

Abstract
Background
Cystic fibrosis (CF) is a common life‐shortening genetic condition caused by a variant in the cystic fibrosis transmembrane conductance regulator (CFTR) protein. A class II CFTR variant F508del (found in up to 90% of people with CF (pwCF)) is the commonest CF‐causing variant. The faulty protein is degraded before reaching the cell membrane, where it needs to be to effect transepithelial salt transport. The F508del variant lacks meaningful CFTR function and corrective therapy could benefit many pwCF. Therapies in this review include single correctors and any combination of correctors and potentiators.
Objectives
To evaluate the effects of CFTR correctors (with or without potentiators) on clinically important benefits and harms in pwCF of any age with class II CFTR mutations (most commonly F508del).
Search methods
We searched the Cochrane Cystic Fibrosis and Genetic Disorders Cystic Fibrosis Trials Register, reference lists of relevant articles and online trials registries. Most recent search: 14 October 2020.
Selection criteria
Randomised controlled trials (RCTs) (parallel design) comparing CFTR correctors to control in pwCF with class II mutations.
Data collection and analysis
Two authors independently extracted data, assessed risk of bias and evidence quality (GRADE); we contacted investigators for additional data.
Main results
We included 19 RCTs (2959 participants), lasting between 1 day and 24 weeks; an extension of two lumacaftor‐ivacaftor studies provided additional 96‐week safety data (1029 participants). We assessed eight monotherapy RCTs (344 participants) (4PBA, CPX, lumacaftor, cavosonstat and FDL169), six dual‐therapy RCTs (1840 participants) (lumacaftor‐ivacaftor or tezacaftor‐ivacaftor) and five triple‐therapy RCTs (775 participants) (elexacaftor‐tezacaftor‐ivacaftor or VX‐659‐tezacaftor‐ivacaftor); below we report only the data from elexacaftor‐tezacaftor‐ivacaftor combination which proceeded to Phase 3 trials. In 14 RCTs participants had F508del/F508del genotypes, in three RCTs F508del/minimal function (MF) genotypes and in two RCTs both genotypes.
Risk of bias judgements varied across different comparisons. Results from 11 RCTs may not be applicable to all pwCF due to age limits (e.g. adults only) or non‐standard design (converting from monotherapy to combination therapy).
Monotherapy
Investigators reported no deaths or clinically‐relevant improvements in quality of life (QoL). There was insufficient evidence to determine any important effects on lung function.
No placebo‐controlled monotherapy RCT demonstrated differences in mild, moderate or severe adverse effects (AEs); the clinical relevance of these events is difficult to assess with their variety and small number of participants (all F508del/F508del).
Dual therapy
Investigators reported no deaths (moderate‐ to high‐quality evidence). QoL scores (respiratory domain) favoured both lumacaftor‐ivacaftor and tezacaftor‐ivacaftor therapy compared to placebo at all time points. At six months lumacaftor 600 mg or 400 mg (both once daily) plus ivacaftor improved Cystic Fibrosis Questionnaire (CFQ) scores slightly compared with placebo (mean difference (MD) 2.62 points (95% confidence interval (CI) 0.64 to 4.59); 1061 participants; high‐quality evidence). A similar effect was observed for twice‐daily lumacaftor (200 mg) plus ivacaftor (250 mg), but with low‐quality evidence (MD 2.50 points (95% CI 0.10 to 5.10)). The mean increase in CFQ scores with twice‐daily tezacaftor (100 mg) and ivacaftor (150 mg) was approximately five points (95% CI 3.20 to 7.00; 504 participants; moderate‐quality evidence). At six months, the relative change in forced expiratory volume in one second (FEV1) % predicted improved with combination therapies compared to placebo by: 5.21% with once‐daily lumacaftor‐ivacaftor (95% CI 3.61% to 6.80%; 504 participants; high‐quality evidence); 2.40% with twice‐daily lumacaftor‐ivacaftor (95% CI 0.40% to 4.40%; 204 participants; low‐quality evidence); and 6.80% with tezacaftor‐ivacaftor (95% CI 5.30 to 8.30%; 520 participants; moderate‐quality evidence).
More pwCF reported early transient breathlessness with lumacaftor‐ivacaftor, odds ratio 2.05 (99% CI 1.10 to 3.83; 739 participants; high‐quality evidence). Over 120 weeks (initial study period and follow‐up) systolic blood pressure rose by 5.1 mmHg and diastolic blood pressure by 4.1 mmHg with twice‐daily 400 mg lumacaftor‐ivacaftor (80 participants; high‐quality evidence). The tezacaftor‐ivacaftor RCTs did not report these adverse effects.
Pulmonary exacerbation rates decreased in pwCF receiving additional therapies to ivacaftor compared to placebo: lumacaftor 600 mg hazard ratio (HR) 0.70 (95% CI 0.57 to 0.87; 739 participants); lumacaftor 400 mg, HR 0.61 (95% CI 0.49 to 0.76; 740 participants); and tezacaftor, HR 0.64 (95% CI, 0.46 to 0.89; 506 participants) (moderate‐quality evidence).
Triple therapy
Three RCTs of elexacaftor to tezacaftor‐ivacaftor in pwCF (aged 12 years and older with either one or two F508del variants) reported no deaths (high‐quality evidence). All other evidence was graded as moderate quality. In 403 participants with F508del/minimal function (MF) elexacaftor‐tezacaftor‐ivacaftor improved QoL respiratory scores (MD 20.2 points (95% CI 16.2 to 24.2)) and absolute change in FEV1 (MD 14.3% predicted (95% CI 12.7 to 15.8)) compared to placebo at 24 weeks. At four weeks in 107 F508del/F508del participants, elexacaftor‐tezacaftor‐ivacaftor improved QoL respiratory scores (17.4 points (95% CI 11.9 to 22.9)) and absolute change in FEV1 (MD 10.0% predicted (95% CI 7.5 to 12.5)) compared to tezacaftor‐ivacaftor. There was probably little or no difference in the number or severity of AEs between elexacaftor‐tezacaftor‐ivacaftor and placebo or control (moderate‐quality evidence). In 403 F508del/F508del participants, there was a longer time to protocol‐defined pulmonary exacerbation with elexacaftor‐tezacaftor‐ivacaftor over 24 weeks (moderate‐quality evidence).
Authors' conclusions
There is insufficient evidence that corrector monotherapy has clinically important effects in pwCF with F508del/F508del.
Both dual therapies (lumacaftor‐ivacaftor, tezacaftor‐ivacaftor) result in similar improvements in QoL and respiratory function with lower pulmonary exacerbation rates. Lumacaftor‐ivacaftor was associated with an increase in early transient shortness of breath and longer‐term increases in blood pressure (not observed for tezacaftor‐ivacaftor). Tezacaftor‐ivacaftor has a better safety profile, although data are lacking in children under 12 years. In this population, lumacaftor‐ivacaftor had an important impact on respiratory function with no apparent immediate safety concerns; but this should be balanced against the blood pressure increase and shortness of breath seen in longer‐term adult data when considering lumacaftor‐ivacaftor.
There is high‐quality evidence of clinical efficacy with probably little or no difference in AEs for triple (elexacaftor‐tezacaftor‐ivacaftor) therapy in pwCF with one or two F508del variants aged 12 years or older. Further RCTs are required in children (under 12 years) and those with more severe respiratory function.
Plain language summary
CFTR correctors, a therapy for cystic fibrosis targeted at specific variants (most commonly F508del)
Review question
We looked at drugs (or drug combinations) for correcting the basic defect in the most common cystic fibrosis (CF)‐causing gene variant (F508del) and assessed their impact on outcomes important to people with CF (pwCF), e.g. survival, quality of life (QoL), lung function and safety.
Background
The CF gene makes a protein that helps salts move across cells in many parts of the body; over 80% of pwCF have at least one copy of F508del, meaning they make a full length of this protein, but it can not move through the cell correctly. Laboratory experiments suggest that if this protein reaches the cell wall, it may be able to function, restore salt movement and correct the chronic problems that pwCF experience. We examined several agents for correcting F508del. Our original review showed that while single drugs alone were not effective, they were when combined with other drugs. This updated review includes single, dual (corrector plus potentiator) and triple therapies (two different correctors plus one potentiator).
Search date
Evidence is current to: 14 October 2020.
Study characteristics
We included 19 studies (2959 pwCF (children and adults)) lasting between 1 day and 24 weeks (with an extension of two studies up to 96 weeks). Eight studies (344 participants) compared monotherapy: 4PBA, CPX, lumacaftor, cavosonstat and FDL169) to placebo (dummy treatment containing no active medicine), six studies (1840 participants) compared dual therapy (lumacaftor‐ivacaftor or tezacaftor‐ivacaftor) to placebo. Five studies (775 participants) assessed triple therapy (elexacaftor‐tezacaftor‐ivacaftor or VX‐659‐tezacaftor‐ivacaftor); only the combination with elexacaftor progressed beyond early studies. In 14 studies participants had two copies of F508del, in two studies participants had one F508del variant and one different variant, while in three studies participants had either two copies of F508del or one copy of F508del and one different variant.
Key results
Monotherapy versus control
These studies did not report any deaths or clinically relevant improvements in QoL scores. There was insufficient evidence to show an effect on lung function. All studies reported side effects, but it is difficult to assess their relevance due to the range of effects and the small number of participants in the studies.
Dual therapy versus control
Neither the lumacaftor‐ivacaftor or tezacaftor‐ivacaftor studies in people with two copies of F508del reported any deaths and there were improvements in QoL and lung function. Pulmonary exacerbation (a flare‐up of symptoms) rates were also lower. Neither combination therapy was linked to severe side effects, although people starting treatment with lumacaftor‐ivacaftor experienced shortness of breath for one to two weeks, this usually stopped without further treatment. More concerningly, in longer studies some people taking lumacaftor‐ivacaftor experienced a rise in blood pressure; two people (out of over 500) even stopped lumacaftor‐ivacaftor treatment because of high blood pressure. These side effects were not reported for tezacaftor‐ivacaftor. Tezacaftor‐ivacaftor therapy has not yet been assessed in children with CF under 12 years old.
Triple therapy versus control.
The three studies reported no deaths. Triple therapies improved QoL scores and lung function, with no difference in the number or severity of side effects; there was a longer time until the next pulmonary exacerbation. There is high‐quality evidence that elexacaftor‐tezacaftor‐ivacaftor therapy is clinically effective with few side effects for pwCF with one or two F508del variants aged 12 years or older. Further RCTs are required in children (under 12 years) and those with more severe respiratory function. The side effect profile of elexacaftor‐tezacaftor‐ivacaftor therapy seems to be similar to tezacaftor‐ivacaftor, but we need to collect information over the longer term.
Quality of the evidence
The overall quality of the evidence varied from low to high. There were generally few details about study design, so we could not make clear judgements on potential biases. We had fewer concerns with the larger more recent studies. In 10 studies, some results were not analysed or reported. Some findings were based on studies that were too small to show important effects and for nine studies the results may not be applicable to all pwCF due to the age (i.e. only adults or only children studied) or an unusual design (pwCF received monotherapy and then combination therapy).
Summary of findings
Background
Description of the condition
Cystic fibrosis (CF) is the most common inherited life‐shortening illness with a prevalence of 1 in 2000 at birth in Northern Europeans (Bobadilla 2002) and varying prevalence in other populations depending on ethnic composition. The affected gene codes for a protein called the cystic fibrosis transmembrane conductance regulator (CFTR) (Riordan 1989; Southern 1997). CFTR protein is transported to the outer cell membrane, where it has a role in the transport of salts (anions, chloride and bicarbonate) in and out of the cell (Rogan 2011). This role is important in all epithelial cells; particularly those lining the airways, pancreatic ducts, sweat gland, bile ducts in the liver and vas deferens.
In the lungs of people with CF (pwCF), defective salt transport leads to a reduction in airway surface liquid volume. This, in turn, leads to compromised mucociliary clearance, which makes the airway susceptible to infection, which initiates a cycle of inflammation, chronic infection and progressive lung damage. Eventually this causes respiratory failure, which is the commonest cause of premature death for pwCF. In addition to the airway problems, the abnormal transepithelial salt transport can lead to complications in other organs. This can result in malnutrition and diabetes (through pancreatic damage), salt depletion (through excess loss in sweat) and subfertility.
Over 2000 variants have been identified in the CFTR gene. These variants are classified according to the impact they have on the synthesis, processing, or function of the CFTR gene (CFMD 2013). Classes of CFTR variant are described in more detail in the additional tables (Table 9) (Rowntree 2003; Southern 2007). Most CFTR variants are associated with a complete loss of CFTR protein and result in a classical CF phenotype. Some CFTR variants are associated with residual function and these tend to be associated with less severe phenotype, e.g. individuals may be pancreatic sufficient and not require pancreatic replacement therapy.
1. Classes of mutations affecting CFTR production, structure and function.
| Class | Example mutation | Impact on CFTR structure and function |
| I | G542X | Synthesis of CFTR is critically impaired, and no functional protein is produced. This is due to the presence of a premature stop codon in the nucleotide sequence. Individuals have minimal CFTR function. |
| II | F508del | A full length of CFTR is produced, but this is structurally abnormal and destroyed by the cell before it reaches the cell membrane. This is called a defect in the intracellular trafficking pathway. Small amounts of CFTR do reach the cell membrane; however here, they display defective ion transport, demonstrating that the F508del mutation is more than just a processing defect. Individuals have minimal CFTR function. |
| III | G551D | CFTR is produced and embedded in the cell membrane, but the chloride channel does not respond ('switch on') to normal stimulation from the cell. This means there is no meaningful ion transport across the protein. Individuals have minimal CFTR function. |
| IV | R347P | CFTR is transported to the outer cell membrane, and responds to normal stimulation, but functions at a low level because chloride ions do not cross the channel appropriately. Individuals have some residual CFTR function. |
| V | A455E | Normal CFTR is produced, but the amount of protein is reduced. Individuals have some residual CFTR function. |
CFTR: cystic fibrosis transmembrane regulator
The commonest CF causing variant, F508del (also known as ΔF508 or delta F508), is found in the majority of pwCF (up to 80% to 90% of some populations, e.g. pwCF from a Northern European heritage). For pwCF with F508del, a full length of protein is transcribed but recognised as misfolded by the cell and is degraded before reaching the cell membrane, where it needs to be positioned to effect transepithelial salt transport. Hence this is a severe variant associated with no meaningful CFTR function. This type of variant is called a class II mutation (or trafficking defect) and much research has explored masking the molecular defect, bypassing the cellular mechanisms and enabling the F508del protein to traffic to the cell membrane, where it may have some normal salt transport capability.
Description of the intervention
Increasing understanding of how different variants affect the production, structure, and function of CFTR has led to the concept of mutation‐specific therapies (Table 9). For class II variants where a full length of protein is produced, recognised as abnormal by the cell and degraded before reaching the cell membrane, scientists have recognised that certain laboratory manoeuvres can affect this process, e.g. reducing cell temperature and the trafficking defect can be overcome (Colledge 1995). In such circumstances the F508del protein may reach the cell membrane, where it has some ability to transport salt. This has lead to the search for molecules that can overcome the F508del trafficking defect and these drugs have been called 'correctors'.
Two distinct scientific approaches have resulted in the recognition of candidate drugs with this mode of action (Amaral 2007):
testing of compounds known to affect CFTR or other ion channels (either pharmaceutical drugs or chemicals which occur naturally in plants, herbs, fruits or food components);
high throughput screening, which involves testing large numbers of diverse chemicals, on laboratory cell lines, to identify which of these may overcome the intracellular trafficking defect.
These approaches have resulted in the identification of small molecules that may be taken orally (Rubenstein 1997; Van Goor 2011).
Since our initial review in 2018, there has been considerable evolution in this field, with the development of further combination agents that address the molecular challenge of correcting the class II variants; these agents are all correctors (e.g. tezacaftor, VX‐659, VX‐445) which are given in combination with the same potentiator ivacaftor. A separate review is available for potentiators (Skilton 2019). This has been accommodated in this updated version of our Cochrane Review and interventions are presented as monotherapy, dual therapy and, more recently for the 2020 update, triple therapy. Given the close relationship of these approaches and to illustrate the development of the field, we have evaluated all of these therapies in this single updated Cochrane Review rather than considering these in separate reviews. Dependent on how the field develops, we may review this decision for future updates of this review.
How the intervention might work
Correction of the basic CF defect may lead to normalisation of airway surface liquid, and correction of mucociliary clearance, reducing the susceptibility to airway infection and inflammation.
In addition to correctors, other drugs which aim to treat the CFTR defect are also under investigation. These include potentiators for class III and IV variants, which enhance the function of mutated CFTR protein embedded in the cell membrane by increasing the time the CFTR salt channel remains open and therapies for class I variant, which act to prevent structural abnormalities of CFTR that occur when premature stop codons terminate protein synthesis. Cochrane Reviews assessing these interventions have been published (Aslam 2017; Skilton 2019).
While correctors are successful at facilitating the F508del protein to reach the cell membrane, it still has suboptimal function. Our initial version of this Cochrane Review suggested that CFTR correctors would need to be combined with other agents (potentiators) to achieve a clinical benefit to pwCF who have a class II variant (e.g F508del) (Southern 2018). For the purposes of this Cochrane Review, we consider combination therapies for class II variants as 'correctors'. We appreciate that these therapies contain single agents with distinct molecular properties, e.g. the dual therapy tezacaftor‐ivacaftor is a combination of a corrector (tezacaftor) and a potentiator (ivacaftor), but together we class this as a corrector therapy.
Why it is important to do this review
CFTR correctors are novel therapies and it is important that randomised controlled trials (RCTs) are conducted and critically appraised to provide clear evidence assessing the benefits and harms of CFTR correctors. It is important that funding bodies have a clear evidence base on which to assess new therapies for CF that aim to correct the basic defect. In addition, critical appraisal of studies will help inform future study design.
New therapies that correct the F508del mutation will have a positive impact on an important proportion of the CF population (Southern 1997). Given the number of pwCF who will be prescribed this treatment, there will be an important healthcare cost. Experience from other licensed agents that correct the underlying CF defect, suggests that these costs may be considerable (NICE 2016).
This review aims to collate evidence from RCTs that have evaluated the benefits and harms of CFTR correctors in pwCF and class II CFTR variants. This is an updated version of the original review (Southern 2018).
Objectives
To evaluate the effects of CFTR correctors (with or without potentiators) on clinically important benefits and harms in pwCF of any age with class II CFTR mutations (most commonly F508del).
Methods
Criteria for considering studies for this review
Types of studies
We have included RCTs of parallel design (published or unpublished). We have not included quasi‐RCTs. We have not included cross‐over studies as we do not feel this study design is appropriate given that the intervention aims to correct the underlying defect of CF and if the intervention is effective it will have an important impact on the course of the disease. This has been established from the data from trials examining ivacaftor for people with class III mutations.
Types of participants
We have included RCTs involving children or adults with CF, as confirmed either by the presence of two disease‐causing variants (at least one class II variant), or by a combination of positive sweat test and recognised clinical features of CF. We have included RCTs that include participants with any level of disease severity. RCTs limited to pwCF who are homozygous for a class II variant are analysed separately.
Types of interventions
A CFTR corrector is defined as a drug which aims to increase the amount of CFTR expressed at the epithelial cell apical membrane, by reducing or preventing degradation of CFTR by normal intracellular mechanisms. The main variant targeted by this approach is F508del. As this review focuses on small molecule therapies that correct the intracellular trafficking defect of variants, such as F508del, interventions that target DNA correction (e.g. antisense technology) are not included.
We have included RCTs comparing CFTR correctors with either placebo or another intervention. We have also included RCTs in which CFTR correctors are administered alongside another class of drug that also aims to improve CFTR function (e.g. potentiators).
Types of outcome measures
We assessed the following outcome measures.
Primary outcomes
Survival
-
Quality of life (QoL) (measured using validated quantitative scales or scores (e.g. Cystic Fibrosis Questionnaire‐Revised (CFQ‐R) (Quittner 2009))
total QoL score
different sub‐domains which may be reported
-
Physiological measures of lung function (L or per cent (%) predicted for age, sex and height)
forced expiratory flow rate at one second (FEV1) (relative change from baseline)
FEV1 absolute values (and change from baseline)
forced vital capacity (FVC) (absolute values and change from baseline)
lung clearance index (LCI) (post hoc change)
other relevant physiological measures of lung function
Secondary outcomes
-
Adverse effects
graded by review authors as mild (therapy does not need to be discontinued)
graded by review authors as moderate (therapy is discontinued, and the adverse effect ceases)
graded by review authors as severe (life‐threatening or debilitating, or which persists even after treatment is discontinued)
other adverse effects of therapy (of any severity) that are not classifiable according to these categories
-
Hospitalisation
number of days
number of episodes
time to next hospitalisation
School or work attendance (i.e. number of days missed)
-
Extra courses of antibiotics (measured as time to the next course of antibiotics and the total number of courses of antibiotics)
oral
intravenous
inhaled
Sweat chloride (change from baseline) as a measure of CFTR function
-
Radiological measures of lung disease (assessed using any scoring system)
chest radiograph scores
computerised tomogram (CT) score
-
Acquisition of respiratory pathogens
Pseudomonas aeruginosa
Staphylococcus aureus
Haemophilus influenzae
other pathogen clinically relevant in CF
-
Eradication of respiratory pathogens (as defined by study authors)
P aeruginosa
S aureus
H influenzae
other pathogen clinically relevant in CF
-
Nutrition and growth (measured as relative change from baseline) (including z scores or centiles)
weight
body mass index (BMI)
height
With regards to exacerbations, investigators of different studies do not use consistent definitions of exacerbations in CF, and sometimes investigators do not explicitly define what they consider to be an exacerbation for their study. Therefore, in order to incorporate data for exacerbations from the different included studies, we have used a broad definition of an exacerbation, such that we consider an exacerbations to be an increase in symptoms, the need for antibiotics or hospital admission, or any combination of these. We report these events under secondary outcome 4.
Search methods for identification of studies
We searched for all relevant published and unpublished studies without restrictions on language (we did not exclude studies reported in a language other than English), year or publication status.
Electronic searches
We identified relevant studies from the Cochrane Cystic Fibrosis and Genetic Disorders Group's Cystic Fibrosis Trials Register using the terms: 'drugs that correct defects in CFTR transcription, translation or processing'. Relevant studies have been tagged with these terms for indexing purposes in the Group's Cystic Fibrosis Trials Register.
The Cystic Fibrosis Trials Register is compiled from electronic searches of the Cochrane Central Register of Controlled Trials (CENTRAL) (updated each new issue of the Cochrane Library), weekly searches of MEDLINE, a search of Embase to 1995 and the handsearching of two journals ‐ Pediatric Pulmonology and the Journal of Cystic Fibrosis. Unpublished work was identified by searching the abstract books of three major cystic fibrosis conferences: the International Cystic Fibrosis Conference; the European Cystic Fibrosis Conference and the North American Cystic Fibrosis Conference. For full details of all searching activities for the register, please see the relevant sections of the Cystic Fibrosis and Genetic Disorders Group website.
Date of the most recent search: 14 October 2020.
We also searched the following trial registries and registers:
US National Institutes of Health Ongoing Trials Register Clinicaltrials.gov (www.clinicaltrials.gov; searched 23 November 2020);
World Health Organization International Clinical Trials Registry Platform (WHO ICTRP) (apps.who.int/trialsearch; searched 23 November 2020);
European Medicines Agency (www.clinicaltrialsregister.eu/ctr-search/search; searched 23 November 2020).
For details of our search strategies, please see Appendix 1.
Searching other resources
We screened the bibliographies of included studies and any relevant systematic reviews identified for further references to potentially relevant studies. We also contacted authors of included studies, leaders in the field, and companies known to be developing and investigating CFTR correctors, to identify any studies which may have been missed by this search. We recorded response rates from this contact process below (Results of the search).
Data collection and analysis
Selection of studies
Two authors (JM and IS or IS and SP or IS and KWS) independently assessed the suitability of each potential study identified by the search. If disagreement arose on the suitability of a study for inclusion in the review, we attempted to reach a consensus by discussion, failing which, a third author arbitrated.
Data extraction and management
Two authors (JM and IS or IS and SP or IS and SJN) independently extracted relevant data from each included study. If disagreement arose on data extraction, we attempted to reach a consensus by discussion, failing which, a third author (KWS) arbitrated. Three authors (JM, SP and SN) entered the data into RevMan for analysis.
If studies had reported data on our primary outcome (survival), we planned to report these as a binary outcome or a time‐to‐event outcome. We planned on extracting QoL scores as relative change from baseline ((measurement at end of treatment ‐ measurement at baseline) / measurement at baseline) x 100). We extracted data presented as post‐treatment values or change from baseline when this was not possible.
With regards to the secondary outcome 'Extra courses of antibiotics', we planned to extract data as time‐to‐the‐next course of antibiotics and the total number of courses of antibiotics. We noted whether episodes of pulmonary exacerbations were physician‐defined or protocol‐defined. If studies reported baseline and post‐treatment sweat chloride concentration values, we calculated the relative change from baseline values ((measurement at end of treatment ‐ measurement at baseline) / measurement at baseline) x 100).
We reported data as immediate (up to and including one month), short‐term (over one month and up to six months) and longer‐term (over six months). The exception to this is one study which presents data for lumacaftor monotherapy for 14 days and then adds ivacaftor for the final seven days of the study; in this case we present data at 14 and 21 days (Boyle 2014). If a study we include in future updates of the review reports multiple time points within each of these ranges, we will report the later time point.
We attempted to extract the most precise data as possible for each outcome; extraction of tabulated data was preferred. If data were presented only graphically, three authors (JM, SP and SJN) estimated the relevant data from graphs and compared estimations for accuracy.
We have not combined data from studies evaluating distinct agents or combination of agents, as they have different mechanisms of actions. Also, where RCTs have recruited pwCF with different genotypes and presented these results separately, we have analysed the data by genotype.
Assessment of risk of bias in included studies
Two authors (JM and IS or IS and SP or IS and SJN) assessed the risk of bias for each study using the Cochrane risk of bias tool (Higgins 2011a). This includes assessment of the following methodological aspects of the included studies:
procedure for randomisation (selection bias);
allocation concealment (selection bias);
masking (blinding) of the intervention from participants, clinicians, and trial personnel evaluating outcomes (performance bias);
missing outcome data (attrition bias);
selective outcome reporting (reporting bias);
other sources of bias (e.g. the influence of funding sources or industry on trial characteristics and presented results).
We also assessed whether all participants were included in an intention‐to‐treat analysis, regardless of whether they completed the treatment schedule or not. If disagreement arose on the assessment of risk of bias of a study, we attempted to reach a consensus by discussion, failing which, a third author (KWS) arbitrated.
Measures of treatment effect
For binary outcomes, we calculated a pooled estimate of the treatment effect for each outcome using the pooled odds ratio (OR) and 95% confidence intervals (CIs) or 99% CIs for analysis of separate adverse events.
For continuous outcomes, we calculated the mean change from baseline for each group or the mean post‐intervention values and standard deviation (SD) for each group. We converted standard errors (SEs) to SDs. We produced a pooled estimate of treatment effect by calculating the mean difference (MD) and 95% CIs.
In future updates of this review, if different trials present data for the same outcomes in different forms (e.g. absolute values of lung function measures, or change in these measures from a baseline), we will combine these in a meta‐analysis where appropriate.
Where the studies did not report change data, but instead presented absolute post‐treatment data without baseline data (so it was not possible to calculate change data) we planned to use absolute post‐treatment data instead of change from baseline. However, if the report presented baseline and post‐treatment data for any outcome, we calculated SDs for the change from baseline, for example if the CI was available. If there was not enough information available to calculate the SDs for the changes, we planned to impute them from other trials in the review, where data were available and trials were similar (i.e. when they used the same measurement scale, had the same degree of measurement error and had the same time periods between baseline and final value measurement). If neither of these methods were possible, we planned to calculate a change‐from‐baseline SD, making use of an imputed correlation coefficient (methods described in section 16.1.3.2 in the Cochrane Handbook of Systematic Reviews of Interventions (Higgins 2011b)).
Where time‐to‐event data were reported (e.g. survival time, time to next hospitalisation, time to first exacerbation), we reported a hazard ratio (HR) and 95% CIs. Where HRs and 95% CIs were not reported for a time‐to‐event outcome, we assessed whether any reported data, including graphical data (e.g. Kaplan‐Meier curves) could be used to indirectly estimate HRs and 95% CIs via the published methods (Parmar 1998; Williamson 2002).
When reporting on outcomes we used the following subheadings to describe the time points: immediate (up to and including ); short term (over one month and up to six months); and longer term (over six months).
Unit of analysis issues
We included results from RCTs of parallel design in which individual study participants are randomised. We have not included cross‐over studies as we do not feel this study design is appropriate given that the intervention aims to correct the underlying defect. If the intervention is effective it will have an important impact on the course of the disease. This has been established from the data from trials examining ivacaftor for people with class III mutations (Skilton 2019).
In one included study, continuous outcomes were analysed via a mixed model repeated measures analysis (MMRM) based on the average effect across the measured time points (Ratjen 2017). Such an analysis is longitudinal and uses all available data at every visit and allows adjustment for covariates such as the baseline measurement of the outcome. All analyses were also adjusted for baseline weight (less than 25 kg versus 25 kg or over) and baseline FEV1 (% predicted ‐ less than 90% versus 90% or above). Results provided by this model can be interpreted as treatment effect averaged from each study visit until week 24. Within this review, results are entered into the analysis via generic inverse variance and are not pooled with other studies, due to the different approaches to analysis.
For the studies of triple therapies we included combinations with VX‐561 (deuterated ivacaftor), as we considered it to be a sufficiently similar intervention to standard ivacaftor. We pooled the data for those participants with F508del/MF genotypes as these pwCF were in the groups which tested the ascending doses and VX‐561. Only one dose was tested in pwCF with the F508del/F508del genotype and VX‐561 was not tested in this group. Pooling data from studies of differing genotypes (participants with one or two class II variants) was not considered appropriate.
Dealing with missing data
In order to allow an intention‐to‐treat analysis, we extracted data on the number of participants with each outcome event, by allocated treated group, irrespective of compliance and whether or not the participant was later thought to be ineligible or otherwise excluded from treatment or follow‐up. If any data were missing or unclear, we contacted the primary investigators for clarification.
As stated above, where HRs and 95% CIs were not reported for a time‐to‐event outcome, we assessed whether any reported data, including graphical data (e.g. Kaplan‐Meier curves) could be used to indirectly estimate HRs and 95% CIs via the published methods (Parmar 1998; Williamson 2002).
Assessment of heterogeneity
We assessed heterogeneity through visual examination of the combined data presented in the forest plots, and by considering overlap of study‐specific CIs, and the I² statistic (Higgins 2003) together with Chi² values (Deeks 2011). The I² statistic reflects the likelihood that variation of results across studies are due to heterogeneity rather than by chance, and we interpreted this statistic using the following simple classification:
0% to 40%: might not be important;
30% to 60%: may represent moderate heterogeneity;
50% to 90%: may represent substantial heterogeneity;
75% to 100%: considerable heterogeneity.
Assessment of reporting biases
In order to identify selective outcome reporting, where possible, we have compared outcomes described in the study protocol with those reported in the publication. We have requested protocols for specific studies from the primary investigators and recorded the proportion of protocols that were available to us. If a protocol was not available, we searched for information about outcomes from trial registry databases. We also compared outcomes listed in the 'Methods' section of the final paper with those presented in the 'Results' section. If the published papers reported negative findings either only partially, or not at all, we contacted primary investigators for these data.
We would have assessed publication bias by constructing and assessing the symmetry of a funnel plot. This would have been possible if we included more than 10 studies in a meta‐analysis in the review. We would have plotted the number of participants in the study against a measure of treatment effect. If the funnel plot was asymmetrical, we would consider whether this was due to publication bias, or whether methodology or small sample size caused results of certain studies to show exaggerated treatment effects.
Data synthesis
As we intended to assess different CFTR correctors within this review, we assumed that there would not be a single common true effect. We also anticipated participants in each study would vary due to different eligibility criteria. Therefore, regardless of I² value, we intended to use a random‐effects model to analyse data from studies.
As the review progressed, we included a number of early‐phase studies of interventions (which were ultimately not taken forward) in addition to large Phase 3 studies of combination therapies; therefore, we felt it more appropriate to employ separate comparisons within the review. As only a relatively small number of studies were included in each comparison (and when meta‐analysis was undertaken), it was considered more appropriate to employ a fixed‐effect model.
Subgroup analysis and investigation of heterogeneity
We would have investigated any heterogeneity that we identified using subgroup analyses of potential confounding factors, if sufficient numbers (at least 10 studies included in a meta‐analysis) were available. For this review, these confounding factors would be:
age (children (defined as younger than 18 years of age) versus adults);
gender;
different variant classes (Table 9);
As we did not seek individual patient data from study investigators and such information was not available within published reports, we did not undertake a subgroup analysis on the basis of disease severity. We may incorporate such an analysis in future updates of this review.
Sensitivity analysis
In future updates of this review, if sufficient data are available, we will examine the impact of bias on the results by comparing meta‐analyses including and excluding studies with concerns of high risk of selection or reporting bias due to issues relating to randomisation, allocation concealment, or masking of interventions from participants or study personnel.
Summary of findings and assessment of the certainty of the evidence
In a post hoc change from protocol, we have presented eight summary of findings tables (Table 1; Table 2; Table 3; Table 4; Table 5; Table 6; Table 7; Table 8).
Summary of findings 1. Summary of findings ‐ monotherapy: lumacaftor compared to placebo for cystic fibrosis.
| Lumacaftor compared with placebo for cystic fibrosis | ||||||
|
Patient or population: adults and children with cystic fibrosis Settings: outpatients Intervention: lumacaftor Comparison: placebo | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Placebo | Lumacaftor | |||||
|
Survival Follow‐up: 14 to 28 days |
No deaths reported. | No deaths reported. | NA | 147 (2 studies) |
⊕⊕⊝⊝ lowa | |
|
Quality of life ‐ total score Follow‐up: 14 to 28 days |
Outcome not reported. | NA | A higher score indicates a better outcome. | |||
|
Quality of life ‐ CFQ‐R respiratory domain: absolute change from baseline Follow‐up: 14 to 28 days |
There was a significant decrease in the CFQ‐R respiratory domain in the 50 mg lumacaftor group compared to placebo. No differences were found in the other dose groups (25 mg, 100 mg, 200 mg) compared to placebo. | NA | 85 (1 study) |
⊕⊕⊝⊝ lowa | A higher score indicates a better outcome. | |
|
FEV1 % predicted: relative change from baseline Follow‐up: 14 to 28 days |
Outcome not reported. | NA | ||||
|
FEV1 % predicted: absolute change from baseline Follow‐up: 14 to 28 days |
The mean change from baseline was 1.7% predicted. | The mean change from baseline was 1.90% predicted lower (4.13 lower to 0.33 higher). | NA | 61 (1 study) |
⊕⊕⊕⊝ moderateb | |
|
Adverse events Follow‐up: 14 to 28 days |
There were no significant differences between groups in terms of participants experiencing any specific adverse event. In 1 of the studies, 1 participant from each of the lumacaftor arms ‐ 1 participant in each of the discontinued the study drug due to respiratory adverse effects. No participants discontinued from the placebo group. |
NA | 115 (2 studies) |
⊕⊝⊝⊝ very lowa,b,c | ||
|
Time to first pulmonary exacerbation Follow‐up: 14 to 28 days |
Outcome not reported (see comment). | NA | Time to first pulmonary exacerbation was not reported. There was no significant difference between groups in the number of participants experiencing pulmonary exacerbations. | |||
| *The basis for the assumed risk is the mean placebo group risk across studies. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CFQ‐R: Cystic Fibrosis Questionnaire‐Revised; CI: confidence interval, EQ‐5D‐3L: 5‐Dimension‐3 Level, FEV1: forced expiratory volume at one second; MD: mean difference. | ||||||
| GRADE Working Group grades of evidence High quality: further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: we are very uncertain about the estimate. | ||||||
a Downgraded twice due to risk of bias: in one study, data were selectively reported and often presentation of data did not allow for inclusion in analysis. There are also incomplete outcome data in the study with participants unaccounted for in analysis.
b Downgraded once due to indirectness: design of the study means that monotherapy treatment was measured for only 14 days before a combination therapy phase was started.
c Downgraded once due to imprecision: few events occurred therefore CIs for occurrence of specific events are very wide.
Summary of findings 2. Summary of findings ‐ monotherapy: cavosonstat compared to placebo for cystic fibrosis.
| Cavosonstat compared with placebo for cystic fibrosis | ||||||
|
Patient or population: adults and children with cystic fibrosis Settings: outpatients Intervention: cavosonstat 200 mg Comparison: placebo | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Placebo | Cavosonstat | |||||
|
Survival Follow‐up: 28 days |
No deaths reported. | No deaths reported. | NA | 26 (1 study) |
⊕⊝⊝⊝ very lowa,b,c | |
|
Quality of life: total score Follow‐up: NA |
Outcome not reported. | NA | A higher score indicates a better outcome. | |||
|
Quality of life: CFQ‐R respiratory domain: absolute change from baseline Follow‐up: 28 days |
The mean absolute change from baseline in CFQ‐R respiratory domain was ‐4.6 points in the placebo group. | The mean absolute change from baseline in CFQ‐R respiratory domain was 3.80 higher (11.30 lower to 18.90 higher) in the Cavosonstat group than the placebo group. | NA | 26 (1 study) |
⊕⊝⊝⊝ very lowa,b,c,d | A higher score indicates a better outcome. |
|
FEV1 % predicted: relative change from baseline Follow‐up: NA |
Outcome not reported. | NA | ||||
|
FEV1 % predicted: absolute change from baseline Follow‐up: 28 days |
There were no treatment‐related changes in FEV1 (% predicted) compared to placebo. | NA | 26 (1 study) |
⊕⊝⊝⊝ very lowa,b,c | A graphical figure of change from baseline in FEV1 (% predicted) is provided but numerical data cannot be extracted to include in analysis due to overlapping lines. | |
|
Adverse events: occurring in at least 10% of cavosonstat treated participants Follow‐up: 28 days |
There was no significant difference between groups in terms of cough, pulmonary exacerbation, chest discomfort and fatigue. | NA | 26 (1 study) |
⊕⊝⊝⊝ very lowa,b,c,e | ||
|
Time to first pulmonary exacerbation Follow‐up: NA |
Outcome not reported. | NA | ||||
| *The basis for the assumed risk is the control group risk across studies. The corresponding risk (and its 95% CIl) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CFQ‐R: Cystic Fibrosis Questionnaire‐Revised; CI: confidence interval; FEV1: forced expiratory volume in 1 second; NA: not applicable. | ||||||
| GRADE Working Group grades of evidence High quality: further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: we are very uncertain about the estimate. | ||||||
a Downgraded once due to potential risk of bias: unclear details related to methodological design and some unbalanced baseline characteristics.
b Downgraded once due to indirectness: adults only were recruited into the study, therefore, results are not applicable to children.
c Downgraded once due to imprecision: a single study with a small sample size.
d Downgraded once due to imprecision: wide CIs around the result.
e Downgraded once due to imprecision: very wide CIs around results (due to small event numbers).
Summary of findings 3. Summary of findings ‐ dual therapy: lumacaftor plus ivacaftor (once daily) compared with placebo for cystic fibrosis (short term).
| Lumacaftor plus ivacaftor compared with placebo for cystic fibrosis | ||||||
|
Patient or population: adults and children with cystic fibrosis Settings: outpatients Intervention: lumacaftor (600 mg once daily or 400 mg once daily) plus ivacaftor (250 mg twice daily) Comparison: placebo | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Placebo | Lumacaftor plus ivacaftor | |||||
|
Survival Follow‐up: 6 months |
No deaths reported. | No deaths reported. | NA | 1108 (2 studies) |
⊕⊕⊕⊕ high | |
|
Quality of life ‐ (EuroQol) EQ‐5D‐3L Index Score (total score): absolute change from baseline Follow‐up: 6 months |
The mean absolute change from baseline ranged from 0.0006 to 0.0017 points. | The mean absolute change from baseline was 0.00 points higher (0.01 lower to 0.01 higher). | NA | 1061 (2 studies) |
⊕⊕⊕⊝ moderatea | A higher score indicates a better outcome. |
|
Quality of life ‐ CFQ‐R respiratory domain: absolute change from baseline Follow‐up: 6 months |
The mean absolute change from baseline ranged from 1.1 to 2.81 points. | The mean absolute change from baseline was 2.62 points higher (0.64 higher to 4.59). | NA | 1076 (2 studies) |
⊕⊕⊕⊝ moderatea | A higher score indicates a better outcome. There was also a significant difference between groups at 28 days, MD 3.70 points (95% CI 1.81 to 5.58). |
|
FEV1 % predicted: relative change from baseline Follow‐up: 6 months |
The mean relative change from baseline ranged from ‐0.34% to 0%. | The mean relative change from baseline was 5.21% higher (3.61% higher to 6.80% higher). | NA | 1072 (2 studies) |
⊕⊕⊕⊕ high | |
|
FEV1 % predicted: absolute change from baseline Follow‐up: 6 months |
The mean absolute change from baseline ranged from ‐0.44 to ‐0.15% predicted. | The mean absolute change from baseline was 3.07% predicted higher (2.17 higher to 3.97 higher). | NA | 1072 (2 studies) |
⊕⊕⊕⊝ moderatea | There was also a significant difference between groups at 28 days, MD 2.37% predicted (95% CI 1.52 to 3.22). |
|
Adverse events Follow‐up: 6 months |
Cough was significantly more common in the placebo group compared to the lumacaftor‐ivacaftor group. Dyspnoea was significantly more common in the lumacaftor‐ivacaftor group compared to the placebo group. There were no significant differences between groups in terms of number of participants experiencing adverse events, serious adverse events or other adverse events. Long‐term open‐label follow‐up data of the 2 studies showed a significant increase in early transient shortness of breath. In participants allocated a 400 mg twice‐daily dose, there was a significant rise in blood pressure. |
NA | 1108 (2 studies) |
⊕⊕⊕⊕ high | ||
|
Time to first pulmonary exacerbation Follow‐up: 6 months |
Time to first pulmonary exacerbation was significantly longer in both in the lumacaftor 600 mg once daily plus ivacaftor 250 mg twice daily and the lumacaftor 400 mg twice daily plus ivacaftor 250 mg twice daily groups | NA | 1108 (2 studies) |
⊕⊕⊕⊝ moderatea | Presentation of data did not allow an analysis of the lumacaftor doses pooled. | |
| *The basis for the assumed risk is the mean placebo group risk across studies. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CFQ‐R: Cystic Fibrosis Questionnaire‐Revised; CI: confidence interval; EQ‐5D‐3L: 5‐Dimension‐3 Level; EuroQol: Euro Quality of Life Scale; FEV1: forced expiratory volume at one second; MD: mean difference. | ||||||
| GRADE Working Group grades of evidence High quality: further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: we are very uncertain about the estimate. | ||||||
a Downgraded once due to risk of bias from selective reporting: data contributing to analyses were extrapolated from published graphs or estimated. We have requested confirmation of the exact data from the study investigators. Any unpublished information we receive will be included in a future update and this judgement will be reconsidered.
Summary of findings 4. Summary of findings ‐ dual therapy: lumacaftor plus ivacaftor (twice daily) compared with placebo for cystic fibrosis (short term).
| Lumacaftor plus ivacaftor compared with placebo for cystic fibrosis | ||||||
|
Patient or population: adults and children with cystic fibrosis Settings: outpatients Intervention: lumacaftor (200 mg twice daily) plus ivacaftor (250 mg twice daily) Comparison: placebo | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
|
Survival Follow‐up: 24 weeks |
No deaths reported. | No deaths reported. | NA | 204 (1 study) | ⊕⊕⊕⊝ moderatea | |
|
Quality of life ‐ total score Follow‐up: 24 weeks |
Outcome not reported. | NA | A higher score indicates a better outcome. | |||
|
Quality of life ‐ CFQ‐R respiratory domain: absolute change from baseline Follow‐up: 24 weeks |
See comment. | The mean change in the CFQ‐R respiratory domain was 2.50 points higher in the lumacaftor‐ivacaftor group compared to the placebo group, ranging from 0.10 lower to 5.10 higher. | NA | 204 (1 study) | ⊕⊕⊝⊝ lowa,b | A higher score indicates a better outcome. Data were analysed via a MMRM. Results provided by this model can be interpreted as treatment effect averaged from each study visit until week 24. |
|
FEV1 % predicted: relative change from baseline Follow‐up: 24 weeks |
Outcome not reported. | NA | Relative change from baseline in FEV1 was listed in the methods of the study but no numerical results were presented. if numerical data becomes available at a later date, it will be included in an update of this review. |
|||
|
FEV1 % predicted: absolute change from baseline Follow‐up: 24 weeks |
See comment. | The mean change in FEV1 % predicted was 2.40 higher in the lumacaftor‐ivacaftor group compared to the placebo group, ranging from 0.40 higher to 4.40 higher. | NA | 204 (1 study) | ⊕⊕⊝⊝ lowa,b | Data were analysed via a MMRM. Results provided by this model can be interpreted as treatment effect averaged from each study visit until week 24. |
|
Adverse events Follow‐up: 24 weeks |
There was no significant difference between the groups in terms of productive cough, nasal congestion, oropharyngeal pain, upper abdominal pain, rhinorrhoea, increased sputum, cough, pyrexia, headache, upper respiratory tract infection, abdominal pain, nausea, vomiting, fatigue and respiratory events (such as wheezing, dyspnoea, asthma and chest discomfort). | NA | 204 (1 study) | ⊕⊕⊝⊝ lowb,c | ||
|
Time to first pulmonary exacerbation Follow‐up: 24 weeks |
Outcome not reported. | NA | Time to first pulmonary exacerbation was listed in the methods of the study but no numerical results were presented. If numerical data become available at a later date, they will be included in an update of this review. |
|||
| *The basis for the assumed risk is the control group risk across studies. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CFQ‐R: Cystic Fibrosis Questionnaire‐Revised; CI: confidence interval; FEV1: forced expiratory volume at 1 second; MMRM: mixed model for repeated measures; NA: not applicable. | ||||||
| GRADE Working Group grades of evidence High quality: further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: we are very uncertain about the estimate. | ||||||
a Downgraded once due to indirectness: children aged 6 ‐ 11 years were recruited in this study, therefore, results are not applicable to other age groups.
b Downgraded once due to risk of bias from selective reporting: limited data available which is adjusted for all visits. Further graphical data were available in the publication but could not be accurately extracted. We have requested confirmation of the exact data from the study investigators. Any unpublished information we receive will be included in a future update and this judgement will be reconsidered
c Downgraded once due to imprecision; few events occurred therefore CIs for occurrence of specific events are very wide.
Summary of findings 5. Summary of findings ‐ dual therapy: lumacaftor plus ivacaftor compared with placebo for cystic fibrosis (immediate term).
| Lumacaftor plus ivacaftor compared with placebo for cystic fibrosis | ||||||
|
Patient or population: adults and children with cystic fibrosis Settings: outpatients Intervention: lumacaftor (200 mg) plus ivacaftor (150 mg or 250 mg twice daily)a Comparison: placebo | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Placebo | Lumacaftor plus ivacaftora | |||||
|
Survival Follow‐up: 21 days1 |
No deaths reported. | No deaths reported. | NA | 62 (1 study) |
⊕⊕⊕⊝ moderateb | |
|
Quality of life: total score Follow‐up: 21 days1 |
Outcome not reported. | NA | A higher score indicates a better outcome. | |||
|
Quality of life: respiratory domain Follow‐up: 21 days1 |
Outcome not reported. | NA | A higher score indicates a better outcome. | |||
|
FEV1 % predicted: relative change from baseline Follow‐up: 21 days1 |
Outcome not reported. | NA | ||||
|
FEV1 % predicted: absolute change from baseline Follow‐up: 21 days1 |
The mean change from baseline was 0.3. | The mean change from baseline was 1.57% predicted higher (‐2.13 lower to 5.27 higher). | NA | 59 (1 study) |
⊕⊕⊕⊝ moderateb | |
|
Adverse events Follow‐up: 21 days1 |
There were no significant differences between groups in terms of participants experiencing: cough, oropharyngeal pain, nasal congestion, dizziness, a prolonged prothrombin time, and upper respiratory tract infection. | NA | 61 (1 study) |
⊕⊕⊝⊝ lowb,c | ||
|
Time to first pulmonary exacerbation Follow‐up: 21 days 1 |
Outcome not reported (see comment). | NA | Time to first pulmonary exacerbation was not reported. There was no significant difference between groups in the number of participants experiencing pulmonary exacerbations. | |||
| *The basis for the assumed risk is the mean placebo group risk across studies. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; FEV1: forced expiratory volume at 1 second. | ||||||
| GRADE Working Group grades of evidence High quality: further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: we are very uncertain about the estimate. | ||||||
a The design of the study was 14 days of lumacaftor monotherapy (200 mg once daily) then a dose of ivacaftor (150 mg or 250 mg once daily) was added on for 7 days of combination therapy. Results presented in this table are from the combination treatment period only.
b Downgraded once due to indirectness: design of the study means that combination treatment was measured for only 7 days and prior lumacaftor monotherapy phase (see footnote 1) may have influenced results of the combination phase.
c Downgraded once due to imprecision: few events occurred therefore CIs for occurrence of specific events are very wide.
Summary of findings 6. Summary of findings ‐ dual therapy: tezacaftor plus ivacaftor compared with placebo or ivacaftor alone for cystic fibrosis.
| Tezacaftor plus ivacaftor compared with placebo or ivacaftor alone for cystic fibrosis | ||||||
|
Patient or population: adults and children with cystic fibrosis Settings: outpatients Intervention: tezacaftor (100 mg daily) plus ivacaftor (150 mg twice daily) Comparison: placebo (i.e. tezacaftor placebo) or ivacaftor (150 mg twice daily) | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Placebo or ivacaftor alone | Tezacaftor plus ivacaftor | |||||
|
Survival Follow‐up: up to 24 weeks |
No deaths reported. | No deaths reported. | NA | 522 (2 studies) | ⊕⊕⊕⊝ moderatea,b | |
|
Quality of life: total score Follow‐up: NA |
Outcome not reported. | NA | A higher score indicates a better outcome. | |||
|
Quality of life: CFQ‐R respiratory domain: absolute change from baseline Follow‐up: up to 24 weeks |
See comment. | The mean absolute change from baseline in CFQ‐R respiratory domain score in the tezacaftor‐ivacaftor group was 5.10 points higher (3.20 higher to 7.00 higher) than the placebo group (result from 1 study with 510 individuals). | NA | 522 (2 studies) | ⊕⊕⊕⊝ moderatea,b | A higher score indicates a better outcome Difference in absolute change from baseline calculated by least‐squares regression, hence assumed risk not presented. The mean absolute change from baseline in CFQ‐R respiratory domain score in the tezacaftor plus ivacaftor group was also significantly higher than the placebo group at 4 weeks: MD 5.10 (95% CI 2.99 to 7.21) The second study (n = 18) showed that the treatment effect of tezacaftor‐ivacaftor versus placebo was 6.81 points of CFQ‐R respiratory domain (P = 0.2451) up to day 28. |
|
FEV1 % predicted: relative change from baseline Follow‐up: up to 24 weeks |
See comment. | The mean relative change from baseline in FEV1 % predicted in the tezacaftor‐ivacaftor group was 6.80% higher (5.30% higher to 8.30% higher) than the placebo group (result from 1 study with 510 individuals). | NA | 522 (2 studies) | ⊕⊕⊕⊝ moderatea,b | Difference in relative change from baseline calculated by least‐squares regression, hence assumed risk not presented. The second study (n = 18) showed no significant difference between groups in mean relative change from baseline in FEV1 % predicted MD 3.72 (95% CI ‐7.77 to 15.21). |
|
FEV1 % predicted: absolute change from baseline Follow‐up: up to 24 weeks |
See comment | The mean absolute change from baseline in FEV1 % predicted in the tezacaftor plus ivacaftor group was 4.00 % predicted higher (3.10 higher to 4.90 higher) than the placebo group (result from one study with 510 individuals). | NA | 522 (2 studies) | ⊕⊕⊕⊝ moderatea,b | Difference in absolute change from baseline calculated by least‐squares regression, hence assumed risk not presented. The mean absolute change from baseline in FEV1 % predicted in the tezacaftor‐ivacaftor group was also significantly higher than the placebo group at 4 weeks, MD 3.59 (95% CI 2.40 to 4.78), 2 studies, n = 528, I² =0%. |
|
Adverse events: most commonly occurring events (occurring in at least 10% of participants) Follow‐up: up to 24 weeks |
The most commonly occurring adverse events in both groups were cough and pulmonary exacerbation. There were no significant differences between groups (99% confidence intervals) in the number of participants experiencing cough, pulmonary exacerbation, headache, nasal congestion or nasopharyngitis, increased sputum, haemoptysis, pyrexia, oropharyngeal pain, nausea or fatigue. |
NA | 527 (2 studies) | ⊕⊕⊕⊝ moderatea,b | ||
|
Time to first pulmonary exacerbation Follow‐up: up to 24 weeks |
The hazard ratio for pulmonary exacerbation in the tezacaftor plus–ivacaftor group, as compared with the placebo group was 0.64 (95% CI 0.46 to 0.89). | NA | 504 (1 study) |
⊕⊕⊕⊝ moderatea,b | A hazard ratio below 1 favours the tezacaftor‐ivacaftor group. | |
| *The basis for the assumed risk is the control group risk across studies. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; FEV1: forced expiratory volume at 1 second; MD: mean difference; NA: not applicable. | ||||||
| GRADE Working Group grades of evidence High quality: further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: we are very uncertain about the estimate. | ||||||
a Downgraded once due to indirectness: 1 study recruited individuals over the age of 12 (Taylor‐Cousar 2017) and 1 study recruited individuals over the age of 18 with one F508del mutation and one G551D mutation (Donaldson 2018). Therefore, results are not applicable to children under the age of 12 and some results are not applicable to individuals homozygous for F508del.
b One study has some unclear details related to methodological design and had unbalanced treatment group sizes and baseline characteristics (Donaldson 2018). However, this study contributed a small proportion of the evidence of this comparison (n = 18, 3% of evidence) compared to the second study in the comparison (n = 509, 97% of evidence, overall low risk of bias) (Taylor‐Cousar 2017). Therefore, no downgrading is made due to potential risks of bias in the smaller study.
Summary of findings 7. Summary of findings ‐ triple therapy: VX‐659‐tezacaftor‐ivacaftor/VX‐561 compared to control for cystic fibrosis.
| VX‐659 plus tezacaftor plus ivacaftor or VX‐561 compared with control for cystic fibrosis | ||||||
|
Patient or population: adults with cystic fibrosis and either F508del/MF or F508del/F508del genotype Settings: outpatients Intervention: VX‐659 (80 mg once daily, 120 mg twice daily, 240 mg once daily or 400 mg once daily) plus tezacaftor 100 mg once per day plus ivacaftor 150 mg twice daily or VX‐561 150 mg once daily Comparison: F508del/MF participants: triple placebo; F508del/F508del participants: placebo tezacaftor 100 mg once daily plus ivacaftor 150 mg twice daily | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Triple placebo or placebo‐tezacaftor‐ivacaftor | VX‐659 plus tezacaftor plus ivacaftor or VX‐561 | |||||
|
Survival Follow‐up: 2 to 4 weeks |
No deaths reported. | No deaths reported. | NA | 129 (2 studies) | ⊕⊕⊕⊕ high | |
|
Quality of life: total score Follow‐up: NA |
Outcome not reported. | NA | ||||
|
Quality of life: CFQ‐R respiratory domain: absolute change from baseline Follow‐up: up to 4 weeks |
See comment. | A significant improvement was seen in the VX‐659 plus tezacaftor plus ivacaftor 80 mg group, MD 10.00 (95% CI 0.29 to 19.71) (F508del/MF genotype); in the VX‐659 plus tezacaftor plus ivacaftor 400 mg group, MD 18.10 (95% CI 10.85 to 25.35) (F508del/F508del genotype); and in the VX‐561 group, MD 20.30 (95% CI 70.5 to 33.55) (F508del/MF genotype) compared to the controls. No such differences were seen in the other dose groups. |
NA | 129 (2 studies) | ⊕⊕⊕⊝ moderatea | A higher score indicates a better outcome. Data were analysed via a MMRM, hence assumed risk not presented. Results provided by this model can be interpreted as treatment effect averaged from week 2 and week 4. |
|
FEV1 (% predicted): relative change from baseline Follow‐up: up to 4 weeks |
See comment. | Significant improvements were seen in the relative change from baseline in FEV1 % predicted across all dose levels and genotypes when compared to placebo. | NA | 117 (1 study) | ⊕⊕⊕⊝ moderatea | Data were analysed via a MMRM, hence assumed risk not presented. Results provided by this model can be interpreted as treatment effect averaged from week 2 and week 4. |
|
FEV1 (% predicted): absolute change from baseline Follow‐up: 2 weeks |
One study found a significant improvement in the absolute change from baseline in FEV1 % predicted at the dose of 120 mg twice daily versus placebo, MD 10.00 % predicted (95% CI 3.04 to 16.96). | NA | 12 (1 study) | ⊕⊕⊕⊝ moderatea | A second study (n = 117) found a significant improvement in the absolute change in FEV1 (L) at all dose levels and genotypes for the interventions compared to control. | |
|
Adverse events Follow‐up: 2 to 4 weeks |
There was no significant difference in the number of participants experiencing at least 1 adverse event between the intervention and placebo groups at any dose or for any genotype. There was also no statistical difference versus placebo relating to the severity of adverse events across all doses and genotype groups. | NA | 129 (2 studies) | ⊕⊕⊕⊝ moderatea | ||
| Time to first pulmonary exacerbation | Outcome not reported. | NA | 1 study (n = 117) did report that there was no difference in the number of courses of antibiotics required or the number of pulmonary exacerbations between groups at all dose levels and genotypes for the interventions compared to control. | |||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CFQ‐R: Cystic Fibrosis Questionnaire‐Revised; CI: confidence interval; FEV1: forced expiratory volume at 1 second; MD: mean difference; MF: minimal function; MMRM: mixed model for repeated measures; NA: not applicable. | ||||||
| GRADE Working Group grades of evidence High quality: further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: we are very uncertain about the estimate. | ||||||
a Downgraded once due to indirectness or lack of applicability: data do not include children under the age of 12 and those with more severe disease. Also short‐term data only.
Summary of findings 8. Summary of findings ‐ triple therapy: elexacaftor‐tezacaftor‐ivacaftor/VX‐561 compared to control for cystic fibrosis.
| Elexacaftor plus tezacaftor plus ivacaftor or VX‐561 compared with placebo for cystic fibrosis | ||||||
|
Patient or population: adults with cystic fibrosis and either F508del/MF or F508del/F508del genotype Settings: outpatients Intervention: elexacaftor (50 mg once daily, 100 mg once daily or 200 mg once daily) plus tezacaftor 100 mg once daily plus ivacaftor 150 mg twice daily or VX‐561 150 mg once daily Comparison: F508del/MF participants: triple placebo; F508del/F508del participants: placebo tezacaftor 100 mg once daily plus ivacaftor 150 mg twice daily | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Triple placebo or placebo tezacaftor plus ivacaftor | Elexacaftor plus tezacaftor plus ivacaftor or VX‐561 | |||||
|
Survival Follow‐up: 4 weeks to 24 weeks |
No deaths reported. | No deaths reported. | NA | 603 (3 studies) | ⊕⊕⊕⊕ high | |
|
Quality of life: total score Follow‐up: NA |
Outcome not reported. | NA | ||||
|
Quality of life: CFQ‐R respiratory domain absolute change from baseline Follow‐up: 4 weeks to 24 weeks |
A significant improvement in the elexacaftor plus tezacaftor plus ivacaftor or VX‐561 groups in the CFQ‐R respiratory domain was observed compared to control versus placebo across all dose levels and both genotypes | NA | 599 (3 studies) | ⊕⊕⊕⊝ moderatea | A higher score indicates a better outcome. | |
|
FEV1 (% predicted): relative change from baseline Follow‐up: 4 weeks to 24 weeks |
A significant improvement in the relative change from baseline in FEV1 % predicted in the elexacaftor plus tezacaftor plus ivacaftor groups was observed across all dose levels and genotypes when compared to control groups . | NA | 603 (3 studies) | ⊕⊕⊕⊝ moderatea | ||
|
FEV1 (% predicted): absolute change from baseline Follow‐up: NA |
A significant improvement in the absolute change from baseline in FEV1 % predicted in the elexacaftor plus tezacaftor plus ivacaftor groups compared to control groups was observed in 2 studies including participants with F508del/MF genotype and F508del/F508del genotype. | NA | 510 (2 studies) | NA | 1 study (n = 123) reported a significant improvement in the absolute change from baseline in FEV1 (L) favouring the intervention across all dose levels and genotypes for the interventions compared to control. | |
|
Adverse events Follow‐up: 4 weeks to 24 weeks |
There was no significant difference in the number of participants experiencing at least 1 adverse event between the intervention and placebo groups at any dose or for any genotype. There was also no statistical difference versus placebo relating to the severity of adverse events across all doses and genotype groups. | NA | 603 (3 studies) | ⊕⊕⊕⊝ moderatea | ||
|
Time to first pulmonary exacerbation Follow‐up: 24 weeks |
A longer time to pulmonary exacerbation (protocol‐defined) was seen in participants in the intervention group compared to participants in the placebo group (F508del/MF genotype). | NA | 403 participants (1 study) | ⊕⊕⊕⊝ moderatea |
Combined data at 1 month from 2 studies (n = 230) reported a lower number of pulmonary exacerbations (either physician‐defined or not clear how they were defined) in the intervention groups across all dose levels for the F508del/F508del genotype. | |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CFQ‐R: Cystic Fibrosis Questionnaire‐Revised; CI: confidence interval; FEV1: forced expiratory volume at 1 second; MD: mean difference; MF: minimal function: NA: not applicable. | ||||||
| GRADE Working Group grades of evidence High quality: further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: we are very uncertain about the estimate. | ||||||
a Downgraded once due to indirectness or lack of applicability: Data do not include children under the age of 12 and those with more severe disease.
We have presented two tables under the comparison of 'Monotherapy compared to control'. In one table we compare lumacaftor monotherapy to placebo (Table 1); we have presented lumacaftor results only rather than other correctors in the table for this comparison due to the relevance of this particular treatment at the time of writing (NICE 2016). In a further table we present results for cavosonstat compared to placebo (Table 2). We have not presented other monotherapy treatments in the summary of findings tables as interventions have not been taken forward on larger more representative populations in Phase 3 studies.
We have presented four tables under the comparison of 'Dual therapy (correctors plus potentiators) compared to control':
lumacaftor (600 mg once daily or 400 mg once daily) plus ivacaftor (250 mg twice daily) versus placebo reporting short‐term results (one month to six months) (Table 3);
lumacaftor (200 mg twice daily) and ivacaftor (250 mg twice daily) versus placebo reporting immediate‐term results (up to one month (Table 4);
lumacaftor (200 mg) plus ivacaftor (150 mg or 250 mg twice daily) versus placebo reporting immediate‐term results (up to one month) (Table 5).
tezacaftor (100 mg once daily) and ivacaftor (150 mg twice daily) versus placebo or ivacaftor (150 mg twice daily alone) (one month to six months) (Table 6).
We have presented tables separately for lumacaftor plus ivacaftor under this comparison due to the differences in doses, measurement times and approaches to analysis.
We have presented two tables for the comparison of 'Triple therapy (correctors plus potentiators) compared to control':
VX‐659 (80 mg once daily, 120 mg twice daily, 240 mg once daily or 400 mg once daily) plus tezacaftor 100 mg once per day plus ivacaftor 150 mg twice daily or VX‐561 150 mg once daily compared to triple placebo (for F508del/MF participants) or placebo tezacaftor 100 mg once daily plus ivacaftor 150 mg twice daily (for F508del/F508del participants) (Table 7); and
elexacaftor (50 mg once daily, 100 mg once daily or 200 mg once daily) plus tezacaftor 100 mg once daily plus ivacaftor 150 mg twice daily or VX‐561 150 mg once daily compared to triple placebo (for F508del/MF participants) or placebo tezacaftor 100 mg once daily plus ivacaftor 150 mg twice daily (for F508del/F508del participants) (Table 8).
We reported the following outcomes in all tables (chosen based on relevance to clinicians and consumers):
survival;
QoL (total score);
QoL (respiratory domain);
FEV1 % predicted (relative and absolute change);
adverse events; and
time to first pulmonary exacerbation.
For clarity in the tables, we do not present adverse events according to the subdomains in Effects of interventions; instead we have inserted a general statement about the summary of findings for these outcomes and graded the evidence based on all of the subdomains combined.
We determined the quality of the evidence using the GRADE approach; and downgraded evidence in the presence of a high risk of bias in at least one study, indirectness of the evidence, unexplained heterogeneity or inconsistency, imprecision of results, high probability of publication bias. We downgraded evidence by one level if we considered the limitation to be serious and by two levels if very serious.
Results
Description of studies
For full information on the characteristics of studies, please see Characteristics of included studies; Characteristics of excluded studies; Characteristics of studies awaiting classification; Characteristics of ongoing studies.
Results of the search
The search of specified databases identified 190 unique references corresponding to 75 studies. No further studies were identified from contacting CF researchers or from screening relevant references. There were 19 studies (97 references) which met the eligibility criteria for inclusion in this review (Boyle 2014; Clancy 2012; Davies 2018a; Davies 2018b; Donaldson 2014; Donaldson 2017; Donaldson 2018; Heijerman 2019; Horsley 2017; Keating 2018; McCarty 2002; Middleton 2019; PROGRESS 2017; Ratjen 2017; Rubenstein 1998; Taylor‐Cousar 2017; TRAFFIC 2015; TRANSPORT 2015; Zeitlin 2002). The results from two of these studies were jointly reported in 20 papers (TRAFFIC 2015; TRANSPORT 2015); a further paper reports two separate studies of the same intervention ‐ a Phase 1 study (Davies 2018a) and a Phase 2 study (Davies 2018b).
We excluded 26 studies (42 references) (Berkers 2014; Chadwick 1998; Chilvers 2017; Drevinek 2017; Leonard 2012; NCT00945347; NCT01899105; NCT03447262; NCT03525574; NCT03537651; NCT03601637; NCT03633526; NCT03691779; NCT04043806; NCT04058366; NCT04105972; NCT04183790; NCT04235140; NCT04362761; NCT04537793; NCT04545515; Nick 2014; Rowe 2017; Rubenstein 2006; Sumner 2014; Ziady 2015).
We have listed 16 studies (25 references) as completed and awaiting classification, to be assessed for inclusion or exclusion at the next update (Downey 2019; EudraCT 2019‐000750‐63; Hunt 2017; Munck 2020; NCT02951195; NCT03447249; NCT03460990; NCT03768089; NCT03911713; NCT03912233; NCT04058353; NCT04353817; PELICAN; Rio‐CF; Taylor‐Cousar 2019; Wainwright 2019).
We identified 14 relevant ongoing studies (26 references) which we will assess for inclusion once completed (ALBATROSS; FLAMINGO; Jain 2018; Meijer 2016; NCT02070744; NCT02323100; NCT02412111; NCT02589236; NCT02718495; NCT02730208; NCT03258424; NCT03559062; NCT03625466; Schwarz 2020).
Results of the online electronic searches are displayed in a PRISMA diagram (Figure 1).
1.
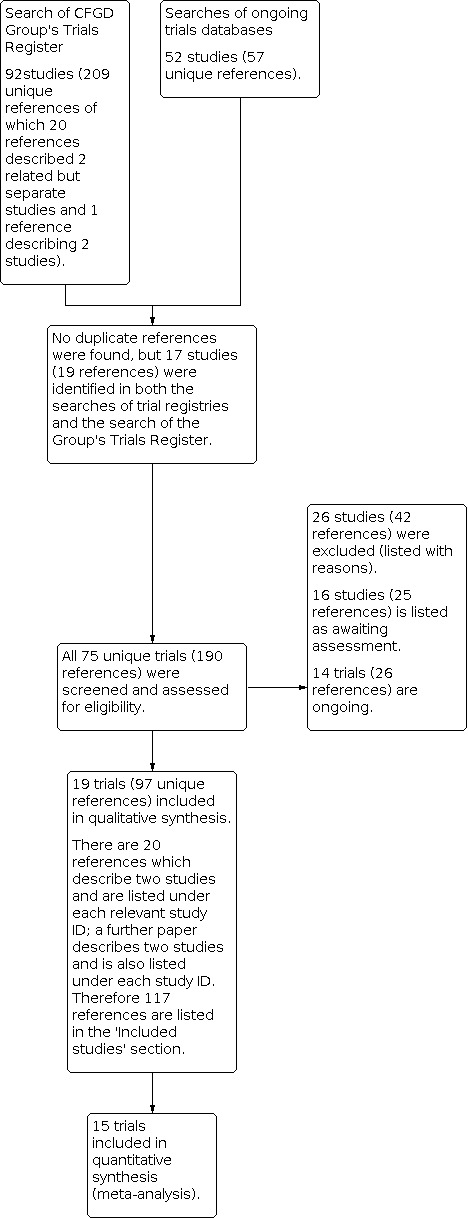
PRISMA study flow diagram
Two included trials were identified through communication with authors, before publication (Heijerman 2019; Middleton 2019).
Included studies
Study design
The 19 included studies ranged from Phase 1 to Phase 3 RCTs, and all employed a parallel study design (Boyle 2014; Clancy 2012; Davies 2018a; Davies 2018b; Donaldson 2014; Donaldson 2017; Donaldson 2018; Horsley 2017; Heijerman 2019; Keating 2018; McCarty 2002; Middleton 2019; PROGRESS 2017; Ratjen 2017; Rubenstein 1998; Taylor‐Cousar 2017; TRAFFIC 2015; TRANSPORT 2015; Zeitlin 2002). The PROGRESS study was an extension study of the TRAFFIC and TRANSPORT studies included in the review (TRAFFIC 2015; TRANSPORT 2015), but with participants in the control group from the initial trials randomised to receive the active treatment at one of two doses (PROGRESS 2017).
A total of 2959 randomised participants were included in this review (participants in the PROGRESS study have only been counted in their original studies and not in this extension study). Study sample sizes ranged from 12 participants (Davies 2018a) to 563 participants (TRANSPORT 2015). One study was composed of three cohorts ‐ cohort 1 (n = 62), cohort 2 (n = 109) and cohort 3 (n = 15); any reference to this study is to participants randomised to cohort 1 only, since data for the placebo participants from cohorts 2 and 3 were pooled, undoing the effects of randomisation and rendering them ineligible for inclusion in this review (Boyle 2014). In the Phase 2 study of tezacaftor‐ivacaftor, only data from the heterozygous population are included (n = 18), as the placebo groups in the homozygous arms of the trial were pooled (Donaldson 2018).
The duration of the included studies ranged from a single day (Phase 1 single‐dose testing) (McCarty 2002) to 24 weeks (Middleton 2019; Ratjen 2017; TRAFFIC 2015; TRANSPORT 2015) with an extension of two of these studies of 96 weeks (PROGRESS 2017).
Two studies were undertaken at single centres (Rubenstein 1998; Zeitlin 2002), but the remaining studies were conducted at multiple centres, ranging from four (McCarty 2002) to 191 sites (PROGRESS 2017). Five studies were conducted in the USA only (Donaldson 2014; Donaldson 2017; McCarty 2002; Rubenstein 1998; Zeitlin 2002), two in the UK only (Davies 2018a; Davies 2018b), four in North America and Europe (Clancy 2012; Donaldson 2018; Heijerman 2019; Ratjen 2017; Taylor‐Cousar 2017), one in Europe and Australia (Horsley 2017) and the remainder across North America, Europe and Australia (Boyle 2014; Keating 2018; Middleton 2019; PROGRESS 2017; TRAFFIC 2015; TRANSPORT 2015).
Full texts were available for 17 studies (Boyle 2014; Clancy 2012; Davies 2018a; Davies 2018b; Donaldson 2017; Donaldson 2018; Heijerman 2019; Keating 2018; McCarty 2002; Middleton 2019; PROGRESS 2017; Ratjen 2017; Rubenstein 1998; Taylor‐Cousar 2017; TRAFFIC 2015; TRANSPORT 2015; Zeitlin 2002); for one study as two conference abstracts (Horsley 2017) and for one further study as two conference abstracts and an online summary on Clinicaltrials.gov (Donaldson 2014).
One Phase 2 study of triple combination therapy indicated there had been a corresponding Phase 1 study, but it was conducted in "healthy volunteers"; the paper does not state if this means people who do not have CF or people who do have CF but are in a good state of health (Keating 2018). The publication does not include any data for the Phase 1 study, although a continuation into a Phase 2 study implies that the safety profile was considered acceptable during the study period. It was not explicitly stated whether any adverse events or safety concerns were observed in the Phase 1 study, nor does it state the dose tested or whether elexacaftor was tested in triple combination or as an individual agent for the purposes of the Phase 1 study (Keating 2018).
Participants
One study recruited pwCF with one F508del variant (the other variant was classified as residual function (ivacaftor responsive)) (Donaldson 2018). Three studies recruited a number of pwCF with two F508del variant copies and a number of pwCF with one F508del copy and a minimal function (MF) (non‐ivacaftor responsive) variant (Davies 2018a; Davies 2018b; Keating 2018). One study recruited adults with F508del/MF genotypes (Middleton 2019). The remaining 15 studies recruited participants who had F508del/F508del genotypes.
One study recruited children between the ages of 6 to 11 years (Ratjen 2017), five studies recruited adolescents and adults (PROGRESS 2017; Rubenstein 1998; Taylor‐Cousar 2017; TRAFFIC 2015; TRANSPORT 2015) and the remaining 13 studies recruited only adults.
Interventions
The included studies examined the effects of 4‐phenylbutyrate (4PBA) (Rubenstein 1998; Zeitlin 2002), 8‐cyclopentyl‐1, 3‐dipropylxanthine (CPX) (McCarty 2002), N6022 (Donaldson 2014), cavosonstat (N91115) (Donaldson 2017), lumacaftor monotherapy (Boyle 2014; Clancy 2012), FDL169 monotherapy (Horsley 2017), lumacaftor‐ivacaftor dual combination therapy (Boyle 2014; PROGRESS 2017; Ratjen 2017; TRAFFIC 2015; TRANSPORT 2015), tezacaftor‐ivacaftor dual combination therapy (Donaldson 2018; Taylor‐Cousar 2017), VX‐659‐tezacaftor‐ivacaftor triple combination therapy (Davies 2018a; Davies 2018b) and elexacaftor‐tezacaftor‐ivacaftor triple combination therapy (Heijerman 2019; Keating 2018; Middleton 2019).
Monotherapy
Eight studies (n = 344) report on monotherapy (Boyle 2014; Clancy 2012; Donaldson 2014; Donaldson 2017; Horsley 2017; McCarty 2002; Rubenstein 1998; Zeitlin 2002).
Two studies compared 4PBA to placebo (Rubenstein 1998; Zeitlin 2002). In the earlier study, participants received either 19 g 4PBA (split into three daily doses) or placebo for one week (Rubenstein 1998). The subsequent Phase 2 study examined the effects 4PBA given at either 20 g (n = 6), 30 g (n = 6) or 40 g (n = 3), given in three daily doses for one week (Zeitlin 2002).
One study compared escalating doses of CPX to placebo (McCarty 2002). Participants were randomised to receive single doses of either placebo (n = 8) or 1 mg (n = 4), 3 mg (n = 4), 10 mg (n = 4), 30 mg (n = 4), 100 mg (n = 5), 300 mg (n = 4) or 1000 mg (n = 4) CPX.
One study compared sequential ascending doses of N6022 to placebo (Donaldson 2014). Participants were randomised to receive placebo (n = 19) or the active drug (intravenous solution of N6022 in normal saline) at a dose of either 5 mg (n = 10), 10 mg (n = 9), 20 mg (n = 9), 40 mg (n = 19). Both treatments were administered by infusion pump over one to eight minutes once per day for seven days.
The study of cavosonstat included both healthy volunteers and pwCF (Donaldson 2017). Those with CF were randomised to receive 50 mg placebo (n = 12) or cavosonstat at different doses (50 mg (n = 12), 100 mg (n = 13), or 200 mg (n = 14)) twice daily for 28 days.
Two included studies compared lumacaftor monotherapy (Boyle 2014; Clancy 2012). One study (n = 64) compared 200 mg lumacaftor once daily for 14 days to placebo; then from day 15, participants took a combination of lumacaftor and ivacaftor twice daily until day 21 thus contributing to two sections of this review (Boyle 2014). The second study of lumacaftor monotherapy used escalating doses of 25 mg (n = 18), 50 mg (n = 18), 100 mg (n = 17) and 200 mg (n = 19), to placebo (n = 17) for 28 days (Clancy 2012).
One study compared FDL169 at doses of 400 mg (n = 6), 600 mg (n = 6) and 800 mg (n = 8), each taken three times daily, versus placebo (n = 7) for 28 days (Horsley 2017).
Dual therapy
Seven studies (n = 1902; including 62 participants from one study which also reported on monotherapy (Boyle 2014)) reported on dual therapy; five studies have evaluated lumacaftor‐ivacaftor combination therapy (Boyle 2014; PROGRESS 2017; Ratjen 2017; TRAFFIC 2015; TRANSPORT 2015) and two studies have evaluated tezacaftor‐ivacaftor combination therapy (Donaldson 2018; Taylor‐Cousar 2017).
Lumacaftor‐ivacaftor combination therapy
In one cohort of a Phase 2 study, participants received 200 mg lumacaftor once daily for 14 days, followed by seven days of 200 mg lumacaftor once daily plus either 150 mg (n = 20) or 250 mg (n = 21) of ivacaftor twice daily (day 15 to 21), or placebo (Boyle 2014). In one Phase 3 study, children received either a combination of lumacaftor 200 mg plus ivacaftor 250 mg every 12 hours or placebo for 24 weeks (Ratjen 2017). Two Phase 3, three‐arm studies (TRAFFIC and TRANSPORT) also compared lumacaftor‐ivacaftor combination therapy to placebo. In these studies, two separate doses of lumacaftor (600 mg once daily and 400 mg twice daily) were combined with twice daily 250 mg of ivacaftor. The placebo group received lumacaftor‐matched placebo every 12 hours in combination with ivacaftor‐matched placebo every 12 hours (TRAFFIC 2015; TRANSPORT 2015). A long‐term extension study (96 weeks) randomised those in the placebo groups of the TRAFFIC and TRANSPORT studies to one of the two lumacaftor‐ivacaftor combination doses; those already receiving an active treatment continued with their existing treatment (PROGRESS 2017).
Tezacaftor‐ivacaftor combination therapy
A Phase 2 study included a dose‐escalation arm, a comparison of various doses of tezacaftor‐ivacaftor in people with the F508del/F508del genotype, and a comparison of tezacaftor‐ivacaftor against ivacaftor alone in people with one F508del variant and one G551D variant (Donaldson 2018). The Phase 3 study compared a combination of tezacaftor 100 mg plus ivacaftor 150 mg every 12 hours to a matched placebo for 24 weeks (Taylor‐Cousar 2017).
Triple therapy
Five studies (n = 775) reported on triple therapy (Davies 2018a; Davies 2018b; Heijerman 2019; Keating 2018; Middleton 2019).
VX‐659‐tezacaftor‐ivacaftor
Two studies compared triple therapy of VX‐659 with tezacaftor and ivacaftor and results were published in a single paper (Davies 2018a; Davies 2018b).
A 14‐day Phase 1 study compared a single dose of 120 mg taken twice daily in combination with tezacaftor 100 mg once daily plus ivacaftor 150 mg twice daily in individuals with a compound heterozygous genotype of F508del/MF (Davies 2018a).
The subsequent four‐week Phase 2 study compared three different doses of VX‐659 in combination with tezacaftor‐ivacaftor to a single placebo group (n = 10) in participants with genotype of F508del/MF variant (n = 53) as follows: VX‐659 80 mg and tezacaftor 100 mg once daily plus ivacaftor 150 mg twice daily (n = 11); VX‐659 240 mg and tezacaftor 100 mg once daily plus ivacaftor 150 mg twice daily (n = 20); VX‐659 400 mg and tezacaftor 100 mg once daily plus ivacaftor 150 mg twice daily (n = 22). These groups taking one of the previously stated doses of the test intervention regimen had a four‐day washout period taking the tezacaftor‐ivacaftor preparation only (same doses). This study also compared once daily VX‐659 400 mg plus tezacaftor 100 mg plus VX‐561 (deuterated ivacaftor) 150 mg to placebo in another group of participants with genotype F508del/MF variant (n = 25) for four weeks. In a further arm of the study, 29 participants with the F508del/F508del variant were randomised to either VX‐659 400 mg plus tezacaftor 100 mg once daily plus ivacaftor 150 mg twice daily (n = 18) or to placebo plus tezacaftor 100 mg once daily plus ivacaftor 150 mg twice daily (this dual therapy combination is currently considered the standard of care in individuals with this genotype) (n = 11). This cohort (n = 29) had a four‐week run‐in period taking the same dose of tezacaftor‐ivacaftor only before starting the triple therapy combination for four weeks. Once the intervention period was over, these participants had a further four‐week washout period of taking the same dose of tezacaftor‐ivacaftor as a dual combination (Davies 2018b).
Elexacaftor‐tezacaftor‐ivacaftor
Three studies examined the triple combination of elexacaftor in combination with tezacaftor and ivacaftor (Heijerman 2019; Keating 2018; Middleton 2019).
One Phase 2 study compared three different doses of elexacaftor to placebo (n = 12) in participants with F508del/MF for four weeks, followed by a one‐week washout period of tezacaftor‐ivacaftor or dual placebo.The intervention doses were as follows: elexacaftor 50 mg and tezacaftor 100 mg once daily plus ivacaftor 150 mg twice daily (n = 10); elexacaftor 100 mg and tezacaftor 100 mg once daily plus ivacaftor 150 mg twice daily (n = 14); and elexacaftor 200 mg and tezacaftor 200 mg once daily plus ivacaftor 150 mg twice daily (n = 21). The same study also compared once daily elexacaftor 200 mg plus tezacaftor 100 mg plus VX‐561 150 mg to triple placebo in a group of participants with F508del/MF (n = 29); these participants had no run‐in or washout period. Also, a further group of F508del/F508del participants (n = 28) had a four‐week run‐in period of once daily tezacaftor 100 mg plus ivacaftor 150 mg, followed by the intervention period of once daily elexacaftor 200 mg or equivalent placebo while continuing with tezacaftor‐ivacaftor at the same doses; this was followed by a four‐week washout period where all participants took just tezacaftor‐ivacaftor at the previous doses (Keating 2018).
The remaining two studies were Phase 3 studies (Heijerman 2019; Middleton 2019). The first of these two studies compared elexacaftor 200 mg once daily plus tezacaftor 100 mg once daily and ivacaftor 150 mg twice daily (n = 55) versus placebo once daily plus tezacaftor 100 mg once daily and ivacaftor 150 mg twice daily (n = 52) over four weeks in participants with a F508del/F508del homozygous genotype (Heijerman 2019). The second study compared elexacaftor 200 mg once daily plus tezacaftor 100 mg once daily and ivacaftor 150 mg twice daily (n = 200) versus triple placebo (n = 203) in participants with a F508del/MF heterozygous genotype for six months (Middleton 2019). The second variant in these participants was a MF mutation, so the trial can be considered to reflect the impact of the triple therapy on the single F508del variant. It should be considered that some of the MF variants may have been responsive to triple therapy as well, but we considered it appropriate to consider this group collectively.
Outcomes
All included studies (monotherapy, dual therapy or triple therapy) reported on survival. There were 14 studies reporting QoL, all of which utilised the respiratory domain of the CFQ‐R (Clancy 2012; Davies 2018a; Davies 2018b; Donaldson 2017; Donaldson 2018; Heijerman 2019; Horsley 2017; Keating 2018; Middleton 2019; PROGRESS 2017; Ratjen 2017; Taylor‐Cousar 2017; TRAFFIC 2015; TRANSPORT 2015). Lung function using FEV1 was reported in 17 studies (Boyle 2014; Clancy 2012; Davies 2018a; Davies 2018b; Donaldson 2014; Donaldson 2017; Donaldson 2018; Heijerman 2019; Horsley 2017; Keating 2018; McCarty 2002; Middleton 2019; PROGRESS 2017; Ratjen 2017; Taylor‐Cousar 2017; TRAFFIC 2015; TRANSPORT 2015). One study additionally reported LCI (Ratjen 2017).
Reporting of the pre‐specified secondary outcomes in this review varied across studies. All included studies monitored the adverse effects of therapy, but the manner in which these safety outcomes were analysed and reported varied considerably. 10 studies reported outcomes relating to pulmonary exacerbations (Davies 2018a; Davies 2018b; Heijerman 2019; Keating 2018; Middleton 2019; PROGRESS 2017; Rubenstein 1998; Taylor‐Cousar 2017; TRAFFIC 2015; TRANSPORT 2015) (please see our definition of exacerbations above (Types of outcome measures)). For monotherapy, two studies stated that exacerbations were physician‐defined (Boyle 2014; Clancy 2012), one study referred to them as 'infective exacerbations' (Donaldson 2017), in two studies it was unclear whether exacerbations were protocol‐ or physician‐defined (Donaldson 2014; Horsley 2017) and in two studies pulmonary exacerbation was not included as an outcome (Rubenstein 1998; Zeitlin 2002). For dual therapy, two studies defined exacerbations as episodes requiring antibiotics or hospitalisation (TRAFFIC 2015; TRANSPORT 2015), for one study, exacerbations were physician‐defined (Boyle 2014) and for four studies, it is unclear whether exacerbations are protocol‐ or physician‐defined (Donaldson 2018; PROGRESS 2017; Ratjen 2017; Taylor‐Cousar 2017). For triple therapy, all trials defined exacerbations as those which were infective in nature or required antibiotics (Davies 2018a; Davies 2018b; Heijerman 2019; Keating 2018; Middleton 2019). One study specifically reported on rates of hospitalisation (Middleton 2019). Changes in sweat chloride, as a marker of CFTR function, were reported by 14 studies (Boyle 2014; Clancy 2012; Davies 2018a; Davies 2018b; Donaldson 2014; Donaldson 2017; Heijerman 2019; Horsley 2017; Keating 2018; Middleton 2019; Ratjen 2017; Rubenstein 1998; Taylor‐Cousar 2017; Zeitlin 2002). A sub‐study from one of the trials reported radiological outcomes (Ratjen 2017). Two studies reported microbiological outcomes (Taylor‐Cousar 2017; Zeitlin 2002). Six studies reported BMI (Heijerman 2019; PROGRESS 2017; Ratjen 2017; Taylor‐Cousar 2017; TRAFFIC 2015; TRANSPORT 2015).
Funding sources
Pharmaceutical companies primarily funded 14 studies (Davies 2018a; Davies 2018b; Donaldson 2014; Donaldson 2017; Heijerman 2019; Horsley 2017; Keating 2018; Middleton 2019; PROGRESS 2017; McCarty 2002; Ratjen 2017; Taylor‐Cousar 2017; TRAFFIC 2015; TRANSPORT 2015). Three studies were funded jointly by pharmaceutical companies and other sources (Boyle 2014; Clancy 2012; Donaldson 2018). Two studies were not funded by pharmaceutical companies at all: one was funded by the Cystic Fibrosis Foundation (CFF) (Zeitlin 2002), and one jointly by the CFF and the NIH (Rubenstein 1998).
Further information about the studies is presented in the tables (Characteristics of included studies).
Excluded studies
We excluded 26 studies in total. Six studies were of cross‐over design (Berkers 2014; Leonard 2012; NCT00945347; NCT01899105; Nick 2014; Rowe 2017). 14 studies were single‐assignment studies, i.e. participants were not randomised to different study arms (Chilvers 2017; NCT03447262; NCT03525574; NCT03537651; NCT03601637; NCT03633526; NCT03691779; NCT04043806; NCT04058366; NCT04183790; NCT04235140; NCT04362761; NCT04545515; Rubenstein 2006). Three studies were not randomised (Chadwick 1998; NCT04105972; NCT04537793). One study was a pre‐clinical laboratory study (Ziady 2015). One study was of general gene therapy and not a mutation‐specific therapy (Sumner 2014). In the final study, the intervention was not considered to be a corrector for type II variants (Drevinek 2017).
Studies awaiting classification
There are 16 studies awaiting classification due to a lack of information (Downey 2019; EudraCT 2019‐000750‐63; Hunt 2017; Munck 2020; NCT02951195; NCT03447249; NCT03460990; NCT03768089; NCT03911713; NCT03912233; NCT04058353; NCT04353817; PELICAN; Rio‐CF; Taylor‐Cousar 2019; Wainwright 2019). For further details on each of these studies, please see the table Characteristics of studies awaiting classification.
All 16 studies are RCTs of parallel design, with varying numbers of arms in the studies ‐ some with only two arms and others with three arms. The duration of studies varies from 14 days (Downey 2019) to 72 weeks (Wainwright 2019). Participants ranged in age with 10 studies recruiting adults aged 18 years and over (Downey 2019; EudraCT 2019‐000750‐63; Hunt 2017; NCT02951195; NCT03768089; NCT03911713; NCT03912233; PELICAN; Rio‐CF; Taylor‐Cousar 2019), five studies recruiting participants aged 12 years and over (Munck 2020; NCT03447249; NCT03460990; NCT04058353; Wainwright 2019) and one study recruiting children aged 6 to 11 years of age (NCT04353817). The genotype of participants also varied with seven studies recruiting participants homozygous for F508del (Downey 2019; EudraCT 2019‐000750‐63; Hunt 2017; NCT03460990; PELICAN; Rio‐CF; Wainwright 2019), four studies recruiting participants with F508del/MF (Munck 2020; NCT03447249; NCT03768089; NCT04353817), two studies recruiting participants with both the genotype F508del/F508del and F508del/MF (NCT02951195; NCT03912233), one study recruiting participants with the genotype F508del/gating variant or F508del/residual function (NCT04058353) and one study recruiting participants with at least one copy of G551D, G178R, S549N, S549R, G551S, G1244E, S1251N, S1255P, or G1349D (NCT03911713). One study did not state the genotype of participants (Taylor‐Cousar 2019).
Most studies are placebo‐controlled, but two studies are described as having 'active‐controlled' arms (NCT02951195; NCT04058353). The active drugs and drug regimens vary. There are four placebo‐controlled monotherapy studies comparing ABBV‐3067 (EudraCT 2019‐000750‐63), riociguat (Rio‐CF), siidenafil (Hunt 2017) and VX‐561 (NCT03911713). Three studies describe dual therapies of ABBV‐3067 with ABBV‐2222 (EudraCT 2019‐000750‐63), PTI‐801 with PTI‐808 (Downey 2019) and tezacaftor‐ivacaftor (Wainwright 2019). Triple therapy is described in 10 studies using: PTI‐801 with PTI‐808 and PTI‐428 (Downey 2019), PTI‐428 with tezacaftor‐ivacaftor (Taylor‐Cousar 2019), GLPG‐2737 with lumacaftor‐ivacaftor (PELICAN), elexacaftor‐tezacaftor‐ivacaftor (NCT04058353; NCT04353817), VX‐121 with tezacaftor‐ivacaftor (NCT03768089), VX‐121 with tezacaftor and VX‐561 (NCT03912233), VX‐152 with tezacaftor‐ivacaftor (NCT02951195) and VX‐659 with tezacaftor‐ivacaftor (NCT03447249; NCT03460990).
Ongoing studies
There are 14 studies listed as ongoing (ALBATROSS; FLAMINGO; Jain 2018; Meijer 2016; NCT02070744; NCT02323100; NCT02412111; NCT02589236; NCT02718495; NCT02730208; NCT03258424; NCT03625466; NCT03559062; Schwarz 2020).
Monotherapy
Seven ongoing clinical studies are currently evaluating five different monotherapy correctors (ALBATROSS; FLAMINGO; Jain 2018; Meijer 2016; NCT02323100; NCT02718495; NCT03258424).
Two studies are currently evaluating GLPG2222 (ALBATROSS; FLAMINGO). The ALBATROSS study is a Phase 2, placebo‐controlled multicentre study based in Australia and Europe and is testing multiple four‐week dose regimens of GLPG2222 in 37 adults with CF with a F508del/Class III variant genotype who are already on stable ivacaftor (ALBATROSS). GLPG2222 is taken orally and the dose levels are either 150 mg daily or 300 mg daily. Outcomes measured include adverse events, pharmacokinetic data, sweat chloride concentration, lung function and QoL (ALBATROSS). The FLAMINGO study is also a multicentre Phase 2 study being conducted in North America and Europe (FLAMINGO). In this study investigators are testing multiple dose regimens of GLPG2222 for four weeks in adults with CF with the F508del/F508del genotype and a baseline FEV1 of at least 40% predicted who have not taken concomitant CFTR correctors in the previous four weeks. Doses range from 50 mg to 400 mg four times daily. Outcomes measured include adverse events, sweat chloride concentration, lung function, QoL and pharmacokinetic data (FLAMINGO).
Two studies are evaluating PTI‐428 (a particular type of CFTR corrector called an amplifier, which augment the actions of other CFTR modulators) (NCT02718495; NCT03258424). The first study expects to recruit 56 adults with CF (mutation not specified) and is being conducted at 29 centres across North America and Europe (NCT02718495). The 28‐day intervention is comparing ascending dose treatment (doses not stated) to placebo. Outcome measures include adverse events, lung function, pharmacokinetics, sweat chloride, weight and QoL (NCT02718495). The second study is a Phase 1 placebo‐controlled RCT being run at two centres in the UK (NCT03258424). It plans to recruit 16 adults with CF who are already receiving ivacaftor for 14 days of treatment, but dose levels of PTI‐428 are not stated. Outcome measures include adverse events, pharmacokinetic outcomes, sweat chloride, lung function and weight (NCT03258424).
One study is evaluating PTI‐801 alone and also in combination with PTI‐428 compared to placebo in a Phase 1 study in adults with CF (homozygous F508del in three cohorts and heterozygous F508del in one cohort) who have a baseline FEV1 of 40% to 90% and who are currently receiving lumacaftor‐ivacaftor as background therapy (Jain 2018). It is a multicentre UK‐based study with an estimated enrolment of 32 participants and a treatment duration of 14 days with a follow‐up visit at 21 days. There are four arms, two 14‐day arms comparing different doses of combined PTI‐808 and PTI‐801 to placebo, one 14‐day arm comparing combined PTI‐808, PTI‐801 and PTI‐428 to placebo and one arm comparing PTI‐808, PTI‐801 and PTI‐428 to placebo for seven days followed by PTI‐808 and PTI‐801 versus placebo for a further seven days (no washout period). Outcomes include adverse events, pharmacokinetics, lung function, sweat chloride, nutritional outcomes and QoL (Jain 2018).
One double‐blind randomised study is comparing two doses (200 mg or 400 mg) of a corrector known as (R)‐roscovitine to placebo in 36 adults with CF with either one or two copies of the F508del mutation (Meijer 2016). This is a multicentre French study with a three‐month duration. The primary outcome measure is safety; other outcomes include pharmacokinetic parameters, QoL, lung function, BMI, sweat chloride concentration and nasal potential difference (Meijer 2016).
One seven‐day study is comparing glycerol phenylbutyrate (GPBA) in the form of an oral liquid in a low‐dose arm and in a high‐dose arm to matching placebo in adults with CF and the genotype F508del/F508del (NCT02323100). Outcomes include the change in nasal potential difference, sweat chloride measurement and adverse events.
Dual therapy
Five ongoing studies are evaluating the safety and efficacy of tezacaftor‐ivacaftor in pwCF (NCT02070744; NCT02412111; NCT02730208; Schwarz 2020; NCT03559062) and one study evaluating lumacaftor‐ivacaftor in children with CF (NCT03625466).
Three of the tezacaftor‐ivacaftor studies and the lumacaftor‐ivacaftor study have enrolled participants with the F508del/F508del genotype (NCT02070744; NCT02730208; NCT03625466; Schwarz 2020). One is a Phase 2 multicentre study (n = 40) comparing tezacaftor 50 mg or 100 mg once daily plus ivacaftor 150 mg twice daily to matched placebo for 12 weeks in adults followed by an open‐label extension. The primary outcome is safety and adverse events; secondary outcomes are both the absolute and relative change in FEV1, the absolute change from baseline in sweat chloride, the absolute change from baseline in body weight and BMI, the absolute change from baseline in CFQ‐R respiratory domain and pharmacological data (NCT02070744). The second study is a Phase 2 double‐blind RCT in 41 participants aged 12 years or older comparing tezacaftor 100 mg once daily plus ivacaftor 150 mg twice daily versus matched placebo. The primary outcome is absolute change in total Brody/CF‐CT score at 72 weeks; the secondary outcome is the number of participants with treatment‐emergent adverse events and serious adverse events (NCT02730208). The third study (n = 98) is an eight‐week Phase 3b parallel, double‐blind, multicentre RCT comparing tezacaftor 100 mg once daily and ivacaftor 150 mg twice daily to matched placebo in participants aged 12 and over who have previously been taking lumacaftor‐ivacaftor, but were not able to continue due to an adverse event or drug reaction. The primary outcome is the incidence of respiratory adverse events of special interest (chest discomfort, dyspnoea, chest tightness, asthma, bronchial hyperreactivity, bronchospasm and wheezing). Secondary outcomes are the absolute and relative change from baseline in FEV1 % predicted, the absolute change in CFQ‐R respiratory domain score, tolerability (the number of participants who discontinue treatment) and number of participants with treatment‐emergent adverse events and serious adverse events (Schwarz 2020). The lumacaftor‐ivacaftor study (n = 51) is a 48‐week parallel‐design study comparing lumacaftor‐ivacaftor to matched placebo in children aged between two and five years of age (NCT03625466). Outcomes include the absolute change in MRI global chest score, the absolute change in LCI 2.5, the absolute change in weight‐for‐age z score, the absolute change in stature‐for‐age z score and the absolute change in BMI‐for‐age z score.
One Phase 3 study (n = 156) is in participants 12 years and older who have one copy of the F508del mutation and one gating mutation that has been found to be responsive to ivacaftor therapy; the active intervention group have a run‐in of ivacaftor for four weeks (150 mg twice daily) followed by dual therapy of tezacaftor 100 mg once daily and ivacaftor 150 mg twice daily for eight weeks compared to a control group receiving ivacaftor 150 mg twice daily and matched placebo. The primary outcome is the absolute change in FEV1 % predicted. Secondary outcomes are the relative change from baseline in FEV1 % predicted, the absolute change in CFQ‐R respiratory domain, the absolute change from baseline in sweat chloride, the number of participants with treatment‐emergent adverse events and serious adverse events and pharmacological measures (NCT02412111).
The final study (n = 69) is an eight‐week Phase 3, double‐blind, parallel study comparing tezacaftor‐ivacaftor (doses and frequencies not yet stated) to placebo in children aged 6 to 11 years who have either one or two copies of F508del (NCT03559062). The primary outcome is LCI2.5 .Secondary outcomes are the absolute change in sweat chloride, the absolute change in CFQ‐R respiratory domain score and safety and tolerability (adverse events and non‐serious adverse events) (NCT03559062).
Triple therapy
One ongoing Phase 2 randomised, placebo‐controlled, parallel study (n = 138) is evaluating triple therapies (NCT02589236). It is assessing the efficacy of adding cavosonstat to pre‐existing lumacaftor‐ivacaftor therapy for 12 weeks in adults with the genotype F508del/F508del. There are three arms: lumacaftor (dose not stated) with ivacaftor (dose not stated) and cavosonstat 200 mg twice daily versus lumacaftor(dose not stated) with ivacaftor (dose not stated) and cavosonstat 400 mg twice daily versus lumacaftor (dose not stated) with ivacaftor (dose not stated) and matched placebo. The primary outcome is the absolute change from baseline in FEV1 % predicted. Secondary outcomes are the relative change from baseline in FEV1 % predicted, the absolute change from baseline in sweat chloride, the absolute change from baseline in CFQ‐R respiratory domain, the absolute change from baseline in BMI, the absolute change from baseline in patient global impression of change (PGIC), the incidence of treatment‐emergent adverse events, pharmacological measures and number of pulmonary exacerbations (NCT02589236).
Risk of bias in included studies
We have summarised our risk of bias judgements in the figures (Figure 2; Figure 3).
2.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
3.

