

Abstract
Children’s sleep quality and duration are important to overall development, health, and wellbeing. However, measuring children’s sleep is challenging, especially in situations where objective assessment is impractical. This study aimed to assess age and proxy effects in comparing subjective sleep duration with objective measures, in a community-based sample of Wisconsin children (aged 6–17 years), recruited from 2014–2017. The sample participants had a mean age of 11.4 (standard deviation, 3.3) years and 52% of them were male. We used linear mixed effects models to test for age effects in proxy- and self-report groups separately, and a quasiexperimental regression discontinuity approach to compare subjective sleep duration with objective actigraphy estimates across proxy- and self-report groups. We found evidence of systematic overestimation of sleep duration when using subjective measurements but did not find evidence of age effects in either group. Based on these analyses, we found evidence of differential overestimation by proxy- or self-report condition. Proxy reporters overestimated sleep duration by 2.3 hours (95% confidence interval: 2.2, 2.4), compared with 1.0 hour (95% confidence interval: 0.7, 1.2) for self-reporters. These findings suggest that proxy- versus self-reporting conditions are an important consideration when designing a study, and that it might be beneficial to reduce the age at which children self-report.
Keywords: accelerometry, minor, proxy, sleep, validity
Abbreviations
- BMI
body mass index
- CI
confidence interval
- SHOW
Survey of the Health of Wisconsin
For children, sleep is a vital feature of health and wellbeing that affects multiple aspects of development. Insufficient sleep duration and quality have been linked with obesity, metabolic disorders, poor memory, and poor school performance (1, 2). Thus, it is important for health researchers and clinicians to accurately assess sleep duration and quality in children, in order to intervene and understand the broad-reaching causes and effects of poor sleep.
Many epidemiologic studies assess sleep using questionnaires, including in pediatric populations (3). Although using accelerometry-measured sleep is attractive because of its reduced susceptibility to recall and other biases, there are settings in which subjective measures are preferred due to logistical or cost constraints, especially in long-duration (e.g., months or years) longitudinal studies.
Among adults, most sleep questionnaires have been found to be biased and only moderately correlated with objective measurements (3). Less is known about self-reported sleep for children and young adults. Subjective measurements of children’s sleep are further complicated by the potential need for a proxy reporter, depending on the age of the child. The usefulness of proxy-reported sleep duration is not clear. Previous studies have found that proxies can satisfactorily estimate sleep start and stop times but are unable to estimate sleep duration because they cannot accurately estimate time that a child spent awake during the night (4). In studies on children’s ability to self-report sleep, previous findings indicate that children can accurately estimate some variables relating to quality of sleep and sleep start and stop times, but there is little evidence that children can accurately self-report sleep duration (5, 6).
While the previous body of research gives insight into the validity of subjective sleep measurements, age effects and the relationship between proxy reporting and the validity of subjective sleep measurements have not been studied in detail. This study’s aims were to assess age effects in both proxy- (younger children) and self-report (older children) groups and to compare measures of subjective sleep duration with objective measures across self- or proxy-report conditions. We estimated the age effects on the difference between subjective and objective sleep measurements in the proxy- and self-report groups separately. We then used a regression discontinuity approach to identify the effect that proxy reporting has on the difference between subjective and objective assessments of sleep. In addressing our aims, we treated actigraphy-assessed sleep as the reference standard, but we acknowledge that it is not a gold standard for validly and accurately measuring sleep behaviors; polysomnography is generally considered a gold standard, but it is not a feasible approach for capturing multiple nights of sleep in large population samples. Although not the gold standard, several studies have demonstrated that actigraphy is an acceptable substitute for polysomnography (7–9).
METHODS
Study population
The data used in this analysis were collected by the Survey of the Health of Wisconsin (SHOW). SHOW is a statewide public health survey of Wisconsin residents, which annually collects information on health behaviors and neighborhood characteristics, biological samples, and physical measurements. Detailed methods have been previously published (10). Beginning in 2014, minors were included in the SHOW sample population. All children who lived in a selected household were eligible to participate; our data set contained participants from 255 unique households. The data used in this analysis were collected between 2014 and 2017, from children who were 6–17 years old. Participants’ mean age was 11.4 (standard deviation, 3.3) years (range, 6–17 years). Of the sample, 52% of the participants were male. SHOW protocol and informed consent documents were approved by the University of Wisconsin–Madison Health Sciences Institutional Review Board. Informed consent of a parent/guardian was obtained on behalf of all minors, and minors were asked for informed assent. There were 572 minors asked to participate in accelerometry measurement. Of those, 42 refused and 51 were removed from the sample due to device error, leaving 479 minors.
Proxies responded to surveys on behalf of minors who were under 12 years old. Any household member who was a legal parent/guardian of the child could be a proxy; if there was more than one eligible proxy, household members chose who would act as the proxy. Children 12 years or older responded to some survey questions for themselves, including those on sleep behaviors.
Objective sleep duration
Participants wore wrist accelerometers (ActiGraph WGT3X-BT; ActiGraph Corporation, Pensacola, Florida) for up to 7 consecutive days to measure their sleep duration. They were asked to wear the monitor continuously, except for any activities that would get the monitor wet. Participants or proxies filled out a log indicating any periods that they did not wear the accelerometer, the time that they went to bed, and the time that they got out of bed.
