13:79–85. Habegger M, Renkema AM, Bronkhorst E, Fudalej PS, Katsaros C. A survey of general dentists regarding orthodontic retention procedures. Eur J Orthod. 2017;39:69–75. Hahn W, Fricke J, Frickie-Zech S, Zapf A, Gruber R, Sadat-Khonsari R. The use of a neodymium-iron-boron magnet device for positioning a multi-stranded wire retainer in lingual retention—a pilot study in humans. Eur J Orthod. 2008;30:433–436. Hotokezaka H, Matsuo T, Nakagawa M, Mizuno A, Kobayashi K. Severe dental open bite malocclusion with tongue reduction after orthodontic treatment. Angle Orthod. 2001;71:228–236. Mena-Serrano AP, Garcia EJ, Perez MM, et al. Effect of the application time of phosphoric acid and self-etch adhesive systems to sclerotic dentin. J Appl Oral Sci. 2013;21:196–202. Kloukos D, Sifakakis I, Eliades T, Brantley W. Bonding of fixed lingual retainers in orthodontics. In: Eliades T, Brandley W. Orthodontic Applications of Biomaterials: A Clinical Guide. United Kingdom: Woodhead Publishing; 2016. p. 241. Labunet AV, Badea M. In vivo orthodontic retainer survival—a review. Clujul Med. 2015;88:298. Lanzer B. Retention after orthodontic treatment—a literature review. Info Aus Orthod Kieferorthopaedie. 2018; 50(1):25–28. Lupatini PM, Vitral RWF, Campos MJS, Gravina MA, Fraga MR, Mota SL Jr. Assessment of long-term stability of leveling of the Curve of Spee after orthodontic treatment in mesocephalic patients—a pilot study. Pesqui Bras Odontopediatria Clín Integr. 2015;15:263–270. Nieves ATE. El tratamiento ortodóntico como auxiliar en el tratamiento restaurador. Acta Odontol Venez. 1998;36:54–61. Nunes L, Quintanilha L, Perinetti G, Capelli JJ. Effect of orthodontic force on expression levels of ten cytokines in gingival crevicular fluid. Arch Oral Biol. 2017;76:70–75. Orozco EE, Gurrola BM, Casasa AA. Tracción de canino maxilar izquierdo impactado con botón bondeable, ligadura metálica y cadena elastomérica. Int J Odontostomatol. 2017;11:77–82. Ozawa E, Honda EI, Parakonthun KN, et al. Influence of orthodontic appliance-derived artifacts on 3-T MRI movies. Prog Orthod. 2018;19:7. Pandis N, Fleming PS, Kloukos D, Polychronopoulou A, Katsaros C, Eliades T. Survival of bonded lingual retainers with chemical or photo polymerization over a 2-year period: a single-center, randomized controlled clinical trial. Am J Orthod Dentofacial Orthop. 2013;144:169–175. |
| Pinheiro FHSL, Garib DG, Janson G, Bombonatti R, Freitas MR. Longitudinal stability of rapid and slow maxillary expansion. Dental Press J Orthod. 2014;19:70–77. Ramazanzadeh B, Ahrari F, Hosseini ZS. The retention characteristics of Hawley and vacuum-formed retainers with different retention protocols. J Clin Exp Dent. 2018;10:e224–e231. Romano FL, Valério RA, Gomes-Silva JM, Ferreira JTL, Faria G, Borsatto MC. Clinical evaluation of the failure rate of metallic brackets bonded with orthodontic composites. Braz Dent J. 2012;23:399–402. Rose E, Frucht S, Jonas IE. Clinical comparison of a multistranded wire and a direct-bonded polyethylene ribbon-reinforced resin composite used for lingual retention. Quintessence Int. 2002;33:579–583. Rosé MM, Rosé RA. La extracción de segundos molares en el tratamiento de la mordida abierta: diagnóstico etiológico. Terapéutica. Una situación clínica. Ortodoncia. 