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
Allocation
Sequence generation
We judged 11 studies to have a low risk of bias (Boyle 2014; Davies 2018a; Davies 2018b; Heijerman 2019; Keating 2018; Middleton 2019; PROGRESS 2017; Ratjen 2017; Taylor‐Cousar 2017; TRAFFIC 2015; TRANSPORT 2015). Of these, one study used a computer‐generated randomisation schedule developed by an independent party (Boyle 2014), and the others randomised participants via an interactive web response system (Davies 2018a; Davies 2018b; Heijerman 2019; Keating 2018; Middleton 2019; PROGRESS 2017; Ratjen 2017; Taylor‐Cousar 2017; TRAFFIC 2015; TRANSPORT 2015). As none of the remaining eight included studies reported details of random sequence generation we have judged the risk of bias as unclear (Clancy 2012; Donaldson 2014; Donaldson 2017; Donaldson 2018; Horsley 2017; McCarty 2002; Rubenstein 1998; Zeitlin 2002).
Allocation concealment
We judged 11 studies to have a low risk of bias (Boyle 2014; Davies 2018a; Davies 2018b; Heijerman 2019; Keating 2018; Middleton 2019; PROGRESS 2017; Ratjen 2017; Taylor‐Cousar 2017; TRAFFIC 2015; TRANSPORT 2015). In the Phase 2 lumacaftor‐ivacaftor study, site pharmacists dispensed drugs on the basis of an interactive voice response system, making it unlikely that participants or study personnel would have been aware of group assignments prior to recruitment into the study (Boyle 2014). The remaining lumacaftor‐ivacaftor studies, the tezacaftor‐ivacaftor study and the elexacaftor‐tezacaftor‐ivacaftor study also employed an interactive web response system to allocate participants to treatment groups (Davies 2018a; Davies 2018b; Heijerman 2019; Keating 2018; Middleton 2019; PROGRESS 2017; Ratjen 2017; Taylor‐Cousar 2017; TRAFFIC 2015; TRANSPORT 2015). Methods to conceal group allocation were not reported by the remaining eight studies, who also failed to report on random sequence generation, so we judged these as having an unclear risk of bias (Clancy 2012; Donaldson 2014; Donaldson 2017; Donaldson 2018; Horsley 2017; McCarty 2002; Rubenstein 1998; Zeitlin 2002).
Blinding
We judged 14 studies to have a low risk of performance and detection bias (Boyle 2014; Davies 2018a; Davies 2018b; Donaldson 2014; Donaldson 2017; Donaldson 2018; Heijerman 2019; Keating 2018; Middleton 2019; PROGRESS 2017; Ratjen 2017; Taylor‐Cousar 2017; TRAFFIC 2015; TRANSPORT 2015). In the Boyle study, drug doses were prepared by an independent unmasked pharmacist and dispensed by site pharmacists who were masked to treatment assignment. Site investigators and the study sponsor were also masked to treatment assignment and to sweat chloride levels ‐ data that could have potentially disclosed treatment assignment. Participant blinding was maintained by placebo which was matched to intervention by the quantity of tablets and by size, colour, coating and packaging (Boyle 2014). In the earlier Donaldson study, participants, care givers, investigators and outcome assessors were double‐blinded via intravenous administration of placebo (saline) using the same volume as the active drug groups (Donaldson 2014). In the two Phase 3 lumacaftor‐ivacaftor studies and the extension study, the participants and study team remained blinded to the treatment assignments and the placebo was matched in appearance and packaging to the active intervention. The online protocol further stated that all site personnel, including the investigator, the site monitor and the study team would remain blinded to treatment group (PROGRESS 2017; TRAFFIC 2015; TRANSPORT 2015). In the paediatric lumacaftor‐ivacaftor study, double blinding was achieved by using placebo tablets visually identical to the test product (Ratjen 2017). Both tezacaftor‐ivacaftor dual combination studies made use of matched placebo and employed double blinding to reduce performance bias (Donaldson 2018; Taylor‐Cousar 2017). The three triple combination studies were all found to have a low risk of performance bias, as the participants and site personnel were blinded to allocation. They were all also considered to have an unclear risk of detection bias, as though all authors were blinded to allocation, no mention is made of other outcome assessors (e.g. clinicians who were not authors, but were involved in seeing participants and measuring outcomes of interest) and whether there was a possibility of them knowing allocated intervention (Davies 2018a; Davies 2018b; Heijerman 2019; Keating 2018; Middleton 2019).
In the pilot 4PBA, CPX, FDL169 and the lumacaftor monotherapy studies, there was insufficient information about how participant, study personnel or outcome assessor blinding was maintained and so we judged these four studies to have an unclear risk of performance and detection bias (Clancy 2012; Horsley 2017; McCarty 2002; Rubenstein 1998).
Participants from the three intervention groups (20 g, 30 g and 40 g) in the Phase 2 4PBA study had different dosing schedules and were given a different number of tablets. Therefore this study was judged to have a high risk of performance bias. Also in this study, there were insufficient data on blinding of outcome assessors and we therefore judged it to have an unclear risk of detection bias (Zeitlin 2002).
Incomplete outcome data
We judged 15 studies to have a low risk of bias due to incomplete outcome data (Davies 2018a; Davies 2018b; Donaldson 2014; Donaldson 2018; Heijerman 2019; Horsley 2017; Keating 2018; Middleton 2019; PROGRESS 2017; McCarty 2002; Ratjen 2017; Rubenstein 1998; Taylor‐Cousar 2017; TRAFFIC 2015; TRANSPORT 2015).
Three studies were judged to have an unclear risk of attrition bias (Boyle 2014; Donaldson 2017; Zeitlin 2002). In the Phase 2 lumacaftor‐ivacaftor study, one out of 62 participants withdrew (1.6%) due to an adverse effect, demonstrating a low withdrawal rate. However, in the analysis only participants for whom data were available were included. Although these participants were excluded because of insufficient data rather than for reasons that could potentially lead to the exclusion of participants with unfavourable characteristics, e.g. adverse effects, we judged this study as having an unclear risk of attrition bias because it was unclear how these exclusions would have affected the balance between groups in baseline characteristics (Boyle 2014). The cavosonstat study was judged as having an unclear risk of bias in this domain because two out of 51 participants are unaccounted for in the final analysis, but it is unlikely that these would affect the overall findings (Donaldson 2017). In the Phase 2 4PBA study, all 19 randomised participants completed the final study visit, but risk of attrition bias was unclear because there was no report of how many of these participants were included in the analysis (Zeitlin 2002). We approached the primary author to clarify this, but did not receive any additional information.
We judged the study of lumacaftor monotherapy to have a high risk of attrition bias (Clancy 2012). Although only four out of 89 (5%) participants withdrew from the study due to adverse events (demonstrating a low withdrawal rate), data for a number of outcomes were excluded from the analysis. A total of 42 participants were excluded from reports of adverse events; nine participants were excluded from reports on change from baseline in sweat chloride concentration (demonstrated by figure 1b in the full‐text article) and four participants were excluded from the information on CFQ‐R domain scores. Our judgement of a high risk of attrition bias was due firstly to the high level of excluded participant data and secondly to the lack of reasons for the exclusion of these participant data. The study's lead investigator was approached for clarification, but we have received no response to date (Clancy 2012).
Selective reporting
Where study protocols were not available, or there were missing outcome data, we approached the studies' primary authors for additional information.
We judged eight studies to have a low risk of reporting bias (Boyle 2014; Donaldson 2017; Donaldson 2018; Heijerman 2019; Middleton 2019; PROGRESS 2017; McCarty 2002; Rubenstein 1998). For the Phase 2 lumacaftor‐ivacaftor study, the protocol was not available, but outcomes were presented on the NIH trials registry (clinicaltrials.gov/); we did not identify any missing outcomes for the included cohort (Boyle 2014). For the pilot 4PBA and CPX studies, protocols were not available and planned outcomes were not listed on ongoing online trials databases (McCarty 2002; Rubenstein 1998). So, we compared the outcomes reported in the 'Methods' sections to the outcomes reported in the 'Results' sections of the publications and did not identify any missing outcomes (McCarty 2002; Rubenstein 1998). For the extension study of TRAFFIC and TRANSPORT, we compared the list of outcomes provided on the NIH trials registry to the results reported in the published paper; all listed outcomes were reported (PROGRESS 2017). Two Phase 3 triple combination studies stated outcomes in both the protocol and results (Heijerman 2019; Middleton 2019).
In total five studies were judged to have an unclear risk of reporting bias (Davies 2018a; Davies 2018b; Donaldson 2014; Horsley 2017; Keating 2018). Two of these studies were of monotherapy (Donaldson 2014; Horsley 2017). For the Donaldson study, only limited results were available from the NIH trials registry and it was unclear if all relevant information has been made available. Similarly, since only limited information was available for the FDL169 study, we also deemed it to have an unclear risk of bias (Horsley 2017). The remaining three studies were of triple combination therapy and each stated in their methods that they would measure 12‐lead ECG and vital signs; however, none of the studies report data or information for these outcomes in their results or supplements (Davies 2018a; Davies 2018b; Keating 2018).
We judged six studies to have a high risk of bias from selective outcome reporting (Clancy 2012; Ratjen 2017; Taylor‐Cousar 2017; TRAFFIC 2015; TRANSPORT 2015; Zeitlin 2002). The protocol for the Clancy lumacaftor study was not available, but the planned outcomes were listed on the NIH trials registry. We compared these outcomes to those reported in the 'Results' section of the published paper and ascertained that no data were reported for FEF25-75% or FVC at 28 days (Clancy 2012). The study protocol for the Phase 2 4PBA study was not available and planned outcomes were not listed on ongoing online trials databases (Zeitlin 2002). We compared the outcomes reported in the 'Methods' section of the paper to the outcomes reported in the 'Results' section and identified that data were not reported for the change from baseline in FEV1 or microbiology scores at day seven (Zeitlin 2002).
In the two Phase 3 lumacaftor‐ivacaftor studies, pre‐specified data were reported on the NIH trials registry (TRAFFIC 2015; TRANSPORT 2015). In these studies, data for the outcomes; absolute change from baseline in FEV1 and relative change from baseline in FEV1 were combined at 16 and 24 weeks. The combination of these data was not pre‐specified and the primary author was contacted from clarification. Furthermore, some results had to be extrapolated from graphical figures and some additional data were only reported on ClinicalTrials.gov for outcomes not reported in the final paper. Also, investigators state that they measured FVC (which was not listed as an end‐point) and do not report this in the joint paper (TRAFFIC 2015; TRANSPORT 2015).
In the paediatric combination study, several outcomes which were listed in the methods of the full publication and also on the ClinicalTrials.gov entry for this study were not reported in the results section of the paper (Ratjen 2017). These outcomes include LCI5.0, weight, height and time to first pulmonary exacerbation.
In the tezacaftor‐ivacaftor combination study, a number of outcomes were recorded according to the study protocol but were not reported in the published paper (Taylor‐Cousar 2017). These outcomes were the CF respiratory symptom diary, duration of daily physical activity (number of minutes), the Pittsburgh Sleep Quality Index (PSQI), SF‐12 health survey, sputum microbiology, the time‐to‐first and number of days with an exacerbation, the time to first hospitalisation and the number of days hospitalised with exacerbation, the number of exacerbations requiring IV therapy, the time to the first IV therapy and the number of days on IV therapy.
For both studies of VX‐659 we judged there to be an unclear risk of selective outcome reporting (Davies 2018a; Davies 2018b). Some of the outcomes stated in the methodology of the Phase 1 study were not reported (safety measures) (Davies 2018a). Similarly in the Phase 2 study, not all outcomes stated in the methodology and identified as of interest in this review were reported in the primary paper; however, all outstanding outcomes which were stated in the methodology, were reported in the online supplement except for vital signs and ECG findings (Davies 2018b).
For the Phase 2 study looking at elexacaftor, we also judged there to be an unclear risk of selective reporting (Keating 2018). Not all outcomes stated in the methodology and identified as of interest in this review were reported in the primary paper: however, all outstanding outcomes, stated in the methodology, were reported in the online supplement except for vital signs and ECG findings (Keating 2018).
Other potential sources of bias
We judged there to be a low risk of other bias due to no significant difference between baseline characteristics in six studies (PROGRESS 2017; Rubenstein 1998; Taylor‐Cousar 2017; TRAFFIC 2015; TRANSPORT 2015; Zeitlin 2002) and due to well‐matched baseline characteristics in a further nine studies (Boyle 2014; Clancy 2012; Donaldson 2014; Ratjen 2017; Davies 2018a; Davies 2018b; Keating 2018; Heijerman 2019; Middleton 2019). Futhermore, in both the TRAFFIC and TRANSPORT studies adherence to treatment was high with similar compliance rates across the different treatment groups (TRAFFIC 2015; TRANSPORT 2015).
In the remaining four studies, there was insufficient detail about baseline characteristics or an apparent imbalance in baseline characteristics, leading to an unclear risk of bias (Donaldson 2017; Donaldson 2018; Horsley 2017; McCarty 2002).
Effects of interventions
See: Table 1; Table 2; Table 3; Table 4; Table 5; Table 6; Table 7; Table 8
As described above, we identified three types of intervention relevant for this review. The first group of studies examined single agents that aimed to correct the F508del trafficking defect (commonly referred to as "correctors"). The second and third groups of studies examined a combination of various correctors with ivacaftor (a drug known to potentiate the function of the CFTR in the membrane). As these interventions have different potential mechanisms of action, we present the results separately for 'Monotherapy compared to control', 'Dual therapy (correctors plus potentiators) compared to control' and 'Triple therapy (correctors plus potentiators) compared to control'. Results are summarised for all doses reported separately and for treatment doses combined where appropriate. In the summary of findings tables, the quality of the evidence has been graded for pre‐defined outcomes (see above) and definitions of these gradings provided.
Monotherapy compared to control
Eight studies with 344 participants contributed to this comparison (Boyle 2014; Clancy 2012; Donaldson 2014; Donaldson 2017; Horsley 2017; McCarty 2002; Rubenstein 1998; Zeitlin 2002).
Two studies (n = 37) compared 4PBA to placebo (Rubenstein 1998; Zeitlin 2002), one study (n = 66) compared N6022 to placebo (Donaldson 2014), one study (n = 37) compared CPX to placebo (McCarty 2002) and two studies (n = 151) compared varying doses of lumacaftor alone to placebo (Boyle 2014; Clancy 2012). One study (n = 51) compared cavosonstat 200 mg (twice daily) to placebo; we only present the 200 mg dose comparison (n = 26) from this early‐phase study as this is the only dose that is being studied further and other doses are not relevant to current clinical practice (Donaldson 2017). Participants in one study (n = 62) received lumacaftor monotherapy for 14 days followed by combination therapy with ivacaftor for seven days, therefore this study contributes to both comparisons of this review (Boyle 2014). One study (n = 27) compared FDL169 at doses of 400 mg (n = 6), 600 mg (n = 6) and 800 mg (n = 8) to placebo (n = 7). All different dose levels were compared to the same placebo group of seven participants (Horsley 2017).
With regards to pulmonary exacerbations, please see our definition above (Types of outcome measures). For monotherapy, two studies stated that exacerbations were physician‐defined (Boyle 2014; Clancy 2012), one study referred to them as 'infective exacerbations' (Donaldson 2017), in two studies it was unclear whether exacerbations were protocol‐ or physician‐defined (Donaldson 2014; Horsley 2017) and in two studies pulmonary exacerbation was not included as an outcome (Rubenstein 1998; Zeitlin 2002).
Important results for the drugs lumacaftor and cavosonstat within this comparison are summarised in the tables (Table 1; Table 2). We have assessed the following outcomes using the GRADE criteria in each of the tables and indicated our findings in the relevant text below.
survival;
QoL (total score);
QoL (respiratory domain);
FEV1 % predicted (relative and absolute change);
adverse events; and
time to first pulmonary exacerbation.
For the comparison of lumacaftor versus placebo, we judged the quality of the evidence to be of moderate to very‐low quality; evidence was downgraded due to serious concerns over risk of bias, due to indirectness related to the design of the studies and due to imprecision where few events occurred and CIs around the result were very wide (Table 1). For the comparison of cavosonstat versus placebo we judged the quality of the evidence to be very low; evidence was downgraded due to concerns over risk of bias, due to indirectness as the results are not applicable to children and due to imprecision as only a single study with a small sample size contributed evidence and for some outcomes CIs around the result were wide (Table 2).
We have not presented other monotherapy treatments in the summary of findings tables as interventions have not been taken forward on larger more representative populations in Phase 3 studies.
Primary outcomes
1. Survival
No deaths were reported during any of the included studies (Boyle 2014; Clancy 2012; Donaldson 2014; Donaldson 2017; Horsley 2017; McCarty 2002; Rubenstein 1998; Zeitlin 2002).
2. QoL
a. Total QoL score
Data for this outcome were not reported by any study (Boyle 2014; Clancy 2012; Donaldson 2014; Donaldson 2017; Horsley 2017; McCarty 2002; Rubenstein 1998; Zeitlin 2002).
b. Different sub‐domains
i. Immediate term (up to and including one month)
Lumacaftor versus placebo
The study by Clancy (n = 89) reported on the change from baseline scores for all CFQ‐R domains at 28 days (Table 10). We have presented these absolute change from baseline scores as we were unable to calculate the relative change from baseline in CFQ‐R scores since baseline CFQ‐R scores were not reported. Furthermore, no SDs or CIs were reported to allow calculation of SDs for entry into the analysis (Clancy 2012).
2. Change from baseline CFQ‐R domain scores at 28 days (Clancy 2012).
| Lumacaftor | Placebo | ||||
| Domain | 25 mg (n = 17) | 50 mg (n = 17) | 100 mg (n = 16) | 200 mg (n =18) | (n = 17) |
| Body | ‐0.21 | ‐1.63 | 2.61 | 0.06 | ‐1.34 |
| Digestion | 2.28 | ‐0.72 | 0.25 | 2.58 | 4.62 |
| Eating | ‐3.66 | ‐7.27* | 3.24 | ‐2.58 | 2.11 |
| Emotion | ‐3.22 | ‐1.36 | 3.49 | ‐2.62 | 4.86 |
| Health Perceptions | ‐2.84 | ‐6.97* | ‐0.44 | ‐1.9 | 5.03 |
| Physical | ‐5.97 | ‐7.38* | ‐3.46 | ‐0.98 | 1.23 |
| Respiratory | ‐5.22 | ‐6.32* | ‐1.29 | 2.22 | 4.53 |
| Role | ‐5.94* | ‐4.6 | 1.1 | ‐6.53* | 2.21 |
| Social | 0 | ‐1.01 | 0.47 | ‐2.64 | ‐0.55 |
| Treatment Burden | 4.19 | ‐5.96* | 1.42 | ‐0.68 | 2.46 |
| Vitality | ‐4.65 | ‐7.23* | ‐1.52 | 0.73 | ‐2.18 |
| Weight | 5.41 | 2.18 | 8.83 | ‐4.19 | 0.3 |
* significant results versus placebo are highlighted by stars
Participants in the 25 mg group reported significantly lower CFQ‐R scores for the role domain (MD ‐8.15) and respiratory domain (MD ‐9.75) compared participants in the placebo group. Participants in the 50 mg lumacaftor group reported significantly lower CFQ‐R scores for the eating domain (MD ‐9.4), health perceptions domain (MD ‐12.0), respiratory domain (MD ‐10.85) and treatment burden domain (MD ‐8.42) compared to participants assigned to placebo. Participants in the 200 mg group reported significantly lower CFQ‐R scores for the role domain (P < 0.05) compared participants in the placebo group (Clancy 2012).
Cavosonstat versus placebo
Donaldson (n = 51) also reported data for both the respiratory and eating domains of the CFQ‐R at 28 days, but neither result showed any difference between cavosonstat and placebo groups at up to one month (Analysis 2.1; Analysis 2.2) (Donaldson 2017).
2.1. Analysis.

Comparison 2: Cavosonstat (N91115) (200 mg twice daily) versus placebo, Outcome 1: CFQR respiratory domain: absolute change from baseline
2.2. Analysis.

Comparison 2: Cavosonstat (N91115) (200 mg twice daily) versus placebo, Outcome 2: CFQR eating domain: absolute change from baseline
FDL169 versus placebo
Horsley reported the change from baseline at up to one month for the CFQ‐R respiratory domain (Horsley 2017); this favoured the 400 mg group (n = 6) compared to placebo (n = 7), MD 5.09 (95% CI ‐2.72 to 12.90) (Analysis 4.1); there was no difference between the 600 mg group (n = 6) and placebo, MD ‐4.33 (95% CI ‐12.01 to 3.35) (Analysis 5.1); and favoured the 800 mg group (n = 8) over placebo, MD 8.84 (95% CI 1.40 to 16.28) (Analysis 6.1)
4.1. Analysis.

Comparison 4: FDL169 (400 mg three times daily) versus placebo, Outcome 1: Mean change in CFQ‐R respiratory domain
5.1. Analysis.

Comparison 5: FDL169 (600 mg three times daily) versus placebo, Outcome 1: Mean change in CFQ‐R respiratory domain
6.1. Analysis.

Comparison 6: FDL169 (800 mg three times daily) versus placebo, Outcome 1: Mean change in CFQ‐R respiratory domain
ii. Short term (over one month and up to and including six months)
Data for this outcome were not reported by any study (Boyle 2014; Clancy 2012; Donaldson 2014; Donaldson 2017; McCarty 2002; Rubenstein 1998; Zeitlin 2002).
3. Physiological measures of lung function
a. FEV1 (relative change from baseline)
i. Immediate term (up to and including one month)
Lumacaftor versus placebo
The study by Clancy (n = 89) reported the mean relative change from baseline in FEV1 % predicted after 28 days of treatment with escalating doses of lumacaftor, but did not present the corresponding SDs precluding analysis (Clancy 2012). No significant differences were reported between the placebo group and the different lumacaftor dose groups: 25 mg, MD ‐2.53% predicted; 50 mg, MD ‐2.22% predicted; 100 mg, MD 0.25% predicted; and 200 mg, MD 0.40% predicted. No SDs or CIs were reported to allow calculation of SDs for entry into the analysis (Clancy 2012).
Cavosonstat versus placebo
Donaldson (n = 51) presents data for cavosonstat versus placebo pictorially in the graph (supplementary tables), but overlapping SD lines render these data difficult to extract. The paper reports that no treatment‐related changes in FEV1 were seen with cavosonstat compared to placebo at up to one month (Donaldson 2017).
N6022 versus placebo
The study by Donaldson (n = 66) reported the mean relative change from baseline in FEV1 % predicted after seven days of treatment with sequential ascending doses of N6022 (5 mg, 10 mg, 20 mg or 40 mg per day) (Donaldson 2014). No significant differences were reported between the placebo group and any of the N6022 dose groups at up to one month (Analysis 3.1).
3.1. Analysis.

Comparison 3: N6022 versus placebo, Outcome 1: FEV1 % predicted (relative change from baseline at up to 1 month)
ii. Short term (over one month and up to and including six months)
Data for this outcome were not reported by any study (Boyle 2014; Clancy 2012; Donaldson 2014; Donaldson 2017; Horsley 2017; McCarty 2002; Rubenstein 1998; Zeitlin 2002).
b. FEV1 (absolute values)
i. Immediate term (up to and including one month)
Lumacaftor versus placebo
The Phase 2 study (n = 62) reported on the absolute change from baseline in FEV1 % predicted after lumacaftor monotherapy (day 14) (Boyle 2014); there was no significant difference between treatment groups at up to one month, MD ‐1.90 (95% CI ‐4.13 to 0.33) (Analysis 1.1) (moderate‐quality evidence).
1.1. Analysis.

Comparison 1: Lumacaftor versus placebo, Outcome 1: FEV1 % predicted (absolute change from baseline)
Cavosonstat versus placebo
As previously stated, Donaldson (n = 51) reported that no treatment‐related changes in FEV1 were seen with cavosonstat compared to placebo (Donaldson 2017) (low‐quality evidence).
FDL169 versus placebo
This study reported the absolute change from baseline in FEV1 % predicted at up to one month (Horsley 2017); there was a greater increase in the 400 mg (n = 6) group than placebo (n = 7), MD 4.68 (95% CI 0.12 to 9.24) (Analysis 4.2); but no difference between the 600 mg group (n = 6) and placebo, MD 2.80 (95% CI ‐1.82 to 7.42) (Analysis 5.2) or between the 800 mg group (n = 8) and placebo, MD 0.68 (95% CI ‐3.80 to 5.16) (Analysis 6.2).
4.2. Analysis.

Comparison 4: FDL169 (400 mg three times daily) versus placebo, Outcome 2: FEV1 % predicted absolute change (% points)
5.2. Analysis.

Comparison 5: FDL169 (600 mg three times daily) versus placebo, Outcome 2: FEV1 % predicted absolute change (% points)
6.2. Analysis.

Comparison 6: FDL169 (800 mg three times daily) versus placebo, Outcome 2: FEV1 % predicted absolute change (% points)
ii. Short term (over one month and up to and including six months)
Data for this outcome were not reported by any study (Boyle 2014; Clancy 2012; Donaldson 2014; Donaldson 2017; Horsley 2017; McCarty 2002; Rubenstein 1998; Zeitlin 2002).
c. FVC
Data for this outcome were not reported by seven studies (Boyle 2014; Clancy 2012; Donaldson 2014; Horsley 2017; McCarty 2002; Rubenstein 1998; Zeitlin 2002)..
i. Immediate term (up to and including one month)
Cavosonstat versus placebo
Similarly, to FEV1, Donaldson (n = 51) reported that no treatment‐related changes in FVC were seen with cavosonstat compared to placebo (Donaldson 2017).
Secondary outcomes
1. Adverse effects
Adverse effects of therapy were reported by all included studies (Boyle 2014; Clancy 2012; Donaldson 2014; Donaldson 2017; Horsley 2017; McCarty 2002; Rubenstein 1998; Zeitlin 2002). The extent and type of adverse event reporting varied between studies.
a. Mild (therapy does not need to be discontinued)
In Phase 2 trials of potential correctors (CPX, 4PBA, N6022, lumacaftor and cavosonstat), there was no evidence of a significant increase in adverse event reporting compared to placebo (Boyle 2014; Clancy 2012; Donaldson 2014; Donaldson 2017; McCarty 2002; Rubenstein 1998; Zeitlin 2002). However, a large number of events were reported and it is difficult to assess the clinical relevance of these events with the small number of participants in the trials. Further details are given below.
Lumacaftor versus placebo
Adverse events occurring in more than one participant in any lumacaftor dose treatment group in the lumacaftor study by Clancy are presented in the additional tables (Table 11) (Clancy 2012). We have combined the total number of participants with adverse events occurring in the 100 mg and 200 mg lumacaftor groups and compared this to the number of participants experiencing adverse effects in the placebo group (Analysis 1.2). Adverse event data for participants receiving a lower dose (25 or 50 mg of lumacaftor) were not included as there was no evidence of efficacy. The most commonly reported side effect was cough; there was no significant difference in the number of participants who reported cough between the participants assigned to either 100 mg or 200 mg lumacaftor and those assigned to placebo, OR 1.28 (99% CI 0.28 to 5.92) (Analysis 1.2) (Clancy 2012).
3. Frequency of adverse effects occurring in more than one participant in any VX‐809 treatment group (Clancy 2012).
|
Placebo n (%) |
Lumacaftor n (%) |
Total n (%) |
||||
| Adverse effect n (%) | (n = 17) | 25 mg (n = 18) | 50 mg (n = 18) | 100 mg (n = 17) | 200 mg (n = 18) | (n = 45)* |
| Cough | 7 (41.2) | 10 (55.6) | 6 (33.3) | 7 (41.2) | 10 (52.6) | 40 (88.9) |
| Headache | 3 (17.6) | 4 (22.2) | 5 (27.8) | 2 (11.8) | 5 (26.3) | 19 (42.2) |
| Rales | 1 (5.9) | 6 (33.3) | 2 (11.1) | 3 (17.6) | 3 (15.8) | 15 (33.3) |
| Productive cough | 3 (17.6) | 2 (11.1) | 0 (0.0) | 4 (23.5) | 6 (31.6) | 15 (17.8) |
| Dyspnoea | 1 (5.9) | 5 (27.8) | 3 (16.7) | 2 (11.8) | 4 (21.1) | 15 (33.3) |
| Pulmonary exacerbation* | 2 (11.8) | 4 (22.2) | 2 (11.1) | 2 (11.8) | 4 (21.1) | 14 (31.1) |
| Fatigue | 2 (11.8) | 3 (16.7) | 3 (16.7) | 2 (11.8) | 3 (15.8) | 13 (28.9) |
| Fever | 2 (11.8) | 2 (11.1) | 1 (5.6) | 1 (5.9) | 5 (26.3) | 11 (24.4) |
| Nasal congestion | 3 (17.6) | 2 (11.1) | 1 (5.6) | 2 (11.8) | 2 (10.5) | 10 (22.2) |
| Wheezing | 3 (17.6) | 1 (5.6) | 4 (22.2) | 1 (5.9) | 0 (0.0) | 9 (20.0) |
| Diarrhoea | 3 (17.6) | 3 (16.7) | 1 (5.6) | 2 (11.8) | 0 (0.0) | 9 (20) |
| Oropharyngeal pain | 3 (17.6) | 0 (0.0) | 3 (16.7) | 0 (0.0) | 2 (10.5) | 8 (17.8) |
| Upper respiratory tract infection | 1 (5.9) | 2 (11.1) | 1 (5.6 | 3 (17.6) | 0 (0.0) | 7 (15.6) |
| Sinus congestion | 2 (11.8) | 1 (5.6) | 2 (11.1) | 0 (0.0) | 1 (5.3) | 6 (13.3) |
| Respiration abnormal | 0 (0.0) | 1 (5.6) | 1 (5.6) | 0 (0.0) | 4 (21.1) | 6 (13.3) |
| Haemoptysis | 2 (11.8) | 1 (5.6) | 1 (5.6) | 0 (0.0) | 2 (10.5) | 6 (13.3) |
| Constipation | 0 (0.0) | 2 (11.1) | 2 (11.1) | 1 (5.9) | 1 (5.3) | 6 (13.3) |
| Abdominal pain | 1 (5.9) | 3 (16.7) | 1 (5.6) | 0 (0.0) | 1 (5.3) | 6 (13.3) |
| Myalgia | 1 (5.9) | 0 (0.0) | 3 (16.7) | 0 (0.0) | 1 (5.3) | 5 (11.1) |
| Post‐tussive vomiting | 0 (0.0) | 0 (0.0) | 2 (11.1) | 1 (5.9) | 1 (5.3) | 4 (8.9) |
| Nausea | 0 (0.0) | 3 (16.7) | 0 (0.0) | 0 (0.0) | 1 (5.3) | 4 (8.9) |
| Nasopharyngitis | 0 (0.0) | 1 (5.6) | 0 (0.0) | 1 (5.9) | 2 (10.5) | 4 (8.9) |
| Dizziness | 0 (0.0) | 1 (5.6) | 0 (0.0) | 2 (11.8) | 1 (5.3) | 4 (8.9) |
| Back pain | 0 (0.0) | 2 (11.1) | 1 (5.6) | 0 (0.0) | 1 (5.3) | 4 (8.9) |
| Abdominal pain upper | 1 (5.9) | 0 (0.0) | 0 (0.0) | 1 (5.9) | 2 (10.5) | 4 (8.9) |
| Sputum abnormal | 0 (0.0) | 2 (11.1) | 0 (0.0) | 0 (0.0) | 1 (5.3) | 3 (6.7) |
| Epistaxis | 1 (5.9) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 2 (10.5) | 3 (6.7) |
| C‐reactive protein increased | 0 (0.0) | 1 (5.6) | 0 (0.0) | 2 (11.8) | 0 (0.0) | 3 (6.7) |
| Paranasal sinus hypersecretion | 0 (0.0) | 2 (11.1) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 2 (4.4) |
| Lung hyperinflation | 0 (0.0) | 0 (0.0) | 0 (0.0) | 2 (11.8) | 0 (0.0) | 2 (4.4) |
* Unclear why the total number of participants in the study is shown to be 45. The author has been contacted for clarification.
1.2. Analysis.

Comparison 1: Lumacaftor versus placebo, Outcome 2: Adverse effects: 100 mg and 200 mg lumacaftor groups (combined data) versus placebo at up to 1 month
Data for 14 days of lumacaftor monotherapy (200 mg once daily) demonstrated no significant differences between participants treated with lumacaftor therapy and placebo in the number of participants experiencing cough, oropharyngeal pain, nasal congestion, dizziness, a prolonged prothrombin time, and upper respiratory tract infection (Analysis 1.3) (Boyle 2014) (very low‐quality evidence).
1.3. Analysis.

Comparison 1: Lumacaftor versus placebo, Outcome 3: Adverse effects: 200 mg lumacaftor group versus placebo at up to 1 month
Cavosonstat versus placebo
In the cavosonstat study, there was no significant difference in cough, pulmonary exacerbation, chest discomfort, or fatigue in the treatment group compared to placebo (Analysis 2.3) (Donaldson 2017) (very low‐quality evidence). All adverse events observed in this study were reported to be 'mild or moderate' in severity.
2.3. Analysis.

Comparison 2: Cavosonstat (N91115) (200 mg twice daily) versus placebo, Outcome 3: Adverse events occurring in > 10% of participants at up to 1 month
N6022 versus placebo
The number of Grade 1 (mild) adverse events across all N6022 doses and placebo were reported (Donaldson 2014). There was no significant difference between any of the N6022 doses and placebo in terms of the number of mild adverse events, specific events were not reported (Analysis 3.2).
3.2. Analysis.

Comparison 3: N6022 versus placebo, Outcome 2: Treatment‐emergent adverse events (mild) at up to 1 month
CPX versus placebo
Participants received a single dose of the assigned CPX dose level (1 mg, 3 mg, 10 mg, 30 mg, 100 mg, 300 mg or 1000 mg) (McCarty 2002). Adverse events were recorded on the day of dosing (day one), day two and followed up one week post‐dosing. Adverse effects that occurred in more than 3% of participants are shown in the additional tables (Table 12). Combined data from all CPX groups versus placebo demonstrated that the following events were less common in the placebo group: abdominal pain, OR 0.45 (99% CI 0.01 to 24.92); asthenia, OR 0.65 (99% CI 0.01 to 39.69); headache, OR 0.33 (99% CI 0.01 to 17.72); pain, OR 0.45 (99% CI 0.01 to 24.92); diarrhoea, OR 0.65 (99% CI 0.01 to 39.69); lung disease, OR 0.45 (99% CI 0.01 to 24.92); and rhinitis, OR 0.45 (99% CI 0.01 to 24.92) (Analysis 7.1). Dizziness was more common amongst participants in the placebo group, OR 9.33 (99% CI 0.32 to 268.92) (Analysis 7.1). The difference between CPX groups (combined data) and placebo was not significant for any adverse event (McCarty 2002).
4. Frequency of occurrence of adverse effects occurring in more than 3% of participants in any CPX treatment group in McCarty 2002.
| Placebo | CPX | |||||||
| Adverse effects, n | (n = 8) | 1 mg (n = 4) | 3 mg (n = 4) | 10 mg (n = 4) | 30 mg (n = 4) | 100 mg (n = 5) | 300 mg (n = 4) | 1000 mg (n = 4) |
| Abdominal pain | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 1 |
| Asthenia | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 |
| Headache | 0 | 0 | 0 | 2 | 1 | 0 | 1 | 0 |
| Pain | 0 | 0 | 0 | 1 | 0 | 0 | 2 | 0 |
| Diarrhoea | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 |
| Dizziness | 2 | 0 | 0 | 1 | 0 | 0 | 0 | 0 |
| Lung Disease | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 2 |
| Rhinitis | 0 | 2 | 0 | 1 | 0 | 0 | 0 | 2 |
CPX: 8‐cyclopentyl‐1, 3‐dipropylxanthine
7.1. Analysis.

Comparison 7: CPX versus placebo, Outcome 1: Adverse events occurring in more than 3% of participants in all treatment groups (combined data) versus placebo at up to 1 month
4PBA versus placebo
In the pilot 4PBA study (n = 18) (Rubenstein 1998), the differences between groups in the number of participants who reported episodes of bad taste in their mouth and diarrhoea were not significant, OR 0.44 (99% CI 0.01 to 13.44) and OR 3.35 (99% CI 0.04 to 267.31) respectively (Analysis 8.1).
8.1. Analysis.

Comparison 8: 4PBA versus placebo, Outcome 1: Adverse events at up to 1 month
In the Phase 2 4PBA study (n = 19), participants randomised to the 20 g cohort reported episodes of transient nausea, headache, sleepiness and body odour after the initial dose; the transient nausea, sleepiness and headache resolved with a dose of Tylenol® (acetominophen). No numerical data were reported regarding adverse events, therefore no data can be entered into analysis for this study (Zeitlin 2002).
b. Moderate (therapy is discontinued, and the adverse effect ceases)
None of the participants in the Phase 2 lumacaftor‐ivacaftor study, the pilot 4PBA study or the CPX study the required study drug interruption for the adverse effects of therapy (Boyle 2014; McCarty 2002; Rubenstein 1998).
Lumacaftor versus placebo
There were no significant differences in terms of any lumacaftor dose compared to placebo in the number of adverse events requiring study drug discontinuation up to day 28 (Analysis 1.4) (Clancy 2012).
1.4. Analysis.

Comparison 1: Lumacaftor versus placebo, Outcome 4: Adverse effects requiring study drug discontinuation at up to 1 month
Cavosonstat versus placebo
In the cavosonstat study, there was no significant difference in cough, pulmonary exacerbation, chest discomfort, or fatigue in the treatment group compared to placebo (Analysis 2.3) (Donaldson 2017) (very low‐quality evidence). All adverse events observed in this study were reported to be 'mild or moderate' in severity.
N6022 versus placebo
The number of Grade 2 (moderate) adverse events across all N6022 doses and placebo were reported (Donaldson 2014). There was no significant differences between any of the N6022 doses and placebo in terms of the number of Grade 2 adverse events; specific events were not reported (Analysis 3.3).
3.3. Analysis.

Comparison 3: N6022 versus placebo, Outcome 3: Treatment‐emergent adverse events (moderate) at up to 1 month
4PBA versus placebo
In the Phase 4 4PBA study, participants who were discontinued from a particular study dose were assigned a reduced dose and this is discussed under severe adverse effects (Zeitlin 2002).
c. Severe (life‐threatening or debilitating, or which persists even after treatment is discontinued)
None of the participants from the CPX study or the cavosonstat study required study drug termination (Rubenstein 1998; Donaldson 2017).
Lumacaftor versus placebo
In the Clancy study, adverse events in eight participants were considered severe: fatigue (n = 1); sinus congestion (n = 1); musculoskeletal discomfort (n = 1); cough (n = 2); and pulmonary exacerbation (n = 3). It is not stated which arm these participants were randomised to. Four out of 89 participants (5%) ‐ one participant from each of the lumacaftor arms ‐ discontinued the study drug due to respiratory adverse effects. No participants discontinued from the placebo group (Clancy 2012).
N6022 versus placebo
The number of Grade 3 or above (serious or life‐threatening) adverse events across all N6022 doses and placebo were reported (Donaldson 2014). There was no significant differences between any of the N6022 doses and placebo in terms of the number of Grade 3 or above adverse events (Analysis 3.4). The events were as follows: one participant with appendicitis in the 5 mg/day N6022 group and three participants with a pulmonary exacerbation of CF one each in the placebo, 5 mg/day and 40 mg/day N6022 groups.
3.4. Analysis.

Comparison 3: N6022 versus placebo, Outcome 4: Treatment‐emergent adverse events (serious or severe) at up to 1 month
4PBA versus placebo
None of the participants from the pilot 4PBA study required study drug termination (McCarty 2002). In the Phase 2 4PBA study, none of the participants in the 20 g group required study drug termination (Zeitlin 2002). "Several" participants (exact number not stated) in the 30 g group reported episodes of transient nausea, headache, sleepiness and transient visual disturbances after the initial dose. Two participants from the 30 g cohort required dose reduction to 20 g due to headache (n = 1) and for an unknown reason (n = 1). One participant who started in this group had to discontinue medication after developing acute distal intestinal obstruction syndrome on day two, but was replaced by another participant. The three participants assigned 40 g of 4PBA reported episodes of nausea, headache and visual disturbances and one participant reported cramp in hands and fingers. One participant tolerated the dose whilst splitting the 40 g into six daily doses, one participant had a dose reduction to 30 g daily and another participant in this group was discontinued from the study due to intolerable symptoms (nausea, headache and visual disturbances). The 40 g cohort was terminated early following analysis of the data by the safety monitoring committee (Zeitlin 2002).
d. Other adverse effects of therapy (of any severity) that are not classifiable according to these categories
Lumacaftor versus placebo
Two studies also reported on the number of participants who experienced episodes of pulmonary exacerbations described as adverse events (Boyle 2014; Clancy 2012). Results are presented in the analyses and described below (see 'Extra courses of antibiotics') (Analysis 1.2; Analysis 1.3).
N6022 versus placebo
Donaldson reported on "none serious" adverse events on each dose of N6022 and placebo (Donaldson 2014). Due to the small numbers of participants experiencing different adverse events, these results are not entered into analysis and are reported in the additional tables (Table 13).
5. Adverse events (non‐serious) reported in Donaldson 2014 (N6022 versus placebo).
| Placebo | N6022 | Total | ||||
| Adverse events, n | (n = 19) | 5 mg (n = 10) | 10 mg (n = 9) | 20 mg (n = 9) | 40 mg (n = 19) | (n = 66) |
| Lymphadenopathy | 1 | 0 | 0 | 0 | 0 | 1 |
| Chest tightness | 1 | 2 | 0 | 0 | 2 | 5 |
| Atrioventricular block second degree | 0 | 0 | 1 | 0 | 0 | 1 |
| Nodal rhythm | 0 | 0 | 0 | 1 | 0 | 1 |
| Supraventricular extrasystoles | 0 | 0 | 0 | 1 | 0 | 1 |
| Supraventricular tachycardia | 0 | 0 | 1 | 0 | 0 | 1 |
| Ventricular extrasystoles | 1 | 0 | 0 | 0 | 0 | 1 |
| Ventricular tachycardia | 0 | 0 | 0 | 1 | 0 | 1 |
| Diarrhoea | 2 | 0 | 1 | 0 | 0 | 3 |
| Nausea | 1 | 1 | 0 | 0 | 1 | 3 |
| Vomiting | 0 | 0 | 0 | 0 | 2 | 2 |
| Flatulence | 0 | 0 | 1 | 0 | 0 | 1 |
| Parosmia | 0 | 0 | 0 | 2 | 0 | 2 |
| Night sweats | 0 | 0 | 2 | 0 | 0 | 2 |
| Fatigue | 1 | 1 | 0 | 0 | 2 | 4 |
| Pyrexia | 0 | 1 | 0 | 0 | 2 | 3 |
| Infective pulmonary exacerbations of CF | 1 | 1 | 0 | 0 | 1 | 3 |
| Upper respiratory tract infection | 1 | 0 | 0 | 0 | 0 | 1 |
| Headache | 1 | 1 | 1 | 2 | 1 | 6 |
| Cough | 7 | 3 | 1 | 3 | 2 | 16 |
| Increased bronchial secretion | 3 | 2 | 2 | 2 | 1 | 10 |
| Nasal congestion | 1 | 3 | 0 | 0 | 1 | 5 |
| Rales | 0 | 3 | 0 | 1 | 0 | 4 |
| Total participants with at least one adverse event, n (%) |
18 (95%) | 9 (90%) | 9 (100%) | 9 (100%) | 15 (79%) | 60 (91%) |
CF: cystic fibrosis
FDL169 versus placebo
Horsley reported the number of participants experiencing at least one adverse event, and the number of 'serious' adverse events, AEs were not categorised under mild, moderate or severe (Horsley 2017). No significant difference was found in the number of participants experiencing at least one adverse event between any tested dose level of FDL169 and placebo (n = 7); for the 400 mg group (n = 6), OR 6.67 (99% CI 0.21 to 207.87) (Analysis 4.3); for the 600 mg group (n = 6), OR 0.06 (99% CI 0.00 to 4.00) (Analysis 5.3); and for the 800 mg group (n = 8), OR 21.86 (99% CI 0.34 to 1419.86) (Analysis 6.3). Similarly, there was no statistical difference observed in the occurrence of any particular adverse event or of serious adverse events (Analysis 4.3; Analysis 5.3; Analysis 6.3).
4.3. Analysis.

Comparison 4: FDL169 (400 mg three times daily) versus placebo, Outcome 3: Adverse events at up to 1 month
5.3. Analysis.

Comparison 5: FDL169 (600 mg three times daily) versus placebo, Outcome 3: Adverse events at up to 1 month
6.3. Analysis.

Comparison 6: FDL169 (800 mg three times daily) versus placebo, Outcome 3: Adverse events at up to 1 month
2. Hospitalisation
Data for this outcome were not reported by any study (Boyle 2014; Clancy 2012; Donaldson 2014; Donaldson 2017; Horsley 2017; McCarty 2002; Rubenstein 1998; Zeitlin 2002).
3. School or work attendance
Data for this outcome were not reported by any study (Boyle 2014; Clancy 2012; Donaldson 2014; Donaldson 2017; Horsley 2017; McCarty 2002; Rubenstein 1998; Zeitlin 2002).
4. Extra courses of antibiotics
a. Time‐to the next course of antibiotics
Data for this outcome were not reported by any study (Boyle 2014; Clancy 2012; Donaldson 2014; Donaldson 2017; Horsley 2017; McCarty 2002; Rubenstein 1998; Zeitlin 2002).
b. Total number of courses of antibiotics
i. Immediate term (up to and including one month)
Lumacaftor versus placebo
In the lumacaftor study (n = 89), pulmonary exacerbations were physician‐defined and there was no significant difference in the frequency of participants who developed pulmonary exacerbations between those in the lumacaftor groups and the placebo group, OR 1.50 (99% CI 0.16 to 14.31) (Analysis 1.2) (Clancy 2012).
In the Boyle study (n = 62), it was unclear whether the reported exacerbations were protocol‐defined or physician‐defined. At day 14, exacerbations were more common in participants receiving 200 mg lumacaftor once daily in comparison to participants receiving placebo, OR 2.72 (99% CI 0.05 to 156.17) (Analysis 1.3). However, the difference between groups was not significant (Boyle 2014).
FDL169 versus placebo
From the published abstract for this Phase 1 study, it is unclear whether exacerbations were physician‐ or protocol‐defined. A total of three participants across all groups were reported to have had an infective respiratory exacerbation; no participants in the 400 mg group (n = 6), one participant in the 600 mg group (n = 6), one participant in the 800 mg (n = 8) and one participant in the placebo group (n = 7) (Horsley 2017).
5. Sweat chloride (change from baseline) as a measure of CFTR function
All included studies reported on sweat chloride concentration (Boyle 2014; Clancy 2012; Donaldson 2014; Donaldson 2017; Horsley 2017; McCarty 2002; Rubenstein 1998; Zeitlin 2002).
i. Immediate (up to one month)
Lumacaftor versus placebo
In the Clancy study (n = 89), data at seven days demonstrated small reductions in the change from baseline in sweat chloride concentration compared to placebo for the participants taking 25 mg lumacaftor, MD 1.7 mmol/L; 50 mg lumacaftor, MD ‐1.5 mmol/L; 100 mg lumacaftor, MD ‐0.1mmol/L; and 200 mg lumacaftor, MD ‐4.4 mmol/L (Clancy 2012). No SDs or CIs were reported to allow the inclusion of these results into the analysis (Clancy 2012). At 28 days, participants in the 25 mg lumacaftor group demonstrated a marginal increase in sweat chloride concentration compared to placebo, MD 0.1 mmol/L and those in the 50 mg lumacaftor group demonstrated a decreased sweat chloride concentration compared to placebo, MD ‐4.61 mmol/L (Clancy 2012). These differences were not significant and no SDs or CIs were reported for inclusion of these results into the analysis (Clancy 2012). Data at one month demonstrated significant reductions in sweat chloride concentration compared to placebo for participants in the once daily 100 mg lumacaftor group, MD ‐6.13 mmol/L (95% CI ‐12.25 to ‐0.01) and once daily 200 mg lumacaftor group, MD ‐8.21 (95% CI ‐14.30 to ‐2.12) (Analysis 1.5) (Clancy 2012).
1.5. Analysis.

Comparison 1: Lumacaftor versus placebo, Outcome 5: Sweat chloride concentration (change from baseline at up to 1 month) [mmol/L]
Boyle reported that at day 14, there was a small reduction in sweat chloride concentration reported in participants taking 200 mg lumacaftor once daily compared to placebo, MD ‐2.75 mmol/L (95% CI ‐7.65 to 2.15) which was not significant (Analysis 1.6) (Boyle 2014). Results for up to 21 days (monotherapy and combination therapy) are reported above (see 'Correctors plus potentiators in combination therapy compared to placebo').
1.6. Analysis.

