

Abstract
The Covid‐19 outbreak was declared a public health emergency by the World Health Organization in January 2020. As a consequence, several protective measures were urged by national governments in order to limit the spread of the pandemic. Drawing on the literature on health behaviours, in the present study, we investigated the psychological factors (i.e., attitudes, social norms, perceived behavioural control, intentions, and risk perception) that were associated with two highly recommended behaviours: frequent hand washing and social distancing (i.e., staying at home except for essential reasons). The study employed a correlational design with a follow‐up. A questionnaire including measures of psychological predictors was administered via social media to a sample of 403 adults residing in Italy during the lockdown. Self‐reported behaviours were assessed one week later. Findings showed that attitudes, social norms, perceived behavioural control were significantly related to hand washing and social distancing through intentions. Risk perception was a significant predictor of social distancing but not of hand washing. These findings suggest that intervention and communication strategies aimed at encouraging preventive measures during the Covid‐19 pandemic should be organized taking into account multiple factors which partially differ depending on the type of behaviour considered. Please refer to the Supplementary Material section to find this article's Community and Social Impact Statement.
Keywords: Covid‐19 pandemic, hand washing, health behaviours, risk perception, self‐protective behaviours, social distancing, Theory of Planned Behaviour
To us all: We all have a role to play to keep COVID‐19 at bay. Our behaviour determines COVID‐19 behaviour (Dr. Kluge, WHO Regional Director for Europe)
In January 2020, the World Health Organization (WHO) declared Covid‐19, the new coronavirus disease, a public health emergency concern and by March 2020, it was declared a global pandemic. Initial alarms of a possible epidemic were given in Wuhan (China) in December 2019, and since then its spread has been unstoppable. After China, Italy was the first country in Europe to be strongly hit and rapidly after, countries all around the world had to face—and are still facing—the huge burden of the outbreak. To date (4th February 2021), it is present in 219 countries with more than 105 million confirmed cases (Worldometers, 2021). Evidence of its high contagiousness became clear after human‐to‐human transmission was found from both symptomatic and asymptomatic individuals (WHO, 2020).
At present, Covid‐19's outbreak does not only worry because of its huge clinical and potential psychological consequences (Zaka, Shamloo, Fiorente, & Tafuri, 2020), but also because of global social and economic concerns (Nicola et al., 2020). As a response, the efforts national governments have made to contain the rapid spread of the virus have been massive such as the changes in the lifestyle the population has had to undergo to minimize and protect itself from the pandemic. As a case in point, WHO as well as ministries of health, developed and defined several protective measures to be adopted by the population. Yet, while some of these behaviours have been imposed (e.g., wearing a protective mask in public spaces, quarantine in case of contagion) other behaviours such as frequent hand washing or social distancing (i.e., staying at home as much as possible) could only be strongly encouraged, leaving the population responsible for their implementation. Adherence to these behaviours face important motivational, practical and social barriers as well as costs on people (West, Michie, Rubin, & Amlôt, 2020), thus possibly challenging adhesion to these behaviours.
Since Covid‐19's outbreak, there have been frequent communications held by several head exponents and top experts, which have acknowledged and explained the crucial role played by the population in contrasting the Covid‐19 pandemic through their behaviour (e.g., Kluge, 2020). Indeed, people's actions have been considered a core aspect of Covid‐19's spread, which calls for individual and social responsibility. This strongly suggests the importance of understanding what motivates people to engage in specific preventive behaviours in times such as a pandemic. Specifically, identifying the factors that better predict the extent to which people will engage in preventive measures is necessary and timely. In sum, research on this topic may not only help to broaden the literature on health behaviour during a pandemic, but knowing what better predicts certain target behaviours could also inform on how to better structure effective interventions and communications to the community in order to elicit positive behavioural responses in such situations.
1. MOTIVATIONAL AND COGNITIVE ANTECEDENTS OF HEALTH BEHAVIOURS
Efforts to prevent the spread of diseases and promote healthy practices have motivated researchers from different fields to understand what leads to successful implementation of behaviour (i.e., adherence to preventive behaviours).
Several theories of general behaviour have been used to describe how people come to engage in certain behaviours by identifying the specific antecedents of behavioural outcomes. One of the most prominent approaches to the study of health behaviours is the Theory of Planned Behaviour (TPB; Ajzen, 1991). In its original version, the theory was known as the Theory of Reasoned Action (TRA; Fishbein & Ajzen, 1975; Ajzen & Fishbein, 1980) and was aimed at proposing an explanatory model of behaviour based on a limited number of socio‐cognitive predictors. According to TRA, the most proximal predictor of behaviour is the intention or willingness to perform it. Behavioural intention represents a deliberate plan or conscious decision to engage in a certain behaviour (Conner & Sparks, 2005). Intentions reflect therefore an individual's motivation to exert effort to perform a behaviour. Intention is in turn predicted by attitude towards a behaviour and by subjective norms. Attitude is the overall evaluation of behaviour, namely the degree to which behaviour is evaluated positively or negatively (Albarracin, Johnson, Fishbein, & Muellerleile, 2001). Subjective norms assess the social pressures toward performing or not performing a particular behaviour (Conner & Sparks, 2005). They represent a set of beliefs about whether significant others think that the individual should engage or not engage in the behaviour. Significant others are defined as individuals or ingroup members whose preferences about the behaviour are important to the person that should engage in that behaviour. Later on, the TRA was extended to broaden its applicability beyond purely volitional behaviours, resulting in the TPB. The new approach introduced perceptions of control over performance as an additional predictor of behaviour (Ajzen, 1991). Specifically, perceived behavioural control (PBC) refers to the individual perception that the target behaviour is easy or difficult to perform. The TPB assumes that PBC is both directly linked to the behaviour and indirectly linked to it through intention. It is worthwhile noting that when the behaviour is completely under volitional control, PBC should not exert any influence over the behaviour. It is only when the behaviour is scarcely determined by volitional control (i.e., intentions only account for a small portion of the variance in behaviour) that PBC should represent a significant predictor of behaviour (Ajzen, 1991; Armitage & Conner, 2001). Moreover, according to Ajzen (1991), “The relative importance of attitude, subjective norm, and perceived behavioural control in the prediction of intention is expected to vary across behaviours and situations” (p.188). Thus, in contexts where attitude or subjective norms are powerful predictors of behaviour, the influence of PBC on intentions could be less strong (Conner & Sparks, 2005).
