

CLINICAL HISTORY
A 15 year old boy presented to our center with progressive headache, vomiting, gait instability and reduced visual acuity of one month's duration. The patient related a head injury as a result of a fall while playing hockey as coinciding with the onset of his symptoms but no other significant history. Physical examination revealed severe bilateral papilledema.
RADIOLOGY
CT demonstrated marked hydrocephalus involving the lateral and third ventricles. T2 (figure 1) and FLAIR (figure 2) MRI revealed the inferior tectum, aqueduct and superior fourth ventricle to be obliterated by a 1.6 × 1.8 × 2 cm mass and associated 2 × 2 × 2.5 cm cyst. The solid portion displayed minimal enhancement (figure 3 pre‐gadolinium; 4, 5, 6, post‐gadolinium). Imaging features favored an ependymoma or low grade astrocytoma.
Figure 1.
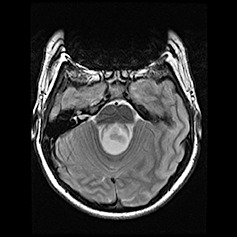
Figure 2.
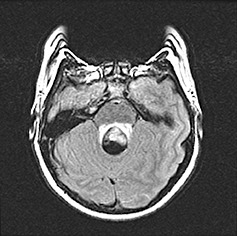
Figure 3.
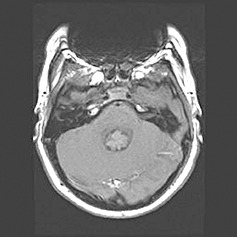
Figure 4.
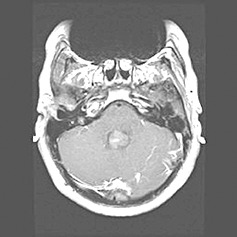
Figure 5.
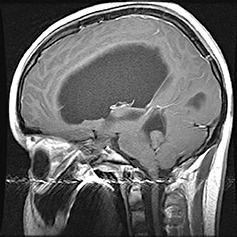
Figure 6.

MACROSCOPIC DESCRIPTION
Surgical excision of the mass found it to be obstructing the sylvian aqueduct. The grey to tan colored fleshy mass was completely resected from the ventricular system and sent for pathological examination.
MICROSCOPIC DESCRIPTION
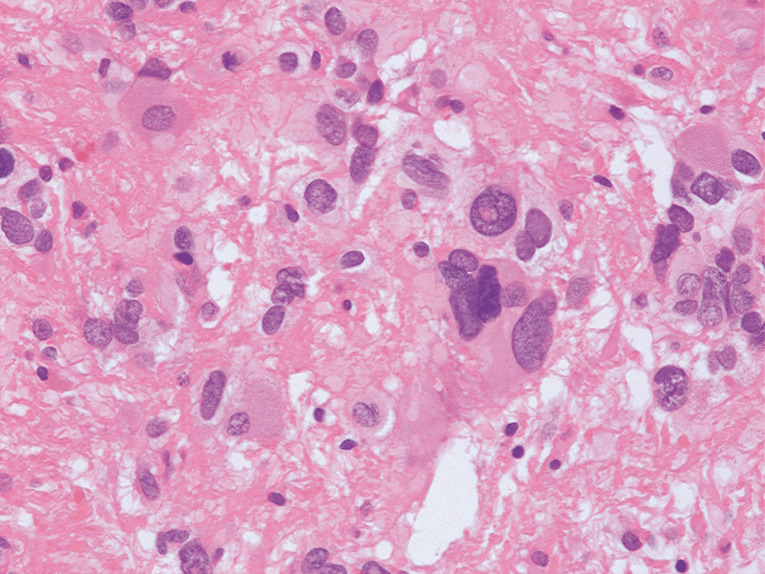
Microscopic examination of the resected tumor revealed a highly pleomorphic and fibrillary lesion (7, 8). Lesional cells varied from pilar to multipolar to giant with multiple and pleomorphic nuclei. Many tumor cells had prominent cytoplasmic vacuolation and/or fine granular brown pigment (figure 8). Perivascular lymphocytes and sparse eosinophilic granular bodies were present. No mitotic activity, endothelial hyperplasia or necrosis were seen.
Figure 7.