Comparison 1: Lumacaftor versus placebo, Outcome 6: Sweat chloride concentration (change from baseline)
Cavosonstat versus placebo
There was no significant difference in sweat chloride concentration between cavosonstat and placebo at up to one month (n = 51), MD ‐3.30 mmol/L (95% CI ‐9.13 to 2.53) (Analysis 2.4) (Donaldson 2017).
2.4. Analysis.

Comparison 2: Cavosonstat (N91115) (200 mg twice daily) versus placebo, Outcome 4: Sweat chloride
CPX versus placebo
In the CPX study (n = 37), McCarty reported post‐treatment sweat chloride concentration values at the end of treatment on day one (McCarty 2002). The baseline sweat chloride values in the CPX group and the placebo group appear to have been pooled. By calculating the values for relative change from baseline, we have assumed that the baseline sweat chloride value represents the baseline sweat chloride concentration value for each arm. At the end of treatment on day one, there were no significant differences in sweat chloride concentration between the placebo group and the 1 mg CPX group, MD 12.8%; the 3 mg CPX group, MD 7.5%; the 10 CPX mg group, MD 11.3%; the 30 CPX mg group, MD 5.4%; the 100 CPX mg group, MD 5.1%; the 300 CPX mg group, MD 14.7%; and the 1000 CPX mg group, MD ‐8.2%. No SDs or CIs were reported to allow calculation of SDs for entry into the analysis (McCarty 2002).
4BPA versus placebo
In the pilot 4PBA study by Rubenstein (n = 18), there was no significant difference in sweat chloride concentration at one week between participants in the 4PBA group and the placebo group (P = 0.387). Data were plotted on a graph and could not be extracted with accuracy (Rubenstein 1998).
The Phase 2 4PBA study by Zeitlin reported post‐treatment sweat chloride concentration values at day two, day three, day four and day seven; we calculated the relative change from baseline values at each time‐point. There was no significant difference in sweat chloride concentration between the 20 g 4PBA group and the placebo group after two days of treatment, MD ‐7.8%; three days, MD ‐4.9%; four days, MD ‐3.3% and seven days, MD ‐8.7%. Furthermore, there was no significant difference in sweat chloride concentration between the 30 g 4PBA group and the placebo group after two days of treatment, MD ‐25.9%; three days, MD 0.5%; four days, MD ‐6.4% and seven days, MD ‐3.9% (Zeitlin 2002). No SDs or CIs were reported to allow calculation of SDs for entry into the analysis. Due to insufficient reporting of data by both 4PBA studies, we were unable to include the results in the analysis (Rubenstein 1998; Zeitlin 2002).
FDL169 versus placebo
Horsley reported the absolute change in sweat chloride (mmol/L) at 28 days (Horsley 2017). There was no difference between the 400 mg group (n = 6) and placebo (n = 7), MD 2.47 (95% CI ‐4.47 to 9.41) (Analysis 4.4) or between the 800 mg group (n = 8) and placebo, MD 3.48 (95% CI ‐3.35 to 10.31) (Analysis 6.4), but there was a greater drop in sweat chloride in the placebo group than the 600 mg group (n = 6), MD 8.07 (95% CI 0.98 to 15.16) (Analysis 5.4).
4.4. Analysis.

Comparison 4: FDL169 (400 mg three times daily) versus placebo, Outcome 4: Sweat chloride change from baseline [mmol/L]
6.4. Analysis.

Comparison 6: FDL169 (800 mg three times daily) versus placebo, Outcome 4: Sweat chloride change from baseline [mmol/L]
5.4. Analysis.

Comparison 5: FDL169 (600 mg three times daily) versus placebo, Outcome 4: Sweat chloride change from baseline [mmol/L]
6. Radiological measures of lung disease
Data for this outcome were not reported by any study (Boyle 2014; Clancy 2012; Donaldson 2014; Donaldson 2017; Horsley 2017; McCarty 2002; Rubenstein 1998; Zeitlin 2002).
7. Acquisition of respiratory pathogens
Data for the acquisition of S aureus, H influenzae or any other clinically relevant pathogens except P aeruginosa, were not reported by any study (Boyle 2014; Clancy 2012; Donaldson 2014; Donaldson 2017; Horsley 2017; McCarty 2002; Rubenstein 1998; Zeitlin 2002).
a. P aeruginosa
This was a pre‐defined outcome of interest in the Phase 1/2 4PBA study, but no study results were reported (Zeitlin 2002). Data for this outcome were not reported the other studies (Boyle 2014; Clancy 2012; Donaldson 2014; Donaldson 2017; Horsley 2017; McCarty 2002; Rubenstein 1998).
8. Eradication of respiratory pathogens
Data for this outcome were not reported by any study (Boyle 2014; Clancy 2012; Donaldson 2014; Donaldson 2017; Horsley 2017McCarty 2002; Rubenstein 1998; Zeitlin 2002).
9. Nutrition and growth
No data for this outcome, either in terms of weight, BMI or height, were reported by any study (Boyle 2014; Clancy 2012; Donaldson 2014; Donaldson 2017; Horsley 2017; McCarty 2002; Rubenstein 1998; Zeitlin 2002).
Dual therapy (correctors plus potentiators) compared to control
Six studies with 1902 participants contributed to the efficacy results in this comparison (of which 62 also contributed to the monotherapy comparison) (Boyle 2014; Donaldson 2018; Ratjen 2017; Taylor‐Cousar 2017; TRAFFIC 2015; TRANSPORT 2015). A further study contributed additional safety data to this comparison (see below) (PROGRESS 2017).
Four studies with 1374 participants compared lumacaftor plus ivacaftor to placebo (Boyle 2014; Ratjen 2017; TRAFFIC 2015; TRANSPORT 2015) and two studies with 528 participants compared tezacaftor plus ivacaftor to placebo or to ivacaftor alone (i.e. ivacaftor as placebo) (Donaldson 2018; Taylor‐Cousar 2017).
Two three‐arm studies (n = 1108) compared 600 mg once daily lumacaftor plus 250 mg twice daily ivacaftor to 400 mg twice daily lumacaftor plus 250 mg twice daily ivacaftor and to placebo (TRAFFIC 2015; TRANSPORT 2015). One study (n = 62) compared lumacaftor 200 mg once daily plus 150 mg or 250 mg twice daily ivacaftor to placebo (Boyle 2014). Participants in this study received lumacaftor monotherapy for 14 days followed by combination therapy with ivacaftor for seven days, therefore this study contributes to both comparisons of this review (Boyle 2014).
The paediatric combination study (n = 204) compared 200 mg lumacaftor twice daily plus 250mg ivacaftor twice daily to placebo for six months (Ratjen 2017). Primary and secondary outcomes of this study were analysed via a mixed model for repeated measures (MMRM), further details of this analysis approach are provided in the tables (Characteristics of included studies). Results provided by this model can be interpreted as treatment effect averaged from each study visit until six months.
The PROGRESS study was an extension to the TRAFFIC and TRANSPORT studies (TRAFFIC 2015; TRANSPORT 2015), in which participants from the original placebo groups were randomised to one of the two interventions (PROGRESS 2017). Due to the overlap of participants in these three studies, we have not included efficacy data for the PROGRESS study under a comparison of lumacaftor (plus ivacaftor) doses. We have included safety data from this study as these are important longer‐term results for participants on this intervention; results for the PROGRESS study are presented in the tables for information (PROGRESS 2017; Table 14; Table 15).
6. Adverse events with an incidence of ≥ 0.20 events per patient‐year in Konstan 2017.
| Event | Lumacaftor 400 mg twice daily/ivacaftor 250 twice daily (n = 340) | Placebo transitioned to lumacaftor 400 mg twice daily/ivacaftor 250 mg twice daily (n = 176) | Lumacaftor 600 mg once daily/ivacaftor 250 mg twice daily (n = 335) | Placebo transitioned to lumacaftor 600 mg once daily/ ivacaftor 250 mg twice daily (n = 178) |
| Total exposure in patient‐years | 570 | 290 | 570 | 300 |
| Infective pulmonary exacerbation | 0.980 | 1.035 | 1.157 | 1.080 |
| Cough | 0.510 | 0.573 | 0.627 | 0.609 |
| Haemoptysis | 0.266 | 0.200 | 0.235 | 0.239 |
| Increased sputum | 0.208 | 0.207 | 0.224 | 0.175 |
| Nasopharyngitis | 0.194 | 0.169 | Not reported | Not reported |
| Headache | 0.140 | 0.107 | 0.129 | 0.101 |
| Dyspnoea | 0.124 | 0.166 | 0.117 | 0.128 |
| Pyrexia | 0.114 | 0.152 | 0.148 | 0.148 |
| Upper respiratory tract infection | 0.129 | 0.131 | Not reported | Not reported |
| Diarrhoea | 0.093 | 0.145 | 0.111 | 0.101 |
| Abnormal respiration | 0.077 | 0.128 | 0.088 | 0.145 |
| Nausea | 0.072 | 0.104 | Not reported | Not reported |
| Fatigue | 0.084 | 0.090 | Not reported | Not reported |
| Abdominal pain | 0.087 | 0.066 | 0.087 | 0.084 |
| Oropharyngeal pain | Not reported | Not reported | 0.101 | 0.081 |
| Nasal congestion | Not reported | Not reported | 0.104 | 0.091 |
| Rhinitis | Not reported | Not reported | 0.064 | 0.030 |
| Any adverse event: n (%) | 333 (97.9) | 176 (100) | 331 (98.8) | 177 (99.4) |
| Any serious adverse event: n (%) | 143 (42.1) | 89 (50.6) | 156 (46.6) | 77 (43.3) |
| Any treatment emergent respiratory event: n (%) | 99 (29) | 67 (38) | 102 (30) | 67 (38) |
7. Secondary efficacy outcomes reported in Konstan 2017.
| Outcome | Lumacaftor 400 mg twice daily/ivacaftor 250 mg twice daily (n = 340) | Placebo transitioned to lumacaftor 400 mg twice daily/ivacaftor 250 mg twice daily (n = 176) | Lumacaftor 600 mg once daily/ivacaftor 250 mg twice daily (n = 335) | Placebo transitioned to lumacaftor 600 mg once daily/ivacaftor 250 mg twice daily (n = 178) |
| FEV1 (% predicted):1 Week 72 |
0.5 (95% CI –0.4 to 1.5) P = 0.2806 |
1.5 (95% CI 0.2, 2.9) P = 0.0254 |
1.2 (95% CI 0.3 to 2.2) P = 0.0127 |
1.9 (95% CI 0.6 to 3.2) P = 0.0037 |
| FEV1 (% predicted): 1 Week 96 |
0.5 (95% CI –0.7 to 1.6) P = 0.4231 |
0.8 (95% CI –0.8, 2.3) P = 0.3495 |
0.0 (95% CI ‐1.1 to 1.1) P = 0.9682 |
1.6 (95% CI ‐0.1 to 3.2) P = 0.0632 |
| FEV1 (% predicted):2 Week 72 |
0.9 (95% CI 0.0 to 1.9) P = 0.0500 |
1.9 (95% CI 0.6 to 3.2) P = 0.0040 |
1.7 (95% CI 0.8 to 2.7) P = 0.0003 |
2.2 (95% CI 1.0 to 3.5) P = 0.0005 |
| FEV1 (% predicted):2 Week 96 |
1.1 (95% CI 0.0 to 2.2) P = 0.0535 |
1.1 (95% CI –0.5 to 2.6) P = 0.1696 |
0.7 (95% CI ‐0.4 to 1.8) P = 0.1966 |
2.0 (95% CI 0.4 to 3.6) P = 0.0149 |
| FEV1 (% predicted): 1 Relative change Week 72 |
1.4 (95% CI –0.3 to 3.2) P = 0.1074 |
2.6 (95% CI 0.2 to 5.0) P = 0.0332 |
2.4 (95% CI 0.6 to 4.1) P = 0.0080 |
3.8 (95% CI 1.4 to 6.1) P = 0.0017 |
| FEV1 (% predicted): 1 Relative change Week 96 |
1.2 (95% CI –0·8 to 3·3) P = 0·2372 |
1·1 (95% CI –1·7 to 3·9) P = 0·4415 |
0.1 (95% CI ‐1.9 to 2.1) P = 0.9297 |
3.6 (95% CI 0.6 to 6.6) P = 0.0172 |
| BMI Week 72 |
0.69 (95% CI 0.56 to 0.81) P < 0.0001 |
0.62 (95% CI 0.45 to 0.79) P < 0.0001 |
0.72 (95% CI 0.60 to 0.84) P < 0.0001 |
0.52 (95% CI 0.36 to 0.69) P < 0.0001 |
| BMI Week 96 |
0.96 (95% CI 0.81 to 1.11) P < 0.0001 |
0.76 (95% CI 0.56 to 0.97) P < 0.0001 |
0.81 (95% CI 0.66 to 0.95) P < 0.0001 |
0.55 (95% CI 0.34 to 0.76) P < 0.0001 |
| CFQ‐R respiratory domain Week 72 |
5.7 (95% CI 3.8 to 7.5) P < 0.0001 |
3.3 (95% CI 0.7 to 5.9) P = 0.0124 |
3.2 (95% CI 1.4 to 5.1) P = 0.0007 |
3.3 (95% CI 0.7 to 5.8) P = 0.0116 |
| CFQ‐R respiratory domain Week 96 |
3.5 (95% CI 1.3 to 5.8) P = 0·0018 |
0.5 (95% CI –2.7 to 3.6) P = 0·7665 |
1.1 (95% CI ‐1.1 to 3.2) P = 0.3339 |
2.0 (95% CI ‐1.1 to 5.1) P = 0.2033 |
| Pulmonary exacerbations: events per patient year |
0.65 (95% CI 0.56 to 0.75) | 0.69 (95% CI 0·56 to 0.85) | 0.80 (95% CI 0.70 to 0.92) | 0.76 (95% CI 0.62 to 0.93) |
| Pulmonary exacerbations: events requiring hospital admission per patient year |
0.24 (95% CI 0.19 to 0.29) | 0.30 (95% CI 0.22 to 0.40) | 0.31 (95% CI 0.25 to 0.38) | 0.35 (95% CI 0.26 to 0.47) |
| Pulmonary exacerbations: events requiring IV antibiotics per patient year |
0.32 (95% CI 0.26 to 0.38) | 0.37 (95% CI 0.29 to 0.49) | 0.38 (95% CI 0.32 to 0.46) | 0.42 (95% CI 0.33 to 0.54) |
BMI: body mass index CFQ‐R: cystic fibrosis questionnaire‐revised CI: confidence interval FEV1: forced expiratory volume at one second IV: intravenous
Unless otherwise stated, all outcomes reported are the mean (95% CI) absolute change from baseline. P values correspond to the within‐group change compared to baseline.
1. Calculated using Wang‐Hankinson equations. 2. Calculated using Global Lungs Initiative equations.
One study (n = 510) compared a combination of tezacaftor 100 mg plus ivacaftor 150 mg every 12 hours to a matched placebo for six months (Taylor‐Cousar 2017) and one study compared tezacaftor (100 mg per day) plus ivacaftor (150 mg twice daily) against placebo (150 mg twice daily ivacaftor alone) in people with one F508del mutation and one G551D mutation (Donaldson 2018).
With regards to pulmonary exacerbations, please see our definition above (Types of outcome measures). For this comparison, two studies defined exacerbations as episodes requiring antibiotics or hospitalisation (TRAFFIC 2015; TRANSPORT 2015), for one study, exacerbations were physician‐defined (Boyle 2014) and for four studies, it is unclear whether exacerbations are protocol‐ or physician‐defined (Donaldson 2018; PROGRESS 2017; Ratjen 2017; Taylor‐Cousar 2017).
We have not combined data from studies evaluating distinct agents or combination of agents, as they have different mechanisms of actions. For each separate comparison we have assessed the following outcomes using the GRADE criteria, presented these gradings in individual tables and indicated our findings in the relevant text below.
survival;
QoL (total score);
QoL (respiratory domain);
FEV1 % predicted (relative and absolute change);
adverse events; and
time to first pulmonary exacerbation.
For the comparison of lumacaftor (600 mg once daily or 400 mg once daily) plus ivacaftor (250 mg twice daily) versus placebo reporting short‐term results (one month to six months), we judged the quality of the evidence to be high to moderate quality; evidence was downgraded due to risk of bias from selective reporting where data contributing to analyses were extrapolated from published graphs or estimated (Table 3).
For the comparison of lumacaftor (200 mg twice daily) and ivacaftor (250 mg twice daily) versus placebo reporting immediate‐term results (up to one month) we judged the quality of the evidence to be moderate to low quality; evidence was downgraded due to risk of bias from selective reporting where data contributing to analyses were extrapolated from published graphs or estimated, due to indirectness as results are applicable only to children between the ages of 6 to 11 years and due to imprecision where few events occurred and CIs around the result were very wide (Table 4).
For the comparison of lumacaftor (200 mg) plus ivacaftor (150 mg or 250 mg twice daily) versus placebo reporting immediate‐term results (up to one month) we judged the quality of the evidence to be moderate to low quality; evidence was downgraded due to indirectness related to the design of the study and due to imprecision where few events occurred and CIs around the result were very wide (Table 5).
For the comparison of tezacaftor (100 mg once daily) and ivacaftor (150 mg twice daily) versus placebo or ivacaftor (150 mg twice daily alone) we judged the quality of the evidence to be moderate quality; evidence was downgraded due to indirectness as results are not applicable to children under the age of 12 and some results are not applicable to individuals homozygous for F508del (Table 6).
Primary outcomes
1. Survival
No deaths were reported during any of the included studies (Boyle 2014; Donaldson 2018; Ratjen 2017; Taylor‐Cousar 2017; TRAFFIC 2015; TRANSPORT 2015) (high to moderate‐quality evidence).
2. QoL
Five studies reported on QoL (Donaldson 2018; Ratjen 2017; Taylor‐Cousar 2017; TRAFFIC 2015; TRANSPORT 2015).
a. Total QoL score
ii. Short term (over one month and up to and including six months)
Lumacaftor plus ivacaftor versus placebo
Two studies reported QoL according to the Euro Quality of Life Scale (EuroQol) 5‐Dimension‐3 Level (EQ‐5D‐3L) Index Score at six months (TRAFFIC 2015; TRANSPORT 2015). This information was not reported in the primary journal article, but is available from the study record on ClinicalTrials.gov (TRAFFIC 2015; TRANSPORT 2015).
There was no significant improvement in the absolute change from baseline of EQ‐5D‐3L index score between the lumacaftor 600 mg once daily plus 250 mg ivacaftor twice daily group and placebo group, MD 0.00 (95% CI ‐0.01 to 0.02) (Analysis 9.1), or the lumacaftor 400 mg twice daily plus 250 mg ivacaftor twice daily group and placebo group, MD 0.00 (95% CI ‐0.01 to 0.02) (Analysis 10.1), or when the two lumacaftor doses were pooled at six months, MD 0.00 (95% CI ‐0.01 to 0.01) (Analysis 11.1) (high‐quality evidence).
9.1. Analysis.

Comparison 9: Lumacaftor (600 mg once daily) plus ivacaftor (250 mg twice daily) versus placebo, Outcome 1: Quality of life ‐ Euro Quality of Life Scale (EuroQol) 5‐Dimension‐3 Level (EQ‐5D‐3L) Index Score (absolute change from baseline)
10.1. Analysis.

Comparison 10: Lumacaftor (400 mg twice daily) plus ivacaftor (250 mg twice daily) versus placebo, Outcome 1: Quality of life ‐ Euro Quality of Life Scale (EuroQol) 5‐Dimension‐3 Level (EQ‐5D‐3L) Index Score (absolute change from baseline)
11.1. Analysis.

Comparison 11: Lumacaftor (600 mg once daily or 400 mg twice daily) plus ivacaftor (250 mg twice daily) versus placebo, Outcome 1: Quality of life ‐ Euro Quality of Life Scale (EuroQol) 5‐Dimension‐3 Level (EQ‐5D‐3L) Index Score (absolute change from baseline)
b. QoL sub‐domains
i. Immediate term (up to and including one month)
Lumacaftor plus ivacaftor versus placebo
In the TRAFFIC and TRANSPORT studies (n = 1108), at 28 days participants in the both the lumacaftor 600 mg once daily plus 250 mg ivacaftor twice daily group and the lumacaftor 400 mg twice daily plus 250 mg ivacaftor twice daily group experienced significantly higher absolute changes from baseline in the CFQ‐R respiratory domain compared to the placebo group, MD 3.32 (95% CI 1.13 to 5.51) (Analysis 9.2) and MD 4.13 (95% CI 1.94 to 6.31) (Analysis 10.2), respectively (TRAFFIC 2015; TRANSPORT 2015). There was also a significantly higher absolute change from baseline in the CFQ‐R respiratory domain compared to the placebo group when the two lumacaftor doses were pooled, MD 3.70 (95% CI 1.81 to 5.58) (Analysis 11.2).
9.2. Analysis.

Comparison 9: Lumacaftor (600 mg once daily) plus ivacaftor (250 mg twice daily) versus placebo, Outcome 2: Quality of life ‐ CFQ‐R respiratory domain (absolute change from baseline)
10.2. Analysis.

Comparison 10: Lumacaftor (400 mg twice daily) plus ivacaftor (250 mg twice daily) versus placebo, Outcome 2: Quality of life ‐ CFQ‐R respiratory domain (absolute change from baseline)
11.2. Analysis.

Comparison 11: Lumacaftor (600 mg once daily or 400 mg twice daily) plus ivacaftor (250 mg twice daily) versus placebo, Outcome 2: Quality of life ‐ CFQ‐R respiratory domain (absolute change from baseline)
Tezacaftor plus ivacaftor versus control
Taylor‐Cousar (n = 510) reported on the CFQ‐R respiratory domain at up to one month (Taylor‐Cousar 2017) and found a significant difference in favour of the treatment group, MD 5.10 (95% CI 2.99 to 7.21) (Analysis 16.1).
16.1. Analysis.

Comparison 16: Tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus either placebo or ivacaftor (150 mg twice daily) alone, Outcome 1: CFQ‐R respiratory domain (absolute change from baseline)
Donaldson (n= 18) presents the within‐group change from baseline to Day 28 for the CFQ‐R respiratory domain and at the end of the study the difference in treatment effect between tezacaftor‐ivacaftor and placebo was 6.81 points (P = 0.2451) (Donaldson 2018). These data were extrapolated and we have requested confirmation of the exact data from the study investigators. Any unpublished information we receive will be included in a future update.
ii. Short term (over one month and up to and including six months)
Lumacaftor plus ivacaftor versus placebo
In the two studies (n = 1108) (TRAFFIC 2015; TRANSPORT 2015), the significant difference in the absolute change from baseline in the CFQ‐R respiratory domain was maintained to six months in the 600 mg lumacaftor group compared to placebo, MD 3.04 (95% CI 0.76 to 5.32) (Analysis 9.2), but not in the 400 mg lumacaftor group compared to placebo, MD 2.18 (95% CI ‐0.11 to 4.47) (Analysis 10.2). There was a significantly higher absolute change from baseline in the CFQ‐R respiratory domain compared to the placebo group when the two lumacaftor doses were pooled, MD 2.62 (95% CI 0.64 to 4.59) (Analysis 11.2) (moderate‐quality evidence). These data were extrapolated and we have requested confirmation of the exact data from the study investigators. Any unpublished information we receive will be included in a future update.
The EQ‐5D‐3L Visual Analog Scale (VAS) domain score was also reported at six months in two studies (TRAFFIC 2015; TRANSPORT 2015). Participants in the both the lumacaftor 600 mg group and the lumacaftor 400 mg group experienced significantly higher absolute changes from baseline in the EQ‐5D‐3L VAS domain compared to the placebo group, MD 2.24 (95% CI 0.18 to 4.31) (Analysis 9.3) and MD 2.30 (95% CI 0.25 to 4.36) (Analysis 10.3) respectively. There was also a significantly higher absolute change from baseline in the EQ‐5D‐3L VAS domain compared to the placebo group when the two lumacaftor doses were pooled, MD 2.28 (95% CI 0.50 to 4.06) (Analysis 11.3). This information was not reported in the primary journal article, but is available from the study record on ClinicalTrials.gov (TRAFFIC 2015; TRANSPORT 2015). Immediate‐term data for this domain have been requested from the study investigators and any unpublished information we receive will be included in a future update.
9.3. Analysis.

Comparison 9: Lumacaftor (600 mg once daily) plus ivacaftor (250 mg twice daily) versus placebo, Outcome 3: Quality of life ‐ EQ‐5D‐3L VAS Score (absolute change from baseline)
10.3. Analysis.

Comparison 10: Lumacaftor (400 mg twice daily) plus ivacaftor (250 mg twice daily) versus placebo, Outcome 3: Quality of life ‐ EQ‐5D‐3L VAS Score (absolute change from baseline)
11.3. Analysis.

Comparison 11: Lumacaftor (600 mg once daily or 400 mg twice daily) plus ivacaftor (250 mg twice daily) versus placebo, Outcome 3: Quality of life ‐ EQ‐5D‐3L VAS Score (absolute change from baseline)
The paediatric combination study also reported the absolute change from baseline (up to and including 24 weeks) of the CFQ‐R respiratory domain (Ratjen 2017). The change within the lumacaftor plus ivacaftor group was higher compared to the placebo group, but this difference did not reach statistical significance, MD 2.50 (95% CI ‐0.10 to 5.10) (Analysis 14.1) (low‐quality evidence). Additional results at earlier time points (day 15, week 4, and week 16) were published graphically in the full study publication, but the graphical plots were too small to allow for accurate extraction of data (Ratjen 2017). Numerical data for these time points have been requested from the study investigators and any unpublished information we receive will be included in a future update.
14.1. Analysis.

Comparison 14: Lumacaftor (200 mg twice daily) plus ivacaftor (250 mg twice daily) versus placebo, Outcome 1: Quality of life ‐ CFQ‐R respiratory domain (absolute change from baseline)
Investigators in this study also list the absolute change in Treatment Satisfaction Questionnaire for Medication (TSQM) domains as a secondary outcome of the study, but results for this outcome are not presented (Ratjen 2017). Numerical data for this outcome have also been requested from the study investigators and any unpublished information we receive will be included in a future update.
Tezacaftor plus ivacaftor versus control
Taylor‐Cousar (n = 510) also reported on the CFQ‐R respiratory domain at six months (Taylor‐Cousar 2017); there was a significant difference in favour of tezacaftor‐ivacaftor, MD 5.10 (95% CI 3.20 to 7.00) (Analysis 16.1) (moderate‐quality evidence). Data from this study examining the other domains of the CFQ‐R questionnaire at six months were also identified. It was found that five out of 12 domains (including the already reported respiratory symptoms domain above) showed a significant greater improvement in the active intervention group compared to placebo: physical functioning, MD 3.80 (95% CI 1.90 to 5.70) (Analysis 16.2); treatment burden, MD 3.40 (95% CI 1.60 to 5.20) (Analysis 16.3); health perceptions, MD 3.20 (95% CI 1.20 to 5.20) (Analysis 16.4); and vitality, MD 2.30 (95% CI 0.10 to 4.50) (Analysis 16.5). The remaining seven domains did not show a significant difference between active treatment and placebo groups: social functioning, MD 1.50 (95% CI 0.00 to 3.00) (Analysis 16.6); role functioning, MD 1.50 (95% CI ‐0.30 to 3.30) (Analysis 16.7); eating problems, MD 1.10 (95% CI ‐0.60 to 2.80) (Analysis 16.8); emotional functioning, MD 0.60 (95% CI ‐1.00 to 2.20) (Analysis 16.9); weight, MD 0.50 (95% CI ‐2.90 to 3.90) (Analysis 16.10); digestive symptoms, MD ‐0.10 (95% CI ‐1.90 to 1.70) (Analysis 16.11); body image, MD ‐0.50 (95% CI ‐2.30 to 1.30) (Analysis 16.12).
16.2. Analysis.

Comparison 16: Tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus either placebo or ivacaftor (150 mg twice daily) alone, Outcome 2: CFQ‐R physical functioning domain (absolute change from baseline)
16.3. Analysis.

Comparison 16: Tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus either placebo or ivacaftor (150 mg twice daily) alone, Outcome 3: CFQ‐R treatment burden domain (absolute change from baseline)
16.4. Analysis.

Comparison 16: Tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus either placebo or ivacaftor (150 mg twice daily) alone, Outcome 4: CFQ‐R health perceptions domain (absolute change from baseline)
16.5. Analysis.

Comparison 16: Tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus either placebo or ivacaftor (150 mg twice daily) alone, Outcome 5: CFQ‐R vitality domain (absolute change from baseline)
16.6. Analysis.

Comparison 16: Tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus either placebo or ivacaftor (150 mg twice daily) alone, Outcome 6: CFQ‐R social functioning domain (absolute change from baseline)
16.7. Analysis.

Comparison 16: Tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus either placebo or ivacaftor (150 mg twice daily) alone, Outcome 7: CFQ‐R role functioning domain (absolute change from baseline)
16.8. Analysis.

Comparison 16: Tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus either placebo or ivacaftor (150 mg twice daily) alone, Outcome 8: CFQ‐R eating problems domain (absolute change from baseline)
16.9. Analysis.

Comparison 16: Tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus either placebo or ivacaftor (150 mg twice daily) alone, Outcome 9: CFQ‐R emotional functioning (absolute change from baseline)
16.10. Analysis.

Comparison 16: Tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus either placebo or ivacaftor (150 mg twice daily) alone, Outcome 10: CFQ‐R weight domain (absolute change from baseline)
16.11. Analysis.

Comparison 16: Tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus either placebo or ivacaftor (150 mg twice daily) alone, Outcome 11: CFQ‐R digestive symptoms domain(absolute change from baseline)
16.12. Analysis.

Comparison 16: Tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus either placebo or ivacaftor (150 mg twice daily) alone, Outcome 12: CFQ‐R body image domain (absolute change from baseline)
3. Physiological measures of lung function
a. FEV1 (relative change from baseline)
i. Immediate term (up to and including one month)
Lumacaftor plus ivacaftor versus placebo
Immediate‐term data for this domain have been requested from the investigators of two studies (TRAFFIC 2015; TRANSPORT 2015). Any unpublished information we receive will be included in a future update.
Tezacaftor plus ivacaftor versus control
There was no significant difference between tezacaftor plus ivacaftor compared to ivacaftor alone at one month (n = 504), MD 3.72 (95% CI ‐7.77 to 15.21) (Analysis 16.13) (Donaldson 2018).
16.13. Analysis.

Comparison 16: Tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus either placebo or ivacaftor (150 mg twice daily) alone, Outcome 13: FEV1 % predicted (relative change from baseline)
ii. Short term (over one month and up to and including six months)
Lumacaftor plus ivacaftor versus placebo
At six months, participants in the TRAFFIC and TRANSPORT studies (n = 1108) in the both the lumacaftor 600 mg group and the lumacaftor 400 mg group experienced significantly higher relative changes from baseline in FEV1 (% predicted) compared to the placebo group, MD 5.63 (95% CI 3.80 to 7.47) (Analysis 9.4) and MD 4.77 (95% CI 2.93 to 6.61) (Analysis 10.4) respectively (TRAFFIC 2015; TRANSPORT 2015). There was also a significantly higher relative change from baseline in FEV1 (% predicted) compared to the placebo group when the two lumacaftor doses were pooled, MD 5.21 (95% CI 3.61 to 6.80) (Analysis 11.4) (high‐quality evidence).
9.4. Analysis.

Comparison 9: Lumacaftor (600 mg once daily) plus ivacaftor (250 mg twice daily) versus placebo, Outcome 4: FEV1 % predicted (relative change from baseline)
10.4. Analysis.

Comparison 10: Lumacaftor (400 mg twice daily) plus ivacaftor (250 mg twice daily) versus placebo, Outcome 4: FEV1 % predicted (relative change from baseline)
11.4. Analysis.

Comparison 11: Lumacaftor (600 mg once daily or 400 mg twice daily) plus ivacaftor (250 mg twice daily) versus placebo, Outcome 4: FEV1 % predicted (relative change from baseline)
Tezacaftor plus ivacaftor versus control
At six months, there was a significantly higher relative change from baseline in FEV1 (% predicted) compared to the placebo group in the tezacaftor‐ivacaftor study (n = 510), MD 6.80 (95% CI 5.30 to 8.30) (Analysis 16.13) (Taylor‐Cousar 2017) (moderate‐quality evidence).
b. FEV1 absolute values
i. Immediate term (up to and including one month)
Lumacaftor plus ivacaftor versus placebo
In two studies (n = 1108), participants in the both the lumacaftor 600 mg group and the lumacaftor 400 mg group experienced significantly higher absolute changes from baseline in FEV1 % predicted at 28 days compared to the placebo group, MD 2.32 (95% CI 1.34 to 3.31) (Analysis 9.5) and MD 2.42 (95% CI 1.43 to 3.40) (Analysis 10.5), respectively (TRAFFIC 2015; TRANSPORT 2015). There was also a significantly higher absolute change from baseline in FEV1 % predicted compared to the placebo group when the two lumacaftor doses were pooled, MD 2.37 (95% CI 1.52 to 3.22) (Analysis 11.5). These data were extrapolated and we have requested confirmation of the exact data from the study investigators. Any unpublished information we receive will be included in a future update.
9.5. Analysis.

Comparison 9: Lumacaftor (600 mg once daily) plus ivacaftor (250 mg twice daily) versus placebo, Outcome 5: FEV1 % predicted (absolute change from baseline)
10.5. Analysis.

Comparison 10: Lumacaftor (400 mg twice daily) plus ivacaftor (250 mg twice daily) versus placebo, Outcome 5: FEV1 % predicted (absolute change from baseline)
11.5. Analysis.

Comparison 11: Lumacaftor (600 mg once daily or 400 mg twice daily) plus ivacaftor (250 mg twice daily) versus placebo, Outcome 5: FEV1 % predicted (absolute change from baseline)
The Phase 2 lumacaftor‐ivacaftor study (n = 62) reported on the absolute change from baseline in FEV1 % predicted after lumacaftor monotherapy (day 14) and lumacaftor (200 mg daily) and ivacaftor (150 mg or 250 mg twice daily) combination therapy (day 21) (Boyle 2014). Results for lumacaftor monotherapy are discussed above (see 'Correctors (monotherapy) compared to placebo').
Small, but non‐ significant improvements in FEV1 % predicted were reported at day 21 for participants treated with 200 mg lumacaftor once daily (day 1 to 21) and either 150 mg ivacaftor twice daily (day 15 to 21), MD 2.80 (95% CI ‐1.39 to 6.99) (Analysis 12.1) or 250 mg ivacaftor twice daily (day 15 to 21), MD 0.20 (95% CI ‐4.20 to 4.60) (Analysis 13.1) respectively and when ivacaftor doses were combined, MD 1.57 (95% CI ‐2.13 to 5.27) (Analysis 15.1) (Boyle 2014) (moderate‐quality evidence).
12.1. Analysis.

Comparison 12: Lumacaftor (200 mg once daily) for 21 days plus ivacaftor (150 mg twice daily) for days 15 to 21 versus placebo, Outcome 1: FEV1 % predicted (absolute change from baseline)
13.1. Analysis.

Comparison 13: Lumacaftor (200 mg once daily) for 21 days plus ivacaftor (250 mg twice daily) for days 15 to 21 versus placebo, Outcome 1: FEV1 % predicted (absolute change from baseline)
15.1. Analysis.

Comparison 15: Lumacaftor (200 mg once daily monotherapy for 14 days) plus ivacaftor (150 mg or 250 mg twice daily for days 15 to 21) for 21 days, Outcome 1: FEV1 % predicted (absolute change from baseline)
Tezacaftor plus ivacaftor versus control
At one month, there was a significant higher absolute change from baseline in FEV1 % predicted compared to the control groups in the two tezacaftor‐ivacaftor studies (n = 528), pooled MD 3.59 (95% CI 2.40 to 4.78) (Analysis 16.14) (Taylor‐Cousar 2017).
16.14. Analysis.

Comparison 16: Tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus either placebo or ivacaftor (150 mg twice daily) alone, Outcome 14: FEV1 % predicted (absolute change from baseline)
ii. Short term (over one month and up to and including six months)
Lumacaftor plus ivacaftor versus placebo
In the TRAFFIC and TRANSPORT studies (n = 1108), at six months the significant difference in absolute changes from baseline in FEV1 % predicted were maintained in the both the lumacaftor 600 mg group and the lumacaftor 400 mg groups, MD 3.34 (95% CI 2.30 to 4.38) (Analysis 9.5) and MD 2.80 (95% CI 1.75 to 3.84) (Analysis 10.5) respectively (TRAFFIC 2015; TRANSPORT 2015). There was also a significantly higher absolute change from baseline in FEV1 % predicted compared to the placebo group when the two lumacaftor doses were pooled, MD 3.07 (95% CI 2.17 to 3.97) (Analysis 11.5) (moderate‐quality evidence).
In the paediatric combination study, investigators reported a significantly higher absolute change from baseline in FEV1 % predicted in the lumacaftor plus ivacaftor group compared to the placebo group up to and including six months (n = 204) (Ratjen 2017), MD 2.40 (95% CI 0.40 to 4.40) (Analysis 14.2) (low‐quality evidence). Additional results at earlier time points (day 15, week 4, and week 16) were published graphically in the study report, but the graphical plots were too small to allow for accurate extraction of data (Ratjen 2017). Numerical data for these time points have been requested from the study investigators and any unpublished information we receive will be included in a future update. Investigators in this study also reported early post‐drug dose declines in FEV1 % predicted at day one in the lumacaftor plus ivacaftor group (Ratjen 2017). A markedly smaller decline was observed post‐dose at day 15, and no decline was observed by four months. These data are not available for all participants so are not entered into analysis for this review; instead these results are presented in the additional tables (Table 16).
14.2. Analysis.

Comparison 14: Lumacaftor (200 mg twice daily) plus ivacaftor (250 mg twice daily) versus placebo, Outcome 2: FEV1 % predicted (absolute change from baseline)
8. Acute changes in FEV1 (% predicted) following study drug administration in Ratjen 2017.
|
Lumacaftor plus ivacaftor mean (SD) |
Placebo mean (SD) |
|
| Day 1, ≤ 2 hours post dose | n = 91 ‐5.5 (8.2) |
n = 97 ‐0.1 (5.1) |
| Day 1, 4 to 6 hours post dose | n = 92 ‐7.7 (7.3) |
n = 96 ‐1.4 (7.1) |
| Day 1, 24 hours post dose | n = 38 ‐4.1 (10.1) |
n = 44 ‐1.7 (6.8) |
| Day 15, ≤ 2 hours post dose | n = 88 ‐1.4 (7.0) |
n = 87 0.9 (5.5) |
| Day 15, 4 to 6 hours post dose | n = 86 ‐1.3 (6.4) |
n = 87 0.1 (5.2) |
| Week 16, ≤ 2 hours post dose | n = 33 1.7 (4.8) |
n = 42 0.8 (5.8) |
| Week 16, 4 to 6 hours post dose | n = 33 0.5 (7.4) |
n = 42 0.6 (7.1) |
| Week 24, ≤ 2 hours post dose | n = 25 0.3 (4.1) |
n = 23 0.0 (3.4) |
| Week 24, 4 to 6 hours post dose | n = 24 ‐2.8 (4.0) |
n = 24 0.1 (4.3) |
SD: standard deviation
Tezacaftor plus ivacaftor versus control
At six months, there was a significantly higher absolute change from baseline in FEV1 % predicted compared to the placebo group in the tezacaftor‐ivacaftor study, MD 4.00 (95% CI 3.10 to 4.90) (Analysis 16.14) (Taylor‐Cousar 2017) (moderate‐quality evidence).
c. FVC (absolute values and change from baseline)
Data for this outcome were not reported by any study in this comparison (Boyle 2014; Donaldson 2018; Ratjen 2017; Taylor‐Cousar 2017; TRAFFIC 2015; TRANSPORT 2015). However, it is stated in the protocol of the TRAFFIC and TRANSPORT studies that FVC data were collected (although not considered as an outcome). Any recorded data relevant to this outcome have been requested from the study investigators and any unpublished information we receive will be included in a future update.
d. LCI
ii. Short term (over one month and up to and including six months)
Lumacaftor plus ivacaftor versus placebo
Only one study (n = 204) reported this outcome and its primary outcome was LCI2.5, i.e. the number of lung volume turnovers required to reach 2.5% of starting tracer gas concentration (Ratjen 2017). There was a significantly larger reduction in LCI2.5 in the lumacaftor plus ivacaftor group compared to the placebo group up to and including six months, MD ‐1.10 (95% CI ‐1.40 to ‐0.80) (Analysis 14.3). Additional results at earlier time points (day 15, one month, and four months) were published graphically in the full study report, but the graphical plots were too small to allow for accurate extraction of data (Ratjen 2017). Numerical data for these time points have been requested from the study investigators and any unpublished information we receive will be included in a future update.
14.3. Analysis.

Comparison 14: Lumacaftor (200 mg twice daily) plus ivacaftor (250 mg twice daily) versus placebo, Outcome 3: LCI2.5 (absolute change from baseline)
The study investigators also list LCI5.0 as a secondary outcome of the study, i.e. number of lung volume turnovers required to reach 5% of starting tracer gas concentration (Ratjen 2017). However, results for this outcome are not presented. Numerical data for this outcome have been requested from the study investigators and any unpublished information we receive will be included in a future update.
Secondary outcomes
1. Adverse events
Adverse events were reported by all studies examining combination therapies (Boyle 2014; Donaldson 2018; Ratjen 2017; Taylor‐Cousar 2017; TRAFFIC 2015; TRANSPORT 2015). The type and extent of adverse event reporting was not consistent across studies making comparison between different treatment regimens and interventions a challenge. For the Phase 3 studies a common adverse events was defined by the researchers as one that occurred in more than 10% of participants.
Lumacaftor plus ivacaftor versus placebo
The TRAFFIC and TRANSPORT studies reported no significant differences in the number of participants experiencing adverse events during the study, either by lumacaftor dose or when lumacaftor doses were pooled, OR 1.00 (99% CI 0.37 to 2.71) (Analysis 9.6), OR 0.77 (99% CI 0.30 to 1.96) (Analysis 10.6) and OR 0.87 (99% CI 0.38 to 2.02) (Analysis 11.6), respectively (TRAFFIC 2015; TRANSPORT 2015) (high‐quality evidence).
9.6. Analysis.

Comparison 9: Lumacaftor (600 mg once daily) plus ivacaftor (250 mg twice daily) versus placebo, Outcome 6: Adverse events by end of study (at 6 months)
10.6. Analysis.

Comparison 10: Lumacaftor (400 mg twice daily) plus ivacaftor (250 mg twice daily) versus placebo, Outcome 6: Adverse events by end of study (at 6 months)
11.6. Analysis.

Comparison 11: Lumacaftor (600 mg once daily or 400 mg twice daily) plus ivacaftor (250 mg twice daily) versus placebo, Outcome 6: Adverse events by end of study (at 6 months)
In the paediatric lumacaftor‐ivacaftor study the overall rate of reporting of adverse events was lower than for the TRAFFIC and TRANSPORT studies with a similar profile, including increased reporting of chest tightness on starting the lumacaftor‐ivacaftor intervention compared to placebo (Ratjen 2017). The studies also reported no significant difference between the lumacaftor plus ivacaftor group compared to placebo in the number of participants experiencing adverse events during the study, OR 0.60 (99% CI 0.09 to 4.08) (Analysis 14.4) (low‐quality evidence).
14.4. Analysis.

Comparison 14: Lumacaftor (200 mg twice daily) plus ivacaftor (250 mg twice daily) versus placebo, Outcome 4: Treatment‐emergent adverse events with incidence > 10% in any treatment group (at 6 months)
Tezacaftor plus ivacaftor versus control
For the tezacaftor‐ivacaftor studies, we present the most common adverse events which occurred in at least 10% of participants in either study (Analysis 16.15). Further less commonly occurring adverse events are presented in the original study reports; none of which showed any difference between groups (Donaldson 2018; Taylor‐Cousar 2017) (moderate‐quality evidence).
16.15. Analysis.

Comparison 16: Tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus either placebo or ivacaftor (150 mg twice daily) alone, Outcome 15: Most common adverse events (occurring in at least 10% of participants in either group)
a. Mild (therapy does not need to be discontinued)
Lumacaftor plus ivacaftor versus placebo
Boyle reported data for lumacaftor‐ivacaftor combination therapy at 21 days (day 14 to 21) (Boyle 2014). The combined analysis showed no significant differences between participants treated with lumacaftor‐ivacaftor combination therapy and placebo in the number of participants experiencing cough, oropharyngeal pain, nasal congestion, dizziness, a prolonged prothrombin time, and upper respiratory tract infection (Analysis 12.2; Analysis 13.2; Analysis 15.2) (low‐quality evidence).
12.2. Analysis.

Comparison 12: Lumacaftor (200 mg once daily) for 21 days plus ivacaftor (150 mg twice daily) for days 15 to 21 versus placebo, Outcome 2: Adverse events occurring in 10% or more participants (from days 15 ‐ 21)
13.2. Analysis.

Comparison 13: Lumacaftor (200 mg once daily) for 21 days plus ivacaftor (250 mg twice daily) for days 15 to 21 versus placebo, Outcome 2: Adverse events occurring in 10% or more participants (from days 15 ‐ 21)
15.2. Analysis.

Comparison 15: Lumacaftor (200 mg once daily monotherapy for 14 days) plus ivacaftor (150 mg or 250 mg twice daily for days 15 to 21) for 21 days, Outcome 2: Adverse events occurring in 10% or more participants (from days 15 ‐ 21)
For participants in the TRAFFIC and TRANSPORT studies receiving the lumacaftor‐ivacaftor therapy, the most regularly reported adverse events were respiratory in nature (e.g. chest tightness) (TRAFFIC 2015; TRANSPORT 2015). Most respiratory adverse events occurred shortly after starting lumacaftor‐ivacaftor therapy and for those who continued with the intervention they were reported to be transient in nature. Dyspnoea was significantly more common in the lumacaftor 600 mg once daily plus ivacaftor 250 mg twice daily group compared to placebo, OR 2.05 (99% CI 1.10 to 3.83) (Analysis 9.6) and when lumacaftor doses were combined, OR 1.90 (99% CI 1.08 to 3.35) (Analysis 11.6). Cough was significantly less common in the lumacaftor 400 mg twice daily plus ivacaftor 250 mg twice daily group compared to placebo, OR 0.58 (99% CI 0.39 to 0.88) (Analysis 10.6) and when lumacaftor doses were combined, OR 0.65 (99% CI 0.46 to 0.92) (Analysis 11.6).
There were no significant differences between lumacaftor 600 mg once daily, lumacaftor 400 mg twice daily plus 250 mg ivacaftor twice daily or lumacaftor doses combined compared to placebo in terms of the number of participants experiencing other adverse events: infective pulmonary exacerbation, headache, haemoptysis, diarrhoea, abnormal respiration, increased sputum, nasopharyngitis, oropharyngeal pain, abdominal pain, fatigue, nausea, pyrexia, nasal congestion, upper respiratory tract infection (Analysis 9.6; Analysis 10.6, Analysis 11.6).
In the TRAFFIC and TRANSPORT studies, in seven participants receiving lumacaftor‐ivacaftor therapy abnormal liver function (elevated liver enzyme) results led to a temporary discontinuation of the intervention, after which liver function improved (to baseline in six participants). Treatment was re‐started in six of these participants; in one participant abnormal liver function was associated with hepatitis E infection (TRAFFIC 2015; TRANSPORT 2015).
For the paediatric lumacaftor‐ivacaftor study, the number of treatment‐emergent adverse events with an incidence over 10% were reported (Ratjen 2017). Productive cough, nasal congestion, oropharyngeal pain, upper abdominal pain, rhinorrhoea and increased sputum were observed more frequently in the lumacaftor‐ivacaftor group compared to the placebo group, but there was no significant difference between the groups (Analysis 14.4). There was also no significant differences between the groups in terms of cough, pyrexia, headache, upper respiratory tract infection, abdominal pain, nausea, vomiting, fatigue and respiratory events (such as wheezing, dyspnoea, asthma and chest discomfort) (Analysis 14.4).
Tezacaftor plus ivacaftor versus control
There were no significant differences between tezacaftor‐ivacaftor and control groups (99% CIs) in the number of participants experiencing cough, pulmonary exacerbation, headache, nasal congestion or nasopharyngitis, increased sputum, haemoptysis, pyrexia, oropharyngeal pain, nausea or fatigue (Analysis 16.15) (Donaldson 2018; Taylor‐Cousar 2017). Taylor‐Cousar specified respiratory compromise on initiation as an adverse event in light of the reports from the TRAFFIC and TRANSPORT studies, but there was no increased reporting of this event (Taylor‐Cousar 2017).
b. Moderate (therapy is discontinued, and the adverse effect ceases)
Lumacaftor plus ivacaftor versus placebo
None of the participants in the Phase 2 lumacaftor‐ivacaftor study required study drug interruption for the adverse effects of therapy (Boyle 2014). It was not stated in the TRAFFIC and TRANSPORT studies whether study drug interruption for the adverse effects of therapy was required for any participants (TRAFFIC 2015; TRANSPORT 2015). The combined safety data demonstrated similar rates of serious adverse event reporting for participants receiving placebo (28.6%) and those receiving the lumacaftor‐ivacaftor combination therapy (17.3% to 22.8%); however, the characteristics of these events were different (Analysis 9.6; Analysis 10.6; Analysis 11.6).
In two studies, 14 participants on lumacaftor 600 mg once daily plus ivacaftor 250 mg twice daily and 17 participants on lumacaftor 400 mg twice daily plus ivacaftor 250 mg twice daily discontinued the study due to adverse events. In total 31 of 738 (4.2%) of participants receiving lumacaftor‐ivacaftor discontinued compared to six of 370 (1.6%) participants receiving placebo (TRAFFIC 2015; TRANSPORT 2015). The differences in the discontinuation rates in the treatment groups were not significant compared to placebo at the 1% statistical significance level to allow for multiple analyses related to adverse events, OR 2.38 (99% CI 0.67 to 8.50) (Analysis 9.6), OR 2.91 (99% CI 0.85 to 10.03) (Analysis 10.6) and OR 2.65 (99% CI 0.83 to 8.45) (Analysis 11.6) respectively.
In the same studies, 84 participants on lumacaftor 600 mg once daily plus ivacaftor 250 mg twice daily, 64 participants on lumacaftor 400 mg twice daily plus ivacaftor 250 mg twice daily and 106 participants on placebo experienced at least one 'serious' adverse event (TRAFFIC 2015; TRANSPORT 2015). A 'serious' adverse event was defined as "death, life threatening adverse experience, in‐patient hospitalization/prolongation of hospitalization, persistent/significant disability or incapacity, congenital anomaly/birth defect, important medical event". The following adverse events, which occurred on more than one occasion, were reported to have resulted in discontinuation of the lumacaftor‐ivacaftor therapy: elevated serum creatinine kinase level (n = 4), haemoptysis (n = 3), bronchospasm (n = 2), dyspnoea (n = 2), pulmonary exacerbation (n = 2) (see below), and rash (n = 2). One participant developed hypertension and discontinued the study (not included in the initial reports of this study); other reasons for discontinuation were not recorded (TRAFFIC 2015; TRANSPORT 2015).
There was no significant difference between the number of adverse events between participants on lumacaftor 600 mg once daily plus ivacaftor 250 mg twice daily compared to placebo, OR 0.73 (99% CI 0.47 to 1.13) (Analysis 9.6). significantly fewer participants experienced serious adverse events on lumacaftor 400 mg twice daily plus ivacaftor 250 mg twice daily compared to placebo, OR 0.52 (99% CI 0.33 to 0.83) (Analysis 10.6); this was also true when lumacaftor doses were combined, OR 0.62 (99% CI 0.42 to 0.91) (Analysis 11.6).
For the paediatric study of lumacaftor‐ivacaftor, there was no significant difference reported between groups in the number of serious adverse events reported, OR 1.18 (99% CI 0.38 to 3.63) (Analysis 14.4). There were 13 participants who had serious adverse events in the lumacaftor plus ivacaftor group; these were considered to be treatment‐related in two participants (one drug interaction and one obstructive airways disorder). In the placebo group, 11 participants had serious adverse events; these were considered to be treatment‐related in three participants (one distal intestinal obstruction syndrome, two elevated aminotransferases) (Ratjen 2017). In this study six out of 103 participants discontinued, three due to adverse events. One participant discontinued due to an early respiratory event, a second due to persistently abnormal liver function tests and the reasons for the remaining four who discontinued were not recorded (Ratjen 2017).
In the longer‐term follow‐up study to the TRAFFIC and TRANSPORT studies (PROGRESS), in which participants were randomised to two different lumacaftor‐ivacaftor dose regimens, the paper reported that 7% of the participants withdrew because of adverse events during the 96 week‐study period; in one participant this was due to hypertension (PROGRESS 2017).
Tezacaftor plus ivacaftor versus control
In the Phase 3 tezacaftor‐ivacaftor study, seven out of 251 participants receiving tezacaftor‐ivacaftor discontinued compared to eight out of 258 participants in the placebo group (Taylor‐Cousar 2017). Reasons for discontinuation in the tezacaftor‐ivacaftor group included abdominal pain (n = 2), raised serum creatinine phosphokinase (n = 1), raised liver enzymes (n = 1) and a generalised tonic‐clonic seizure (n = 1).
c. Severe (life‐threatening or debilitating, or which persists even after treatment is discontinued)
Lumacaftor plus ivacaftor versus placebo
For trials evaluating lumacaftor‐ivacaftor, there were no adverse events reported, that in our assessment, were life‐threatening or debilitating. When treatments were discontinued the reported adverse events resolved (Boyle 2014; Ratjen 2017; TRAFFIC 2015; TRANSPORT 2015).
Tezacaftor plus ivacaftor versus control
In the large tezacaftor‐ivacaftor study (n = 510) one life‐threatening adverse event (haemoptysis) was reported in a participant in the tezacaftor‐ivacaftor treatment group (Taylor‐Cousar 2017).
d. Other adverse effects of therapy (of any severity) that are not classifiable according to these categories
All studies reported on the number of participants who experienced episodes of pulmonary exacerbations described as adverse events (Boyle 2014; Donaldson 2018; Ratjen 2017; Taylor‐Cousar 2017; TRAFFIC 2015; TRANSPORT 2015). Results are presented in the analyses (Analysis 9.6; Analysis 10.6; Analysis 11.6; Analysis 12.2; Analysis 13.2; Analysis 15.2; Analysis 14.4; Analysis 16.15) and described below (see 'Extra courses of antibiotics').
Lumacaftor plus ivacaftor versus placebo
After a second participant on lumacaftor‐ivacaftor was withdrawn with hypertension, the researchers for the TRAFFIC and TRANSPORT and PROGRESS studies reported the blood pressure measurements for the participants over the total study period (PROGRESS 2017; TRAFFIC 2015; TRANSPORT 2015). Average blood pressure data were presented from participants over the total 120‐week study period of TRAFFIC and TRANSPORT and PROGRESS for participants who continued on lumacaftor‐ivacaftor, but only for those who received the 400 mg twice daily dose, as this was the dose for which the company received a product licence (PROGRESS 2017). There was a significant mean (SE) increase in systolic blood pressure of 5.1 (1.5) mm Hg and in diastolic blood pressure of 4.1 (1.2) mm Hg (n = 80) (PROGRESS 2017).
2. Hospitalisation
Data for this outcome were reported in two lumacaftor‐ivacaftor studies (TRAFFIC 2015; TRANSPORT 2015) and for the tezacaftor‐ivacaftor study (Taylor‐Cousar 2017), but not by the remaining studies in this comparison (Boyle 2014; Donaldson 2018; Ratjen 2017).
ii. Short term (over one month and up to and including six months)
Tezacaftor plus ivacaftor versus control
The rate of pulmonary exacerbations that led to hospitalisation or treatment with intravenous antibiotic agents (or both) was also lower in the tezacaftor–ivacaftor group than in the placebo group (0.29 versus 0.54 events per year; rate ratio, 0.53; 95% CI, 0.34 to 0.82) (Taylor‐Cousar 2017).
iii. Long term (over six months)
Lumacaftor plus ivacaftor versus placebo
Excerbations were protocol‐defined in the TRAFFIC and TRANSPORT studies as exacerbations leading to hospitalisation or treatment with intravenous antibiotics (TRAFFIC 2015; TRANSPORT 2015). We present information relating to events leading to hospitalisation here and information relating to all pulmonary exacerbations below (see 'Extra courses of antibiotics').
The study publications reported on the rate of events per participant leading to hospitalisation over 48 weeks, graphically pooled across both studies (TRAFFIC 2015; TRANSPORT 2015). We estimate that the event rate per participant over 48 weeks in the placebo group was 0.45. The corresponding event rate in the lumacaftor 600 mg once daily plus ivacaftor 250 mg twice daily group was 0.27 (equal to a 39% decrease compared to the placebo group, P = 0.003). In the lumacaftor 400 mg twice daily plus ivacaftor 250 mg twice daily the event rate was 0.18 (equal to a 61% decrease compared to the placebo group, P < 0.001). The presentation of data did not allow us to estimate the rate over the two lumacaftor doses combined. These data were extrapolated and we have requested confirmation of the exact data from the study investigators. Any unpublished information we receive will be included in a future update.
3. School or work attendance
Data for this outcome were not reported by any study (Boyle 2014; Donaldson 2018; Ratjen 2017; Taylor‐Cousar 2017; TRAFFIC 2015; TRANSPORT 2015).
4. Extra courses of antibiotics
Excerbations were protocol‐defined in two studies as exacerbations leading to hospitalisation or treatment with intravenous antibiotics (TRAFFIC 2015; TRANSPORT 2015). Therefore we present information relating to pulmonary exacerbations (as well as information specifically relating to antibiotic use) here. In the other studies, it was unclear whether reported exacerbations were protocol‐defined or physician‐defined (Boyle 2014; Ratjen 2017).
a. Time‐to the next course of antibiotics
The paediatric combination study listed the time to first pulmonary exacerbation as a secondary outcome of the study, but results for this outcome are not presented (Ratjen 2017). Numerical data for this outcome have been requested from the trial investigators and any unpublished information we receive will be included in a future update.
ii. Short term (over one month and up to and including six months)
Lumacaftor plus ivacaftor versus placebo
In the TRAFFIC and TRANSPORT studies, when compared to placebo the time‐to‐first pulmonary exacerbation was significantly longer in both in the lumacaftor 600 mg once daily plus ivacaftor 250 mg twice daily group, hazard ratio (HR) 0.70 (95% CI 0.57 to 0.87) (Analysis 9.7) and the lumacaftor 400 mg twice daily plus ivacaftor 250 mg twice daily group, HR 0.61 (95% CI 0.49 to 0.76) (Analysis 10.7) (both moderate‐quality evidence). Similarly, the rate of exacerbations was significantly lower in both the active intervention groups compared to placebo; the lumacaftor 600 mg once daily plus ivacaftor 250 mg twice daily group, rate ratio 0.70 (95% CI 0.57 to 0.87) (Analysis 9.8) and the lumacaftor 400 mg twice daily plus ivacaftor 250 mg twice daily group, rate ratio 0.61 (95% CI 0.49 to 0.76) (Analysis 10.8). This information was not reported in the primary journal article, but is available from the study record on ClinicalTrials.gov (TRAFFIC 2015; TRANSPORT 2015). Information regarding time to first pulmonary exacerbation was reported only as a hazard ratio and P value; the SE used in this analysis was estimated using the methods of Parmar (Parmar 1998).
9.7. Analysis.

Comparison 9: Lumacaftor (600 mg once daily) plus ivacaftor (250 mg twice daily) versus placebo, Outcome 7: Time to first pulmonary exacerbation
10.7. Analysis.

Comparison 10: Lumacaftor (400 mg twice daily) plus ivacaftor (250 mg twice daily) versus placebo, Outcome 7: Time to first pulmonary exacerbation
9.8. Analysis.

Comparison 9: Lumacaftor (600 mg once daily) plus ivacaftor (250 mg twice daily) versus placebo, Outcome 8: Rate of exacerbations
10.8. Analysis.

Comparison 10: Lumacaftor (400 mg twice daily) plus ivacaftor (250 mg twice daily) versus placebo, Outcome 8: Rate of exacerbations
Tezacaftor plus ivacaftor versus control
The time‐to‐first pulmonary exacerbation was significantly longer in the tezacaftor‐ivacaftor group compared to the placebo group, HR 0.64 (95% CI, 0.46 to 0.89) (Taylor‐Cousar 2017) (Analysis 16.16) (moderate‐quality evidence).
16.16. Analysis.

Comparison 16: Tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus either placebo or ivacaftor (150 mg twice daily) alone, Outcome 16: Time to first pulmonary exacerbation
b. Total number of courses of antibiotics
ii. Immediate term (up to one month)
Data from the Phase 2 lumacaftor‐ivacaftor study on the number of exacerbations were reported at day 21 (Boyle 2014). These data demonstrated no significant differences between treatment groups from participants receiving 200 mg lumacaftor once daily plus either 150 mg or 250 mg of ivacaftor twice daily or ivacaftor doses combined compared to placebo, OR 2.22 (99% CI 0.08 to 58.11) (Analysis 12.2), OR 1.05 (99% CI 0.03 to 44.10) (Analysis 13.2) and OR 1.62 (99% CI 0.08 to 34.55) (Analysis 15.2), respectively.
ii. Short term (over one month and up to and including six months)
Lumacaftor plus ivacaftor versus placebo
In two studies, both the lumacaftor 600 mg once daily plus 250 mg ivacaftor twice daily and 400 mg twice daily plus 250 mg ivacaftor twice daily groups experienced significantly fewer pulmonary exacerbations than the placebo group, OR 0.66 (99% CI 0.45 to 0.97) (Analysis 9.6) and OR 0.57 (99% CI 0.39 to 0.84) (Analysis 10.6), respectively (TRAFFIC 2015; TRANSPORT 2015). This significant difference was also observed for the two lumacaftor doses combined compared to placebo, OR 0.62 (99% CI 0.44 to 0.86) (Analysis 11.6).
The presentation of data did not allow us to estimate the time to first pulmonary exacerbation or rate of exacerbations over the two lumacaftor doses combined. These data were extrapolated and we have requested confirmation of the exact data from the study investigators. Any unpublished information we receive will be included in a future update.
There were no significance differences between treatment groups in the number of pulmonary exacerbations experienced in the paediatric combination study, OR 1.11 (99% CI 0.44 to 2.81) (Ratjen 2017) (Analysis 14.4).
Tezacaftor plus ivacaftor versus control
The larger study (n = 510) also reported rate of pulmonary exacerbations that led to hospitalisation or treatment with intravenous antibiotic agents (or both); see secondary outcome 'Hospitalisation' above for further details (Taylor‐Cousar 2017).
ii. Long term (over six months)
The TRAFFIC and TRANSPORT studies also reported the rate of events per participant leading to intravenous antibiotic treatment over 48 weeks graphically pooled across the two studies (TRAFFIC 2015; TRANSPORT 2015). These data were extrapolated and we have requested confirmation of the exact data from the study investigators. Any unpublished information we receive will be included in a future update.
We estimate that the event rate per participant over 48 weeks in the placebo group was 0.58. The corresponding event rate in the lumacaftor 600 mg once daily plus ivacaftor 250 mg twice daily group was 0.32 (equal to a 45% decrease compared to the placebo group, P < 0.001) and in the lumacaftor 400 mg twice daily plus ivacaftor 250 mg twice daily was 0.18 (equal to a 56% decrease compared to the placebo group, P < 0.001).
5. Sweat chloride (change from baseline) as a measure of CFTR function
Two studies did not report this outcome (TRAFFIC 2015; TRANSPORT 2015).
ii. Immediate term (up to one month)
Lumacaftor plus ivacaftor versus placebo
Boyle reported that following lumacaftor (day 1 to 21) and ivacaftor (day 15 to 21) combination therapy, data at 21 days demonstrated reductions in sweat chloride concentration in the 150 mg ivacaftor group, MD ‐5.00 mmol/L (95% CI ‐11.60 to 1.60) (Analysis 12.3) and 250 mg ivacaftor group, MD ‐10.90 mmol/L (95% CI ‐17.60 to ‐4.20) (Analysis 13.3), the latter of which was significant (Boyle 2014). There was also a significant reduction in sweat chloride concentration when ivacaftor doses were combined MD ‐7.95 (95% CI ‐13.81 to ‐2.09) (Analysis 15.3).
12.3. Analysis.

Comparison 12: Lumacaftor (200 mg once daily) for 21 days plus ivacaftor (150 mg twice daily) for days 15 to 21 versus placebo, Outcome 3: Sweat chloride concentration (mmol/L) (change from baseline)
13.3. Analysis.

Comparison 13: Lumacaftor (200 mg once daily) for 21 days plus ivacaftor (250 mg twice daily) for days 15 to 21 versus placebo, Outcome 3: Sweat chloride concentration (mmol/L) (change from baseline)
15.3. Analysis.

Comparison 15: Lumacaftor (200 mg once daily monotherapy for 14 days) plus ivacaftor (150 mg or 250 mg twice daily for days 15 to 21) for 21 days, Outcome 3: Sweat chloride concentration (mmol/L) (change from baseline)
Tezacaftor plus ivacaftor versus control
There was a significant reduction in sweat chloride concentration in the tezacaftor‐ivacaftor groups at one month compared to the control groups, pooled MD ‐9.24 mmol/L (95% CI ‐11.12 to ‐7.35) (Analysis 16.17) (Donaldson 2018; Taylor‐Cousar 2017).
16.17. Analysis.

Comparison 16: Tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus either placebo or ivacaftor (150 mg twice daily) alone, Outcome 17: Sweat chloride (change from baseline)
ii. Short term (over one month and up to and including six months)
The paediatric combination study reported a significantly greater absolute reduction in sweat chloride concentration from baseline in the lumacaftor plus ivacaftor group compared to the placebo group, up to and including four weeks, MD ‐20.80 (95% CI ‐23.40 to ‐18.20) (Analysis 14.5). Additional results (at time points day 15, four months, and six months) were published graphically in the study publication, but the graphical plots were too small to allow for accurate extraction of data (Ratjen 2017). Numerical data for these time points have been requested from the study investigators and any unpublished information we receive will be included in a future update.
14.5. Analysis.

Comparison 14: Lumacaftor (200 mg twice daily) plus ivacaftor (250 mg twice daily) versus placebo, Outcome 5: Sweat chloride concentration (absolute change from baseline)
Tezacaftor plus ivacaftor versus control
The reduction in sweat chloride concentration in the tezacaftor‐ivacaftor groups seen at one month compared to the control groups was maintained at six months in the Taylor‐Cousar study, MD ‐10.10 mmol/L (95% CI ‐11.40 to ‐8.80) (Analysis 16.17) (Taylor‐Cousar 2017).
6. Radiological measures of lung disease (assessed using any scoring system)
Data for this outcome were not reported by five studies (Boyle 2014; Donaldson 2018; Taylor‐Cousar 2017; TRAFFIC 2015; TRANSPORT 2015).
ii. Short term (over one month and up to and including six months)
A substudy was performed for the Ratjen study (lumacaftor 200 mg twice daily plus ivacaftor 250 mg twice daily) and investigators reported data for CT scans and Brody score for 10 children, seven on active treatment and three on placebo (Ratjen 2017). There was no difference between groups in the change in overall Brody score at up to 24 weeks, MD ‐16.70 (95% CI ‐36.05 to 2.65) (Analysis 14.6), or in the mean change in the bronchiectasis component of the Brody score, MD ‐2.40 (95% CI ‐4.96 to 0.16) (Analysis 14.7) or in the mean change in the air trapping component of the Brody score, MD ‐6.60 (95% CI ‐20.77 to 7.57) (Analysis 14.8).
14.6. Analysis.

Comparison 14: Lumacaftor (200 mg twice daily) plus ivacaftor (250 mg twice daily) versus placebo, Outcome 6: CT Brody score (mean change)
14.7. Analysis.

Comparison 14: Lumacaftor (200 mg twice daily) plus ivacaftor (250 mg twice daily) versus placebo, Outcome 7: CT Brody score bronchiectasis score (mean change)
14.8. Analysis.

Comparison 14: Lumacaftor (200 mg twice daily) plus ivacaftor (250 mg twice daily) versus placebo, Outcome 8: CT Brody score air trapping score (mean change)
7. Acquisition of respiratory pathogens
No study reported on the acquisition of any respiratory pathogens (P aeruginosa, S aureus, H influenzae, or any other clinically relevant pathogen in CF) (Boyle 2014; Donaldson 2018; Ratjen 2017; Taylor‐Cousar 2017; TRAFFIC 2015; TRANSPORT 2015).
8. Eradication of respiratory pathogens
Data for this outcome were not reported by any study (Boyle 2014; Donaldson 2018; Ratjen 2017; Taylor‐Cousar 2017; TRAFFIC 2015; TRANSPORT 2015).
9. Nutrition and growth
a. Weight
ii. Short term (over one month and up to and including six months)
Lumacaftor plus ivacaftor versus placebo
Data for this outcome were reported by three studies (Ratjen 2017; TRAFFIC 2015; TRANSPORT 2015).
Two studies presented results for the absolute change from baseline in weight (kg) at six months (TRAFFIC 2015; TRANSPORT 2015). Participants in both the lumacaftor 600 mg once daily plus 250 mg ivacaftor twice daily group and the 400 mg twice daily plus 250 mg ivacaftor twice daily group experienced a significantly higher absolute weight gain from baseline compared to the placebo group, MD 0.80 kg (95% CI 0.42 to 1.18) (Analysis 9.9) and MD 0.65 kg (95% CI 0.27 to 1.03) (Analysis 10.9), respectively. There was also a significantly higher absolute weight gain from baseline compared to the placebo group when the two lumacaftor doses were pooled, MD 0.72 kg (95% CI 0.39 to 1.05) (Analysis 11.7).
9.9. Analysis.

Comparison 9: Lumacaftor (600 mg once daily) plus ivacaftor (250 mg twice daily) versus placebo, Outcome 9: Weight (kg) (absolute change from baseline)
10.9. Analysis.

Comparison 10: Lumacaftor (400 mg twice daily) plus ivacaftor (250 mg twice daily) versus placebo, Outcome 9: Weight (kg) (absolute change from baseline)
11.7. Analysis.

Comparison 11: Lumacaftor (600 mg once daily or 400 mg twice daily) plus ivacaftor (250 mg twice daily) versus placebo, Outcome 7: Weight (kg) (absolute change from baseline)
The paediatric combination study listed absolute change in weight and absolute change in weight‐for‐age z score as a secondary outcome of the study, but results for this outcome are not presented (Ratjen 2017). Numerical data for this outcome have been requested from the study investigators and any unpublished information we receive will be included in a future update.
b. BMI
Data for the absolute change from baseline in BMI were reported by four studies (Ratjen 2017; Taylor‐Cousar 2017; TRAFFIC 2015; TRANSPORT 2015); one study additionally reported absolute change in BMI‐for‐age z score (Ratjen 2017).
i. Immediate term (up to and including one month)
Lumacaftor plus ivacaftor versus placebo
At one month, there was no significant difference in the absolute change in BMI from baseline between the lumacaftor 600 mg once daily plus 250 mg ivacaftor twice daily and placebo groups, MD 0.01 (95% CI ‐0.07 to 0.09) (Analysis 9.10) or the lumacaftor 400 mg twice daily plus 250 mg ivacaftor twice daily and placebo groups, MD 0.02 (95% CI ‐0.06 to 0.10) (Analysis 10.10). There was also no significant difference in absolute change in BMI from baseline compared to the placebo group when the two lumacaftor doses were pooled, MD 0.02 (95% CI ‐0.05 to 0.08) (Analysis 11.8).
9.10. Analysis.

Comparison 9: Lumacaftor (600 mg once daily) plus ivacaftor (250 mg twice daily) versus placebo, Outcome 10: BMI (absolute change from baseline)
10.10. Analysis.

Comparison 10: Lumacaftor (400 mg twice daily) plus ivacaftor (250 mg twice daily) versus placebo, Outcome 10: BMI (absolute change from baseline)
11.8. Analysis.

Comparison 11: Lumacaftor (600 mg once daily or 400 mg twice daily) plus ivacaftor (250 mg twice daily) versus placebo, Outcome 8: BMI (absolute change from baseline)
Tezacaftor plus ivacaftor versus control
There was no significant difference between tezacaftor‐ivacaftor and placebo in terms of change from baseline in BMI in the Taylor‐Cousar study at one month, MD ‐0.03 (95% CI ‐0.13 to 0.07) (Analysis 16.18) (Taylor‐Cousar 2017).
16.18. Analysis.

Comparison 16: Tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus either placebo or ivacaftor (150 mg twice daily) alone, Outcome 18: BMI (change from baseline)
ii. Short term (over one month and up to and including six months)
Lumacaftor plus ivacaftor versus placebo
Despite no immediate differences between treatment groups, at six months participants in the both the lumacaftor 600 mg once daily plus 250 mg ivacaftor twice daily and 400 mg twice daily plus 250 mg ivacaftor twice daily groups experienced a significantly higher absolute change in BMI from baseline compared to the placebo group, MD 0.29 (95% CI 0.16 to 0.43) (Analysis 9.10) and MD 0.25 (95% CI 0.12 to 0.39) (Analysis 10.10) respectively. There was also a significantly higher absolute change in BMI from baseline compared to the placebo group when the two lumacaftor doses were pooled; MD 0.27 (95% CI 0.16 to 0.39) (Analysis 11.8)
At six months Rajten reported no significant difference between groups in the absolute change in BMI or the absolute change in BMI‐for‐age z score, MD 0.10 (95% CI ‐0.10 to 0.30) (Analysis 14.9) and MD 0.00 (95% CI ‐0.10 to 0.10) (Analysis 14.10) respectively. Additional results for BMI at earlier time points (day 15, one month, and four months) were published graphically in the full paper, but the graphical plots were too small to allow for accurate extraction of data (Ratjen 2017). Numerical data for these time points have been requested from the study investigators and any unpublished information we receive will be included in a future update.
14.9. Analysis.

Comparison 14: Lumacaftor (200 mg twice daily) plus ivacaftor (250 mg twice daily) versus placebo, Outcome 9: BMI (absolute change from baseline)
14.10. Analysis.