The TRA and the TPB have been widely applied to the prediction of different health behaviours (for meta‐analyses, see, for example, Albarracin et al., 2001; Hausenblas, Carron, & Mack, 1997; Sheeran & Taylor, 1999; Rich, Brandes, Mullan, & Hagger, 2015). In the context of infectious disease outbreaks, one study by Cheng and Ng (2006) examined the efficacy of the TRA/TPB variables in the prediction of SARS‐preventive behaviours in four major affected regions (Guangdong, China; Hong Kong; Singapore; Toronto, Canada). Their results provided general support for the role of attitude and social norms on the enactment of SARS‐preventive behaviours, while PBC was a significant predictor in three of the four samples. However, behavioural intention was not entered as a predictor of actual behaviour, thus resulting in an incomplete test of TRA/TPB. In addition, the measure of preventive behaviours was obtained by aggregating 15 different behaviours, thus making it impossible to discern whether the predictors were equally effective for each of the behaviours examined. Other studies have used the TPB to predict vaccination intentions and vaccination receipt in relation to the H1N1 pandemic. Myers and Goodwin (2011) found that a model including attitude, subjective norms, and PBC, accounted for 44% of additional variance in the intention to have a swine flu vaccination compared to a model including demographic variables (e.g., age, gender). Perceived susceptibility and perceived severity were also tested as further predictors, but their effect was non‐significant. Liao, Cowling, Lam, Fielding, and Semple (2011) tested a modified version of TPB to predict self‐reported vaccination in a large sample of adults in Hong Kong. In line with TPB, results showed that subjective norms and PBC were significant predictors of intentions to vaccinate, which in turn predicted self‐reported vaccination two‐months later. Attitude was not assessed as a unitary construct in this study, but as positive and negative beliefs about vaccination. However, both positive and negative attitudes were significantly associated with intentions in the predicted direction.
Although TPB offers a major understanding of how people end up engaging in certain behaviours, it does not directly consider arousal or emotional factors, which suggests that the TPB may be restricted to the rational part of a decision (Oliver & Berger, 1979; see Conner & Norman, 2005, for a discussion).
In this regard, several other models of health behaviour have also advocated for the role of threat associated to a health problem by also considering how the perception of risk may influence behaviour. For example, according to the Health Belief Model (Champion & Skinner, 2008; Rosenstock, 1974; Rosenstock, Strecher, & Becker, 1988) and Protection Motivation Theory (Rogers, 1975; for a meta‐analysis Floyd, Prentice‐Dunn, & Rogers, 2000), people will be more keen to undertake preventive health behaviours when they consider the disease as a threat and specifically when (a) they consider the disease as severe in terms of consequences, (b) they feel personally susceptible to the disease. Perceived severity specifically refers to feelings about the seriousness of contracting an illness in terms of both medical and social consequences (e.g., death; impairment in daily activities, respectively). In turn, perceived susceptibility indicates individuals' beliefs about the likelihood of getting a disease or condition, more precisely belief of constitutional vulnerability to it. The combination of susceptibility and severity is labelled as perceived threat. In other words, if individuals perceive a condition would have serious consequences or if they think of themselves as susceptible to it, they will be more likely to initiate behaviour to limit their risks (Champion & Skinner, 2008). This is especially true for those behaviours which are easy to implement as for example vaccination behaviour (Brewer et al., 2007).
In addition to the two dimensions of perceived risk mentioned above, a third dimension of perceived risk may be identified which refers to perceived likelihood. It refers to ″one's probability of being harmed by a hazard under certain behaviour condition″ (e.g., ″What is the likelihood that you will get the flu this year if you don't get a flu shot?″; Brewer et al., 2007, p. 137). This dimension is often used interchangeably with the term susceptibility but should be seen as distinct, although partially overlapping with it (Brewer et al., 2007).
Although risk perception is considered a central dimension of several health models, its role in shaping behaviour is not clear. Indeed, theories of health behaviour and empirical studies have not reached to solid conclusions. Several studies have found positive associations between risk perceptions and engagement in protective behaviour in the case of other pandemics (for a review, see Bish & Michie, 2010), other studies have found negative relationships as in the case of Covid‐19 risk perceptions and protective behaviours (Taghrir, Borazjani, & Shiraly, 2020). Nevertheless, meta‐analytic evidence has shown that the effect sizes found for risk perceptions are generally small but significant (Brewer et al., 2007; for a meta‐analysis on risk perceptions and behaviour, see Brewer et al., 2007; Harrison, Mullen, & Green, 1992; Milne, Sheeran, & Orbell, 2000).
2. THE PRESENT RESEARCH
In this study, we aimed at investigating the psychological predictors of protective behaviours during the Covid‐19 pandemic. We selected two specific health behaviours highly recommended during Covid‐19 in Italy: frequent hand washing and social distancing (i.e., staying at home except for essential reasons). We chose to rely on frequent hand washing as a target of behaviour, since it is one of the most effective actions to reduce the spread of pathogens and prevent infections and it has been encouraged by the national government and WHO. In addition, we chose social distancing, here conceptualized as limiting outings as much as possible except for essential reasons, as another behaviour because it has been one of the main harsh social consequences people had to face during the lockdown. As previously mentioned, Italy was one of the first countries in Europe to face the burden of the pandemic. Starting from 9th March until the 18th of May 2020 Italy went through a phase of national lockdown. People were required to stay home as much as possible. From the 4th of May people were allowed to see relatives and from the 18th of May onwards people were again allowed to see their friends although people have always been required to respect the one‐meter distance policy.
Drawing on the TPB, we tested a model including attitude, social norms, perceived behavioural control, and intention as predictors of hand washing and social distancing. Yet, as previously mentioned, the TPB emphasises the rational dimension of health behaviour engagement (Conner & Norman, 2005; Oliver & Berger, 1979). Thus, we also included risk perception as a predictor of behaviour in our model in order to test whether it may also explain, to a certain extent, engagement in these two core preventive behaviours. Several health models have considered risk perceptions to be important predictors of behaviour, especially when the behaviour is easy to carry out (Brewer et al., 2007). One may think that individuals who are aware of a risk may take action in order to choose the appropriate health‐related responses, yet this link has not always been demonstrated (Schwarzer, 2001).
Consistent with previous studies on TPB and health behaviours, we hypothesized that attitudes about the behaviour, social norms as well as perceived behavioural control would predict intention to engage in both behaviours (frequent hand washing and social distancing) and that, in turn, intentions would predict actual behaviour. As to risk perception, previous findings usually suggest that it can be either positively related to the enactment of protective behaviour or unrelated. Even if it is not possible to develop a clear hypothesis, we still believe it is useful to test both rational and emotional predictors of self‐protective behaviours in the context of the Covid‐19 pandemic.
