

Abstract
Background:
Ideal pulpectomy for primary dentition demands fast, simple procedures, with short treatment times and minimal appointments. Recently, exclusive pediatric rotary files are available for use in primary teeth. There is a paucity of literature on the clinical efficacy of pediatric rotary files. Hence, this study was planned to evaluate and compare pediatric rotary files and K-files.
Aim:
The aim of this study was to evaluate and compare instrumentation time, obturation time, and radiographic quality of obturation using rotary systems (Kedo-S; Pro-AF Baby GOLD files) and manual (K-files) technique in primary molar pulpectomies.
Materials and Methods:
Forty-five primary mandibular molars from 42 children aged 5–9 were selected. Single-visit pulpectomy was performed after dividing selected teeth into three equal groups: (i) K-files, (ii) Kedo-S files, (iii) Pro-AF Baby GOLD files. Instrumentation and obturation times were recorded during the procedure. Immediate postoperative radiographs were taken and evaluated later for obturation quality by two independent evaluators blinded to the instrumentation technique. The results were then statistically analyzed.
Results:
Kedo-S (Group II) files required the least instrumentation time followed by Pro-AF (Group III) and K-files (Group I). The superior quality of obturation in lesser time was achieved using Pro-AF files (Group III) followed by Kedo-S (Group II) and K-files (Group I).
Conclusion:
Pediatric rotary files are efficient alternatives to hand instrumentation and can be considered as the standard of care in pulpectomies of primary teeth.
Keywords: Kedo-S files, K-files, pediatric rotary files, primary mandibular molars, Pro-AF files, single visit pulpectomy
Introduction
Pulpectomy is the preferred treatment modality for preserving infected deciduous teeth with irreversible pulpitis or pulpal necrosis.[1] Endodontic treatment in primary teeth is challenging due to the anatomy and morphology of root canals. Complete biomechanical preparation of the canals provides a path for irrigants and also aids in sealing the canals with biocompatible obturating material while preserving the radicular anatomy.[2] Hence, biomechanical preparation of canals is the major determinant in the success of pulpectomy.[3] Maintenance of the initial morphology of canals in the root, to conserve the healthy dentin while effectively enlarging the canal to remove its infected contents is generally recommended.
Conventionally, hand K-files are used to clean and prepare the root canals of infected deciduous teeth. Despite being commonly used, hand instrumentation can result in iatrogenic errors due to the indiscriminate and aggressive cutting action of stainless-steel files.[4,5]
The use of rotary instrumentation for cleaning and shaping of deciduous teeth was initially reported in 2000. It was found to be an efficient technique resulting in a uniform shape of canals with predictable obturation. Its ability to provide conical-shaped canals and decrease in canal preparation time favors its use.[5,6,7,8,9] In child patients, shorter appointment length is suggested to enhance co-operation.[10,11]
Multiple rotary systems are available and investigated for root canal preparation of permanent and primary teeth.[4,6,8,9,12,13] These systems are primarily designed for permanent teeth. The length and taper are limitations in using existing rotary systems in primary teeth.[14] Recently, exclusive pediatric rotary files of length 16 or 17 mm are available for use in primary teeth. There is a paucity of literature on the clinical efficacy of these pediatric rotary files in achieving good quality obturation, a predictor of long-term success in pulpectomized primary teeth. Thus, this in-vivo study was designed to evaluate and compare the instrumentation time, obturation time, and obturation quality using two rotary systems against hand K-files in primary molar pulpectomies.
Materials and Methods
The study was carried out in the Department of Paediatric and Preventive Dentistry at Dr. D. Y. Patil Dental College and Hospital, Pimpri, Pune, Maharashtra, India, after obtaining permission from the Scientific and Ethics committee. Forty-two children between ages 5 and 9 were selected among the patients who visited OPD of the department to participate in this clinical study after fulfilling the selection criteria and obtaining written informed consent.
Criteria for patient selection
Inclusion criteria:
Following were the Inclusion criteria[15]
Children in the age group of 5–9 years
Patients exhibiting Frankl's behavior rating scale score of 3 and 4 i.e., positive (+) and definitely positive (++)
At least two-thirds of remaining root length
Amount of tooth structure sufficient for application of rubber dam clamp
Primary molar teeth with chronic irreversible pulpitis
Primary molar teeth with at least one canal which is necrotic or has abscess or sinus tract
Radiolucent area(s) in the furcal region or peri-radicular region.