Comparison 14: Lumacaftor (200 mg twice daily) plus ivacaftor (250 mg twice daily) versus placebo, Outcome 10: BMI for age z‐score (absolute change from baseline)
Tezacaftor plus ivacaftor versus control
There was no significant difference between tezacaftor‐ivacaftor and placebo in terms of change from baseline in BMI in the Taylor‐Cousar study at six months, MD ‐0.06 (95% CI ‐0.08 to 0.20) (Analysis 16.18) (Taylor‐Cousar 2017).
c. Height
This outcome was not reported in four studies (Boyle 2014; Taylor‐Cousar 2017; TRAFFIC 2015; TRANSPORT 2015).
ii. Short term (over one month and up to and including six months)
Lumacaftor plus ivacaftor versus placebo
One study listed the absolute change in height and absolute change in height‐for‐age z score as a secondary outcome of the study, but results for this outcome are not presented (Ratjen 2017). Numerical data for this outcome have been requested from the study investigators and any unpublished information we receive will be included in a future update.
Triple therapy (correctors plus potentiators) compared to control
Five studies (775 participants) contributed to the efficacy and safety results in this comparison (Davies 2018a; Davies 2018b; Keating 2018; Heijerman 2019; Middleton 2019). Two studies (133 participants) compared VX‐659‐tezacaftor‐ivacaftor to placebo‐tezacaftor‐ivacaftor or triple placebo in participants with the genotype F508del/MF or F508del/F508del (Davies 2018a; Davies 2018b). The different doses employed and further study details are described above (Included studies).
Three studies (632 participants) compared elexacaftor‐tezacaftor‐ivacaftor to placebo‐tezacaftor‐ivacaftor or triple placebo in participants with the genotype F508del/MF or F508del/F508del (Heijerman 2019; Keating 2018; Middleton 2019). The different doses employed and further study details are described above (Included studies).
With regards to pulmonary exacerbations, please see our definition above (Types of outcome measures). For triple therapy, all trials defined exacerbations as those which were infective in nature or required antibiotics (Davies 2018a; Davies 2018b; Heijerman 2019; Keating 2018; Middleton 2019).
Important results for this comparison are summarised in the tables (Table 7; Table 8). We have assessed the following outcomes using the GRADE criteria in each of the tables and indicated our findings in the relevant text below.
survival;
QoL (total score);
QoL (respiratory domain);
FEV1 % predicted (relative and absolute change);
adverse events; and
time to first pulmonary exacerbation.
For both of the comparisons examined, we judged the quality of the evidence to be high to moderate quality. We downgraded the evidence due to indirectness as results are not applicable to children under the age of 12 and those with more severe disease. We have presented the findings for the comparison of VX‐659 (80 mg once daily, 120 mg twice daily, 240 mg once daily or 400 mg once daily) plus tezacaftor 100 mg once per day plus ivacaftor 150 mg twice daily or VX‐561 150 mg once daily compared to triple placebo (for F508del/MF participants) or placebo tezacaftor 100 mg once daily plus ivacaftor 150 mg twice daily (for F508del/F508del participants) in one table (Table 7) and for the comparison of elexacaftor (50 mg once daily, 100 mg once daily or 200 mg once daily) plus tezacaftor 100 mg once daily plus ivacaftor 150 mg twice daily or VX‐561 150 mg once daily compared to triple placebo (for F508del/MF participants) or placebo tezacaftor 100 mg once daily plus ivacaftor 150 mg twice daily (for F508del/F508del participants) in a separate table (Table 8).
Primary outcomes
1. Survival
No deaths were reported in any of the included studies (Davies 2018a; Davies 2018b; Heijerman 2019; Keating 2018; Middleton 2019) (high‐quality evidence).
2. QoL
a. Total QoL score
None of the triple combination therapy studies reported on total QoL score (Davies 2018a; Davies 2018b; Heijerman 2019; Keating 2018; Middleton 2019).
b. QoL sub‐domains
i. Immediate term (up to and including one month)
Four studies reported on QoL sub‐domains at one month (Davies 2018b; Heijerman 2019; Keating 2018; Middleton 2019).
VX‐659 plus tezacaftor plus ivacaftor
Participants with F508del/MF
One study (n = 117) reported the absolute change in the respiratory domain of the CFQ‐R score after one month of treatment (Davies 2018b). At the 80 mg dose (n = 11), results favoured the intervention over placebo, MD 10.00 (95% CI 0.29 to 19.71) (Analysis 17.1). However, no difference was found for the 240 mg group (n = 20), MD 4.00 (95% CI ‐4.70 to 12.70) (Analysis 19.1) or the 400 mg group (n = 22), MD 7.90 (95% CI ‐0.58 to 16.38) (Analysis 20.1) (moderate‐quality evidence).
17.1. Analysis.

Comparison 17: VX‐659 (80 mg once daily) plus tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo [F508del/MF], Outcome 1: Quality of life: change in CFQ‐R respiratory domain
19.1. Analysis.

Comparison 19: VX‐659 (240 mg once daily) plus tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo [F508del/MF], Outcome 1: Quality of life: change in CFQ‐R respiratory domain
20.1. Analysis.

Comparison 20: VX‐659 (400 mg once daily) plus tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo [F508del/MF], Outcome 1: Quality of life: change in CFQ‐R respiratory domain
Participants with F508del/F508del
One study (n = 10) reported a significant improvement in the CFQ‐R respiratory domain at a dose of VX‐659 400 mg with tezacaftor‐ivacaftor compared to tezacaftor‐ivacaftor‐placebo (Davies 2018b), MD 18.10 (95% CI 10.85 to 25.35) (Analysis 21.1) (moderate‐quality evidence).
21.1. Analysis.

Comparison 21: VX‐659 (400 mg once daily) plus tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo+tez+iva [F508del homozygous], Outcome 1: Quality of life: change in CFQ‐R respiratory domain
VX‐659 plus tezacaftor plus VX‐561
This combination was tested in another group of participants with F508del/MF in one study (n = 19), but only at a dose of VX‐659 400 mg (Davies 2018b). Results showed a significant improvement with the active intervention versus placebo in the respiratory domain, MD 20.30 (95% CI 7.05 to 33.55) (Analysis 22.1) (moderate‐quality evidence).
22.1. Analysis.

Comparison 22: VX‐659 (400 mg once daily) plus tezacaftor (100 mg once daily) plus VX‐561 (150 mg once daily) versus placebo [F508del/MF], Outcome 1: Quality of life: change in CFQ‐R respiratory domain
Elexacaftor plus tezacaftor plus ivacaftor
Participants with F508del/MF
In one study, elexacaftor showed significant improvements versus placebo in the CFQ‐R respiratory domain at one month (Keating 2018): at the 50 mg dose (n = 10), MD 17.20 (95% CI 4.44 to 29.96) (Analysis 24.1) and at the 100 mg dose (n = 22), MD 14.50 (95% CI 3.72 to 25.28) (Analysis 25.1). Two studies reported data for the 200 mg dose at one month (Keating 2018; Middleton 2019); combined data (436 participants) showed a significant improvement in CFQ‐R respiratory domain compared to triple placebo, MD 19.15 (95% CI 16.12 to 22.19) (Analysis 27.1) (moderate‐quality evidence).
24.1. Analysis.

Comparison 24: Elexacaftor (50 mg once daily) tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo [F508del/MF], Outcome 1: Quality of life: change in CFQ‐R respiratory domain
25.1. Analysis.

Comparison 25: Elexacaftor (100 mg once daily) tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo [F508del/MF], Outcome 1: Quality of life: change in CFQ‐R respiratory sub‐domain
27.1. Analysis.

Comparison 27: Elexacaftor (200 mg once daily) tezacaftor (100 mg once daily) plus ivacaftor 150 mg twice daily versus triple placebo‐ F508del/MF, Outcome 1: Quality of life: CFQ‐R respiratory domain (change from baseline)
Participants with F508del/F508del
Two studies (135 participants) reported data at one month (Keating 2018; Heijerman 2019); combined results showed a significant improvement in QoL with elexacaftor 200 mg group compared to tezacaftor‐ivacaftor‐placebo, MD 17.78 (95% CI 12.90 to 22.66) (Analysis 28.1) (moderate‐quality evidence).
28.1. Analysis.

Comparison 28: Elexacaftor (200 mg once daily) tezacaftor (100 mg once daily) plus ivacaftor 150 mg twice daily versus placebo‐tez‐iva‐ F508del/F508del, Outcome 1: Quality of life: CFQ‐R respiratory domain (change from baseline)
Elexacaftor plus tezacaftor plus VX‐561
Participants with F508del/MF
This regimen was only tested at a dose of elexacaftor 200 mg in one study (n = 21) (Keating 2018). Results showed a significant improvement in the respiratory domain of CFQ‐R compared to placebo, MD 12.80 (95% CI 0.93 to 24.67) (Analysis 26.1) (moderate‐quality evidence).
26.1. Analysis.

Comparison 26: Elexacaftor (200 mg once daily) tezacaftor (100 mg once daily) plus VX‐561 (150 mg once daily) versus placebo [F508del/MF], Outcome 1: Quality of life: change in CFQ‐R respiratory domain
ii. Short term (over one month and up to and including six months)
Only one Phase 3 study (403 participants) reported the change in CFQ‐R respiratory domain at six months for participants with F508del/MF. Results showed a significant improvement with the intervention compared to control, MD 20.20 (95% CI 16.19 to 24.21) (Analysis 27.1) (Middleton 2019) (moderate‐quality evidence).
3. Physiological measures of lung function
a. FEV1 (relative change from baseline)
i. Immediate term (up to and including one month)
Two studies reported on the relative change from baseline in FEV1 % predicted at one month (Davies 2018b; Keating 2018).
VX‐659 plus tezacaftor plus ivacaftor
Participants with F508del/MF
One study reported a greater relative change from baseline in FEV1 % predicted with the test intervention compared to placebo (n = 10) for the 80 mg dose (n = 11), MD 18.36% (95% CI 3.63 to 33.09) (Analysis 17.2), the 240 mg dose (n = 20), MD 20.17% (95% CI 8.73 to 31.61) (Analysis 19.2) and the 400 mg dose (n = 22), MD 23.85% (95% CI 14.52 to 33.18) (Analysis 20.2) (Davies 2018b) (moderate‐quality evidence).
17.2. Analysis.

Comparison 17: VX‐659 (80 mg once daily) plus tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo [F508del/MF], Outcome 2: FEV1 % predicted (relative change from baseline)
19.2. Analysis.

Comparison 19: VX‐659 (240 mg once daily) plus tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo [F508del/MF], Outcome 2: FEV1 % predicted (relative change from baseline)
20.2. Analysis.

Comparison 20: VX‐659 (400 mg once daily) plus tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo [F508del/MF], Outcome 2: FEV1 % predicted (relative change from baseline)
Participants with F508del/F508del
One study reported a significant greater relative change in FEV1 % predicted with VX‐659 400 mg (n = 18) than with tezacaftor‐ivacaftor‐placebo (n = 11), MD 15.99% (95% CI 8.61 to 23.37) (Analysis 21.2) (Davies 2018b) (moderate‐quality evidence).
21.2. Analysis.

Comparison 21: VX‐659 (400 mg once daily) plus tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo+tez+iva [F508del homozygous], Outcome 2: FEV1 % predicted (relative change from baseline)
VX‐659 plus tezacaftor plus VX‐561
Participants with F508del/MF
This regimen was only assessed at a dose of VX‐659 400 mg in participants with F508del/MF (n = 25); and results showed a significant greater relative change from baseline in FEV1 % predictedcompared to placebo (n = 6), MD 33.05% (95% CI 22.05 to 44.05) (Analysis 22.2) (Davies 2018b) (moderate‐quality evidence).
22.2. Analysis.

Comparison 22: VX‐659 (400 mg once daily) plus tezacaftor (100 mg once daily) plus VX‐561 (150 mg once daily) versus placebo [F508del/MF], Outcome 2: FEV1 % predicted (relative change from baseline)
Elexacaftor plus tezacaftor plus ivacaftor
Participants with F508del/MF
Results showed greater relative improvements in FEV1 % predicted from baseline compared to placebo (n = 12) at each dose of elexacaftor: at 50 mg (n = 10), MD 19.00% (95% CI 7.08 to 30.92) (Analysis 24.2); at 100 mg (n = 22), MD 13.50% (95% CI 3.28 to 23.72) (Analysis 25.2); and at 200 mg (n = 21), MD 25.90% (95% CI 15.57 to 36.23) (Analysis 27.2) (Keating 2018) (moderate‐quality evidence).
24.2. Analysis.

Comparison 24: Elexacaftor (50 mg once daily) tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo [F508del/MF], Outcome 2: FEV1 % predicted (relative change from baseline)
25.2. Analysis.

Comparison 25: Elexacaftor (100 mg once daily) tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo [F508del/MF], Outcome 2: FEV1 % predicted (relative change from baseline)
27.2. Analysis.

Comparison 27: Elexacaftor (200 mg once daily) tezacaftor (100 mg once daily) plus ivacaftor 150 mg twice daily versus triple placebo‐ F508del/MF, Outcome 2: FEV1 % predicted (relative change from baseline)
Participants with F508del/F508del
One study reported a greater relative change from baseline in FEV1 % predicted in the elexacaftor 200 mg group (n = 21) compared to the tezacaftor‐ivacaftor‐placebo group (n = 7) and this was significant, MD 17.80% (95% CI 6.66 to 28.94) (Analysis 27.2) (Keating 2018) (moderate‐quality evidence).
Elexacaftor plus tezacaftor plus VX‐561
Participants with F508del/MF
Only the elexacaftor 200 mg dose was tested in this group and results again showed a significant greater improvement in FEV1 % predicted from baseline in the test intervention group (n = 21) compared to placebo (n = 8), MD 18.30% (95% CI 7.64 to 28.96) (Analysis 26.2) (Keating 2018) (moderate‐quality evidence).
26.2. Analysis.

Comparison 26: Elexacaftor (200 mg once daily) tezacaftor (100 mg once daily) plus VX‐561 (150 mg once daily) versus placebo [F508del/MF], Outcome 2: FEV1 % predicted (relative change from baseline)
ii. Short term (over one month and up to and including six months)
None of the triple therapy trials reported over this time frame (Davies 2018a; Davies 2018b; Heijerman 2019; Keating 2018; Middleton 2019).
b. FEV1 (absolute values and change from baseline)
All five of the triple combination trials reported on the absolute change in FEV1; two studies reported in L at one month (Davies 2018b; Keating 2018) and three studies reported in % predicted; one at two weeks (Davies 2018a), one at one month (Heijerman 2019) and one at both one and six months (Middleton 2019).
i. Immediate term (up to and including one month)
VX‐659 plus tezacaftor plus ivacaftor
Participants with F508del/MF
The 14‐day study reporting the absolute change in FEV1 % predicted only looked at a treatment regimen using VX‐659 120 mg twice daily in participants with the genotype F508del/MF (Davies 2018a); results showed that the intervention (n = 9) improved FEV1 % predicted compared to placebo (n = 3), MD 10.00% (95% CI 3.04 to 16.96) (Analysis 18.1) (moderate‐quality evidence).
18.1. Analysis.

Comparison 18: VX‐659 (120 mg twice daily) plus tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo [F508del/MF], Outcome 1: FEV1 % predicted (absolute change from baseline)
The second Davies study reported a greater absolute change in FEV1 (L) with the intervention regimen compared to placebo (n = 10) for all dose levels (Davies 2018b): 80 mg dose (n = 11), MD 0.37 L (95% CI 0.15 to 0.59) (Analysis 17.3); 240 mg (n = 20), MD 0.42 L (95% CI 0.20 to 0.64) (Analysis 19.3); and 400 mg (n = 22), MD 0.52 L (95% CI 0.34 to 0.70) (Analysis 20.3) (moderate‐quality evidence).
17.3. Analysis.

Comparison 17: VX‐659 (80 mg once daily) plus tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo [F508del/MF], Outcome 3: FEV1 L (absolute change from baseline)
19.3. Analysis.

Comparison 19: VX‐659 (240 mg once daily) plus tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo [F508del/MF], Outcome 3: FEV1 L (absolute change from baseline)
20.3. Analysis.

Comparison 20: VX‐659 (400 mg once daily) plus tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo [F508del/MF], Outcome 3: FEV1 L (absolute change from baseline)
Participants with F508del/F508del
One study reported the absolute change in FEV1 (L) at one month in participants with F508del/F508del with the dose VX‐659 400 mg (Davies 2018b). Results showed the improvement in the intervention group (n = 18) compared to the control group (n = 11) was significantly greater, MD 0.35 L (95% CI 0.19 to 0.51) (Analysis 21.3) (moderate‐quality evidence).
21.3. Analysis.

Comparison 21: VX‐659 (400 mg once daily) plus tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo+tez+iva [F508del homozygous], Outcome 3: FEV1 L (absolute change from baseline)
VX‐659 plus tezacaftor plus VX‐561
Only a dose of VX‐659 400 mg was tested in participants with the F508del/MF genotype and results showed a greater absolute change from baseline in FEV1 (L) in the intervention group (n = 19) compared to placebo (n = 6) which was significant, MD 0.68 L (95% CI 0.45 to 0.91) (Analysis 22.3; Davies 2018b) (moderate‐quality evidence).
22.3. Analysis.

Comparison 22: VX‐659 (400 mg once daily) plus tezacaftor (100 mg once daily) plus VX‐561 (150 mg once daily) versus placebo [F508del/MF], Outcome 3: FEV1 L (absolute change from baseline)
Elexacaftor plus tezacaftor plus ivacaftor
Participants with F508del/MF
One study reported on the absolute change in FEV1 % predicted at one month in this population (Middleton 2019). Results showed that the triple therapy combination led to a greater absolute change in FEV1 % predicted compared to triple placebo which was significant, MD 13.80 (95% CI 12.18 to 15.42) (Analysis 27.3) (Middleton 2019).
27.3. Analysis.

Comparison 27: Elexacaftor (200 mg once daily) tezacaftor (100 mg once daily) plus ivacaftor 150 mg twice daily versus triple placebo‐ F508del/MF, Outcome 3: FEV1 % predicted (absolute change from baseline)
One study reported on the absolute change in FEV1 (L) from baseline at one month (Keating 2018). The triple therapy combination led to significant greater changes at all doses of the test intervention compared to placebo (n = 12): 50 mg (n = 10), MD 0.46 L (95% CI 0.19, 0.73) (Analysis 24.3); 100 mg group (n = 22), MD 0.38 L (95% CI 0.20 to 0.56) (Analysis 25.3); and 200 mg group (n = 21), MD 0.57 L (95% CI 0.36, to 0.78) (Analysis 27.4).
24.3. Analysis.

Comparison 24: Elexacaftor (50 mg once daily) tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo [F508del/MF], Outcome 3: FEV1 L (absolute change from baseline)
25.3. Analysis.

Comparison 25: Elexacaftor (100 mg once daily) tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo [F508del/MF], Outcome 3: FEV1 L (absolute change from baseline)
27.4. Analysis.

Comparison 27: Elexacaftor (200 mg once daily) tezacaftor (100 mg once daily) plus ivacaftor 150 mg twice daily versus triple placebo‐ F508del/MF, Outcome 4: FEV1 L (absolute change from baseline)
Participants with F508del/F508del
One study reported on the absolute change in FEV1 % predicted at one month and showed that the elexacaftor‐tezacaftor‐ivacaftor combination (n = 55) led to a greater absolute change compared to tezacaftor‐ivacaftor‐placebo (n = 52) which was significant, MD 10.00% predicted (95% CI 7.51 to 12.49) (Analysis 28.3) (Heijerman 2019).
28.3. Analysis.

Comparison 28: Elexacaftor (200 mg once daily) tezacaftor (100 mg once daily) plus ivacaftor 150 mg twice daily versus placebo‐tez‐iva‐ F508del/F508del, Outcome 3: FEV1 % predicted (absolute change from baseline)
A further study reported on the absolute change in FEV1 (L) at one month (Keating 2018). Results showed a significant greater absolute change in the elexacaftor 200 mg (plus tezacaftor and ivacaftor) group (n = 21) compared to the tezacaftor‐ivacaftor‐placebo group (n = 7), MD 0.46 L (95% CI 0.26 to 0.66) (Analysis 28.4) (moderate‐quality evidence).
28.4. Analysis.

Comparison 28: Elexacaftor (200 mg once daily) tezacaftor (100 mg once daily) plus ivacaftor 150 mg twice daily versus placebo‐tez‐iva‐ F508del/F508del, Outcome 4: FEV1 L (absolute change from baseline)
Elexacaftor plus tezacaftor plus VX‐561
Participants with F508del/MF
Keating only tested a dose of elexacaftor 200 mg (n = 21) in participants with the F508del/MF genotype (Keating 2018) and results showed a significant greater absolute change in FEV1 (L) versus placebo (n = 8), MD 0.44 L (95% CI 0.25 to 0.63) (Analysis 26.3) (moderate‐quality evidence).
26.3. Analysis.

Comparison 26: Elexacaftor (200 mg once daily) tezacaftor (100 mg once daily) plus VX‐561 (150 mg once daily) versus placebo [F508del/MF], Outcome 3: FEV1 L (absolute change from baseline)
ii. Short term (over one month and up to and including six months)
Elexacaftor‐tezacaftor‐ivacaftor
Participants with F508del/MF
Only one triple therapy study (n = 403) reported on the absolute change in FEV1 % predicted at six months (Middleton 2019). It found a significant greater change from baseline in the treatment group compared to the triple placebo group, MD 14.30 (95% CI 12.76 to 15.84) (Analysis 27.3) (moderate‐quality evidence).
c. FVC (absolute values and change from baseline)
Data for this outcome were not reported by any study for this comparison (Davies 2018a; Davies 2018b; Heijerman 2019; Keating 2018; Middleton 2019).
d. LCI
Data for this outcome were not reported by any study for this comparison (Davies 2018a; Davies 2018b; Heijerman 2019; Keating 2018; Middleton 2019).
Secondary outcomes
1. Adverse events
Adverse events were reported by all of the studies examining triple combination therapies, in one study over a period of two weeks (Davies 2018a), in three studies over a period of one month (Davies 2018b; Heijerman 2019; Keating 2018) and in one study at one month and at six months (Middleton 2019) (moderate‐quality evidence). All three of the studies reported adverse events in terms of mild, moderate or severe; they also recorded the "most common adverse events" which they defined as occurring in at least 5% participants. We have set CIs for adverse events at 99%, as per "measure of treatment effect" in this review's methodology.
VX‐659 plus tezacaftor plus ivacaftor versus placebo
There was no significant difference in the number of participants experiencing at least one adverse event between the test intervention and placebo at any dose or for any genotype.
Participants with F508del/MF
One Phase 1 study reported on this comparison with a dose level of VX‐659 120 mg (n = 9) and found no differences between groups, OR 31.67 (99% CI 0.32 to 3111.29) (Analysis 18.2) (Davies 2018a). One Phase 2 study reported on this comparison at three dose levels of VX‐659 and found no difference between intervention and placebo groups at any level (Davies 2018b): 80 mg (n = 11), OR 1.11 (99% CI 0.02 to 51.19) (Analysis 17.4); 240 mg (n = 20), OR 0.33 (99% CI 0.02 to 6.85) (Analysis 19.4); and 400 mg dose level (n = 22), OR 0.38 (99% CI 0.02 to 7.70) (Analysis 20.4). All doses are once daily except for 120 mg, which was taken twice daily in the Phase 1 study (moderate‐quality evidence).
18.2. Analysis.

Comparison 18: VX‐659 (120 mg twice daily) plus tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo [F508del/MF], Outcome 2: Adverse events (at up to 1 month)
17.4. Analysis.

Comparison 17: VX‐659 (80 mg once daily) plus tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo [F508del/MF], Outcome 4: Adverse events (at 1 month)
19.4. Analysis.

Comparison 19: VX‐659 (240 mg once daily) plus tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo [F508del/MF], Outcome 4: Adverse events (at 1 month)
20.4. Analysis.

Comparison 20: VX‐659 (400 mg once daily) plus tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo [F508del/MF], Outcome 4: Adverse events (at 1 month)
Participants with F508del/F508del
Only one study reported on this genotype for this combination (Davies 2018b). At the VX‐659 400 mg dose level (n = 18), there was no difference between intervention and placebo groups, OR 1.11 (99% CI 0.08 to 14.81) (Analysis 21.4) (moderate‐quality evidence).
21.4. Analysis.

Comparison 21: VX‐659 (400 mg once daily) plus tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo+tez+iva [F508del homozygous], Outcome 4: Adverse events (at 1 month)
VX‐659 plus tezacaftor plus VX‐561 versus placebo
Participants with F508del/MF
For this comparison, there was no significant difference in the number of participants experiencing at least one adverse event between the test intervention (n = 19) and placebo (n = 6) groups, OR 0.95 (99% CI 0.01 to 74.78) (Analysis 22.4) (Davies 2018b) (moderate‐quality evidence).
22.4. Analysis.

Comparison 22: VX‐659 (400 mg once daily) plus tezacaftor (100 mg once daily) plus VX‐561 (150 mg once daily) versus placebo [F508del/MF], Outcome 4: Adverse events (at 1 month)
Elexacaftor plus tezacaftor plus ivacaftor versus placebo
Participants with F508del/MF
The Phase 2 study reported that for the 50 mg cohort, every participant in both the intervention and placebo groups had an adverse event, therefore an OR was not estimable (Analysis 24.4) (Keating 2018). For the other doses in this study, the corresponding ORs and CIs are: 100 mg (n = 22), OR 0.57 (99% CI 0.01 to 42.46) (Analysis 25.4); and 200 mg (n = 21), OR 0.21 (99% CI 0.00 to 11.62) (Analysis 27.5). The Phase 3 study of participants with this genotype reported at six months and found no significant difference in the total number of adverse events between the 200 mg elexacaftor and placebo groups, OR 0.56 (99% CI 0.23 to 1.36) (Analysis 27.6) (Middleton 2019).
24.4. Analysis.

Comparison 24: Elexacaftor (50 mg once daily) tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo [F508del/MF], Outcome 4: Adverse events (at 1 month)
25.4. Analysis.

Comparison 25: Elexacaftor (100 mg once daily) tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo [F508del/MF], Outcome 4: Adverse events at (1 month)
27.5. Analysis.

Comparison 27: Elexacaftor (200 mg once daily) tezacaftor (100 mg once daily) plus ivacaftor 150 mg twice daily versus triple placebo‐ F508del/MF, Outcome 5: Adverse events (at up to 1 month)
27.6. Analysis.

Comparison 27: Elexacaftor (200 mg once daily) tezacaftor (100 mg once daily) plus ivacaftor 150 mg twice daily versus triple placebo‐ F508del/MF, Outcome 6: Adverse events (at up to 6 months)
Participants with F508del/F508del
Data from two studies combined (135 participants) showed no difference in the number of people experiencing an adverse event at one month, OR 0.94 (99% CI 0.46 to 1.96). (Analysis 28.5; Heijerman 2019; Keating 2018). (moderate‐quality evidence).
28.5. Analysis.

Comparison 28: Elexacaftor (200 mg once daily) tezacaftor (100 mg once daily) plus ivacaftor 150 mg twice daily versus placebo‐tez‐iva‐ F508del/F508del, Outcome 5: Adverse events (at up to 1 month)
Elexacaftor plus tezacaftor plus VX‐561 versus placebo
Participants with F508del/MF
At one month, no significant difference in the number of adverse events was observed between the intervention (n = 21) and placebo (n = 8) groups, OR 1.36 (99% CI 0.05 to 38.84) (Analysis 26.4) (Keating 2018) (moderate‐quality evidence).
26.4. Analysis.

Comparison 26: Elexacaftor (200 mg once daily) tezacaftor (100 mg once daily) plus VX‐561 (150 mg once daily) versus placebo [F508del/MF], Outcome 4: Adverse events (at 1 month)
a. Mild (therapy does not need to be discontinued)
We could not accurately record the number of mild adverse events occurring in any of the triple therapy studies since they record the number of participants experiencing at least one adverse event, by the maximum severity, meaning that a participant may have had numerous 'mild' adverse events and a single moderate or severe event, but we would only be aware of the single most severe event (Davies 2018a; Davies 2018b; Heijerman 2019; Keating 2018; Middleton 2019).
b. Moderate (therapy is discontinued, and the adverse effect ceases)
Our definition of a moderate adverse effect differed to that used in the studies, however the studies also reported the number of adverse events which led to discontinuation of therapy. We therefore used this number to record the number of moderate adverse events according to our definition.
VX‐659 plus tezacaftor plus ivacaftor
Participants with F508del/MF
No participants in either the intervention or placebo groups were recorded as having a moderate adverse event in the dose groups VX‐659 80 mg, VX‐659 120 mg twice daily group and VX‐659 400 mg meaning an OR was not calculable (Analysis 17.4; Analysis 18.2; Analysis 20.4) (moderate‐quality evidence). For the VX‐659 240 mg group, there was no significant difference in the number of moderate adverse events between the intervention (n = 20) and placebo groups (n = 10), OR 1.62 (99% CI 0.02 to 121.50) (Analysis 19.4) (Davies 2018b) (moderate‐quality evidence).
Participants with F508del/F508del
At one month no participants in either the intervention or placebo groups were recorded as having a moderate adverse event at the dose VX‐659 400 mg meaning an OR was not calculable (Analysis 21.4) (Davies 2018b) (moderate‐quality evidence).
VX‐659 plus tezacaftor plus VX‐561
Participants with F508del/MF
No significant difference was observed in the number of moderate adverse events between the intervention (n = 19) and placebo groups (n = 6) after one month of this treatment regimen, OR 1.86 (99% CI 0.03 to 119.25) (Analysis 22.4) (Davies 2018b) (moderate‐quality evidence).
Elexacaftor plus tezacaftor plus ivacaftor
Participants with F508del/MF
No participants in either the In the elexacaftor 50 mg or the elexacaftor 100 mg groups or the placebo groups were recorded as having a moderate adverse event at one month, meaning an OR was not calculable for the groups taking this dose (Analysis 24.4; Analysis 25.4) (moderate‐quality evidence). There were no significant differences in the number of moderate adverse events experienced by the elexacaftor 200 mg (n = 21) and placebo groups, OR 3.21 (99% CI 0.05 to 193.04) (Analysis 27.5) (Keating 2018).
Participants with F508del/F508del
Two studies reported the number of participants experiencing moderate adverse events at one month (Heijerman 2019; Keating 2018) and found no difference between the elexacaftor 200 mg (n = 76) and placebo groups (n = 59), OR 0.94 (99% CI 0.39 to 2.26) (Analysis 28.5) (Keating 2018) (moderate‐quality evidence).
Elexacaftor plus tezacaftor plus VX‐561
Participants with F508del/MF
No participants in either the intervention or placebo groups experienced a moderate adverse effect, meaning an OR was not calculable for this group (Analysis 26.4) (Keating 2018) (moderate‐quality evidence).
c. Severe (life‐threatening or debilitating, or which persists even after stopping treatment)
Our definition of severe adverse events was equivalent to the studies' definition of a serious adverse event, therefore we counted the number of participants reporting serious adverse events.
VX‐659 plus tezacaftor plus ivacaftor
Participants with F508del/MF
Severe adverse events also occurred at every dose level in both intervention and placebo groups for participants with this genotype (Davies 2018a; Davies 2018b). Results showed no differences between groups at any dose level: VX‐659 80 mg (n = 11), OR 0.23 (99% CI 0.01 to 5.92) (Analysis 17.4); VX‐659 120 mg twice daily (n = 9), OR 2.33 (99% CI 0.03 to 176.29) (Analysis 18.2); VX‐659 240 mg (n = 20), OR 0.58 (99% CI 0.06 to 5.75) (Analysis 19.4); and VX‐659 400 mg (n = 22), OR 0.11 (99% CI 0.00 to 2.67) (Analysis 20.4); (moderate‐quality evidence).
Participants with F508del/F508del
Severe adverse events occurred in the VX‐659 400 mg (n = 18) and placebo groups and there was no significant difference between groups, OR 0.26 (99% CI 0.01 to 7.39) (Analysis 21.4) (Davies 2018b).
VX‐659 plus tezacaftor plus VX‐561
Participants with F508del/MF
No statistical difference was found between the VX‐659 400 mg (n = 19) and placebo (n = 6) groups for the number of severe adverse effects at one month, OR 0.12 (99% CI 0.01 to 2.04) (Analysis 22.4) (Davies 2018b) (moderate‐quality evidence).
Elexacaftor plus tezacaftor plus ivacaftor
Participants with F508del/MF
No significant differences were observed between the intervention and placebo groups at one month, across doses for this genotype: elexacaftor 50 mg (n = 10), OR 0.56 (99% CI 0.02 to 16.15) (Analysis 24.4); elexacaftor 100 mg (n = 22), OR 0.50 (99% CI 0.03 to 7.92) (Analysis 25.4); elexacaftor 200 mg (n = 21), OR 0.10 (99% CI 0.00 to 5.93) (Analysis 27.5) (Keating 2018) (low‐quality evidence). At six months, one study (33 participants) also reported no difference in the number of severe adverse events between groups, OR 1.39 (99% CI 0.54 to 3.57) (Analysis 27.6) (Middleton 2019).
Participants with F508del/F508del
Two studies (135 participants) compared elexacaftor 200 mg to placebo and found no difference in the number of severe adverse events between groups at one month, OR 0.19 (99% CI 0.02 to 1.92) (Analysis 28.5) (Keating 2018) (moderate‐quality evidence).
Elexacaftor plus tezacaftor plus VX‐561
Participants with F508del/MF
None of the 21 participants in the intervention group and one out of eight participants in the placebo group experienced a severe adverse event, resulting in no significant difference between the groups, OR 0.12 (99% CI 0.00 to 8.97) (Analysis 26.4) (Keating 2018) (moderate‐quality evidence).
2. Hospitalisation
ii. Short term (over one month and up to and including six months)
Elexacaftor plus tezacaftor plus ivacaftor
Participants with F508del/MF
Only one Phase 3 study reported this outcome (Middleton 2019); investigators found that elexacaftor 200 mg in combination with tezacaftor and ivacaftor reduced the odds of hospitalisation versus triple placebo, OR 0.29 (95% CI 0.14 to 0.60) (Analysis 27.7).
27.7. Analysis.

Comparison 27: Elexacaftor (200 mg once daily) tezacaftor (100 mg once daily) plus ivacaftor 150 mg twice daily versus triple placebo‐ F508del/MF, Outcome 7: Hospitalisation
3. School or work attendance
Data for this outcome were not reported by any study (Davies 2018a; Davies 2018b; Heijerman 2019; Keating 2018; Middleton 2019).
4. Extra courses of antibiotics
a. Time‐to the next course of antibiotics
Data for this outcome were not reported by any study (Davies 2018a; Davies 2018b; Heijerman 2019; Keating 2018; Middleton 2019).
b. Total number of courses of antibiotics
As for the monotherapy and dual combination therapy sections, under this outcome we report the occurrence of infective pulmonary exacerbations.
i. Immediate term (up to one month)
VX‐659 plus tezacaftor plus ivacaftor
Participants with F508del/MF
Again there were no differences between treatment and placebo groups at any dose level. The 14‐day Phase 1 study found that in the 120 mg twice daily group, two out of nine participants in the intervention group and none of the three participants in the placebo group had an infective pulmonary exacerbation which showed no difference between groups, OR 2.33 (95% CI 0.03 to 176.29) (Analysis 18.2) (Davies 2018a)
ii. Short term (over one month and up to and including six months)
VX‐659 plus tezacaftor plus ivacaftor
Participants with F508del/MF
The Phase 2 study (Davies 2018b) found that after one month, three out of 11 participants in the 80 mg group group and two out of 10 participants in the placebo group had an exacerbation, OR 1.50 (95% CI 0.10 to 21.90) (Analysis 17.4); three out of 20 participants in the 240 mg once daily group and two out of 10 in the placebo group had an exacerbation, OR 0.71 (95% CI 0.05 to 9.48) (Analysis 19.4); and four out of 22 participants in the 400 mg group and two out of 10 in the placebo group had an exacerbation, OR 0.89 (95% CI 0.07 to 10.67) (Analysis 20.4)
Participants with F508del/F508del
At the dose level of 400 mg there was no difference between groups since five out of 18 participants in the VX‐659 group and three out of 11 in the placebo group had an exacerbation, OR 1.03 (95% CI 0.11 to 9.34) (Analysis 21.4) (Davies 2018b)
VX‐659 plus tezacaftor plus VX‐561
Participants with F508del/MF
Davies reported that at one month two out of 19 participants in the VX‐659 400 mg group and three out of six participants in the placebo group had experienced an exacerbation, OR 1.03 (95% CI 0.11 to 15.47) (Analysis 23.4) (Davies 2018b)
23.4. Analysis.

Comparison 23: VX‐659 400 mg tezacaftor ‐ pooled ivacaftor and VX‐561, Outcome 4: Adverse events (at 1 month)
Elexacaftor plus tezacaftor plus ivacaftor
Participants with F508del/MF
Keating also reported data at one month for these participants and found that three out of 10 participants in the 50 mg group and four out of 12 participants in the placebo group had an infective pulmonary exacerbation, OR 0.86 (95% CI 0.08 to 9.23) (Analysis 24.4). At the same time point, five out of 22 participants in the 100 mg group and three out of 12 participants on placebo had an exacerbation, OR 0.59 (95% CI 0.08 to 4.57) (Analysis 25.4); and two out of 21 participants on the 200 mg treatment regimen and four out of 12 on placebo had an exacerbation, OR 0.21 (95% CI 0.02 to 2.52) (Analysis 26.4).
Middleton reported that at 24 weeks, 11 out of 202 participants in the 200 mg elexacaftor group and 33 out of 201 participants in the control group had an exacerbation requiring antibiotics; this led to significantly lower odds of having an exacerbation requiring antibiotics, OR 0.29 (95% CI 0.14 to 0.60) (Analysis 27.8) (Middleton 2019). Time to exacerbation was significantly shorter for participants on placebo, HR 0.34 (95% CI 0.22 to 0.52), as reported in the supplementary paper (complete data requested from the authors) (Middleton 2019).
27.8. Analysis.

Comparison 27: Elexacaftor (200 mg once daily) tezacaftor (100 mg once daily) plus ivacaftor 150 mg twice daily versus triple placebo‐ F508del/MF, Outcome 8: Exacerbation (need for antibiotics)
Participants with F508del/F508del
At one month, five out of 21 participants in the 200 mg group and one out of seven participants in the placebo group had experienced an exacerbation,it was not clear whether the exacerbations were protocol‐defined or physician‐defined (Keating 2018). Heijerman reports one out of 55 participants receiving elexacaftor‐tezacaftor‐ivacaftor experienced physician‐defined pulmonary exacerbation compared to six out of 52 participants in the placebo group at the same time point (Heijerman 2019). The combined data showed a significant difference in favour of elexacaftor‐tezacaftor‐ivacaftor, OR 0.15 (95% CI 0.02 to 1.00) (Analysis 26.4).
Elexacaftor plus tezacaftor plus VX‐561
Participants with F508del/MF
Keating reported that three out of 21 of those on the active regimen and four out of eight participants on placebo had an infective respiratory exacerbation during the one‐month study, OR 0.17 (95% CI 0.01 to 1.89) (Analysis 26.4) (Keating 2018).
5. Sweat chloride (change from baseline) as a measure of CFTR function
i. Immediate term (up to one month)
VX‐659 plus tezacaftor plus ivacaftor
Participants with F508del/MF
At two weeks, the Phase 1 study found that the 120 mg twice‐daily dose of VX‐659 (n = 9) reduced sweat chloride more than with placebo (n = 3), MD ‐30.60 mmol/L (95% CI ‐46.38 to ‐14.82) (Analysis 18.3) (Davies 2018a) (low‐quality evidence).
18.3. Analysis.

Comparison 18: VX‐659 (120 mg twice daily) plus tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo [F508del/MF], Outcome 3: Sweat chloride (absolute change from baseline)
At one month, the Phase 2 study found that, all active intervention groups showed a reduction in sweat chloride compared to placebo (Davies 2018b) (low‐quality evidence). At the 80 mg dose level, the treatment group (n = 11) reduced sweat chloride by 45.70 mmol/L whereas the placebo group (n = 10) experienced an increase in sweat chloride by 2.9 mmol/L, MD ‐48.60 mmol/L (95% CI ‐60.94 to ‐36.26) (Analysis 17.5); the 240 mg intervention group (n = 20) reduced sweat chloride by 43.8 mmol/L, MD ‐46.70 mmol/L (95% CI ‐57.91 to ‐35.49) (Analysis 19.5); and the 400 mg intervention group (n = 22) reduced sweat chloride by 51.4 mmol/L, MD ‐54.30 mmol/L (95% CI ‐65.28 to ‐43.32) (Analysis 20.5).
17.5. Analysis.

Comparison 17: VX‐659 (80 mg once daily) plus tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo [F508del/MF], Outcome 5: Sweat chloride (change from baseline) [mmol/L]
19.5. Analysis.

Comparison 19: VX‐659 (240 mg once daily) plus tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo [F508del/MF], Outcome 5: Sweat chloride (change from baseline) [mmol/L]
20.5. Analysis.

Comparison 20: VX‐659 (400 mg once daily) plus tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo [F508del/MF], Outcome 5: Sweat chloride (mmol/L) change from baseline
Participants with F508del/F508del
Davies reported a greater reduction in sweat chloride at one month in the 400 mg group (n = 18) compared to placebo, MD ‐45.20 mmol/L (95% CI ‐52.18 to ‐38.22) (Analysis 21.5) (Davies 2018b).
21.5. Analysis.

Comparison 21: VX‐659 (400 mg once daily) plus tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo+tez+iva [F508del homozygous], Outcome 5: Sweat chloride (change from baseline) [mmol/L]
VX‐659 plus ivacaftor plus VX‐561
Participants with F508del/MF
At one month, Davies reported a greater reduction in sweat chloride in the 400 mg intervention group (n = 19) than in the placebo group (n = 6), MD ‐36.80 mmol/L (95% CI ‐48.74 to ‐24.86) (Analysis 22.5) (Davies 2018b) (low‐quality evidence).
22.5. Analysis.

Comparison 22: VX‐659 (400 mg once daily) plus tezacaftor (100 mg once daily) plus VX‐561 (150 mg once daily) versus placebo [F508del/MF], Outcome 5: Sweat chloride (change from baseline) [mmol/L]
Elexacaftor plus tezacaftor plus ivacaftor
Participants with F508del/MF
At one month, Keating found that all active intervention groups in this comparison showed a difference in the change in sweat chloride compared to placebo (Keating 2018). The placebo group for the ascending dose groups (n = 12) showed a decrease in sweat chloride of ‐2.2 mmol/L and the 50 mg elexacaftor group (n = 10) showed a decrease of 38.2 mmol/L, MD ‐36.00 mmol/L (95% CI ‐47.23 to ‐24.77) (Analysis 24.5); the 100 mg elexacaftor group (n = 22) showed a decrease of 33.2 mmol/L, MD ‐31.00 mmol/L (95% CI ‐40.41 to ‐21.59) (Analysis 25.5); and the 200 mg elexacaftor group (n = 21) showed a decrease of 39.1 mmol/L, MD ‐36.90 mmol/L (95% CI ‐46.43 to ‐27.37) (Analysis 27.9). At the same time point, Middleton reported a significantly greater decrease in sweat chloride versus placebo, MD ‐41.30 mmol/L (95% CI ‐44.04, ‐38.56) (Middleton 2019); when combined these data showed a decrease in sweat chloride with the triple therapy, MD ‐40.96 (95% CI ‐43.60 to ‐38.33) (Analysis 27.9).
24.5. Analysis.

Comparison 24: Elexacaftor (50 mg once daily) tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo [F508del/MF], Outcome 5: Sweat chloride (change from baseline) [mmol/L]
25.5. Analysis.

Comparison 25: Elexacaftor (100 mg once daily) tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo [F508del/MF], Outcome 5: Sweat chloride (change from baseline) [mmol/L]
27.9. Analysis.

Comparison 27: Elexacaftor (200 mg once daily) tezacaftor (100 mg once daily) plus ivacaftor 150 mg twice daily versus triple placebo‐ F508del/MF, Outcome 9: Sweat chloride (absolute change from baseline)
Middleton also reported a significantly greater reduction in sweat chloride in the treatment group compared to the placebo group at six months, MD ‐41.80 mmol/L (95% CI ‐44.33, ‐39.27) (Analysis 27.9) (Middleton 2019).
Participants with F508del/F508del
At one month, two studies (135 participants) reported that triple therapy with elexacaftor 200 mg showed a greater decrease in sweat chloride than placebo, MD ‐44.32 mmol/L (95% CI ‐48.80 to ‐39.60) (Analysis 28.6) (Heijerman 2019; Keating 2018).
28.6. Analysis.

Comparison 28: Elexacaftor (200 mg once daily) tezacaftor (100 mg once daily) plus ivacaftor 150 mg twice daily versus placebo‐tez‐iva‐ F508del/F508del, Outcome 6: Sweat chloride (absolute change from baseline)
Elexacaftor plus tezacaftor plus VX‐561
Participants with F508del/MF
Keating also reported a decrease in sweat chloride at one month for this intervention, MD ‐34.60 mmol/L (95% CI ‐45.15 to ‐24.05) (Analysis 26.5) (Keating 2018).
26.5. Analysis.

Comparison 26: Elexacaftor (200 mg once daily) tezacaftor (100 mg once daily) plus VX‐561 (150 mg once daily) versus placebo [F508del/MF], Outcome 5: Sweat chloride (change from baseline) [mmol/L]
6. Radiological measures of lung disease
Data for this outcome were not reported by any study (Davies 2018a; Davies 2018b; Heijerman 2019; Keating 2018; Middleton 2019).
7. Acquisition of respiratory pathogens
No study reported data on the acquisition of pre‐specified or any other clinically relevant pathogens (Davies 2018a; Davies 2018b; Heijerman 2019; Keating 2018; Middleton 2019).
8. Eradication of respiratory pathogens
Data on eradication of respiratory pathogens were not reported by any study (Davies 2018a; Davies 2018b; Heijerman 2019; Keating 2018; Middleton 2019).
9. Nutrition and growth
Data on nutrition and growth parameters were reported by two studies (Heijerman 2019; Middleton 2019).
ii. Short term (over one month and up to six months)
Elexacaftor plus tezacaftor plus ivacaftor
Participants with F508del/MF
Middleton reported on the change from baseline in weight (kg) and BMI z score at six months (Middleton 2019). Results favoured triple therapy for both weight, MD 2.90 kg (95% CI 2.40 to 3.40) (Analysis 27.10) and BMI z score, MD 0.30 (95% CI 0.17 to 0.43) (Analysis 27.11).
27.10. Analysis.

Comparison 27: Elexacaftor (200 mg once daily) tezacaftor (100 mg once daily) plus ivacaftor 150 mg twice daily versus triple placebo‐ F508del/MF, Outcome 10: Weight (absolute change from baseline)
27.11. Analysis.

Comparison 27: Elexacaftor (200 mg once daily) tezacaftor (100 mg once daily) plus ivacaftor 150 mg twice daily versus triple placebo‐ F508del/MF, Outcome 11: BMI z score (absolute change from baseline)
Participants with F508del/F508del
The four‐week Phase 3 study reported a least squares mean for the change from baseline of both weight and BMI (Heijerman 2019). Investigators reported a significantly greater increase in weight in the elexacaftor group, MD 1.6 kg (95% CI 1.0 to 2.10) (Analysis 28.7). Similarly, there was a greater increase in BMI in the intervention group, MD 0.6 kg/m² (95% CI 0.41 to 0.79) (Analysis 28.8).
28.7. Analysis.

Comparison 28: Elexacaftor (200 mg once daily) tezacaftor (100 mg once daily) plus ivacaftor 150 mg twice daily versus placebo‐tez‐iva‐ F508del/F508del, Outcome 7: Weight (change from baseline)
28.8. Analysis.

Comparison 28: Elexacaftor (200 mg once daily) tezacaftor (100 mg once daily) plus ivacaftor 150 mg twice daily versus placebo‐tez‐iva‐ F508del/F508del, Outcome 8: BMI (change from baseline)
Discussion
Class II variants of the CFTR gene are defined as those that form a full length of protein, but the abnormal protein does not reach the cell membrane in any significant quantity. This is referred to as a trafficking defect. F508del, the most prevalent variant to cause CF, is a class II variant. A therapy that corrects the F508del trafficking defect would have a profound impact on the field of CF, providing a treatment option for the majority of pwCF.
Summary of main results
We identified 19 eligible RCTs evaluating correctors for pwCF and class II CFTR mutations (Boyle 2014; Clancy 2012; Davies 2018a; Davies 2018bDonaldson 2014; Donaldson 2017; Donaldson 2018; Horsley 2017; Keating 2018; McCarty 2002; PROGRESS 2017; Ratjen 2017; Rubenstein 1998; Taylor‐Cousar 2017; TRAFFIC 2015; TRANSPORT 2015; Zeitlin 2002). Eight studies examined monotherapy with different correctors (Boyle 2014; Clancy 2012; Donaldson 2014; Donaldson 2017; Horsley 2017; McCarty 2002; Rubenstein 1998; Zeitlin 2002). Seven studies (including the multi‐arm Boyle trial) examined dual combination therapy of either lumacaftor‐ivacaftor or tezacaftor‐ivacaftor (Boyle 2014; Donaldson 2018; PROGRESS 2017; Ratjen 2017; Taylor‐Cousar 2017; TRAFFIC 2015; TRANSPORT 2015). Four of these were well‐powered Phase 3 studies that enrolled pwCF (including children aged 6 to 11 years) with two copies of the F508del variant (F508del homozygotes) (Ratjen 2017; Taylor‐Cousar 2017; TRAFFIC 2015; TRANSPORT 2015). Five studies examined triple combination therapy, a combination of a novel corrector with tezacaftor and ivacaftor (Davies 2018a; Davies 2018b; Heijerman 2019; Keating 2018; Middleton 2019); two of these were Phase 3 studies of the combination elexacaftor‐tezacaftor‐ivacaftor (Heijerman 2019; Middleton 2019).
Monotherapy versus control
Early phase trials evaluated potential molecules 4PBA (Rubenstein 1998; Zeitlin 2002), CPX (McCarty 2002), N6022 (Donaldson 2014), cavosonstat (Donaldson 2017), lumacaftor (Boyle 2014; Clancy 2012;) and FDL169 (Horsley 2017). No study reported on survival and there were only limited data available for QoL which did not show any clinically relevant improvements. There was no significant impact on clinical outcomes (including sweat chloride) with either 4BPA, CPX or N6022 and Phase 3 studies of these drugs were not conducted. The study of FDL169 versus placebo indicated a significant improvement in the absolute change in FEV1 % predicted at the 400 mg dose, MD 4.68 % predicted (95% CI 0.12 to 9.24) (Analysis 5.2). Though significant, it is uncertain whether this improvement is clinically significant, meaning that based on the strength of relevant evidence currently we can only say that this intervention may lead to a benefit for pwCF (Horsley 2017). There are no significant concerns in safety for any corrector at any dose when compared to placebo. In an early phase study of cavosonstat monotherapy, there was a reduction in sweat chloride of ‐4.1 mmol/L (P = 0.032) at the highest dose (200 mg), however this reduction was not considered significant. There was a modest improvement in sweat chloride with lumacaftor alone compared with placebo after one month, MD ‐8.21 mmol/L (95% CI ‐14.30 to ‐2.12) (Clancy 2012), but not sufficient to warrant investigation of this agent as monotherapy in later phase studies. A significant MD was observed in the change from baseline of sweat chloride for the 600 mg dose of FDL169 versus placebo, in this case showing FDL169 to increase sweat chloride level versus placebo, MD 8.84 mmol/L (95% CI 1.40 to 16.28) (Analysis 5.4).
We have identified a further ongoing study of cavosonstat, which may potentially be eligible for inclusion in this review at a later date (NCT02589236) and one abstract stated that FDL169 will be studied in combination with a potentiator FDL176 (Horsley 2017).
Dual therapy versus control
Four studies with 1374 participants compared lumacaftor plus ivacaftor to placebo (Boyle 2014; Ratjen 2017; TRAFFIC 2015; TRANSPORT 2015) and two studies with 528 participants compared tezacaftor plus ivacaftor to placebo or to ivacaftor alone (i.e. tezacaftor placebo) (Donaldson 2018; Taylor‐Cousar 2017). The efficacy outcomes (primary and secondary) for the tezacaftor‐ivacaftor Phase 3 study were similar to those reported with lumacaftor‐ivacaftor (Taylor‐Cousar 2017). All participants had the F508del/F508del genotype.
No deaths were reported during any of the included studies (Boyle 2014; Donaldson 2018; Ratjen 2017; Taylor‐Cousar 2017; TRAFFIC 2015; TRANSPORT 2015) (high to moderate‐quality evidence). In participants allocated to the lumacaftor‐ivacaftor combination, combined trial data demonstrated no difference with regards to change in a generic measure of QoL (measured by the EQ‐5L‐3D tool). There was a significant improvement in the respiratory domain of the CF‐specific QoL measure (CFQ‐R) at six months, MD 2.62 (95% CI 0.64 to 4.59) (Analysis 11.2) (moderate‐quality evidence). The tezacaftor‐ivacaftor study enrolled adults and young pwCF (from 12 years and with a mean age of approximately 26 years). A subsequent abstract reported each domain of the validated QoL score (CFQ‐R), in contrast to exclusively reporting the respiratory domain. Five of 12 domains demonstrated significant improvement for the pwCF on tezacaftor‐ivacaftor (Taylor‐Cousar 2017). Data from this study (n = 510) found a significant difference in the respiratory domain of the CFQ‐R at six months in favour of the treatment group, MD 5.10 (95% CI 3.20 to 7.00) (Taylor‐Cousar 2017; Analysis 16.1). An improvement of four points on this scale is considered the minimal clinically important difference (MCID) for this outcome measure (Quittner 2009; Ramsey 2011). This means that, based on moderate‐quality evidence for these interventions and this outcome, lumacaftor‐ivacaftor likely would not make a MCID to CFQ‐R, but tezacaftor‐ivacaftor likely would make a MCID to CFQ‐R.
With respect to respiratory function (as measured by FEV1 % predicted), at six months there were significant differences in change from baseline in favour of the lumacaftor‐ivacaftor combination over placebo in both relative change, MD 5.21 (95% CI 3.61 to 6.80) (Analysis 11.4) (high‐quality evidence) and when the two lumacaftor doses were pooled in absolute change, MD 3.07 (95% CI 2.17 to 3.97) (Analysis 11.5) (moderate‐quality evidence). In one tezacaftor‐ivacaftor study (n = 510) participants in the intervention group demonstrated a significantly higher relative change from baseline in FEV1 (% predicted) compared to the placebo group, MD 6.80 (95% CI 5.30 to 8.30) (Analysis 16.13) (moderate‐quality evidence) as well as a significantly higher absolute change from baseline in FEV1 % predicted, MD 4.00 (95% CI 3.10 to 4.90) (Analysis 16.14) (Taylor‐Cousar 2017) (moderate‐quality evidence). Improvement in FEV1 is considered an important surrogate outcome measure for pwCF. The European Medicines Agency (EMA) has suggested that "as FEV1 is linked to mortality, any significant difference between placebo and active treatment is potentially clinically relevant" (EMA 2012); therefore based on effect size and strength of evidence, both lumacaftor‐ivacaftor and tezacaftor‐ivacaftor likely make an improvement to FEV1 when compared to control. In the study protocol, the MCID in absolute change in FEV1 % predicted used to calculate the sample sizes for the TRAFFIC and TRANSPORT studies was 5% (TRAFFIC 2015; TRANSPORT 2015). This magnitude of improvement in respiratory function was not achieved with the lumacaftor‐ivacaftor combination. In a post hoc change to the protocol, the primary outcome for TRAFFIC and TRANSPORT was altered from absolute change from baseline in FEV1 % predicted at six months to an average of the FEV1 values at four and six months. The study on children reported the change in LCI as its primary outcome; although this measure is a well‐validated research outcome assessing respiratory function, it is not yet routinely used in clinical practice. The children allocated to lumacaftor‐ivacaftor demonstrated a significant reduction in LCI compared to those receiving placebo, least squares MD ‐1.10 (95% CI ‐1.40 to ‐0.80) (Analysis 14.3). Although this difference is significant, it is difficult to assess the clinical relevance of this result for young pwCF. A study involving a subgroup of participants (n = 10, seven in the active treatment group and three in the placebo group) reported no significant improvement in chest CT scan score from baseline to 24 weeks; this was a secondary outcome in our review (Analysis 14.6; Analysis 14.7; Analysis 14.8; Ratjen 2017).
A number of this review's important secondary outcomes were reported in the studies that were included in this review. Overall the safety data reported for the lumacaftor‐ivacaftor combination were reassuring, but there was clear evidence of increased reporting of early respiratory compromise, OR 2.05 (99% CI 1.10 to 3.83) (Analysis 9.6). The aetiology of this event is unclear and it was reported to settle after a few weeks if the intervention was continued (TRAFFIC 2015; TRANSPORT 2015). Two participants were withdrawn because of hypertension (one in the follow‐up study (PROGRESS 2017). For participants (n = 80) receiving 400 mg twice a day of lumacaftor there was a significant mean (SE) increase in systolic blood pressure of 5.1 (1.5) mm Hg and in diastolic blood pressure of 4.1 (1.2) mm Hg (PROGRESS 2017). For children (aged 6 to 11 years) enrolled in the Phase 3 study of lumacaftor‐ivacaftor combination therapy, the safety profile reported was similar to the TRAFFIC and TRANSPORT studies, including transient early respiratory compromise and infrequent elevation in serum transaminases (liver enzymes) (Ratjen 2017). There was no increased reporting of adverse events for the tezacaftor‐ivacaftor Phase 3 study, in particular the early transient dyspnoea reported with the lumacaftor‐ivacaftor combination, and no increased withdrawals of tezacaftor‐ivacaftor participants compared to those receiving placebo (Taylor‐Cousar 2017).
In the TRAFFIC and TRANSPORT studies, pulmonary exacerbations were reported more frequently in participants allocated to placebo compared to those receiving the lumacaftor‐ivacaftor combination (Analysis 9.6; Analysis 10.6) (TRAFFIC 2015; TRANSPORT 2015); pulmonary exacerbations are challenging to record accurately, but important to pwCF. The tezacaftor‐ivacaftor study reported the time to first pulmonary exacerbation and found a significantly decreased HR in the intervention group versus the placebo group (Taylor‐Cousar 2017). Additionally, BMI improved in participants allocated to the lumacaftor‐ivacaftor combination therapy after six months (Analysis 9.10; Analysis 10.10). Early phase studies of lumacaftor combined with ivacaftor demonstrated a greater magnitude of effect with a reduction in sweat chloride compared to lumacaftor monotherapy with the higher dose of ivacaftor, MD ‐10.9 mmol/L (95% CI ‐17.6 to ‐4.2) (Analysis 13.3; Boyle 2014). Although the tezacaftor‐ivacaftor study recruited fewer participants than TRAFFIC/TRANSPORT, the results were similar with respect to secondary outcomes (Taylor‐Cousar 2017). Data on school or work attendance, acquisition or eradication of microbial pathogens, or radiological outcomes were not reported for any study.
Triple therapy versus control or dual therapy
A number of agents have been evaluated in combination with tezacaftor‐ivacaftor (triple therapy) in the five studies included in this comparison (Davies 2018a; Davies 2018b; Heijerman 2019; Keating 2018; Middleton 2019). One triple combination, elexacaftor‐tezacaftor‐ivacaftor, was taken forward for Phase 3 studies for pwCF with one or two F508del variants (Middleton 2019; Heijerman 2019). For pwCF with one F508del variant, this was the first exposure to a variant specific therapy and the comparator was a placebo (Middleton 2019). For those with two F508del variants, the participants were already on tezacaftor‐ivacaftor and this was the comparator used for the study (Heijerman 2019).
No deaths were reported in any of the included studies (Davies 2018a; Davies 2018b; Heijerman 2019; Keating 2018; Middleton 2019) (high‐quality evidence).
In early phase studies (Davies 2018a; Davies 2018b; Keating 2018), at one month triple therapy combinations likely increased QoL across multiple doses for pwCF who have one or two F508del gene variants (Analysis 25.1; Analysis 26.1; Analysis 27.1; Analysis 28.1), but this effect was not seen in two of the doses of VX‐659 (240 mg and 400 mg) tested in people with the F508del/MF genotype (Davies 2018b; Keating 2018). For pwCF with two F508del variants, over one month elexacaftor‐tezacaftor‐ivacaftor improved QoL respiratory domain scores compared to tezacaftor‐ivacaftor combination therapy, MD 17.40 (95% CI 11.94 to 22.86) (Analysis 28.1; Heijerman 2019) (moderate‐quality evidence). Similarly, at six months elexacaftor‐tezacaftor‐ivacaftor improved QoL respiratory domain scores versus placebo in F508del/MF participants by a MD of 20.2 points (95% CI 16.2 to 24.2) (Analysis 27.1; Middleton 2019).
For triple combinations including VX‐659, there was a improvement in both absolute and relative change in FEV1 from baseline at one month compared to placebo for pwCF with one or two copies of F508del (Davies 2018b) (moderate‐quality evidence). Similar results were found for the elexacaftor combination (Keating 2018) (moderate‐quality evidence). For F508del/MF participants, at six months the elexacaftor‐tezacaftor‐ivacaftor group demonstrated an improvement in absolute change in FEV1 % predicted compared to placebo, MD 14.30 % predicted (95% CI 12.8 to 15.8) (Analysis 27.3; Middleton 2019) (moderate‐quality evidence). For pwCF with two F508del variants, at one month elexacaftor‐tezacaftor‐ivacaftor improved absolute change in FEV1, MD 10.0% predicted (95% CI 7.5 to 12.5) (Heijerman 2019; Analysis 28.3) (moderate‐quality evidence).
There was likely no difference in the occurrence of adverse events for any combination compared to placebo across both genotype groups (study period of four weeks) and no unexpected adverse events related to the study drug (moderate‐quality evidence) (Davies 2018a; Davies 2018b; Keating 2018). Elexacaftor‐tezacaftor‐ivacaftor led to no difference in the number or severity of adverse events compared to placebo or control (Heijerman 2019; Middleton 2019). One study showed a longer time to the next pulmonary exacerbation in participants with F508del/MF taking elexacaftor‐tezacaftor‐ivacaftor compared to placebo over the six months study (Middleton 2019). The number of pulmonary exacerbations were reported as an adverse event in the remaining studies. Data from two studies showed fewer exacerbations in F508del/F508del participants taking elexacaftor‐tezacaftor‐ivacaftor compared to control (Heijerman 2019; Keating 2018), but there was no difference found for other interventions or other genotypes at any time point.
Reductions in sweat chloride were reported in both the early and Phase 3 studies. In participants with two F508del variants, at one month there was a greater mean reduction in sweat chloride (mmol/L) in the elexacaftor‐tezacaftor ivacaftor group compared to the tezacaftor‐ivacaftor group, MD ‐44.32 mmol/L (95% C I ‐48.80 to ‐39.84) (Analysis 28.6; Heijerman 2019; Keating 2018). For F508del/MF participants, the reduction was similar at one month, MD ‐40.96 mmol/L (95% CI ‐43.60 to ‐38.33) (Analysis 27.9; Keating 2018; Middleton 2019) and at six months, MD ‐41.80 mmol/L (95% CI ‐44.3 to ‐39.3) (Analysis 27.9; Middleton 2019).
In two studies, triple therapy saw an improvement in measures of nutrition and growth versus control in participants with both F508del/F508del and F508del/MF genotypes (Heijerman 2019; Middleton 2019). In homozygous participants, the intervention saw a greater increase in weight, least squares MD 1.6 kg (95% CI 1.0 to 2.10) (Analysis 28.7), as well as a greater increase in BMI, MD 0.6 kg/m² (95% CI 0.41 to 0.79) (Analysis 28.8; Heijerman 2019). In the second study, heterozygous participants in the intervention group saw a greater increase in weight compared to control group, MD 2.90 kg (95% CI 2.40 to 3.40) (Analysis 27.10), and also a greater increase in BMI z score, MD 0.30 (95% CI 0.17 to 0.43) (Analysis 27.11; Middleton 2019).
Overall completeness and applicability of evidence
This review has examined evidence for efficacy and safety. We have not included outcomes relating to cost‐effectiveness.
Monotherapy versus control
The single‐agent studies enrolled participants with two copies of the F508del variant. These studies have not been taken forward on larger more representative populations into Phase 3 studies. New agents (such as cavosonstat) are currently being assessed in early phase studies (Donaldson 2017). Data for the FDL169 Phase 1 study were provided in a poster and conference abstract (Horsley 2017).
Dual therapy versus control
The Phase 2 study and the Phase 3 studies of both lumacaftor and tezacaftor combined with ivacaftor have examined this therapy for people with two copies of the F508del variant (F508del homozygotes) (Donaldson 2018; Ratjen 2017; Taylor‐Cousar 2017; TRAFFIC 2015; TRANSPORT 2015). The Phase 2 study of tezacaftor‐ivacaftor additionally examined the impact of this therapy on adults with one F508del variant and the G551D variant (Donaldson 2018); however, there have been no further Phase 3 studies for pwCF who are compound heterozygotes of F508del with another CF‐causing mutation. One cross‐over study has examined pwCF with one F508del variant combined with an ivacaftor‐sensitive residual function mutation, to evaluate any potential additive impact of tezacaftor on the recognised ivacaftor benefit (Rowe 2017). We excluded this study because of concerns over study design, in particular carryover effects of an intervention (ivacaftor) that has been shown to correct the basic defect in CF.
The Phase 3 studies of both the lumacaftor and ivacaftor dual therapy are well‐powered and provide clear statistical evidence of improvement in clinical outcomes, even if these are limited in magnitude compared to the changes anticipated in the protocol and to those reported for individuals with G551D receiving ivacaftor (Ratjen 2017; TRAFFIC 2015; TRANSPORT 2015). These Phase 3 studies were conducted across a large number of CF centres in North America, Europe and Australia, and the results are applicable to pwCF who are homozygous for F508del in these regions with mild to moderate lung disease.
The Phase 3 studies of lumacaftor‐ivacaftor enrolled children and adults (age range 6 to 64 years) (Ratjen 2017; TRAFFIC 2015; TRANSPORT 2015). For lumacaftor‐ivacaftor, results were consistent across age groups, although for the 24‐week study of 6 to 11 year olds the absolute change in FEV1 % predicted was less marked, MD 2.40 (95% CI 0.40 to 4.40) (Analysis 14.2; Ratjen 2017) (low‐quality evidence).
Triple therapy versus control
The Phase 1 study by Davies which was published as part of the same paper as the Phase 2 study, enrolled 12 pwCF with one copy of F508del and one MF variant (F508del/MF) and all were aged over 18 years; data on younger pwCF will be required (Davies 2018a).
The Phase 2 trials of triple therapy enrolled pwCF homozygous for F508del (F508del/F508del) and also pwCF F508del/MF. They did not include people under 18 years of age (Davies 2018b; Keating 2018); data on younger pwCF will be required.
The Phase 2 studies tested the triple therapy combination of VX‐659 or elexacaftor plus tezacaftor 100 mg once daily plus VX‐561, a deuterated form of ivacaftor that has a longer half‐life in the body than the typical ivacaftor formulation. This means it is taken once daily at the same dose (150 mg), rather than the typical 150 mg twice per day with standard ivacaftor. This combination was only tested in a group of participants with the F508del/MF heterozygous genotype, it is only used in combination with the maximum tested doses of VX‐659 and elexacaftor. The studies do not state why a combination of VX‐561 is tested in these trials, or why it is only tested in people with F508del/MF genotypes, or why it is only tested in combination with the maximum doses of the above medications (Davies 2018b; Keating 2018).
Two Phase 3 studies have tested elexacaftor‐tezacaftor‐ivacaftor versus placebo (for participants with F508del/MF) or versus tezacaftor‐ivacaftor (for participants with F508del/F508del); the studies spanned three continents and included adults and children 12 years and older (Heijerman 2019; Middleton 2019). The study on pwCF with one F508del variant was for six months (Middleton 2019), but the study on homozygotes was only one month in duration and longer studies are needed in this population (Heijerman 2019).
Quality of the evidence
Studies included in this review were often difficult to appraise and interpret due to complex study design that incorporated several drug doses and genotype combinations.
Monotherapy versus control
Authors of some studies were only able to provide abstracts or posters (or both) as sources of data. For the early phase studies of 4PBA, CPX, N6022 and FDL169 relevant outcome data to this review were limited and the risk of bias for various domains was difficult to judge. Important results for the drugs lumacaftor and cavosonstat within this comparison are summarised in the tables (Table 1; Table 2). We have not presented other monotherapy treatments in the summary of findings tables as interventions have not yet been taken forward on larger more representative populations in Phase 3 studies.
The quality of the evidence from a short‐term study of cavosonstat compared to placebo was low to very low due to concerns over unclear methodological design, indirectness (lack of applicability of results to children) and limited outcome data resulting in wide CIs around effect sizes (Table 2).
Dual therapy versus control
We judged the quality of the evidence from the three large multicentre RCTs of lumacaftor‐ivacaftor combination therapy to be moderate to high (Table 3). Not all outcomes were reported in the final study publications; some were available in the online supplement, some were extrapolated from graphical figures and others were available on the NIH database (ClinicalTrials.gov). Although the time‐point for assessment of the primary outcome changed after the data had been collected, from FEV1 % predicted at six months to an aggregate of four and six months (which was in fact a larger treatment effect), we did not judge this to reflect a high risk of bias. This was because the results at six months were also significant, and the amended protocol states that "This change was made during final review by senior management. It is important to note that this change was made based on theoretical considerations alone. No data analysis was used to support this change and, in fact, the spirometry data were maintained at the designated vendor and were not available to any Vertex personnel".
We judged the quality of the evidence from an additional large multicentre RCT of lumacaftor‐ivacaftor combination therapy to be moderate to low (Table 4). The study recruited children aged 6 to 11 years, so results are not applicable to other age groups. Not all outcomes were reported in the final study report and additional data could not be extracted from graphical figures. Furthermore the analysis approach taken within this review adjusted for earlier time points in the analysis at six months, therefore results should be interpreted as the treatment effect averaged from each study visit until six months.
We judged the quality of the evidence from two tezacaftor‐ivacaftor combination therapy studies (including one large multicentre RCT) to be of moderate quality (Table 6); results are not applicable to children under the age of 12 and some results are not applicable to individuals homozygous for F508del. Furthermore, in the large tezacaftor‐ivacaftor combination study, a number of outcomes which were not presented in the summary of findings table of this review were recorded according to the study protocol, but not presented in the published study report (Taylor‐Cousar 2017).
We judged the quality of the evidence from a small, very short‐term study of lumacaftor‐ivacaftor combination therapy and from a small study of lumacaftor monotherapy to be very low to moderate due to concerns over incomplete outcome data, selective reporting and limited outcome data resulting in wide CIs around effect sizes (Table 1; Table 5).
Triple therapy versus control
The early phase triple therapy studies were complex because they evaluated a number of factors; different doses, different genotypes (F508del/F508del and F508del/MF), different correctors and different forms of ivacaftor. This resulted in eight different comparator groups. The evidence for the comparison of VX‐659 plus tezacaftor plus ivacaftor or VX‐561 compared with control was judged to be moderate‐ to high‐quality (Table 7), but this intervention has not been taken beyond Phase 2 studies. However, elexacaftor was selected for Phase 3 studies in combination with tezacaftor and ivacaftor.
The Phase 3 studies of elexacaftor‐tezacaftor‐ivacaftor were high quality with respect to study design, implementation and reporting (Table 8). The studies were restricted to pwCF aged 12 years and older, which reduces GRADE classification to moderate overall. For the age group 12 years and above the evidence was strong with potential for considerable clinically significant benefit for pwCF with one or two F508del variants.
Potential biases in the review process
The review authors conducted a comprehensive literature search of the Cystic Fibrosis and Genetic Disorders Review Group's CF Trials Register, online trials databases (Appendix 1) and also manual searching of journal conference abstracts. Two authors individually applied the inclusion and exclusion criteria to the identified studies and excluded studies that were not relevant. Included studies were appraised more thoroughly and data extracted independently using a pre‐determined form. The authors assessed the risk of bias of the included studies and if they failed to reach a consensus on the risk of bias, a third author (KWS) arbitrated. The analyses were undertaken by two review authors (SP and IS for the original review and JM and IS for the first update) and checked for appropriateness by the review statistician (SN). This approach minimized the risks of bias in the review process.
None of the authors have received direct or indirect payments from the companies responsible for the development of any agents included in this review; however, KWS has previously attended and has organised educational events that have received financial support from Vertex, the company that has developed and is evaluating some of the agents included in this review (outside the time limits for declarations for Cochrane Conflict of Interest statements).
Not all results were reported in a format from which they could be accurately extracted, and so we have had to extrapolate data for several important outcomes from graphs and figures. We are awaiting confirmation from Vertex that these estimates are accurate. This review has assessed all available published study data. Study authors were contacted for relevant unpublished information and individual participant data. None have been made available to date. We are not aware of any unpublished trials.
Definitions of exacerbations varied between included studies and sometimes were not specifically defined by investigators as to what was recorded as an exacerbation. To incorporate data on exacerbations from different studies, the authors of this review set a broad definition of what they would record as an exacerbation (Types of outcome measures). This broad definition, together with variation between defining and recording exacerbations in included studies, means that synthesising and reporting data on exacerbations could be viewed as a limitation of this review.
Agreements and disagreements with other studies or reviews
The National Institute for Health and Care Excellence (NICE) in the UK has undertaken a health technology appraisal for lumacaftor‐ivacaftor which was published on 27 July 2016 (NICE 2016). The appraisal included the TRAFFIC, TRANSPORT and PROGRESS studies (PROGRESS 2017; TRAFFIC 2015; TRANSPORT 2015); the report concluded that the quality of these studies was generally good and that the results were generalisable to a UK population with mild‐moderate disease severity. The evidence review group (ERG) noted that there were significant effects on key outcomes compared with standard care alone, but it was unclear how clinically significant the effects were. Adverse event data were recorded as per the published papers, but withdrawals due to hypertension and the overall increase in blood pressure in participants receiving 400 mg twice a day were not recorded. In addition, the ERG examined a detailed cost‐effectiveness assessment (including an estimate of incremental cost‐effectiveness ratio) and concluded, on that basis, that lumacaftor‐ivacaftor is not recommended, within its marketing authorisation, for treating CF in people 12 years and older who are homozygous for F508del mutation of the CFTR gene.
An evaluation of the safety of lumacaftor and ivacaftor highlighted the finding of "transaminitis" (raised transaminases) in ivacaftor and combination studies (Talamo Guervara 2017). In addition, the review reported non‐congenital cataracts identified in pre‐clinical studies and in children taking ivacaftor and combined therapy. The review also highlighted that lumacaftor is a strong inducer of the liver enzyme, cytochrome P3A and the implications for co‐prescribing of drugs metabolised through this route.
A review, and meta‐analysis published in December 2018 examined efficacy and safety of dual therapy with CFTR correctors and potentiators (Wu 2018). It looked at pwCF with F508del/F508del (monotherapy not assessed). Two studies included in this Cochrane Review were not included in the Wu review, although they did meet the eligibility criteria (PROGRESS 2017; Taylor‐Cousar 2017). Also, for the Boyle study, we included data from cohort 1, but not cohorts 2 and 3 due to concerns over pooling the control group (Boyle 2014); the Wu review includes these data. Furthermore, we included heterozygous participants from the 2018 Donaldson tezacaftor‐ivacaftor study, due to other participants being pooled which negated the effects of randomisation (Donaldson 2018). The Wu review includes all pooled and unpooled participants (including those not homozygous for F508del), impacting on potential bias by disrupting randomisation and blinding. We did not include pooled placebo data in our review, which explains the different number of participants. The Wu review presents a meta‐analysis of efficacy data for both lumacaftor‐ivacaftor and tezacaftor‐ivacaftor therapies, consistent with our data. Finally, Wu did not report the adverse event of hypertension found with lumacaftor‐ivacaftor therapy which we reported. The strong conclusions of the Wu review are not supported by their meta‐analysis and overstate improvement in efficacy measures. In addition, the authors claim to demonstrate a dose‐response effect, but there is no evidence of this from the data presented. Some interpretation within the Wu review is based on observational and "experimental" studies not included in the review, rather than evidence from their meta‐analysis.
This is the first systematic review to consider triple therapies.
Authors' conclusions
Implications for practice.
There is no evidence to support monotherapy with a corrector for people with cystic fibrosis (pwCF) who have two F508del variants (F508del/F508del).
There is some evidence to support dual therapies (lumacaftor‐ivacaftor and tezacaftor‐ivacaftor) for pwCF with the genotype F508del/F508del. There are still no data to assess the effectiveness of tezacaftor‐ivacaftor in children. There are no new data on these compounds to alter the conclusions presented in the previous version of this review (Southern 2018).
Combined data from Phase 3 studies of dual therapy with both lumacaftor and tezacaftor combined with ivacaftor demonstrate small but consistent improvements in key clinical outcomes. The size and quality of evidence from the studies gives us confidence in the validity of these results. Overall the drugs were well‐tolerated, but important adverse effects were reported, in particular with the lumacaftor‐ivacaftor combination. Adverse events noted with lumacaftor‐ivacaftor were not recorded in the tezacaftor‐ivacaftor studies and this combination appears to have a more acceptable safety profile.
In children younger than 12 years of age, there are no data to assess tezacaftor‐ivacaftor. In a study of lumacaftor‐ivacaftor in children aged 6 to 11 years, there was some evidence of clinical efficacy (decreasing lung clearance index (LCI) value), but the clinical relevance of these changes is not clear. The reports of increased adverse events for lumacaftor‐ivacaftor in this age group and in older pwCF should be taken into account when considering this intervention for this age group until further data or an alternative agent (e.g. tezacaftor‐ivacaftor) are available.
The results of Phase 3 studies of triple therapy of elexacaftor‐tezacaftor‐ivacaftor were consistent with early phase studies of triple therapy. The triple combination had an acceptable safety profile and tolerability with significant improvements in respiratory function and quality of life (QoL) compared to placebo in pwCF with one F508del variant and to tezacaftor‐ivacaftor in pwCF with two F508del variants with mild to moderate lung disease. The magnitude of the reported improvements in efficacy measures suggests the potential of these agents to provide a significant intervention for pwCF with one or two F508del variants. Of most interest, was the magnitude of improvement seen in QoL, measured through a validated disease‐specific tool (the CFQ‐R). This is one of the primary outcomes included in this review with respect to the impact of this intervention on pwCF. However, studies in individuals with F508del/residual function genotypes have not yet been undertaken; therefore, we do not yet know if the therapies analysed in this review will see the same effects, or magnitude of effects in pwCF who have these genotypes.
Implications for research.
It is important that post‐market surveillance is undertaken for all agents that correct the molecular variant associated with F508del and other class II variants. It is clear that lumacaftor‐ivacaftor is associated with adverse effects, some of which have necessitated the withdrawal of therapy. Tezacaftor‐ivacaftor appears to have a more favourable safety profile, but there are no data in children younger than 12 years and close monitoring is required for all individuals on this drug combination.
Evidence of efficacy for the population of pwCF who have two copies of the F508del variant cannot be automatically translated to pwCF who have one copy of F508del or another class II variant (such as G85E) and research strategies need to be developed that assess impact on these individuals. Small numbers of potential participants for these studies makes this a challenge. It is encouraging that pwCF with F508del/MF genotypes have been included in the early phase studies of triple combination therapies. For new agents being developed, we would encourage their evaluation of people with both F508del/F508del and F508del/MF genotypes.
The current available data for the elexacaftor‐tezacaftor‐ivacaftor combination for pwCF with one or two F508del variants is limited to pwCF aged 12 years and older. Studies are needed to evaluate the impact of elexacaftor‐tezacaftor‐ivacaftor on pwCF under 12 years of age and those with more severe lung disease. There is also a need for information from longer‐term monitoring of this intervention.
As new variant‐specific therapies emerge, it is important that lessons learnt from this review are taken on board. Investigators should report clearly on methodological approaches to reduce the risk of bias, in particular with regards to random sequence generation, allocation concealment and blinding; they should also ensure that randomisation is maintained when analysing data. It is important that future studies examine and clearly report on outcomes relevant to pwCF and their families.
With novel therapies and approaches, reporting of adverse events is critical and this should be undertaken in a comprehensive and consistent manner.
What's new
| Date | Event | Description |
|---|---|---|
| 16 December 2020 | New search has been performed | A search of the Cystic Fibrosis and Genetic Disorders Review Group's Cystic Fibrosis Trials Register and registry searches identified 65 new references. Included studies There were two new references to one included monotherapy study previously listed as ongoing (Horsley 2017). There was one new reference to one already included dual combination study (Donaldson 2018), eight new references to a further dual combination study (Ratjen 2017) and seven references to another already included dual combination study (Taylor‐Cousar 2017). There were two new references to two further dual combination studies (TRAFFIC 2015; TRANSPORT 2015). Five new references describe three newly included triple combination studies which were previously listed as ongoing (trial registry entries) (Davies 2018a; Davies 2018b; Keating 2018) and five references to two further new triple combination studies (Heijerman 2019; Middleton 2019). Excluded studies Two references were to a newly excluded study (Drevinek 2017) and eight references were additional references to the already excluded studies (Chilvers 2017; Rowe 2017). Studies awaiting assessment Three references are to one new study of monotherapy (Rio‐CF). There was a single new reference to a dual therapy study (Wainwright 2019) and three references to a new study of dual therapy versus triple therapy versus placebo (Downey 2019). There were eight references to new triple therapy studies (Munck 2020; NCT03912233; PELICAN; Taylor‐Cousar 2019). Ongoing studies One reference was added to an already ongoing study of monotherapy (Meijer 2016) and four references were to two new ongoing studies of monotherapy (ALBATROSS; FLAMINGO). There was one reference to a new study looking at both monotherapy and dual combination therapy (Jain 2018) and four references to ongoing studies of dual therapy (NCT03625466; Schwarz 2020). A search of ongoing trials registers identified 25 references: one additional reference to an already included study; 15 references that were excluded; seven references to studies awaiting assessment; and two references to ongoing studies. |
| 16 December 2020 | New citation required and conclusions have changed | The title of the review has been changed to more accurately reflect its scope (previously 'Correctors (specific therapies for class II CFTR mutations) for cystic fibrosis'). The inclusion of a new comparison of triple combination therapy has been added and changed the conclusions of our review. One author (Dr Sanjay Patel) has stepped down and a new author (Dr Jared Murphy) has joined the team. |
History
Protocol first published: Issue 2, 2014 Review first published: Issue 8, 2018
| Date | Event | Description |
|---|---|---|
| 28 August 2018 | Amended | Wording in Background section of the Abstract revised with regard to the populations where CF occurs. |
Acknowledgements
The review authors would like to acknowledge help and support of the CF and Genetic Disorders Review Group in particular Nikki Jahnke and Tracey Remmington. Toby Lasserson and Newton Opiyo, from the Cochrane Editorial Unit, provided valuable and precise editorial oversight. We would also like to acknowledge the study investigators, Professors/Doctors Elborn, Boyle, Clancy, McCarty, Ratjen, Rubenstein, Taylor‐Cousar, Davies, Drevinek and Zeitlin, who engaged constructively with this review and thank them for providing additional requested information.
The current review team would also like to thank Dr Sanjay Patel for his contributions to the protocol and the original version of this review.
This project was supported by the National Institute for Health Research, via Cochrane Infrastructure funding to the Cochrane Cystic Fibrosis and Genetic Disorders Group. The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the Systematic Reviews Programme, NIHR, NHS or the Department of Health.
Appendices
Appendix 1. Search methods ‐ electronic searches
| Database/resource | Date searched | Seach strategy |
| US National Institutes of Health database (clinicaltrials.gov/) |
23 November 2020 | [Advanced Search Form] Condition or disease: cystic fibrosis Other terms: VX OR corrector Study type: Interventional Studies (Clinical Trials) |
| WHO ICTRP (www.who.int/ictrp/en/) |
23 November 2020 | Cystic fibrosis AND (VX OR corrector) |
| European Medicines Agency (www.clinicaltrialsregister.eu/) |
23 November 2020 | Cystic fibrosis AND (VX OR corrector) |
Data and analyses
Comparison 1. Lumacaftor versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1.1 FEV1 % predicted (absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 1.1.1 At up to 1 month | 1 | 61 | Mean Difference (IV, Fixed, 95% CI) | ‐1.90 [‐4.13, 0.33] |
| 1.2 Adverse effects: 100 mg and 200 mg lumacaftor groups (combined data) versus placebo at up to 1 month | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Subtotals only | |
| 1.2.1 Cough | 1 | 53 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.28 [0.28, 5.92] |
| 1.2.2 Headache | 1 | 53 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.13 [0.16, 8.04] |
| 1.2.3 Rales | 1 | 53 | Odds Ratio (M‐H, Fixed, 99% CI) | 3.20 [0.18, 57.82] |
| 1.2.4 Productive cough | 1 | 53 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.79 [0.27, 11.98] |
| 1.2.5 Dyspnoea | 1 | 53 | Odds Ratio (M‐H, Fixed, 99% CI) | 3.20 [0.18, 57.82] |
| 1.2.6 Pulmonary exacerbation | 1 | 53 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.50 [0.16, 14.31] |
| 1.2.7 Fatigue | 1 | 53 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.21 [0.12, 12.09] |
| 1.2.8 Fever | 1 | 53 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.50 [0.16, 14.31] |
| 1.2.9 Nasal congestion | 1 | 53 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.58 [0.07, 4.93] |
| 1.2.10 Wheezing | 1 | 53 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.13 [0.01, 2.91] |
| 1.2.11 Diarrhoea | 1 | 53 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.27 [0.02, 3.31] |
| 1.2.12 Oropharyngeal pain | 1 | 53 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.27 [0.02, 3.31] |
| 1.2.13 Upper respiratory tract infection | 1 | 53 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.45 [0.07, 31.52] |
| 1.2.14 Sinus congestion | 1 | 53 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.21 [0.01, 5.55] |
| 1.2.15 Respiration abnormal | 1 | 53 | Odds Ratio (M‐H, Fixed, 99% CI) | 4.85 [0.10, 243.04] |
| 1.2.16 Haemoptysis | 1 | 53 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.44 [0.03, 6.54] |
| 1.2.17 Constipation | 1 | 53 | Odds Ratio (M‐H, Fixed, 99% CI) | 2.54 [0.04, 147.25] |
| 1.2.18 Abdominal pain | 1 | 53 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.46 [0.01, 18.95] |
| 1.2.19 Myalgia | 1 | 53 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.46 [0.01, 18.95] |
| 1.2.20 Post‐tussive vomiting | 1 | 53 | Odds Ratio (M‐H, Fixed, 99% CI) | 2.54 [0.04, 147.25] |
| 1.2.21 Nausea | 1 | 53 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.48 [0.02, 106.10] |
| 1.2.22 Nasopharyngitis | 1 | 53 | Odds Ratio (M‐H, Fixed, 99% CI) | 3.66 [0.07, 193.30] |
| 1.2.23 Dizziness | 1 | 53 | Odds Ratio (M‐H, Fixed, 99% CI) | 3.66 [0.07, 193.30] |
| 1.2.24 Back pain | 1 | 53 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.48 [0.02, 106.10] |
| 1.2.25 Upper abdominal pain | 1 | 53 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.45 [0.07, 31.52] |
| 1.2.26 Sputum abnormal | 1 | 53 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.48 [0.02, 106.10] |
| 1.2.27 Epistaxis | 1 | 53 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.94 [0.04, 24.27] |
| 1.2.28 C‐reactive protein increased | 1 | 53 | Odds Ratio (M‐H, Fixed, 99% CI) | 2.54 [0.04, 147.25] |
| 1.2.29 Paranasal sinus hypersecretion | 1 | 53 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 1.2.30 Lung hyperinflation | 1 | 53 | Odds Ratio (M‐H, Fixed, 99% CI) | 2.54 [0.04, 147.25] |
| 1.3 Adverse effects: 200 mg lumacaftor group versus placebo at up to 1 month | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Subtotals only | |
| 1.3.1 Cough | 1 | 62 | Odds Ratio (M‐H, Fixed, 99% CI) | 3.43 [0.19, 60.73] |
| 1.3.2 Pulmonary exacerbation | 1 | 62 | Odds Ratio (M‐H, Fixed, 99% CI) | 2.72 [0.05, 156.17] |
| 1.3.3 Oropharyngeal pain | 1 | 62 | Odds Ratio (M‐H, Fixed, 99% CI) | 2.72 [0.05, 156.17] |
| 1.3.4 Nasal congestion | 1 | 62 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 1.3.5 Dizziness | 1 | 62 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 1.3.6 Prothrombin time prolonged | 1 | 62 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.59 [0.02, 113.01] |
| 1.3.7 Upper respiratory tract infection | 1 | 62 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 1.4 Adverse effects requiring study drug discontinuation at up to 1 month | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.4.1 25 mg lumacaftor | 1 | 35 | Odds Ratio (M‐H, Fixed, 95% CI) | 3.00 [0.11, 78.81] |
| 1.4.2 50 mg lumacaftor | 1 | 35 | Odds Ratio (M‐H, Fixed, 95% CI) | 3.00 [0.11, 78.81] |
| 1.4.3 100 mg lumacaftor | 1 | 34 | Odds Ratio (M‐H, Fixed, 95% CI) | 3.18 [0.12, 83.76] |
| 1.4.4 200 mg lumacaftor | 1 | 36 | Odds Ratio (M‐H, Fixed, 95% CI) | 2.84 [0.11, 74.42] |
| 1.5 Sweat chloride concentration (change from baseline at up to 1 month) [mmol/L] | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 1.5.1 100 mg lumacaftor | 1 | 34 | Mean Difference (IV, Fixed, 95% CI) | ‐6.13 [‐12.25, ‐0.01] |
| 1.5.2 200 mg lumacaftor | 1 | 36 | Mean Difference (IV, Fixed, 95% CI) | ‐8.21 [‐14.30, ‐2.12] |
| 1.6 Sweat chloride concentration (change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 1.6.1 At up to 1 month | 1 | 51 | Mean Difference (IV, Fixed, 95% CI) | ‐2.75 [‐7.65, 2.15] |
Comparison 2. Cavosonstat (N91115) (200 mg twice daily) versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 2.1 CFQR respiratory domain: absolute change from baseline | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 2.1.1 At up to 1 month | 1 | 24 | Mean Difference (IV, Fixed, 95% CI) | 3.80 [‐11.30, 18.90] |
| 2.2 CFQR eating domain: absolute change from baseline | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 2.2.1 At up to 1 month | 1 | 24 | Mean Difference (IV, Fixed, 95% CI) | 2.40 [‐2.75, 7.55] |
| 2.3 Adverse events occurring in > 10% of participants at up to 1 month | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Subtotals only | |
| 2.3.1 Cough | 1 | 26 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.05 [0.13, 8.17] |
| 2.3.2 Pulmonary exacerbation | 1 | 26 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.26 [0.00, 20.03] |
| 2.3.3 Chest discomfort | 1 | 26 | Odds Ratio (M‐H, Fixed, 99% CI) | 5.00 [0.08, 308.20] |
| 2.3.4 Fatigue | 1 | 26 | Odds Ratio (M‐H, Fixed, 99% CI) | 3.00 [0.13, 71.47] |
| 2.4 Sweat chloride | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 2.4.1 At up to 1 month | 1 | 24 | Mean Difference (IV, Fixed, 95% CI) | ‐3.30 [‐9.13, 2.53] |
Comparison 3. N6022 versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 3.1 FEV1 % predicted (relative change from baseline at up to 1 month) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 3.1.1 5 mg/day N6022 | 1 | 29 | Mean Difference (IV, Fixed, 95% CI) | ‐2.00 [‐5.31, 1.31] |
| 3.1.2 10 mg/day N6022 | 1 | 28 | Mean Difference (IV, Fixed, 95% CI) | ‐1.70 [‐4.73, 1.33] |
| 3.1.3 20 mg/day N6022 | 1 | 28 | Mean Difference (IV, Fixed, 95% CI) | ‐2.20 [‐5.28, 0.88] |
| 3.1.4 40 mg/day N6022 | 1 | 38 | Mean Difference (IV, Fixed, 95% CI) | ‐1.00 [‐3.06, 1.06] |
| 3.2 Treatment‐emergent adverse events (mild) at up to 1 month | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 3.2.1 5 mg/day N6022 | 1 | 29 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.48 [0.10, 2.30] |
| 3.2.2 10 mg/day N6022 | 1 | 28 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.45 [0.28, 7.64] |
| 3.2.3 20 mg/day N6022 | 1 | 28 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.58 [0.12, 2.88] |
| 3.2.4 40 mg/day N6022 | 1 | 38 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.25 [0.34, 4.59] |
| 3.3 Treatment‐emergent adverse events (moderate) at up to 1 month | 1 | 123 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.92 [0.41, 2.04] |
| 3.3.1 5 mg/day N6022 | 1 | 29 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.93 [0.18, 4.90] |
| 3.3.2 10 mg/day N6022 | 1 | 28 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.08 [0.20, 5.87] |
| 3.3.3 20 mg/day N6022 | 1 | 28 | Odds Ratio (M‐H, Fixed, 95% CI) | 2.71 [0.53, 13.85] |
| 3.3.4 40 mg/day N6022 | 1 | 38 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.25 [0.04, 1.48] |
| 3.4 Treatment‐emergent adverse events (serious or severe) at up to 1 month | 1 | 123 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.37 [0.35, 5.41] |
| 3.4.1 5 mg/day N6022 | 1 | 29 | Odds Ratio (M‐H, Fixed, 95% CI) | 4.50 [0.35, 57.11] |
| 3.4.2 10 mg/day N6022 | 1 | 28 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.65 [0.02, 17.51] |
| 3.4.3 20 mg/day N6022 | 1 | 28 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.65 [0.02, 17.51] |
| 3.4.4 40 mg/day N6022 | 1 | 38 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.00 [0.06, 17.25] |
Comparison 4. FDL169 (400 mg three times daily) versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 4.1 Mean change in CFQ‐R respiratory domain | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 4.1.1 At up to 1 month | 1 | 13 | Mean Difference (IV, Fixed, 95% CI) | 5.09 [‐2.72, 12.90] |
| 4.2 FEV1 % predicted absolute change (% points) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 4.2.1 At up to 1 month | 1 | 13 | Mean Difference (IV, Fixed, 95% CI) | 4.68 [0.12, 9.24] |
| 4.3 Adverse events at up to 1 month | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Subtotals only | |
| 4.3.1 Total number of participants experiencing at least 1 adverse events | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | 6.67 [0.21, 207.87] |
| 4.3.2 Serious adverse events | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.20 [0.02, 63.12] |
| 4.3.3 Headache | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | 6.00 [0.18, 196.26] |
| 4.3.4 Nasopharyngitis | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.20 [0.02, 63.12] |
| 4.3.5 Fatigue | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | 4.09 [0.05, 349.57] |
| 4.3.6 Blood CK increase | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | 4.09 [0.05, 349.57] |
| 4.3.7 Cough | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | 4.09 [0.05, 349.57] |
| 4.3.8 Flatulence | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 4.3.9 Respiratory exacerbation | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.33 [0.00, 28.33] |
| 4.3.10 Rhinorrhoea | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.20 [0.02, 63.12] |
| 4.3.11 Increased sputum | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 4.3.12 Abdominal pain | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.33 [0.00, 28.33] |
| 4.3.13 Dry mouth | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.33 [0.00, 28.33] |
| 4.3.14 Lethargy | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.17 [0.00, 11.99] |
| 4.3.15 Myalgia | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 4.3.16 Nasal congestion | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 4.3.17 Nausea | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 4.3.18 Oropharyngeal pain | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.20 [0.02, 63.12] |
| 4.3.19 Productive cough | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | 4.09 [0.05, 349.57] |
| 4.3.20 Upper respiratory tract infection | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.33 [0.00, 28.33] |
| 4.4 Sweat chloride change from baseline [mmol/L] | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 4.4.1 At up to 1 month | 1 | 13 | Mean Difference (IV, Fixed, 95% CI) | 2.47 [‐4.47, 9.41] |
Comparison 5. FDL169 (600 mg three times daily) versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 5.1 Mean change in CFQ‐R respiratory domain | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 5.1.1 At up to 1 month | 1 | 13 | Mean Difference (IV, Fixed, 95% CI) | ‐4.33 [‐12.01, 3.35] |
| 5.2 FEV1 % predicted absolute change (% points) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 5.2.1 At up to 1 month | 1 | 13 | Mean Difference (IV, Fixed, 95% CI) | 2.80 [‐1.82, 7.42] |
| 5.3 Adverse events at up to 1 month | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Subtotals only | |
| 5.3.1 Total number of participants experiencing at least 1 adverse events | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.06 [0.00, 4.00] |
| 5.3.2 Serious adverse events | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | 3.00 [0.04, 254.93] |
| 5.3.3 Headache | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.08 [0.00, 2.95] |
| 5.3.4 Nasopharyngitis | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.83 [0.02, 43.83] |
| 5.3.5 Fatigue | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.24 [0.00, 20.89] |
| 5.3.6 Blood CK increase | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 5.3.7 Cough | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.12 [0.00, 8.63] |
| 5.3.8 Flatulence | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 5.3.9 Infective respiratory exacerbation | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.20 [0.02, 63.12] |
| 5.3.10 Rhinorrhoea | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.20 [0.02, 63.12] |
| 5.3.11 Increased sputum | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | 8.33 [0.12, 599.51] |
| 5.3.12 Abdominal pain | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.20 [0.02, 63.12] |
| 5.3.13 Dry mouth | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.33 [0.00, 28.33] |
| 5.3.14 Lethargy | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.17 [0.00, 11.99] |
| 5.3.15 Myalgia | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | 8.33 [0.12, 599.51] |
| 5.3.16 Nasal congestion | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | 8.33 [0.12, 599.51] |
| 5.3.17 Nausea | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | 4.09 [0.05, 349.57] |
| 5.3.18 Oropharyngeal pain | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.33 [0.00, 28.33] |
| 5.3.19 Productive cough | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | 4.09 [0.05, 349.57] |
| 5.3.20 Upper respiratory tract infection | 1 | 13 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.33 [0.00, 28.33] |
| 5.4 Sweat chloride change from baseline [mmol/L] | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 5.4.1 At up to 1 month | 1 | 13 | Mean Difference (IV, Fixed, 95% CI) | 8.07 [0.98, 15.16] |
Comparison 6. FDL169 (800 mg three times daily) versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 6.1 Mean change in CFQ‐R respiratory domain | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 6.1.1 At up to 1 month | 1 | 15 | Mean Difference (IV, Fixed, 95% CI) | 8.84 [1.40, 16.28] |
| 6.2 FEV1 % predicted absolute change (% points) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 6.2.1 At up to 1 month | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 6.3 Adverse events at up to 1 month | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Totals not selected | |
| 6.3.1 Total number of participants experiencing at least 1 adverse events | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Totals not selected | |
| 6.3.2 Serious adverse events | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Totals not selected | |
| 6.3.3 Headache | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Totals not selected | |
| 6.3.4 Nasopharyngitis | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Totals not selected | |
| 6.3.5 Fatigue | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Totals not selected | |
| 6.3.6 Blood CK increase | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Totals not selected | |
| 6.3.7 Cough | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Totals not selected | |
| 6.3.8 Flatulence | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Totals not selected | |
| 6.3.9 Infective respiratory exacerbation | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Totals not selected | |
| 6.3.10 Rhinorrhoea | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Totals not selected | |
| 6.3.11 Increased sputum | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Totals not selected | |
| 6.3.12 Abdominal pain | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Totals not selected | |
| 6.3.13 Dry mouth | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Totals not selected | |
| 6.3.14 Lethargy | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Totals not selected | |
| 6.3.15 Myalgia | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Totals not selected | |
| 6.3.16 Nasal congestion | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Totals not selected | |
| 6.3.17 Nausea | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Totals not selected | |
| 6.3.18 Oropharyngeal pain | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Totals not selected | |
| 6.3.19 Productive cough | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Totals not selected | |
| 6.3.20 Upper respiratory tract infection | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Totals not selected | |
| 6.4 Sweat chloride change from baseline [mmol/L] | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 6.4.1 At up to 1 month | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected |
Comparison 7. CPX versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 7.1 Adverse events occurring in more than 3% of participants in all treatment groups (combined data) versus placebo at up to 1 month | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Subtotals only | |
| 7.1.1 Abdominal pain | 1 | 37 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.45 [0.01, 24.92] |
| 7.1.2 Asthenia | 1 | 37 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.65 [0.01, 39.69] |
| 7.1.3 Headache | 1 | 37 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.33 [0.01, 17.72] |
| 7.1.4 Pain | 1 | 37 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.45 [0.01, 24.92] |
| 7.1.5 Diarrhoea | 1 | 37 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.65 [0.01, 39.69] |
| 7.1.6 Dizziness | 1 | 37 | Odds Ratio (M‐H, Fixed, 99% CI) | 9.33 [0.32, 268.92] |
| 7.1.7 Lung disease | 1 | 37 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.45 [0.01, 24.92] |
| 7.1.8 Rhinitis | 1 | 37 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.45 [0.01, 24.92] |
Comparison 8. 4PBA versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 8.1 Adverse events at up to 1 month | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Subtotals only | |
| 8.1.1 Bad taste in mouth | 1 | 18 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.44 [0.01, 13.44] |
| 8.1.2 Diarrhoea | 1 | 18 | Odds Ratio (M‐H, Fixed, 99% CI) | 3.35 [0.04, 267.31] |
| 8.2 Participants requiring study drug termination or a reduced dosage at up to 1 month | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 8.2.1 30 g 4PBA | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected |
8.2. Analysis.