The literature on the antecedents of protective behaviours during a pandemic suggests that age and sex might play a significant role (see Bish & Michie, 2010). Some studies showed that during the SARS outbreak older people were more likely to engage in protective behaviours (Leung et al., 2003; Quah & Hin‐Peng, 2004), such as hand washing, disinfecting one's living quarter, and avoiding crowding places (Lau, Yang, Tsui, & Kim, 2003). However, other studies have shown an opposite pattern, with younger people being more inclined to adopt protective behaviours (Rubin, Amlôt, Page, & Wessely, 2009; Wong & Tang, 2005), or a non‐significant relationship between age and self‐protective behaviours (e.g., Brug et al., 2004). The pattern of findings for sex is somewhat more consistent (see Bish & Michie, 2010). Even though a number of studies have not found a significant relationship between sex and protective behaviours (e.g., Barr et al., 2008; Brug et al., 2004), studies reporting a significant difference consistently show that women are more likely to engage in recommended self‐protective behaviours than men (e.g., Eastwood et al., 2009; Jones & Salathe, 2009; Rubin et al., 2009). In light of these findings, we tested age and sex as covariates in additional analyses.
3. METHOD
3.1. Participants
Four hundred and three adults residing in Italy during the lockdown participated in the study on a voluntary basis. Participants who did not complete the behavioural measures (administered one week after the first questionnaire, see the Procedure section; n = 151) and participants who reported they had been infected with Covid‐19 (n = 4) were discarded from analyses, leaving N = 248 (176 females, 72 males; mean age = 34.78, SD = 14.76, range = 18–72). In the final sample, 11.7% reported having one or more relatives who had been infected (M = 0.15, SD = 0.44; range = 0–3); 24.2% had one or more friends who had been infected (M = 0.52, SD = 1.28; range = 0–10 or more), 65.3% reported having one or more acquaintances who had been infected (M = 1.92, SD = 2.43; range = 0–10 or more). Among the respondents, the majority (almost 75% of the sample) came from two of the most hit regions in Italy: 54.8% of the sample resided in the Veneto region while 19.8% came from Lombardy.
3.2. Procedure
The study received ethical approval from the Ethics Committee at the Dept. of Human Sciences (University of Verona). Participants were contacted via social media (i.e., Facebook and WhatsApp groups) and through snowball sampling during the national quarantine imposed by the Italian government. They were invited to voluntarily participate in an online survey on attitudes and behaviours during the Covid‐19 emergency. Participants were asked to flag an informed consent prior to participation. They were informed that due to methodological reasons the survey consisted of two questionnaires. One week after completing the first questionnaire, participants were e‐mailed a link to the second questionnaire.
3.3. Measures
The first questionnaire included demographic questions and measures of attitude, subjective norms, perceived behavioural control, intention, and risk perception. The second questionnaire included measures of the target behaviours. All the TPB measures were based on Ajzen's (2010) guidelines for developing TPB measures. Each measure was assessed twice, once in relation to frequent hand washing (‘Washing your hands every time you come into contact with objects or external environments in the next week’) and once in relation to social distancing (‘Limiting your outings to the bare minimum in the next week’).
3.3.1. Attitude
Participants were asked to report their attitude separately towards each of the two behaviours on four 7‐point semantic differential scales (bad/good; harmful/beneficial; foolish/wise; useless/useful; see White, Smith, Terry, Greenslade, & McKimmie, 2009). Alpha values were satisfactory (hand washing: α = .82; social distancing: α = .91).
3.3.2. Subjective norms
Four items were used to assess injunctive (″Most people who are important to me approve of the fact that I [behaviour]″; ″Among the people who are important to you, how many would approve your [behaviour]″; 1 = none, 7 = all) and descriptive aspects of subjective norms (″Most people like me engage in [behaviour]″; 1 = strongly disagree, 7 = strongly agree; ″Think about the people who are important to you. In your opinion, what percentage of them [behaviour]″; 1 = 0%, 7 = 100%). Alpha values were satisfactory (hand washing: α = .73; social distancing: α = .81).
3.3.3. Perceived behavioural control
To assess perceived behavioural control, we used three items: ″The number of events outside my control which could prevent me from engaging in [behaviour]″ (1 = very few, 7 = numerous; reverse‐scored); ″I think I can easily control whether I can [behaviour]″ (1 = definitely false, 7 = definitely true); ″For me, [behaviour] would be″ (1 = very difficult, 7 = very easy). Alpha values were satisfactory (hand washing: α = .77; social distancing: α = .72).
3.3.4. Intention
Two items were created ad‐hoc to measure intention in relation to each protective behaviour: ″I intend to [behaviour]″, and ″I think I will [behaviour]″ (1 = strongly disagree, 7 = strongly agree). The Spearman‐Brown coefficient for two‐item scale reliability (Eisinga, Grotenhuis, & Pelzer, 2013) was significant (hand washing: ρ = .93, p < .001; social distancing: ρ = .95, p < .001).
3.3.5. Risk perception
In line with previous literature on health behaviours (Brewer et al., 2007), we assessed three dimensions of risk perception: perceived likelihood, susceptibility and severity. Perceived likelihood was assessed with three items adapted from Weinstein et al. (2007): ″If I can't get the vaccine, I think the chance I have of contracting Covid‐19 in the coming months will be…″ (1 = almost zero; 7 = almost certain); ″If I don't comply with the preventive measures, I think the chance I have of contracting Covid‐19 in the coming months will be…″ (1 = almost zero; 7 = almost certain); ″Without the vaccine, do you think you're likely to get the Covid‐19 in the next months?″ (1 = very unlikely; 7 = very likely; α = .86). Perceived susceptibility was assessed with three items adapted from Rimal and Real (2003): ″Compared to most people my age, my risk of getting Covid‐19 is…″; ″The likelihood of me getting Covid‐19 is…″; ″Compared to most people, the possibility of me getting infected with Covid‐19 is…″ (1 = extremely low; 7 = extremely high; α = .89). Perceived severity was assessed with three items adapted from Rimal and Real (2003): ″Covid‐19 is a much more dangerous epidemic than the others″; ″Covid‐19 is more deadly than most people realize″; ‘″Stopping Covid‐19 will be much more difficult than other epidemics″ (1 = strongly disagree; 7 = strongly agree; α = .74).
3.3.6. Protective behaviours
Frequent hand washing (″In the last week I have washed my hands every time I came into contact with objects or external environments″; 1 = false, 7 = true) and social distancing (″In the last week I have limited my outings to the bare minimum″; 1 = false, 7 = true) were assessed each with one ad‐hoc item.
4. RESULTS
4.1. Analytic strategy
A multivariate analysis of variance (MANOVA) and a a test were run to determine attrition in the sample, that is, whether those individuals who completed only the first questionnaire (n = 151) were significantly different from those respondents who completed both questionnaires (n = 252). The MANOVA was applied to age and to all the predictor variables for social distancing and hand washing, the χ2 test was applied to sex of participants. The data were inspected for missingness. Missing data represented 0.08% of total responses. Little's MCAR test was significant, χ2 (178) = 231.84, p = .01, suggesting that the data were not missing completely at random. Although the percentage of missing data was very small, following Graham's (2009) indications, we replaced missing data by using the EM algorithm.
