

Abstract
Case series
Patients: Female, 34-year-old • Female, 36-year-old
Final Diagnosis: Leiomyoma
Symptoms: Pregnancy
Medication: —
Clinical Procedure: Myomectomy
Specialty: Obstetrics and Gynecology
Objective:
Unusual setting of medical care
Background:
No standard guidelines have been specified for a cesarean myomectomy, and several centers remain divided on the justification to perform this procedure, especially for large fibroids. Only a few case reports have been published of cesarean myomectomy for large fibroids. Here, we report 2 cases of successful cesarean myomectomies for large fibroids (>15 cm) during the 38th week of pregnancy.
Case Reports:
We encountered 2 primigravida patients, aged 34 and 36 years, respectively, with large fibroids >15 cm in diameter. Using the Pfannenstiel incision, we performed cesarean myomectomies in both patients at term pregnancy. The surgeries were performed by a gynecologic oncologist in a tertiary hospital. Both patients experienced a postoperative decrease in hemoglobin but neither required a blood transfusion. Three days after the operation, the patients were discharged from the hospital in good condition. One year later, the patients and their babies continued to be in good health. The patients did not experience chronic pelvic pain or menstrual abnormalities. Neither patient is currently planning another pregnancy.
Conclusions:
Based on our report, it may be assumed that cesarean myomectomy for a large fibroid (even for fibroids >15 cm in diameter) is safe if performed by experts in a tertiary hospital. Further larger studies of cesarean myomectomy of large fibroids are required to confirm the safety of this procedure.
Keywords: Cesarean Section, Leiomyoma, Myoma, Uterine Myomectomy
Background
Cesarean myomectomy remains controversial [1,2]. There are currently no standard guidelines regarding myomectomy at the time of cesarean section. Some centers delay myomectomy to prevent potential heavy bleeding due to myomectomy. However, some studies support the safety of cesarean myomectomy [2,3]. We report 2 cases of successful cesarean myomectomy of large fibroids (diameter >15 cm).
Case Reports
Case 1
The first case was of a 34-year-old primigravida non-smoker with existing fibroids before pregnancy. Her only symptom of fibroids prior to the pregnancy was being aware of a lump in her abdomen. She had been married for 6 months. Her height, weight, and body mass index were 145 cm, 55 kg, and 26.2 kg/m2, respectively. The first-trimester ultrasound revealed a large fibroid (diameter: 16 cm) in the fundus. The growth of the fetus during antenatal care was normal, and there was no malpresentation. The size of the fibroids did not increase during pregnancy, and the patient did not experience fibroid-related complications. She did not develop hypertension, diabetes mellitus, or any other disorders during pregnancy. The short-term complications of cesarean myomectomy, such as hemorrhage, and the long-term complications, such as chronic pelvic pain, abnormal menstruation, infertility, fibroid recurrence, and the risk of uterine rupture during subsequent pregnancies were explained to the patient. After she had provided written informed consent for the procedure, a cesarean section with spinal anesthesia was performed during the 38th week of pregnancy. The fetus was in the cephalic position. A Pfannenstiel incision was performed (Figure 1). After the baby was delivered, the uterus was exteriorized to facilitate exploration. A bolus push of 10 IU of oxytocin was administered intravenously to induce uterine contractions. Three fibroids were detected. A large intramural fibroid was observed on the left corpus up to the fundus, and the 2 smaller fibroids were observed adjacent to the large fibroid (Figure 2). The large fibroid was removed through the cesarean section incision in the lower segment of the uterus (Figure 3). The smaller fibroids were removed through the new uterine incision above the fibroids (Figure 4). Two-layer closure of the uterine wall was performed using Monosyn 1.0. The operative time was 1 h and 10 min. The baby weighed 2800 g, and the blood loss during surgery was 400 cc. The hemoglobin levels were 10.5 and 8.8 g/dL before and after surgery, respectively. No blood transfusions were administered. The patient was discharged from the hospital 3 days after surgery. The mother and the baby were in good condition. Histopathological examination confirmed the diagnosis of a fibroid with dimensions 17×16×14 cm. Cystic and hyaline degenerations were observed in the fibroid.
Figure 1.

Case 1. Pfannenstiel incision with hypervascularization is observed in the lower segment of the uterus.
Figure 2.