Comparison 8: 4PBA versus placebo, Outcome 2: Participants requiring study drug termination or a reduced dosage at up to 1 month
Comparison 9. Lumacaftor (600 mg once daily) plus ivacaftor (250 mg twice daily) versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 9.1 Quality of life ‐ Euro Quality of Life Scale (EuroQol) 5‐Dimension‐3 Level (EQ‐5D‐3L) Index Score (absolute change from baseline) | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 9.1.1 At 6 months | 2 | 715 | Mean Difference (IV, Fixed, 95% CI) | 0.00 [‐0.01, 0.02] |
| 9.2 Quality of life ‐ CFQ‐R respiratory domain (absolute change from baseline) | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 9.2.1 At up to 1 month | 2 | 739 | Mean Difference (IV, Fixed, 95% CI) | 3.32 [1.13, 5.51] |
| 9.2.2 At 6 months | 2 | 725 | Mean Difference (IV, Fixed, 95% CI) | 3.04 [0.76, 5.32] |
| 9.3 Quality of life ‐ EQ‐5D‐3L VAS Score (absolute change from baseline) | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 9.3.1 At 6 months | 2 | 712 | Mean Difference (IV, Fixed, 95% CI) | 2.24 [0.18, 4.31] |
| 9.4 FEV1 % predicted (relative change from baseline) | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 9.4.1 At 6 months | 2 | 720 | Mean Difference (IV, Fixed, 95% CI) | 5.63 [3.80, 7.47] |
| 9.5 FEV1 % predicted (absolute change from baseline) | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 9.5.1 At up to 1 month | 2 | 739 | Mean Difference (IV, Fixed, 95% CI) | 2.32 [1.34, 3.31] |
| 9.5.2 At 6 months | 2 | 720 | Mean Difference (IV, Fixed, 95% CI) | 3.34 [2.30, 4.38] |
| 9.6 Adverse events by end of study (at 6 months) | 2 | Odds Ratio (M‐H, Fixed, 99% CI) | Subtotals only | |
| 9.6.1 Any adverse event | 2 | 739 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.00 [0.37, 2.71] |
| 9.6.2 Discontinuation due to an adverse event | 2 | 739 | Odds Ratio (M‐H, Fixed, 99% CI) | 2.38 [0.67, 8.50] |
| 9.6.3 At least 1 serious adverse event | 2 | 739 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.73 [0.47, 1.13] |
| 9.6.4 Infective pulmonary exacerbation | 2 | 739 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.66 [0.45, 0.97] |
| 9.6.5 Cough | 2 | 739 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.72 [0.49, 1.08] |
| 9.6.6 Headache | 2 | 739 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.00 [0.59, 1.68] |
| 9.6.7 Haemoptysis | 2 | 739 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.04 [0.60, 1.81] |
| 9.6.8 Diarrhoea | 2 | 739 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.18 [0.61, 2.28] |
| 9.6.9 Abnormal respiration | 2 | 739 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.91 [0.94, 3.88] |
| 9.6.10 Increased sputum | 2 | 739 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.74 [0.44, 1.24] |
| 9.6.11 Dyspnoea | 2 | 739 | Odds Ratio (M‐H, Fixed, 99% CI) | 2.05 [1.10, 3.83] |
| 9.6.12 Nasopharyngitis | 2 | 739 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.55 [0.27, 1.10] |
| 9.6.13 Oropharyngeal pain | 2 | 739 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.52 [0.80, 2.89] |
| 9.6.14 Abdominal pain | 2 | 739 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.80 [0.39, 1.62] |
| 9.6.15 Fatigue | 2 | 739 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.03 [0.51, 2.08] |
| 9.6.16 Nausea | 2 | 739 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.04 [0.51, 2.11] |
| 9.6.17 Pyrexia | 2 | 739 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.03 [0.54, 1.98] |
| 9.6.18 Nasal congestion | 2 | 739 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.73 [0.39, 1.35] |
| 9.6.19 Upper respiratory tract infection | 2 | 739 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.21 [0.54, 2.70] |
| 9.7 Time to first pulmonary exacerbation | 2 | 739 | Hazard Ratio (IV, Fixed, 95% CI) | 0.70 [0.57, 0.87] |
| 9.8 Rate of exacerbations | 2 | 739 | Rate Ratio (IV, Fixed, 95% CI) | 0.70 [0.57, 0.87] |
| 9.9 Weight (kg) (absolute change from baseline) | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 9.9.1 At 6 months | 2 | 725 | Mean Difference (IV, Fixed, 95% CI) | 0.80 [0.42, 1.18] |
| 9.10 BMI (absolute change from baseline) | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 9.10.1 At up to 1 month | 2 | 739 | Mean Difference (IV, Fixed, 95% CI) | 0.01 [‐0.07, 0.09] |
| 9.10.2 At 6 months | 2 | 725 | Mean Difference (IV, Fixed, 95% CI) | 0.29 [0.16, 0.43] |
Comparison 10. Lumacaftor (400 mg twice daily) plus ivacaftor (250 mg twice daily) versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 10.1 Quality of life ‐ Euro Quality of Life Scale (EuroQol) 5‐Dimension‐3 Level (EQ‐5D‐3L) Index Score (absolute change from baseline) | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 10.1.1 At 6 months | 2 | 708 | Mean Difference (IV, Fixed, 95% CI) | 0.00 [‐0.01, 0.02] |
| 10.2 Quality of life ‐ CFQ‐R respiratory domain (absolute change from baseline) | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 10.2.1 At up to 1 month | 2 | 740 | Mean Difference (IV, Fixed, 95% CI) | 4.13 [1.94, 6.31] |
| 10.2.2 At 6 months | 2 | 720 | Mean Difference (IV, Fixed, 95% CI) | 2.18 [‐0.11, 4.47] |
| 10.3 Quality of life ‐ EQ‐5D‐3L VAS Score (absolute change from baseline) | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 10.3.1 At 6 months | 2 | 710 | Mean Difference (IV, Fixed, 95% CI) | 2.30 [0.25, 4.36] |
| 10.4 FEV1 % predicted (relative change from baseline) | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 10.4.1 At 6 months | 2 | 715 | Mean Difference (IV, Fixed, 95% CI) | 4.77 [2.93, 6.61] |
| 10.5 FEV1 % predicted (absolute change from baseline) | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 10.5.1 At up to 1 month | 2 | 740 | Mean Difference (IV, Fixed, 95% CI) | 2.42 [1.43, 3.40] |
| 10.5.2 At 6 months | 2 | 715 | Mean Difference (IV, Fixed, 95% CI) | 2.80 [1.75, 3.84] |
| 10.6 Adverse events by end of study (at 6 months) | 2 | Odds Ratio (M‐H, Fixed, 99% CI) | Subtotals only | |
| 10.6.1 Any adverse event | 2 | 738 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.77 [0.30, 1.96] |
| 10.6.2 Discontinuation due to an adverse event | 2 | 738 | Odds Ratio (M‐H, Fixed, 99% CI) | 2.91 [0.85, 10.03] |
| 10.6.3 At least 1 serious adverse event | 2 | 738 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.52 [0.33, 0.83] |
| 10.6.4 Infective pulmonary exacerbation | 2 | 738 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.57 [0.39, 0.84] |
| 10.6.5 Cough | 2 | 738 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.58 [0.39, 0.88] |
| 10.6.6 Headache | 2 | 738 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.00 [0.59, 1.68] |
| 10.6.7 Haemoptysis | 2 | 738 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.00 [0.58, 1.74] |
| 10.6.8 Diarrhoea | 2 | 738 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.51 [0.80, 2.85] |
| 10.6.9 Abnormal respiration | 2 | 738 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.50 [0.71, 3.14] |
| 10.6.10 Increased sputum | 2 | 738 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.73 [0.44, 1.22] |
| 10.6.11 Dyspnea | 2 | 738 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.75 [0.93, 3.32] |
| 10.6.12 Nasopharyngitis | 2 | 738 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.23 [0.68, 2.21] |
| 10.6.13 Oropharyngeal pain | 2 | 738 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.78 [0.38, 1.63] |
| 10.6.14 Abdominal pain | 2 | 738 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.03 [0.53, 2.01] |
| 10.6.15 Fatigue | 2 | 738 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.19 [0.60, 2.35] |
| 10.6.16 Nausea | 2 | 738 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.74 [0.91, 3.34] |
| 10.6.17 Pyrexia | 2 | 738 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.97 [0.50, 1.87] |
| 10.6.18 Nasal congestion | 2 | 738 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.51 [0.26, 1.02] |
| 10.6.19 Upper respiratory tract infection | 2 | 738 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.94 [0.93, 4.08] |
| 10.7 Time to first pulmonary exacerbation | 2 | 740 | Hazard Ratio (IV, Fixed, 95% CI) | 0.61 [0.49, 0.76] |
| 10.8 Rate of exacerbations | 2 | 740 | Rate Ratio (IV, Fixed, 95% CI) | 0.61 [0.49, 0.76] |
| 10.9 Weight (kg) (absolute change from baseline) | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 10.9.1 At 6 months | 2 | 723 | Mean Difference (IV, Fixed, 95% CI) | 0.65 [0.27, 1.03] |
| 10.10 BMI (absolute change from baseline) | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 10.10.1 At up to 1 month | 2 | 740 | Mean Difference (IV, Fixed, 95% CI) | 0.02 [‐0.06, 0.10] |
| 10.10.2 At 6 months | 2 | 723 | Mean Difference (IV, Fixed, 95% CI) | 0.25 [0.12, 0.39] |
Comparison 11. Lumacaftor (600 mg once daily or 400 mg twice daily) plus ivacaftor (250 mg twice daily) versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 11.1 Quality of life ‐ Euro Quality of Life Scale (EuroQol) 5‐Dimension‐3 Level (EQ‐5D‐3L) Index Score (absolute change from baseline) | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 11.1.1 At 6 months | 2 | 1061 | Mean Difference (IV, Fixed, 95% CI) | 0.00 [‐0.01, 0.01] |
| 11.2 Quality of life ‐ CFQ‐R respiratory domain (absolute change from baseline) | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 11.2.1 At up to 1 month | 2 | 1108 | Mean Difference (IV, Fixed, 95% CI) | 3.70 [1.81, 5.58] |
| 11.2.2 At 6 months | 2 | 1076 | Mean Difference (IV, Fixed, 95% CI) | 2.62 [0.64, 4.59] |
| 11.3 Quality of life ‐ EQ‐5D‐3L VAS Score (absolute change from baseline) | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 11.3.1 At 6 months | 2 | 1060 | Mean Difference (IV, Fixed, 95% CI) | 2.28 [0.50, 4.06] |
| 11.4 FEV1 % predicted (relative change from baseline) | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 11.4.1 At 6 months | 2 | 1072 | Mean Difference (IV, Fixed, 95% CI) | 5.21 [3.61, 6.80] |
| 11.5 FEV1 % predicted (absolute change from baseline) | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 11.5.1 At up to 1 month | 2 | 1108 | Mean Difference (IV, Fixed, 95% CI) | 2.37 [1.52, 3.22] |
| 11.5.2 At 6 months | 2 | 1072 | Mean Difference (IV, Fixed, 95% CI) | 3.07 [2.17, 3.97] |
| 11.6 Adverse events by end of study (at 6 months) | 2 | Odds Ratio (M‐H, Fixed, 99% CI) | Subtotals only | |
| 11.6.1 Any adverse event | 2 | 1108 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.87 [0.38, 2.02] |
| 11.6.2 Discontinuation due to an adverse event | 2 | 1108 | Odds Ratio (M‐H, Fixed, 99% CI) | 2.65 [0.83, 8.45] |
| 11.6.3 At least 1 serious adverse event | 2 | 1108 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.62 [0.42, 0.91] |
| 11.6.4 Infective pulmonary exacerbation | 2 | 1108 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.62 [0.44, 0.86] |
| 11.6.5 Cough | 2 | 1108 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.65 [0.46, 0.92] |
| 11.6.6 Headache | 2 | 1108 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.00 [0.64, 1.57] |
| 11.6.7 Haemoptysis | 2 | 1108 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.02 [0.63, 1.65] |
| 11.6.8 Diarrhea | 2 | 1108 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.34 [0.76, 2.37] |
| 11.6.9 Abnormal respiration | 2 | 1108 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.70 [0.89, 3.26] |
| 11.6.10 Increased sputum | 2 | 1108 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.73 [0.47, 1.14] |
| 11.6.11 Dyspnea | 2 | 1108 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.90 [1.08, 3.35] |
| 11.6.12 Nasopharyngitis | 2 | 1108 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.87 [0.51, 1.50] |
| 11.6.13 Oropharyngeal pain | 2 | 1108 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.14 [0.63, 2.06] |
| 11.6.14 Abdominal pain | 2 | 1108 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.91 [0.51, 1.65] |
| 11.6.15 Fatigue | 2 | 1108 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.11 [0.61, 2.03] |
| 11.6.16 Nausea | 2 | 1108 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.38 [0.76, 2.51] |
| 11.6.17 Pyrexia | 2 | 1108 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.00 [0.57, 1.76] |
| 11.6.18 Nasal congestion | 2 | 1108 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.62 [0.36, 1.07] |
| 11.6.19 Upper respiratory tract infection | 2 | 1108 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.57 [0.79, 3.11] |
| 11.7 Weight (kg) (absolute change from baseline) | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 11.7.1 At 6 months | 2 | 1081 | Mean Difference (IV, Fixed, 95% CI) | 0.72 [0.39, 1.05] |
| 11.8 BMI (absolute change from baseline) | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 11.8.1 At up to 1 month | 2 | 1108 | Mean Difference (IV, Fixed, 95% CI) | 0.02 [‐0.05, 0.08] |
| 11.8.2 At 6 months | 2 | 1081 | Mean Difference (IV, Fixed, 95% CI) | 0.27 [0.16, 0.39] |
Comparison 12. Lumacaftor (200 mg once daily) for 21 days plus ivacaftor (150 mg twice daily) for days 15 to 21 versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 12.1 FEV1 % predicted (absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 12.1.1 At 14 days (before addition of ivacaftor) | 1 | 41 | Mean Difference (IV, Fixed, 95% CI) | ‐1.80 [‐4.39, 0.79] |
| 12.1.2 At 21 days | 1 | 41 | Mean Difference (IV, Fixed, 95% CI) | 2.80 [‐1.39, 6.99] |
| 12.2 Adverse events occurring in 10% or more participants (from days 15 ‐ 21) | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Subtotals only | |
| 12.2.1 Cough | 1 | 41 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.06 [0.14, 8.09] |
| 12.2.2 Pulmonary Exacerbation | 1 | 41 | Odds Ratio (M‐H, Fixed, 99% CI) | 2.22 [0.08, 58.11] |
| 12.2.3 Oropharyngeal pain | 1 | 41 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.50 [0.02, 13.07] |
| 12.2.4 Nasal congestion | 1 | 41 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.50 [0.02, 13.07] |
| 12.2.5 Dizziness | 1 | 41 | Odds Ratio (M‐H, Fixed, 99% CI) | 5.81 [0.10, 341.36] |
| 12.2.6 Prothrombin time prolonged | 1 | 41 | Odds Ratio (M‐H, Fixed, 99% CI) | 5.81 [0.10, 341.36] |
| 12.2.7 Upper respiratory tract infection | 1 | 41 | Odds Ratio (M‐H, Fixed, 99% CI) | 5.81 [0.10, 341.36] |
| 12.3 Sweat chloride concentration (mmol/L) (change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 12.3.1 At 14 days (before addition of ivacaftor) | 1 | 34 | Mean Difference (IV, Fixed, 95% CI) | ‐3.10 [‐8.58, 2.38] |
| 12.3.2 At 21 days | 1 | 33 | Mean Difference (IV, Fixed, 95% CI) | ‐5.00 [‐11.61, 1.61] |
Comparison 13. Lumacaftor (200 mg once daily) for 21 days plus ivacaftor (250 mg twice daily) for days 15 to 21 versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 13.1 FEV1 % predicted (absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 13.1.1 At 14 days (before addition of ivacaftor) | 1 | 41 | Mean Difference (IV, Fixed, 95% CI) | ‐2.00 [‐4.66, 0.66] |
| 13.1.2 At 21 days | 1 | 39 | Mean Difference (IV, Fixed, 95% CI) | 0.20 [‐4.20, 4.60] |
| 13.2 Adverse events occurring in 10% or more participants (from days 15 ‐ 21) | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Subtotals only | |
| 13.2.1 Cough | 1 | 41 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.22 [0.01, 4.52] |
| 13.2.2 Pulmonary Exacerbation | 1 | 41 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.05 [0.03, 44.10] |
| 13.2.3 Oropharyngeal pain | 1 | 41 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.06 [0.07, 15.89] |
| 13.2.4 Nasal congestion | 1 | 41 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.68 [0.14, 20.50] |
| 13.2.5 Dizziness | 1 | 41 | Odds Ratio (M‐H, Fixed, 99% CI) | 3.31 [0.05, 239.61] |
| 13.2.6 Prothrombin time prolonged | 1 | 41 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 13.2.7 Upper respiratory tract infection | 1 | 41 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 13.3 Sweat chloride concentration (mmol/L) (change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 13.3.1 At 14 days (before addition of ivacaftor) | 1 | 34 | Mean Difference (IV, Fixed, 95% CI) | ‐2.40 [‐8.00, 3.20] |
| 13.3.2 At 21 days | 1 | 33 | Mean Difference (IV, Fixed, 95% CI) | ‐10.90 [‐17.60, ‐4.20] |
Comparison 14. Lumacaftor (200 mg twice daily) plus ivacaftor (250 mg twice daily) versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 14.1 Quality of life ‐ CFQ‐R respiratory domain (absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 14.1.1 At 6 months | 1 | 204 | Mean Difference (IV, Fixed, 95% CI) | 2.50 [‐0.10, 5.10] |
| 14.2 FEV1 % predicted (absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 14.2.1 At 6 months | 1 | 204 | Mean Difference (IV, Fixed, 95% CI) | 2.40 [0.40, 4.40] |
| 14.3 LCI2.5 (absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 14.3.1 At 6 months | 1 | 204 | Mean Difference (IV, Fixed, 95% CI) | ‐1.10 [‐1.40, ‐0.80] |
| 14.4 Treatment‐emergent adverse events with incidence > 10% in any treatment group (at 6 months) | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 14.4.1 Any adverse event | 1 | 204 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.60 [0.14, 2.58] |
| 14.4.2 Any serious adverse event | 1 | 204 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.18 [0.50, 2.78] |
| 14.4.3 Cough | 1 | 204 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.93 [0.53, 1.61] |
| 14.4.4 Pulmonary exacerbation | 1 | 204 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.11 [0.55, 2.25] |
| 14.4.5 Productive cough | 1 | 204 | Odds Ratio (M‐H, Fixed, 95% CI) | 3.35 [1.27, 8.84] |
| 14.4.6 Nasal congestion | 1 | 204 | Odds Ratio (M‐H, Fixed, 95% CI) | 2.30 [0.94, 5.60] |
| 14.4.7 Oropharyngeal pain | 1 | 204 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.55 [0.66, 3.64] |
| 14.4.8 Pyrexia | 1 | 204 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.69 [0.33, 1.44] |
| 14.4.9 Upper abdominal pain | 1 | 204 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.94 [0.74, 5.08] |
| 14.4.10 Headache | 1 | 204 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.48 [0.60, 3.63] |
| 14.4.11 Upper respiratory tract infection | 1 | 204 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.31 [0.55, 3.15] |
| 14.4.12 Sputum increased | 1 | 204 | Odds Ratio (M‐H, Fixed, 95% CI) | 5.92 [1.28, 27.42] |
| 14.4.13 Abdominal pain | 1 | 204 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.98 [0.39, 2.46] |
| 14.4.14 Nausea | 1 | 204 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.10 [0.43, 2.83] |
| 14.4.15 Rhinorrhoea | 1 | 204 | Odds Ratio (M‐H, Fixed, 95% CI) | 2.06 [0.68, 6.27] |
| 14.4.16 Vomiting | 1 | 204 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.98 [0.39, 2.46] |
| 14.4.17 Fatigue | 1 | 204 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.78 [0.31, 1.98] |
| 14.4.18 Respiratory events | 1 | 204 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.53 [0.71, 3.29] |
| 14.5 Sweat chloride concentration (absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 14.5.1 At up to 1 month | 1 | 204 | Mean Difference (IV, Fixed, 95% CI) | ‐20.80 [‐23.40, ‐18.20] |
| 14.6 CT Brody score (mean change) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 14.6.1 At 6 months | 1 | 10 | Mean Difference (IV, Fixed, 95% CI) | ‐16.70 [‐36.05, 2.65] |
| 14.7 CT Brody score bronchiectasis score (mean change) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 14.7.1 At 6 months | 1 | 10 | Mean Difference (IV, Fixed, 95% CI) | ‐2.40 [‐4.96, 0.16] |
| 14.8 CT Brody score air trapping score (mean change) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 14.8.1 At 6 months | 1 | 10 | Mean Difference (IV, Fixed, 95% CI) | ‐6.60 [‐20.77, 7.57] |
| 14.9 BMI (absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 14.9.1 At 6 months | 1 | 204 | Mean Difference (IV, Fixed, 95% CI) | 0.10 [‐0.10, 0.30] |
| 14.10 BMI for age z‐score (absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 14.10.1 At 6 months | 1 | 204 | Mean Difference (IV, Fixed, 95% CI) | 0.00 [‐0.10, 0.10] |
Comparison 15. Lumacaftor (200 mg once daily monotherapy for 14 days) plus ivacaftor (150 mg or 250 mg twice daily for days 15 to 21) for 21 days.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 15.1 FEV1 % predicted (absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 15.1.1 At 21 days | 1 | 59 | Mean Difference (IV, Fixed, 95% CI) | 1.57 [‐2.13, 5.27] |
| 15.2 Adverse events occurring in 10% or more participants (from days 15 ‐ 21) | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Subtotals only | |
| 15.2.1 Cough | 1 | 61 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.61 [0.09, 4.01] |
| 15.2.2 Pulmonary exacerbation | 1 | 61 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.62 [0.08, 34.55] |
| 15.2.3 Oropharyngeal pain | 1 | 61 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.77 [0.07, 9.03] |
| 15.2.4 Nasal congestion | 1 | 61 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.06 [0.10, 11.04] |
| 15.2.5 Dizziness | 1 | 61 | Odds Ratio (M‐H, Fixed, 99% CI) | 4.01 [0.08, 209.72] |
| 15.2.6 Prothrombin time prolonged | 1 | 61 | Odds Ratio (M‐H, Fixed, 99% CI) | 2.79 [0.05, 160.31] |
| 15.2.7 Upper respiratory tract infection | 1 | 61 | Odds Ratio (M‐H, Fixed, 99% CI) | 2.79 [0.05, 160.31] |
| 15.3 Sweat chloride concentration (mmol/L) (change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 15.3.1 At 21 days | 1 | 50 | Mean Difference (IV, Fixed, 95% CI) | ‐7.95 [‐13.81, ‐2.09] |
Comparison 16. Tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus either placebo or ivacaftor (150 mg twice daily) alone.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 16.1 CFQ‐R respiratory domain (absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 16.1.1 At 1 month | 1 | 504 | Mean Difference (IV, Fixed, 95% CI) | 5.10 [2.99, 7.21] |
| 16.1.2 At 6 months | 1 | 504 | Mean Difference (IV, Fixed, 95% CI) | 5.10 [3.20, 7.00] |
| 16.2 CFQ‐R physical functioning domain (absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 16.2.1 At 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 3.80 [1.90, 5.70] | |
| 16.3 CFQ‐R treatment burden domain (absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 16.3.1 At 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 3.40 [1.60, 5.20] | |
| 16.4 CFQ‐R health perceptions domain (absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 16.4.1 At 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 3.20 [1.20, 5.20] | |
| 16.5 CFQ‐R vitality domain (absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 16.5.1 At 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 2.30 [0.10, 4.50] | |
| 16.6 CFQ‐R social functioning domain (absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 16.6.1 At 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 1.50 [0.00, 3.00] | |
| 16.7 CFQ‐R role functioning domain (absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 16.7.1 At 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 1.50 [‐0.30, 3.30] | |
| 16.8 CFQ‐R eating problems domain (absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 16.8.1 At 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 1.10 [‐0.60, 2.80] | |
| 16.9 CFQ‐R emotional functioning (absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 16.9.1 At 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.60 [‐1.00, 2.20] | |
| 16.10 CFQ‐R weight domain (absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 16.10.1 At 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.50 [‐2.90, 3.90] | |
| 16.11 CFQ‐R digestive symptoms domain(absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 16.11.1 At 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | ‐0.10 [‐1.90, 1.70] | |
| 16.12 CFQ‐R body image domain (absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 16.12.1 At 6 months | 1 | Mean Difference (IV, Fixed, 95% CI) | ‐0.50 [‐2.30, 1.30] | |
| 16.13 FEV1 % predicted (relative change from baseline) | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 16.13.1 At 1 month | 1 | 18 | Mean Difference (IV, Fixed, 95% CI) | 3.72 [‐7.77, 15.21] |
| 16.13.2 At 6 months | 1 | 504 | Mean Difference (IV, Fixed, 95% CI) | 6.80 [5.30, 8.30] |
| 16.14 FEV1 % predicted (absolute change from baseline) | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 16.14.1 At 1 month | 2 | 522 | Mean Difference (IV, Fixed, 95% CI) | 3.59 [2.40, 4.78] |
| 16.14.2 At 6 months | 1 | 504 | Mean Difference (IV, Fixed, 95% CI) | 4.00 [3.10, 4.90] |
| 16.15 Most common adverse events (occurring in at least 10% of participants in either group) | 2 | Odds Ratio (M‐H, Fixed, 99% CI) | Subtotals only | |
| 16.15.1 Cough | 2 | 527 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.70 [0.43, 1.15] |
| 16.15.2 Pulmonary exacerbation | 2 | 527 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.71 [0.44, 1.16] |
| 16.15.3 Headache | 2 | 527 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.26 [0.68, 2.35] |
| 16.15.4 Nasal congestion or nasopharyngitis | 2 | 527 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.09 [0.59, 2.02] |
| 16.15.5 Increased sputum | 1 | 509 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.86 [0.46, 1.63] |
| 16.15.6 Haemoptysis | 2 | 527 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.74 [0.37, 1.49] |
| 16.15.7 Pyrexia | 2 | 527 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.89 [0.44, 1.79] |
| 16.15.8 Oropharyngeal pain | 1 | 509 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.76 [0.35, 1.63] |
| 16.15.9 Fatigue | 2 | 527 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.51 [0.23, 1.15] |
| 16.15.10 Nausea | 2 | 527 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.36 [0.60, 3.12] |
| 16.16 Time to first pulmonary exacerbation | 1 | Hazard Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 16.16.1 At 6 months | 1 | 506 | Hazard Ratio (IV, Fixed, 95% CI) | 0.64 [0.46, 0.89] |
| 16.17 Sweat chloride (change from baseline) | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 16.17.1 At 1 month | 2 | 522 | Mean Difference (IV, Fixed, 95% CI) | ‐9.24 [‐11.12, ‐7.35] |
| 16.17.2 At 6 months | 1 | 504 | Mean Difference (IV, Fixed, 95% CI) | ‐10.10 [‐11.40, ‐8.80] |
| 16.18 BMI (change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 16.18.1 At 1 month | 1 | 504 | Mean Difference (IV, Fixed, 95% CI) | ‐0.03 [‐0.13, 0.07] |
| 16.18.2 At 6 months | 1 | 504 | Mean Difference (IV, Fixed, 95% CI) | 0.06 [‐0.08, 0.20] |
Comparison 17. VX‐659 (80 mg once daily) plus tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo [F508del/MF].
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 17.1 Quality of life: change in CFQ‐R respiratory domain | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 17.1.1 At 1 month | 1 | 21 | Mean Difference (IV, Fixed, 95% CI) | 10.00 [0.29, 19.71] |
| 17.2 FEV1 % predicted (relative change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 17.2.1 At 1 month | 1 | 21 | Mean Difference (IV, Fixed, 95% CI) | 18.36 [3.63, 33.09] |
| 17.3 FEV1 L (absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 17.3.1 At 1 month | 1 | 21 | Mean Difference (IV, Fixed, 95% CI) | 0.37 [0.15, 0.59] |
| 17.4 Adverse events (at 1 month) | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Subtotals only | |
| 17.4.1 Total number of participants experiencing at least one adverse event | 1 | 21 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.11 [0.02, 51.19] |
| 17.4.2 number experiencing moderate AEs | 1 | 21 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 17.4.3 number experiencing severe AEs | 1 | 21 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.23 [0.01, 5.92] |
| 17.4.4 cough | 1 | 21 | Odds Ratio (M‐H, Fixed, 99% CI) | 3.38 [0.13, 85.06] |
| 17.4.5 infective respiratory exacerbation | 1 | 21 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.50 [0.10, 21.90] |
| 17.4.6 headache | 1 | 21 | Odds Ratio (M‐H, Fixed, 99% CI) | 3.00 [0.04, 233.35] |
| 17.4.7 oropharyngeal pain | 1 | 21 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 17.4.8 increased sputum | 1 | 21 | Odds Ratio (M‐H, Fixed, 99% CI) | 5.53 [0.09, 351.89] |
| 17.4.9 raised blood creatine phosphokinase | 1 | 21 | Odds Ratio (M‐H, Fixed, 99% CI) | 3.00 [0.04, 233.35] |
| 17.4.10 nasopharyngitis | 1 | 21 | Odds Ratio (M‐H, Fixed, 99% CI) | 2.00 [0.07, 58.76] |
| 17.4.11 nasal congestion | 1 | 21 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 17.4.12 nausea | 1 | 21 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 17.4.13 pyrexia | 1 | 21 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.90 [0.02, 41.46] |
| 17.4.14 abnormal respiration | 1 | 21 | Odds Ratio (M‐H, Fixed, 99% CI) | 3.00 [0.04, 233.35] |
| 17.4.15 constipation | 1 | 21 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 17.4.16 diarrhoea | 1 | 21 | Odds Ratio (M‐H, Fixed, 99% CI) | 3.00 [0.04, 233.35] |
| 17.4.17 fatigue | 1 | 21 | Odds Ratio (M‐H, Fixed, 99% CI) | 5.53 [0.09, 351.89] |
| 17.4.18 haemoptysis | 1 | 21 | Odds Ratio (M‐H, Fixed, 99% CI) | 5.53 [0.09, 351.89] |
| 17.4.19 productive cough | 1 | 21 | Odds Ratio (M‐H, Fixed, 99% CI) | 5.53 [0.09, 351.89] |
| 17.4.20 URTI | 1 | 21 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.28 [0.00, 21.45] |
| 17.4.21 rash | 1 | 21 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 17.4.22 sinus congestion | 1 | 21 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 17.4.23 influenza | 1 | 21 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 17.4.24 pain | 1 | 21 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 17.4.25 rales | 1 | 21 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 17.5 Sweat chloride (change from baseline) [mmol/L] | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 17.5.1 At 1 month | 1 | 21 | Mean Difference (IV, Fixed, 95% CI) | ‐48.60 [‐60.94, ‐36.26] |
Comparison 18. VX‐659 (120 mg twice daily) plus tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo [F508del/MF].
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 18.1 FEV1 % predicted (absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 18.1.1 At up to 1 month | 1 | 12 | Mean Difference (IV, Fixed, 95% CI) | 10.00 [3.04, 16.96] |
| 18.2 Adverse events (at up to 1 month) | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Subtotals only | |
| 18.2.1 Total number of participants experiencing at least one adverse event | 1 | 12 | Odds Ratio (M‐H, Fixed, 99% CI) | 31.67 [0.32, 3111.29] |
| 18.2.2 number experiencing moderate AEs | 1 | 12 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 18.2.3 number experiencing severe AEs | 1 | 12 | Odds Ratio (M‐H, Fixed, 99% CI) | 2.33 [0.03, 176.29] |
| 18.2.4 cough | 1 | 12 | Odds Ratio (M‐H, Fixed, 99% CI) | 2.33 [0.03, 176.29] |
| 18.2.5 infective respiratory exacerbation | 1 | 12 | Odds Ratio (M‐H, Fixed, 99% CI) | 2.33 [0.03, 176.29] |
| 18.2.6 productive cough | 1 | 12 | Odds Ratio (M‐H, Fixed, 99% CI) | 2.33 [0.03, 176.29] |
| 18.2.7 oral candidiasis | 1 | 12 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.25 [0.00, 16.23] |
| 18.2.8 abdominal discomfort | 1 | 12 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.24 [0.01, 112.68] |
| 18.2.9 raised blood creatine phosphokinase | 1 | 12 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.24 [0.01, 112.68] |
| 18.2.10 diarrhoea | 1 | 12 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.24 [0.01, 112.68] |
| 18.2.11 ear pain | 1 | 12 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.24 [0.01, 112.68] |
| 18.2.12 fatigue | 1 | 12 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.24 [0.01, 112.68] |
| 18.2.13 flatulence | 1 | 12 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.24 [0.01, 112.68] |
| 18.2.14 hypertension | 1 | 12 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.24 [0.01, 112.68] |
| 18.2.15 insomnia | 1 | 12 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.24 [0.01, 112.68] |
| 18.2.16 nausea | 1 | 12 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.24 [0.01, 112.68] |
| 18.2.17 photosensitivity reaction | 1 | 12 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.24 [0.01, 112.68] |
| 18.2.18 decreased pulmonary function tests | 1 | 12 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.24 [0.01, 112.68] |
| 18.2.19 increased sputum | 1 | 12 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.24 [0.01, 112.68] |
| 18.2.20 tinnitus | 1 | 12 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.24 [0.01, 112.68] |
| 18.2.21 viral URTI | 1 | 12 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.24 [0.01, 112.68] |
| 18.3 Sweat chloride (absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 18.3.1 At up to 1 month | 1 | 12 | Mean Difference (IV, Fixed, 95% CI) | ‐30.60 [‐46.38, ‐14.82] |
Comparison 19. VX‐659 (240 mg once daily) plus tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo [F508del/MF].
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 19.1 Quality of life: change in CFQ‐R respiratory domain | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 19.1.1 At 1 month | 1 | 30 | Mean Difference (IV, Fixed, 95% CI) | 4.00 [‐4.70, 12.70] |
| 19.2 FEV1 % predicted (relative change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 19.2.1 At 1 month | 1 | 30 | Mean Difference (IV, Fixed, 95% CI) | 20.17 [8.73, 31.61] |
| 19.3 FEV1 L (absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 19.3.1 At 1 month | 1 | 30 | Mean Difference (IV, Fixed, 95% CI) | 0.42 [0.20, 0.64] |
| 19.4 Adverse events (at 1 month) | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Subtotals only | |
| 19.4.1 Total number of participants experiencing at least one adverse event | 1 | 30 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.33 [0.02, 6.85] |
| 19.4.2 number experiencing moderate AEs | 1 | 30 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.62 [0.02, 121.50] |
| 19.4.3 number experiencing severe AEs | 1 | 30 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.58 [0.06, 5.75] |
| 19.4.4 cough | 1 | 30 | Odds Ratio (M‐H, Fixed, 99% CI) | 3.86 [0.19, 76.85] |
| 19.4.5 infective respiratory exacerbation | 1 | 30 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.71 [0.05, 9.48] |
| 19.4.6 headache | 1 | 30 | Odds Ratio (M‐H, Fixed, 99% CI) | 5.73 [0.11, 304.12] |
| 19.4.7 oropharyngeal pain | 1 | 30 | Odds Ratio (M‐H, Fixed, 99% CI) | 4.20 [0.08, 234.41] |
| 19.4.8 increased sputum | 1 | 30 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.62 [0.02, 121.50] |
| 19.4.9 raised blood creatine phosphokinase | 1 | 30 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.62 [0.02, 121.50] |
| 19.4.10 nasopharyngitis | 1 | 30 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.47 [0.01, 20.94] |
| 19.4.11 nasal congestion | 1 | 30 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.62 [0.02, 121.50] |
| 19.4.12 nausea | 1 | 30 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 19.4.13 pyrexia | 1 | 30 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.47 [0.01, 20.94] |
| 19.4.14 abnormal respiration | 1 | 30 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.62 [0.02, 121.50] |
| 19.4.15 constipation | 1 | 30 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.62 [0.02, 121.50] |
| 19.4.16 diarrhoea | 1 | 30 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 19.4.17 fatigue | 1 | 30 | Odds Ratio (M‐H, Fixed, 99% CI) | 2.84 [0.05, 173.42] |
| 19.4.18 haemoptysis | 1 | 30 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.62 [0.02, 121.50] |
| 19.4.19 productive cough | 1 | 30 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.62 [0.02, 121.50] |
| 19.4.20 URTI | 1 | 30 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.15 [0.00, 11.69] |
| 19.4.21 rash | 1 | 30 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 19.4.22 sinus congestion | 1 | 30 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 19.4.23 influenza | 1 | 30 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 19.4.24 pain | 1 | 30 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 19.4.25 rales | 1 | 30 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 19.5 Sweat chloride (change from baseline) [mmol/L] | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 19.5.1 At 1 month | 1 | 30 | Mean Difference (IV, Fixed, 95% CI) | ‐46.70 [‐57.91, ‐35.49] |
Comparison 20. VX‐659 (400 mg once daily) plus tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo [F508del/MF].
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 20.1 Quality of life: change in CFQ‐R respiratory domain | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 20.1.1 At 1 month | 1 | 32 | Mean Difference (IV, Fixed, 95% CI) | 7.90 [‐0.58, 16.38] |
| 20.2 FEV1 % predicted (relative change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 20.2.1 At 1 month | 1 | 32 | Mean Difference (IV, Fixed, 95% CI) | 23.85 [14.52, 33.18] |
| 20.3 FEV1 L (absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 20.3.1 At 1 month | 1 | 32 | Mean Difference (IV, Fixed, 95% CI) | 0.52 [0.34, 0.70] |
| 20.4 Adverse events (at 1 month) | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Subtotals only | |
| 20.4.1 Total number of participants experiencing at least one adverse event | 1 | 32 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.38 [0.02, 7.70] |
| 20.4.2 number experiencing moderate AEs | 1 | 32 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 20.4.3 number experiencing severe AEs | 1 | 32 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.11 [0.00, 2.67] |
| 20.4.4 cough | 1 | 32 | Odds Ratio (M‐H, Fixed, 99% CI) | 2.00 [0.09, 42.91] |
| 20.4.5 infective respiratory exacerbation | 1 | 32 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.89 [0.07, 10.67] |
| 20.4.6 headache | 1 | 32 | Odds Ratio (M‐H, Fixed, 99% CI) | 5.11 [0.10, 269.76] |
| 20.4.7 oropharyngeal pain | 1 | 32 | Odds Ratio (M‐H, Fixed, 99% CI) | 5.11 [0.10, 269.76] |
| 20.4.8 increased sputum | 1 | 32 | Odds Ratio (M‐H, Fixed, 99% CI) | 3.77 [0.07, 209.36] |
| 20.4.9 raised blood creatine phosphokinase | 1 | 32 | Odds Ratio (M‐H, Fixed, 99% CI) | 3.77 [0.07, 209.36] |
| 20.4.10 nasopharyngitis | 1 | 32 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.42 [0.06, 33.22] |
| 20.4.11 nasal congestion | 1 | 32 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 20.4.12 nausea | 1 | 32 | Odds Ratio (M‐H, Fixed, 99% CI) | 3.77 [0.07, 209.36] |
| 20.4.13 pyrexia | 1 | 32 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.43 [0.01, 18.86] |
| 20.4.14 abnormal respiration | 1 | 32 | Odds Ratio (M‐H, Fixed, 99% CI) | 3.77 [0.07, 209.36] |
| 20.4.15 constipation | 1 | 32 | Odds Ratio (M‐H, Fixed, 99% CI) | 3.77 [0.07, 209.36] |
| 20.4.16 diarrhoea | 1 | 32 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.47 [0.02, 109.79] |
| 20.4.17 fatigue | 1 | 32 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 20.4.18 haemoptysis | 1 | 32 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 20.4.19 productive cough | 1 | 32 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 20.4.20 URTI | 1 | 32 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.90 [0.03, 24.89] |
| 20.4.21 rash | 1 | 32 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 20.4.22 sinus congestion | 1 | 32 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 20.4.23 influenza | 1 | 32 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 20.4.24 pain | 1 | 32 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 20.4.25 rales | 1 | 32 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 20.5 Sweat chloride (mmol/L) change from baseline | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 20.5.1 At 1 month | 1 | 32 | Mean Difference (IV, Fixed, 95% CI) | ‐54.30 [‐65.28, ‐43.32] |
Comparison 21. VX‐659 (400 mg once daily) plus tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo+tez+iva [F508del homozygous].
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 21.1 Quality of life: change in CFQ‐R respiratory domain | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 21.1.1 At 1 month | 1 | 29 | Mean Difference (IV, Fixed, 95% CI) | 18.10 [10.85, 25.35] |
| 21.2 FEV1 % predicted (relative change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 21.2.1 At 1 month | 1 | 29 | Mean Difference (IV, Fixed, 95% CI) | 15.99 [8.61, 23.37] |
| 21.3 FEV1 L (absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 21.3.1 At 1 month | 1 | 29 | Mean Difference (IV, Fixed, 95% CI) | 0.35 [0.19, 0.51] |
| 21.4 Adverse events (at 1 month) | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Subtotals only | |
| 21.4.1 Total number of participants experiencing at least one adverse event | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.11 [0.08, 14.81] |
| 21.4.2 number experiencing moderate AEs | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 21.4.3 number experiencing severe AEs | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.26 [0.01, 7.39] |
| 21.4.4 cough | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.29 [0.11, 15.47] |
| 21.4.5 infective respiratory exacerbation | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.03 [0.11, 9.34] |
| 21.4.6 headache | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 5.19 [0.09, 289.65] |
| 21.4.7 oropharyngeal pain | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 3.48 [0.06, 212.67] |
| 21.4.8 increased sputum | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 2.00 [0.09, 46.89] |
| 21.4.9 raised blood creatine phosphokinase | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.26 [0.01, 7.39] |
| 21.4.10 nasopharyngitis | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 21.4.11 nasal congestion | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 7.14 [0.13, 379.05] |
| 21.4.12 nausea | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.56 [0.03, 9.16] |
| 21.4.13 pyrexia | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.25 [0.05, 34.62] |
| 21.4.14 abnormal respiration | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 21.4.15 constipation | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 21.4.16 diarrhoea | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 3.48 [0.06, 212.67] |
| 21.4.17 fatigue | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.19 [0.00, 14.26] |
| 21.4.18 haemoptysis | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.97 [0.03, 148.00] |
| 21.4.19 productive cough | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.97 [0.03, 148.00] |
| 21.4.20 URTI | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 3.48 [0.06, 212.67] |
| 21.4.21 rash | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 21.4.22 sinus congestion | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 21.4.23 influenza | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 21.4.24 pain | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 21.4.25 rales | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 21.5 Sweat chloride (change from baseline) [mmol/L] | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 21.5.1 At 1 month | 1 | 29 | Mean Difference (IV, Fixed, 95% CI) | ‐45.20 [‐52.18, ‐38.22] |
Comparison 22. VX‐659 (400 mg once daily) plus tezacaftor (100 mg once daily) plus VX‐561 (150 mg once daily) versus placebo [F508del/MF].
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 22.1 Quality of life: change in CFQ‐R respiratory domain | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 22.1.1 At 1 month | 1 | 25 | Mean Difference (IV, Fixed, 95% CI) | 20.30 [7.05, 33.55] |
| 22.2 FEV1 % predicted (relative change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 22.2.1 At 1 month | 1 | 25 | Mean Difference (IV, Fixed, 95% CI) | 33.05 [22.05, 44.05] |
| 22.3 FEV1 L (absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 22.3.1 At 1 month | 1 | 25 | Mean Difference (IV, Fixed, 95% CI) | 0.68 [0.45, 0.91] |
| 22.4 Adverse events (at 1 month) | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Subtotals only | |
| 22.4.1 Total number of participants experiencing at least one adverse event | 1 | 25 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.95 [0.01, 74.78] |
| 22.4.2 number experiencing moderate AEs | 1 | 25 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.86 [0.03, 119.25] |
| 22.4.3 number experiencing severe AEs | 1 | 25 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.12 [0.01, 2.04] |
| 22.4.4 cough | 1 | 25 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.53 [0.04, 7.63] |
| 22.4.5 infective respiratory exacerbation | 1 | 25 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.12 [0.01, 2.04] |
| 22.4.6 headache | 1 | 25 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 22.4.7 oropharyngeal pain | 1 | 25 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.86 [0.03, 119.25] |
| 22.4.8 increased sputum | 1 | 25 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 22.4.9 raised blood creatine phosphokinase | 1 | 25 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 22.4.10 nasopharyngitis | 1 | 25 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 22.4.11 nasal congestion | 1 | 25 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 22.4.12 nausea | 1 | 25 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.86 [0.03, 119.25] |
| 22.4.13 pyrexia | 1 | 25 | Odds Ratio (M‐H, Fixed, 99% CI) | 2.76 [0.05, 161.94] |
| 22.4.14 abnormal respiration | 1 | 25 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 22.4.15 constipation | 1 | 25 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 22.4.16 diarrhoea | 1 | 25 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 22.4.17 fatigue | 1 | 25 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 22.4.18 haemoptysis | 1 | 25 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 22.4.19 productive cough | 1 | 25 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 22.4.20 URTI | 1 | 25 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 22.4.21 rash | 1 | 25 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.86 [0.03, 119.25] |
| 22.4.22 sinus congestion | 1 | 25 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.86 [0.03, 119.25] |
| 22.4.23 influenza | 1 | 25 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.86 [0.03, 119.25] |
| 22.4.24 pain | 1 | 25 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.86 [0.03, 119.25] |
| 22.4.25 rales | 1 | 25 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.05 [0.00, 3.11] |
| 22.5 Sweat chloride (change from baseline) [mmol/L] | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 22.5.1 At 1 month | 1 | 25 | Mean Difference (IV, Fixed, 95% CI) | ‐36.80 [‐48.74, ‐24.86] |
Comparison 23. VX‐659 400 mg tezacaftor ‐ pooled ivacaftor and VX‐561.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 23.1 Quality of life: change in CFQ‐R respiratory domain | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 23.1.1 At 1 month | 1 | 57 | Mean Difference (IV, Fixed, 95% CI) | 14.10 [10.49, 17.71] |
| 23.2 FEV1 % predicted (relative change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 23.2.1 At 1 month | 1 | 57 | Mean Difference (IV, Fixed, 95% CI) | 28.45 [25.44, 31.46] |
| 23.3 FEV1 L (absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 23.3.1 At 1 month | 1 | 57 | Mean Difference (IV, Fixed, 95% CI) | Not estimable |
| 23.4 Adverse events (at 1 month) | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Subtotals only | |
| 23.4.1 total number of participants experiencing at least one adverse event | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.11 [0.08, 14.81] |
| 23.4.2 number experiencing moderate AEs | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 23.4.3 number experiencing severe AEs | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.26 [0.01, 7.39] |
| 23.4.4 cough | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.29 [0.11, 15.47] |
| 23.4.5 infective respiratory exacerbation | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.03 [0.11, 9.34] |
| 23.4.6 headache | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 5.19 [0.09, 289.65] |
| 23.4.7 oropharyngeal pain | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 3.48 [0.06, 212.67] |
| 23.4.8 increased sputum | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 2.00 [0.09, 46.89] |
| 23.4.9 raised blood creatine phosphokinase | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.26 [0.01, 7.39] |
| 23.4.10 nasopharyngitis | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 23.4.11 nasal congestion | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 7.14 [0.13, 379.05] |
| 23.4.12 nausea | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.56 [0.03, 9.16] |
| 23.4.13 pyrexia | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.25 [0.05, 34.62] |
| 23.4.14 abnormal respiration | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 23.4.15 constipation | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 23.4.16 diarrhoea | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 3.48 [0.06, 212.67] |
| 23.4.17 fatigue | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.19 [0.00, 14.26] |
| 23.4.18 haemoptysis | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.97 [0.03, 148.00] |
| 23.4.19 productive cough | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.97 [0.03, 148.00] |
| 23.4.20 URTI | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 3.48 [0.06, 212.67] |
| 23.4.21 rash | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 23.4.22 sinus congestion | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 23.4.23 influenza | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 23.4.24 pain | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 23.4.25 rales | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 23.5 Sweat chloride (change from baseline) [mmol/L] | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 23.5.1 At 1 month | 1 | 29 | Mean Difference (IV, Fixed, 95% CI) | ‐45.20 [‐52.18, ‐38.22] |
23.1. Analysis.