Bivariate correlations between the study variables were computed. Two regression models with latent variables were tested in LISREL 8.80 (Jöreskog & Sörbom, 2006), one for each protective behaviour (see Figures 1 and 2). The maximum likelihood estimation method was used. In each model, attitudes, subjective norms, perceived behavioural control, and risk perception were entered as predictors, intention was entered as the mediator (of attitudes, subjective norms, and perceived behavioural control effects), and the protective behaviour was the outcome variable. In accordance with TPB, in each model, the direct path from perceived behavioural control to the protective behaviour was estimated. In addition, we estimated in each model the direct path from risk perception to the protective behaviour. Single items were used as manifest indicators for attitudes, subjective norms, perceived behavioural control, and intention. For risk perception, the three composite scores of probability, susceptibility, and severity were used as manifest indicators. In both models, the latent variable of behaviour was identified by fixing the measurement error of the single item indicator to zero.
FIGURE 1.
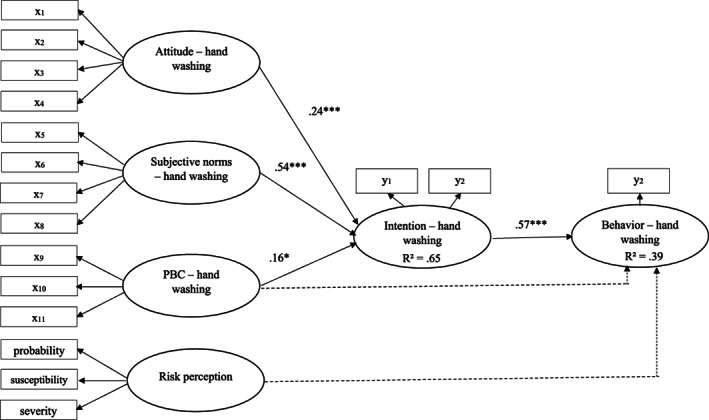
Regression model with latent variables, outcome variable: hand washing (N = 248). Dotted arrows indicate non‐significant paths. Standardized coefficients are reported
FIGURE 2.
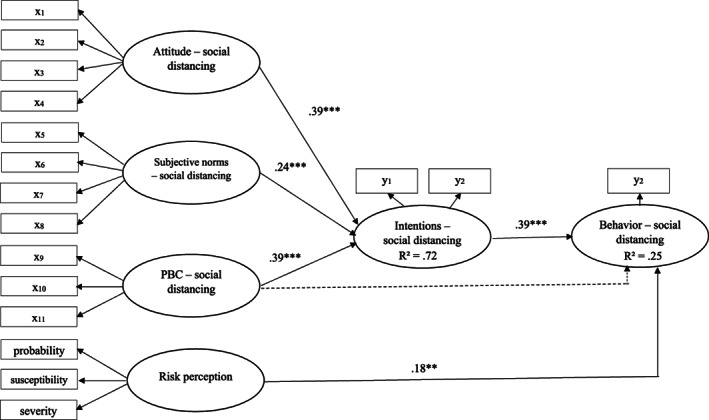
Regression model with latent variables, outcome variable: social distancing (N = 248). Dotted arrows indicate non‐significant paths. Standardized coefficients are reported
The goodness‐of‐fit of the tested models was evaluated using the chi‐square statistic (χ2), the χ2/df ratio, the comparative fit index (CFI), the root‐mean‐square error of approximation (RMSEA), and the standardized root‐mean‐square residual (SRMR). The fit of a model is satisfactory with a χ2/df ratio smaller than 3 (Kline, 2010), a CFI value equal or greater than .95, an RMSEA value equal or lower than .06, an SRMR equal or lower than .08 (Hu & Bentler, 1999). Mediation was tested using bootstrapping procedures (Hayes & Preacher, 2013) with 2000 resamples and 95% confidence intervals.
Finally, the two regression models were tested again including age and sex of participants as covariates.
4.2. Attrition in the sample
As far as sex of participants is concerned, the χ2 test did not reveal any differences between the two groups χ2(1) = 2.16, p = .14, φ = 0.14. Results of the MANOVA showed a significant multivariate effect: F(13,380) = 1.98, p = .02, η 2 p = 0.06. A closer inspection of univariate effects showed, however, very few significant differences. Respondents who dropped out after completing the first questionnaire were significantly older (M = 38.17 years, SD = 1.26) than participants who responded to both questionnaires (M = 34.82 years, SD = 0.95), F(1,392) = 4.54, p = .03, η 2 p = 0.01. In addition, participants who dropped out after completing the first questionnaire showed lower perceived behavioural control in relation to social distancing (M = 5.23, SD = 1.25) compared to participants who responded both questionnaires (M = 5.54, SD = 1.22), F(1,392) = 5.78, p = .02, η 2 p = 0.02. Finally, participants who answered the first questionnaire only reported more cases of Covid‐19 in their family (M = 0.27, SD = 0.69) compared to participants who completed the whole study (M = 0.15, SD = 0.44), F(1,392) = 1.22, p = .03, η 2 p = 0.01.
4.3. Bivariate correlations
Correlations between the study variables are reported in Table 1. All the correlations were in the expected direction. Attitude, norms and PBC were all associated with the relative behavioural intentions, which in turn were significantly related to the respective behaviour. The two target intentions as well as behaviours were only moderately correlated.
TABLE 1.
Correlations between the study variables (N = 248)
| 1. | 2. | 3. | 4. | 5. | 6. | 7. | 8. | 9. | 10. | 11. | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Attitude (1) | ‐ | ||||||||||
| 2. Norms (1) | 0.38 *** | ‐ | |||||||||
| 3. PBC (1) | 0.22 *** | 0.40 *** | ‐ | ||||||||
| 4. Intention (1) | 0.49 *** | 0.63 *** | 0.46 *** | ‐ | |||||||
| 5. Attitude (2) | 0.30 *** | 0.25 *** | 0.19 ** | 0.38 *** | ‐ | ||||||
| 6. Norms (2) | 0.17 ** | 0.54 *** | 0.22 *** | 0.35 *** | 0.46 *** | ‐ | |||||
| 7. PBC (2) | 0.10 | 0.18 ** | 0.29 *** | 0.30 *** | 0.39 *** | 0.41 *** | ‐ | ||||
| 8. Intention (2) | 0.22 ** | 0.29 *** | 0.22 *** | 0.47 *** | 0.68 ** | 0.60 *** | 0.60 *** | ‐ | |||
| 9. Risk Perception | 0.32 *** | 0.10 | −0.05 | 0.24 *** | 0.43 *** | 0.10 | −0.01 | 0.28 *** | ‐ | ||
| 10. Behaviour (1) | 0.37 *** | 0.41 *** | 0.35 *** | 0.61 *** | 0.20 *** | 0.26 *** | 0.19 ** | 0.25 *** | 0.13 * | ‐ | |
| 11. Behaviour (2) | 0.22 *** | 0.13 * | 0.06 | 0.22 *** | 0.44 *** | 0.32 *** | 0.25 *** | 0.46 *** | 0.26 *** | 0.31 *** | ‐ |
| M | 6.54 | 5.74 | 5.31 | 6.24 | 6.12 | 5.58 | 5.54 | 6.04 | 4.16 | 6.20 | 6.18 |
| SD | 0.69 | 0.84 | 1.22 | 1.10 | 1.07 | 0.97 | 1.23 | 1.30 | 0.98 | 1.12 | 1.21 |
Note: (1) = Frequent hand washing; (2) = Social distancing; PBC, perceived behavioural control.
p ≤ .05.
p ≤ .01.
p ≤ .001.