Data were aggregated into 60-second epochs for validation, scoring, and analysis. In-bed and out-bed times were identified manually based on activity recorded by the ActiGraph and the logs filled out by participants. The Sadeh algorithm was used to distinguish sleeping and waking periods during time spent in bed (11). On average, participants who consented to participate in accelerometry wore the device for 6.8 days (95% confidence interval (CI): 6.7, 6.9).
Average overall, weekday, and weekend sleep durations were calculated for participants who wore the accelerometer for at least 1 weeknight and 1 weekend night. Of the 479 participants, 421 recorded at least 1 weekday and 1 one weekend night. There were 7 participants who did not respond to subjective sleep questions, resulting in an analytical sample of 414 children. Overall sleep duration was calculated as a weighted average: (5 × average weeknight duration + 2 × average weekend duration) / 7. Weeknights were Sunday through Thursday, and weekend nights were Friday and Saturday.
Objective time in bed
Objective time in bed included all time that the participant was physically in bed, regardless of whether they were awake or asleep. This includes the initial time that the participant took to fall asleep (sleep latency), and wake after sleep onset, which is the time that was spent awake during the night between initial sleep onset and waking.
Subjective sleep duration
Subjective sleep duration was collected by asking minors or proxies about typical sleep patterns. Participants aged 12 years or older were asked, “On a typical work or school day, over the past month, how many hours and minutes do you think you actually slept?” and “On a typical NON-work or non-school day, over the past month, how many hours and minutes do you think you actually slept?” to estimate their typical sleep duration on both school days (usually weekdays) and nonschool days (usually weekend). For participants under the age of 12, proxies were asked, “What is your child’s usual bedtime on weeknights/weekends?” and “What time does your child usually wake up on weekdays/weekends?” Children 12 years or older were asked questions about actual time spent sleeping, while proxies were asked about minors’ time spent in bed. While these 2 measures of sleep duration are not identical, they are often used interchangeably to estimate sleep duration (12–14).
Other information
Children’s weight was measured using a calibrated digital scale and height was measured in duplicate using a stadiometer during an in-home interview by a trained interviewer. These values (the average of 2 measures for height) were used to calculate the child’s body mass index (BMI) age- and sex-specific percentile based on the protocols of the US Centers for Disease Control and Prevention (15).
For all participants, an adult in the household was asked to report on the total household income before taxes in the past 12 months. Household income is reported as the total household income divided by the number of people (children included) who were supported by the household income in the past 12 months.
Households were classified as urban/rural using the US 2010 Census urbanized areas and urban cluster classification. In our analyses, we consider both urbanized clusters and urbanized areas to be urban, and all other areas to be rural (16).
Race and ethnicity were determined via proxy report for all children. For this analysis, race and ethnicity were categorized as non-Hispanic Black, non-Hispanic White, Hispanic, or other.
Data analysis
We used linear mixed effects models to estimate age effects on the validity of subjective sleep measurements, stratified by proxy status and with random intercepts and robust variance estimates to account for household-level effects for participants from the same household. In the regression analyses that were adjusted for demographic characteristics, participants with missing information on sex, age, race/ethnicity, per-person household income, rural/urban status, or BMI were not included, resulting in an analytical data set with 386 observations.
This study’s design also allowed us to use a regression discontinuity approach, which is a quasiexperimental design that can be used to estimate average treatment effects when randomization into treatment and control groups is not possible. The approach uses exogenous characteristics of the treatment to estimate causal effects, by comparing those who were nearly sorted into the treatment group with those who were nearly sorted to the control group, based on the underlying forcing variable, which assigns participants to treatment groups (17).
In this analysis, the treatment is proxy versus self-reporting, which was assigned based on participants’ age, with a sharp discontinuity at 12 years. Participants younger than 12 years had a proxy report on their behalf, while those 12 years or older self-reported. Age is an especially good candidate for a forcing variable because there is no risk that participants can manipulate age around the cutoff, especially because age was ascertained prior to revealing the self- versus proxy-report condition. Regression discontinuity analyses were not adjusted for other variables because, within a narrow age range (i.e., the bandwidth of the regression discontinuity), assignment to proxy or self-report should be as good as random, because the assignment is determined by age, and age is exogenous to other factors in the “neighborhood” of the discontinuity. We tested whether this assumption is justified by comparing characteristics of the sample within the local bandwidth, stratified by proxy status.
Several regression discontinuity analyses were conducted to assess the validity of self- and proxy reports of sleep duration. We assessed the validity of the subjective sleep reports by comparing them with the objective accelerometer measures, using accelerometry as the reference standard for comparison. Participants who were missing sleep duration estimates could not be included in the regression discontinuity analyses, but missingness of other demographic variables did not affect inclusion in this part of the analyses. As a robustness check, we performed multiple imputation on the missing data and found that imputation of missing data did not significantly affect our results. Results of these analyses can be found in Web Tables 1 and 2 (available at https://doi.org/10.1093/aje/kwaa254).
Descriptive statistics were calculated using base R (R Foundation for Statistical Computing, Vienna, Austria). All regression discontinuity analyses were performed in R, using the Regression Discontinuity Estimation package (18). Bandwidth, or the number of years on either side of the discontinuity to use in the local linear regression, was determined using the Imbens-Kalyanaraman optimal bandwidth for local linear regression (19).