Exclusion criteria
Patients with a diagnosed systemic disease
Patients showing disruptive behavior during the procedure
Patients with nonrestorable teeth clinically, pulpal floor perforation, excessive mobility
Presence of frank dentoalveolar abscess or extra-oral swelling (presence of purulence in the canals)
Patients with more than one-third of pathologic root resorption.
Study design
Selected teeth were randomly placed into any one of the three groups:
Group 1 - Manual instrumentation using K-files (Mani, Tochigi, Japan) (n = 15)
Group 2 - Rotary instrumentation using Kedo-S files (Reeganz Dental Care Pvt. Ltd.) (n = 15)
Group 3 - Rotary instrumentation using Pro-AF Baby Gold files (Dentobizz, India) (n = 15).
Treatment procedure
Single-visit pulpectomy was carried out for all the included teeth by a single operator. After administering local anesthesia, pulpectomy was carried out under rubber dam isolation for all cases. All the teeth were subjected to intraoral periapical radiographs following obturation.
Access cavity preparation
Removal of carious tissue was done. Access opening was done using round and straight fissure burs (BR-41 and SF-41) at high speed. Following coronal pulp amputation, DG16 instrument was used for canal location. Extirpation of pulp was done using K-files. Pulp chamber was copiously irrigated using 3% of sodium hypochlorite and normal saline.
Working length determination
Following pulp chamber irrigation, insertion of no. 10 K-file in the canal was done. Radiographic working length, determined by the conventional Ingle's method, was 1 mm short of radiographic apex.
Biomechanical preparation
Group 1: Root canal preparation was done using conventional step-back method using stainless steel K–files and quarter-turn pull technique from #15 to #30
Group 2: Root canal instrumentation was done using Kedo-S files, after using #15 K-file. D1 file (0.25 mm tip diameter) was used in narrow canals, and the E1 file (0.30 mm tip diameter) was utilized in wide canals
Group 3: Instrumentation of root canals was done using Pro-AF files after enlarging the canals using K-file up to #15. Progressive filing of all the canals was carried out using the following files in the same sequence: B0 (#20/04), B1 (#25/04), B2 (#25/06). File B3 (#30/04) was used in wider canals.
The files devoid of any deformity were disposed of after utilizing them in a maximum of three teeth.
Obturation
All the canals were obturated in the same visit only if the canals could be dried with paper points. Final irrigation of the root canals, for all three groups, using 3% sodium hypochlorite was done. Absorbent, sterile paper points were then utilized to dry the canals, which were then obturated using Metapex. The tooth was then restored with Type IX GIC. Postoperative digital radiograph was taken for the assessment of the obturation quality.
Assessment of teeth
Instrumentation and obturation time
The instrumentation time was noted from the start of instrumentation until the completion of the biomechanical preparation of canals utilizing a stopwatch. The obturation time was similarly noted from the beginning of the drying of canals till the obturation was completed.
Immediate radiographic assessment
Immediate postoperative radiograph was evaluated for the quality and length of root canal obturation by two evaluators, blinded to instrumentation technique, by assessing the presence of voids and extent of fill based on the following criteria:[16] [Figures 1-3].
Figure 1.

(a and b) Group 1 [K-files]: Observed voids and overfill
Figure 3.

(a and b) Group 3 [Pro-AF files]: Observed optimal and overfill
Figure 2.

(a and b) Group 2 [Kedo-S files]: Observed voids, overfill and Obturation fill
Score 0 – Complete absence of voids
Score 1 – Presence of one void
Score 2 – Presence of two voids
Score 3 – Presence of three voids
Score 4 – Presence of four voids
Score 5 – Presence of five voids.
The extent of fill was scored from grade A to D based on the following criteria:
Grade A – Less than one-half of the canal obturated
Grade B – Greater than one-half but less than optimal fill
Grade C – Optimal fill
Grade D – Extrusion of material beyond apex.
Results
Data obtained was compiled, tabulated, and subjected to statistical analysis. The consistency and reliability of evaluators were assessed using kappa statistics. A strong inter-rater reliability was found with K value of 0.96 and 0.79 at 0.0001 significance. It means there was a strong agreement between two evaluators in evaluating the extent of fill of canals and the presence of voids.
Instrumentation time
Instrumentation time was recorded for all three groups in minutes [Table 1]. The mean time required for the instrumentation of canals using K-files (Group 1) was 27.87 min. Similarly, for Kedo-S (Group 2), meantime was 19.25 min. The mean time required for instrumentation using Pro-AF files (Group 3) was 21.89 min.
Table 1.