4.4. Regression models
The two regression models are shown in Figures 1 and 2, respectively. Goodness‐of‐fit statistics were satisfactory for the model including hand washing as the outcome variable: χ2(108) = 204.57, p = .00; χ2/df = 1.89; CFI = .97; SRMR = .06; RMSEA = .06, as well as for the model including social distancing as the outcome variable: χ2(108) = 221.76, p = .00; χ2/df = 2.05; CFI = .98; SRMR = .07; RMSEA = .06. As can be seen in Figure 1, attitude, subjective norms, and PBC were significant predictors of intentions, with subjective norms being the strongest predictor. Intentions in turn significantly predicted hand washing. However, risk perception was not significantly associated with hand washing. The direct path from PBC to hand washing was also not significant. In the model including social distancing as the outcome variable (Figure 2), the TPB variables were all significantly related to intentions, but attitude and PBC were more strongly associated with intentions than subjective norms. The direct path from PBC to social distancing was also significant. Moreover, risk perception was significantly associated with social distancing, though this path appeared to be weaker than the path linking intention to social distancing.
4.5. Mediation analyses
Bootstrapped confidence intervals are shown in Table 2. In the model including hand washing as the outcome variable, mediation of intention was significant for attitude and subjective norms, but not for perceived behavioural control. In the model including social distancing as the outcome variable, the three mediation effects were all significant.
TABLE 2.
Test of indirect effects of intention with bootstrapping procedures
| Outcome variable | Predictor | Mean bootstrap estimate | 95% confidence interval |
|---|---|---|---|
| Hand washing | Attitude | 0.43 | [0.07, 0.82] |
| Subjective norm | 0.95 | [0.49, 1.67] | |
| Perceived behavioural control | 0.19 | [−0.06, 0.47] | |
| Limiting exits | Attitude | 0.47 | [0.11, 0.70] |
| Subjective norm | 0.33 | [0.02, 0.56] | |
| Perceived behavioural control | 0.70 | [0.17, 1.94] |
Note: Mean bootstrap estimates are based on 2,000 bootstrap samples.
4.6. Testing sex and age as covariates
The fit of the two models including sex and age as covariates (N = 247; 1 missing on age) was acceptable, albeit slightly poorer than the original models; for the model with hand washing as the outcome variable: χ2(132) = 263.86, p = .00; χ2/df = 2.00; CFI = .96; SRMR = .06; RMSEA = .06; for the model with social distancing as the outcome variable: χ2(132) = 297.29, p = .00; χ2/df = 2.25; CFI = .97; SRMR = .07; RMSEA = .07. Age was a significant predictor of both hand washing (γ = 0.17, p < .001) and social distancing (γ = 0.12, p < .05), while the regression paths for sex were non‐significant (hand washing: γ = −0.03, ns; social distancing: γ = −0.07, ns). Importantly, the pattern of results for the other variables was unchanged.
5. DISCUSSION
The Covid‐19 health emergency has highlighted how human behaviour is of vital importance in controlling the spread of epidemics (Flaxman et al., 2020; Islam et al., 2020; Michie & West, 2020). Preventive measures such as social distancing, hand washing, mask wearing are the only means to contain infections, at least in the absence of a vaccine or treatment. In order to enhance adherence to these measures, it is crucial to have adequate knowledge about the factors underlying the enactment of recommended behaviours. Our results highlight some important issues. One major finding is that TPB constructs are overall better predictors of the protective behaviours examined here compared to risk perception. Although it would be straightforward to think that humans will respond to risk by engaging in protective behaviours, this may not always be the case (Schwarzer, 2001). Indeed, our results found no relationship between risk perceptions and frequent hand washing and the relationship between risk perception and social distancing, albeit significant, was weaker compared to the relationship between intention and social distancing. Overall, these results indicate that risk perceptions compared to TPB variables did not play a fundamental role in shaping subsequent behaviour in our sample. This is in line with recent studies, which have showed risk perceptions (i.e., vulnerability) to be only weakly related to preventive behaviours in the context of Covid‐19 (Clark, Davila, Regis, & Kraus, 2020).
Another finding that warrants attention is the different association of TPB variables with intentions to engage in the two behaviours examined. While in the case of social distancing attitude and PBC exerted greater influence, for frequent hand washing subjective norms were a major predictor. It is important to note that the subjective norm component has been regarded as the weakest element of TRA/TPB, because of its predictive power. In a meta‐analysis, Armitage and Conner (2001) showed that the average relationship between subjective norms and intentions was weaker than the relationship between the other constructs and intentions. Different explanations have been proposed for this result, including poor measurement (i.e., single item measures) and the need to enlarge the subjective norm concept (i.e., including the descriptive source of normative influence; see White et al., 2009). Both these recommendations were followed in the present study. However, in the present study, subjective norms showed a strong association with hand washing, but only a discrete association with social distancing. One possible explanation for the different effect of social norms on behaviour might rely on the costs (perceived and objective) associated to the implementation of different behaviours. Behaviours which are thought to be more costly for a person should be less dependent on normative influence (Chung & Rimal, 2016). In this regard, hand washing compared to social distancing is very likely to be perceived as easier to carry out. On the contrary, given that social distancing implies the effort of having to stay home and distant from close others, it likely challenges the person also from an emotional point of view making it harder to comply with this behaviour. Normative influence should, in this case, have a weaker effect on behaviour as demonstrated in this study. In addition, our results suggest that in the case of costly behaviours (e.g., social distancing) intentions to perform behaviour will predominantly rely on personal attitudes and beliefs.
The present results provide support for the contention that the relative importance of TPB constructs varies across behaviours (Fishbein & Ajzen, 1975) and suggest that interventions to enhance compliance with recommended behaviours during a pandemic should be diversified by taking into account the different factors underlying the behaviour. During spring 2020, a #stayathome campaign was sustained not only by the governments, but also by celebrities who represented a considerable source of normative influence. However, our results suggest that this sort of intervention might have been more relevant for other preventive measures such as frequent hand washing, thus providing support for the claim that large‐scale behaviour change should be informed by a scientific understanding of the processes underlying behaviour (Michie & West, 2020).