2003;67:66–77. Scarpati AOEK. Fracture strength of different techniques for re-attachment of teeth submitted or not to endodontic treatment [thesis]. S�o Paulo:Faculdade de Odontologia;2007. Sfondrini MF, Fraticelli D, Castellazzi L, Scribante A, Gandini P. Clinical evaluation of bond failures and survival between mandibular canine-to-canine retainers made of flexible spiral wire and fiber-reinforced composite. J Clin Exp Dent. 2014;6:e145–e149. Shirasu BK, Hayacibara RM, Ramos AL. Comparison of periodontal parameters after use of orthodontic multi-stranded wire retainers and modified retainers. Rev Dent Press Ortod Ortop Facial. 2007;12:41–47. Sifakakis I, Eliades T, Bourauel C. Residual stress analysis of fixed retainer wires after in vitro loading: can mastication-induced stresses produce an unfavorable effect? Biomed Tech (Berl). 2015;60:617–622. Siqueira MR, Stanislawczuk R, Kossatz S, Reis A, Loguercio AD. Clinical evaluation of a self-adhesive material to bonded orthodontic brackets. Ortodontia. 2011;44:435–441. Souza RA, Pithon MM, Freitas LMA. [Skeletal Class II Retreatment with Mini-implants Orthodontics: case report]. Ortho Sci Orthod Sci Pract 2012;5:563–569. Sturno R, Chiappe G. Presentación de un caso donde se efectuó la rehabilitación gnatológica con un planeo y trabajo multidisciplinario. Ondontol Bonaer. 1999;22:7–9. Tanaka OM, Fornazari IA, Parra AXG, de Castilhos BB, Franco A. Complete Maxillary Crossbite Correction with a Rapid Palatal Expansion in Mixed Dentition Followed by a Corrective Orthodontic Treatment. Case Reports in Dentistry. 2016, 1–6. Varga S, Spalj S, Anic Milosevic S, et al. Changes of bite force and occlusal contacts in the retention phase of orthodontic treatment: a controlled clinical trial. Am J Orthod Dentofacial Orthop. 2017;152:767–777. Westerlund A, Oikimoui C, Ransjo M, Ekestubbe A, Bresin A, Lund H. Cone-beam computed tomographic evaluation of the long-term effects of orthodontic retainers on marginal bone levels. Am J Orthod Dentofacial Orthop. 2017;151:74–81. Wolf M, Schumacher P, Jager F, et al. Novel lingual retainer created using CAD/CA, technology evaluation of its positioning accuracy. J Orofacial Orthop Fortschritte Kieferorthopadie. 2015;76:164–174. Zreagat MA, Hassan R, Hanoun AF. CAD/CAM zirconium bar as a bonded mandibular fixed retainer: a novel approach with two-year follow-up. Case Rep Dent. 2017;1583403. |
APPENDIX 3: All attempts to contact any authors and their fate




REFERENCES
- 1.Angle EH. Treatment of Malocclusion of the Teeth Angle System. Philadelphia, Pa: The S. S. White Dental Manufacturing Company; 1907. [Google Scholar]
- 2.Proffit WR, Fields JR, Henry W. Contemporary Orthodontics. 2002. 3rd ed. St. Louis, Missouri: Elsevier;
- 3.Ursi WJS, Okazaki LK, Falleiros DAB. Fibrotomia circunferencial supra-alveolar. Ortodontia. 1998;31(1):97–103. [Google Scholar]
- 4.Maia NG, Normando D, Maia FA, Ferreira MAF, do Socorro Costa Feitosa Alves M. Factors associated with long-term patient satisfaction. Angle Orthod. 2010;80(6):1155–8. doi: 10.2319/120909-708.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Normando D, Capelozza Filho L. A method to re-treat the relapse of dental misalignment. Dental Press J Orthod. 2011;16(5):48–53. [Google Scholar]