Descriptive data regarding mean timings taken for instrumentation for different file systems [minutes]
| File systems | n | Minimum | Maximum | Mean | SD |
|---|---|---|---|---|---|
| K-File manual instrumentation time | 15 | 25.87 | 30.30 | 27.87 | 1.35 |
| Kedo-S file rotary instrumentation time | 15 | 16.05 | 25.55 | 19.25 | 2.98 |
| Pro-AF file rotary instrumentation time | 15 | 18.25 | 25.05 | 21.89 | 2.43 |
SD: Standard deviation
Post hoc analysis revealed that a significant difference was observed between the three groups with P < 0.05. The least timing taken for instrumentation was found with Kedo-S rotary files followed by Pro-AF files, and the highest time was taken by K-files through manual method.
Obturation time
Time taken for obturation was also recorded in minutes [Table 2]. Meantime taken for obturation after preparing canals with K-files (Group 1) was 5.44 mins. Following preparation with Kedo-S rotary files (Group 2), the mean time taken for obturation was 4.71 mins while that after preparation with Pro-AF files (Group 3) was 4.62 mins.
Table 2.
Descriptive data regarding mean timings taken for obturation for different file systems [minutes]
| File systems | n | Minimum | Maximum | Mean | SD |
|---|---|---|---|---|---|
| K-File manual obturation time | 15 | 4.80 | 5.78 | 5.44 | 0.319 |
| Kedo-S file rotary obturation time | 15 | 3.30 | 5.67 | 4.71 | 0.743 |
| Pro-AF file rotary obturation time | 15 | 3.83 | 5.20 | 4.62 | 0.427 |
SD: Standard deviation
Post hoc test revealed that a significant difference was observed between the K-file group (Group 1) and rotary systems-Kedo-S (Group 2) and Pro-AF (Group 3) with P < 0.05. This indicated that rotary file systems are superior over manual K-files in completing the obturation process faster. No significant difference was observed between the two rotary file systems. The least timing taken for obturation was the following instrumentation using Pro-AF rotary system as compared to Kedo-S rotary system.
Radiographic quality of obturation
Radiographic quality of obturation was assessed by assessing the length of obturation and presence or absence of voids. On statistical analysis, no significant difference was observed between the three groups based on the extent of canal fill and the presence or absence of voids. On analyzing the radiographic quality of obturation after instrumentation with K-files (Group 1), 35.3% canals were optimally filled without any voids. In the canals instrumented using Kedo-S files (Group 2), 39.2% of optimally filled canals exhibited a complete absence of voids. In the third group, which was instrumented using Pro-AF files, 58.5% canals, which were optimally filled, were devoid of any voids. Thus, these results show that superior quality obturation was seen after the use of Pro-AF files followed by Kedo-S files and K-files. Graphs 1 and 2 depict the extent of fill and the presence of voids for all three groups.
Graph 1.
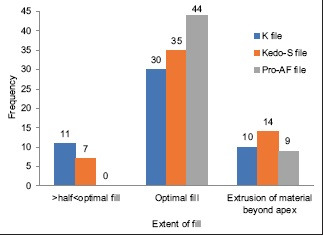
Difference in extent of fill with different file systems
Graph 2.
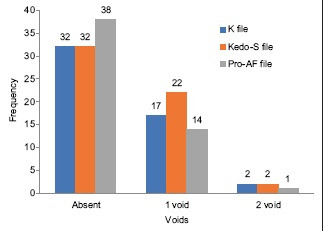
Difference in the number of voids with different file systems
Discussion
The clinical management of deciduous teeth varies considerably due to factors like the longevity of primary dentition, the integrity of the coronal structure, root canal anatomy and morphology as well as physiologic resorption. These factors make endodontic treatment in primary teeth challenging.[17,18]
Micro-organisms are the principal etiologic factors for pulpal and periapical pathology. The most desirable result in the endodontic treatment of primary teeth is based on the reduction of microbial load post chemico-mechanical preparation, removal of debris and residual pulp, and maintaining original canal shape during instrumentation.[19] Achieving this decrease in microbial load in a single visit is still an ongoing debate in cases of apical periodontitis. Owing to complex anatomy of canals, its complete disinfection is difficult in deciduous molars regardless of the number of visits.[20] The most important advantage of single visit pulpectomy is the prevention of contamination and/or bacterial re-growth in the root canal that might take place on prolonging the treatment period. Furthermore, it saves time, reduces treatment cost, and is expected to be less stressful to an anxious child.[20,21] Hence, in this study, pulpectomy was performed in a single visit.