RESULTS
Table 1 shows the descriptive characteristics of participants, stratified by proxy- and self-report group. Participants had a proxy report on their behalf if they were aged 6 years to less than 12 years. On average, participants with a proxy reporter were 8.9 years old (95% CI: 8.7, 9.1). Participants aged 12–17 years self-reported subjective sleep duration. Self-reporters were on average 14.7 years old (95% CI: 14.4, 14.9). Sex, race/ethnicity, BMI percentile, household income, and urban/rural distribution were similar across proxy- and self-report categories, indicating that the 2 groups were not substantially different on any measures other than their age, which was by design.
Table 1.
Descriptive Sample Characteristics, Stratified by Proxy- or Self-Report Status, Survey of the Health of Wisconsin, 2014–2017
| Characteristic | Proxy Reported (n = 235) | Self-Reported (n = 179) | ||||||
|---|---|---|---|---|---|---|---|---|
| Mean | 95% CI | No. | % | Mean | 95% CI | No. | % | |
| Age, years | 8.9 | 8.7, 9.1 | 14.7 | 14.4, 14.9 | ||||
| Sex | ||||||||
| Male | 122 | 52 | 93 | 52 | ||||
| Female | 113 | 48 | 86 | 48 | ||||
| Race/ethnicity | ||||||||
| White | 183 | 78 | 131 | 73 | ||||
| Black | 26 | 11 | 25 | 14 | ||||
| Hispanic | 9 | 4 | 13 | 7 | ||||
| Other | 17 | 7 | 10 | 6 | ||||
| BMI percentile | 63.3 | 59.5, 67.0 | 62.1 | 57.7, 66.5 | ||||
| Household income per person, $ | 18,413 | 16,691, 20,135 | 20,698 | 18,604, 22,792 | ||||
| Urban/Rural | ||||||||
| Rural | 76 | 32 | 63 | 35 | ||||
| Urban | 151 | 64 | 109 | 61 | ||||
| Missing | 8 | 3 | 7 | 4 | ||||
| Self- or proxy- rated health | ||||||||
| Excellent | 116 | 49 | 73 | 41 | ||||
| Very good | 92 | 39 | 75 | 42 | ||||
| Good | 22 | 9 | 22 | 12 | ||||
| Fair | 3 | 1 | 6 | 3 | ||||
| Missing | 2 | 1 | 3 | 2 | ||||
| Objective sleep duration per night, hours | 7.8 | 7.7, 7.9 | 7.3 | 7.1, 7.4 | ||||
| Objective weekday sleep | 7.8 | 7.7, 7.9 | 7.1 | 6.9, 7.3 | ||||
| Objective weekend sleep | 7.7 | 7.6, 7.9 | 7.7 | 7.4, 8.0 | ||||
| Objective average wake after sleep onset, hours | 1.3 | 1.3, 1.4 | 1.1 | 1.0, 1.2 | ||||
| Objective average sleep latency, minutes | 4.8 | 4.3, 5.3 | 4.0 | 3.5, 4.6 | ||||
| Objective average time spent in bed, hours | 9.2 | 9.1, 9.3 | 8.5 | 8.3, 8.6 | ||||
| Subjective sleep duration per night, hours | 10.1 | 10.0, 10.2 | 8.2 | 8.0, 8.4 | ||||
| Subjective weekday sleep | 10.0 | 9.9, 10.1 | 7.9 | 7.7, 8.1 | ||||
| Subjective weekend sleep | 10.2 | 10.0, 10.3 | 9.0 | 8.7, 9.2 | ||||
Abbreviations: BMI, body mass index; CI, confidence interval.
Children aged 6 years to less than 12 years had a mean objective sleep duration of 7.8 hours (95% CI: 7.7, 7.9), and children aged 12–17 years had a mean objective sleep duration of 7.3 hours (95% CI: 7.1, 7.4).
Table 2 summarizes the differences between subjective and objective sleep duration. Both proxy- and self-report groups’ subjective sleep duration estimates were larger than the objective measurements—full week, weekday only, and weekend only (i.e., reported sleep duration was systematically greater than accelerometry-assessed sleep duration). Proxy-reported subjective sleep duration was larger than objective sleep by 2.3 hours (95% CI: 2.2, 2.4), while self-reported subjective sleep duration was greater than objective sleep duration by 1.0 hour (95% CI: 0.7, 1.2). The discrepancy between subjective and objective weekend sleep duration was larger than weekday sleep duration for both proxy- and self-report groups, with the proxy-report group’s subjective estimate larger than the objective estimate by 2.5 hours (95% CI: 2.3, 2.7) and the self-reported group’s by 1.3 hours (95% CI: 0.9, 1.7) compared with 2.2 hours (95% CI: 2.1, 2.3) and 0.8 hours (95% CI: 0.6, 1.1), respectively, on weekdays. However, when comparing subjective sleep with objective time in bed, the proxy-report group’s subjective estimates were larger on average by 0.8 hours (95% CI: 0.7, 0.9), while the self-report group’s subjective estimate was less than objectively measured time in bed by 0.2 hours (12 minutes) (95% CI: −0.5, 0.003 hours—or 30 minutes and 0.2 minutes).
Table 2.