Our findings show that PBC also played a different role in predicting intentions of hand washing and social distancing, being more influential for the latter. The fact that PBC was a stronger predictor of intention of social distancing compared to hand washing is in line with the contention that PBC is more relevant when potential constraints are perceived on action (Ajzen, 1991; Armitage & Conner, 2001). In other words, the impact of PBC on intentions would be a function of the controllability of the behaviour such that for behaviours, which are under volitional control and thus more easily carried out such as hand washing, PBC should not improve prediction of intentions (Ajzen, 1985; Kiriakidis, 2015). Therefore, in the case of behaviours that are not totally under volitional control and thus more difficult to accomplish such as social distancing, interventions should be designed with the aim of enhancing self‐efficacy, for instance by showing ways to effectively implement social distancing.
As to the direct link between PBC and behaviour, no significant relation emerged for both hand washing and social distancing. According to Ajzen and Madden (1986), in order for PBC to predict behaviour, the latter should not be under complete volitional control—as in the case of social distancing—and importantly, PBC should reflect actual control with a certain degree of accuracy. Research has shown that PBC generally explains only a small amount in the variance explained of behaviour after controlling for intention (Armitage & Conner, 2001). This may be due to the fact that individuals are generally not very good at judging the degree of actual control they have over a behaviour (Sheeran, Trafimow, & Armitage, 2003) and this might represent a reason for the weak or null link to behaviour found in this study.
Finally, results also showed that risk perceptions were related to social distancing but not hand washing. This is somehow counterintuitive given that risk perception should be more strongly related to behaviours, which are relatively easy to carry out compared to behaviours that are more difficult to carry out (Brewer et al., 2007). The results found in this context hint to the fact that additional variables may have played a role in the relation between risk perceptions and the behaviours we considered (especially hand washing). Thus, further research should investigate the role of possible moderators (e.g., worry; see Ferrer, Portnoy, & Klein, 2013; Klein, Zajac, & Monin, 2009) which may partially explain the results found in this study.
Some limitations of the present research need to be acknowledged. First, unfortunately the number of participants who dropped out after completing the first part of the questionnaire was very high. This strongly reduced our final sample. Second, attrition analyses revealed significant differences between participants who completed only the first part of the questionnaire and participants who completed the whole study. Yet, it is worth mentioning that these differences were small in terms of effect size. Third, we investigated only two protective behaviours. It should be noted that the assessment of TPB constructs requires that each variable is assessed with reference to the relative behaviour. In order to limit the length of our questionnaire, we selected only two behaviours that at the time, the research was conducted were highly relevant for participants. Future research might benefit from testing a wider range of protective behaviours in order to identify their specific antecedents. Last but not least, our sample was limited to people residing in Italy. As already noted, Italy was the second country after China experiencing the diffusion of Covid‐19. While this research was being carried out, other countries were at a different stage of the pandemic. Nevertheless, the antecedents of protective behaviours during the later stages of the pandemic could be investigated in a wide range of countries in future studies.
In sum, this work offers a comprehensive picture of which antecedents impact on people's compliance to different recommended behaviours during the COVID‐19 pandemic. Specifically, these results suggest that in order to be effective, preventive campaigns and communications should consider different aspects strictly depending on the type of behaviour they want to promote/limit. Gathering information and awareness of what factors will lead to implementation of preventive behaviours is of crucial importance not only to inform academics on this topic but also to provide governments and local institutions with clear and updated information, which will ultimately benefit the community during the delicate phase of the pandemic.
Supporting information
Community and Social Impact Statement
ACKNOWLEDGEMENTS
We would like to thank Andrea Baruzzi for her assistance in data collection.
Trifiletti E, Shamloo SE, Faccini M, Zaka A. Psychological predictors of protective behaviours during the Covid‐19 pandemic: Theory of planned behaviour and risk perception. J Community Appl Soc Psychol. 2022;32(3):382–397. 10.1002/casp.2509
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are openly available in Open Science Framework at https://osf.io/v5jgm/?view_only=0978e1a36bbb4b74ba4d0ca9ebba75e9
REFERENCES
- Ajzen, I. (1985). From intentions to actions: A theory of planned behavior. In Kuhl J. & Beckmann J. (Eds.), Action control: From cognition to behavior. Heidelberg: Springer. [Google Scholar]
- Ajzen, I. (1991). The theory of planned behavior. Organizational Behavior and Human Decision Processes, 50(2), 179–211. 10.1016/0749-5978(91)90020-T [DOI] [Google Scholar]
- Ajzen, I . (2010). Constructing a theory of planned behaviour questionnaire. Retrieved April 11, 2020, from http://people.umass.edu/aizen/pdf/tpb.measurement.pdf
- Ajzen, I. , & Fishbein, M. (1980). Understanding Attitudes and Predicting Social Behavior. Englewood‐Cliff, NJ: Prentice‐Hall. [Google Scholar]
- Ajzen, I. , & Madden, T. J. (1986). Prediction of goal‐directed behavior: Attitudes, intentions, and perceived behavioral control. Journal of Experimental Social Psychology, 22(5), 453–474. 10.1016/0022-1031(86)90045-4 [DOI] [Google Scholar]
- Albarracin, D. , Johnson, B. T. , Fishbein, M. , & Muellerleile, P. A. (2001). Theories of reasoned action and planned behavior as models of condom use: A meta‐analysis. Psychological Bulletin, 127(1), 142–161. 10.1037/0033-2909.127.1.142 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Armitage, C. J. , & Conner, M. (2001). Efficacy of the theory of planned behaviour: A meta‐analytic review. British Journal of Social Psychology, 40(4), 471–499. 10.1348/014466601164939 [DOI] [PubMed] [Google Scholar]