Furthermore, studies have shown that children under the age of 4 are more sensitive to painful stimuli and that younger children tend to display more negative behaviour than older children.[22,23]
Hence, the age range included was 5–9 years. This also fulfilled the presence of fully developed, un-resorbed or minimally resorbed roots required for carrying out pulpectomy.
Mechanical cleaning can be done using endodontic broaches, hand files, reamers and nickel-titanium (Ni-Ti) rotary files. However, manual instrumentation by stainless steel files remains the conventional technique. This technique is time-consuming and often causes fatigue to the operator and child. Rotary file systems, on the contrary, are efficient in creating predetermined conical shapes with the minimal amount of risk. An inherent stiffness is present in the stainless-steel (SS) files that result in the various aberrations that may be seen during canal preparation.[24] Thus, in narrow curved canals, the use of these SS files is difficult. This, limits the apical enlargement, hindering good quality obturation.
Nickel-titanium (NiTi) rotary files not only conserve the initial shape of curved canals but also decrease the procedural mishaps due to features such as super-elasticity, shape memory, and strength.[25,26] Since its introduction, wide range of systems have been established in the market.
A major concern of using files designed for permanent teeth in primary tooth endodontics is that lateral perforation may occur on the inner aspect of the curved root canals in deciduous molar teeth.[7,27] Moreover, the deciduous root canals have ribbon-shaped morphology, and hence due to these limitations, Kuo et al. in 2006 stated that new NiTi rotary files designed exclusively for primary teeth would be more advantageous.[7,18] Furthermore, a greater amount of instrument separation has been seen in deciduous teeth while utilizing the available rotary systems.[28] According to the survey in 2017, 66% of dentists needed an exclusive pediatric rotary file for better accessibility and faster preparation.[14]
Considering these needs, rotary files have been exclusively designed for primary teeth. The length and taper of these files are designed such that it makes them more advantageous for use in primary teeth. Kedo-S rotary files, introduced in 2017, belong to the second generation of NiTi rotary files.[29] This was followed by the development of Pro-AF Baby Gold files belonging to third-generation NiTi files.[30]
Kedo-S system comprises three NiTi rotary files that are 16 mm long. The active length is 12 mm. These files with a variably variable taper are D1, E1, U1. The speed should ideally be 150–300 rpm, whereas the torque is 2.2–2.4 N.[29] It is recommended to utilize these files in an “in and out” action in well-lubricated canals to prevent the instrument from deformation and separation. Furthermore, the files should be withdrawn once the working length is reached.
Pro-AF Baby Gold consists of 5 files made up of NiTi-CM wire, making it more flexible and resistant to cyclic fatigue.[31] It has a constant taper of 4%, 6%. The length of these files is 17 mm, while the active length is 13 mm. It is recommended to use Pro-AF files at 250–300 rpm at 2.0–2.2 N torque in well-lubricated canals. These files should be used until the complete working length once or twice in brushing motion.
According to an in-vitro study by Mittal et al. in 2015, metallurgy and taper affected the cleaning and shaping of root canals.[32] The two rotary systems-Kedo-S and Pro-AF, differ in both metallurgy and taper. Therefore, these two rotary systems, in addition to the manual system, were compared in our study to evaluate if these changes in metallurgy and taper of rotary files had an effect on the clinical outcome of pulpectomy. Hence, three groups were investigated in the study.
Chair-side time is a very critical factor in the acceptance of endodontic therapy in children because of their shorter attention span. Hence, the present study evaluates instrumentation time and obturation time with the three different methods of biomechanical preparation.
In the present study, significant differences were observed between the instrumentation time as well as obturation time between rotary and manual techniques. Instrumentation time was least with Kedo-S rotary files followed by Pro-AF files while it was maximum with manual K-files. The results obtained were similar to the results of the studies done by Ochoa-Romero et al. in 2011,[15] Makerem et al. in 2014,[33] Vieyra and Enriquez 2014,[34] Govindaraju et al. 2017,[9] Jeevanandan and Govindaraju 2018,[35] Babaji et al. 2019,[36] Panchal et al. 2019,[37] and Lakshmanan et al. 2020.[38] Instrumentation using rotary decreases the fatigue and thus, increases the operator efficiency. This can be a possible explanation for reduced instrumentation time. The two rotary systems showed a notable difference with respect to instrumentation time, with the least time being required by the Kedo-S system. The shorter time required is probably related to the reduced number of instruments.