Difference Between Subjective and Objective Sleep on All Days, Weekdays Only, and Weekends Only, Stratified by Proxy- and Self-Report Status, Survey of the Health of Wisconsin, 2014–2017
| Sleep Measure | Proxy Reported | Self-Reported | ||
|---|---|---|---|---|
| Mean | 95% CI | Mean | 95% CI | |
| Subjective minus objective sleep duration, hours | 2.3 | 2.2, 2.4 | 1.0 | 0.7, 1.2 |
| Subjective minus objective sleep duration (weekday only) | 2.2 | 2.1, 2.3 | 0.8 | 0.6, 1.1 |
| Subjective minus objective sleep duration (weekend only) | 2.5 | 2.3, 2.7 | 1.3 | 0.9, 1.7 |
| Subjective sleep duration minus objective time in bed, hours | 0.8 | 0.7, 0.9 | −0.2 | −0.5, 0.003 |
Abbreviation: CI, confidence interval.
Table 3 shows the results of linear mixed effects models used to estimate the age effects on the difference between subjective and objective sleep duration estimates, stratified by proxy status. We did not find strong evidence of an age effect on the difference between subjective and objective sleep duration in either group.
Table 3.
Estimation of Age Effects on Subjective Minus Objective Sleep Duration (Hours) for All Days, Using Linear Mixed Effects Model With Random Intercepts Accounting for Clustering by Household, With Proxy Status and Demographic Variables, Survey of the Health of Wisconsin, 2014–2017
| Proxy Reported | Self-Reported | |||||||
|---|---|---|---|---|---|---|---|---|
| Characteristic | Model 1 | Model 2 | Model 1 | Model 2 | ||||
| Estimate | 95% CI | Estimate | 95% CI | Estimate | 95% CI | Estimate | 95% CI | |
| Age, years | −0.04 | −0.1, 0.03 | −0.04 | −0.1, 0.03 | −0.05 | −0.2, 0.1 | −0.07 | −0.2, 0.09 |
| Sex | ||||||||
| Male | 0.06 | −0.2, 0.3 | −0.09 | −0.6, 0.4 | ||||
| Female | 0.00 | Referent | 0.00 | Referent | ||||
| Race/Ethnicity | ||||||||
| White | 0.00 | Referent | 0.00 | Referent | ||||
| Black | −0.3 | −0.7, 0.2 | 0.7 | −0.06, 1.6 | ||||
| Hispanic | 0.08 | −0.6, 0.7 | −0.7 | −1.7, 0.3 | ||||
| Other | −0.1 | −0.6, 0.4 | −1.2 | −2.3, −0.2 | ||||
| Household income per person, per $1,000 | −0.005 | −0.01, 0.005 | 0.003 | −0.02, 0.02 | ||||
| Rural/urban status | ||||||||
| Rural | −0.2 | −0.5, 0.1 | −0.5 | −1.0, 0.09 | ||||
| Urban | 0.00 | Referent | 0.00 | Referent | ||||
| BMI percentile | 0.003 | −0.0007, 0.008 | 0.002 | −0.007, 0.01 | ||||
Abbreviations: BMI, body mass index; CI, confidence interval.
Table 4 shows the results of the linear mixed effects model used to estimate the age effects on the difference between subjective and objective sleep duration estimates for weekdays only, and Table 5 shows the results for weekends only. After stratification by weekday or weekend nights, we still did not find strong evidence of an age effect.
Table 4.
Estimation of Age Effects on Subjective Minus Objective Sleep Duration (Hours) for Weekdays Only, Using Linear Mixed Effects Model With Random Intercepts Accounting for Clustering by Household, With Proxy Status and Demographic Variables, Survey of the Health of Wisconsin, 2014–2017
| Proxy Reported | Self-Reported | |||||||
|---|---|---|---|---|---|---|---|---|
| Characteristic | Model 1 | Model 2 | Model 1 | Model 2 | ||||
| Estimate | 95% CI | Estimate | 95% CI | Estimate | 95% CI | Estimate | 95% CI | |
| Age | −0.06 | −0.1, 0.005 | −0.06 | −0.1, 0.004 | −0.1 | −0.2, 0.05 | −0.1 | −0.3, 0.04 |
| Sex | ||||||||
| Male | 0.1 | −0.1, 0.3 | 0.01 | −0.5, 0.5 | ||||
| Female | 0.00 | Referent | 0.00 | Referent | ||||
| Race/ethnicity | ||||||||
| White | 0.00 | Referent | 0.00 | Referent | ||||
| Black | −0.5 | −1.0, −0.1 | 1.0 | 0.2, 1.8 | ||||
| Hispanic | 0.2 | −0.5, 0.8 | −0.8 | −1.8, 0.2 | ||||
| Other | 0.07 | −0.4, 0.5 | −0.9 | −2.0, 0.2 | ||||
| Household income per person, per $1,000 | −0.002 | −0.01, 0.008 | 0.004 | −0.02, 0.02 | ||||
| Rural/urban status | ||||||||
| Rural | 0.00 | Referent | 0.00 | Referent | ||||
| Urban | −0.2 | −0.4, 0.1 | −0.4 | −1.0, 0.1 | ||||
| BMI percentile | 0.004 | −0.0005, 0.008 | 0.001 | −0.007, 0.01 | ||||
Abbreviations: BMI, body mass index; CI, confidence interval.
Table 5.