- Barr, M. , Raphael, B. , Taylor, M. , Stevens, G. , Jorm, L. , Giffin, M. , & Lujic, S. (2008). Pandemic influenza in Australia: Using telephone surveys to measure perceptions of threat and willingness to comply. Infectious Diseases, 8, 117–130. 10.1186/1471-2334-8-117 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bish, A. , & Michie, S. (2010). Demographic and attitudinal determinants of protective behaviours during a pandemic: A review. British Journal of Health Psychology, 15(4), 797–824. 10.1348/135910710X485826 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brewer, N. T. , Chapman, G. B. , Gibbons, F. X. , Gerrard, M. , McCaul, K. D. , & Weinstein, N. D. (2007). Meta‐analysis of the relationship between risk perception and health behaviour: The example of vaccination. Health Psychology, 26(2), 136–145. 10.1037/0278-6133.26.2.136 [DOI] [PubMed] [Google Scholar]
- Brug, J. , Aro, A. R. , Oenema, A. , de Zwart, O. , Richardus, J. H. , & Bishop, G. D. (2004). SARS risk perception, knowledge, precautions, and information sources, The Netherlands. Emerging Infectious Disease, 10(8), 1486–1489. 10.3201/eid1008.040283 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Champion, V. L. , & Skinner, C. S. (2008). The health belief model. Health Behaviour and Health Education: Theory, Research, And Practice, 4, 45–65. [Google Scholar]
- Cheng, C. , & Ng, A. (2006). Psychosocial factors predicting SARS‐preventive behaviors in four major SARS‐affected regions. Journal of Applied Social Psychology, 36(1), 222–247. 10.1111/j.0021-9029.2006.00059.x [DOI] [Google Scholar]
- Chung, A. , & Rimal, R. N. (2016). Social norms: A review. Review of Communication Research, 4, 1–28. 10.12840/issn.2255-4165.2016.04.01.008 [DOI] [Google Scholar]
- Clark, C. , Davila, A. , Regis, M. , & Kraus, S. (2020). Predictors of COVID‐19 voluntary compliance behaviors: An international investigation. Global Transitions, 2, 76–82. 10.1016/j.glt.2020.06.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Conner, M. , & Norman, P. (2005). Predicting health behaviour: A social cognition approach. In Conner M. & Norman P. (Eds.), Predicting health behaviour. Maidenhead, England: Open University Press. [Google Scholar]
- Conner, M. , & Sparks, P. (2005). Theory of planned behaviour and health behaviour. In Conner M. & Norman P. (Eds.), Predicting health behaviour. Maidenhead, England: Open University Press. [Google Scholar]
- Eastwood, K. , Durrheim, D. , Francis, J. L. , Tursan d'Espaignet, E. , Duncan, S. , Islam, F. , & Speare, R. (2009). Knowledge about pandemic influenza and compliance with containment measures among Australians. Bulletin World Health Organisation, 87, 588–594. 10.2471/BLT.08.060772 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eisinga, R. , Grotenhuis, M. , & Pelzer, B. (2013). The reliability of a two‐item scale: Pearson, Cronbach, or Spearman‐Brown? International Journal of Public Health, 58, 637–642. 10.1007/s00038-012-0416-3 [DOI] [PubMed] [Google Scholar]
- Ferrer, R. A. , Portnoy, D. B. , & Klein, W. M. (2013). Worry and risk perceptions as independent and interacting predictors of health protective behaviors. Journal of Health Communication, 18(4), 397–409. 10.1080/10810730.2012.727954 [DOI] [PubMed] [Google Scholar]
- Fishbein, M. , & Ajzen, I. (1975). Belief, attitude, intention, and behavior: An introduction to theory and research. New York, NY: Wiley. [Google Scholar]
- Flaxman, S. , Mishra, S. , Gandy, A. , Unwin, H. , Mellan, T. , Coupland, H. , … Bhatt, S. (2020). Estimating the effects of non‐pharmaceutical interventions on COVID‐19 in Europe. Nature, 584, 257–261. 10.1038/s41586-020-2405-7 [DOI] [PubMed] [Google Scholar]
- Floyd, D. L. , Prentice‐Dunn, S. , & Rogers, R. W. (2000). A meta‐analysis of research on protection motivation theory. Journal of Applied Social Psychology, 30(2), 407–429. 10.1111/j.1559-1816.2000.tb02323.x [DOI] [Google Scholar]
- Graham, J. W. (2009). Missing data analysis: Making it work in the real world. Annual Review of Psychology, 60, 549–576. 10.1146/annurev.psych.58.110405.085530 [DOI] [PubMed] [Google Scholar]
- Harrison, J. A. , Mullen, P. D. , & Green, L. W. (1992). A meta‐analysis of studies of the health belief model with adults. Health Education Research, 7(1), 107–116. 10.1093/her/7.1.107 [DOI] [PubMed] [Google Scholar]
- Hausenblas, H. A. , Carron, A. V. , & Mack, D. E. (1997). Application of the theories of reasoned action and planned behavior to exercise behavior: a meta‐analysis. Journal of Sport and Exercise Psychology, 19(1), 36–51. 10.1123/jsep.19.1.36 [DOI] [Google Scholar]
- Hayes, A. F. , & Preacher, K. J. (2013). Conditional process modeling: Using structural equation modeling to examine contingent causal processes. In Hancock G. R. & Mueller R. O. (Eds.), Structural equation modeling: A second course (2nd ed., pp. 217–264). Greenwich, CT: Information Age. [Google Scholar]
- Hu, L. , & Bentler, P. (1999). Cut‐off criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling, 6(1), 1–55. 10.1080/10705519909540118 [DOI] [Google Scholar]
- Islam, N. , Sharp, S. J. , Chowell, G. , Shabnam, S. , Kawachi, I. , Lacey, B. , … White, M. (2020). Physical distancing interventions and incidence of coronavirus disease 2019: natural experiment in 149 countries. British Medical Journal, 370, m2743. 10.1136/bmj.m2743 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jones, J. H. , & Salathe, M. (2009). Early assessment of anxiety and behavioural response to novel swine‐origin influenza A(H1N1). PLoS One, 4(12), e8032. 10.1371/journal.pone.0008032 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jöreskog, K. , & Sörbom, D. (2006). LISREL 8.8 for Windows. Skokie, IL: Scientific Software International, Inc. [Google Scholar]
- Kiriakidis, S. (2015). Theory of planned behaviour: The intention‐behaviour relationship and the perceived behavioural control (PBC) relationship with intention and behaviour. International Journal of Strategic Innovative Marketing, 3(2), 40–51. 10.15556/ijsim.02.03.004 [DOI] [Google Scholar]
- Klein, W. M. , Zajac, L. E. , & Monin, M. M. (2009). Worry as a moderator of the association between risk perceptions and quitting intentions in young adult and adult smokers. Annals of Behavioral Medicine, 38(3), 256–261. 10.1007/s12160-009-9143-2 [DOI] [PubMed] [Google Scholar]
- Kline, R. B. (2010). Principles and practice of structural equation modelling. New York, NY: The Guilford Press. [Google Scholar]
- Kluge, H. H. P. (2020). Statement – Behavioural insights are valuable to inform the planning of appropriate pandemic response measures [Press release]. Retrieved from https://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/statements/statement-behavioural-insights-are-valuable-to-inform-the-planning-of-appropriate-pandemic-response-measures