Case 1. After the baby is delivered, the uterus is exteriorized and the fibroids are observed in the uterine corpus-fundus.
Figure 3.
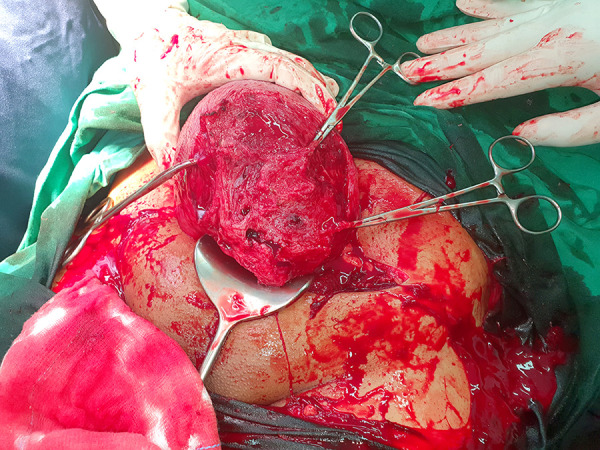
Case 1. The largest fibroid is removed through the cesarean section incision.
Figure 4.

Case 1. Three fibroids were removed.
Case 2
The second case was of a 36-year-old primigravida non-smoker who had an existing fibroid before pregnancy. Her only symptom of the fibroid prior to the pregnancy was being aware of a lump in the abdomen. She had been married for 5 months. Her height, weight, and body mass index were 155 cm, 64 kg, and 26.6 kg/m2, respectively. The first-trimester ultrasound revealed a large fibroid (diameter: 13 cm) in the fundus. The growth of the fetus was normal until delivery. She did not develop hypertension, diabetes mellitus, or any other disorders during pregnancy. The fibroid did not increase in size during the pregnancy. The short-term and long-term complications of cesarean myomectomy were explained to the patient. After she had provided written informed consent for the procedure, cesarean section was performed during the 38th week of gestation with a Pfannenstiel incision and spinal anesthesia. We ensured that the Pfannenstiel incision was large enough to exteriorize the uterus and the fibroids. We performed the myomectomy procedure with the uterus exteriorized. The fetus was in the cephalic position. The pre- and postoperative hemoglobin levels were 11 and 9.6 g/dL, respectively, with a blood loss of 500 mL. The operative time was 50 min. A baby weighing 2700 g was delivered, and the uterus was exteriorized. A bolus push of 10 IU of oxytocin was administered intravenously to induce uterine contractions. A large intramural fibroid (diameter: 20 cm) was observed in the right fundus and the smaller ones in the left fundus (Figure 5). New incisions were made in the uterus to remove the fibroids; the cesarean section incision (Figure 6) was not used. Hyaline and cystic degenerations were observed (Figure 7). The large fibroid was successfully removed (Figure 8), followed by removal of the smaller fibroids. We injected 500 mg of tranexamic acid to aid hemostasis. A continuous suture was used to repair the uterine wall using Monosyn® 1.0 (Figure 9). Three fibroids were sent for histo-pathological examination (Figure 10). No blood transfusions were administered. The mother and baby were in good condition after surgery. The patient was discharged from the hospital on postoperative day 3. Histopathological examination confirmed the diagnosis of fibroids with cystic and hyaline de-generations. The size of the largest fibroid was 22×19×9 cm.
Figure 5.

Case 2. After delivery, the uterus is exteriorized and the cesarean section incision is closed. A large fibroid is observed in the fundus.
Figure 6.

Case 2. Incision to remove the fibroid.
Figure 7.

Case 2. Hyaline and cystic degeneration are observed.
Figure 8.

Case 2. The large fibroid is removed.
Figure 9.

Case 2. Uterus after myomectomies.
Figure 10.