Estimation of Age Effects on Subjective Minus Objective Sleep Duration (Hours) for Weekends Only, Using Linear Mixed Effects Model With Random Intercepts Accounting for Clustering by Household, With Proxy Status and Demographic Variables, Survey of the Health of Wisconsin, 2014–2017
| Proxy Reported | Self-Reported | |||||||
|---|---|---|---|---|---|---|---|---|
| Characteristic | Model 1 | Model 2 | Model 1 | Model 2 | ||||
| Estimate | 95% CI | Estimate | 95% CI | Estimate | 95% CI | Estimate | 95% CI | |
| Age, years | 0.02 | −0.09, 0.1 | 0.02 | −0.09, 0.1 | 0.08 | (−0.1, 0.3) | 0.04 | −0.2, 0.3 |
| Sex | ||||||||
| Male | −0.1 | −0.5, 0.3 | −0.3 | −1.1, 0.4 | ||||
| Female | 0.00 | Referent | 0.0 | Referent | ||||
| Race/ethnicity | ||||||||
| White | 0.00 | Referent | 0.00 | Referent | ||||
| Black | 0.4 | 0.3, 1.2 | 0.1 | −1.1, 1.4 | ||||
| Hispanic | −0.3 | −1.3, 0.8 | −0.6 | −2.0, 0.9 | ||||
| Other | −0.6 | −1.4, 0.3 | −2.2 | −3.8, −0.6 | ||||
| Household income per person, per $1,000 | −0.01 | −0.03, 0.005 | 0.003 | −0.03, 0.03 | ||||
| Rural/urban status | ||||||||
| Rural | −0.2 | −0.7, 0.3 | −0.6 | −1.4, 0.3 | ||||
| Urban | 0.00 | Referent | 0.00 | Referent | ||||
| BMI percentile | 0.003 | −0.004, 0.01 | 0.003 | −0.01, 0.02 | ||||
Abbreviations: BMI, body mass index; CI, confidence interval.
Table 6 shows the results of linear mixed effects regression when time spent in bed is used as the objective comparison with subjective sleep duration. We also did not find strong evidence of an age effect in the difference between time in bed and subjective sleep duration after stratifying on proxy status.
Table 6.
Estimation of Age Effects on Subjective Minus Objective Time in Bed (Hours) Using Linear Mixed Effects Model With Random Intercepts Accounting for Clustering by Household, With Proxy Status and Demographic Variables, Survey of the Health of Wisconsin, 2014–2017
| Proxy Reported | Self-Reported | |||||||
|---|---|---|---|---|---|---|---|---|
| Characteristic | Model 1 | Model 2 | Model 1 | Model 2 | ||||
| Estimate | 95% CI | Estimate | 95% CI | Estimate | 95% CI | Estimate | 95% CI | |
| Age, years | 0.02 | −0.04, 0.07 | 0.01 | −0.05, 0.08 | −0.05 | −0.2, 0.1 | −0.05 | −0.2, 0.1 |
| Sex | ||||||||
| Male | −0.03 | −0.2, 0.2 | −0.4 | −0.9, 0.1 | ||||
| Female | 0.00 | Referent | 0.00 | Referent | ||||
| Race/ethnicity | ||||||||
| White | 0.00 | Referent | 0.00 | Referent | ||||
| Black | −0.2 | −0.6, 0.2 | 0.6 | −0.2, 1.4 | ||||
| Hispanic | −0.06 | −0.7, 0.5 | −0.9 | −1.8, 0.07 | ||||
| Other | −0.06 | −0.5, 0.4 | −0.9 | −1.9, 0.1 | ||||
| Household income per person, per $1,000 | −0.008 | −0.02, 0.002 | −0.00005 | −0.02, 0.02 | ||||
| Rural/urban status | ||||||||
| Rural | −0.3 | −0.6, −0.06 | −0.4 | −1.0, 0.1 | ||||
| Urban | 0.0 | Referent | 0.00 | Referent | ||||
| BMI percentile | 0.003 | −0.0008, 0.007 | −0.003 | −0.01, 0.006 | ||||
Abbreviations: BMI, body mass index; CI, confidence interval.
Figure 1 shows the regression discontinuity results for total weekly sleep duration comparing the subjective and objective measures with 95% confidence bands. The optimal bandwidth was estimated to be 4.1 years and the estimated discontinuity was −1.0 hours (P = 0.007). Thus, while both proxy and self-reporters overestimated sleep duration, proxy reporters yielded an approximately 1.0-hour larger discrepancy compared with self-reporters. As a robustness check for bandwidth choice, we also estimated the discontinuity using half of the optimal bandwidth (2.1 years on either side of the discontinuity). The discontinuity was −0.9 hours (P = 0.1).
Figure 1.
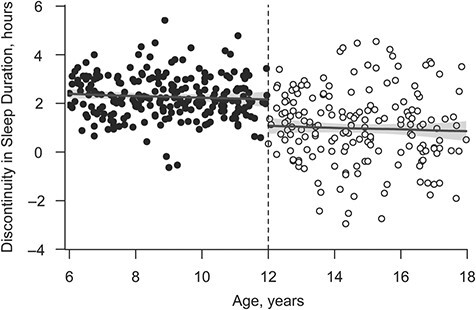
Regression discontinuity results for subjective minus objective sleep duration, with discontinuity in proxy- versus self-report status at age 12 years, Survey of the Health of Wisconsin, 2014–2017.
Figure 2 shows the regression discontinuity results for the weekday measurements of subjective and objective sleep. The optimal bandwidth was estimated to be 4.0 years and the estimated discontinuity between proxy and self-reporters was −0.9 hours (P = 0.01), and a similar magnitude of difference was found using a 2.0-year bandwidth.
Figure 2.