Obturation time was significantly lesser with rotary instrumentation when compared with manual instrumentation. Similar results were obtained in the study by Ochoa-Romero et al. 2011,[15] where obturation time was decreased by 68% of cases and Babaji et al. 2019.[36] On the contrary, no notable differences in obturation time were observed using rotary and manual instrumentation in studies conducted by Makerem et al. in 2014,[33] and Gomes 2014.[39] No appreciable difference was seen within two rotary groups in the present study. Hence, it is seen that with the use of rotary instrumentation, chair-side time is significantly reduced.
The prognosis of pulpectomy depends on many variables. One of the important variables is the length of the root canal filling. In the study by Coll and Sadrian in 1996, they concluded that teeth that were filled completely till the apex or those filled short of the apex had a significantly better success rate than those which are overfilled.[40] Yacobi et al. reported that canals that were underfilled failed significantly more than those that are completely filled in vital teeth.[41] Thus, the optimal filling of canals ensures the higher success of pulpectomy. Therefore, the quality of the obturation was evaluated in the present study.
Traditionally used zinc oxide eugenol has a slow resorption rate and may retain even after tooth exfoliation if extruded. This has shown to affect the permanent tooth bud resulting in defects or deviation of the eruption pathway. Therefore, premixed calcium hydroxide and iodoform pastes, available for over 20 years, are claimed to be nearly ideal root canal filling material for primary teeth.[42] Calcium hydroxide and iodoform formulations are not harmful for permanent tooth buds and are known to resorb if extruded. Furthermore, the mode of delivering Metapex, i.e., the use of capillary tips, proved to be the most effective obturation technique in a recent study.[43] Even, whenever there is a doubt about the patient's return for follow-up, it has been considered safer to use Metapex.[44] When considering the different calcium hydroxide-iodoform obturating materials available in the market, Metapex is more cost-effective. Therefore, Metapex was used for obturation in our study. Digital radiography aids in achieving high-quality image with minimal radiation exposure.[45,46] It is the only cost-effective clinical way to evaluate the quality of obturation. Hence this technique was used for evaluation.
In the present study, maximum canals instrumented using Pro-AF files showed the optimal length of obturation followed by Kedo-S files while K-files showed the maximum number of underfilled canals. Although the study shows no significant differences in the length of obturation using rotary and manual preparation, similar significant results were stated by Ochoa-Romero et al. in 2011,[15] Makerem et al. in 2014,[33] Govindaraju et al. in 2017,[9] Jeevanandan and Govindaraju 2018,[35] Babaji et al. 2019,[36] Panchal et al. 2019,[37] Divya et al. 2019,[47] and Lakshmanan et al. 2020.[38]
Another key element that determines the quality of obturation is the presence or absence of voids. The presence of voids might provide pathways for leakage and possible retention of microorganisms and toxins, which might lead to posttreatment failures.[16,45,48,49] The cleaning and shaping of the canals is compromised by the procedural errors, which results in incomplete or inferior quality of canal filling, which may jeopardize the treatment success. Another reason for the creation of voids is the presence of moisture in the canals. Therefore, evaluation of voids was done using postobturation radiograph with the maximum possible visibility of canals.
In the current study, rotary instrumentation using Pro-AF resulted in an overall lesser number of voids when compared with Kedo-S and K-files. No notable difference was seen in the presence of voids in obturation after the preparation of canals using rotary and manual techniques in this study. It can be therefore stated that instrumentation using rotary files resulted in superior quality obturations in minimal chair-side time.
Assessment of quality of obturation was done using digital radiographs, which gave two-dimensional images of three-dimensional structure. It can be the limitation of the current study. Futhermore, follow-up of the cases for success or failure is not recorded, which is an important factor in judging the success of endodontic therapy.
In the current study, only mandibular molars were included as maxillary molars present with a different set of challenges as far as radiographic interpretation is concerned. The present study is a single-blinded study as the operator could not be blinded to the different file systems.
Conclusion
Within the limitations of the present study, it can be concluded that:
In primary molar endodontics, efficacy in terms of chair-side time is indispensable. Remarkable decrease in chair-side instrumentation and obturation times was achieved using Kedo-S and Pro-AF rotary files
Instrumentation using pediatric rotary files, under complete isolation using a rubber dam, promotes superior quality of obturation, increasing the clinical success. Pro-AF files showed the maximum number of optimal obturations with the least number of voids followed by Kedo-S rotary files.