Case 2. Three fibroids were removed.
Discussion
We report the cases of 2 patients with large fibroids (>15 cm) who underwent successful cesarean myomectomy (Table 1). Both patients were nulligravida and became pregnant within 1 year following marriage. The fibroids did not affect the fertility of these 2 patients. The fertility of women with fibroids depends on the location of the fibroid in the uterus. Patients with submucosal fibroids experience a lower pregnancy rate (27.2%) than those with intramural fibroids (41%) [4]. Both patients had intramural fibroids. There is no strong evidence that myomectomy of intramural fibroids increases fertility [5]. Both patients requested cesarean myomectomy because they live in small cities and would experience difficulty returning to the tertiary hospital for fibroid removal. They were informed about the risk of uterine rupture in subsequent pregnancies and informed that they would require antenatal care in a tertiary hospital if they had further pregnancies. Currently, neither patient is planning a pregnancy.
Table 1.
Clinical characteristics of the patients.
| Case number | Age of patient (years) and smoking status | Gravidity | Height (cm), weight (kg), body mass index | Disorder complicating pregnancy | Gestational age at Cesarean section (weeks) | Pre- and post-operative hemoglobin (g/dL) | Blood loss (mL) | Duration of surgery (min) | Number of fibroids removed | Size of the largest fibroid (cm) | Baby’s weight (g) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 34, non-smoker | Primigravida | 145, 55, 26.2 | No | 38 | 10.5, 8.8 | 400 | 70 | 3 | 17×16×14 | 2800 |
| 2 | 36, non-smoker | Primigravida | 155, 64, 26.6 | No | 38 | 11.0, 9.9 | 500 | 50 | 3 | 22×19×9 | 2700 |
Possible effects of fibroids in women during pregnancy include intrauterine growth retardation, placental abruption, placenta previa, post-partum hemorrhage, retained placenta, and a higher risk of cesarean section compared with women without fibroids (48.5% vs 13.3%, P<0.05) [6]. The fetuses in our patients were in the cephalic position, and there was no malpresentation. The risk of malpresentation of the fetus in women with fibroids is 13%, which is higher than in women without fibroids (4.5%) [6]. The location of the fibroids determines the occurrence of malpresentation and risk of cesarean section. Fibroids in the lower segment of the uterus can interfere with fetal head engagement. In this case report, the patients’ fibroids were located in the corpus and fundus, making the presentation of the fetus normal. The most common complaint of women with fibroids in pregnancy is pain, which usually occurs in the second and third trimesters and in women with large fibroids (>5 cm) [7]. The most common causes of pain are red degeneration and torsion of the pedunculated subserosal fibroid [8]. In our case, both patients had fibroids that exhibited hyaline and cystic degenerations, and both patients did not experience pain during pregnancy. At the one-year follow-up, both infants were healthy, and both patients were experiencing normal menstrual periods without any complaints. Both patients are currently taking oral contraceptives.
To date, there are no standard guidelines regarding cesarean myomectomy. The treatment of fibroids in pregnancy is different at each center, particularly regarding whether the fibroids should be removed during cesarean section. A fibroid is considered large if the diameter exceeds 5 cm [9]. A study showed that cesarean myomectomy is a safe procedure for large fibroids. There was no difference in mean change of the hemoglobin level before and after surgery between cesarean myomectomy and cesarean without myomectomy [9]. However, the aforementioned study did not include fibroids >15 cm in size. Zhao et al reported that among 2565 women with fibroids in pregnancy, 9.4% underwent cesarean myomectomy safely, and there was no difference in blood loss between cesarean myomectomy and cesarean section only (835±42.3 mL vs 758±52.3 mL, P=0.447) [3]. Another large study, by Song et al [10], found that women who underwent a cesarean myomectomy had a 0.30 g/dL greater drop in hemoglobin than women who underwent a cesarean section only, but this difference was not statistically significant. We report 2 cases of cesarean myomectomy for fibroids >15 cm with blood loss of 400 and 500 mL, respectively.