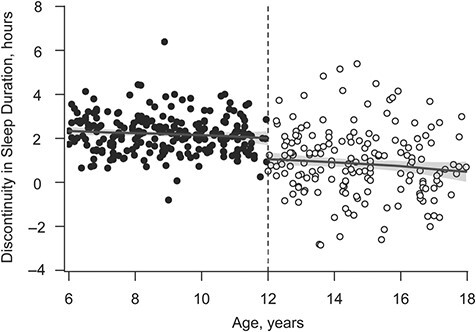
Regression discontinuity results for subjective minus objective sleep duration, including only subjective and objective measurements of weekday (Sunday through Thursday) nights with discontinuity in proxy- versus self-report status at age 12 years, Survey of the Health of Wisconsin, 2014–2017.
Figure 3 summarizes the regression discontinuity results for weekend measurements of sleep duration. The bandwidth used in this analysis was 5.0 years, the estimated discontinuity between proxy and self-reporters was −1.4 hours (P = 0.01), and a similar magnitude of difference was found using a 2.5-year bandwidth.
Figure 3.
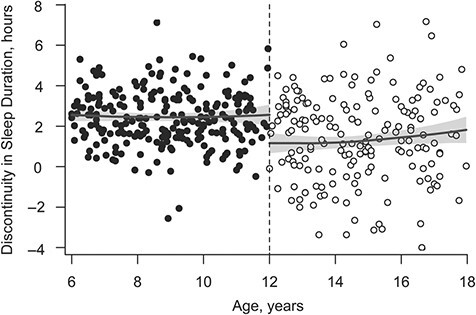
Regression discontinuity results for subjective minus objective sleep duration, including only subjective and objective measurements of weekend (Friday and Saturday) nights, with discontinuity in proxy- versus self-report status at age 12 years, Survey of the Health of Wisconsin, 2014–2017.
Figure 4 summarizes the regression discontinuity results for subjective sleep duration minus objective time in bed. The bandwidth used in this analysis was 3.4 years, the estimated discontinuity between proxy and self-reporters was −0.8 hours (P = 0.01), and a similar magnitude of difference was found using a 1.7-year bandwidth.
Figure 4.
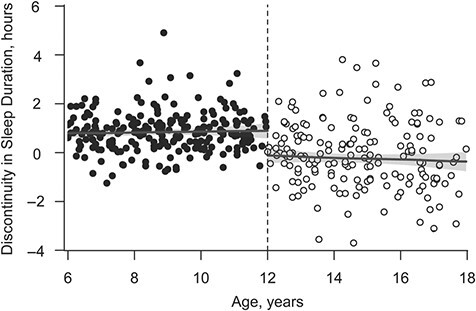
Regression discontinuity results for subjective sleep duration minus objective time in bed (sleep duration + wake after sleep onset + latency), with discontinuity in proxy- versus self-report status at age 12 years, Survey of the Health of Wisconsin, 2014–2017.
To further assess choice of bandwidth and the assumption that there are no important differences in the variables that systematically affect sleep within the local linear regression, Table 7 shows characteristics of participants who fell within either a 5-year range of the discontinuity (i.e., were 7–17 years old) or a 2.5-year range of the discontinuity (i.e., were 9.5–14.5 years), stratified by proxy- or self-report status. Most characteristics are balanced between self- and proxy reporters, apart from sex. In Web Table 3, we presents results of a test of whether sex was associated with the accuracy of self- and proxy reports; we found no strong evidence of an effect according to sex.
Table 7.
Descriptive Characteristics of Participants Within 5- and 2.5-Year Bandwidths From the Discontinuity in Proxy Versus Self-Report, Survey of the Health of Wisconsin, 2014–2017
| 5-Year Bandwidth | 2.5-Year Bandwidth | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Characteristic | Proxy Reported (n = 192), Age 7.0–11.9 Years | Self-Reported (n = 161), Ag 12.0–17.0 Years | Proxy Reported (n = 88), Age 9.5–11.9 Years | Self-Reported (n = 85), Age 12.0–14.5 Years | ||||||||||||
| Mean | 95% CI | No. | % | Mean | 95% CI | No. | % | Mean | 95% CI | No | % | Mean | 95% CI | No | % | |
| Sex | ||||||||||||||||
| Male | 100 | 52 | 81 | 50 | 51 | 58 | 38 | 45 | ||||||||
| Female | 92 | 48 | 80 | 50 | 37 | 42 | 47 | 55 | ||||||||
| Race/ethnicity | ||||||||||||||||
| White | 146 | 76 | 116 | 72 | 69 | 78 | 61 | 72 | ||||||||
| Black | 22 | 11 | 23 | 14 | 10 | 11 | 11 | 13 | ||||||||
| Hispanic | 9 | 5 | 12 | 7 | 4 | 5 | 7 | 8 | ||||||||
| Other | 15 | 8 | 10 | 6 | 5 | 6 | 6 | 7 | ||||||||
| BMI percentile | 63.1 | 58.8, 67.4 | 62.6 | 57.9, 69.3 | 61.5 | 55.5, 67.5 | 60.5 | 54.1, 67.0 | ||||||||
| Household income per person, per $1,000 | 18.2 | 16.3, 20.1 | 19.6 | 17.6, 21.6 | 19.4 | 16.4, 22.5 | 18.3 | 15.7, 20.8 | ||||||||
| Urban/rural | ||||||||||||||||
| Rural | 64 | 33 | 56 | 35 | 27 | 31 | 28 | 33 | ||||||||
| Urban | 120 | 63 | 98 | 61 | 54 | 61 | 53 | 62 | ||||||||
| Missing | 8 | 4 | 7 | 4 | 7 | 8 | 4 | 5 | ||||||||
| Self- or proxy-rated health | ||||||||||||||||
| Excellent | 89 | 46 | 65 | 40 | 41 | 47 | 40 | 47 | ||||||||
| Very good | 80 | 42 | 70 | 43 | 38 | 43 | 30 | 35 | ||||||||
| Good | 18 | 9 | 19 | 12 | 8 | 9 | 12 | 14 | ||||||||
| Fair | 3 | 2 | 5 | 3 | 1 | 1 | 1 | 1 | ||||||||
| Missing | 2 | 1 | 2 | 1 | 0 | 0 | 2 | 2 | ||||||||
Abbreviations: BMI, body mass index; CI, confidence interval.