- 6.Al Yami EA, Kuijpers-Jagtman AM, van‘t Hof MA. Stability of orthodontic treatment outcome: follow-up until 10 years postretention. Am J Orthod Dentofacial Orthop. 1999;115:300–304. doi: 10.1016/s0889-5406(99)70333-1. [DOI] [PubMed] [Google Scholar]
- 7.Booth FA, Edelman JM, Proffit WR. Twenty-year follow-up of patients with permanently bonded mandibular canine-to-canine retainers. Am J Orthod Dentofacial Orthop. 2008;133:70–76. doi: 10.1016/j.ajodo.2006.10.023. [DOI] [PubMed] [Google Scholar]
- 8.Oppenheim A. The crisis in orthodontia. Int J Orthod. 1934;20:242–254. [Google Scholar]
- 9.Silva Filho OG, Kubitski M, Marinho E. Lower orthodontic fixed retainer 3×3: considerations on confection, direct bonding and removal. Rev Dental Press Ortod Ortop Facial. 2004;3:17–24. [Google Scholar]
- 10.Corbett AI, Leggitt VL, Angelov N, Olson G, Caruso JM. Periodontal health of anterior teeth with two types of fixed retainers. Angle Orthod. 2015;85:699–705. doi: 10.2319/060314-398.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Al-Moghrabi D, Nikolaos P, Padhraing FS. The effects of fixed and removable orthodontics retainers: a systematic review. Prog Orthod. 2016;17:24. doi: 10.1186/s40510-016-0137-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Bahije M, Ennaji A, Benyahia H, Zaoui F. A systematic review of orthodontic retention systems: the verdict. Int Orthod. 2018;16:409–424. doi: 10.1016/j.ortho.2018.06.023. [DOI] [PubMed] [Google Scholar]
- 13.Buzatta LN, Shimizu RH, Shimizu IA, et al. Gingival condition associated with two types of orthodontic fixed retainers: a meta-analysis. Eur J Orthod. 2017 Aug 1;39(4):446–452. doi: 10.1093/ejo/cjw057. [DOI] [PubMed] [Google Scholar]
- 14.Littlewood SJ, Millett DT, Doubleday B, Bearn DR, Worthington HV. Retention procedures for stabilising tooth position after treatment with orthodontic braces. Cochrane Database Syst Rev. 2016. 1:CD002283. [DOI] [PubMed]
- 15.Littlewood SJ, Kandasamy S, Huang G. Retention and relapse in clinical practice. Aust Dent J. 2017;62(suppl 1):51–57. doi: 10.1111/adj.12475. [DOI] [PubMed] [Google Scholar]
- 16.Padmos JAD, Fudalei PS, Renkema AM. Epidemiologic study of orthodontic retention procedures. Am J Orthod Dentofacial Orthop. 2018;153:496–504. doi: 10.1016/j.ajodo.2017.08.013. [DOI] [PubMed] [Google Scholar]
- 17.Moher D, Liberati A, Tetzlaff J, Altman DG, Group P Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6:e1000097. doi: 10.1371/journal.pmed.1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Higgins JP, Altman DG, Gotzsche PC, et al. The Cochrane Collaboration’s tool for assessing risk of bias randomized trials. BMJ. 2011. Oct 18;343:d5928. [DOI] [PMC free article] [PubMed]
- 19.Higgins JP, Savovic J, Page MJ, et al. Revised Cochrane risk of bias tool for randomized trials (Rob 2.0) Cochrane Handbook. 2016. Oct,
- 20.Balshem H, Helfand M, Schunemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64:401–406. doi: 10.1016/j.jclinepi.2010.07.015. [DOI] [PubMed] [Google Scholar]
- 21.Artun J, Spadafora AT, Shapiro AP. A 3-year follow-up study of various types of orthodontic canine-to-canine retainers. Eur J Orthod. 1997 Oct;19(5):501–509. doi: 10.1093/ejo/19.5.501. [DOI] [PubMed] [Google Scholar]
- 22.Stormann I, Ehmer U. A prospective randomized study of different retainer types. J Orofacial Orthop/FortschrKieferorthop. 2002;63:42–50. doi: 10.1007/s00056-002-0040-6. [DOI] [PubMed] [Google Scholar]