Myomectomy should only be performed after closure of the cesarean section incision to minimize bleeding, unless the fibroid is to be removed via the same incision. Depending on the location of the fibroid, if it is not around the incision, we make a new incision above the fibroid. After myomectomy, the uterine wall was sutured quickly and carefully with 1–2 layers of sutures, depending on the thickness of the uterine wall. Tranexamic acid was administered to our patients to aid hemostasis. A previous study showed the benefit of tranexamic acid in myomectomy [11], although another study showed that tranexamic acid had no influence on blood loss during myomectomy [12]. Cesarean myomectomy only added around 10 min to the time needed for cesarean section [13,14]. The mean operative time for cesarean myomectomy was 53.3±18.6 min [14]. The aforementioned study included fibroids of all sizes. The operative time of cesarean myomectomies for large fibroids in this report was acceptable (50 and 70 min, respectively).
Conclusions
The important factors in performing a safe cesarean myomectomy for a large fibroid are adequate preparation, expertise in pelvic surgery, patient selection, and the hospital facilities. Cesarean myomectomy should only be performed at tertiary hospitals where experts and adequate intensive care facilities are available. The surgeries in our cases were performed at a tertiary hospital by a gynecologic oncologist. Short-term outcomes were positive, the babies are now 1 year old, and the patients are in good condition and having normal menstruation. The long-term effect of cesarean myomectomy still needs to be studied. This report showed that cesarean myomectomy for a large fibroid is safe, even for fibroids >15 cm in diameter. Further larger studies of cesarean myomectomy for large fibroids are required to confirm the safety of this procedure.
Acknowledgments
We thank Dr. Faroek Hoesin for histopathological examination.
References:
- 1.Sparić R, Malvasi A, Kadija S, et al. Cesarean myomectomy trends and controversies: an appraisal. J Matern Fetal Neonatal Med. 2017;30(9):1114–23. doi: 10.1080/14767058.2016.1205024. [DOI] [PubMed] [Google Scholar]
- 2.Ramya T, Sabnis SS, Chitra TV, Panicker S. Cesarean myomectomy: An experience from a Tertiary Care Teaching Hospital. J Obstet Gynaecol India. 2019;69(5):426–30. doi: 10.1007/s13224-019-01239-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Zhao R, Wang X, Zou L, Zhang W. Outcomes of myomectomy at the time of cesarean section among pregnant women with uterine fibroids: A retrospective cohort study. Biomed Res Int. 2019;2019:7576934. doi: 10.1155/2019/7576934. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Casini ML, Rossi F, Agostini R, Unfer V. Effects of the position of fibroids on fertility. Gynecol Endocrinol. 2006;22(2):106–9. doi: 10.1080/09513590600604673. [DOI] [PubMed] [Google Scholar]
- 5.Van Heertum K, Barmat L. Uterine fibroids associated with infertility. Women’s Health (Lond) 2014;10(6):645–53. doi: 10.2217/whe.14.27. [DOI] [PubMed] [Google Scholar]
- 6.Sampat K, Alleemudder DI. Fibroids in pregnancy: Management and outcomes. Obstet Gynaecol. 2018;20(3):187–95. [Google Scholar]
- 7.Lee HJ, Norwitz ER, Shaw J. Contemporary management of fibroids in pregnancy. Rev Obstet Gynecol. 2010;3(1):20–27. [PMC free article] [PubMed] [Google Scholar]
- 8.Cerdeira AS, Tome M, Moore N, Lim L. Seeing red degeneration in uterine fibroids in pregnancy: Proceed with caution. Lancet. 2019;394(10212):e37. doi: 10.1016/S0140-6736(19)32322-0. [DOI] [PubMed] [Google Scholar]
- 9.Kwon DH, Song JE, Yoon KR, Lee KY. The safety of cesarean myomectomy in women with large myomas. Obstet Gynecol Sci. 2014;57(5):367–72. doi: 10.5468/ogs.2014.57.5.367. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Song D, Zhang W, Chames MC, Guo J. Myomectomy during cesarean delivery. Int J Gynaecol Obstet. 2013;121(3):208–13. doi: 10.1016/j.ijgo.2013.01.021. [DOI] [PubMed] [Google Scholar]
- 11.Abdul IF, Amadu MB, Adesina KT, et al. Adjunctive use of tranexamic acid to tourniquet in reducing haemorrhage during abdominal myomectomy – A randomized controlled trial. Eur J Obstet Gynecol Reprod Biol. 2019;242:150–58. doi: 10.1016/j.ejogrb.2019.09.010. [DOI] [PubMed] [Google Scholar]
- 12.Opoku-Anane J, Vargas MV, Marfori CQ, et al. Intraoperative tranexamic acid to decrease blood loss during myomectomy: A randomized, double-blind, placebo-controlled trial. Am J Obstet Gynecol. 2020;223(3):413. doi: 10.1016/j.ajog.2020.02.019. e1–e7. [DOI] [PubMed] [Google Scholar]
- 13.Ghaemmaghami F, Karimi-Zarchi M, Gharebaghian M, Kermani T. Successful myomectomy during cesarean section: Case report & literature review. Int J Biomed Sci. 2017;13(2):119–21. [PMC free article] [PubMed] [Google Scholar]
- 14.Kaymak O, Ustunyurt E, Okyay RE, et al. Myomectomy during cesarean section. Int J Gynaecol Obstet. 2005;89(2):90–93. doi: 10.1016/j.ijgo.2004.12.035. [DOI] [PubMed] [Google Scholar]