To further test our assumption that there are no important differences in variables that systematically affect sleep duration, we tested whether there is an association between household income and age and found that a 0.03-year increase in child’s age was associated with a $1,000 increase in household income per person (P = 0.007). While there is evidence that socioeconomic status is associated with sleep patterns in adolescents (20), to our knowledge there is no evidence that small differences in socioeconomic status affect the accuracy with which children or their parents report on sleep.
A limitation of the regression discontinuity approach is its inability to account for clustered (within-household) data, and the effect of clustering is most concerning when there are 2 or more children from the same household with proxy-reported information (because the same proxy is likely reporting on all children for that household, correlating errors). Within the 5-year bandwidth used in the regression discontinuity, there were 192 participants in the proxy-report group and 144 unique households. As a final robustness check, we recalculated the regression discontinuity analysis for total weekly sleep duration, excluding any participants in the proxy-report group who lived in the same household. We estimated that the discontinuity was −0.9 hours (P = 0.03), which is almost the same as the −1.0-hour discrepancy we found using all available data. Thus, we expect our findings to be robust to the inclusion of multiple children per household.
DISCUSSION
In this analysis, we estimated the difference between subjective and objective measures of sleep, tested whether there were systematic differences between self- and proxy-reported subjective estimates, and investigated whether there was an age effect on the accuracy of subjective sleep measures. We found evidence of systematic overestimation of sleep duration by subjective measurements, with proxy reporters overestimating sleep duration by 2.3 hours (95% CI: 2.2, 2.4) and self-reporters overestimating sleep by 1.0 hour (95% CI: 0.7, 1.2). We did not find evidence of an age effect on the difference between subjective and objective sleep measures.
Gaina et al. (5) found that subjective sleep duration estimates were larger than objective estimates in a population of 13- and 14-year-olds who self-reported on their sleep, but the discrepancy was only 8 minutes, whereas our study found a difference of 1 hour between subjective and objective sleep. However, when comparing objective time in bed with subjective sleep time, we found a discrepancy of 12 minutes. Our findings on the difference between objective and subjective measures when using a proxy reporter support the previous findings of Werner et al. (4), who compared objective measures with proxy-reported measures and found a difference of about 1.8 hours, while we found a discrepancy of 2.3 hours.
The overestimation of sleep duration by proxies might be due to the wording of the subjective question, which asks about time the child spent in bed rather than the time spent sleeping. In this analysis, we measured a sleep latency of 4.8 minutes and wake after sleep onset of 1.3 hours in the proxy-report group. This sleep latency estimate is low compared with other studies, which have estimated that average sleep latency in healthy children is between 18 and 30 minutes (7, 21). However, even 30 minutes of difference between time in bed and time falling asleep, combined with our measured wake-after-sleep-onset values comes to approximately 1.8 hours and does not fully account for the average overestimation of sleep duration by proxies, which was 2.3 hours. Further, when we compare objective time in bed with subjective sleep-duration estimates, the overestimation is reduced in both groups, with proxy reporters overestimating by 0.8 hours, and self-reporters underestimating by 12 minutes. This finding supports the possibility that self-reporters are unable to accurately estimate time spent awake at night. Proxies are unlikely to know time spent awake during the night and might have additional limitations compared with self-reporters.
An important strength of this study was its ability to assess the effect of proxy reporting on the validity of sleep duration estimates. Because of the study’s design, we had the unique opportunity to implement a regression discontinuity approach, which is a quasiexperimental method and should allow us to identify the effect of proxy reporting compared with self-reporting on subjective sleep duration estimates.
One limitation of this study is the use of 1 week of accelerometry measurement to represent a “typical” week in the past month. Because the subjective questionnaire asked about sleep duration in the past month, we would ideally compare these subjective measurements with 1 month of accelerometry. However, because only 1 week of accelerometry measurements was collected, we assume these measurements are representative of the past month.
Another limitation in this study is the use of actigraphy as the measurement standard. Typically, polysomnography would be preferred as the gold standard, but several studies have demonstrated that actigraphy is an acceptable substitute when measuring sleep duration (7–9), and polysomnography per se can affect sleep duration and quality.
In conclusion, contrasting subjective self- and proxy reports with objective actigraphy measures, we found that proxy reporters overestimated sleep duration by an hour more than self-reporters. These results are robust to the choice of objective sleep duration estimate (time in bed vs. sleep duration) and highlight the importance of the age at which children are asked to self-report. Our findings suggest that it might be beneficial to reduce the age at which children are asked to self-report or to make empirically supported adjustments to proxy-reported sleep time in young children.