Thus, pediatric rotary files - Pro-AF Baby Gold and Kedo-S files, can be considered safe and more efficient alternatives to manual instrumentation technique. Pediatric rotary files form an integral part of pediatric dentist's armamentarium and can be considered as the standard of care in primary molar pulpectomies.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.AAPD. Guideline on pulp therapy for primary and young permanent teeth. Pediatr Dent. 2004;26:115–9. [PubMed] [Google Scholar]
- 2.Siqueira JsF, Jr, Araújo MC, Garcia PF, Fraga RC, Dantas CJ. Histological evaluation of the effectiveness of five instrumentation techniques for cleaning the apical third of root canals. J Endod. 1997;23:499–502. doi: 10.1016/S0099-2399(97)80309-3. [DOI] [PubMed] [Google Scholar]
- 3.Haapasalo M, Endal U, Zandi H, Coil JM. Eradication of endodontic infection by instrumentation and irrigation solutions. Endod Topics. 2005;10:77–102. [Google Scholar]
- 4.Barr ES, Kleier DJ, Barr NV. Use of nickel-titanium rotary files for root canal preparation in primary teeth. Pediatr Dent. 1999;21:453–4. [PubMed] [Google Scholar]
- 5.Barr ES, Kleier DJ, Barr NV. Use of nickel-titanium rotary files for root canal preparation in primary teeth. AAPD. 2000;22:77–8. [PubMed] [Google Scholar]
- 6.Pinheiro SL, Araujo G, Bincelli I, Cunha R, Bueno C. Evaluation of cleaning capacity and instrumentation time of manual, hybrid and rotary instrumentation techniques in primary molars. Int Endod J. 2012;45:379–85. doi: 10.1111/j.1365-2591.2011.01987.x. [DOI] [PubMed] [Google Scholar]
- 7.Kuo CI, Wang YL, Chang HH, Huang GF, Lin CP, Guo MK. Application of Ni-Ti rotary files for pulpectomy in primary molars. J Dent Sci. 2006;1:10–5. [Google Scholar]
- 8.Silva LA, Leonardo MR, Nelson-Filho P, Tanomaru JM. Comparison of rotary and manual instrumentation techniques on cleaning capacity and instrumentation time in deciduous molars. J Dent Child. 2004;71:45–7. [PubMed] [Google Scholar]
- 9.Govindaraju L, Jeevanandan G, Subramanian EM. Comparison of quality of obturation and instrumentation time using hand files and two rotary file systems in primary molars: A single-blinded randomized controlled trial. Eur J Dent. 2017;11:376–9. doi: 10.4103/ejd.ejd_345_16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Aminabadi NA, Oskouei SG, Farahani RM. Dental treatment duration as an indicator of the behavior of 3-to 9-year-old pediatric patients in clinical dental settings. J Contemp Dent Pract. 2009;10:E025–32. [PubMed] [Google Scholar]
- 11.Lenchner V. The effect of appointment length on behavior of the pedodontic patient and his attitude toward dentistry. J Dent Child. 1966;33:61–74. [PubMed] [Google Scholar]
- 12.Azar MR, Mokhtare M. Rotary Mtwo system versus manual K-file instruments: Efficacy in preparing primary and permanent molar root canals. Ind J Dent Res. 2011;22:363–7. doi: 10.4103/0970-9290.84283. [DOI] [PubMed] [Google Scholar]
- 13.Musale PK, Mujawar SA. Evaluation of the efficacy of rotary versus hand files in root canal preparation of primary teeth in vitro using CBCT. Eur Arch Paediatr Dent. 2014;15:113–20. doi: 10.1007/s40368-013-0072-1. [DOI] [PubMed] [Google Scholar]
- 14.Govindaraju L, Jeevanandan G, Subramanian E. Knowledge and practice of rotary instrumentation in primary teeth among Indian dentists: A questionnaire survey. J Int Oral Health. 2017;9:45–8. [Google Scholar]
- 15.Ochoa-Romero T, Mendez-Gonzalez V, Flores-Reyes H, Pozos-Guillen AJ. Comparison between rotary and manual techniques on duration of instrumentation and obturation times in primary teeth. J Clin Pediatr Dent. 2011;35:359–63. doi: 10.17796/jcpd.35.4.8k013k21t39245n8. [DOI] [PubMed] [Google Scholar]
- 16.Khubchandani M, Baliga MS, Rawlani SS, Rawlani SM, Khubchandani KM, Thosar N. Comparative evaluation of different obturation techniques in primary molars: An in vivo study. Eur J Gen Dent. 2017;6:42–7. [Google Scholar]