Comparison 23: VX‐659 400 mg tezacaftor ‐ pooled ivacaftor and VX‐561, Outcome 1: Quality of life: change in CFQ‐R respiratory domain
23.2. Analysis.

Comparison 23: VX‐659 400 mg tezacaftor ‐ pooled ivacaftor and VX‐561, Outcome 2: FEV1 % predicted (relative change from baseline)
23.3. Analysis.

Comparison 23: VX‐659 400 mg tezacaftor ‐ pooled ivacaftor and VX‐561, Outcome 3: FEV1 L (absolute change from baseline)
23.5. Analysis.

Comparison 23: VX‐659 400 mg tezacaftor ‐ pooled ivacaftor and VX‐561, Outcome 5: Sweat chloride (change from baseline) [mmol/L]
Comparison 24. Elexacaftor (50 mg once daily) tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo [F508del/MF].
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 24.1 Quality of life: change in CFQ‐R respiratory domain | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 24.1.1 At 1 month | 1 | 22 | Mean Difference (IV, Fixed, 95% CI) | 17.20 [4.44, 29.96] |
| 24.2 FEV1 % predicted (relative change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 24.2.1 At 1 month | 1 | 22 | Mean Difference (IV, Fixed, 95% CI) | 19.00 [7.08, 30.92] |
| 24.3 FEV1 L (absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 24.3.1 At 1 month | 1 | 22 | Mean Difference (IV, Fixed, 95% CI) | 0.46 [0.19, 0.73] |
| 24.4 Adverse events (at 1 month) | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Subtotals only | |
| 24.4.1 Total number of participants experiencing at least one adverse event | 1 | 22 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 24.4.2 number experiencing moderate AEs | 1 | 22 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 24.4.3 number experiencing severe AEs | 1 | 22 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.56 [0.02, 16.15] |
| 24.4.4 cough | 1 | 22 | Odds Ratio (M‐H, Fixed, 99% CI) | 7.33 [0.31, 173.32] |
| 24.4.5 increased sputum | 1 | 22 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.29 [0.11, 15.22] |
| 24.4.6 infective respiratory exacerbation | 1 | 22 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.86 [0.08, 9.23] |
| 24.4.7 haemoptysis | 1 | 22 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.20 [0.00, 12.63] |
| 24.4.8 pyrexia | 1 | 22 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.37 [0.00, 28.22] |
| 24.4.9 nausea | 1 | 22 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.25 [0.07, 21.63] |
| 24.4.10 oropharyngeal pain | 1 | 22 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.25 [0.07, 21.63] |
| 24.4.11 headache | 1 | 22 | Odds Ratio (M‐H, Fixed, 99% CI) | 2.75 [0.09, 80.30] |
| 24.4.12 nasal congestion | 1 | 22 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.25 [0.07, 21.63] |
| 24.4.13 nasopharyngitis | 1 | 22 | Odds Ratio (M‐H, Fixed, 99% CI) | 3.95 [0.05, 305.83] |
| 24.4.14 increased blood creatine phosphokinase | 1 | 22 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 24.4.15 fatigue | 1 | 22 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.22 [0.01, 5.13] |
| 24.4.16 elevated AST | 1 | 22 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 24.4.17 diarrhoea | 1 | 22 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.22 [0.03, 55.87] |
| 24.4.18 abnormal respiration | 1 | 22 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 24.4.19 rhinorrhea | 1 | 22 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 24.5 Sweat chloride (change from baseline) [mmol/L] | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 24.5.1 At 1 month | 1 | 22 | Mean Difference (IV, Fixed, 95% CI) | ‐36.00 [‐47.23, ‐24.77] |
Comparison 25. Elexacaftor (100 mg once daily) tezacaftor (100 mg once daily) plus ivacaftor (150 mg twice daily) versus placebo [F508del/MF].
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 25.1 Quality of life: change in CFQ‐R respiratory sub‐domain | 1 | 34 | Mean Difference (IV, Fixed, 95% CI) | 14.50 [3.72, 25.28] |
| 25.1.1 At 1 month | 1 | 34 | Mean Difference (IV, Fixed, 95% CI) | 14.50 [3.72, 25.28] |
| 25.2 FEV1 % predicted (relative change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 25.2.1 At 1 month | 1 | 34 | Mean Difference (IV, Fixed, 95% CI) | 13.50 [3.28, 23.72] |
| 25.3 FEV1 L (absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 25.3.1 At 1 month | 1 | 34 | Mean Difference (IV, Fixed, 95% CI) | 0.38 [0.20, 0.56] |
| 25.4 Adverse events at (1 month) | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Subtotals only | |
| 25.4.1 Total number of participants experiencing at least one adverse event | 1 | 34 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.57 [0.01, 42.46] |
| 25.4.2 number experiencing moderate AEs | 1 | 34 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 25.4.3 number experiencing severe AEs | 1 | 34 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.50 [0.03, 7.92] |
| 25.4.4 cough | 1 | 34 | Odds Ratio (M‐H, Fixed, 99% CI) | 3.24 [0.16, 64.50] |
| 25.4.5 increased sputum | 1 | 34 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.67 [0.07, 6.20] |
| 25.4.6 infective respiratory exacerbation | 1 | 34 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.59 [0.08, 4.57] |
| 25.4.7 haemoptysis | 1 | 34 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.47 [0.14, 16.00] |
| 25.4.8 pyrexia | 1 | 34 | Odds Ratio (M‐H, Fixed, 99% CI) | 3.24 [0.16, 64.50] |
| 25.4.9 nausea | 1 | 34 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.79 [0.06, 10.19] |
| 25.4.10 oropharyngeal pain | 1 | 34 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.50 [0.03, 7.92] |
| 25.4.11 headache | 1 | 34 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.50 [0.03, 7.92] |
| 25.4.12 nasal congestion | 1 | 34 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.50 [0.03, 7.92] |
| 25.4.13 nasopharyngitis | 1 | 34 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 25.4.14 increased blood creatine phosphokinase | 1 | 34 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 25.4.15 fatigue | 1 | 34 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.04 [0.00, 2.24] |
| 25.4.16 elevated AST | 1 | 34 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 25.4.17 diarrhoea | 1 | 34 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.74 [0.08, 39.74] |
| 25.4.18 abnormal respiration | 1 | 34 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.74 [0.02, 129.18] |
| 25.4.19 rhinorrhea | 1 | 34 | Odds Ratio (M‐H, Fixed, 99% CI) | 4.49 [0.08, 246.11] |
| 25.5 Sweat chloride (change from baseline) [mmol/L] | 1 | 34 | Mean Difference (IV, Fixed, 95% CI) | ‐31.00 [‐40.41, ‐21.59] |
| 25.5.1 At 1 month | 1 | 34 | Mean Difference (IV, Fixed, 95% CI) | ‐31.00 [‐40.41, ‐21.59] |
Comparison 26. Elexacaftor (200 mg once daily) tezacaftor (100 mg once daily) plus VX‐561 (150 mg once daily) versus placebo [F508del/MF].
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 26.1 Quality of life: change in CFQ‐R respiratory domain | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 26.1.1 At 1 month | 1 | 29 | Mean Difference (IV, Fixed, 95% CI) | 12.80 [0.93, 24.67] |
| 26.2 FEV1 % predicted (relative change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 26.2.1 At 1 month | 1 | 29 | Mean Difference (IV, Fixed, 95% CI) | 18.30 [7.64, 28.96] |
| 26.3 FEV1 L (absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 26.3.1 At 1 month | 1 | 29 | Mean Difference (IV, Fixed, 95% CI) | 0.44 [0.25, 0.63] |
| 26.4 Adverse events (at 1 month) | 2 | Odds Ratio (M‐H, Fixed, 99% CI) | Subtotals only | |
| 26.4.1 Total number of participants experiencing at least one adverse event | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.36 [0.05, 38.84] |
| 26.4.2 number experiencing moderate AEs | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 26.4.3 number experiencing severe AEs | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.12 [0.00, 8.97] |
| 26.4.4 cough | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.94 [0.08, 11.23] |
| 26.4.5 increased sputum | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.17 [0.05, 28.28] |
| 26.4.6 infective respiratory exacerbation | 2 | 136 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.15 [0.02, 1.00] |
| 26.4.7 nausea | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.18 [0.01, 2.57] |
| 26.4.8 oropharyngeal pain | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.94 [0.08, 11.23] |
| 26.4.9 nasal congestion | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.17 [0.05, 28.28] |
| 26.4.10 productive cough | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.74 [0.03, 21.09] |
| 26.4.11 chest pain | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 2.18 [0.04, 135.31] |
| 26.4.12 paranasal sinus discomfort | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 2.18 [0.04, 135.31] |
| 26.4.13 sinus congestion | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 2.18 [0.04, 135.31] |
| 26.4.14 URTI | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 2.18 [0.04, 135.31] |
| 26.4.15 vomiting | 1 | 29 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.06 [0.00, 3.85] |
| 26.5 Sweat chloride (change from baseline) [mmol/L] | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 26.5.1 At 1 month | 1 | 29 | Mean Difference (IV, Fixed, 95% CI) | ‐34.60 [‐45.15, ‐24.05] |
Comparison 27. Elexacaftor (200 mg once daily) tezacaftor (100 mg once daily) plus ivacaftor 150 mg twice daily versus triple placebo‐ F508del/MF.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 27.1 Quality of life: CFQ‐R respiratory domain (change from baseline) | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 27.1.1 At up to 1 month | 2 | 436 | Mean Difference (IV, Fixed, 95% CI) | 19.15 [16.12, 22.19] |
| 27.1.2 At up to 6 months | 1 | 403 | Mean Difference (IV, Fixed, 95% CI) | 20.20 [16.19, 24.21] |
| 27.2 FEV1 % predicted (relative change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 27.2.1 At up to 1 month | 1 | 33 | Mean Difference (IV, Fixed, 95% CI) | 25.90 [15.57, 36.23] |
| 27.3 FEV1 % predicted (absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 27.3.1 At up to 1 month | 1 | 403 | Mean Difference (IV, Fixed, 95% CI) | 13.80 [12.18, 15.42] |
| 27.3.2 At up to 6 months | 1 | 403 | Mean Difference (IV, Fixed, 95% CI) | 14.30 [12.76, 15.84] |
| 27.4 FEV1 L (absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 27.4.1 At up to 1 month | 1 | 33 | Mean Difference (IV, Fixed, 95% CI) | 0.57 [0.36, 0.78] |
| 27.5 Adverse events (at up to 1 month) | 1 | Odds Ratio (M‐H, Fixed, 99% CI) | Subtotals only | |
| 27.5.1 Total number of participants experiencing at least one adverse event | 1 | 33 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.21 [0.00, 11.62] |
| 27.5.2 number experiencing moderate AEs | 1 | 33 | Odds Ratio (M‐H, Fixed, 99% CI) | 3.21 [0.05, 193.04] |
| 27.5.3 number experiencing severe AEs | 1 | 33 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.10 [0.00, 5.93] |
| 27.5.4 cough | 1 | 33 | Odds Ratio (M‐H, Fixed, 99% CI) | 5.50 [0.29, 104.32] |
| 27.5.5 increased sputum | 1 | 33 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.94 [0.11, 8.18] |
| 27.5.6 infective respiratory exacerbation | 1 | 33 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.21 [0.02, 2.52] |
| 27.5.7 haemoptysis | 1 | 33 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.53 [0.03, 8.36] |
| 27.5.8 pyrexia | 1 | 33 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.55 [0.01, 23.83] |
| 27.5.9 nausea | 1 | 33 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.25 [0.01, 6.84] |
| 27.5.10 oropharyngeal pain | 1 | 33 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.53 [0.03, 8.36] |
| 27.5.11 headache | 1 | 33 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.53 [0.03, 8.36] |
| 27.5.12 nasal congestion | 1 | 33 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.53 [0.03, 8.36] |
| 27.5.13 nasopharyngitis | 1 | 33 | Odds Ratio (M‐H, Fixed, 99% CI) | 6.43 [0.12, 336.06] |
| 27.5.14 increased blood creatine phosphokinase | 1 | 33 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.83 [0.02, 135.72] |
| 27.5.15 fatigue | 1 | 33 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.04 [0.00, 2.35] |
| 27.5.16 elevated AST | 1 | 33 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.83 [0.02, 135.72] |
| 27.5.17 diarrhoea | 1 | 33 | Odds Ratio (M‐H, Fixed, 99% CI) | 0.18 [0.00, 13.28] |
| 27.5.18 abnormal respiration | 1 | 33 | Odds Ratio (M‐H, Fixed, 99% CI) | 1.83 [0.02, 135.72] |
| 27.5.19 rhinorrhea | 1 | 33 | Odds Ratio (M‐H, Fixed, 99% CI) | Not estimable |
| 27.6 Adverse events (at up to 6 months) | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 27.6.1 Any adverse event | 1 | 403 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.56 [0.23, 1.36] |
| 27.6.2 Mild adverse events | 1 | 403 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.39 [0.90, 2.13] |
| 27.6.3 Moderate adverse events | 1 | 403 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.62 [0.42, 0.92] |
| 27.6.4 Severe adverse events | 1 | 403 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.39 [0.68, 2.85] |
| 27.6.5 Serious adverse events | 1 | 403 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.61 [0.36, 1.03] |
| 27.6.6 Adverse event leading to discontinuation of treatment | 1 | 403 | Odds Ratio (M‐H, Fixed, 95% CI) | 5.02 [0.24, 105.33] |
| 27.6.7 Infective pulmonary exacerbation of CF | 1 | 403 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.31 [0.20, 0.48] |
| 27.6.8 Sputum increased | 1 | 403 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.03 [0.63, 1.68] |
| 27.6.9 Headache | 1 | 403 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.19 [0.70, 2.03] |
| 27.6.10 Cough | 1 | 403 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.33 [0.20, 0.52] |
| 27.6.11 Diarrhoea | 1 | 403 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.33 [0.20, 0.52] |
| 27.6.12 Upper respiratory tract infection | 1 | 403 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.10 [0.59, 2.03] |
| 27.6.13 Nasopharyngitis | 1 | 403 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.82 [0.45, 1.51] |
| 27.6.14 Oropharyngeal pain | 1 | 403 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.77 [0.41, 1.44] |
| 27.6.15 Haemoptysis | 1 | 403 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.36 [0.17, 0.74] |
| 27.6.16 Fatigue | 1 | 403 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.42 [0.19, 0.95] |
| 27.7 Hospitalisation | 1 | Rate Ratio (IV, Fixed, 95% CI) | Subtotals only | |
| 27.7.1 At up to 6 months | 1 | Rate Ratio (IV, Fixed, 95% CI) | 0.29 [0.14, 0.60] | |
| 27.8 Exacerbation (need for antibiotics) | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 27.8.1 At up to 6 months | 1 | 403 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.29 [0.14, 0.60] |
| 27.9 Sweat chloride (absolute change from baseline) | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 27.9.1 At up to 1 month | 2 | 436 | Mean Difference (IV, Fixed, 95% CI) | ‐40.96 [‐43.60, ‐38.33] |
| 27.9.2 At up to 6 months | 1 | 403 | Mean Difference (IV, Fixed, 95% CI) | ‐41.80 [‐44.33, ‐39.27] |
| 27.10 Weight (absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 27.10.1 At up to 6 months | 1 | 403 | Mean Difference (IV, Fixed, 95% CI) | 2.90 [2.40, 3.40] |
| 27.11 BMI z score (absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 27.11.1 At up to 6 months | 1 | 403 | Mean Difference (IV, Fixed, 95% CI) | 0.30 [0.17, 0.43] |
Comparison 28. Elexacaftor (200 mg once daily) tezacaftor (100 mg once daily) plus ivacaftor 150 mg twice daily versus placebo‐tez‐iva‐ F508del/F508del.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 28.1 Quality of life: CFQ‐R respiratory domain (change from baseline) | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 28.1.1 At up to 1 month | 2 | 135 | Mean Difference (IV, Fixed, 95% CI) | 17.78 [12.90, 22.66] |
| 28.2 FEV1 % predicted (relative change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 28.2.1 At up to 1 month | 1 | 28 | Mean Difference (IV, Fixed, 95% CI) | 17.80 [6.66, 28.94] |
| 28.3 FEV1 % predicted (absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 28.3.1 At up to 1 month | 1 | 107 | Mean Difference (IV, Fixed, 95% CI) | 10.00 [7.51, 12.49] |
| 28.4 FEV1 L (absolute change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 28.4.1 At up to 1 month | 1 | 28 | Mean Difference (IV, Fixed, 95% CI) | 0.46 [0.26, 0.66] |
| 28.5 Adverse events (at up to 1 month) | 2 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 28.5.1 Total number of participants experiencing at least one adverse event | 2 | 135 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.94 [0.46, 1.96] |
| 28.5.2 Mild adverse events | 1 | 107 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.06 [0.49, 2.29] |
| 28.5.3 Moderate adverse events | 2 | 135 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.94 [0.39, 2.26] |
| 28.5.4 Severe adverse events | 2 | 135 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.19 [0.02, 1.92] |
| 28.5.5 Serious adverse events | 1 | 107 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.92 [0.17, 21.88] |
| 28.5.6 Adverse event leading to discontinuation of trial drug | 1 | 107 | Odds Ratio (M‐H, Fixed, 95% CI) | Not estimable |
| 28.5.7 Elevated transaminase | 1 | 107 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.92 [0.17, 21.88] |
| 28.5.8 Rash | 1 | 107 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.94 [0.13, 6.95] |
| 28.5.9 Cough | 2 | 135 | Odds Ratio (M‐H, Fixed, 95% CI) | 2.67 [0.90, 7.93] |
| 28.5.10 Nasopharyngitis | 2 | 135 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.25 [0.29, 5.33] |
| 28.5.11 Upper respiratory tract infection | 1 | 107 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.96 [0.34, 11.19] |
| 28.5.12 Infective respiratory exacerbation | 1 | 28 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.88 [0.18, 19.53] |
| 28.5.13 Headache | 2 | 135 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.48 [0.12, 1.88] |
| 28.5.14 Haemoptysis | 2 | 135 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.63 [0.17, 2.34] |
| 28.5.15 Pulmonary exacerbation | 1 | 107 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.14 [0.02, 1.22] |
| 28.5.16 Oropharyngeal pain | 2 | 135 | Odds Ratio (M‐H, Fixed, 95% CI) | 2.51 [0.44, 14.37] |
| 28.5.17 Increased sputum | 1 | 28 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.54 [0.24, 9.90] |
| 28.5.18 Pyrexia | 1 | 28 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.00 [0.09, 11.52] |
| 28.5.19 Nausea | 1 | 28 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.30 [0.02, 5.55] |
| 28.5.20 Nasal congestion | 1 | 28 | Odds Ratio (M‐H, Fixed, 95% CI) | Not estimable |
| 28.5.21 Increased blood creatine phosphokinase | 1 | 28 | Odds Ratio (M‐H, Fixed, 95% CI) | 3.86 [0.18, 80.99] |
| 28.5.22 Fatigue | 1 | 28 | Odds Ratio (M‐H, Fixed, 95% CI) | 3.86 [0.18, 80.99] |
| 28.5.23 Elevated AST | 1 | 28 | Odds Ratio (M‐H, Fixed, 95% CI) | 2.84 [0.13, 61.89] |
| 28.5.24 Diarrhoea | 1 | 28 | Odds Ratio (M‐H, Fixed, 95% CI) | Not estimable |
| 28.5.25 Abnormal respiration | 1 | 28 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.92 [0.08, 44.92] |
| 28.5.26 Rhinorrhea | 1 | 28 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.10 [0.04, 30.00] |
| 28.6 Sweat chloride (absolute change from baseline) | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 28.6.1 At up to 1 month | 2 | 135 | Mean Difference (IV, Fixed, 95% CI) | ‐44.32 [‐48.80, ‐39.84] |
| 28.7 Weight (change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 28.7.1 At up to 1 month | 1 | Mean Difference (IV, Fixed, 95% CI) | 1.60 [1.00, 2.20] | |
| 28.8 BMI (change from baseline) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 28.8.1 At up to 1 month | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.60 [0.41, 0.79] |
28.2. Analysis.