Supplementary Material
ACKNOWLEDGMENTS
Author affiliations: Department of Population Health Sciences, University of Wisconsin–Madison, Madison, Wisconsin, United States (Elizabeth A. Holzhausen, Erika W. Hagen, Tamara LeCaire, Lisa Cadmus-Bertram, Kristen C. Malecki, Paul E. Peppard); and Department of Kinesiology, University of Wisconsin–Madison, Madison, Wisconsin, United States (Lisa Cadmus-Bertram).
This research was supported by a Eunice Kennedy Shriver National Institute of Child Health and Human Development grant to the Center for Demography and Ecology at the University of Wisconsin–Madison (grants P2C HD047873 and T32 HD07014) and a National Institute on Aging grant to the Center for Demography of Health and Aging at the University of Wisconsin–Madison (P30 AG17266). K.C.M.’s time is also supported by the National Institutes of Health (grant R01 AG061080). Funding for the Survey of the Health of Wisconsin was provided by the Wisconsin Partnership Program PERC Award (233 PRJ 25DJ).
Conflict of interest: none declared.
REFERENCES
- 1. Spruyt K, Molfese DL, Gozal D. Sleep duration, sleep regularity, body weight and metabolic homeostasis in school-aged children. Pediatrics. 2011;127(2):e345–e352. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Dewald JF, Meijer AM, Oort FJ, et al. The influence of sleep quality, sleep duration and sleepiness on school performance in children and adolescents: a meta-analytic review. Sleep Med Rev. 2010;14(3):179–189. [DOI] [PubMed] [Google Scholar]
- 3. Erwin AM, Bashore L. Subjective sleep measures in children: self-report. Front Pediatr. 2017;5:22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Werner H, Molinari L, Guyer C, et al. Agreement rates between actigraphy, diary and questionnaire for children's sleep patterns. Arch Pediatr Adolesc Med. 2008;162(4):350–358. [DOI] [PubMed] [Google Scholar]
- 5. Gaina A, Sekine M, Chen X, et al. Validity of child sleep diary questionnaire among junior high school children. J Epidemiol. 2004;14(1):1–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Meltzer LJ, Biggs S, Reynolds A, et al. The Children's Report of Sleep Patterns–Sleepiness Scale: a self-report measure for school-aged children. Sleep Med. 2012;13(4):385–389. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Spruyt K, Gozal D, Dayyat E, et al. Sleep assessments in healthy school-aged children using actigraphy: concordance with polysomnography. J Sleep Res. 2011;20(1):223–232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Meltzer LJ, Walsh CM, Traylor J, et al. Direct comparison of two new actigraphs and polysomnography in children and adolescents. Sleep. 2012;35(1):159–166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Weiss AR, Johnson NL, Berger NA, et al. Validity of activity-based devices to estimate sleep. J Clin Sleep Med. 2010;6(4):336–342. [PMC free article] [PubMed] [Google Scholar]
- 10. Nieto FJ, Peppard PE, Engelman CD, et al. The Survey of the Health of Wisconsin (SHOW), a novel infrastructure for population health research: rationale and methods. BMC Public Health. 2010;10:785. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Sadeh A, Sharkey M, Carskadon MA. Activity-based sleep-wake identification: an empirical test of methodological issues. Sleep. 1994;17(3):201–207. [DOI] [PubMed] [Google Scholar]
- 12. Blumberg SJ, Halfon N, Olson LM. The National Survey of Early Childhood Health. Pediatrics. 2004;113(6):1899–1906. [PubMed] [Google Scholar]
- 13. Rouquette A, Côté SM, Pryor LE, et al. Cohort profile: the Quebec Longitudinal Study of Kindergarten Children (QLSKC). Int J Epidemiol. 2014;43(1):23–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Sonnega A, Faul JD, Ofstedal MB, et al. Cohort profile: the Health and Retirement Study (HRS). Int J Epidemiol. 2014;43(2):576–585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Centers for Disease Control and Prevention . A SAS Program for the 2000 CDC Growth Charts (ages 0 to <20 years). https://www.cdc.gov/nccdphp/dnpao/growthcharts/resources/sas.htm. Accessed March 27, 2020.
- 16. United States Census Bureau , 2010 Census Urban and Rural Classification and Urban Area Criteria. https://www.census.gov/programs-surveys/geography/guidance/geo-areas/urban-rural/2010-urban-rural.html. Accessed March 27, 2020.
- 17. Thisthlethwaite DL, Campbell DT. Regression-discontinuity analysis: an alternative to the ex post facto experiment. J Educ Psychol. 1960;51(6):309–317. [Google Scholar]
- 18. Dimmery, D. R package for regression discontinuity estimation. 2016. https://cran.r-project.org/web/packages/rdd/. Accessed February 18, 2021.
- 19. Imbens G, Kalyanaraman K. Optimal bandwidth choice for the regression discontinuity estimator. Rev Econ Stud. 2012;79(3):933–959. [Google Scholar]
- 20. Marco CA, Wolfson AR, Sparling BA, et al. Family socioeconomic status and sleep patterns of young adolescents. Behav Sleep Med. 2011;10(1):70–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Dayaat EA, Spruyt K, Molfese DL, et al. Sleep estimates in children: parental versus actigraphic assessments. Nat Sci Sleep. 2011;3:115–123. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.