- 17.Hedge V. Pediatric Endodontics- Endodontist's view. People's J Sci Res. 2011;4:71–4. [Google Scholar]
- 18.Finn SB. Clinical Pedodontics. 4th ed. Finn SB: Saunders Co, Philadelphia; 1973. Morphology of primary teeth; pp. 59–70. [Google Scholar]
- 19.Jha D, Guerrero A, Ngo T, Helfer A, Hasselgren G. Inability of laser and rotary instrumentation to eliminate root canal infection. J Am Dent Assoc. 2006;137:67–70. doi: 10.14219/jada.archive.2006.0023. [DOI] [PubMed] [Google Scholar]
- 20.Bharuka SB, Mandroli PS. Single- versus two-visit pulpectomy treatment in primary teeth with apical periodontitis: A double-blind, parallel group, randomized controlled trial. J Indian Soc Pedod Prev Dent. 2016;34:383–90. doi: 10.4103/0970-4388.191429. [DOI] [PubMed] [Google Scholar]
- 21.Prashanth MB, Tavane PN, Abraham S, Chacko L. Comparative evaluation of pain, tenderness and swelling followed by radiographic evaluation of periapical changes at various intervals of time following single and multiple visit endodontic therapy: An in vivo study. J Contemp Dent Pract. 2011;12:187–91. doi: 10.5005/jp-journals-10024-1032. [DOI] [PubMed] [Google Scholar]
- 22.Sharma A, Kumar D, Anand A, Mittal V, Singh A, Aggarwal N. Factors predicting Behavior Management Problems during Initial Dental Examination in Children Aged 2 to 8 Years. Int J Clin Pediatr Dent. 2017;10:5–9. doi: 10.5005/jp-journals-10005-1397. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Cademartori MG, Corrêa MB, Silva RA, Goettems ML. Childhood social, emotional, and behavioural problems and their association with behaviour in the dental setting. Int J Paediatric Dent. 2019;29:43–9. doi: 10.1111/ipd.12436. [DOI] [PubMed] [Google Scholar]
- 24.Rashid AA, Saleh AR. Shaping ability of different endodontic single-file systems using simulated resin blocks. Indian J Multidisciplinary Dent. 2016;6:61. [Google Scholar]
- 25.Thompson SA. An overview of nickel-titanium alloys used in dentistry. Int Endod J. 2000;33:297–310. doi: 10.1046/j.1365-2591.2000.00339.x. [DOI] [PubMed] [Google Scholar]
- 26.Guelzow A, Stamm O, Martus P, Kielbassa AM. Comparative study of six rotary nickel-titanium systems and hand instrumentation for root canal preparation. Int Endod J. 2005;38:743–52. doi: 10.1111/j.1365-2591.2005.01010.x. [DOI] [PubMed] [Google Scholar]
- 27.Abou-Rass M, Frank AL, Glick DH. The anticurvature filing method to prepare the curved root canal. J Am Dent Assoc. 1980;101:792–4. doi: 10.14219/jada.archive.1980.0427. [DOI] [PubMed] [Google Scholar]
- 28.Nagaratna PJ, Shashikiran ND, Subbareddy VV. In vitro comparison of Ni-Ti rotary instruments and stainless-steel hand instruments in root canal preparations of primary and permanent molar. J Indian Soc Pedod Prev Dent. 2006;24:186–91. doi: 10.4103/0970-4388.28075. [DOI] [PubMed] [Google Scholar]
- 29.Jeevanandan G. Kedo-S paediatric rotary files for root canal preparation in primary teeth-case report. J Clin Diagnostic Res JCDR. 2017;11:ZR03. doi: 10.7860/JCDR/2017/25856.9508. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Thakkar TK. Advances in rotary endodontics in pediatric dentistry. EC Dent Sci. 2019;18:1320–30. [Google Scholar]
- 31.Srivastava S, Alghadouni MA, Alotheem HS. Current strategies in metallurgical advances of rotary NiTi instruments: A review. J Dent Health Oral Disord Ther. 2018;9:75–80. [Google Scholar]
- 32.Mittal S, Gupta S, Sharma DK, Sharma AK, Mittal K. Effect of taper and metallurgy on cleaning efficacy of endodontic files in primary teeth: An in-vitro study. J Pediatr Dent. 2015;3:75–81. [Google Scholar]
- 33.Makerem A, Ravandeh N, Ebrahimi M. Radiographic assessment and chair time of rotary instruments in the pulpectomy of primary second molar teeth: A randomized controlled clinical trial. J Dent Res Dent Clin Dent Prospect. 2014;8:84–9. doi: 10.5681/joddd.2014.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Vieyra JP, Enriquez FJ. Instrumentation time efficiency of rotary and hand instrumentation performed on vital and necrotic human primary teeth: A randomized clinical trial. Dentistry. 2014;4:214. [Google Scholar]