Comparison 28: Elexacaftor (200 mg once daily) tezacaftor (100 mg once daily) plus ivacaftor 150 mg twice daily versus placebo‐tez‐iva‐ F508del/F508del, Outcome 2: FEV1 % predicted (relative change from baseline)
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Boyle 2014.
| Study characteristics | ||
| Methods | Phase 2 placebo‐controlled RCT with 3 different cohorts. Only cohort 1 was included in this review (n = 62). (The following information will refer to cohort 1 only ‐ see 'Notes'.) Parallel design. Multicentre study conducted at 69 different sites in North America, Europe and Australia. Duration: Cohort 1 lasted 21 days. |
|
| Participants | Mutation: participants homozygous for F508del mutation. Age: participants in Cohort 1 have a mean age of 29.1 years. Gender split: 50% of participants are male Lung function: all participants in Cohort 1 have a FEV1 ≥ 40% of predicted normal for age, gender, and height and a mean (range) predicted FEV1 of 66.9% (32.8 ‐ 117.1). Sweat chloride levels: participants in Cohort 1 have a mean (range) level of 101.9 mmol/L (87.5 ‐ 121.0). |
|
| Interventions |
Intervention 1: lumacaftor (also known as VX‐809, a CFTR corrector) alone. Intervention 2: lumacaftor in combination with ivacaftor (also known as VX‐770, a CFTR potentiator). Intervention 3: placebo. Cohort 1 (n = 62) Study drug participants: 200 mg lumacaftor once daily for 14 days; then from day 15, participants continue to take 200 mg of lumacaftor in addition to either 150 mg or 250 mg of ivacaftor twice daily until day 21. Placebo participants: placebo for 21 days. |
|
| Outcomes |
Primary outcomes 1. Change in sweat chloride when ivacaftor is administered in combination with lumacaftor* 2. Safety and tolerability assessments based on adverse events, plasma samples (haematology, clinical chemistry, coagulation), urinalysis, ECGs, and vital signs* Secondary outcomes 1. Change in % predicted FEV1* 2. Change in sweat chloride of increasing doses of lumacaftor administered alone* 3. PK parameters (including exposure, concentration and half‐life) of lumacaftor and metabolite in plasma in the presence and absence of ivacaftor 4. PK parameters (including exposure, concentration and half‐life) of ivacaftor and metabolites in plasma in the presence of lumacaftor |
|
| Funding source | Vertex Pharmaceuticals, and the Cystic Fibrosis Foundation Therapeutics Development Network. | |
| Notes | * denotes outcomes relevant to this review. Only data from Cohort 1 were included in this review. This was because data for placebo participants from Cohorts 2 and 3 were pooled, although randomisation in these cohorts occurred separately. This meant that the effects of randomisation in these cohorts were undone. Data for participants in Cohorts 2 and 3 were excluded. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | A random sequence was generated by a computer by an independent party. |
| Allocation concealment (selection bias) | Low risk | "Site pharmacists dispensed drugs on the basis of an interactive voice response system". |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Drug doses were prepared by an independent unmasked pharmacist and dispensed by site pharmacists who were masked to treatment assignment. Participant blinding was maintained by placebo which was matched to intervention by the quantity of tablets and by size, colour, coating and packaging. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Site investigators and the study sponsor were also masked to treatment assignment and to sweat chloride levels ‐ data that could have potentially disclosed treatment assignment. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Participant data were excluded from the analysis due to insufficient data, e.g. participants were excluded from the analysis of sweat chloride concentration if insufficient amount of sweat were provided. We judged this trial as having an unclear risk of attrition bias because it was unclear how these exclusions would have affected the balance between groups in baseline characteristics. |
| Selective reporting (reporting bias) | Low risk | We compared the outcomes reported on the US NIH trials registry (www.clinicaltrials.gov) to the outcomes reported in the results of the published paper as the protocol was not available. No selective outcome reporting was identified. |
| Other bias | Low risk | Similar baseline characteristics. |
Clancy 2012.
| Study characteristics | ||
| Methods | Phase 2a placebo‐controlled RCT. Parallel design. Multicentre study conducted at 25 study locations over North America and Europe. Duration: 28 days. |
|
| Participants | Mutation: all 89 randomised participants had a confirmed diagnosis of CF and all but 1 were homozygous for the F508del mutation. Age: median (range) age of 26 (18 ‐ 54) years. Gender split: 60% of the participants were males. Lung function: a baseline FEV1 > 40% predicted was an eligibility criteria; but scores ranged from 34.2 to 126.3 with a median of 71. Sweat chloride levels: 103.5 (66.0 ‐ 129.0) mmol/L. Nutritional status: median (range) baseline BMI of 22 (16 ‐ 34). |
|
| Interventions |
Intervention 1: placebo (n = 17). Intervention 2: lumacaftor (VX‐809) 25 mg once daily (n = 18). Intervention 3: lumacaftor 50 mg once daily (n = 18). Intervention 4: lumacaftor 100 mg once daily (n = 17). Intervention 5: lumacaftor 200 mg once daily (n = 19). |
|
| Outcomes |
Primary outcome
1. Evaluation of safety and tolerability of lumacaftor based on adverse events*, haematology, clinical chemistry, urinalysis, ECGs, vital signs, and physical examinations Secondary outcomes 1. Evaluation of the pharmacodynamic impact of lumacaftor on CFTR function 2. Change from baseline in sweat chloride concentration* 3. Nasal potential difference (optional) 4. Spirometry* (FEV1, FEF25-75%, FVC) 5. Change from baseline in CFQ‐R score* |
|
| Funding source | Vertex Pharmaceuticals, and grants from the NIH. | |
| Notes | * denotes outcomes relevant to this review. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not stated. |
| Allocation concealment (selection bias) | Unclear risk | Not stated. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | There was insufficient information on how participant or study personnel blinding were maintained. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | There was insufficient information on how outcome assessor blind was maintained. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | In the adverse events table, the total number of participants shown (n = 45) is less than the total number of participants randomised (n = 89). In Figure 1B the number of participants analysed in the outcome 'Change from baseline in sweat chloride' (n = 63) is less than the total number of participants randomised to the intervention (n = 72). Therefore, 9 participants have been unaccounted for. In the table of results of total CFQ‐R scores, 1 participant appears to be excluded from each of the treatment groups. |
| Selective reporting (reporting bias) | High risk | No results have been presented for FEF25-75% or FVC despite being stated as an outcome. |
| Other bias | Low risk | Baseline characteristics well matched except for the less severe lung disease in 25 mg and placebo groups. |
Davies 2018a.
| Study characteristics | ||
| Methods | Phase 1 placebo‐controlled, double‐blind RCT. Parallel design. Multicentre study conducted at 9 sites across the UK. Duration: 14 days. |
|
| Participants | 12 participants enrolled and randomised. All 12 participants completed the 14‐day trial period. Mutation: confirmed CF diagnosis and F508del/MF. Age: 18 years or older. Disease severity: body weight ≥ 35 kg and FEV1 % predicted 40% to 90% at screening. Intervention group (n = 9). Age, mean (SD): 36.8 (9.9) years. Gender split: 8 males, 1 female. FEV1 % predicted, mean (SD): 48.0 (12.7)%. Sweat chloride, mean (SD): 107.7 (10.5) mmol/L. Placebo group (n = 3). Age, mean (SD): 30.3 (5.1) years. Gender split: 3 males. FEV1 % predicted, mean (SD): 44.9 (9.6)%. Sweat chloride, mean (SD): 104.3 (4.9) mmol/L |
|
| Interventions |
Intervention: VX‐659 120 mg every 12 hours plus ivacaftor 150 mg every 12 hours plus tezacaftor 100 mg once daily . Control: triple placebo. |
|
| Outcomes | Adverse effects. Clinically significant laboratory test results. 12‐lead ECG. Vital signs. Spirometric measurements. |
|
| Funding source | Vertex Pharmaceutical supported the trial, who in turn received funding from the Cystic Fibrosis Foundation for development of VX‐659. Also grants from The National Institute for Health Research and NIH. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation list made by Vertex Biostatistics or a randomisation vendor. Final list reviewed and approved by a designated unblinded statistician who is independent of the study team. Interactive web response sytem used to assign participants to treatment. |
| Allocation concealment (selection bias) | Low risk | Random allocation independent of study team. Use of interactive web response system. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | All participants, site personnel and Vertex study team were blinded to allocation. Protocol sets out conditions when blinding could/should be broken. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | All authors were only allowed access to study data after they were unblinded. No mention is made of other outcome assessors (e.g. clinicians who were not authors, but were involved in seeing participants and measuring outcomes of interest) and whether there was a possibility of them knowing allocated intervention. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All participants who were randomised are accounted for. |
| Selective reporting (reporting bias) | Unclear risk | States in methods that it would measure 12‐lead ECG and vital signs, though these may have been measured, they are not stated in results or supplement regardless of if they were unremarkable or not. |
| Other bias | Low risk | Different groups of participants are balanced in baseline characteristics, no significant difference between them. Detail in paper and its supplement does not cause any concern for other sources of bias not previously mentioned. |
Davies 2018b.
| Study characteristics | ||
| Methods | Phase 2 placebo‐controlled, double blind RCT. Parallel design with 3 arms; each arm comparing different doses to placebo. Multicentre study conducted at 48 sites in the UK, US, Ireland and Israel. Duration: 4 weeks active intervention (up to 12 weeks including run‐in and washout periods). |
|
| Participants | Eligible participants are aged 18 or older, with a confirmed CF diagnosis and a CFTR genotype of either F508del/MF or F508del/F508del. Arm 1 63 participants enrolled and randomised; all with genotype F508del/MF. Placebo (n = 10). Age, mean (SD): 26.6 (6.0) years. Gender split: 6 males, 4 females. FEV1 % predicted, mean (SD): 53.9 (12.0)%. Sweat chloride, mean (SD): 98.2 (13.3) mmol/L. CFQ‐R score (respiratory domain), mean (SD): 98.2 (13.3). VX‐659 80 mg (n = 11). Age, mean (SD): 32.0 (11.7) years. Gender split: 4 males, 7 females. FEV1 % predicted, mean (SD): 57.9 (10.8)%. Sweat chloride, mean (SD): 102.7 (7.0) mmol/L. CFQ‐R score (respiratory domain), mean (SD): 63.1 (18.5). VX‐659 240 mg (n = 20). Age, mean (SD): 31.4 (9.7) years. Gender split: 13 males, 7 females. FEV1 % predicted, mean (SD): 58.0 (16.8)%. Sweat chloride, mean (SD): 100.5 (9.0) mmol/L. CFQ‐R score (respiratory domain), mean (SD): 64.4 (17.8). VX‐659 400 mg (n = 22). Age, mean (SD): 27.2 (6.6) years. Gender split: 10 males, 12 females. FEV1 % predicted, mean (SD): 59.6 (15.4)%. Sweat chloride, mean (SD): 100.7 (11.6) mmol/L. CFQ‐R score (respiratory domain), mean (SD): 64.6 (20.7). Arm 2 29 participants enrolled and randomised all with the genotype F508del/F508del. Placebo plus tezacaftor plus ivacaftor (n = 11). Age, mean (SD): 32.5 (7.5) years. Gender split: 7 males, 4 females. FEV1 % predicted, mean (SD): 60.0 (12.6)%. Sweat chloride, mean (SD): 96.6 (11.4) mmol/L. CFQ‐R score (respiratory domain), mean (SD): 65.7 (17.4). VX‐659 400 mg plus tezacaftor plus ivacaftor (n = 18). Age, mean (SD): 33.4 (9.2) years. Gender split: 12 males, 6 females. FEV1 % predicted, mean (SD): 58.6 (13.3)%. Sweat chloride, mean (SD): 91.9 (11.6) mmol/L. CFQ‐R score (respiratory domain), mean (SD): 68.5 (14.1). Arm 3 29 participants enrolled and randomised, all with genotype F508del/MF Triple placebo (n = 6). Age, mean (SD): 24.5 (5.3) years. Gender split: 3 males, 3 females. FEV1 % predicted, mean (SD): 53.0 (12.3)%. Sweat chloride, mean (SD): 96.6 (4.3) mmol/L. CFQ‐R score (respiratory domain), mean (SD): 64.8 (24.0). VX‐659 400 mg plus tezacaftor plus VX‐561 (n = 19). Age, mean (SD): 32.5 (9.4) years. Gender split: 8 males, 11 females. FEV1 % predicted, mean (SD): 59.8 (12.6)%. Sweat chloride, mean (SD): 101.2 (9.5) mmol/L. CFQ‐R score (respiratory domain), mean (SD): 69.3 (13.9). |
|
| Interventions |
Arm 1 (F508del/MF genotype): once daily VX‐659 80 mg or 240 mg or 400 mg plus tezacaftor 100 mg once daily plus ivacaftor 150 mg twice daily versus triple placebo for 4 weeks. Arm 2 (F508del/F508del) : 4‐week run‐in of tezacaftor 100 mg once daily plus ivacaftor 150 mg twice daily (standard of care) followed by the addition of once daily VX‐659 400 mg or matched placebo to existing regimen for 4 weeks followed by 4‐week washout period of tezacaftor 100mg once daily plus ivacaftor 150 mg twice daily (standard of care). Arm 3 (F508del/MF): once daily VX‐659 400 mg plus tezacaftor 100 mg once daily plus VX‐561* 150 mg once daily versus triple placebo. *deuterated ivacaftor‐ administered once daily instead of twice daily. |
|
| Outcomes | Safety and side effects/adverse events: clinical laboratory values, electrocardiograms, vital signs. Absolute change in FEV1 % predicted at day 29 compared to baseline. Absolute change in sweat chloride concentration from baseline to day 29. Absolute change from baseline in quality of life: CFQ‐R respiratory domain at day 29. |
|
| Funding source | Vertex Pharmaceuticals supported the study, who in turn received funding from the Cystic Fibrosis Foundation for development of VX‐659. Also grants from The National Institute for Health Research and NIH. | |
| Notes | Different groups of participants are balanced in baseline characteristics, no significant difference between them. Detail in paper and it's supplement does not cause any concern for other sources of bias not previously mentioned. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation code made by Vertex Biometrics or a 'qualified randomisation vendor'. Randomisation stratified by ppFEV1 being less than or equal to/greater than 70%. |
| Allocation concealment (selection bias) | Low risk | Use of interactive web response system to allocate participants to groups. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | All participants, site personnel and Vertex study team were blinded to allocation. Protocol sets out conditions when blinding could/should be broken. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | All authors were only allowed access to trial data after they were unblinded. No mention is made of other outcome assessors (e.g. clinicians who weren't authors, but were involved in seeing participating patients and measuring outcomes of interest) and whether there was a possibility of them knowing allocated intervention. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All patients who were randomised are accounted for. |
| Selective reporting (reporting bias) | Unclear risk | States in methods that it would measure 12 lead ECG and vital signs, though these may have been measured, they are not stated in result or supplement regardless of if they were unremarkable or not. |
| Other bias | Low risk | Different groups of participants are balanced in baseline characteristics, no significant difference between them. Detail in paper and its supplement does not cause any concern for other sources of bias not previously mentioned. |
Donaldson 2014.
| Study characteristics | ||
| Methods | Double‐blind, placebo‐controlled RCT. Parallel design. Duration: 7 days. Multicentre: 17 sites in USA. |
|
| Participants | 66 participants. Mean (SD) age: 29 (8) years. Gender split: 40 female and 26 male. Disease severity: mean (SD) % predicted FEV1 70 (21)%, and mean (SD) sweat chloride 101 (11) mmol/L. There were no significant differences among the treatment groups at baseline. |
|
| Interventions |
Intervention: 4 sequential ascending doses of N6022 were assessed (5, 10, 20, and 40 mg/day) given by intravenous infusion once daily. Control: placebo (normal saline). |
|
| Outcomes |
Primary outcome Safety and tolerability (over 7 treatment days and 7 days of follow‐up)* Secondary outcomes Change from baseline in % predicted FEV1 (at Day 7)* Change from baseline in biomarkers of CFTR Function measured as sweat chloride mEq/L (at Day 7) |
|
| Funding source | Sponsored by Nivalis Therapeutics. | |
| Notes | * denotes outcomes relevant to this review. 4 sequential ascending doses of N6022 were assessed (5, 10, 20, and 40 mg/day) followed by a confirmatory cohort of participants at the highest dose. An independent Data Monitoring Committee adjudicated dose escalation at the completion of each cohort after review of unblinded safety data. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not stated. |
| Allocation concealment (selection bias) | Unclear risk | Not stated. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blind (participant, caregiver, investigator, outcomes assessor) achieved with intravenous administration of placebo (saline) using the same volume as the active drug groups. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Double‐blind (participant, caregiver, investigator, outcomes assessor) achieved with intravenous administration of placebo (saline) using the same volume as the active drug groups. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All randomised participants completed the 7 days of follow‐up. |
| Selective reporting (reporting bias) | Unclear risk | No full text publication of the study available. Limited results (without any statistical analysis) available on the ongoing trials database (www.clinicaltrials.gov). Unclear if all relevant information has been made available. |
| Other bias | Low risk | Baseline characteristics across the 5 treatment groups seem fairly well‐balanced despite small numbers in each group. |
Donaldson 2017.
| Study characteristics | ||
| Methods | Phase 1 double‐blind RCT. Parallel design. Duration: 28 days treatment. Multicentre (10 centres). |
|
| Participants | 51 adults with CF randomised. Mutation: CF homozygous for the F508del mutation. Age: over 18 years. Gender: 32 out of 51 participants were female. Lung function: FEV1 ≥ 40% of predicted normal for age, gender, and height (Hankinson standards). pre‐ or post‐bronchodilator value, at screening. Sweat chloride: ≥ 60 mEq/L. |
|
| Interventions |
Intervention: cavosonstat 2x daily 50 mg, 100 mg, or 200 mg. Control: placebo 2x daily. |
|
| Outcomes |
Primary outcome (no prespecified sample size) Safety (AE and SAE) * Secondary outcomes (at 28 days) Sweat chloride * FEV1* *CFQ‐R |
|
| Funding source | Sponsored by Nivalis Therapeutics. | |
| Notes | * Denotes an outcome relevant to this review. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No description of method. |
| Allocation concealment (selection bias) | Unclear risk | No description of method. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Likely low risk as double‐blind and placebo‐controlled but further information about this aspect of methodology not described. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Likely low risk as double‐blind and placebo‐controlled but further information about this aspect of methodology not described. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 2 participants unaccounted for in analysis, but unlikely to have affected result. |
| Selective reporting (reporting bias) | Low risk | Likely low risk ‐ all outcomes reported, but they appear to have been measured at other time‐points that are not reported (7 days and 14 days). |
| Other bias | Unclear risk | "Approximately two‐thirds of CF subjects were female; however, there was a greater proportion of males in the 200 mg BID dose group. Other baseline characteristics were similar across the treatment groups." Unclear if this gender imbalance may have influenced the results. |
Donaldson 2018.
| Study characteristics | ||
| Methods | Double‐blind, controlled Phase 2 RCT, which included a dose‐ranging arm. Parallel design. Duration: 28 days treatment followed by 28 days observation. Multicentre. |
|
| Participants | Mutation: participants homozygous for F508del mutation, and heterozygous participants with 1 F508del mutation and 1 G551D mutation. Only the 18 heterozygous participants are included in the analysis of this review (this is because the placebo participants in the homozygous arms of the trial were pooled, and this was judged to negate the effects of randomisation). Age: heterozygous participants ‐ active drug arm mean (SD) age 26.6 (7.0) years, placebo arm mean (SD) age 34.5 (7.6) years. Gender split: heterozygous participants ‐ active drug arm 6/14 (43%) participants female; placebo arm 3/4 (75%) female. Lung function, mean (SD): heterozygous participants ‐ active drug arm baseline FEV1 59.1 (16.6)% predicted, placebo arm baseline FEV1 62.6 (12.7)% predicted. Sweat chloride levels, mean (SD): heterozygous participants ‐ active drug arm baseline 52.9 (19.6); placebo arm baseline 56.7 (22.1). |
|
| Interventions |
Intervention: tezacaftor 100 mg/day and ivacaftor 150 mg. Control: ivacaftor 150 mg (heterozygous arm only). |
|
| Outcomes |
Primary outcome
Safety through day 56* Secondary outcomes Absolute change in FEV1 at day 28* Relative change in FEV1 at day 28* Change in CFQ‐R respiratory domain (day 28)* |
|
| Funding source | Vertex Pharmaceuticals and grants from the NIH. | |
| Notes | * Denotes outcomes relevant to this review. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not described. |
| Allocation concealment (selection bias) | Unclear risk | Method not described. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Matched placebo ‐ double‐blind RCT. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Matched placebo ‐ double‐blind RCT. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All randomised participants included in analysis. |
| Selective reporting (reporting bias) | Low risk | All outcomes appear to have been reported. |
| Other bias | Unclear risk | Baseline characteristics of heterozygous participants somewhat imbalanced across groups (e.g. sex, age, FEV1). However, this imbalance may be due to small numbers (active drug arm n = 14 and placebo arm n = 4) and unclear if the imbalance has influenced results. |
Heijerman 2019.
| Study characteristics | ||
| Methods | Phase 3 double‐blind RCT. Parallel design. Multicentre study conducted at 44 sites in 4 countries (Belgium, the Netherlands, the UK and the USA). Duration: 4 weeks with a further 4 weeks follow‐up period followed by participants being invited to a 96‐week open‐label extension study (VX17‐445‐105; NCT03525574). |
|
| Participants | Eligible participants were aged 12 or above with a confirmed diagnosis of CF and 2 copies of F508del, FEV1 % predicted 40% ‐ 90% and in 'stable condition' as judged by study investigators. 108 participants were randomised and 107 participants who received a dose of the study drug during the treatment period were included in analyses. Intervention group (n = 55) Gender, females: 31 (56%). Age, mean (SD): 28.8 (11.5) years. Age distribution: ≥12 to <18 years: 16 (29%); ≥18 years: 39 (71%). FEV1 % predicted, mean (SD): 61.6 (15.4). FEV1 % predicted, distribution: <40%: 6 (11%); ≥40% to <70%: 31 (56%); ≥70% to ≤90%: 18 (33%); >90%: 0. BMI, mean (SD): 21.75 (3.19) kg/m². Sweat chloride concentration, mean (SD): 91.4 (11·0) mmol/L. CFQ‐R respiratory domain score, mean (SD): 70.6 (16.2). CFTR modulator therapy: yes 32 (58%); no 23 (42%). Control group (n = 52). Gender, females: 24 (44%). Age, mean (SD): 27·9 (10.8) years. Age distribution: ≥12 to <18 years: 14 (27%); ≥18 years: 38 (73%). FEV1 % predicted, mean (SD): 60.2 (14.4). FEV1 % predicted, distribution: <40%: 4 (8%); ≥40% to <70%: 34 (65%); ≥70% to ≤90%: 14 (27%); >90%: 0. BMI, mean (SD): 21.88 (4.12) kg/m². Sweat chloride concentration, mean (SD): 90.0 (12.3) mmol/L. CFQ‐R respiratory domain score, mean (SD): 72.6 (17.9). CFTR modulator therapy: yes 34 (65%); no 18 (35%). |
|
| Interventions | 4‐week run‐in period for both intervention and control groups: tezacaftor 100 mg daily, ivacaftor 150 mg every 12 hours. Intervention (n = 55): elexacaftor 200 mg once daily plus tezacaftor 100 mg once daily plus ivacaftor 150 mg every 12 hours. Control (n = 52): placebo matched to elexacaftor once daily plus tezacaftor 100 mg once daily plus ivacaftor 150 mg every 12 hours. |
|
| Outcomes | Outcomes measured at baseline, 2 weeks and 4 weeks. Primary outcome FEV1 % predicted (absolute change from baseline) Secondary outcomes Survival QoL‐ CFQ‐R respiratory domain Adverse effects Sweat chloride (change from baseline) Weight (relative change from baseline) Height (relative change from baseline) ECG Clinical laboratory values Pulse oximetry |
|
| Funding source | Vertex Pharmaceuticals supported the study and were also involved in writing the study; however, the corresponding author had final responsibility for the decision to submit for publication. | |
| Notes | ClinicalTrials.gov: NCT03525548. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Participants randomly assigned in a 1:1 ratio by an interactive web response system. Randomisation was stratified by FEV1 % predicted. |
| Allocation concealment (selection bias) | Low risk | Study sites entered participant demographic information and stratification criteria into the interactive web response system, which established the treatment group and corresponding treatment kit numbers. ELX/TEZ/IVA and TEZ/IVA regimens were distributed via identical treatment kits. An independent vendor, which was not involved in any other operational parts of this trial, operated and maintained the system. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Participants and people responsible for participants care are all blinded to treatment allocation by use of identical treatment kits, which were matched in the appearance and number of tablets. Treatment kits were provided to participants in sealed blister cards only when the participants were on site. All participants, investigators and trial personnel were masked to treatment assignments during the conduct of this trial. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | All investigators and trial personnel were masked to treatment assignments during the conduct of this trial. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 108 participants were randomised and 107 participants who received a dose of the study drug during the treatment period were included in analyses.. |
| Selective reporting (reporting bias) | Low risk | All outcomes stated in protocol were reported upon. |
| Other bias | Unclear risk | None noted; well‐matched baseline characteristics. However as it is stated that Vertex funded the study, it is unclear as to the extent to which they were involved in designing, writing up and publishing the report. |
Horsley 2017.
| Study characteristics | ||
| Methods | Phase 1b RCT. Parallel design. 14 centres in Australia, Czech Republic, Germany and UK. Duration: 28 days. |
|
| Participants | 27 participants aged 18 or over, homozygous for F508del and with FEV1 % predicted at least 40% at baseline. FDL169 400 mg (n = 6). Age, mean (range): 31.5 (18 ‐ 56) years. Gender split: 3 males, 3 females. FEV1 % predicted, mean (SD): 82.2 (22.5)%. Sweat chloride, mean (SD): 96.9 (9.5) mmol/L. CFQ‐R score (respiratory domain), mean (SD): 89.7 (8.1). FDL169 600 mg (n = 6). Age, mean (range): 37.7 (18 ‐ 62) years. Gender split: 3 males, 3 females. FEV1 % predicted, mean (SD): 59.3 (9.9)%. Sweat chloride, mean (SD): 101.8 (10.1) mmol/L. CFQ‐R score (respiratory domain), mean (SD): 74.0 (11.5). FDL169 800 mg (n = 8). Age, mean (range): 26.5 (21 ‐ 37) years. Gender split: 4 males, 4 females. FEV1 % predicted, mean (SD): 85.3 (13.5)%. Sweat chloride, mean (SD): 98.5 (9.8) mmol/L. CFQ‐R score (respiratory domain), mean (SD): 77.0 (18.8). Placebo (n = 7). Age, mean (range): 30.4 (20 ‐ 51) years. Gender split: 2 males, 5 females. FEV1 % predicted, mean (SD): 64.3 (21.5)%. Sweat chloride, mean (SD): 104.4 (14.1) mmol/L. CFQ‐R score (respiratory domain), mean (SD): 75.4 (11.6). |
|
| Interventions |
Cohort 1 (n = 15): FDL169 400 mg 3x daily (n = 6) versus FDL169 600 mg 3x daily (n = 6) versus placebo (n = 3). Cohort 2 (n = 12): FDL169 800 mg 3x daily (n = 8) versus placebo (n = 4). |
|
| Outcomes | Safety and tolerability including adverse effects, laboratory tests, ECG, and vital signs. Pharmacokinetics of numerous doses of FDL169. Exploratory outcomes: changes in "CFTR activity" (sweat chloride levels), pulmonary function (FEV1 % predicted, respiratory symptoms), CFQ‐R respiratory domain. |
|
| Funding source | Flatley Discovery Lab was the sponsor for this Phase 1b study. | |
| Notes | We also obtained a poster from the author which was presented at a conference. A study is planned for 2019 to evaluate the corrector FDL169 in combination with potentiator FDL176 in individuals with CF homozygous for F508del. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | States that participants are randomised, but does not state the method by which they are randomised. |
| Allocation concealment (selection bias) | Unclear risk | Does not state methods of allocation concealment. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Does not state who was and was not blinded during the study. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Does not state how outcome assessors were blinded during study. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All participants who were randomised are accounted for. |
| Selective reporting (reporting bias) | Low risk | All outcomes stated in the methods are reported in the results. |
| Other bias | Unclear risk | As the only information available was as part of a poster and a full detailed publication has not been published, it is difficult to say with any certainty whether there are other sources of bias in the process of this study. |
Keating 2018.
| Study characteristics | ||
| Methods | Phase 2 double‐blind RCT. Parallel design. Multicentre: 38 sites in the US, the Netherlands, Belgium and Australia. Duration: 4 weeks intervention period (12 weeks for those arms with a 4‐week run‐in and 4‐week washout). Randomisation of participants was stratified by FEV1 % predicted being less than or equal to 70% versus greater than 70%, except for the first 10 F508del/MF participants who were not stratified. |
|
| Participants | All participants were aged 18 years or older, with CFTR genotype of either F508del/MF or F508del/F508del. They must have had FEV1 % predicted between 40% and 90% at screening, as well as stable disease. 123 participants underwent randomisation and received at least 1 dose of the intervention. Participants with F508del/MF (n = 65). Elexacaftor 50 mg 1x daily plus tezacaftor 100 mg 1x daily plus ivacaftor 150 mg every 12 hours (n = 10). Age, mean (SD): 27.1 (7.4) years. Gender split: 4 males, 6 females. FEV1 % predicted, mean (SD): 56.4 (14.6)%. Sweat chloride, mean (SD): 103.1 (7.8) mmol/L. CFQ‐R score (respiratory domain), mean (SD): 62.8 (21.9). Elexacaftor 100 mg 1x daily plus tezacaftor 100 mg 1x daily plus ivacaftor 150 mg every 12 hours (n = 22). Age, mean (SD): 31.8 (8.3) years. Gender split: 15 males, 7 females. FEV1 % predicted, mean (SD): 60.0 (15.5)%. Sweat chloride, mean (SD): 103.6 (12.2) mmol/L. CFQ‐R score (respiratory domain), mean (SD): 65.9 (13.4). Elexacaftor 200 mg 1x daily plus tezacaftor 100 mg 1x daily plus ivacaftor 150 mg every 12 hours (n = 21). Age, mean (SD): 33.3 (10.3) years. Gender split: 10 males 11 females. FEV1 % predicted, mean (SD): 59.4 (18.0)%. Sweat chloride, mean (SD): 103.9 (9.7) mmol/L. CFQ‐R score (respiratory domain), mean (SD): 61.1 (17.5). Triple placebo (n = 12). Age, mean (SD): 29.7 (7.5) years. Gender split: 10 males, 2 females. FEV1 % predicted, mean (SD): 59.0 (14.9)%. Sweat chloride, mean (SD): 103.1 (8.2) mmol/L. CFQ‐R score (respiratory domain), mean (SD): 57.4 (14.1). Participants with F508del/F508del (n = 28)* Elexacaftor 200 mg plus tezacaftor plus ivacaftor (n = 21). Age, mean (SD): 29.9 (7.6) years. Gender split: 12 males, 9 females. FEV1 % predicted, mean (SD): 60.0 (15.1)%. Sweat chloride, mean (SD): 92.7 (11.1) mmol/L. CFQ‐R score (respiratory domain), mean (SD): 71.2 (17.3). Placebo plus tezacaftor plus ivacaftor (n = 8). Age, mean (SD): 27.9 (8.0) years. Gender split: 6 males, 2 females. FEV1 % predicted, mean (SD): 62.8 (13.2)%. Sweat chloride, mean (SD): 99.5 (9.0) mmol/L. CFQ‐R score (respiratory domain), mean (SD): 73.0 (22.3). * had a 4‐week run in of tezacaftor‐ivacaftor and a further 4‐week post‐invention washout period of tezacaftor‐ivacaftor. Participants with F508del/MF (n = 29) Elexacaftor 200 mg plus tezacaftor plus VX‐561 (n = 21). Age, mean (SD): 30.6 (9.5) years. Gender split: 11 males, 10 females. FEV1 % predicted, mean (SD): 60.6 (17.5)%. Sweat chloride, mean (SD): 100.8 (15.4) mmol/L. CFQ‐R score (respiratory domain), mean (SD): 63.8 (18.2). Triple placebo (n = 8). Age, mean (SD): 27.8 (5.2) years. Gender split: 3 males, 5 females. FEV1 % predicted, mean (SD): 60.7 (14.0)%. Sweat chloride, mean (SD): 96.4 (1.5) mmol/L. CFQ‐R score (respiratory domain), mean (SD): 43.8 (21.9). |
|
| Interventions |
Arm 1: 1x daily elexacaftor 50 mg or elexacaftor 100 mg or elexacaftor 200 mg plus tezacaftor 100 mg plus 2x daily (every 12 hours) ivacaftor 150 mg versus triple placebo. Arm 2: 4‐week run in period of 1x daily tezacaftor 100 mg plus ivacaftor 150 mg for all participants; then 4‐week intervention period of 1x daily elexacaftor 200 mg and tezacaftor 100 mg plus 2x daily (every 12 hours) ivacaftor 150 mg versus matched placebo; then a 4 week washout period of 1x daily tezacaftor 100 mg plus ivacaftor 150 mg for all participants. Arm 3: 1x daily elexacaftor 200 mg and tezacaftor 100 mg and VX‐561 150 mg once daily versus triple placebo. |
|
| Outcomes |
Primary outcomes 1. Safety (adverse events, clinical lab values, electrocardiograms, vital signs, pulse oximetry) 2. Tolerability 3. Absolute change in FEV1 % predicted from baseline to day 29 Secondary outcomes 1. Absolute change in sweat chloride concentrations from baseline to day 29 2. Quality of life ‐ absolute change in CFQ‐R respiratory domain from baseline to day 29. |
|
| Funding source | Vertex Pharmaceuticals who received funding from the CF Foundation to develop elexacaftor. The NIH gave a grant to the University of Alabama at Birmingham. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation code made by Vertex Biostatistics or a 'qualified randomisation vendor'. Randomisation stratified by FEV1 % predicted (less than or equal to 70% versus greater than 70%). |
| Allocation concealment (selection bias) | Low risk | Use of interactive web response system for allocation. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | All participants, site personnel and Vertex study team related to the study were blinded. A clear statement on when unblinding is necessary or permitted is provided in the protocol. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | All authors were only allowed access to study data after they were unblinded. No mention is made of other outcome assessors (e.g. clinicians who were not authors, but were involved in seeing participants and measuring outcomes of interest) and whether there was a possibility of them knowing allocated intervention. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All participants who were randomised are accounted for. |
| Selective reporting (reporting bias) | Unclear risk | States in methods that it would measure 12‐lead ECG and vital signs, though these may have been measured, they are not stated in results or supplement regardless of if they were unremarkable or not. |
| Other bias | Low risk | Different groups of participants are balanced in baseline characteristics, no significant difference between them. Detail in paper and its supplement does not cause any concern for other sources of bias not previously mentioned. |
McCarty 2002.
| Study characteristics | ||
| Methods | Phase 1, placebo‐controlled RCT. Parallel design. Multicentre conducted at 4 sites in North America. Duration: single‐dose assessment. Participants were monitored for 2 days followed up at 1 week. |
|
| Participants | Mutation: all 37 participants were homozygous for the F508del mutation and were described as having mild CF. Age: 18 years or over; age range 18 ‐ 38 years. Gender split: 21 males and 16 females. Lung function: participants were eligible if they had a baseline FEV1 ≥ 60% predicted and had not endured pulmonary colonisation by a drug resistant organism within 12 months of screening. |
|
| Interventions |
Intervention 1: placebo. Intervention 2: CPX in the following escalating doses: 1 mg CPX; 3 mg CPX; 10 mg CPX; 30 mg CPX; 100 mg CPX; 300 mg CPX; 1000 mg CPX. |
|
| Outcomes |
Primary outcome 1. Safety profile of CPX including occurrence of adverse events* Secondary outcomes 1. Nasal potential difference values 2. Sweat chloride values (mEq/L) * 3. Analysis of blood haemoglobin and serum potassium |
|
| Funding source | SciClone Pharmaceuticals, and grants from the NIH. | |
| Notes | * denotes outcomes relevant to this review. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not stated. |
| Allocation concealment (selection bias) | Unclear risk | Not stated. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | There was insufficient information on how participant or study personnel blinding were maintained. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | There was insufficient information on how outcome assessor blind was maintained. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No report of withdrawals and all originally randomised participants were included in the analysis. |
| Selective reporting (reporting bias) | Low risk | Protocol not available and outcomes not reported on the ongoing online database (www.clinicaltrials.gov). Reported results corresponded to outcomes listed in methods section. |
| Other bias | Unclear risk | Unclear whether baseline characteristics were well matched. |
Middleton 2019.
| Study characteristics | ||
| Methods | Phase 3 double‐blind RCT. Parallel design. Multicentre study conducted at 115 sites in 13 countries across North America, Europe and Australia. Duration: 28‐day screening period followed by a 24‐week intervention period followed by a further 28‐day safety follow‐up, after which participants were invited to a 96‐week open‐label extension study in which all participants receive active treatment (VX17‐445‐105; ClinicalTrials.gov number, NCT03525574). |
|
| Participants | Eligible participants were 12 years of age or older with CF and 1 copy of F508del and 1 copy of a MF allele, FEV1 % predicted 40% ‐ 90% and in 'stable condition' as judged by study investigators. 405 participants randomised, 403 received at least 1 dose of intended treatment and were included in the analyses. Intervention group (n = 202). Gender, females: 96 (48.0%). Age, mean (SD): 25.6 (9.7) years. Age distribution: ≥12 to <18 years: 56 (28.0%); ≥18 years: 144 (72.0%). FEV1 % predicted, mean (SD): 61.6 (15.0). FEV1 % predicted, distribution: <40%: 18 (9.0%); ≥40% to <70%: 114 (57.0%); ≥70% to ≤90%: 66 (33.0%); >90%: 2 (1.0%). BMI, mean (SD): 21.49 (3.07) kg/m². Sweat chloride concentration, mean (SD): 102.3 (11.9) mmol/L. CFQ‐R respiratory domain score, mean (SD): 68.3 (16.9). Control group (n = 201). Gender, females: 98 (48.3%). Age, mean (SD): 26.8 (11.3) years. Age distribution: ≥12 to <18 years: 60 (29.6%); ≥18 years: 143 (70.4%). FEV1 % predicted, mean (SD): 61.3 (15.5). FEV1 % predicted, distribution: <40%: 16 (7.9%); ≥40% to <70%: 120 (59.1%); ≥70% to ≤90%: 62 (30.5%); >90%: 5 (2.5%). BMI, mean (SD): 21.31 (3.14) kg/m². Sweat chloride concentration, mean (SD): 102.9 (9.8) mmol/L. CFQ‐R respiratory domain score, mean (SD): 70.0 (17.8). |
|
| Interventions |
Intervention (n = 202): elexacaftor 200 mg once daily plus tezacaftor 100 mg once daily plus ivacaftor 150 mg every 12 hours. Control (n = 201): triple‐matched placebo. |
|
| Outcomes | Outcomes measured at weeks 4, 8, 12, 16 and 24. Primary outcome FEV1 % predicted (absolute change from baseline at week 4) Secondary outcomes FEV1 % predicted (absolute change from baseline at week 24) Extra courses of antibiotic (exacerbations) at week 24 Sweat chloride (absolute change from baseline at week 4 and week 24) QoL (CFQ‐R respiratory domain) (change from baseline at week 4 and week 24) BMI (absolute change from baseline at week 24) BMI‐for‐age z score (absolute change from baseline at week 24) Weight (absolute change from baseline at week 24) Survival Adverse effects and safety Hospitalisation |
|
| Funding source | Vertex Pharmaceuticals supported the study and were also involved in writing the study; however, the first 2 authors and last 2 authors wrote the first draft of the manuscript and made final decisions regarding the content of the submitted manuscript. | |
| Notes | Eudract No. 2018‐000183‐28. 403 participants underwent randomisation and received at least 1 dose, therefore included in analyses; 400 participants went on to the open‐label extension. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | An interactive web response system used to assign participants to treatment in a 1:1 ratio stratified by FEV1 % predicted, age at screening and gender. Protocol states that the randomization code list would be produced by Vertex Biometrics or a qualified randomization vendor. |
| Allocation concealment (selection bias) | Low risk | Interactive web response system used to assign participants to treatment. The pharmacist or designated study site staff will maintain information regarding the dates and amounts of (1) study drug received; (2) study drug dispensed to the participants; and (3) study drug returned by the participants. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Study drug and matched placebo administered orally and all participants received the same number of tablets each day to maintain the blind. All participants (and their parents/caregivers/companions), site personnel (including the investigator, the site monitor, and the study team), and members of the Vertex study team blinded to the treatment codes. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | All site personnel (including the investigator, the site monitor, and the study team), and members of the Vertex study team blinded to the treatment codes.The interim analysis was performed by an external independent biostatistician who was not involved in the study, and the results were reviewed by the independent data monitoring committee. After the interim analysis, the study continued to completion and remained double‐blinded through week 24, apart from the planned unblinding of a limited Vertex team that was tasked with preparing regulatory submissions. To protect study integrity, members of the limited Vertex unblinded team were not involved in and did not influence the ongoing conduct of the study. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 403/405 people who were randomised received at least 1 dose. They were all included in all applicable analyses. 3 discontinued in the intervention group (1 became pregnant and 2 due to AEs) after receiving at least 1 dose. All 400 remaining participants were enrolled into an open‐label extension study. |
| Selective reporting (reporting bias) | Low risk | All outcomes stated in the protocol are reported in either the primary publication or supplement. |
| Other bias | Unclear risk | None noted; well‐matched baseline characteristics. However as it is stated that Vertex funded the study, it is unclear as to the extent to which they were involved in designing, writing up and publishing the report. |
PROGRESS 2017.
| Study characteristics | ||
| Methods | Phase 3 RCT.
Double‐blinded rollover study (participants on active treatment continued their treatment, participants on placebo were randomised to 1 of the 2 active interventions).
Parallel design. Multicentre: 191 sites in 15 countries across North America, Australia and Europe Duration: 96 weeks. |
|
| Participants | Mutation: homozygous or heterozygous for the F508del mutation. Age: 12 years and older. Gender: both males and females. Confirmed diagnosis of CF. Participants have previously participated in TRAFFIC or TRANSPORT and completed 24 weeks of treatment. |
|
| Interventions |
Intervention 1: 600 mg lumacaftor once daily + 250 mg ivacaftor every 12 hours (continued treatment). Intervention 2: 600 mg lumacaftor once daily + 250 mg ivacaftor every 12 hours (rolled over from placebo). Intervention 3: 400 mg lumacaftor every 12 hours + 250 mg ivacaftor every 12 hours (continued treatment). Intervention 4: 400 mg lumacaftor every 12 hours + 250 mg ivacaftor every 12 hours (rolled over from placebo). |
|
| Outcomes |
Primary outcome measure
Treatment cohorts: safety of long‐term treatment based on AEs, clinical laboratory values (serum chemistry, haematology, coagulation studies, and urinalysis), standard digital ECGs, vital signs, and pulse oximetry at 100 weeks
Secondary outcome measures 1. Absolute change from baseline in % predicted FEV1 at 96 weeks 2. Relative change from baseline in % predicted FEV1 at 96 weeks 3. Absolute change from baseline in CFQ‐R respiratory domain score at 96 weeks 4. Absolute change from baseline in BMI at 100 weeks 5. Number of pulmonary exacerbations starting from the previous study through 96 weeks 8. Event of having at least 1 pulmonary exacerbation in the current study through 96 weeks |
|
| Funding source | Sponsored by Vertex Pharmaceuticals Inc. | |
| Notes | Long‐term extension of the TRAFFIC and TRANSPORT studies in which participants receiving an active treatment continued with this treatment and those receiving placebo were randomised to receive 1 of the 2 active treatments from the TRAFFIC and TRANSPORT. Additional analyses were conducted comparing participants receiving 400 mg lumacaftor every 12 hours + 250 mg ivacaftor every 12 hours to an observational registry cohort of matched controls. These analyses are not reported in this review. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Only the placebo groups from the previous studies were randomised. Participants randomly assigned (in a 1:1:1 ratio) to 1 of 3 study groups; the randomisation was established by an interactive web response system. Randomisation was stratified according to age (< 18 years versus ≥ 18 years), sex, and pulmonary function (% predicted FEV1 at screening, < 70 versus ≥ 70). |
| Allocation concealment (selection bias) | Low risk | Only the placebo groups from the previous studies were randomised. The randomisation was established by an interactive web response system. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | These were double‐blind studies in which the participant and study team remained blinded to the treatment assignments. Interventions were matched in appearance and packaging. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | These were double‐blind studies in which the participant and study team remained blinded to the treatment assignments. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Attrition rates reported, all participants randomised who received at least 1 dose of study medication were included in analysis. Missing data were investigated in sensitivity analyses. |
| Selective reporting (reporting bias) | Low risk | All listed outcomes reported in the results. |
| Other bias | Low risk | A 'rate of change' analysis showed that baseline characteristics across the groups were well balanced. |
Ratjen 2017.
| Study characteristics | ||
| Methods | Phase 3, placebo‐controlled RCT. Parallel design. Multicentre: 54 sites in 9 countries (USA, Australia, Belgium, Canada, Denmark, France, Germany, Sweden, and the UK). Duration: 24 weeks. |
|
| Participants | 206 participants randomised (ivacaftor n = 104; placebo n = 102); 1 from each arm withdrew before first dose leaving 204 participants in the analysis. Mutation: all participants were homozygous for the F508del mutation. Age: eligibility criteria 6 ‐ 11 years, mean (SD) age was 8.8 (1.6) years. Gender split: 83 males and 121 females. Lung function: participants must have a FEV1 (% predicted) of 70 or more, and LCI2.5 of 7.5 or more. |
|
| Interventions |
Intervention: lumacaftor 200 mg every 12 hours in combination with ivacaftor 250 mg every 12 hours. Control: matched placebo. |
|
| Outcomes |
Primary outcome
Mean absolute change in LCI2.5 from baseline at all study visits up to and including week 24* Secondary outcomes Absolute change in BMI up to and including week 24* Absolute change in CFQ‐R respiratory domain score up to and including week 24* Absolute change in LCI5.0 up to and including week 24* Absolute change in sweat chloride up to and including week 24* Absolute change in FEV1 (% predicted) up to and including week 24* Relative change in FEV1 (% predicted) up to and including week 24* Absolute change in BMI‐for‐age z score up to and including week 24* Absolute change in weight up to and including week 24* Absolute change in weight‐for‐age z score up to and including week 24* Absolute change in height up to and including week 24* Absolute change in height‐for‐age z score up to and including week 24* Absolute change in TSQM domains up to and including week 24 Time‐to‐first pulmonary exacerbation up to and including week 24 Event of having at least 1 pulmonary exacerbation up to and including week 24 Number of pulmonary exacerbations up to and including week 24 Number of participants with adverse events and serious adverse events up to week 24* |
|
| Funding source | Vertex Pharmaceuticals. | |
| Notes | * denotes outcomes relevant to this review. Analyses were performed as the absolute change from baseline (including all measurements up to and including week 24, both on‐treatment measurements and measurements after treatment discontinuation) ‐ was based on a MMRM, adjusted for the baseline measurement of the outcome, baseline weight (less than 25 kg versus 25 kg or over and baseline FEV1 (% predicted) (less than 90% compared to 90% or more), with treatment‐by‐visit interaction as fixed effects, participant as a random effect. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Blocked randomisation was performed via an interactive web response system, stratified by baseline weight and FEV1 (% predicted). |
| Allocation concealment (selection bias) | Low risk | Randomisation was performed centrally via the interactive web response system. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double‐blinding was achieved by using placebo tablets visually identical to the test product. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | It was not stated whether outcome assessment was blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Attrition rates were reported and an ITT approach was taken to analysis, with all randomised participants who received at least 1 dose of the study drug included in analysis (1 participant in each group was randomised but did not receive the study drug). |
| Selective reporting (reporting bias) | High risk | Several outcomes which are listed in the methods (e.g. LCI5.0, time‐to‐first pulmonary exacerbation, absolute change in TSQM domains) but are not presented in the results. |
| Other bias | Low risk | Baseline characteristics were similar across the 2 groups. |
Rubenstein 1998.
| Study characteristics | ||
| Methods | A pilot, placebo‐controlled RCT. Parallel design. Single centre. Duration: 1 week. |
|
| Participants | Mutation: homozygous for F508del mutation. Age, mean (SD): participants were eligible if 14 years or older, placebo group 24.8 (4.9) years; intervention group: 22.3 (5.9) years. Gender split: placebo group 4 males and 5 females; intervention group 5 males and 4 females. Lung function: baseline mean (SD) FVC % predicted placebo group: 65.5 (18.6); intervention group 73.4 (20.3). Baseline mean (SD) FEV1 % predicted placebo group 47.5 (22.1); intervention group 57.8 (27.2). |
|
| Interventions | 18 participants were allocated to either intervention or placebo group (9 participants in each group). Intervention 1: placebo. Intervention 2: sodium 4‐phenylbutyrate (also known as Buphenyl or 4PBA) 19 g, orally administered, in 3 daily doses of 6 g, 6 g, and 7 g. |
|
| Outcomes | 1. Changes from baseline in nasal potential difference in 1 week 2. Change from baseline in sweat chloride in 1 week* 3. 4BPA metabolites in plasma and urine after 1 week 4. Side effects* |
|
| Funding source | NIH and Cystic Fibrosis Foundation. | |
| Notes | * denotes outcomes relevant to this review. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Study article states that "randomization and blinding were performed by the Johns Hopkins Hospital Investigational Drug Pharmacy" but exact method of randomisation has not been described. |
| Allocation concealment (selection bias) | Unclear risk | Study article states that "randomization and blinding were performed by the Johns Hopkins Hospital Investigational Drug Pharmacy" but exact method of allocation concealment has not been described. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Described as double‐blind. Study article states that "randomization and blinding were performed by the Johns Hopkins Hospital Investigational Drug Pharmacy" but exact method of blinding has not been described. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Described as double‐blind. Study article states that "randomization and blinding were performed by the Johns Hopkins Hospital Investigational Drug Pharmacy" but exact method of blinding has not been described. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Data were analysed with 9 participants each group, equivalent to the number originally randomised. |
| Selective reporting (reporting bias) | Low risk | Protocol not available and outcome not presented on the ongoing trials database (www.clinicaltrials.gov/). Outcomes reported in the 'methods' were reported in the 'results' so selective reporting bias is low. |
| Other bias | Low risk | "... baseline characteristics between the groups were similar with respect to age, gender, pancreatic sufficiency, and baseline pulmonary function." |
Taylor‐Cousar 2017.
| Study characteristics | ||
| Methods | Placebo‐controlled RCT. Parallel design. Duration: 24 weeks. Multicentre in North America and Europe. |
|
| Participants | 510 participants diagnosed with CF. Age: inclusion criteria 12 years and older, 23% were aged 12 ‐ 18 years. Mutation: homozygous for F508del. Gender: 49% female. Mean FEV1 at baseline: 60% (9.4% had baseline FEV1 < 40% predicted, 2% had baseline FEV1 > 90% predicted). Mean baseline sweat chloride: 100.5. Mean BMI: 21. |
|
| Interventions |
Intervention: 100 mg tezacaftor 1x daily and 150 mg ivacaftor 2x daily. Control: placebo. |
|
| Outcomes |
Primary outcome Absolute change in FEV1 % predicted (from baseline through week 24) Secondary outcomes Relative change in FEV1 % predicted (from baseline through week 24) Number of pulmonary exacerbations (through week 24) Absolute change in BMI (from baseline at week 24) Absolute change in CFQ‐R respiratory domain score (from baseline through week 24) Safety and tolerability assessments based on AEs, clinical laboratory values (i.e., haematology, serum chemistry, coagulation studies, vitamin levels, lipid panel, and urinalysis), standard 12‐lead ECGs, vital signs, pulse oximetry, and spirometry Time‐to‐first pulmonary exacerbation (through week 24) Absolute change in sweat chloride (from baseline through week 24) Absolute change in BMI z score (from baseline at week 24 (in participants under 20 years of age at time of screening)) Absolute change in body weight (from baseline at week 24) PK parameters of VX‐661, M1‐661, M2‐661, ivacaftor, and M1‐ivacaftor Absolute change in CFRSD severity score (from baseline through week 24) Absolute change in duration of physical activity during the day (from baseline through week 24) Absolute change in duration of sleep time and sleep quality during the night (from baseline through week 24) Absolute change in PSQI score (from baseline through week 24 (in participants under 18 years of age)) Absolute change in QoL assessment (SF‐12) physical, mental, and utility component scores (at weeks 12 and 24) Absolute change in inflammatory mediators (from baseline at week 24) Absolute change in sputum microbiology (from baseline at week 24) Absolute change in serum IRT (from baseline at week 24) |
|
| Funding source | Vertex Pharmaceuticals. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Statistician separate to study team produced a list of randomisation codes and allocations assigned via web‐based interactive system (information provided in online protocol). |
| Allocation concealment (selection bias) | Low risk | Web‐based interactive system. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Matched placebo ‐ all relevant people blinded (participants and study personnel). |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Matched placebo ‐ all relevant people blinded (participants and study personnel). |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 1 participant who was randomised but did not receive the trial intervention was excluded from efficacy and safety analyses. A further 5 participants who were randomised and received the trial intervention were found to have an ineligible or unconfirmed CFTR genotype were excluded from efficacy analyses. Small numbers of excluded participants (up to 6 out of 510) unlikely to have introduced bias. |
| Selective reporting (reporting bias) | High risk | The following outcomes were measured (according to the protocol), but not reported.
|
| Other bias | Low risk | Final manuscript written with the assistance of medical writers funded by the sponsor, however, this is unlikely to have introduced bias. |
TRAFFIC 2015.
| Study characteristics | ||
| Methods | Double‐blind, placebo‐controlled Phase 3 RCT. Parallel design. Multicentre: 90 sites in North America, Australia and Europe. Estimated sample size: 559. Duration: 24 weeks. |
|
| Participants | 549 participants with a confirmed diagnosis of CF and stable disease (as judged by the investigator). Mean age (range): treatment arm 1 24.7 (12 ‐ 54) years; treatment arm 2 25.5 (12 ‐ 57) years; placebo 25.0 (12 to 64 years). Gender: 295 (54%) males; 254 (46%) females. Mutation: homozygous for the F508del mutation. Lung function: FEV1 between ≥ 40% and ≤ 90% of predicted normal for age, sex, and height. |
|
| Interventions |
Intervention 1 (n = 183): 600 mg of lumacaftor 1x daily and 250 mg of ivacaftor every 12 hours. Intervention 2 (n = 182): 400 mg of lumacaftor every 12 hours and 250 mg of ivacaftor every 12 hours. Intervention 3 (n = 184): lumacaftor‐matched placebo every 12 hours in combination with ivacaftor‐matched placebo every 12 hours. |
|
| Outcomes |
Primary outcome measure Absolute change in % predicted FEV1 (% predicted) at 24 weeks Secondary outcome measures 1. Relative change in % predicted FEV1 (% predicted) at 24 weeks 2. Absolute change in BMI at 24 weeks 3. Number of pulmonary exacerbations at 24 weeks 4. Absolute change in CFQ‐R respiratory domain score at 24 weeks 5. Absolute change in BMI z score at 24 weeks 6. Absolute change in body weight at 24 weeks 7. Time‐to‐first pulmonary exacerbation at 24 weeks 8. Event of having at least 1 pulmonary exacerbation through week 24 9. Absolute change in EuroQol 3 Level (EQ 5D 3L) at 24 weeks 10. Absolute change in TSQM domains at 24 weeks 11. Safety and tolerability assessments based on adverse events, clinical laboratory values (haematology, serum chemistry, coagulation studies, and urinalysis), standard digital ECGs, ambulatory ECGs, vital signs, and pulse oximetry up to 28 weeks 12. PK parameters of lumacaftor, M28 lumacaftor, ivacaftor, M1 ivacaftor, and M6 ivacaftor at 16 weeks |
|
| Funding source | Sponsored by Vertex Pharmaceuticals Inc. | |
| Notes | Known as TRAFFIC study. The TRAFFIC and TRANSPORT studies were identical with the following exceptions: TRAFFIC included ambulatory ECG screening at days 1 and 15 in approximately 165 participants in the USA; TRANSPORT included additional pharmacokinetics assessments performed in approximately 28 adolescents in the USA. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Participants randomly assigned (in a 1:1:1 ratio) to 1 of 3 study groups; the randomisation was established by an interactive web response system. Randomisation was stratified according to age (< 18 years versus ≥ 18 years), sex, and pulmonary function (% predicted FEV1 (% predicted) at screening, < 70 versus ≥ 70). |
| Allocation concealment (selection bias) | Low risk | The randomisation was established by an interactive web response system. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | These were double‐blind studies in which the participant and study team remained blinded to the treatment assignments. Placebo was matched in appearance and packaging. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | These were double‐blind studies in which the participant and study team remained blinded to the treatment assignments. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Correct number of participants included in the analysis (i.e. those who received at least one dose of the study drug – ITT). Prior to first dose 10 out of 559 participants withdrew: 2 withdrew from treatment arm 1; 5 withdrew from treatment arm 2; 3 withdrew from placebo group. Post first dose 25 out of 549 participants withdrew (with reasons): 11 from treatment arm 1; 10 withdrew from treatment arm 2; 4 withdrew from placebo group. |
| Selective reporting (reporting bias) | High risk | Additional data available on www.clinicaltrials.gov for outcomes not reported in the final paper such as: 1. absolute change in EQ‐5D‐3L score from baseline at week 24; 2. absolute change in TSQM domains from baseline at week 24; 3. time to first exacerbation; 4. event of having at least one pulmonary exacerbation. Some results had to be extrapolated from graphical figures, we await confirmation from the study sponsor of the accuracy of the results. Investigators state that they measured FVC (which was not listed as an end‐point) and do not report this in the joint paper. |
| Other bias | Low risk | Adherence to study treatment was high and the mean compliance rate (determined by site personnel and ongoing study drug count) was similar across lumacaftor‐ivacaftor and placebo groups (99.1% versus 98.5%). |
TRANSPORT 2015.
| Study characteristics | ||
| Methods | Double‐blind, placebo‐controlled Phase 3 RCT.
Parallel design. Multicentre: 82 sites in North America, Australia and Europe. Estimated sample size: 563. Duration: 24 weeks. |
|
| Participants | 559 participants with confirmed diagnosis of CF and with stable disease (as judged by the investigator). Mean age (range): treatment arm 1 24.3 (12 ‐ 48) years; treatment arm 2 25.0 (12 ‐ 54) years; placebo 25.7 (12 ‐ 55) years. Gender: 268 (48%) males; 291 (52%) females. Mutation: homozygous for the F508del mutation. Lung function: FEV1 (% predicted) between ≥ 40% and ≤ 90% of predicted normal for age, sex, and height. |
|
| Interventions |
Intervention 1: 600 mg of lumacaftor 1x daily and 250 mg of ivacaftor every 12 hours for 24 weeks. Intervention 2: 400 mg of lumacaftor every 12 hours and 250 mg of ivacaftor every 12 hours for 24 weeks. Intervention 3: placebo. |
|
| Outcomes |
Primary outcome measure Absolute change in % predicted FEV1 (% predicted) at 24 weeks Secondary outcome measures 1. Relative change in % predicted FEV1 (% predicted) at 24 weeks 2. Absolute change in BMI at 24 weeks 3. Number of pulmonary exacerbations at 24 weeks 4. Absolute change in CFQ‐R respiratory domain score at 24 weeks 5. Absolute change in BMI z score at 24 weeks 6. Absolute change in body weight at 24 weeks 7. Time‐to‐first pulmonary exacerbation at 24 weeks 8. Event of having at least 1 pulmonary exacerbation at week 24 9. Absolute change in EQ 5D 3L at 24 weeks 10. Absolute change in TSQM domains at 24 weeks 11. Safety and tolerability assessments based on adverse events, clinical laboratory values (haematology, serum chemistry, coagulation studies, and urinalysis), standard digital ECGs, ambulatory ECGs, vital signs, and pulse oximetry up to 28 weeks 12. PK parameters of lumacaftor, M28 lumacaftor, ivacaftor, M1 ivacaftor, and M6 ivacaftor at 16 weeks |
|
| Funding source | Sponsored by Vertex Pharmaceuticals Inc. | |
| Notes | Known as TRANSPORT study. The TRAFFIC and TRANSPORT studies were identical with the following exceptions: TRAFFIC included ambulatory ECG screening at days 1 and 15 in approximately 165 participants in the USA; TRANSPORT included additional pharmacokinetics assessments performed in approximately 28 adolescents in the USA. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Participants randomly assigned (in a 1:1:1 ratio) to 1 of 3 study groups; the randomisation was established by an interactive web response system. Randomisation was stratified according to age (< 18 years versus ≥ 18 years), sex, and pulmonary function (% predicted FEV1 (% predicted) at screening, < 70 versus ≥ 70). |
| Allocation concealment (selection bias) | Low risk | The randomisation was established by an interactive web response system. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | These were double‐blind studies in which the participant and study team remained blinded to the treatment assignments. Placebo was matched in appearance and packaging. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | These were double‐blind studies in which the participant and study team remained blinded to the treatment assignments. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Correct number of participants included in the analysis (i.e. those who received at least one dose of the study drug – ITT). Prior to first dose 4 out of 563 participants withdrew: 2 withdrew from treatment arm 1; 2 withdrew from treatment arm 2; none withdrew from placebo group. Post first dose 29 out of 559 participants withdrew (with reasons): 9 from treatment arm 1; 15 withdrew from treatment arm 2; 5 withdrew from placebo group. |
| Selective reporting (reporting bias) | High risk | Additional data available on www.clinicaltrials.gov for outcomes not reported in the final paper such as: 1. absolute change in EQ‐5D‐3L score from baseline at week 24; 2. absolute change in TSQM domains from baseline at week 24; 3.. time to first exacerbation; 4. event of having at least 1 pulmonary exacerbation. Some results had to be extrapolated from graphical figures, we await confirmation from the study sponsor of the accuracy of the results. Investigators state that they measured FVC (which was not listed as an end‐point) and do not report this in the joint paper. |
| Other bias | Low risk | Adherence to study treatment was high and the mean compliance rate (determined by site personnel and ongoing study drug count) was similar across lumacaftor‐ivacaftor and placebo groups (99.1% versus 98.5%). |
Zeitlin 2002.
| Study characteristics | ||
| Methods | Phase 1/2 placebo‐controlled RCT. Parallel design. Single centre. Duration: 1 week. This study follows on from a pilot study (see above) (Rubenstein 1998). |
|
| Participants | 19 participants were supposed to be randomised in a 3:1 ratio to either study drug or placebo. Randomisation to 40 g group discontinued due to safety reasons; therefore 6 participants were allocated to the 20 g and 30 g groups, 3 to the 40 g group and 4 to the placebo group. It is unclear why only 4 participants were randomised to the placebo group. Mutation: all participants were homozygous for the F508del mutation. Age: mean (SD) age of 28.5 years. Gender split: 12 males and 7 females. Lung function: mean (SD) FEV1 % predicted of 63.7 (17.0). Nutritional status: mean (SD) weight 62.6 (17.0) kg. |
|
| Interventions |
Intervention 1: placebo. Intervention 2: 4‐phenylbutyrate (4PBA) 20 g. Intervention 3: 4‐phenylbutyrate (4PBA) 30 g. Intervention 4: 4‐phenylbutyrate (4PBA) 40 g. All active interventions split into 3 daily doses. |
|
| Outcomes | 1. Nasal epithelial chloride transport measured by nasal potential difference 2. Adverse events* 3. Absolute values in sweat chloride concentrations 4. Hepatic enzyme profile 5. Uric acid levels 6. Change from baseline in pulmonary function (% predicted FEV1 (% predicted)) 7. Semi‐quantitative scoring of sputum microbiology |
|
| Funding source | Cystic Fibrosis Foundation. | |
| Notes | * denotes outcomes relevant to this review. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Stated as randomised but it is not clear how this was conducted. |
| Allocation concealment (selection bias) | Unclear risk | Not described. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Escalation to the next dose level was preceded by an examination of the safety profile of the preceding dose. Therefore, study personnel would have been aware of treatment allocation. Also between the 3 intervention groups, participants received a different number of tablets and had different dosage schedules:
Therefore it is unlikely that study personnel blinding and participant blinding was maintained throughout the study. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | There was insufficient information on how outcome assessor blind was maintained. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | All 19 participants completed the final study visit, but it is unclear how many participants were used in the analysis. |
| Selective reporting (reporting bias) | High risk | Protocol not available. Pulmonary function or microbiology scores at day 7 not reported. |
| Other bias | Low risk | "There were no significant differences in gender, baseline age, weight, or FEV1 (% predicted) among participants in the four groups." |
AE: adverse event BMI: body mass index CF: cystic fibrosis CFQ‐R: Cystic Fibrosis Questionnaire‐Revised CFRSD: Cystic Fibrosis Respiratory Symptom Diary CPX: 8‐cyclopentyl‐1, 3‐dipropylxanthine ECG: electrocardiograms EQ 5D 3L: EuroQol 3 Level FEF25-75%: forced expiratory flow FEV1: forced expiratory volume in one second FVC: forced vital capacity IRT: immunoreactive trypsinogen ITT: intention to treat IV: intravenous LCI: lung clearance index mEq/L: millequivalents/L MF: minimal function MMRM: mixed effects model for repeated measurements NIH: National Institutes of Health PK: pharmacokinetic PSQI: Pittsburgh Sleep Quality Index QoL: quality of life RCT: randomised controlled trial SAE: serious adverse event TSQM: Treatment Satisfaction Questionnaire for Medication
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Berkers 2014 | Cross‐over study with participants with gating defects and not a class II variant. |
| Chadwick 1998 | Investigators informed review authors that study was not randomised. |
| Chilvers 2017 | Participants not randomised, single‐group assignment. |
| Drevinek 2017 | QR‐010 is an anti‐sense oligonucleotide, which we did not consider to be a corrector. |
| Leonard 2012 | Cross‐over design. |
| NCT00945347 | Cross‐over design. |
| NCT01899105 | Cross‐over design. |
| NCT03447262 | Participants not randomised, single‐group assignment, no masking, open‐label. |
| NCT03525574 | Participants not randomised, single‐group assignment, no masking, open‐label. |
| NCT03537651 | Participants not randomised, single‐group assignment, no masking, open‐label. |
| NCT03601637 | Participants not randomised, single‐group assignment, no masking, open‐label. |
| NCT03633526 | Participants not randomised, single‐group assignment, no masking, open‐label. |
| NCT03691779 | Participants not randomised, single‐group assignment, no masking, open‐label. |
| NCT04043806 | Participants not randomised, single‐group assignment, no masking, open‐label. |
| NCT04058366 | Participants not randomised, single‐group assignment, no masking, open‐label. |
| NCT04105972 | Participants not randomised, sequential assignment, no masking. |
| NCT04183790 | Participants not randomised, single‐group assignment, no masking, open‐label. |
| NCT04235140 | Participants not randomised, single‐group assignment, no masking, open‐label. |
| NCT04362761 | Participants not randomised, single‐group assignment, no masking, open‐label. |
| NCT04537793 | Participants not randomised, sequential assignment, no masking, open‐label. |
| NCT04545515 | Participants not randomised, single‐group assignment, no masking, open‐label. |
| Nick 2014 | Cross‐over study assessing CFTR mutations eligible for treatment with ivacaftor (not relevant to this review). |
| Rowe 2017 | Cross‐over design. |
| Rubenstein 2006 | Participants were not randomised. |
| Sumner 2014 | Gene therapy study, not a mutation‐specific therapy. |
| Ziady 2015 | Laboratory study conducted within cells donated by CF and non‐CF donors. Not a study of people with CF. |
CF: cystic fibrosis CFTR: cystic fibrosis transmembrane conductance regulator
Characteristics of studies awaiting classification [ordered by study ID]
Downey 2019.
| Methods | RCT, double‐blind and placebo‐controlled. Parallel design, 3 arms. Duration: 14 days |
| Participants | Adults (over 18 years of age) with CF homozygous for F508del and with FEV1 40% to 90% predicted. |
| Interventions | Intervention 1: dual therapy of PTI‐801 + PTI‐808. Intervention 2: triple therapy of PTI‐801 + PTI‐808 + PTI‐428. Intervention 3: placebo. |
| Outcomes | Safety/tolerability, pharmacokinetics, change in FEV1, change in sweat chloride. |
| Notes | Further details (full paper) not yet available. |
EudraCT 2019‐000750‐63.
| Methods | RCT, double‐blind and placebo‐controlled. Parallel design, 3 arms. Duration: 29 days. |
| Participants | Adults (over 18 years of age) with CF, homozygous for F508del. |
| Interventions | Intervention 1: ABBV‐3067. Intervention 2: ABBV‐3067 plus ABBV‐2222. Intervention 3: placebo. |
| Outcomes | Change from baseline in spirometry and lung function, change from baseline in sweat chloride. |
| Notes | A Phase 2 Study of ABBV‐3067 Alone and in Combination with ABBV‐2222 in Cystic Fibrosis Subjects Who Are Homozygous for the F508del Mutation |
Hunt 2017.
| Methods | RCT, placebo‐controlled (randomised 2:1 to sildenafil or placebo). Parallel design. Duration: 4 weeks. |
| Participants | 18 adults homozygous for F508del. Age, mean (SD): 28.7 (6.6) years. Gender: 7/18 males (35%), 11/18 females (65%). FEV1 % predicted, mean (SD): 82.5% (12.9). BMI, mean (SD): 23.2 kg/m² (6.6). |
| Interventions |
Intervention: oral sildenafil 40 mg 3x daily. Control: matching placebo. All participants also on standard of care and lumacaftor/ivacaftor. |
| Outcomes | CFQ‐R, nasal potential difference, LCI, exhaled nitric oxide, spirometry (FEV1 % predicted), BMI and routine laboratory tests measured at baseline. |
| Notes |
Munck 2020.
| Methods | RCT, double‐blind, placebo‐controlled. Duration: 12 weeks. Parallel design. |
| Participants | 168 participants aged over 12 years of age with CF with genotype F508del/MF. |
| Interventions | Intervention 1: tezacaftor‐ivacaftor. Intervention 2: placebo. |
| Outcomes | Absolute change from baseline in FEV1 % predicted, change from baseline in CFQ‐R respiratory domain, number of pulmonary exacerbations, absolute change in BMI. |
| Notes |
NCT02951195.
| Methods | RCT, double‐blind, placebo and active‐controlled. Phase 2. Parallel design. Duration: 15 days treatment (up to 8 weeks for safety follow‐up). Location: multicentre in the USA. |
| Participants | 80 adults with CF enrolled. Inclusion criteria Body weight ≥ 35 kg. Sweat chloride value ≥ 60 mmol/L from test results obtained during screening. CFTR genotype: Cohorts 1A, 1B, 1C are F508del/MF (mutation known or predicted not to respond to tezacaftor and/or ivacaftor); Cohorts 2A, 2B are homozygous for F508del. FEV1 ≥ 40% and ≤ 90% of predicted normal for age, sex, and height at the screening visit. Stable CF disease as judged by the investigator. |
| Interventions |
Initial cohort Intervention: VX‐152 100 mg administered every 12 hours, tezacaftor 100 mg 1x daily, ivacaftor 150 mg every 12 hours. Control: triple placebo (i.e. no active VX‐152, tezacaftor, or ivacaftor). In subsequent cohorts, investigators administered the same combination of drugs with different doses of VX‐152, adjusted as the study progresses. |
| Outcomes |
Primary outcome AEs and serious AEs (up to 8 weeks) Secondary outcomes Absolute change in sweat chloride concentrations (from baseline to day 15) Absolute change in % predicted FEV1 (from baseline to day 15) Relative change in % predicted FEV1 (from baseline to day 15) Absolute change in CFQ‐R respiratory domain score (from baseline to day 15) Pharmacokinetic and pharmacodynamic parameters |
| Notes | Entry on ClinicalTrials.gov states that trial completed, but no results have been posted. Sponsored by Vertex Pharmaceuticals Inc. |
NCT03447249.
| Methods | RCT, double‐blind, placebo‐controlled. Parallel design. Duration: 24 weeks |
| Participants | 385 participants (aged 12 years and older) with CF and the genotype F508del/MF and FEV1 40% ‐ 90% predicted. |
| Interventions | Intervention 1: VX‐659 240 mg/tezacaftor 100 mg/ivacaftor 150 mg as fixed‐dose combination tablets in the morning and ivacaftor 150 mg as mono tablet in the evening. Intervention 2: matched placebo morning and evening. |
| Outcomes | Absolute change in FEV1 % predicted, number of pulmonary exacerbations, absolute change in sweat chloride, absolute change in CFQ‐R respiratory domain, absolute change in BMI, absolute change in body weight, safety and tolerability (AEs), observed pre‐dose concentration of VX‐659, TEZ, M1‐TEZ, and IVA |
| Notes |
NCT03460990.
| Methods | RCT, double‐blind, placebo‐controlled. Parallel design. Duration: 8 weeks. |
| Participants | 116 participants (aged 12 years and older) with CF and homozygous for F508del and FEV1 40% ‐ 90% predicted. |
| Interventions | Run‐in period of 4 weeks with tezacaftor/ivacaftor, then: Intervention 1: VX‐659 240 mg/tezacaftor 100 mg/ivacaftor 150 mg as fixed‐dose combination tablets in the morning and ivacaftor 150 mg as mono tablet in the evening. Intervention 2: placebo/tezacaftor 100 mg/ivacaftor 150 mg as fixed‐dose combination tablets in the morning and ivacaftor 150 mg as mono tablet in the evening. |
| Outcomes | Absolute change in FEV1 % predcited, absolute change in sweat chloride, absolute change in CFQ‐R respiratory domain, safety and tolerability (AEs), observed pre‐dose concentration of VX‐659, tezacaftor, M1‐TEZ, and ivacaftor. |
| Notes | A Study of VX‐659 Combination Therapy in CF Subjects Homozygous for F508del (F/F) |
NCT03768089.
| Methods | RCT, double‐blind, placebo‐controlled. sequential assignment/escalating dose |
| Participants | 114 adults (aged 18 years and over) ‐ both healthy adults without CF and BMI 18 ‐ 32 and weight over 50 kg and people with CF with F508del/MF genotype and FEV1 40% ‐ 90% predicted and weight over 35 kg. Only CF participants eligible for inclusion in review. |
| Interventions | Intervention 1: VX‐121 tablet plus 100 mg tezacaftor/150‐mg ivacaftor fixed‐dose combination tablet and ivacaftor 150 mg film‐coated tablet. Intervention 2: triple placebo. |
| Outcomes | Safety and tolerability (AEs), pharmacokinetics, absolute change in sweat chloride, absolute change in FEV1 % predicted. |
| Notes | A Phase 1/2 Study of VX‐121 in Healthy Subjects and in Subjects With Cystic Fibrosis |
NCT03911713.
| Methods | RCT, double‐blind and placebo‐controlled. Parallel design. Duration: 16 weeks. |
| Participants | 77 adults with CF with at least one copy of G551D, G178R, S549N, S549R, G551S, G1244E, S1251N, S1255P, or G1349D, already on ivacaftor. |
| Interventions | Intervention 1: 1 of 4 dose levels of VX‐561 plus placebo. Intervention 2: ivacaftor 150‐mg film‐coated tablet plus placebo. |
| Outcomes | Absolute change in FEV1 % predicted, absolute change in sweat chloride, pharmacokinetics, safety and tolerability (AEs). |
| Notes | A Phase 2 Study to Evaluate Efficacy and Safety of VX‐561 in Subjects Aged 18 Years and Older With Cystic Fibrosis. Unclear as to wheter this will include participants F508del‐ await to see if appropriate for inclusion in this review. |
NCT03912233.
| Methods | RCT, double‐blind, placebo‐controlled. Parallel design. Sequential assignment. Duration: 75 days. |
| Participants | 87 adults (aged 18 years and over) with CF either homozygous for F508del or with genotype F508del/MF and FEV1 40% ‐ 90% predicted. |
| Interventions |
F508del/MF group Intervention 1: VX‐121‐tezacaftor‐VX‐561. Intervention 2: matched placebo. F508del/F508del group Intervention 1: VX‐121‐ tezacaftor‐VX‐561. Intervention 2: placebo‐tezacaftor‐VX‐561. |
| Outcomes | Safety and tolerability (AEs), absolute change in FEV1 % predicted, absolute change in sweat chloride concentrations, absolute change in CFQ‐R respiratory domain, maximum observed concentration of VX‐121, tezacaftor, VX‐561, ivacaftor, and relevant metabolites, area under the concentration versus time curve during a dosing interval of VX‐121, tezacaftor, VX‐561, ivacaftor, and relevant metabolites, observed pre‐dose concentration of VX‐121, tezacaftor, VX‐561, ivacaftor, and relevant metabolites. |
| Notes |
NCT04058353.
| Methods | RCT, double‐blind, active controlled trial. Parallel design. Duration: 12 weeks. |
| Participants | 271 participants (aged 12 years and older) with CF and the F508del/gating variant or F508del/residual function and FEV1 40% ‐ 90% predicted. |
| Interventions | Intervention 1: elexacaftor/tezacaftor/ivacaftor combined tablet in the morning and ivacaftor as mono tablet in the evening. Intervention 2: ivacaftor as mono tablet OR tezacaftor/ivacaftor combined tablet in the morning and ivacaftor as mono tablet in the evening. |
| Outcomes | Absolute change in FEV1 % predicted, absolute change in sweat chloride, absolute change in CFQ‐R respiratory domain, safety and tolerability (AEs) |
| Notes | A Phase 3 Study of VX‐445 Combination Therapy in Cystic Fibrosis Subjects Heterozygous for F508del and a Gating or Residual Function Mutation (F/G and F/RF Genotypes) |
NCT04353817.
| Methods | RCT, placebo‐controlled, double‐blind. Parallel design. Duration: 24 weeks (safety 28 weeks). |
| Participants | 108 children (aged 6 ‐ 11 years) with CF and genotype F508del/MF with FEV1 over 70 % predicted. |
| Interventions | Intervention 1: elexacaftor/tezacaftor/ivacaftor combined tablet in the morning and ivacaftor as mono tablet in the evening. Intervention 2: triple matched placebo in the morning and matched placebo in the evening. |
| Outcomes | Absolute change in LCI 2.5, absolute change in sweat chloride, safety and tolerability (AEs). |
| Notes | A Study Evaluating Efficacy and Safety of Elexacaftor/Tezacaftor/Ivacaftor in Subjects 6 Through 11 Years of Age With Cystic Fibrosis and F/MF Genotypes |
PELICAN.
| Methods | RCT, double‐blind, placebo‐controlled. Parallel design. Duration: 28 days |
| Participants | 22 adults (aged 18 and over) with CF, homozygous for F508del, who had previously been taking lumacaftor‐ivacaftor for at least 12 weeks before start of trial, FEV1 at least 40% predicted, sweat chloride at least 60 mmol/L. |
| Interventions | Intervention 1: GLPG‐2737 plus lumacaftor‐ivacaftor twice daily. Intervention 2: placebo plus lumacaftor‐ivacaftor twice daily. |
| Outcomes | Change from baseline in sweat chloride concentration, AEs, change in FEV1 % predicted, change in CFQ‐R respiratory domain, maximum observed plasma concentration of GLPG2737, area under the plasma concentration‐time curve from time zero until 8 hours post‐dose calculated by the linear up ‐ logarithmic down trapezoidal rule, trough plasma concentration observed at the end of the dosing interval. |
| Notes |
Rio‐CF.
| Methods | RCT, placebo‐controlled, quadruple‐blinded. Randomised 2:1 (intervention n = 14, placebo n = 7). Phase 2. Parallel design. Mulitcentre: USA, Canada, Europe. Duration: 28 days. |
| Participants | 21 adults with CF, homozygous for F508del, FEV1 % predicted 40% ‐ 100%. Age, mean (SD): total cohort 27.8 (6.9) years; intervention 27.1 (6.9) years; placebo 29.1 (7.2) years. Gender split: total cohort 16 males (76.2%); intervention 10 males (71.4%); placebo 6 males (85.7%). Sweat chloride mean (SD): total cohort (n = 16) 95.53 (15.03) mmol/L; intervention (n = 9) 96.33 (17.28) mmol/L; placebo (n = 7) 94.50 (12.82) mmol/L. |
| Interventions |
Intervention: riociguat 0.5 mg 3x daily for 14 days, then 1.0 mg 3 x daily for the next 14 days. Control: matched placebo 3x daily. |
| Outcomes |
Primary outcome 1. Sweat chloride concentration 2. Nasal potential difference Secondary outcomes 1. FEV1 % predicted 2. LCI 3. Adverse events Outcomes measured at baseline, day 14 and day 28. |
| Notes | Author of the study was contacted and stated that further detail is awaited in a published manuscript. However, we note from clinicaltrials.gov that part 2 of this study has been terminated after no longer being deemed appropriate. |
Taylor‐Cousar 2019.
| Methods | RCT, double‐blind, placebo‐controlled. Parallel design. Escalating dose. Duration: 28 days. |
| Participants | 40 adults (aged 18 years and older) with CF, FEV1 40% ‐ 90% predicted. Participants had previously been taking tezacaftor/ivacaftor. |
| Interventions | Intervention 1: two different doses of PTI‐428 (doses not stated) plus tezacaftor/ivacaftor. Intervention 2: placebo plus tezacaftor/ivacaftor. |
| Outcomes | Safety and tolerability (AEs), pharmacodynamics (expression of CFTR in nasal mucosa), changes in pulmonary function. |
| Notes |
Wainwright 2019.
| Methods | RCT, double‐blind, placebo‐controlled. Parallel design. Duration: 72 weeks |
| Participants | Participants (aged 12 years and older) with CF homozygous for F508del and FEV1 at least 70% predicted. |
| Interventions | Intervention 1: tezacaftor/ivacaftor. Intervention 2: placebo. |
| Outcomes | Absolute change from baseline in total CF‐CT score, safety, changes in CF‐CT subscores, absolute change in FEV1 % predicted. |
| Notes |
AE: adverse event BMI: body mass index CF: cystic fibrosis CT: computer tomography CFQ‐R: cystic fibrosis questionnaire ‐ revised FEV1: forced expiratory volume in one second LCI: lung clearance index MF: minimal function RCT: randomised controlled trial SD: standard deviation
Characteristics of ongoing studies [ordered by study ID]
ALBATROSS.
| Study name | GLPG2222 in subjects with cystic fibrosis and the F508del/class III mutation on stable treatment with ivacaftor: results from a Phase II study (ALBATROSS) |
| Methods | Phase IIa double‐blind, placebo‐controlled RCT. Multicentre in Australia and Europe. Duration: 4 weeks. |
| Participants | The Phase 2a study included 37 participants on stable ivacaftor treatment for at least the past 4 weeks (during the study they also continued to take ivacaftor). Age: 18 years or older. Genotype: F508del/class III mutation. Disease status: baseline FEV1 % predicted 40% or greater. |
| Interventions | Intervention 1: GLPG2222 150 mg orally for 4 weeks. Intervention 2: GLPG2222 300 mg orally for 4 weeks. Control: placebo. All participants were already on stable ivacaftor treatment for at least 4 weeks prior to this trial and continued taking their ivacaftor throughout this study period. 30 participants took one of the GLPG2222 doses and 7 participants took placebo. |
| Outcomes | Primary outcomes
Secondary outcomes
Initial abstracts report AEs, pharmacokinetic and pharmacodynamic data, sweat chloride change and absolute change in FEV1 % predicted. |
| Starting date | January 2017. |
| Contact information | Study director: Olivier Van Steen, MD, MBA, Galapagos NV. |
| Notes | Clinicaltrials.gov: NCT03045523 |
FLAMINGO.
| Study name | A Study to Evaluate Multiple Doses of GLPG2222 in Adult Subjects With Cystic Fibrosis (FLAMINGO) |
| Methods | Phase 2, double‐blind, placebo‐controlled RCT. Duration: 29 days. Location: multicentre in North America and Europe. |
| Participants | 59 adults diagnosed with CF randomised (11 in placebo group). Not on concomitant CFTR modulator therapy within 4 weeks of study start. Aged: 18 years and over. Genotype: F508del/F508del genotype. Disease status: FEV1 40% predicted or greater. |
| Interventions | GLPG2222 once daily dose of either (50, 100, 200 or 400 mg) 4 different doses taken once daily were tested (50, 100, 200, 400 mg) for 4 weeks. Cohort A GLPG2222 50 mg tablet and 2x matching placebo tablets orally, 4x daily for 29 days. GLPG2222 100 mg tablet and 2x matching placebo tablets orally, 4x daily for 29 days. Cohort B GLPG2222 2x 100 mg tablets and 1x matching placebo tablet orally, 4x daily for 29 days. GLPG2222 2x 150 mg tablets and GLPG2222 1x 100 mg tablet orally, 4x daily for 29 days. |
| Outcomes |
Primary outcome measure Treatment‐emergent AEs (any treatment‐emergent AE and serious or treatment‐related AE, treatment‐emergent AE by worst intensity reported (mild, moderate, or severe)) Secondary outcome measures Sweat chloride concentration (mean change from baseline at Day 29) FEV1 % predicted (mean change from baseline at Day 29) CFQ‐R respiratory domain (mean change from baseline at Day 29) Mean maximum observed plasma concentration (Cmax) (mg/mL) of GLPG2222 Mean GLPG2222 plasma concentration observed at predose (Ctrough) (ng/mL) Median time to occurrence of GLPG2222 Cmax (Tmax; hours) Mean AUC from baseline up to 24 hours following multiple dosing (AUC[0‐t]; ng.h/mL) of GLPG2222 AEs, sweat chloride concentration, ppFEV1, pharmacokinetics. |
| Starting date | 18 March 2017. |
| Contact information | Actual primary completion date: 19 October 2017. Actual study completion date: 19 October 2017. |
| Notes |
Jain 2018.
| Study name | A Phase 1 / 2, double‐blind, placebo‐controlled RCT designed to evaluate the safety, tolerability, and pharmacokinetics of PTI‐808, PTI‐801, and PTI‐428 combination therapy in people with CF. Initial result evaluating third generation CFTR corrector PTI‐801 in people with CF. |
| Methods | Phase 1 double‐blind RCT testing ascending doses of PTI‐801. Multicentre in UK. Duration: 14 days of treatment with follow‐up visit at 21 days. Phase 1 randomised, double blind, placebo controlled. Testing multiple ascending doses of PTI‐801 |
| Participants | Estimated enrolment 32 participants with CF diagnosed clinically and by genetic testing. Age: 18 years and older. Genotype: for cohorts 1, 2 and 4 F508del/F508del; for cohort 3 at least one copy of F508del. Disease status: baseline FEV1 40% ‐90%. CF diagnosis, age 18 years or older with FEV1 40‐90% predicted. Particpants were all currently receiving lumacaftor/ivacaftor as background therapy. |
| Interventions | Cohort 1: once daily PTI‐808 with PTI‐801 versus once daily PTI‐808 plus placebo for 14 days. Cohort 2: once daily PTI‐808 with PTI‐801 versus once daily PTI‐808 plus placebo for 14 days. Cohort 3: once daily PTI‐808 with PTI‐801 and PTI‐428 versus once daily placebos for 14 days. Cohort 4: once daily PTI‐808 with PTI‐801 and PTI‐428 versus placebos once daily for 7 days immediately followed by PTI‐808 with PTI‐801 versus placebos for 7 days. Multiple ascending doses of PTI‐801 versus placebo. Initial abstract does not provide detail on the actual doses, frequency, route of administration or details of placebo. |
| Outcomes |
Primary outcome 1. Safety (AEs and potentially significant clinical laboratory assessments, electrocardiography, physical examinations, vital signs) Secondary outcomes 1. Terminal half‐life (t1/2) of multiple oral doses of PTI‐808 + PTI‐801 and PTI‐428 (cohorts 3 & 4 only) 2. Time to reach maximum plasma concentration (Tmax) of multiple oral doses of PTI‐808 + PTI‐801 and PTI‐428 (cohorts 3 & 4 only) 3. Plasma Cmax of multiple oral doses of PTI‐808 + PTI‐801 and PTI‐428 (cohorts 3 & 4 only) 4. Change in FEV1 over time Other outcomes 1. Change in sweat chloride 2. Change in weight 3. Change in BMI 4. Change in CFQ‐R respiratory domain 5. Change in nasal epithelial mRNA expression 6. Change in nasal protein expression Safety and tolerability, pharmacokinetics, change in lung function, change in sweat chloride |
| Starting date | January 2018. |
| Contact information | Proteostasis Therapeutics Inc. |
| Notes | Estimated primary completion date: April 2019. Estimated study completion date: May 2019. |
Meijer 2016.
| Study name | Evaluation of (R)‐Roscovitine Safety and Effects in Subjects With Cystic Fibrosis, Homozygous for the F508del‐CFTR Mutation (ROSCO‐CF) |
| Methods | Phase 2, dose‐ranging, double‐blind, placebo‐controlled RCT. Duration: 3 months. Multicentre RCT conducted in France. |
| Participants | 36 adults with CF carrying 2 CF‐causing mutations with at least 1 F508del‐CFTR mutation and chronically infected with P aeruginosa. |
| Interventions | Intervention: roscovitine 200 mg or 400 mg. Control: placebo. |
| Outcomes |
Primary outcome measure Safety of increasing doses of roscovitine Secondary outcome measures Change in the concentration of P aeruginosa Change in the concentration (CFU/mL) of P aeruginosa in the sputum at each visit from V1 (screening) up to V7 (completion visit) PK parameters: Cmax, time to reach Cmax, AUC (AUCt and AUCInf), half‐life (t1/2) for roscovitine and its M3 metabolite Pro‐ and anti‐inflammatory cytokines Change in C‐reactive protein at each visit from V1 (screening) up to V7 (completion) Change in CFQ‐R at each visit from V1 up to V8 (safety follow‐up) Change in BMI at each visit from V1 (screening) up to V7 (completion visit) Change in FEV1 at each visit from V1 (screening) up to V7 (completion visit) Change in sweat chloride concentration at V2, V3, V5 and V7 (Completion) Change in nasal potential difference at V1 (screening) and V6 (for participants included in Paris Cochin CF Center) Pain questionnaire |
| Starting date | February 2016. |
| Contact information | Principle investigator: Dr Gilles Rault (gilles.rault@perharidy.fr). |
| Notes | Estimated study completion date: October 2017. Estimated primary completion date: August 2017 (Final data collection date for primary outcome measure). |
NCT02070744.
| Study name | Study to Evaluate Safety and Efficacy of VX‐661 in Combination With Ivacaftor in Subjects With Cystic Fibrosis, Homozygous for the F508del‐CFTR Mutation |
| Methods | Double‐blind, placebo‐controlled, 3‐part Phase 2 RCT. Parallel design. Multicentre: 20 sites. Sample size: expected to enrol 40 participants. Duration: 12 weeks of treatment. |
| Participants | Age: 18 years or older. Gender: both male and female. Mutation: homozygous for the F508del mutation. Lung function: FEV1 ≥ 40% and ≤ 90% of predicted normal for age, sex, and height. Participants must have stable CF disease as judged by the investigator. |
| Interventions |
Group 1 Treatment: VX‐661 + ivacaftor (every 12 hours schedule). Control: VX‐661 placebo + ivacaftor placebo (every 12 hours schedule). Group 2 Treatment: VX‐661 + ivacaftor (once daily and schedule). Control: VX‐661 placebo + ivacaftor placebo (once daily and schedule). |
| Outcomes |
Primary outcome measure 1. Safety as determined by AEs, physical examination, clinical laboratory values, standard digital ECGs, vital signs and pulse oximetry at 16 weeks Secondary outcome measures 1. Absolute change in % predicted FEV1 at 12 weeks 2. Relative change in % predicted FEV1 at 12 weeks 3. Absolute change in body weight at 12 weeks 4. Absolute change in BMI at 12 weeks 5. Absolute change in the respiratory domain of the CFQ‐R at 12 weeks 6. PK parameters estimates of VX‐661 and ivacaftor and their respective metabolites, derived from plasma concentration‐time data at 16 weeks 7. Absolute change in sweat chloride at 12 weeks |
| Starting date | March 2014. |
| Contact information | No contact information provided. |