- Lau, J. T. F. , Yang, X. , Tsui, H. Y. , & Kim, J. H. (2003). Monitoring community responses to the SARS epidemic in Hong Kong: From day 10 to day 62. Journal of Epidemiology and Community Health, 57, 864–870. 10.1136/jech.57.11.864 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leung, G. M. , Lam, T. H. , Ho, L. M. , Ho, S. Y. , Chan, B. H. Y. , Wong, I. O. L. , & Hedley, A. J. (2003). The impact of community psychological responses on outbreak control for severe acute respiratory syndrome in Hong Kong. Journal of Epidemiology and Community Health, 57, 857–863. 10.1136/jech.57.11.857 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liao, Q. , Cowling, B. J. , Lam, W. W. T. , Fielding, R. , & Semple, M. (2011). Factors affecting intention to receive and self‐reported receipt of 2009 pandemic (H1N1) vaccine in Hong Kong: A longitudinal study. PLoS One, 6(3), e17713. 10.1371/journal.pone.0017713 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Michie, S. , & West, R. (2020). Behavioural, environmental, social, and systems interventions against covid‐19. British Medical Journal, 370, m2982. 10.1136/bmj.m2982 [DOI] [PubMed] [Google Scholar]
- Milne, S. , Sheeran, P. , & Orbell, S. (2000). Prediction and intervention in health‐related behaviour: A meta‐analytic review of protection motivation theory. Journal of Applied Social Psychology, 30(1), 106–143. 10.1111/j.1559-1816.2000.tb02308.x [DOI] [Google Scholar]
- Myers, L. B. , & Goodwin, R. (2011). Determinants of adults' intention to vaccinate against pandemic swine flu. BMC Public Health, 11, 15. 10.1186/1471-2458-11-15 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nicola, M. , Alsafi, Z. , Sohrabi, C. , Kerwan, A. , Al‐Jabir, A. , Iosifidis, C. , … Agha, R. (2020). The socio‐economic implications of the coronavirus pandemic (COVID‐19): A review. International Journal of Surgery, 78, 185–193. 10.1016/j.ijsu.2020.04.018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oliver, R. L. , & Berger, P. K. (1979). A path analysis of preventive health care decision models. Journal of Consumer Research, 6(2), 113–122. 10.1086/208755 [DOI] [Google Scholar]
- Quah, S. R. , & Hin‐Peng, L. (2004). Crisis prevention and management during SARS outbreak, Singapore. Emerging Infectious Disease, 10, 364–368. 10.3201/eid1002.030418 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rich, A. , Brandes, K. , Mullan, B. A. , & Hagger, M. S. (2015). Theory of planned behavior and adherence in chronic illness: A meta‐analysis. Journal of Behavioral Medicine, 38, 673–688. 10.1007/s10865-015-9644-3 [DOI] [PubMed] [Google Scholar]
- Rimal, R. N. , & Real, K. (2003). Perceived risk and efficacy beliefs as motivators of change: Use of the risk perception attitude (RPA) framework to understand health behaviors. Human Communication Research, 29(3), 370–399. 10.1111/j.1468-2958.2003.tb00844.x [DOI] [Google Scholar]
- Rogers, R. W. (1975). A protection motivation theory of fear appeals and attitude change. The Journal of Psychology, 91(1), 93–114. 10.1080/00223980.1975.9915803 [DOI] [PubMed] [Google Scholar]
- Rosenstock, I. (1974). Historical origins of the health belief model. Health Education Monographs, 2, 328–335. 10.1177/109019817400200403 [DOI] [PubMed] [Google Scholar]
- Rosenstock, I. M. , Strecher, V. J. , & Becker, M. H. (1988). Social learning theory and the health belief model. Health Education & Behaviour, 15, 175–183. 10.1177/109019818801500203 [DOI] [PubMed] [Google Scholar]
- Rubin, G. J. , Amlôt, R. , Page, L. , & Wessely, S. (2009). Public perceptions, anxiety and behavioural change in relation to the swine flu outbreak: A cross‐sectional telephone survey. British Medical Journal, 339, b2651. 10.1136/bmj.b2651 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schwarzer, R. (2001). Social‐cognitive factors in changing health‐related behaviours. Current Directions in Psychological Science, 10(2), 47–51. 10.1111/1467-8721.00112 [DOI] [Google Scholar]
- Sheeran, P. , & Taylor, S. (1999). Predicting intentions to use condoms: A meta‐analysis and comparison of the theories of reasoned action and planned behavior. Journal of Applied Social Psychology, 29(8), 1624–1675. 10.1111/j.1559-1816.1999.tb02045.x [DOI] [Google Scholar]
- Sheeran, P. , Trafimow, D. , & Armitage, C. J. (2003). Predicting behaviour from perceived behavioural control: Tests of the accuracy assumption of the theory of planned behaviour. British Journal of Social Psychology, 42(3), 393–410. 10.1348/014466603322438224 [DOI] [PubMed] [Google Scholar]
- Taghrir, M. H. , Borazjani, R. , & Shiraly, R. (2020). COVID‐19 and Iranian medical students; A survey on their related‐knowledge, preventive behaviours and risk perception. Archives of Iranian medicine, 23(4), 249–254. 10.34172/aim.2020.06 [DOI] [PubMed] [Google Scholar]
- Weinstein, N. D. , Kwitel, A. , McCaul, K. D. , Magnan, R. E. , Gerrard, M. , & Gibbons, F. X. (2007). Risk perceptions: Assessment and relationship to influenza vaccination. Health Psychology, 26(2), 146–151. 10.1037/0278-6133.26.2.146 [DOI] [PubMed] [Google Scholar]
- West, R. , Michie, S. , Rubin, G. J. , & Amlôt, R. (2020). Applying principles of behaviour change to reduce SARS‐CoV‐2 transmission. Nature Human Behavior, 4, 451–459. 10.1038/s41562-020-0887-9 [DOI] [PubMed] [Google Scholar]
- White, K. M. , Smith, J. R. , Terry, D. J. , Greenslade, J. H. , & McKimmie, B. M. (2009). Social influence in the theory of planned behaviour: The role of descriptive, injunctive, and in‐group norms. British Journal of Social Psychology, 48(1), 135–158. 10.1348/014466608X295207 [DOI] [PubMed] [Google Scholar]
- Wong, C. Y. , & Tang, C. S. K. (2005). Practice of habitual and volitional health behaviours to prevent severe acute respiratory syndrome among Chinese adolescents in Hong Kong. Journal of Adolescent Health, 36(3), 193–200. 10.1016/j.jadohealth.2004.02.024 [DOI] [PMC free article] [PubMed] [Google Scholar]
- World Health Organization (2020). Timeline of WHO's response to Covid‐19. Retrieved from https://www.who.int/news-room/detail/29-06-2020-covidtimeline.
- Worldmeters (2021). Covid‐19 coronavirus pandemic. Retrieved from https://www.worldometers.info/coronavirus/. [Google Scholar]
- Zaka, A. , Shamloo, S. E. , Fiorente, P. , & Tafuri, A. (2020). COVID‐19 pandemic as a watershed moment: A call for systematic psychological health care for frontline medical staff. Journal of Health Psychology, 25(7), 883–887. 10.1177/1359105320925148 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Community and Social Impact Statement
Data Availability Statement
The data that support the findings of this study are openly available in Open Science Framework at https://osf.io/v5jgm/?view_only=0978e1a36bbb4b74ba4d0ca9ebba75e9