- 35.Jeevanandan G, Govindaraju L. Clinical comparison of Kedo-S paediatric rotary files vs manual instrumentation for root canal preparation in primary molars: A double blinded randomised clinical trial. Eur Arch Paediatr Dent. 2018;19:273–8. doi: 10.1007/s40368-018-0356-6. [DOI] [PubMed] [Google Scholar]
- 36.Babaji P, Mehta V, Manjooran T. Clinical evaluation of rotary system over manual system in deciduous molars: A clinical trial. Int J Pedod Rehabil. 2019;4:13–6. [Google Scholar]
- 37.Panchal V, Jeevanandan G, Subramanian E. Comparison of instrumentation time and obturation quality between hand K-file, H-files, and rotary Kedo-S in root canal treatment of primary teeth: A randomized controlled trial. J Indian Soc Pedod Prev Dent. 2019;37:75–9. doi: 10.4103/JISPPD.JISPPD_72_18. [DOI] [PubMed] [Google Scholar]
- 38.Lakshmanan L, Mani G, Jeevanandan G, Ravindran V, Ganapathi SE. Assessing the quality of root canal filling and instrumentation time using kedo-s files, reciprocating files and k-files. Brazilian Dent Sci. 2020;23:7. [Google Scholar]
- 39.Gomes GB, Bonow ML, Carlotto D, Jacinto RC. In vivo comparison of the duration between two endodontic instrumentation techniques in deciduous teeth. Braz Res Pediatric Dent Integrated Clin. 2014;14:199–205. [Google Scholar]
- 40.Coll JA, Sadrian R. Predicting pulpectomy success and its relationship to exfoliation and succedaneous dentition. Pediatric Dent. 1996;18:57–63. [PubMed] [Google Scholar]
- 41.Yacobi R, Kenny DJ, Judd PL, Johnston DH. Evolving primary pulp therapy techniques. J Am Dent Assoc. 1991;122:83–5. doi: 10.14219/jada.archive.1991.0054. [DOI] [PubMed] [Google Scholar]
- 42.Vakil N, Singh A, Chhoker VK, Tafseer S, Ali S. Evaluation of zinc oxide eugenol and vitapex for carrying out endodontic therapy of necrotic primary teeth. Saudi J Oral Dent Res. 2019;4:309–12. [Google Scholar]
- 43.Rajasekhar S, Mallineni SK, Nuvvula S. Comparative evaluation of three obturation systems in primary molars-A randomized clinical trial. J Indian Soc Pedod Prev Dent. 2019;37:297–302. doi: 10.4103/JISPPD.JISPPD_276_18. [DOI] [PubMed] [Google Scholar]
- 44.Gupta S, Das G. Clinical and radiographic evaluation of zinc oxide eugenol and metapex in root canal treatment of primary teeth. J Indian Soc Pedod Prev Dent. 2011;29:222–8. doi: 10.4103/0970-4388.85829. [DOI] [PubMed] [Google Scholar]
- 45.Aghdasi MM, Asnaashari M, Aliari A, Fahimipour F, Soheilifar S. Conventional versus digital radiographs in detecting artificial voids in root canal filling material. Iran Endod J. 2011;6:99–102. [PMC free article] [PubMed] [Google Scholar]
- 46.Bansal GJ. Digital radiography. A comparison with modern conventional imaging. Postgrad Med J. 2006;82:425–8. doi: 10.1136/pgmj.2005.038448. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Divya S, Jeevanandan G, Sujatha S, Subramanian EMG, Ravindran V. Comparison of quality of obturation and post-operative pain using manual vs rotary files in primary teeth - A randomised clinical trial. Indian J Dent Res. 2019;30:904–8. doi: 10.4103/ijdr.IJDR_37_18. [DOI] [PubMed] [Google Scholar]
- 48.Kositbowornchai S, Hanwachirapong D, Somsopon R, Pirmsinthavee S, Sooksuntisakoonchai N. Ex vivo comparison of digital images with conventional radiographs for detection of simulated voids in root canal filling material. Int Endod J. 2006;39:287–92. doi: 10.1111/j.1365-2591.2006.01087.x. [DOI] [PubMed] [Google Scholar]
- 49.Bodanezi A, Munhoz Ede A, Bernardineli N, Capelozza AL, de Moraes IG, Bramante CM. Radiographic analysis of root canal fillings: Influence of two sealers on the perception of voids. Braz Dent J. 2010;21:142–7. doi: 10.1590/s0103-64402010000200009. [DOI] [PubMed] [Google Scholar]