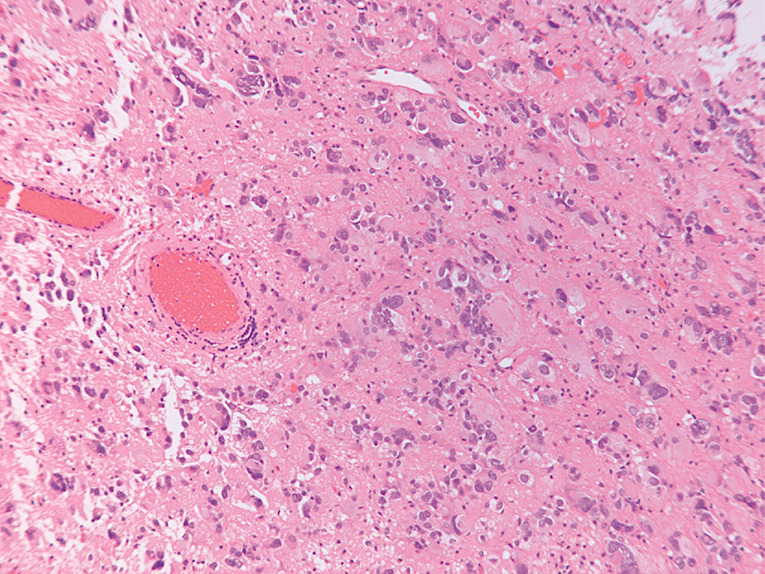
Figure 8.
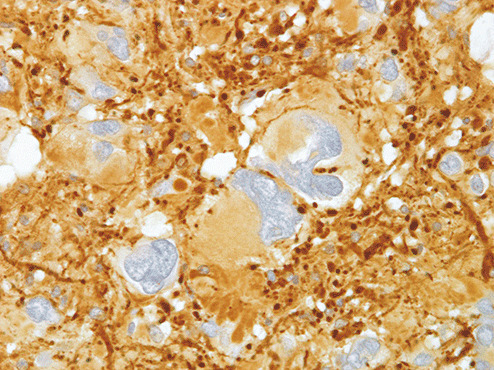
The granular brown cytoplasmic pigment stained black with Masson‐Fontana preparation (figure 9). Gomori and Sweet's reticulin stain revealed generous reticulin surrounding individual cells or groups of cells (figure 10). The neoplastic cells expressed abundant GFAP (figure 11) and select cells lightly coexpressed synaptophysin and neurofilament. Ki‐67 labeling was sparse (below 1% in 10 random fields).
Figure 9.
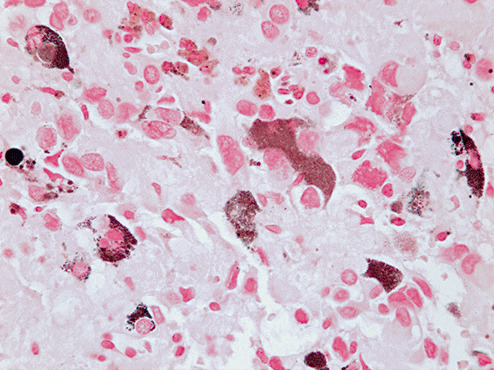
Figure 10.
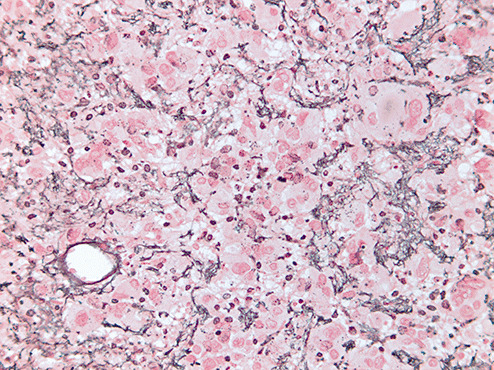
Figure 11.
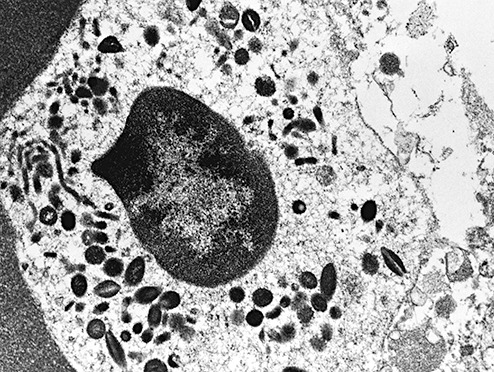
Ultrastructural studies confirmed the presence of melanosomes within the tumor cells (figure 12).
Figure 12.
DIAGNOSIS
Pigmented Pleomorphic Xanthoastrocytoma.
DISCUSSION
Pleomorphic Xanthoastrocytomas (PXA) account for less than 1% of astrocytic neoplasms (10). PXAs most commonly affect those in their first and second decades, and typically present with seizures. More than 98% of PXAs are found supratentorially (1). Imaging usually reveals the tumor mass and associated cyst. Tumors are most often superficial with meningeal attachment (10). Typical histological features include cytoplasmic and nuclear pleomorphism, variable xanthomatous change, reticulin fibers surrounding cells, eosinophilic granular bodies and collections of perivascular lymphocytes. Mitotic figures are usually absent or sparse and Ki‐67 labelling is <1% (10).