| Notes | This study is listed as completed but no results are available on www.clinicaltrials.gov. Sponsored by Vertex Pharmaceuticals Inc. |
NCT02323100.
| Study name | Glycerol Phenylbutyrate Corrector Therapy For CF (Cystic Fibrosis) (GPBA) |
| Methods | Double‐blind, placebo‐controlled, 3‐part Phase 2 RCT. Parallel design. Multicentre: 3 sites. Sample size: expected to enrol 36 participants. Duration: 7 days of treatment. |
| Participants |
Inclusion criteria Age: 18 years or over. Gender: male or female . Mutation: homozygous for F508del, and taking pancreatic enzyme replacement therapy. Lung function: FEV1 > 30% of predicted normal for age, gender, and height (Hankinson standards). |
| Interventions |
Arm 1: low‐dose glycerol phenylbutyrate (Ravicti®) oral liquid at 6 mL (6.6 g) by mouth or gastrostomy tube at 8 am, 5.5 mL (6.05 g) at 4 pm and midnight for 7 days. Arm 2: high‐dose glycerol phenylbutyrate (Ravicti®) oral liquid at 9 mL (9.9 g) at 8 am and 8.25 mL (9.08 g) at 4pm and midnight for 7 days. Arm 3: matching placebo. |
| Outcomes |
Primary outcome Change in average measurement of nasal potential difference between day 7 and baseline (at 7 days) Secondary outcomes Change from baseline in other nasal potential difference measures (baseline potential difference, change in amiloride, low chloride, and low chloride plus isoproterenol) (at 4 days, 7 days and 14 days) Change from baseline in sodium and chloride transport Change from baseline in average sweat chloride measurement (at 4 days, 7 days and 14 days) Change from baseline in sweat chloride Safety and tolerability (standard safety and tolerability lab values) (at 14 days) |
| Starting date | December 2017. |
| Contact information | Britany Zeglin (bzeglin1@jhmi.edu). |
| Notes |
NCT02412111.
| Study name | A Phase 3 study of VX‐661 in Combination With Ivacaftor in Subjects Aged 12 Years and Older With Cystic Fibrosis, Who Have One F508del‐CFTR Mutation and a Second Mutation That Has Been Demonstrated to be Clinically Responsive to Ivacaftor |
| Methods | Double‐blind, placebo‐controlled Phase 2 RCT. Parallel design. Multicentre: 68 centres. Sample size: expected to enrol 156 participants. Duration: unclear duration of treatment. |
| Participants | Age: 12 years and older. Mutation: heterozygous for F508del‐CFTR mutation and a second CFTR allele with a gating defect that is clinically demonstrated to be ivacaftor responsive Lung function: FEV1 ≥ 40% and ≤ 90% of predicted. |
| Interventions |
GROUP 1: morning VX‐661 100 mg/ivacaftor 150 mg fixed‐dose tablet with ivacaftor matching placebo tablet; evening ivacaftor 150 mg tablet. GROUP 2: morning VX‐661/ivacaftor matching placebo tablet plus ivacaftor 150 mg tablet; evening ivacaftor 150 mg tablet. |
| Outcomes |
Primary outcome Absolute change in % predicted FEV1 (from baseline through week 8) Secondary outcomes Relative change in % predicted FEV1 (from baseline through week 8) Absolute change in sweat chloride (from baseline through week 8) Absolute change in CFQ‐R respiratory domain score (from baseline through week 8) Number of participants with AEs and serious AEs (up to 4 weeks after receiving last dose) PK parameters of VX‐661, M1‐661, ivacaftor, and M1‐ivacaftor |
| Starting date | June 2015. |
| Contact information | Sponsored by Vertex Pharmaceuticals ‐ no contact details given. |
| Notes | This study is evaluating VX‐661 in combination with ivacaftor versus placebo with ivacaftor. |
NCT02589236.
| Study name | Study of Cavosonstat (N91115) in Patients With CF Homozygous for the F508del‐CFTR Mutation (SNO‐6) |
| Methods | Double‐blind, placebo‐controlled, parallel RCT. |
| Participants | Participants must have been treated with lumacaftor‐ivacaftor for at least 8 weeks prior to day 1. Age: 18 years and older. FEV1: 40% ‐ 85% predicted. |
| Interventions | Group 1: lumacaftor‐ivacaftor‐cavosonstat 200 mg 2x daily. Group 2: lumacaftor‐ivacaftor‐cavosonstat 400 mg 2x daily. Group 3: lumacaftor‐ivacaftor‐matched placebo. |
| Outcomes |
Primary outcome Absolute change in FEV1 % predicted (from baseline to 12 weeks) Secondary outcomes Relative change in FEV1 % predicted (from baseline to 12 weeks) Absolute change in sweat chloride (from baseline to 12 weeks) Absolute change in CFQ‐R (respiratory symptom scale) (from baseline to 16 weeks) Absolute change in BMI (from baseline to 12 weeks) Absolute change in Patient Global Impression of Change (patient‐reported outcome journal) (from baseline to 12 weeks) Incidence of treatment‐emergent AEs (including clinical laboratory values, ECG, pulmonary exacerbations, or vital sign changes) (from baseline to 16 weeks) Number of pulmonary exacerbations (up to 12 weeks) |
| Starting date | November 2015. |
| Contact information | Principal Investigator: Scott Donaldson, MD, University of North Carolina, Chapel Hill. Sponsors and collaborators: Nivalis Therapeutics, Inc. and Medidata Solutions. |
| Notes |
NCT02718495.
| Study name | Study Assessing PTI‐428 Safety, Tolerability, and Pharmacokinetics in Subjects With Cystic Fibrosis |
| Methods | Quadruple‐blind, placebo‐controlled, 3‐arm Phase 2 RCT. Parallel design. Multicentre: 29 centres in North America and Europe. Sample size: expected to enrol 56 participants. Duration: 28 days of treatment. |
| Participants | Age: 18 years and older.
Mutation: not specified. Lung function: FEV1 40% ‐ 90% predicted. |
| Interventions | PTI‐428 versus placebo. Part A has 2 groups: the 1st group will enrol adults with CF into a single ascending‐dose treatment group; the 2nd group will enrol adults with CF, including those on background treatment with ORKAMBI® and those not on a CFTR modulator into a multiple‐ascending dose treatment group. Part B will enrol adults with CF currently on stable ORKAMBI® background therapy for a minimum of 3 months into a Phase 2 treatment group consisting of 2 cohorts. Part C will enrol adults with CF, including those on background treatment with KALYDECO® and those not on a CFTR modulator, into a Phase 2 treatment group consisting of 3 cohorts. |
| Outcomes |
Primary outcome Safety and tolerability as assessed by AEs, pulmonary function tests, safety labs (haematology, chemistry, and urinalysis, ECGs, physical examinations, and vital signs) Secondary outcomes PK and pharmacodynamic parameters Change in FEV1 Change in sweat chloride Change in weight Change in CFQ‐R Change in nasal epithelial CFTR mRNA and protein expression |
| Starting date | November 2017. |
| Contact information | Proteostasis Therapeutics, Inc. |
| Notes |
NCT02730208.
| Study name | A Phase 2, Randomized, Placebo‐Controlled, Double‐blind Study to Evaluate the Effect of VX‐661 in Combination With Ivacaftor on Chest Imaging Endpoints in Subjects Aged 12 Years and Older With Cystic Fibrosis, Homozygous for the F508del CFTR Mutation |
| Methods | Placebo‐controlled, double‐blind Phase 2 RCT. |
| Participants | 12 years and older. Homozygous for F508del CFTR mutation. Stable CF disease as judged by the investigator. FEV1 ≥ 40% and ≤ 90% of predicted; ≥ 70% of predicted normal for age, sex, and height during screening. |
| Interventions |
Group 1: morning dose VX‐661 100 mg/ivacaftor 150 mg and an evening dose (approximately 12 hours after the morning dose) ivacaftor 150 mg. Group 2: placebo. |
| Outcomes |
Primary outcome Change in CT imaging score (from baseline to week 72) Secondary outcomes Safety and tolerability assessments including number of participants with AEs and serious AEs (up to week 72) |
| Starting date | September 2016. |
| Contact information | Vertex Pharmaceuticals, Inc.(medicalinfo@vrtx.com). |
| Notes |
NCT03258424.
| Study name | Study Assessing PTI‐428 Safety, Tolerability, and Pharmacokinetics in Subjects With Cystic Fibrosis on KALYDECO® as Background Therapy |
| Methods | Phase 1 placebo‐controlled RCT. Parallel design. 2 centres. Sample size: expected to enrol 16 participants. Duration: 14 days of treatment. |
| Participants |
Inclusion criteria Age: 18 years and older. Mutation: taking ivacaftor but no specific mutations specified as eligible or ineligible. Lung function: FEV1 40% ‐ 90% predicted. |
| Interventions |
Group 1: 1x daily dosing of PTI‐428. Group 2: placebo for 14 days. All participants continue on ivacaftor. |
| Outcomes |
Primary outcome Safety and tolerability as assessed by AEs, safety labs, ECGs, physical examinations, and vital signs (at day 21) Secondary outcomes t1/2 of multiple oral doses (change from baseline to day 21) Tmax of multiple oral doses (change from baseline to day 21) Cmax of multiple oral doses (change from baseline to day 21) AUC0‐t of multiple oral doses (change from baseline to day 21) Other outcomes Nasal epithelial mRNA and protein expression over time (change from baseline to day 21) Sweat chloride (change from baseline to day 21) FEV1 (change from baseline to day 21) Weight (change from baseline to day 21) |
| Starting date | July 2017. |
| Contact information | Proteostasis Clinical Trials (pticlinicaltrials@proteostasis.com). |
| Notes |
NCT03559062.
| Study name | A Phase 3, Double‐blind, Parallel‐group Study to Evaluate the Efficacy and Safety of Tezacaftor in Combination With Ivacaftor in Subjects Aged 6 Through 11 Years With Cystic Fibrosis, Homozygous or Heterozygous for the F508del‐CFTR Mutation |
| Methods | Phase 3 double‐blind, parallel design, 4‐arm RCT. |
| Participants | Age 6 ‐ 11 years. Inclusion criteria F508del/F508del or F508del/residual function genotypes FEV1 % predicted ≥70%, adjusted for age, sex, height Screening LCI2.5 result ≥7.5 Able to swallow tablets Exclusion criteria Clinically significant cirrhosis +/‐ portal hypertension Colonization with organisms associated with a more rapid decline in pulmonary status Solid organ or hematological transplantation |
| Interventions |
Arm 1: F508del/F508del ‐ fixed‐dose combination tablet (tezacaftor/ivacaftor) Arm 2: F508del/F508del ‐ matching placebo Arm 3: F508del/residual function ‐ fixed‐dose combination tablet (tezacaftor/ivacaftor) Arm 4: F508del/residual function ‐ matching placebo |
| Outcomes |
Primary outcome measure Absolute change in LCI2.5 from baseline through week 8 Secondary outcome measures Absolute change in sweat chloride from baseline through week 8 Absolute change in CFQ‐R respiratory domain score from baseline through week 8 Safety and tolerability as measured by AEs and non‐serious AEs from baseline through safety follow‐up (16 weeks) |
| Starting date | 17 May 2018. |
| Contact information | Vertex Pharmaceuticals, Inc. (medicalinfo@vrtx.com). |
| Notes |
NCT03625466.
| Study name | A Study to Explore the Impact of Lumacaftor/Ivacaftor on Disease Progression in Subjects Aged 2 Through 5 Years With Cystic Fibrosis, Homozygous for F508del |
| Methods | Double‐blind, placebo‐controlled RCT. Parallel design. Duration: 48 weeks. Location: Germany. |
| Participants | 51 children aged 2 ‐ 5 years with CF and homozygous for F508del. |
| Interventions |
Arm 1: lumacaftor‐ivacaftor. Arm 2: matched placebo. |
| Outcomes | Absolute change in MRI global chest score, absolute change in LCI2.5, absolute change in weight‐for‐age z score, absolute change in stature‐for‐age z score, absolute change in BMI‐for‐age z score. |
| Starting date | 10 August 2018. |
| Contact information | Vertex Pharmaceuticals Incorporated. |
| Notes | 2017‐003761‐99 (EudraCT Number). |
Schwarz 2020.
| Study name | A Study to Evaluate Safety, Efficacy, and Tolerability of TEZ/IVA in Orkambi® (Lumacaftor/Ivacaftor) ‐ Experienced Subjects With Cystic Fibrosis (CF) |
| Methods | Double‐blind, placebo‐controlled, 3‐part Phase 3b RCT. Parallel design. Multicentre: 32 centres. Sample size: expected to enrol 90 participants. Duration: 28 days of treatment. |
| Participants | Age: 12 years and older. Mutation: homozygous for F508del mutation. Lung function: FEV1 ≥ 25% and ≤ 90% of predicted. |
| Interventions |
Group 1: tezacaftor 100 mg plus ivacaftor 150 mg fixed‐dose combination tablet in the morning plus ivacaftor 150 mg tablet in the evening. Group 2: placebo. |
| Outcomes |
Primary outcome Respiratory AEs (at day 56) Secondary outcomes Absolute change in % predicted FEV1 (from baseline to the average of the day 28 and day 56 measurements) Relative change in % predicted FEV1 (from baseline to the average of the day 28 and day 56 measurements) Absolute change in CFQ‐R respiratory domain score % predicted FEV1 (from baseline to the average of the day 28 and day 56 measurements) Tolerability (defined as the number and proportion of study participants who discontinue treatment) (up to day 56) AEs and serious AEs (AEs, abnormal laboratory values, vital signs or pulse oximetry) (safety follow‐up (up to 28 days after last dose of study drug)) |
| Starting date | April 2017. |
| Contact information | Vertex Pharmaceuticals, Inc.(medicalinfo@vrtx.com). |
| Notes |
AE: adverse event AUC: area under the curve BMI: body mass index CF: cystic fibrosis CFTR: cystic fibrosis transmembrane conductance regulator CFU: colony forming units CFQ‐R: Cystic Fibrosis Questionnaire‐Revised Cmax: maximum concentration CT: computer tomography ECG: electrocardiograms FEV1: forced expiratory volume in one second LCI: lung clearance index MRI: magnetic resonance imaging P aeruginosa: Pseudomonas aeruginosa PK: pharmacokinetic RCT: randomised controlled trial TEZ/IVA: tezacaftor‐ivacaftor TSQM: Treatment Satisfaction Questionnaire for Medication
Differences between protocol and review
Lung clearance index (LCI) was added as an outcome due to the increasing use of this outcome as a measure of lung function in the younger population.
We have added a statement to the Methods section that 99% confidence intervals will be used to analyse separate adverse events. This is the most appropriate statistical approach for considering adverse events individually.
Originally, we intended to combine all studies included in the review using a random‐effects approach to meta‐analysis. However, due to the substantial differences in the designs and interventions employed within the studies, we considered it more appropriate to make separate comparisons within the review, and where small numbers of studies of a similar design and intervention were pooled in meta‐analysis, a fixed‐effect approach was appropriate.
Upon identification and inclusion of new studies which examined triple combination therapies, we made the decision to analyse dual combination and triple combination therapy regimens separately.
In line with current Cochrane guidance, we have included summary of findings tables for all comparisons.
We have clarified the time points that data are reported and stated our intention that if a study which we include in future updates presents data at more than one time point within any of our stated time ranges we will present the later data set from the study.
Contributions of authors
| Roles and responsibilities | |
| TASK | RESPONSIBILITY |
| Protocol stage: draft the protocol | IS, SP with comments from all |
| Review stage: select which trials to include (2 + 1 arbiter) | JM, IS, SP (+ KWS) |
| Review stage: extract data from trials (2 people) | JM, IS, SP |
| Review stage: enter data into RevMan | JM, SP, SJN |
| Review stage: carry out the analysis | JM, SP, SJN |
| Review stage: interpret the analysis | JM, IS, SP, SJN |
| Review stage: draft the final review | JM, IS, SP, KWS with comments from all |
| Update stage: update the review | JM, IS, KWS and SJN |
Sources of support
Internal sources
No sources of support supplied
External sources
-
National Institute for Health Research, UK
This systematic review was supported by the National Institute for Health Research, via Cochrane Infrastructure funding to the Cochrane Cystic Fibrosis and Genetic Disorders Group.
Declarations of interest
Professor Kevin Southern declares no potential conflict of interest.
Dr Ian Sinha is in receipt of a NIHR HTA grant for paediatric asthma and is a member of the NICE asthma committee; however, neither of these are related to cystic fibrosis or this review and thus do not constitute a potential conflict of interest.
Dr Sarah J Nevitt declares no potential conflict of interest.
Dr Jared Murphy declares no potential conflict of interest.
New search for studies and content updated (conclusions changed)
References
References to studies included in this review
Boyle 2014 {published data only}2010‐020413‐90
- Boyle M, Bell SC, Konstan M, McColley S, Flume P, Kang L, et al. Lumacaftor, an investigational CFTR corrector, in combination with ivacaftor, a CFTR potentiator, in CF patients with the F508del-CFTR mutation: phase 2 interim analysis. Journal of Cystic Fibrosis 2013;12 Suppl 1:S14. [ABSTRACT NO.: WS7.4] [CENTRAL: 921640] [CFGD REGISTER: BD169c] [Google Scholar]
- Boyle MP, Bell S, Konstan M, McColley SA, Kang L, Patel N, et al. The investigational CFTR corrector, VX-809 (lumacaftor) co-administered with the oral potentiator ivacaftor improved CFTR and lung function in F509-8DEL homozygous patients: phase II study results. Pediatric Pulmonology 2012;47 Suppl 35:315. [ABSTRACT NO.: 260] [CENTRAL: 921644] [CFGD REGISTER: BD169b] [Google Scholar]
- Boyle MP, Bell S, Konstan MW, McColley SA, Wisseh S, Spencer-Green G. VX-809, an investigational CFTR corrector, in combination with VX-770, an investigational CFTR potentiator, in subjects with CF and homozygous for the F508DEL-CFTR Mutation. Pediatric Pulmonology 2011;46 Suppl 34:287. [ABSTRACT NO.: 212] [CENTRAL: 848840] [CFGD REGISTER: BD169a] [Google Scholar]
- Boyle MP, Bell SC, Konstan MW, McColley SA, Rowe SM, Rietschel E, et al. A CFTR corrector (lumacaftor) and a CFTR potentiator (ivacaftor) for treatment of patients with cystic fibrosis who have a phe508del CFTR mutation: A phase 2 randomised controlled trial. Lancet. Respiratory Medicine 2014;2(7):527-38. [CENTRAL: 994993] [CFGD REGISTER: BD169d] [EMBASE: 2014458184] [DOI] [PubMed] [Google Scholar]
- Boyle MP, Bell SC, Konstan MW, McColley SA, Rowe SM, Rietschel E, et al. Supplementary Appendix to "A CFTR corrector (lumacaftor) and a CFTR potentiator (ivacaftor) for treatment of patients with cystic fibrosis who have a phe508del CFTR mutation: A phase 2 randomised controlled trial.". Lancet. Respiratory Medicine 2014;2(7):527-38. Online. [CENTRAL: 997711] [CFGD REGISTER: BD169e] [DOI] [PubMed] [Google Scholar]
- Rowe SM, McColley SA, Rietschel E, Li X, Bell SC, Konstan MW, et al. Lumacaftor/ivacaftor treatment of patients with cystic fibrosis heterozygous for F508del-CFTR. Annals of the American Thoracic Society 2017;14(2):213-219. Online supplement: data. [CFGD REGISTER: BD169h] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rowe SM, McColley SA, Rietschel E, Li X, Bell SC, Konstan MW, et al. Lumacaftor/ivacaftor treatment of patients with cystic fibrosis heterozygous for F508del-CFTR. Annals of the American Thoracic Society 2017;14(2):213-219. Online supplement: disclosures. [CFGD REGISTER: BD169g] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rowe SM, McColley SA, Rietschel E, Li X, Bell SC, Konstan MW, et al. Lumacaftor/ivacaftor treatment of patients with cystic fibrosis heterozygous for F508del-CFTR. Annals of the American Thoracic Society 2017;14(2):213-9. [CFGD REGISTER: BD169f] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Clancy 2012 {published data only}
- Clancy JP, Rowe SM, Accurso FJ, Aitken ML, Amin RS, Ashlock MA, et al. Results of a phase IIa study of VX-809, an investigational CFTR corrector compound, in subjects with cystic fibrosis homozygous for the F508del-CFTR mutation. Thorax 2012;67(1):12-8. [CENTRAL: 806692] [CFGD REGISTER: BD166c] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clancy JP, Rowe SM, Accurso FJ, Ballmann M, Boyle MP, DeBoeck C, et al. A phase II, randomized, placebo-controlled, clinical trial of four doses of VX-809 in CF patients homozygous for the F508del CFTR mutation. Pediatric Pulmonology 2010;45 Suppl 33(S33):298. [ABSTRACT NO.: 224] [CENTRAL: 848845] [CFGD REGISTER: BD166b] [Google Scholar]
- Clancy JP, Rowe SM, Liu B, Hathorne H, Dong Q, Wisseh S, et al. Variability of nasal potential difference measurements in clinical testing of CFTR modulators. Pediatric Pulmonology 2011;46 Suppl 34(S34):283. [ABSTRACT NO.: 202] [CENTRAL: 848842] [CFGD REGISTER: BD166d // BD165n] [Google Scholar]
- Clancy JP, Spencer-Green G, for theVX-809-101SG. Clinical evaluation of VX-809, a novel investigational oral F508del-CFTR corrector, in subjects with cystic fibrosis homozygous for the F508del-CFTR mutation. Journal of Cystic Fibrosis 2010;9 Suppl 1:S20. [ABSTRACT NO.: 73] [CENTRAL: 848846] [CFGD REGISTER: BD166a] [Google Scholar]
Davies 2018a {published data only}
- Davies JC, Moskowitz SM, Brown C, Horsley A, Mall MA, McKone EF, et al. VX-659-tezacaftor-ivacaftor in patients with cystic fibrosis and one or two Phe508del alleles. New England Journal of Medicine 2018;379(17):1599-611. [CENTRAL: CN-01650323] [CFGD REGISTER: BD260] [EMBASE: 624591628] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Davies 2018b {published data only}
- Colombo C, Tullis E, Davies JC, McKee C, DeSouza C, Waltz D, et al. Preliminary safety and efficacy of triple combination CFTR modulator regimens in CF. Italian Journal of Pediatrics 2018;44(Suppl 1):6. [ABSTRACT NO.: 03] [CFGD REGISTER: BD248b] [Google Scholar]
- Davies JC, Colombo C, Tullis E, Mckee C, Desouza C, Waltz D, et al. Preliminary safety and efficacy of triple combination CFTR modulator regimens in cystic fibrosis. Journal of Cystic Fibrosis 2018;17(Suppl 3):S3. [CENTRAL: CN-01730786] [CFGD REGISTER: BD248a] [EMBASE: 622930757] [Google Scholar]
- Davies JC, Moskowitz SM, Brown C, Horsley A, Mall MA, McKone EF, et al. VX-659-tezacaftor-ivacaftor in patients with cystic fibrosis and one or two Phe508del alleles. New England Journal of Medicine 2018;379(17):1599-611. [CENTRAL: CN-01650323] [CFGD REGISTER: BD260] [DOI: 10.1056/NEJMoa1807119] [EMBASE: 624591628] [PMID: 30334693 ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tullis E, Colombo C, Davies J, Wark P, McKee C, Desouza C, et al. Preliminary safety and efficacy of triple-combination CFTR modulator regimens. Respirology 2018;23(Suppl 1):33. [ABSTRACT NO.: TO 026] [CFGD REGISTER: BD248c] [Google Scholar]
Donaldson 2014 {published data only}
- Donaldson SH, Shoemaker S, Mandagere A, Troha J. Novel modifiers of CFTR: emerging clinical experience with GSNOR inhibitors. Pediatric Pulmonology 2014;49 Suppl 38:154. [ABSTRACT NO.: S10.2] [CENTRAL: 1015872] [CFGD REGISTER: BD217b] [Google Scholar]
- Donaldson SH, Taylor-Cousar JL, Rosenbluth D, Zeitlin P, Chmiel J, Jain M, et al. Safety, tolerability, and pharmacokinetics of the intravenous S-nitrosoglutathione reductase inhibitor N6022: an ascending-dose study in subjects homozygous for the F508DEL-CFTR mutation. Pediatric Pulmonology 2014;49 Suppl 38:308. [ABSTRACT NO.: 258] [CENTRAL: 1012386] [CFGD REGISTER: BD217a] [Google Scholar]
- NCT01746784. Safety and Pharmacokinetic Study of N6022 in Subjects With Cystic Fibrosis Homozygous for the F508del CFTR Mutation (SNO1) [A Phase 1b, randomized, double-blind, placebo-controlled, dose escalation study of N6022 to evaluate safety and pharmacokinetics in subjects with cystic fibrosis homozygous for the F508del-CFTR mutation (SNO1)]. clinicaltrials.gov/ct2/show/NCT01746784 (first posted 11 December 2012). [CLINICALTRIALS.GOV: NCT01746784]
Donaldson 2017 {published data only}
- Donaldson SH, Solomon GM, Zeitlin PL, Flume PA, Casey A, McCoy K, et al. Pharmacokinetics and safety of cavosonstat (N91115) in healthy and cystic fibrosis adults homozygous for F508DEL-CFTR. Journal of Cystic Fibrosis 2017;16(3):371-379. Online supplementary tables and figures. [CFGD REGISTER: BD226c] [DOI] [PubMed] [Google Scholar]
- Donaldson SH, Solomon GM, Zeitlin PL, Flume PA, Casey A, McCoy K, et al. Pharmacokinetics and safety of cavosonstat (N91115) in healthy and cystic fibrosis adults homozygous for F508DEL-CFTR. Journal of Cystic Fibrosis 2017;16(3):371-9. [CFGD REGISTER: BD226b] [DOI] [PubMed] [Google Scholar]
- Donaldson SH. Safety and pharmacokinetics of N91115 in patients with cystic fibrosis homozygous for the F508DEL-CFTR mutation. Pediatric Pulmonology 2015;50 Suppl 41:293. [ABSTRACT NO.: 270] [CENTRAL: 1092200] [CFGD REGISTER: BD226a] [Google Scholar]
- NCT02275936. Study of N91115 in patients with cystic fibrosis homozygous F508del-CFTR mutation (SNO4) [A phase 1b, randomized, double-blind, placebo-controlled, parallel, group study of N91115 to evaluate safety and pharmacokinetics in patients with cystic fibrosis homozygous for the F508del-CFTR mutation]. clinicaltrials.gov/ct2/show/NCT02275936 (first posted 27 October 2014).
Donaldson 2018 {published data only}
- Donaldson S, Pilewski J, Griese M, Dong Q, Lee PS, for theVX11-661-101SG. VX-661, an investigational CFTR corrector, in combination with ivacaftor, a CFTR potentiator, in patients with CF and homozygous for the F508Del-CFTR mutation: interim analysis. Journal of Cystic Fibrosis 2013;12 Suppl 1:S14. [ABSTRACT NO.: WS7.3] [CENTRAL: 872941] [CFGD REGISTER: BD190a] [Google Scholar]
- Donaldson SH, Pilewski JM, Cooke J, Himes-Lekstrom J, VX11-661-101 SG. Addition of VX-661, an investigational CFTR corrector, to ivacaftor, a CFTR potentiator, in patients with CF and heterozygous for F508DEL/G551D-CFTR. Pediatric Pulmonology 2014;49 Suppl 38:308-9. [ABSTRACT NO.: 260] [CENTRAL: 1012385] [CFGD REGISTER: BD190c] [Google Scholar]
- Donaldson SH, Pilewski JM, Griese M, Cooke J, Viswanathan L, Tullis E, et al. Tezacaftor/ivacaftor in subjects with cystic fibrosis and F508del/F508del-CFTR or F508del/G551D-CFTR. American Journal of Respiratory and Critical Care Medicine 2018;197(2):214-224. Online data supplement. [CFGD REGISTER: BD190f] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Donaldson SH, Pilewski JM, Griese M, Cooke J, Viswanathan L, Tullis E, et al. Tezacaftor/ivacaftor in subjects with cystic fibrosis and F508del/F508del-CFTR or F508del/G551D-CFTR. American Journal of Respiratory and Critical Care Medicine 2018;197(2):214-24. [CFGD REGISTER: BD190e] [DOI] [PMC free article] [PubMed] [Google Scholar]
- EUCTR2011-003821-93-DE. A phase 2, multicenter, double blinded, placebo controlled study to evaluate safety, efficacy, pharmacokinetics, and pharmacodynamics of VX-661 monotherapy and vx-661/ivacaftor cotherapy in subjects with cystic fibrosis, homozygous or heterozygous for the f508del CFTR mutation. www.who.int/trialsearch/Trial2.aspx?TrialID=EUCTR2011-003821-93-DE (first received 2011). [CENTRAL: CN-01882341] [CFGD REGISTER: BD190g]
- NCT01531673. Study of VX-661 alone and in combination with ivacaftor in subjects homozygous or heterozygous to the F508del-Cystic Fibrosis Transmembrane Conductance Regulator(CFTR) mutation [A phase 2, multicenter, double-blinded, placebo controlled study to evaluate safety, efficacy, pharmacokinetics, and pharmacodynamics of VX-661 monotherapy and VX-661/ivacaftor cotherapy in subjects with cystic fibrosis, homozygous or heterozygous for the F508del-CFTR mutation]. clinicaltrials.gov/ct2/show/NCT01531673 (first posted 13 February 2012).
- Pilewski JM, Cooke J, Lekstrom-Himes J, Donaldson S, for the VX-661IG. VX-661 in combination with ivacaftor in patients with cystic fibrosis and the F508del-CFTR mutation. Journal of Cystic Fibrosis 2015;14 Suppl 1:S1. [ABSTRACT NO.: WS01.4] [CENTRAL: 1081479] [CFGD REGISTER: BD190d] [Google Scholar]
- Pilewski JM, Donaldson SH, Cooke J, Lekstrom-Himes J. Phase 2 studies reveal additive effects of VX-661, an investigational CFTR corrector, and ivacaftor, a CFTR potentiator, in patients with CF who carry the F508Del-CFTR mutation. Pediatric Pulmonology 2014;49 Suppl 38:157-9. [CENTRAL: 1015871] [CFGD REGISTER: BD190b] [Google Scholar]
Heijerman 2019 {published data only}
- Department of Error. Erratum: Department of Error (The Lancet (2019) 394(10212) (1940–1948), (S0140673619325978), (10.1016/S0140-6736(19)32597-8)). Lancet 2020;395(10238):1694. [CENTRAL: CN-02164017] [CFGD REGISTER: BD268c] [EMBASE: 2006013175] [PMID: 32473673]32473673 [Google Scholar]
- Heijerman H, McKone E, Downey DG, Mall M, Ramsey B, Rowe S, et al. Phase 3 efficacy and safety of the ELX/TEZ/ iva triple combination in people with CF homozygous for the F508del mutation. Pediatric Pulmonology 2019;54 Suppl 2:347. [CENTRAL: CN-01990652] [CFGD REGISTER: BD268a] [EMBASE: 629389111] [Google Scholar]
- Heijerman HGM, McKone EF, Downey DG, Van Braeckel E, Rowe SM, Tullis E, et al. Efficacy and safety of the elexacaftor plus tezacaftor plus ivacaftor combination regimen in people with cystic fibrosis homozygous for the F508del mutation: a double-blind, randomised, phase 3 trial. Lancet 2019;394(10212):1940-8. [CENTRAL: CN-02006814] [CFGD REGISTER: BD268b] [DOI: 10.1016/S0140-6736(19)32597-8] [EMBASE: 2003873327] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- NCT03525548. A study of VX-445 combination therapy in CF subjects homozygous for F508del (F/F). clinicaltrials.gov/ct2/show/NCT03525548 (first posted 15 May 2018). [EUDRACT NUMBER: 2018-000184-89]
Horsley 2017 {published and unpublished data}
- Horsley A, Burr L, Kotsimbos T, Ledson M, Schwarz C, Simmonds N, et al. Safety, pharmacokinetics and pharmacodynamics of the CFTR corrector FDL169. Journal of Cystic Fibrosis 2018;17(Suppl 3):S42. [CFGD REGISTER: BD250a] [Google Scholar]
- Horsley AR, Blaas S, Burr L, Caroll M, Downey DG, Drevinek P, et al. Novel CFTR corrector FDL169: safety, pharmacokinetics and pharmacodynamics. Journal of Cystic Fibrosis 2018;17 Suppl 3:S42. [ABSTRACT NO.: EPS3.06] [CFGD REGISTER: BD250b] [Google Scholar]
Keating 2018 {published data only}2017‐000797‐11
- Keating D, Marigowda G, Burr L, Daines C, Mall MA, McKone EF, et al. VX-445-Tezacaftor-Ivacaftor in Patients with Cystic Fibrosis and One or Two Phe508del Alleles. New England Journal of Medicine 2018;379(17):1612-20. [CENTRAL: CN-01650324] [CFGD REGISTER: BD259] [EMBASE: 624591484] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- NCT03227471. A study of VX-445 in healthy subjects and subjects with cystic fibrosis [A phase 1/2 study of VX-445 in healthy subjects and subjects with cystic fibrosis]. clinicaltrials.gov/ct2/show/NCT03227471 (first posted 24 July 2017).
McCarty 2002 {published data only}
- Ahrens RC, Standaert TA, Launspach J, Han SH, Teresi ME, Aitken ML, et al. Use of nasal potential difference and sweat chloride as outcome measures in multicenter clinical trials in subjects with cystic fibrosis. Pediatric Pulmonology 2002;33(2):142-50. [CENTRAL: 385693] [CFGD REGISTER: BD136d ] [DOI] [PubMed] [Google Scholar]
- Aitken ML, Ahrens RC, Karlin DA, Konstan MW, McNamara SC, Regelman WE, et al. Safety of a phase I double-blind placebo-controlled dose escalation trial of oral CPX in adult CF patients. Pediatric Pulmonology 1998;26 Suppl 17:276. [CENTRAL: 385694] [CFGD REGISTER: BD136b] [Google Scholar]
- McCarty NA, Standaert TA, Teresi M, Tuthill C, Launspach J, Kelley TJ, et al. A phase I randomized, multicenter trial of CPX in adult subjects with mild cystic fibrosis. Pediatric Pulmonology 2002;33(2):90-8. [CENTRAL: 377220] [CFGD REGISTER: BD136c] [PMID: ] [DOI] [PubMed] [Google Scholar]
- McCarty NA, Weatherly MR, Kelley TJ, Konstan MW, Milgram LJ, Teresi M, et al. Multicenter phase I trial of CPX in adults patients with mild CF: results of nasal potential difference measurements. Pediatric Pulmonology 1998;26 Suppl 17:276. [CENTRAL: 291449] [CFGD REGISTER: BD136a] [Google Scholar]
Middleton 2019 {published data only}
- Fajac I, Van Brunt K, Daines C, Durieu I, Goralski J, Heijerman H, et al. Impact of elexacaftor/tezacaftor/ivacaftor triple combination therapy on health-related quality of life in people with cystic fibrosis heterozygous for F508del and a minimal function mutation: results from a Phase 3 clinical study. Journal of Cystic Fibrosis 2020;19:S118-9. [CENTRAL: CN-02140149] [CFGD REGISTER: BD267c] [EMBASE: 2006056615] [Google Scholar]
- Jain R, Mall M, Drevinek P, Lands L, McKone E, Polineni D, et al. Phase 3 efficacy and safety of the ELX/TEZ/ iva triple combination in people with CF and F508del/minimal function genotypes. Pediatric Pulmonology 2019;54 Suppl:346-7. [CENTRAL: CN-01987255] [CFGD REGISTER: BD267a] [EMBASE: 629389084] [Google Scholar]
- Middleton PG, Mall MA, Drevinek P, Lands LC, McKone EF, Polineni D, et al. Elexacaftor-tezacaftor-ivacaftor for cystic fibrosis with a single phe508del allele. New England Journal of Medicine 2019;381(19):1809-19. [CENTRAL: CN-02004607] [CFGD REGISTER: BD267b] [DOI: 10.1056/NEJMoa1908639] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- NCT03525444. A phase 3 study of VX-445 combination therapy in subjects with cystic fibrosis heterozygous for the f508del mutation and a minimal function mutation (F/MF) [A phase 3, randomized, double-blind, controlled study evaluating the efficacy and safety of VX-445 combination therapy in subjects with cystic fibrosis who are heterozygous for the f508del mutation and a minimal function mutation (F/MF)]. clinicaltrials.gov/show/NCT03525444 (first received 15 May 2018). [CENTRAL: CN-01659552] [CFGD REGISTER: BD267d] [EUDRACT NUMBER: 2018-000183-28]
PROGRESS 2017 {published data only}
- Konstan M, McKone E, Moss R, Marigowda G, Cooke J, Lubarsky B, et al. Evidence of reduction in annual rate of FEV1 decline and sustained benefits with lumacaftor and ivacaftor (LUM/IVA) in patients (pts) with cf homozygous for F508DEL-CFTR. Pediatric Pulmonology 2016;51 Suppl 45:260. [ABSTRACT NO.: 180] [CFGD REGISTER: BD213p // BD214p] [Google Scholar]
- Konstan MW, McKone EF, Moss RB, Marigowda G, Tian S, Waltz D, et al. Assessment of safety and efficacy of long-term treatment with combination lumacaftor and ivacaftor therapy in patients with cystic fibrosis homozygous for the F508del-CFTR mutation (PROGRESS): a phase 3, extension study. Lancet. Respiratory Medicine 2017;5(2):107-118. Online supplementary appendix. [CFGD REGISTER: BD213r // BD214r] [DOI] [PubMed] [Google Scholar]
- Konstan MW, McKone EF, Moss RB, Marigowda G, Tian S, Waltz D, et al. Assessment of safety and efficacy of long-term treatment with combination lumacaftor and ivacaftor therapy in patients with cystic fibrosis homozygous for the F508del-CFTR mutation (PROGRESS): a phase 3, extension study. Lancet. Respiratory Medicine 2017;5(2):107-18. [CFGD REGISTER: BD213q // BD214q] [PMID: ] [DOI] [PubMed] [Google Scholar]
- NCT01931839. A phase 3 rollover study of lumacaftor in combination with ivacaftor in subjects 12 years and older with cystic fibrosis [A phase 3, rollover study to evaluate the safety and efficacy of long-term treatment with lumacaftor in combination with ivacaftor in subjects aged 12 Years and older with cystic fibrosis, homozygous or heterozygous for the F508del-CFTR mutation]. clinicaltrials.gov/ct2/show/NCT01931839 (first posted 29 August 2013). [CLINICALTRIALS.GOV: NCT01931839]
Ratjen 2017 {published data only}
- Anonymous. Corrections [Corrections: efficacy and safety of lumacaftor and ivacaftor in patients aged 6-11 years with cystic fibrosis homozygous for F508del-CFTR: a randomised, placebo-controlled phase 3 trial (The Lancet Respiratory Medicine (2017) 5(7) (557-567)(S2213260017302151)(10.1016/S2213-2600(17)30215-1))]. Lancet Respiratory Medicine 2017 Aug;5(8):e28. [CENTRAL: CN-01473292] [CFGD REGISTER: BD233k] [EMBASE: 617478198] [PMID: ] [DOI] [PubMed] [Google Scholar]
- Brody A, Nagle SK, Owen C, Marigowda G, Waltz D, Goldin J, et al. Effect of lumacaftor/ivacaftor on total, bronchiectasis, and air trapping computed tomography scores in children homozygous for F508DEL-CFTR: exploratory imaging substudy. Pediatric Pulmonology 2017;52 Suppl 47:286. [CFGD REGISTER: BD233d] [Google Scholar]
- Brody AS, Nagle S, Hug C, Marigowda G, Waltz D, Goldin J, et al. Effect of lumacaftor/ivacaftor on total, bronchiectasis, and air trapping computed tomography (CT) scores in children homozygous for F508del-CFTR: exploratory imaging substudy. Thorax 2017;72(Supplement 3):A57. [CENTRAL: CN-01643820] [CFGD REGISTER: BD233e] [EMBASE: 619739057] [Google Scholar]
- Brody AS, Nagle S, Hug C, Marigowda G, Waltz D, Goldin J, et al. Effect of lumacaftor/ivacaftor on total, bronchiectasis and air trapping computed tomography (CT) scores in children homozygous for F508del-CFTR: exploratory imaging substudy. Thorax 2017;72(Suppl 3):A57. [CFGD REGISTER: BD233e] [Google Scholar]
- Milla C, Ratjen F, Marigowda G, Liu F, Waltz D, Rosenfeld M. Safety, tolerability, and pharmacodynamics of combination lumacaftor/ivacaftor therapy in patients aged 6-11 yrs with CF homozygous for the F508DEL-CFTR mutation. Pediatric Pulmonology 2016;51 Suppl:259. [CENTRAL: CN-01212610] [CFGD REGISTER: BD233j] [EMBASE: 612358598] [Google Scholar]
- Nagle S, Brody AS, Woods J, Johnson KM, Wang L, Marigowda G, et al. Feasibility of ultrashort echo time (UTE) MRI to evaluate the effect of lumacaftor/ivacaftor therapy in children with cystic fibrosis (CF) homozygous for F508DEL. Thorax 2017;72(Suppl 3):A221. [CENTRAL: CN-01643817] [CFGD REGISTER: BD233g] [EMBASE: 619738999] [Google Scholar]
- Nagle SK, Brody A, Woods JC, Johnson KM, Wang L, Marigowda G, et al. Feasibility of ultrashort echo time MRI to evaluate the effect of lumacaftor/ ivacaftor therapy in children with cystic fibrosis homozygous for f508del. Pediatric Pulmonology 2017;52 Suppl 47:314-5. [CENTRAL: CN-01622615] [CFGD REGISTER: BD233f] [EMBASE: 619069874] [Google Scholar]
- Ratjen F, Hug C, Marigowda G, Tian S, Huang X, Stanojevic S, et al. Efficacy and safety of lumacaftor and ivacaftor in patients aged 6–11 years with cystic fibrosis homozygous forF508del-CFTR: a randomised, placebo-controlled, phase 3 trial. Lancet Respiratory Medicine 2017;5(7):557-67. [CFGD REGISTER: BD233b] [DOI] [PubMed] [Google Scholar]
- Ratjen F, Hug C, Marigowda G, Tian S, Huang X, Stanojevic S, et al. Efficacy and safety of lumacaftor and ivacaftor in patients aged 6-11 years with cystic fibrosis homozygous for F508del-CFTR: a randomised, placebo-controlled phase 3 trial. Lancet. Respiratory Medicine 2017;5(7):557-567. Online supplementary appendix. [CFGD REGISTER: BD233c] [DOI] [PubMed] [Google Scholar]
- Ratjen F, Tian S, Marigowda G, Hug C, Huang X, Stanojevic S, et al. Efficacy and safety of lumacaftor/ivacaftor (LUM/IVA) in patients (pts) aged 6-11 years (yrs) with cystic fibrosis (CF) homozygous for F508del-CFTR: a randomized placebo (PBO)-controlled phase 3 trial. Journal of Cystic Fibrosis 2017;16 Suppl 1:S24. [ABSTRACT NO.: WS13.4] [CENTRAL: 1383249] [CFGD REGISTER: BD233a] [Google Scholar]
- Wainwright C, Brody A, Nagle S, Hug C, Marigowda G, Waltz D, et al. Effect of lumacaftor/ivacaftor on ct scores: exploratory imaging substudy. Respirology 2018;23(Suppl 1):57. [CENTRAL: CN-01920038] [CFGD REGISTER: BD233h] [EMBASE: 622091817] [Google Scholar]
- Wainwright C, Nagle S, Brody A, Woods J, Johnson K, Wang L, et al. Ultrashort echo time MRI can evaluate treatment effect of Lumacaftor/Ivacaftor. Respirology 2018;23(Suppl 1):141. [CENTRAL: CN-01919971] [CFGD REGISTER: BD233i] [EMBASE: 622091399] [Google Scholar]
Rubenstein 1998 {published data only}
- Rubenstein RC, Zeitlin PL. A pilot clinical trial of oral sodium 4-phenylbutyrate (Buphenyl) in deltaF508-homozygous cystic fibrosis patients: partial restoration of nasal epithelial CFTR function. American Journal of Respiratory and Critical Care Medicine 1998;157(2):484-90. [CENTRAL: 201485] [CFGD REGISTER: BD146b] [EMBASE: 1998064104] [PMID: ] [DOI] [PubMed] [Google Scholar]
- Rubenstein RC, Zeitlin PL. A randomized, double blind, placebo-controlled trial of sodium 4-phenylbutyrate (Buphenyl) in deltaF508-homozygous cystic fibrosis patients: partial restoration of nasal epithelial CFTR function. Pediatric Pulmonology 1997;Suppl 14:272. [CENTRAL: 291563] [CFGD REGISTER: BD146a] [DOI] [PubMed] [Google Scholar]
Taylor‐Cousar 2017 {published data only}
- Flume P, Lekstrom-Himes J, Fischer Biner R, Simard C, Downey DG, Zhou H, et al. A phase 3, open-label study of tezacaftor/ivacaftor (TEZ/IVA) therapy, interim analysis of pooled safety, and efficacy in patients homozygous for F508del-CFTR. Journal of Cystic Fibrosis 2018;17 Suppl 3:S64-5. [CFGD REGISTER: BD236d] [Google Scholar]
- Ingenito E, Nair N, Yi B, Lekstrom-Himes J, Elborn JS, Rowe SM. Retrospective analysis of physiological response patterns to tezacaftor/ivacaftor in patients with cystic fibrosis homozygous for F508DEL-CFTR or heterozygous for F508DEL-CFTR and a residual function mutation. Thorax 2018;73(Suppl 4):A42-3. [CENTRAL: CN-02002310] [CFGD REGISTER: BD236i // BD237h] [EMBASE: 627697348] [Google Scholar]
- Smith D, Flume P, Lekstrom-Himes J, Fischer Biner R, Simard C, Downey D, et al. Phase 3 interim analysis: tezacaftor/ivacaftor (TEZ/IVA) in patients homozygous for F508delcystic fibrosis transmembrane conductance regulator (CFTR). Respirology 2019;24(S1):30. [ABSTRACT NO.: TO017] [CENTRAL: CN-02002181] [CFGD REGISTER: BD236j] [EMBASE: 626940397] [Google Scholar]
- Sommerburg O, Yang Y, Rizio AA, Loop B, You X, Kosinski M, et al. Effects of tezacaftor/ivacaftor (TEZ/IVA) treatment in patients with cystic fibrosis and F508del/F508del-CFTR: patient-reported outcomes in a Phase 3, randomised, controlled trial (EVOLVE). Pneumologie 2019;73(Suppl 1). [CENTRAL: CN-01960604] [CFGD REGISTER: BD236h] [EMBASE: 628475389] [Google Scholar]
- Sutharsan S, Taylor-Cousar J, Lekstrom-Himes J, Wang L, Lu Y, Elborn JS. Efficacy and safety of tezacaftor/ivacaftor in patients aged >= 12 years with CF homozygous for F508del-CFTR: a randomized placebo (PBO)-controlled phase 3 trial. Pneumologie (Stuttgart, Germany) 2018;72(Suppl 1):S36. [CFGD REGISTER: BD236e] [Google Scholar]
- Taylor-Cousar JL, Elborn S. Advances in treating patients homozygous for F508del. Pediatric Pulmonology 2017;52 Suppl 47:173-5. [CFGD REGISTER: BD236c] [Google Scholar]
- Taylor-Cousar JL, Lekstrom-Himes J, Wang L, Lu Y, Elborn S. Efficacy and safety of tezacaftor/ ivacaftor in patients aged >=12 years with cf homozygous for f508del-cftr: a randomized placebo-controlled phase 3 trial. Pediatric Pulmonology 2017;52 Suppl 47:307. [CFGD REGISTER: BD236a] [Google Scholar]
- Taylor-Cousar JL, Munck A, McKone EF, Ent CK, Moeller A, Simard C, et al. Tezacaftor-ivacaftor in patients with cystic fibrosis homozygous for Phe508del. New England Journal of Medicine 2017;377(21):2013-23. [CFGD REGISTER: BD236b] [DOI: 10.1056/NEJMoa1709846] [DOI] [PubMed] [Google Scholar]
- Yang Y, Rizio A, Chuang C, Loop B, You X, Kosinski M, et al. Effects of tezacaftor/ivacaftor treatment in patients with cystic fibrosis and F508del/F508del-CFTR: patient-reported outcomes in a phase 3 randomized, controlled trial. Pediatric Pulmonology 2018;53(S2):264. [CFGD REGISTER: BD236f] [Google Scholar]
- Yang Y, Rizio AA, Chuang C-C, Loop B, You X, Kosinski M, et al. Effects of tezacaftor/ivacaftor (TEZ/IVA) treatment in patients with cystic fibrosis homozygous for F508DEL-CFTR: patient-reported outcomes in a phase 3 randomized, controlled trial (EVOLVE). Thorax 2018;73(Suppl 4):A42. [CENTRAL: CN-01936246] [CFGD REGISTER: BD236g] [DOI: 10.1136/thorax-2018-212555.74 ] [EMBASE: 627697250] [Google Scholar]
TRAFFIC 2015 {published data only}
- Anstead M, Tupayachi G, Murphy D, Autry E, Bulkley V, Kuhn R. Lumacaftor/ivacaftor: real world experience in a CF center. Pediatric Pulmonology 2016;51 Suppl:302. [CFGD REGISTER: BD213s // BD214s] [Google Scholar]
- De Boeck C. Long-term clinical effects of CFTR co-therapy with lumacaftor/ivacaftor. Pediatric Pulmonology 2015;50:135-7. [CENTRAL: 1163954] [CFGD REGISTER: BD213m/BD214m] [EMBASE: 72081237] [SYMPOSIUM SUMMARY: S9.1] [Google Scholar]
- De Boeck K, Elborn J, Ramsey B, Boyle MP, Konstan MW, Huang X, et al. Efficacy and safety of lumacaftor+ivacaftor combination therapy in patients with CF homozygous for F508DEL-CFTR by FEV1 subgroups. Pediatric Pulmonology 2015;50 Suppl 41:283. [ABSTRACT NO.: 245] [CENTRAL: 1092180] [CFGD REGISTER: BD213f/BD214f] [Google Scholar]
- Elborn J, Wainwright CE, Ramsey B, Huang X, Margowda G, Waltz D, et al. Effect of lumacaftor in combination with ivacaftor in patients with cystic fibrosis who are homozygous for F508-DEL-CFTR: the TRAFFIC Study. Pediatric Pulmonology 2014;49 Suppl 38:304. [ABSTRACT NO.: 249] [CENTRAL: 1012382] [CFGD REGISTER: BD213a] [Google Scholar]
- Elborn JS, Ramsey B, Boyle MP, Wainwright C, Konstan M, Huang X, et al. Lumacaftor in combination with ivacaftor in patients with cystic fibrosis who are homozygous for the F508del-CFTR mutation. Journal of Cystic Fibrosis 2015;14 Suppl 1:S1. [ABSTRACT NO.: WS01.3] [CENTRAL: 1077209] [CFGD REGISTER: BD213e/BD214d] [Google Scholar]
- Elborn JS, Ramsey BW, Boyle MP, Konstan MW, Huang X, Marigowda G, et al. Efficacy and safety of lumacaftor/ivacaftor combination therapy in patients with cystic fibrosis homozygous for Phe508del CFTR by pulmonary function subgroup: a pooled analysis. Lancet. Respiratory Medicine 2016;4(8):617-26. [CENTRAL: 1157425] [CFGD REGISTER: BD213i/BD214i] [DOI: 10.1016/S2213-2600(16)30121-7] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elborn JS, Ramsey BW, Boyle MP, Konstan MW, Huang X, Marigowda G, et al. Efficacy and safety of lumacaftor/ivacaftor combination therapy in patients with cystic fibrosis homozygous for Phe508del CFTR by pulmonary function subgroup: a pooled analysis. Lancet. Respiratory Medicine 2016;4(8):617-26. Online supplementary appendix. [CFGD REGISTER: BD213o/BD214o ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elborn JS, Ramsey BW, Boyle MP, Wainwright CE, Konstan MW, Huang X, et al. Lumacaftor/ ivacaftor combination therapy in CF patients homozygous for F508del-CFTR with severe lung dysfunction. Journal of Cystic Fibrosis 2015;14 Suppl 1:S94. [ABSTRACT NO.: 143] [CENTRAL: 1077207] [CFGD REGISTER: BD213c/BD214d] [Google Scholar]
- Flume PA, Suthoff ED, Kosinski M, Marigowda G, Quittner AL. Measuring recovery in health-related quality of life during and after pulmonary exacerbations in patients with cystic fibrosis. Journal of Cystic Fibrosis 2019;18(5):737-42. [CENTRAL: CN-01742131] [CFGD REGISTER: BD213u // BD214u] [DOI: 10.1016/j.jcf.2018.12.004] [EMBASE: 2001400109] [DOI] [PubMed] [Google Scholar]
- Konstan M, McKone E, Moss R, Marigowda G, Cooke J, Lubarsky B, et al. Evidence of reduction in annual rate of FEV1 decline and sustained benefits with lumacaftor and ivacaftor (LUM/IVA) in patients (pts) with cf homozygous for F508DEL-CFTR. Pediatric Pulmonology 2016;51 Suppl 45:260. [ABSTRACT NO: 180] [CFGD REGISTER: BD213p // BD214p] [Google Scholar]
- Konstan MW, Ramsey BW, Elborn J, Boyle MP, Waltz D, Marigowda G, et al. Safety and efficacy of treatments with lumacaftor in combination with ivacaftor in patients with CF homozygous for F508DEL-CFTR. Pediatric Pulmonology 2015;50 Suppl 41:269. [ABSTRACT NO.: 211] [CENTRAL: 1092192] [CFGD REGISTER: BD213h/BD214h] [Google Scholar]
- McColley SA, Konstan MW, Ramsey BW, Elborn J, Boyle MP, Wainwright CE, et al. Association between changes in percent predicted FEV1 and incidence of pulmonary exacerbations, including those requiring hospitalization and/ or IV antibiotics, in patients with CF treated with lumacaftor in combination with ivacaftor. Pediatric Pulmonology 2015;50 Suppl 41:282. [ABSTRACT NO.: 241] [CENTRAL: 1092182] [CFGD REGISTER: BD213g/BD214g] [Google Scholar]
- McColley SA, Konstan MW, Ramsey BW, Stuart Elborn J, Boyle MP, Wainwright CE, et al. Lumacaftor/Ivacaftor reduces pulmonary exacerbations in patients irrespective of initial changes in FEV1. Journal of Cystic Fibrosis 2019;18(1):94-101. [CENTRAL: CN-01921335] [CFGD REGISTER: BD213t // BD214t] [EMBASE: 2001047042] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- NCT01807923. A study of lumacaftor in combination with ivacaftor in cystic fibrosis subjects aged 12 Years and older who are homozygous for the F508del-CFTR Mutation (TRAFFIC) [A phase 3, randomized, double blind, placebo controlled, parallel group study to evaluate the efficacy and safety of lumacaftor in combination with ivacaftor in subjects aged 12 years and older with cystic fibrosis, homozygous for the F508del CFTR mutation]. clinicaltrials.gov/ct2/show/NCT01807923 (first posted 08 March 2013). [CLINICALTRIALS.GOV: NCT01807923]
- Seliger V, Bai Y, Volkova N, Tian S, Waltz. Prevalance of cataracts in a population of cystic fibrosis patients homozygous for the F508del mutation. Journal of Cystic Fibrosis 2015;14 Suppl 1:S108. [ABSTRACT NO.: 196] [CENTRAL: 1077208] [CFGD REGISTER: BD213d/BD214c] [Google Scholar]
- Sullivan JC, Accurso FJ, Marigowda G, Beusmans J, Geho D, Zhang E, et al. Combination lumacaftor/ivacaftor therapy improves inflammatory biomarkers in patients with cf homozygous for the f508DEL-CFTR mutations. Pediatric Pulmonology 2016;51 Suppl 45:274. [ABSTRACT NO.: 218] [CFGD REGISTER: BD213n/BD214n ] [Google Scholar]
- Sullivan JC, Accurso FJ, Marigowda G, Beusmans J, Geho D, Zhang E, et al. Improvement in inflammatory biomarkers in patients (pts) wth cystic fibrosis (CF) homozygous for the F508del-CFTR mutation treated with lumacaftor (LUM) and ivacaftor (IVA). Journal of Cystic Fibrosis 2016;15 Suppl 1:S6. [ABSTRACT NO.: WS04.2] [CENTRAL: 1157463] [CFGD REGISTER: BD213k/BD214k] [Google Scholar]
- Suthoff ED, Kosinski M, Sikirica S, Quittner AL, Flume P. Impact of pulmonary exacerbations (PEx) on health-related quality of life (HRQoL) assessed by the Cystic Fibrosis Questionnaire-Revised (CFQ-R) in TRAFFIC and TRANSPORT. Journal of Cystic Fibrosis 2016;15 Suppl 1:S86. [ABSTRACT NO.: 138] [CENTRAL: 1157462] [CFGD REGISTER: BD213j/BD214j] [Google Scholar]
- Wainwright CE, Elborn JS, Ramsey B, Huang X, Marigowda G, Waltz D, et al. Effect of lumacaftor in combination with ivacaftor in patients with cf who are homozygous for F508-CFTR: phase 3 TRAFFIC and TRANSPORT studies. Pediatric Pulmonology 2014;49 Suppl 38:156. [ABSTRACT NO.: S10.3] [CENTRAL: 1383236] [CFGD REGISTER: BD213L/BD214L ] [Google Scholar]
- Wainwright CE, Elborn JS, Ramsey BW, Marigowda G, Huang X, Cipolli M, et al. Lumacaftor-ivacaftor in patients with cystic fibrosis homozygous for Phe508del CFTR. New England Journal of Medicine 2015;373(3):220-31. [CENTRAL: 1067433] [CFGD REGISTER: BD213b/BD214b] [5500133000000031] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
TRANSPORT 2015 {published data only}
- Anstead M, Tupayachi G, Murphy D, Autry E, Bulkley V, Kuhn R. Lumacaftor/ivacaftor: real world experience in a CF center. Pediatric Pulmonology 2016;51 Suppl:302. [CFGD REGISTER: BD213s // BD214s] [Google Scholar]
- De Boeck C. Long-term clinical effects of CFTR co-therapy with Lumacaftor/Ivacaftor. Pediatric Pulmonology 2015;50:135-7. [CENTRAL: 1163954] [CFGD REGISTER: BD214m/BD213m] [EMBASE: 72081237] [SYMPOSIUM SUMMARY: S9.1] [Google Scholar]
- De Boeck K, Elborn J, Ramsey B, Boyle MP, Konstan MW, Huang X, et al. Efficacy and safety of lumacaftor+ivacaftor combination therapy in patients with CF homozygous for F508DEL-CFTR by FEV1 subgroups. Pediatric Pulmonology 2015;50 Suppl 41:283. [ABSTRACT NO.: 245] [CENTRAL: 1092180] [CFGD REGISTER: BD214f/BD213f] [Google Scholar]
- Elborn JS, Ramsey B, Boyle MP, Wainwright C, Konstan M, Huang X, et al. Lumacaftor in combination with ivacaftor in patients with cystic fibrosis who are homozygous for the F508del-CFTR mutation. Journal of Cystic Fibrosis 2015;14 Suppl 1:S1. [ABSTRACT NO.: WS01.3] [CENTRAL: 1077209] [CFDG REGISTER: BD214d/BD213e] [Google Scholar]
- Elborn JS, Ramsey BW, Boyle MP, Konstan MW, Huang X, Marigowda G, et al. Efficacy and safety of lumacaftor/ivacaftor combination therapy in patients with cystic fibrosis homozygous for Phe508del CFTR by pulmonary function subgroup: a pooled analysis. Lancet. Respiratory Medicine 2016;4(8):617-26. [CENTRAL: 1157425] [CFGD REGISTER: BD214i/BD213i] [DOI: 10.1016/S2213-2600(16)30121-7] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elborn JS, Ramsey BW, Boyle MP, Konstan MW, Huang X, Marigowda G, et al. Efficacy and safety of lumacaftor/ivacaftor combination therapy in patients with cystic fibrosis homozygous for Phe508del CFTR by pulmonary function subgroup: a pooled analysis. Lancet. Respiratory Medicine 2016;4(8):617-26. Online supplementary appendix. [CFGD REGISTER: BD214o/BD213o ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elborn JS, Ramsey BW, Boyle MP, Wainwright CE, Konstan MW, Huang X, et al. Lumacaftor/ ivacaftor combination therapy in CF patients homozygous for F508del-CFTR with severe lung dysfunction. Journal of Cystic Fibrosis 2015;14 Suppl 1:S94. [ABSTRACT NO.: 143] [CENTRAL: 1077207] [CFGD REGISTER: BD214d/BD213c] [Google Scholar]
- Flume PA, Suthoff ED, Kosinski M, Marigowda G, Quittner AL. Measuring recovery in health-related quality of life during and after pulmonary exacerbations in patients with cystic fibrosis. Journal of Cystic Fibrosis 2019;18(5):737-42. [CENTRAL: CN-01742131] [CFGD REGISTER: BD213u // BD214u] [DOI: 10.1016/j.jcf.2018.12.004] [EMBASE: 2001400109] [DOI] [PubMed] [Google Scholar]
- Konstan M, McKone E, Moss R, Marigowda G, Cooke J, Lubarsky B, et al. Evidence of reduction in annual rate of FEV1 decline and sustained benefits with lumacaftor and ivacaftor (LUM/IVA) in patients (pts) with cf homozygous for F508DEL-CFTR. Pediatric Pulmonology 2016;51 Suppl 45:260. [ABSTRACT NO: 180] [CFGD REGISTER: BD213p // BD214p] [Google Scholar]
- Konstan MW, Ramsey BW, Elborn J, Boyle MP, Waltz D, Marigowda G, et al. Safety and efficacy of treatments with lumacaftor in combination with ivacaftor in patients with CF homozygous for F508DEL-CFTR. Pediatric Pulmonology 2015;50 Suppl 41:269. [ABSTRACT NO.: 211] [CENTRAL: 1092192] [CFGD REGISTER: BD214h/BD213h] [Google Scholar]
- McColley SA, Konstan MW, Ramsey BW, Elborn J, Boyle MP, Wainwright CE, et al. Association between changes in percent predicted FEV1 and incidence of pulmonary exacerbations, including those requiring hospitalization and/ or IV antibiotics, in patients with CF treated with lumacaftor in combination with ivacaftor. Pediatric Pulmonology 2015;50 Suppl 41:282. [ABSTRACT NO.: 241] [CENTRAL: 1092182] [CFGD REGISTER: BD214g/BD213g] [Google Scholar]
- McColley SA, Konstan MW, Ramsey BW, Stuart Elborn J, Boyle MP, Wainwright CE, et al. Lumacaftor/Ivacaftor reduces pulmonary exacerbations in patients irrespective of initial changes in FEV1. Journal of Cystic Fibrosis 2019;18(1):94-101. [CENTRAL: CN-01921335] [CFGD REGISTER: BD213t // BD214t] [EMBASE: 2001047042] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- NCT01807949. A study of lumacaftor in combination with ivacaftor in cystic fibrosis subjects aged 12 years and older who are homozygous for the F508del-CFTR Mutation (TRANSPORT) [A phase 3, randomized, double blind, placebo controlled, parallel group study to evaluate the efficacy and safety of lumacaftor in combination with ivacaftor in subjects aged 12 years and older with cystic fibrosis, homozygous for the F508del CFTR mutation]. clinicaltrials.gov/ct2/show/NCT01807949 (first posted 08 March 2013). [CLINICALTRIALS.GOV: NCT01807949]
- Ramsey B, Boyle MP, Elborn J, Huang X, Marigowda G, Waltz D, et al. Effect of lumacaftor in combination with ivacaftor in patients with cystic fibrosis who are homozygous for F508DEL-CFTR: TRANSPORT Study. Pediatric Pulmonology 2014;49 Suppl 38:305. [ABSTRACT NO.: 250] [CENTRAL: 1012383] [CFGD REGISTER: BD214a] [Google Scholar]
- Seliger V, Bai Y, Volkova N, Tian S, Waltz. Prevalance of cataracts in a population of cystic fibrosis patients homozygous for the F508del mutation. Journal of Cystic Fibrosis 2015;14 Suppl 1:S108. [ABSTRACT NO.: 196] [CENTRAL: 1077208] [CFGD REGISTER: BD214c/BD213d] [Google Scholar]
- Sullivan JC, Accurso FJ, Marigowda G, Beusmans J, Geho D, Zhang E, et al. Combination lumacaftor/ivacaftor therapy improves inflammatory biomarkers in patients with cf homozygous for the f508DEL-CFTR mutations. Pediatric Pulmonology 2016;51 Suppl 45:274. [ABSTRACT NO.: 218] [CFGD REGISTER: BD214n/BD213n ] [Google Scholar]
- Sullivan JC, Accurso FJ, Marigowda G, Beusmans J, Geho D, Zhang E, et al. Improvement in inflammatory biomarkers in patients (pts) wth cystic fibrosis (CF) homozygous for the F508del-CFTR mutation treated with lumacaftor (LUM) and ivacaftor (IVA). Journal of Cystic Fibrosis 2016;15 Suppl 1:S6. [ABSTRACT NO.: WS04.2] [CENTRAL: 1157463] [CFGD REGISTER: BD214k/BD213k] [Google Scholar]
- Suthoff ED, Kosinski M, Sikirica S, Quittner AL, Flume P. Impact of pulmonary exacerbations (PEx) on health-related quality of life (HRQoL) assessed by the Cystic Fibrosis Questionnaire-Revised (CFQ-R) in TRAFFIC and TRANSPORT. Journal of Cystic Fibrosis 2016;15 Suppl 1:S86. [ABSTRACT NO.: 138] [CENTRAL: 1157462] [CFGD REGISTER: BD214j/BD213j] [Google Scholar]
- Wainwright CE, Elborn JS, Ramsey B, Huang X, Marigowda G, Waltz D, et al. Effect of lumacaftor in combination with ivacaftor in patients with CF who are homozygous for F508-CFTR: phase 3 TRAFFIC and TRANSPORT studies. Pediatric Pulmonology 2014;49 Suppl 38:156. [ABSTRACT NO.: S10.3] [CENTRAL: 1383236] [CFGD REGISTER: BD214L/BD213L ] [Google Scholar]
- Wainwright CE, Elborn JS, Ramsey BW, Marigowda G, Huang X, Cipolli M, et al. Lumacaftor-ivacaftor in patients with cystic fibrosis homozygous for Phe508del CFTR. New England Journal of Medicine 2015;373(3):220-31. [CENTRAL: 1067433] [CFGD REGISTER: BD214b/BD213b] [5500133000000031] [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Zeitlin 2002 {published data only}
- Zeitlin PL, Diener-West M, Rubenstein RC, Boyle MP, Lee CK, Brass-Ernst L. Evidence of CFTR function in cystic fibrosis after systemic administration of 4-phenylbutyrate. Molecular Therapy 2002;6(1):119-26. [CENTRAL: 409030] [CFGD REGISTER: BD148] [PMID: ] [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Berkers 2014 {published data only}
- Berkers G, Vijftigschild L, Bronsveld I, Arets H, Winter-de Groot K, Heijerman H, et al. A beta-2 agonist as a CFTR activator in CF; the ABBA study. Pediatric Pulmonology 2014;49 Suppl 38:299-300. [ABSTRACT NO.: 236] [CENTRAL: 1012380] [CFGD REGISTER: BD212] [Google Scholar]
Chadwick 1998 {published data only}
- Chadwick S, Browning JE, Stern M, Cheng SH, Gruenert DC, Geddes DM, et al. Nasal application of glycerol in DF508 cystic fibrosis patients. Pediatric Pulmonology 1998;Suppl 17:278. [ABSTRACT NO.: 275] [CENTRAL: 208568] [CFGD REGISTER: BD147] [Google Scholar]
Chilvers 2017 {published data only}
- Chilvers M, Davies JC, Ratjen F, Milla C, Owen CA, Tian S, et al. Long-term safety and efficacy of lumacaftor/ivacaftor therapy in patients aged 6-11 years with cystic fibrosis homozygous for the F508del-CFTR mutation (F/F). Journal of Cystic Fibrosis 2019;18 Suppl 1:S23. [ABSTRACT NO.: WS12-4] [CENTRAL: CN-02011205] [CFGD REGISTER: BD232c] [EMBASE: 2001976603] [Google Scholar]
- Chilvers M, Owen C, Marigowda G, Tian S, Solomon M, Black P, et al. Safety and efficacy of lumacaftor/ ivacaftor in patients aged =6 years with cf homozygous for F508DEL-CFTR (phase 3 extension study). Pediatric Pulmonology 2017;52 Suppl 47:319. [CFGD REGISTER: BD232b] [Google Scholar]
- Chilvers M, Tian S, Marigowda G, Bsharat M, Hug C, Solomon M, et al. An open-label extension (EXT) study of lumacaftor/ivacaftor (LIM/IVA) therapy in patients (pts) aged 6-11 years (yrs) with cystic fibrosis (CF) homozygous for F508del-CFTR. Journal of Cystic Fibrosis 2017;16 Suppl 1:S77. [ABSTRACT NO: 52] [CENTRAL: 1383248] [CFGD REGISTER: BD232a] [CLINICALTRIALS.GOV: NCT01897233] [Google Scholar]
- NCT01897233. Study of lumacaftor in combination with ivacaftor in subjects 6 through 11 years of age with cystic fibrosis, homozygous for the F508del-CFTR mutation [A phase 3, open-label study to evaluate the pharmacokinetics, safety, and tolerability of lumacaftor in combination with ivacaftor in subjects 6 through 11 years of age with cystic fibrosis, homozygous for the F508del-CFTR mutation]. clinicaltrials.gov/ct2/show/NCT01897233 (first posted 2013 July 11). [CFGD REGISTER: BD232d] [CLINICALTRIALS.GOV: NCT01897233]
Drevinek 2017 {published data only (unpublished sought but not used)}
- Drevinek P, Pready N, Lamontagne N, Montgomery S, Henig N. QR-010 via inhalation is safe, well tolerated and achieves systemic concentrations in a single ascending dose study in subjects with cystic fibrosis homozygous for the F508del CFTR mutation. Journal of Cystic Fibrosis 2017;16 Suppl 1:S73-4. [CFGD REGISTER: BD244a] [Google Scholar]
- Elborn S, Bouisset F, Checcio T, Perquin J, Lamontagne N, Montgomery S, et al. A first-in-human, phase 1b, dose escalation study of QR-010, a novel antisense oligonucleotide administered in subjects with cystic fibrosis homozygous for the F508del CFTR mutation. Paediatric Pulmonology 2017;52 Suppl 47:289. [CFGD REGISTER: BD244b] [Google Scholar]
Leonard 2012 {published data only}
- Leonard A, Dingemanse J, Lebecque P, Leal T. Oral miglustat in homozygous F508del CF patients. Journal of Cystic Fibrosis 2010;9 Suppl 1:S20. [ABSTRACT NO.: 75] [CENTRAL: 921950] [CFGD REGISTER: BD193a] [Google Scholar]
- Leonard A, Lebecque P, Dingemanse J, Leal T. A randomized placebo-controlled trial of miglustat in cystic fibrosis based on nasal potential difference. Journal of Cystic Fibrosis 2012;11:231-6. [CENTRAL: 840524] [CFGD REGISTER: BD193b] [PMID: ] [DOI] [PubMed] [Google Scholar]
NCT00945347 {published data only}
- NCT00945347. Does a nasal instillation of miglustat normalize the nasal potential difference in cystic fibrosis patients? [Does a nasal instillation of miglustat normalize the nasal potential difference in cystic fibrosis patients homozygous for the F508del mutation? A randomized, double blind placebo-controlled study]. clinicaltrials.gov/show/NCT00945347 (first posted 24 July 2009).
NCT01899105 {published data only}
- NCT01899105. A phase 1 study to investigate the food effect of lumacaftor in combination with ivacaftor [A phase 1, randomized, single-dose, open-label crossover study to investigate the effect of food on the relative bioavailability of 2 fixed-dose combinations of lumacaftor and ivacaftor tablet formulations in healthy adult subjects]. clinicaltrials.gov/show/NCT01899105 (first posted 15 July 2013). [CLINICALTRIALS.GOV: NCT01899105]
NCT03447262 {published data only}
- NCT03447262. A study evaluating the long term safety and efficacy of VX-659 combination therapy. clinicaltrials.gov/ct2/show/NCT03447262 (first posted 27 February 2018).
NCT03525574 {published data only}
- NCT03525574. A study evaluating the long-term safety and efficacy of VX-445 combination therapy. clinicaltrials.gov/ct2/show/NCT03525574 (first posted 15 May 2018).
NCT03537651 {published data only}
- NCT03537651. A study to evaluate the safety and efficacy of long-term treatment with TEZ/IVA in CF subjects with an F508del CFTR mutation. clinicaltrials.gov/ct2/show/NCT03537651 (first posted 25 May 2018).
NCT03601637 {published data only}
- NCT03601637. Safety and pharmacokinetic study of lumacaftor/ivacaftor in subjects 1 to less than 2 years of age with cystic fibrosis, homozygous for F508del. clinicaltrials.gov/ct2/show/NCT03601637 (first posted 26 July 2018).
NCT03633526 {published data only}
- NCT03633526. Evaluation of VX-659/TEZ/IVA in cystic fibrosis subjects 6 through 11 years of age. clinicaltrials.gov/ct2/show/NCT03633526 (first posted 16 August 2018).
NCT03691779 {published data only}
- NCT03691779. Evaluation of VX 445/TEZ/IVA in cystic fibrosis subjects 6 through 11 years of age. clinicaltrials.gov/ct2/show/NCT03691779 (first posted 02 October 2018).
NCT04043806 {published data only}
- NCT04043806. A study evaluating the long-term safety of VX-445 combination therapy. clinicaltrials.gov/ct2/show/NCT04043806 (first posted 02 August 2019).
NCT04058366 {published data only}
- NCT04058366. Study evaluating the long-term safety and efficacy of VX-445 combination therapy. clinicaltrials.gov/ct2/show/NCT04058366 (first posted 15 August 2019).
NCT04105972 {published data only}
- NCT04105972. A study evaluating the efficacy and safety of VX-445/tezacaftor/ivacaftor in cystic fibrosis subjects, homozygous for F508del. clinicaltrials.gov/ct2/show/NCT04105972 (first posted 26 September 2019).
NCT04183790 {published data only}
- NCT04183790. Evaluation of long-term safety and efficacy of VX-445 combination therapy in subjects with cystic fibrosis who are 6 years of age and older. clinicaltrials.gov/ct2/show/NCT04183790 (first posted 03 December 2019).
NCT04235140 {published data only}
- NCT04235140. Long-term safety of lumacaftor/ivacaftor in subjects with cystic fibrosis who are homozygous for F508del and 12 to <24 months of age at treatment initiation. clinicaltrials.gov/ct2/show/NCT04235140 (first posted 21 January 2020).
NCT04362761 {published data only}
- NCT04362761. A study evaluating the long-term safety of elexacaftor combination therapy. clinicaltrials.gov/ct2/show/NCT04362761 (first posted 27 April 2020).
NCT04537793 {published data only}
- NCT04537793. Evaluation of ELX/TEZ/IVA in fFibrosis (CF) subjects 2 through 5 Years. clinicaltrials.gov/ct2/show/NCT04537793 (first posted 03 September 2020).
NCT04545515 {published data only}
- NCT04545515. A study evaluating the long-term safety and efficacy of elexacaftor/tezacaftor/ivacaftor in cystic fibrosis (CF) subjects 6 years and older and F/MF genotypes. clinicaltrials.gov/ct2/show/NCT04545515 (first posted 11 September 2020).
Nick 2014 {published data only}
- Nick JA, Rodman D, St Clair C, Jones MC, Li H, Higgins M, et al. Effect of ivacaftor in patients with cystic fibrosis, residual CFTR function, and FEV1 ≥40% of predicted, N-of-1 study. Pediatric Pulmonology 2014;49 Suppl 38:285. [ABSTRACT NO.: 196] [CENTRAL: 1012379] [CFGD REGISTER: BD211a ] [Google Scholar]
- Nick JA, Rodman D, St Clair C, Jones MC, Li H, Higgins M. Utilization of an "n-of-1" study design to test the effect of ivacaftor in CF patients with residual CFTR function and FEV1 >40% of predicted. Pediatric Pulmonology 2014;49:188-9. [CENTRAL: 1008991] [CFGD REGISTER: BD211b] [EMBASE: 71616032] [Google Scholar]
Rowe 2017 {published data only}
- Chuang C, Rizio A, Loop B, Lekstrom-Himes J, You X, Kosinski M, et al. Effects of tezacaftor/ivacaftor treatment in patients heterozygous for f508del-cftr and a residual function mutation: patient reported outcomes in a phase 3 randomized, controlled trial. Paediatric Pulmonology 2018;53 Suppl 2:S264. [CFGD REGISTER: BD237e] [CTG: ] [DOI: 10.1002/ppul.24152] [DOI] [Google Scholar]
- Chuang C-C, Rizio AA, Loop B, Lekstrom-Himes J, You X, Kosinski M, et al. Effects of tezacaftor/ivacaftor (TEZ/IVA) treatment in patients heterozygous for F508DEL-CFTR and a residual function mutation: patient-reported outcomes in a phase 3 randomized, controlled trial (expand). Thorax 2018;73:A41. [CENTRAL: CN-01934562] [CFGD REGISTER: BD237f] [EMBASE: 627697165] [Google Scholar]
- Fischer R, Rizio AA, Loop B, Lekstrom-Himes J, You X, Kosinski M, et al. Effects of tezacaftor/ivacaftor (TEZ/IVA) treatment in patients heterozygous for F508del-CFTR and a residual function mutation: patient-reported outcomes in a Phase 3, randomised, controlled trial (EXPAND). Pneumologie 2019;73(Suppl 1). [CENTRAL: CN-01960601] [CFGD REGISTER: BD237g] [EMBASE: 628475378] [Google Scholar]
- Fischer R, Rowe SM, Davies JC, Nair N, Han L, Lekstrom-Himes J. Efficacy and safety of tezacaftor/ivacaftor in patients (Pts) aged >= 12 Years with CF heterozygous for F508del and a residual function mutation: a randomized, double-blind, placebo-controlled, crossover phase 3 study. Pneumologie 2018;72 Suppl 1:S35. [CFGD REGISTER: BD237d] [DOI: 10.1055/s-0037-1619210] [NCT: 02392234] [DOI] [Google Scholar]
- Ingenito E, Nair N, Yi B, Lekstrom-Himes J, Elborn JS, Rowe SM. Retrospective analysis of physiological response patterns to tezacaftor/ivacaftor in patients with cystic fibrosis homozygous for F508DEL-CFTR or heterozygous for F508DEL-CFTR and a residual function mutation. Thorax 2018;73(Suppl 4):A42-3. [CFGD REGISTER: BD237h] [DOI: 10.1136/thorax-2018-212555.75] [DOI] [Google Scholar]
- NCT02392234. A phase 3 study to evaluate the efficacy and safety of ivacaftor and VX-661 in combination with ivacaftor in subjects aged 12 years and older with cystic fibrosis, heterozygous for the f508del-cystic fibrosis transmembrane conductance regulator (CFTR) mutation [A phase 3, randomized, double-blind, placebo-controlled, crossover study to evaluate the efficacy and safety of ivacaftor and VX-661 in combination with ivacaftor in subjects aged 12 years and older with cystic fibrosis, heterozygous for the f508del-cftr mutation, and a second allele with a CFTR mutation predicted to have residual function]. clinicaltrials.gov/show/NCT02392234 (first received 18 March 2015). [CENTRAL: CN-02040467] [CFGD REGISTER: BD237i]
- Rowe SM, Daines C, Ringshausen FC, Kerem E, Wilson J, Tullis E, et al. Tezacaftor-ivacaftor in residual-function heterozygotes with cystic fibrosis. New England Journal of Medicine 2017;377(21):2024-35. [CFGD REGISTER: BD237c] [CLINICALTRIALS.GOV: NCT02392234] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rowe SM, Davies J. CFTR modulation with tezacaftor/ivacaftor in patients heterozygous for F508del and a residual function mutation. Pediatric Pulmonology 2017;52 Suppl 47:175-6. [CFGD REGISTER: BD237a] [CLINICALTRIALS.GOV: NCT02392234] [Google Scholar]
- Rowe SM, Davies JC, Nair N, Han L, Lekstrom-Himes J. Efficacy and safety of tezacaftor/ ivacaftor and ivacaftor in patients aged >=12 years with cf heterozygous for f508del and a residual function mutation: a randomized, double-blind, placebo-controlled, crossover phase 3 study. Pediatric Pulmonology 2017;52 Suppl 47:317. [CFGD REGISTER: BD237b] [CLINICALTRIALS.GOV: NCT02392234] [Google Scholar]
Rubenstein 2006 {published data only}
- Rubenstein RC, Propert KJ, Reenstra WW, Skotleski ML. A pilot trial of the combination of phenylbutyrate and genistein. Pediatric Pulmonology 2006;41 Suppl 29:294. [ABSTRACT NO.: 248] [CENTRAL: 593141] [CFGD REGISTER: BD149] [Google Scholar]
Sumner 2014 {published data only}
- Sumner Jones SG, Alton EW, Boyd A, Chang SH, Davies JC, Davies LA, et al. Molecular analyses of vector delivery and gene expression in a multidose trial of non-viral gene therapy in patients with CF. Pediatric Pulmonology 2014;49 Suppl 38:302. [ABSTRACT NO.: 243] [CENTRAL: 1012381] [CFGD REGISTER: BD210b] [Google Scholar]
- Waller MD, Harman KM, Boyd A, Chang SH, Gill DR, Griesenbach U, et al. Measurement of CFTR function in cystic fibrosis patients in response to multidose CFTR gene therapy. Pediatric Pulmonology 2014;49 Suppl 38:249. [ABSTRACT NO.: 97] [CENTRAL: 1012378] [CFGD REGISTER: BD210a] [Google Scholar]
Ziady 2015 {published data only}
- Ziady AG, Lin S, Heltshe SL, Kelley T, Muhlebach MS, Accurso FJ, et al. Protein expression in CF primary airway epithelia following treatment with VX-809 reveals significant changes in pkc-mediated signalling, proton and iron transport, and lipid metabolism. Pediatric Pulmonology 2015;50 Suppl 41:300. [ABSTRACT NO.: 290] [CENTRAL: 1092203] [CFGD REGISTER: BD225] [Google Scholar]
References to studies awaiting assessment
Downey 2019 {published data only}
- Downey D, Flume P, Jain M, Fajac I, Schwarz C, Pressler T, et al. Initial results evaluating combinations of the novel CFTR corrector PTI-801, potentiator PTI-808, and amplifier PTI-428 in cystic fibrosis subjects. Journal of Cystic Fibrosis 2019;18 Suppl 1:S10. [CENTRAL: CN-01990618] [CFGD REGISTER: BD269a] [EMBASE: 2001976571] [Google Scholar]
- Flume P, Downey DG, Jain M, Fajac I, Schwarz C, Pressler T, et al. Evaluation of novel CFTR modulator combinations of the corrector PTI-801, potentiator PTI-808, and amplifier PTI-428 in CF subjects. Pediatric Pulmonology 2019;54 Suppl 2:348. [CENTRAL: CN-01989480] [CFGD REGISTER: BD269c] [EMBASE: 629387551] [Google Scholar]
- Jain M, Pilewski J, Flume P, Taylor-Cousar J, Rowe S, Milla C, et al. Initial results evaluating the add-on effect of the novel CFTR corrector PTI-801 in cystic fibrosis subjects. Journal of Cystic Fibrosis 2019;18 Suppl 1:S10-1. [CENTRAL: CN-02007011] [CFGD REGISTER: BD269b] [EMBASE: 2001976532] [Google Scholar]
EudraCT 2019‐000750‐63 {published data only}
- EudraCT 2019-000750-63. A phase 2 study of ABBV-3067 alone and in combination with ABBV-2222 in cystic fibrosis subjects who are homozygous for the F508del mutation. www.clinicaltrialsregister.eu/ctr-search/search?query=2019-000750-63 (first posted 31 October 2019).
Hunt 2017 {published data only}
- Hunt K, St Clair C, Curran-Everett D, Solomon GM, Saavedra MT, Nick JA, et al. CFTR effects of oral sildenafil in combination with lumacaftor/ivacaftor in adults with CF. Pediatric Pulmonology 2017;52(Suppl 47):322. [CFGD REGISTER: IB117] [Google Scholar]
Munck 2020 {published data only}
- Munck A, Kerem E, Ellemunter H, Campbell D, Wang LT, Ahluwalia N, et al. Tezacaftor/ivacaftor in people with cystic fibrosis heterozygous for minimal function CFTR mutations. Journal of Cystic Fibrosis 2020 Jun 13 [epub ahead of print];S1569-1993(20):30128-4. [CENTRAL: CN-02142331] [CFGD REGISTER: BD274b] [DOI: 10.1016/j.jcf.2020.04.015] [EMBASE: 2006729203] [PMID: ] [DOI] [PubMed] [Google Scholar]
- NCT02516410. A study to evaluate the efficacy and safety of VX-661 in combination with ivacaftor in subjects aged 12 years and older with cystic fibrosis, heterozygous for the F508del-CFTR mutation. clinicaltrials.gov/ct2/show/NCT02516410 first posted 05 August 2015. [CFGD REGISTER: BD274a]
NCT02951195 {published data only}
- NCT02951195. A study evaluating the safety of VX-152 combination therapy in adults with cystic fibrosis [A phase 2, randomized, double blind, controlled study to evaluate the safety of VX-152 combination therapy in adults with cystic fibrosis]. clinicaltrials.gov/ct2/show/NCT02951195 (first posted 01 November 2016).
NCT03447249 {published data only}
- NCT03447249. A phase 3, randomized, double-blind, controlled study evaluating the efficacy and safety of VX-659 combination therapy in subjects with cystic fibrosis who are heterozygous for the F508del mutation and a minimal function mutation (F/MF). clinicaltrials.gov/ct2/show/NCT03447249 (first posted 27 February 2018). [EUDRACT NUMBER: 2017-004132-11]
NCT03460990 {published data only}
- NCT03460990. A study of VX-659 combination therapy in CF subjects homozygous for F508del (F/F). clinicaltrials.gov/ct2/show/NCT03460990 (first posted 09 March 2018). [EUDRACT NUMBER: 2017-004133-82]
NCT03768089 {published data only}
- EudraCT 2018-000126-55. A phase 1/2 Study of VX-121 in healthy subjects and in subjects with cystic fibrosis. www.clinicaltrialsregister.eu/ctr-search/search?query=2018-000126-55 (first posted 15 March 2018).
- NCT03768089. Study of VX-121 in healthy subjects and in subjects with cystic fibrosis. clinicaltrials.gov/ct2/show/NCT03768089 (first posted 07 December 2018). [2018-000126-55 ( EudraCT Number )]
NCT03911713 {published data only}
- NCT03911713. A phase 2 study to evaluate efficacy and safety of VX-561 in subjects aged 18 years and older with cystic fibrosis. clinicaltrials.gov/ct2/show/NCT03911713 (first posted 11 April 2019). [EUDRACT NUMBER: 2018-003970-28]
NCT03912233 {published data only}
- EUCTR2018-002496-18-PT. A study to evaluate the safety and efficacy of VX-121 combination therapy in subjects with cystic fibrosis [A phase 2, randomized, double-blind, controlled study to evaluate the safety and efficacy of VX-121 combination therapy in subjects aged 18 years and older with cystic fibrosis]. www.who.int/trialsearch/Trial2.aspx?TrialID=EUCTR2018-002496-18-PT (first received 2019). [CENTRAL: CN-02068097] [CFGD REGISTER: BD277b]
- NCT03912233. A study to evaluate the safety and efficacy of VX-121 combination therapy in subjects with cystic fibrosis [A phase 2, randomized, double-blind, controlled study to evaluate the safety and efficacy of VX-121 combination therapy in subjects aged 18 years and older with cystic fibrosis]. clinicaltrials.gov/show/NCT03912233 (first received 11 April 2019). [CENTRAL: CN-01912167] [CFGD REGISTER: BD277a]
NCT04058353 {published data only}
- NCT04058353. A phase 3 study of VX-445 combination therapy in cystic fibrosis (CF) subjects heterozygous for F508del and a gating or residual function mutation (F/G and F/RF genotypes). clinicaltrials.gov/ct2/show/NCT04058353 (first posted 15 August 2019). [EUDRACT NUMBER: 2018-002835-76]
NCT04353817 {published data only}
- NCT04353817. A study evaluating efficacy and safety of elexacaftor/tezacaftor/ivacaftor in subjects 6 through 11 years of age with cystic fibrosis and F/MF genotypes. clinicaltrials.gov/ct2/show/NCT04353817 (first posted 20 April 2020). [EUDRACT NUMBER: 2019-003554-86]
PELICAN {published data only}
- EUCTR2017-002181-42-DE. GLPG2737 on top of Orkambi in subjects with cystic fibrosis [A Phase IIa, randomized, double-blind, placebo-controlled study to evaluate GLPG2737 in Orkambi-treated subjects with cystic fibrosis homozygous for the F508del mutation]. www.who.int/trialsearch/Trial2.aspx?TrialID=EUCTR2017-002181-42-DE (first received 2017). [CENTRAL: CN-01887243] [CFGD REGISTER: BD272b]
- NCT03474042. GLPG2737 on top of orkambi in subjects with cystic fibrosis [A phase iia, randomized, double-blind, placebo-controlled study to evaluate GLPG2737 in orkambi-treated subjects with cystic fibrosis homozygous for the f508del mutation]. clinicaltrials.gov/show/NCT03474042 (first received 2018 March 22). [CFGD REGISTER: BD272a]
- Koningsbruggen-Rietschel S, Conrath K, Fischer R, Sutharsan S, Kempa A, Gleiber W, et al. GLPG2737 in lumacaftor/ivacaftor-treated CF subjects homozygous for the F508del mutation: a randomized phase 2A trial (PELICAN). Journal of Cystic Fibrosis 2020;19(2):292-8. [CENTRAL: CN-01999311] [CFGD REGISTER: BD272c] [EMBASE: 2003281625] [PMID: ] [DOI] [PubMed] [Google Scholar]
Rio‐CF {published data only (unpublished sought but not used)}
- Derichs N, Taylor-Cousar J, Tullis E, Davies J, Nazareth D, Downey DG, et al. Safety, tolerability and early signs of efficacy with riociguat for the treatment of adult phe508del homozygous cystic fibrosis patients: study design and rationale for the Rio-CF study. Journal of Cystic Fibrosis 2017;16 Suppl 1:S36. [CFGD REGISTER: BD246b] [Google Scholar]
- NCT02170025. Early signs of efficacy study with riociguat in adult homozygous delta F508 cystic fibrosis patients [Multi-center phase 2 study to assess the safety, tolerability and early signs of efficacy of tid orally administered BAY63-2521 in adult delta F508 homozygous cystic fibrosis patients]. clinicaltrials.gov/ct2/show/results/NCT02170025 (first posted 23 June 2014).
- Taylor-Cousar JL, Tullis E, Derichs N, Davies JC, Nazareth D, Downey R, et al. Riociguat for the treatment of adult phe508del homozygous cystic fibrosis: efficacy data from the phase II Rio-CF study. Journal of Cystic Fibrosis 2018;17 Suppl 3:S67. [CFGD REGISTER: BD246a] [DOI] [PubMed] [Google Scholar]
Taylor‐Cousar 2019 {published data only}
- Taylor-Cousar J, Gifford AH, Flume P, Sawicki GS, Pilewski JM, Jain M, et al. Initial results evaluating the first-in-class CFTR amplifier, PTI-428, in subjects with CF on background treatment with tezacaftor/ ivacaftor. Pediatric Pulmonology 2019;54 Suppl 2:332. [CENTRAL: CN-01988388] [CFGD REGISTER: BD270] [EMBASE: 629388001] [Google Scholar]
Wainwright 2019 {published data only}
- Wainwright C, Stick S, Goldin J, Lekstrom-Himes J, Wang L, Campbell D, et al. Change in low-dose chest computed tomography (CT) scores after 72 weeks of tezacaftor/ivacaftor (TEZ/IVA) in patients (pts) with cystic fibrosis and ppFEV1 >=70%: an exploratory phase 2 study. Journal of Cystic Fibrosis 2019;18 Suppl 1:S11-2. [CENTRAL: CN-02009338] [CFGD REGISTER: BD275] [EMBASE: 2001976227] [Google Scholar]
References to ongoing studies
ALBATROSS {published data only (unpublished sought but not used)}BD247
- Bell S, De Boeck K, Drevinek P, Plant B, Barry P, Elborn S, et al. GLPG2222 in subjects with cystic fibrosis and the F508del/Class III mutation on stable treatment with ivacaftor: results from a phase II study (ALBATROSS). Journal of Cystic Fibrosis 2018;17 Suppl 3:S2. [ABSTRACT NO.: WS01.4] [CFGD REGISTER: BD247a] [Google Scholar]
- Bell S, De Boeck K, Drevinek P, Plant B, Barry P, Elborn S, et al. Results from a phase II study- ALBATROSS - evaluation of GLPG2222 in subjects with CF and the F508del/class III mutation on stable treatment with ivacaftor. Pediatric Pulmonology 2018;53 Suppl 2:249. [ABSTRACT NO.: 269] [CFGD REGISTER: BD247b] [Google Scholar]
- Bell SC, Barry PJ, De Boeck K, Drevinek P, Elborn JS, Plant BJ, et al. CFTR activity is enhanced by the novel corrector GLPG2222, given with and without ivacaftor in two randomized trials. Journal of Cystic Fibrosis 2019;18(5):700-7. [CENTRAL: CN-01936893] [CFGD REGISTER: BD247c // BD254c] [DOI: 10.1016/j.jcf.2019.04.014] [EMBASE: 2001903987] [PMID: ] [DOI] [PubMed] [Google Scholar]
- NCT03045523. A study to evaluate GLPG2222 in ivacaftor-treated subjects with cystic fibrosis. clinicaltrials.gov/ct2/show/NCT03045523 (first posted 07 February 2017). [STUDY NO.: GLPG2222-CL-201]
FLAMINGO {published data only (unpublished sought but not used)}
- Bell SC, Barry PJ, De Boeck K, Drevinek P, Elborn JS, Plant BJ, et al. CFTR activity is enhanced by the novel corrector GLPG2222, given with and without ivacaftor in two randomized trials. Journal of Cystic Fibrosis 2019;18(5):700-7. [DOI: 10.1016/j.jcf.2019.04.014] [DOI] [PubMed] [Google Scholar]
- NCT03119649. A study to evaluate multiple doses of GLPG2222 in adult subjects with cystic fibrosis. clinicaltrials.gov/ct2/show/NCT03119649 (first posted 18 April 2017). [STUDY NO.: GLPG2222-CL-202]
- Ent KC, Minic P, Verhulst S, Van Brackel E, Flume P, Boas S, et al. GLPG2222 in subjects with cystic fibrosis homozygous for F508del: results from a phase II study (FLAMINGO). Journal of Cystic Fibrosis 2018;17 Suppl 3:S42. [ABSTRACT NO.: EPS3.05 ] [CFGD REGISTER: BD254a] [Google Scholar]
- Ent KC, Minic P, Verhulst S, Van Brackel E, Flume P, Boas S, et al. GLPG2222 in subjects with cystic fibrosis homozygous for F508del: results from a phase II study (FLAMINGO). Pediatric Pulmonology 2018;53 Suppl 2:250. [ABSTRACT NO.: 271] [CFGD REGISTER: BD254b] [Google Scholar]
Jain 2018 {published data only (unpublished sought but not used)}
- Jain M, Flume P, Escobar H, Taylor-Cousar JL, Pressler T, Liou TG, et al. Initial results evaluating third generation CFTR corrector PTI-801 in CF subjects. Paediatric Pulmonology 2018;53 Suppl 2:246. [CFGD REGISTER: BD257] [Google Scholar]
Meijer 2016 {published data only}
- Meijer L, Hery-Arnaud G, Le Berre R, Nowak E, Le Roux L, Gueganton L, et al. Rosco-CF, a safety and efficacy clinical trial of (R)-roscovitine in CF patients. Journal of Cystic Fibrosis 2016;15 Suppl 1:S42. [ABSTRACT NO.: ePS03.7] [CENTRAL: 1157464] [CFGD REGISTER: BD230a] [Google Scholar]
- Meijer L, Hery-Arnaud G, Le Berre R, Nowak E, Le Roux L, Gueganton L, et al. ROSCO-CF, a safety and efficacy clinical trial of (r)-roscovitine in CF patients. Pediatric Pulmonology 2016;51 Suppl 45:269. [CFGD REGISTER: BD230b] [Google Scholar]
- Meijer L, Hery-Arnaud G, Le Berre R, Nowak E, Rault G, Mottier D. ROSCO-CF, a safety and efficacy clinical trial of (R)-roscovitine in cystic fibrosis patients. Journal of Cystic Fibrosis 2018;17 Suppl 3:S25. [CFGD REGISTER: BD230c] [Google Scholar]
- NCT02649751. Evaluation of (R)-roscovitine safety and effects in subjects with cystic fibrosis, homozygous for the F508del-CFTR mutation (ROSCO-CF) [A phase II, dose ranging, multicenter, double-blind, placebo controlled study to evaluate safety and effects of (R)-Roscovitine in adults subjects with cystic fibrosis, carrying 2 cystic fibrosis causing mutations with at least one F508del-CFTR mutation and chronically infected with Pseudomonas aeruginosa, a study involving 36 CF patients (24 treated, 12 controls). ROSCO-CF]. clinicaltrials.gov/ct2/show/NCT02649751 (first posted 07 January 2016).
NCT02070744 {published data only}
- NCT02070744. Study to evaluate safety and efficacy of VX-661 in combination with ivacaftor in subjects with cystic fibrosis, homozygous for the F508del-CFTR mutation with an open-label expansion [A phase 2, randomized, multicenter, double blind, placebo controlled study to evaluate safety, efficacy, pharmacokinetics, and pharmacodynamics of VX-661 in combination with ivacaftor for 12 weeks in subjects with cystic fibrosis, homozygous for the F508del CFTR mutation with an open-label extension]. clinicaltrials.gov/ct2/show/NCT02070744 (first posted 25 February 2014). [CLINICALTRIALS.GOV: NCT02070744]
NCT02323100 {published data only}
- NCT02323100. Glycerol phenylbutyrate corrector therapy for CF (Cystic Fibrosis) (GPBA) [A double blind, placebo controlled, dose escalation trial of glycerol phenylbutyrate corrector therapy for cystic fibrosis]. clinicaltrials.gov/ct2/show/NCT02323100 (first posted 23 December 2014).
NCT02412111 {published data only}
- NCT02412111. A phase 3 study of VX-661 in combination with ivacaftor in subjects aged 12 years and older with cystic fibrosis, who have one F508del-CFTR mutation and a second mutation that has been demonstrated to be clinically responsive to ivacaftor [A phase 3, randomized, double-blind, Ivacaftor-controlled, parallel-group study to evaluate the efficacy and safety of VX-661 in combination with ivacaftor in subjects aged 12 years and older with cystic fibrosis, heterozygous for the F508del-CFTR mutation and a second CFTR allele with a gating defect that Is clinically demonstrated to be ivacaftor responsive]. clinicaltrials.gov/ct2/show/NCT02412111 (first posted 08 April 2015).
NCT02589236 {published data only}
- NCT02589236. Study of cavosonstat (N91115) in patients with CF homozygous for the F508del-CFTR mutation (SNO-6) [A phase 2, randomized, double-blind, placebo-controlled, parallel-group study of N91115 to evaluate efficacy and safety in patients with cystic fibrosis who are homozygous for the F508del-CFTR mutation treated with lumacaftor/ivacaftor]. clinicaltrials.gov/ct2/show/NCT02589236 (first posted 28 October 2015).
NCT02718495 {published data only}
- NCT02718495. Study assessing PTI-428 safety, tolerability, and pharmacokinetics in subjects with cystic fibrosis [A phase I/II, multi-center, randomized, placebo-controlled, study designed to assess the safety, tolerability, and pharmacokinetics of PTI-428 in subjects with cystic fibrosis]. clinicaltrials.gov/ct2/show/NCT02718495 (first posted 24 March 2016).
NCT02730208 {published data only}
- NCT02730208. A study to evaluate the effect of VX-661 in combination with ivacaftor on chest imaging endpoints in subjects with cystic fibrosis, homozygous for the F508del CFTR mutation [A phase 2, randomized, placebo-controlled, double-blind study to evaluate the effect of VX-661 in combination with ivacaftor on chest imaging endpoints in subjects aged 12 years and older with cystic fibrosis, homozygous for the F508del CFTR mutation]. clinicaltrials.gov/ct2/show/NCT02730208 (first posted 06 April 2016).
NCT03258424 {published data only}
- NCT03258424. Study assessing PTI-428 safety, tolerability, and pharmacokinetics in subjects with cystic fibrosis on KALYDECO® as background therapy [A phase I, randomized, placebo-controlled, study designed to assess the safety, tolerability, and pharmacokinetics of PTI-428 in subjects with cystic fibrosis]. clinicaltrials.gov/ct2/show/NCT03258424 (first posted 23 August 2017).
NCT03559062 {published data only}
- NCT03559062. A study to evaluate efficacy and safety of tez/iva in subjects aged 6 through 11 years with cystic fibrosis [A phase 3, double-blind, parallel-group study to evaluate the efficacy and safety of tezacaftor in combination with ivacaftor in subjects aged 6 through 11 years with cystic fibrosis, homozygous or heterozygous for the F508del-CFTR mutation]. clinicaltrials.gov/ct2/show/NCT03559062 (first posted 15 June 2018).
NCT03625466 {published data only}
- EUCTR2017-003761-99-DE. A study of the effects of lumacaftor/ivacaftor on disease progression in subjects aged 2 through 5 years with cystic fibrosis, homozygous for f508del [An exploratory phase 2, 2-part, randomized, double blind, placebo controlled study with a long term, open label period to explore the impact of lumacaftor/ivacaftor on disease progression in subjects aged 2 through 5 years with cystic fibrosis, homozygous for f508del]. www.who.int/trialsearch/Trial2.aspx?TrialID=EUCTR2017-003761-99-DE (first received 2018). [CENTRAL: CN-01908852] [CFGD REGISTER: BD276b]
- NCT03625466. A study to explore the impact of lumacaftor/ivacaftor on disease progression in subjects aged 2 through 5 years with cystic fibrosis, homozygous for f508del [An exploratory phase 2, 2-part, randomized, double-blind, placebo-controlled study with a long-term, open-label period to explore the impact of lumacaftor/ivacaftor on disease progression in subjects aged 2 through 5 years with cystic fibrosis, homozygous for f508del]. clinicaltrials.gov/show/NCT03625466 (first received 10 August 2018). [CENTRAL: CN-01626171] [CFGD REGISTER: BD276a]
Schwarz 2020 {published data only}
- NCT03150719. A study to evaluate safety, efficacy, and tolerability of TEZ/IVA in Orkambi® (lumacaftor/ivacaftor) - experienced subjects with cystic fibrosis (CF) [Phase 3b, randomized, double-blind, placebo-controlled, parallel group study to assess the safety, efficacy, and tolerability of tezacaftor/ivacaftor (TEZ/IVA) in an Orkambi-experienced population who are homozygous for the F508del CFTR mutation]. clinicaltrials.gov/ct2/show/NCT03150719 (first posted 12 May 2017). [CFGD REGISTER: BD273a]
- Schwarz C, Sutharsan S, Epaud R, Klingsberg R, Fischer R, Rowe SM, et al. Safety, efficacy, and tolerability of tezacaftor/ivacaftor in cystic fibrosis patients who previously discontinued lumacaftor/ivacaftor due to respiratory adverse events: a randomized, double-blind, placebo-controlled phase 3b study. Pneumologie 2019;73(Suppl 1). [CENTRAL: CN-01960602] [CFGD REGISTER: BD273b] [EMBASE: 628475379] [Google Scholar]
- Schwarz C, Sutharsan S, Epaud R, Klingsberg RC, Fischer R, Rowe SM, et al. Tezacaftor/ivacaftor in people with cystic fibrosis who stopped lumacaftor/ivacaftor due to respiratory adverse events. Journal of Cystic Fibrosis 2020 Jun 23 [epub ahead of print];S1569-1993(20):30730-X. [CENTRAL: CN-02143375] [CFGD REGISTER: BD273c] [DOI: 10.1016/j.jcf.2020.06.001] [EMBASE: 2006829285] [PMID: ] [DOI] [PMC free article] [PubMed]
Additional references
Amaral 2007
- Amaral MD, Kunzelmann K. Molecular targeting of CFTR as a therapeutic approach to cystic fibrosis. Trends in Pharmacological Sciences 2007;28(7):334-41. [DOI] [PubMed] [Google Scholar]
Aslam 2017
- Aslam AA, Higgins C, Sinha IP, Southern KW. Ataluren and similar compounds (specific therapies for premature termination codon class I mutations) for cystic fibrosis. Cochrane Database of Systematic Reviews 2017, Issue 1. Art. No: CD012040. [DOI: 10.1002/14651858.CD012040.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Bobadilla 2002
- Bobadilla JL, Macek M, Fine JP, Farrell PM. Cystic fibrosis: a worldwide analysis of CFTR mutations - correlation with incidence data and application to screening. Human Mutation 2002;19(6):575-606. [DOI] [PubMed] [Google Scholar]
CFMD 2013
- Cystic Fibrosis Centre at the Hospital for Sick Children in Toronto, Canada. Cystic fibrosis mutation database. www.genet.sickkids.on.ca/app (accessed 23 September 2013).
Colledge 1995
- Colledge WH, Abella BS, Southern KW, Ratcliff R, Jiang C, Cheng SH, et al. Generation and characterization of a delta F508 cystic fibrosis mouse model. Nature Genetics 1995;10(4):445-52. [DOI] [PubMed] [Google Scholar]
Deeks 2011
- Deeks JJ, Higgins JP, Altman DG. Chapter 9: Analysing data and undertaking meta-analysis. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
EMA 2012
- European Medicines Agency. Report of the workshop on endpoints for cystic fibrosis clinical trials (EMA/769571/2012); November 2012. Available at www.ema.europa.eu/docs/en_GB/document_library/Report/2012/12/WC500136159.pdf.
Higgins 2003
- Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ 2003;327(7414):557-60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2011a
- Higgins JP, Altman DG, editor(s). Chapter 8: Assessing risk of bias in included studies. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Higgins 2011b
- Higgins JP, Deeks JJ, Altman DG on behalf of the CSMG . Chapter 16: Special topics in statistics. In: Higgins JP, Green S, editor(s). Cochrane Handbook of Systematic Reviews of Interventions. Version 5.1 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
NICE 2016
- Lumacaftor–ivacaftor for treating cystic fibrosis homozygous for the F508del mutation. www.nice.org.uk/guidance/ta398 (accessed 01 September 2020).
Parmar 1998
- Parmar MK, Torri V, Stewart L. Extracting summary statistics to perform meta-analyses of the published literature for survival endpoints. Statistics in Medicine 1998;17:2815-34. [DOI] [PubMed] [Google Scholar]
Quittner 2009
- Quittner AL, Modi AC, Wainwright C, Otto K, Kirihara J, Montgomery AB. Determination of the minimal clinically important difference scores for the Cystic Fibrosis Questionnaire-Revised respiratory symptom scale in two populations of patients with cystic fibrosis and chronic Pseudomonas aeruginosa airway infection. Chest 2009;135(6):1610-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ramsey 2011
- Ramsey BW, Davies J, McElvaney NG, Tullis E, Bell SC, Dřevínek P, et al. A CFTR potentiator in patients with cystic fibrosis and the G551D mutation. New England Journal of Medicine 2011;365(18):1663-72. [DOI] [PMC free article] [PubMed] [Google Scholar]
Riordan 1989
- Riordan JR, Rommens JM, Kerem BS, Alon N, Rozmahel R, Grzelczak Z, et al. Identification of the cystic fibrosis gene – cloning and characterization of complementary. Science 1989;245(4922):1066-72. [DOI] [PubMed] [Google Scholar]
Rogan 2011
- Rogan MP, Stoltz DA, Hornick DB. Cystic fibrosis transmembrane conductance regulator intracellular processing, trafficking, and opportunities for mutation-specific treatment. Chest 2011;139(6):1480-90. [DOI: 10.1378/chest.10-2077] [DOI] [PubMed] [Google Scholar]
Rowntree 2003
- Rowntree RK, Harris A. The phenotypic consequences of CFTR mutations. Annals of Human Genetics 2003;67(5):471-85. [DOI] [PubMed] [Google Scholar]
Rubenstein 1997
- Rubenstein RC, Egan ME, Zeitlin PL. In vitro pharmacologic restoration of CFTR-mediated chloride transport with sodium 4-phenylbutyrate in cystic fibrosis epithelial cells containing delta F508-CFTR. Journal of Clinical Investigation 1997;100(10):2457–65. [DOI] [PMC free article] [PubMed] [Google Scholar]
Skilton 2019
- Skilton M, Krishan A, Patel S, Sinha IP, Southern KW. Potentiators (specific therapies for class III and IV mutations) for cystic fibrosis. Cochrane Database of Systematic Reviews 2019, Issue 1. Art. No: CD009841. [DOI: 10.1002/14651858.CD009841.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
Southern 1997
- Southern KW. Delta F508 in cystic fibrosis: willing but not able. Archives of Disease in Childhood 1997;76(3):278-82. [DOI] [PMC free article] [PubMed] [Google Scholar]
Southern 2007
- Southern KW. Cystic fibrosis and formes frustes of CFTR-related disease. Respiration: International Review of Thoracic Diseases 2007;74(3):241-51. [DOI] [PubMed] [Google Scholar]
Van Goor 2011
- Van Goor F, Hadida S, Grootenhuis PD, Burton B, Stack JH, Straley KS, et al. Correction of the F508del-CFTR protein processing defect in vitro by the investigational drug VX-809. Proceedings of the National Academy of Sciences of the United States of America 2011;108(46):18843-8. [DOI: 10.1073/pnas.1105787108] [DOI] [PMC free article] [PubMed] [Google Scholar]
Williamson 2002
- Williamson PR, Tudur Smith C, Hutton JL, Marson AG. Aggregate data meta-analysis with time-to-event outcomes. Statistics in Medicine 2002;21(11):3337-51. [DOI] [PubMed] [Google Scholar]
Wu 2018
- Wu HX, Zhu M, Xiong XF, Wei J, Zhuo KQ, Cheng DY. Efficacy and safety of CFTR corrector and potentiator combination therapy in patients with cystic fibrosis for the F508del-CFTR homozygous mutation: a systematic review and meta-analysis. Advances in Therapy 2018;36(2):451-61. [DOI: 10.1007/s12325-018-0860-4] [PMID: ] [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Southern 2018
- Southern KW, Patel S, Sinha IP, Nevitt SJ. Correctors (specific therapies for class II CFTR mutations) for cystic fibrosis. Cochrane Database of Systematic Reviews 2018, Issue 8. Art. No: CD010966. [DOI: 10.1002/14651858.CD010966.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]