- 23.Kazem Al-Nimri Rola Al H, Mohamed O. Gingival health and relapse tendency: a prospective study of two types of lower fixed retainers. Aust Orthod J. 2009;25:142–146. [PubMed] [Google Scholar]
- 24.Steinnes J, Johnsen G, Kerosuob H. Stability of orthodontic treatment outcome in relation to retention status: an 8-year follow-up. Am J Orthod Dentofacial Orthop. 2017;151:1027–1033. doi: 10.1016/j.ajodo.2016.10.032. [DOI] [PubMed] [Google Scholar]
- 25.Schutz-Frazon U, Lindsten R, Bjerklin K, Bondemark L. Twelve-year follow-up of mandibular incisor stability: comparison between two bonded lingual orthodontic retainers. Angle Orthod. 2017;87:200–208. doi: 10.2319/031716-227.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Watted N, Wieber M, Teuscher T, Schmitz N. Comparison of incisor mobility after insertion of canine-to-canine lingual retainers bonded to two or to six teeth. J Orofac Orthop. 2001;62:387–396. doi: 10.1007/pl00001944. [DOI] [PubMed] [Google Scholar]
- 27.Little RM. The Irregularity Index: a quantitative score of mandibular anterior alignment. Am J Orthod. 1975;68:554–563. doi: 10.1016/0002-9416(75)90086-x. [DOI] [PubMed] [Google Scholar]
- 28.Richmond S, Shaw WC, Roberts CT, Andrews M. The PAR index (peer assessment rating): methods to determine outcome of orthodontic treatment in terms of improvement and standards. Eur J Orthod. 1992;14:180–187. doi: 10.1093/ejo/14.3.180. [DOI] [PubMed] [Google Scholar]
- 29.Zachrisson BU. On excellence in finishing, Part II. J Clin Orthod. 1986;20:536–556. [PubMed] [Google Scholar]
- 30.Renkema AM, Al-Assad S, Bronkhorst E, Weindel S, Katsaros C, Lisson JA. Effectiveness of lingual retainers bonded to the canines in preventing mandibular incisor relapse. Am J Orthod Dentofacial Orthop. 2008;134:179e1–179e8. doi: 10.1016/j.ajodo.2008.06.003. [DOI] [PubMed] [Google Scholar]
- 31.Renkema AM. Long-term effectiveness of canine-to-canine bonded flexible spiral wire lingual retainers. Am J Orthod Dentofacial Orthop. 2011;139:614–621. doi: 10.1016/j.ajodo.2009.06.041. [DOI] [PubMed] [Google Scholar]
- 32.Wolf M, Schulte U, Kupper K, et al. Post-treatment changes in permanent retention. J Orofac Orthop. 2016;77:446–453. doi: 10.1007/s00056-016-0054-0. [DOI] [PubMed] [Google Scholar]
- 33.Gravina MA, Motta ATS, Almeida MAO, Quintão CCA. Orthodontic wires: knowledge to optimize clinical application. Rev Dental Press Orthod Ortop Facial. 2014;9:113–128. [Google Scholar]
- 34.Kucera J, Marek I. Unexpected complications associated with mandibular fixed retainers: a retrospective study. Am J Orthod Dentofacial Orthop. 2016;149:202–211. doi: 10.1016/j.ajodo.2015.07.035. [DOI] [PubMed] [Google Scholar]
- 35.Normando D, Almeida MAO, Quintão CCA. Analysis of the use of sample size calculation and error of method in research published in Brazilian and international orthodontic journals. Dental Press J Orthod. 2011;16:33.e1–33.e9. [Google Scholar]
- 36.Pandis N, Polychronopoulou A, Eliades T. Sample size estimation: an overview with applications to orthodontic clinical trial design. Am J Orthod Dentofacial Orthop. 2011;140:e141–e146. doi: 10.1016/j.ajodo.2011.04.021. [DOI] [PubMed] [Google Scholar]
- 37.Pandis N. Randomized clinical trials (RCTs) and systematic reviews (SRs) in the context of evidence-based orthodontics (EBO) Semin Orthod. 2013;19:142–157. [Google Scholar]