PXAs are considered to be of glial origin with tumor cells expressing GFAP and S‐100 protein. PXAs frequently harbor select cells which variably express neuronal markers including synaptophysin, neurofilament, NeuN, MAP2, and class III B tubulin (2).
PXAs are uncommon but well known WHO grade II tumors with a generally favorable prognosis; survival is reported as 81% at 5 years (10). Malignant progression is, however, reported to occur in up to 20% of cases (6). The present case was of added interest for its atypical location and for being one of only three pigmented examples reported. The two previously reported cases of pigmented PXA were suprasellar and medial temporal in location 5, 7. Although the tumor cells expressed abundant GFAP, select cells expressed neuronal markers synaptophysin and neurofilament suggesting that PXAs may be neuroglial in nature 2, 3.
The feature of particular interest in the present case was the presence of melanin. Examples of pigmented primary tumors are well documented with pigments including neuromelanin, melanin and lipofuscin. Five melanotic astrocytic tumors have been previously reported: two were PXAs, one had PXA‐like features, one was a ganglioglioma with PXA as the astrocytic component and one was a pilocytic astrocytoma 4, 5, 7, 8, 9. In the present case, Masson‐Fontana preparations and ultrastructural examination confirmed the pigment to be melanosomal melanin. Of the five previously reported melanotic tumors, all but the pilocytic astrocytoma, were also found to contain melanosomal melanin as their pigment 5, 7.
The present case is the third pigmented PXA to be reported, adding to a small collection of melanotic gliomas. While melanin production in gliomas is a curious finding, its prognostic significance is uncertain. In a twelve year follow up of one pigmented PXA there was no recurrence (5). In the present case there is no evidence of recurrence on MRI one year post‐operatively.
ABSTRACT
A 15 year old male presented with hydrocephalus from a tectal mass obstructing the cerebral aqueduct and upper fourth ventricle. The solid‐cystic partly enhancing mass proved to be a pigmented pleomorphic xanthoastrocytoma, the third such example reported. The lesion revealed typical features of a PXA with the unusual addition of intracytoplasmic melanin in select lesional cells. Melanin pigment production is uncommon in glial tumors and of uncertain significance. The present case is recurrence‐free one year post‐operatively.
REFERENCES
- 1. Giannini C, Paulus W, Louis DN, Liberski P (2000) Pleomorphic xanthoastrocytoma. In: Pathology and Genetics of Tumors of the Nervous System, Kleihues P, Cavanee WK (eds), pp. 22–24, IARC Press: Lyon. [Google Scholar]
- 2. Giannini C, Scheithauer BW, Lopes MB, Hirose T, Kros JM, VandenBerg SR (2002) Immunophenotype of pleomorphic xanthoastrocytoma. Am J Surg Pathol 26:479–485. [DOI] [PubMed] [Google Scholar]
- 3. Im SH, Chung CK, Kim SK, Cho BK, Kim MK, Chi JG (2004) Pleomorphic xanthoastrocytoma: A developmental glioneuronal tumor with prominent glioproliferative changes. J Neurooncol 66:17–27. [DOI] [PubMed] [Google Scholar]
- 4. Kanzawa T, Takahashi H, Hayano M, Mori S, Shimbo Y, Kitazawa T (1997) Melanotic cerebral astrocytoma: Case report and literature review. Acta Neuropathol 93:200–204. [DOI] [PubMed] [Google Scholar]
- 5. Krossnes BK, Mella O, Wester K, Mork SJ (2004) Pigmented astrocytoma with suprasellar location: Case report and literature review. Acta Neuropathol 108:461–466. [DOI] [PubMed] [Google Scholar]
- 6. Marton E, Feletti A, Orvieto E, Longatti P (2007) Malignant progression in pleomorphic xanthoastrocytoma: Personal experience and review of the literature. J Neurol Sci 252:144–153. [DOI] [PubMed] [Google Scholar]
- 7. Sharma MC, Arora R, Khanna N, Singh VP, Sarkar C (2001) Pigmented pleomorphic xanthoastrocytoma: Report of a rare case with review of the literature. Arch Pathol Lab Med 125:808–811. [DOI] [PubMed] [Google Scholar]
- 8. Soffer D, Lach B, Constantini S (1992) Melanotic cerebral ganglioglioma: Evidence for melanogenesis in neoplastic astrocytes. Acta Neuropathol 83:315–323. [DOI] [PubMed] [Google Scholar]
- 9. Vajtai I, Yonekawa Y, Schauble B, Paulus W (1996) Melanotic astrocytoma. Acta Neuropathol 91:549–553. [DOI] [PubMed] [Google Scholar]
- 10. Walker DG, Kaye AH (2003) Low grade glial neoplasms. J Clin Neurosci 10:1–13. [DOI] [PubMed] [Google Scholar]