

Abstract
Introduction Otosclerosis is a primary osteodystrophy of the otic capsule, frequently responsible for acquired hearing loss in adults. Although the diagnostic value of imaging investigations in otosclerosis is debatable, they might still be employed with different goals within the context of the disease.
Objectives The present paper aims to review the most recent literature on the use of imaging studies in otosclerosis for the most varied purposes, from routine application and differential diagnosis to prognostic prediction and investigation of surgical failure.
Data Synthesis The diagnosis of otosclerosis is usually clinical, but computed tomography (CT) is paramount in particular cases for the differential diagnosis. The routine use, however, is not supported by strong evidence. Even so, there is growing evidence of the role of this method in surgical planning and prediction of postoperative prognosis. In specific scenarios, for example when superior semicircular canal dehiscence (SSCD) syndrome is suspected or in surgical failure, CT is crucial indeed. Magnetic resonance imaging (MRI), however, has limited – although important – indications in the management of individuals with otosclerosis, especially in the evaluation of postoperative complications and in the follow-up of medical treatment in active ostosclerosis.
Conclusion Imaging studies have a broad range of well-established indications in otosclerosis. Besides, although the routine use of CT remains controversial, the most recent papers have shed light into new potential benefits of imaging prior to surgery.
Keywords: otosclerosis, tomography, X-Ray, computed, magnetic resonance imaging, stapes surgery, diagnostic imaging
Introduction
Otosclerosis is a primary focal osteodystrophy of the otic capsule affecting genetically predisposed individuals and whose etiology remains unknown. 1 When the disease is active – a phase also called otospongiosis – the histologically normal endochondral bone of the otic capsule is replaced by disorganized foci of Haversian bone; with progression and reduced disease activity, however, the bone involved becomes dense and sclerotic. 2 When the otosclerotic lesions compromise the stapediovestibular joint and/or inner ear components, patients develop hearing loss (HL) that might be conductive, sensorineural or mixed. 3
Classically, otosclerosis is divided into two types: fenestral and retrofenestral. The first one, which is far more typical, is determined by lesions preferably located on the lateral wall of the otic capsule. On the other hand, retrofenestral otosclerosis is defined by the occurrence of more medial otosclerotic foci , within the labyrinthine capsule. Overall, the most frequently involved site in clinically overt otosclerosis is the fissula ante fenestram (FAF), which is an island of fibrocartilaginous connective tissue within the endochondral layer of the otic capsule, between the oval window and the cochleariform process. 4
The diagnosis of otosclerosis is traditionally suspected upon clinical grounds, often endorsed by audiometric findings. Conversely, the diagnostic value of routine imaging studies is often a matter of debate. However, high resolution computed tomography (HRCT, CT scans) and magnetic resonance imaging (MRI) might be employed with different goals within the context of otosclerosis and an increasing number of indications for their use have been reported and discussed in recent years. The present review aims to describe the imaging findings and their role in otosclerosis in the light of the current literature.
Review of a Particular Subject
Computed Tomography Scans in Otosclerosis - Main Findings and Classical Uses
The use of imaging methods has been increasingly studied in the diagnosis, staging, prognosis, surgical planning, prediction of postoperative results and management of complications related to otosclerosis. High resolution computed tomography is the method of choice in the assessment of structural abnormalities of the temporal bone in cases of conductive or mixed HL, including those in which osteodistrophy is suspected. 2 The exact value of CT scans in otosclerosis is still a matter of controversy in clinical practice, so patients with a typical history are not often subjected to systematic radiological assessment prior to surgery.
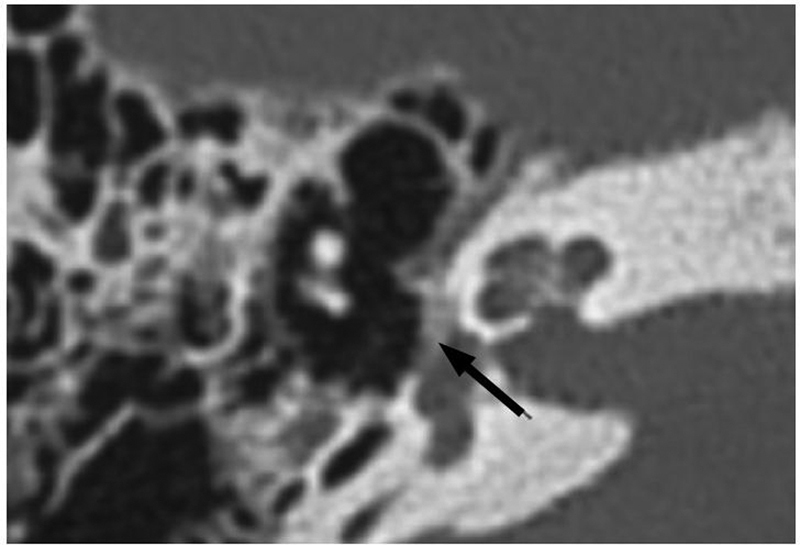
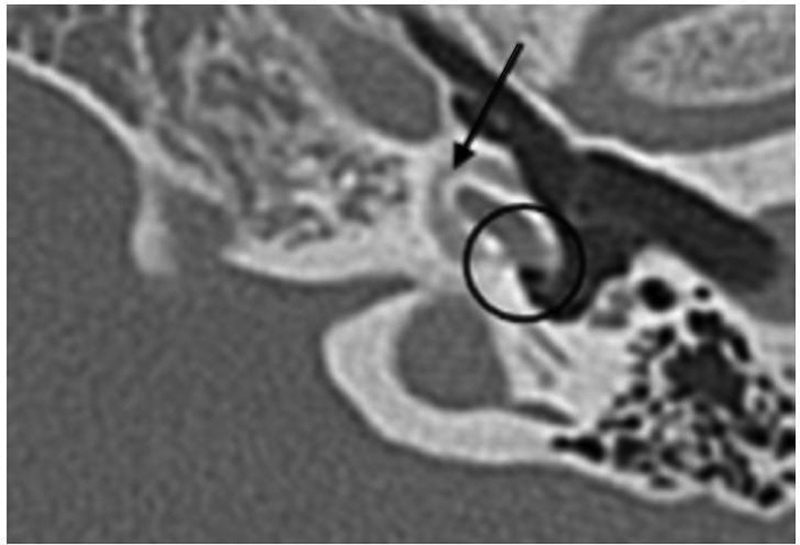
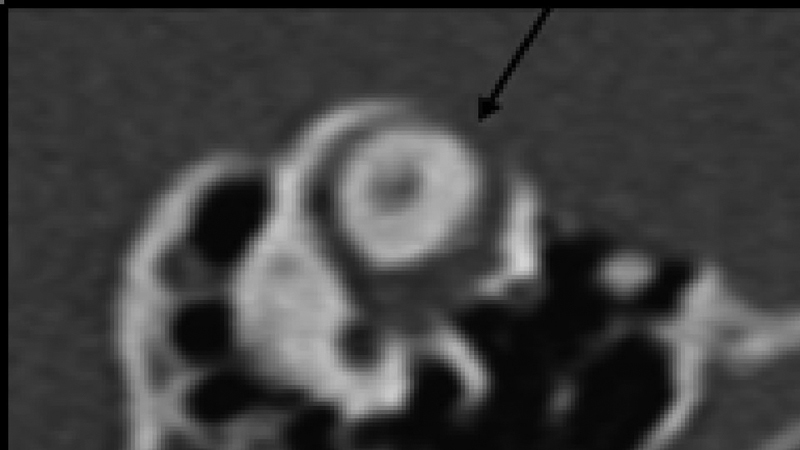
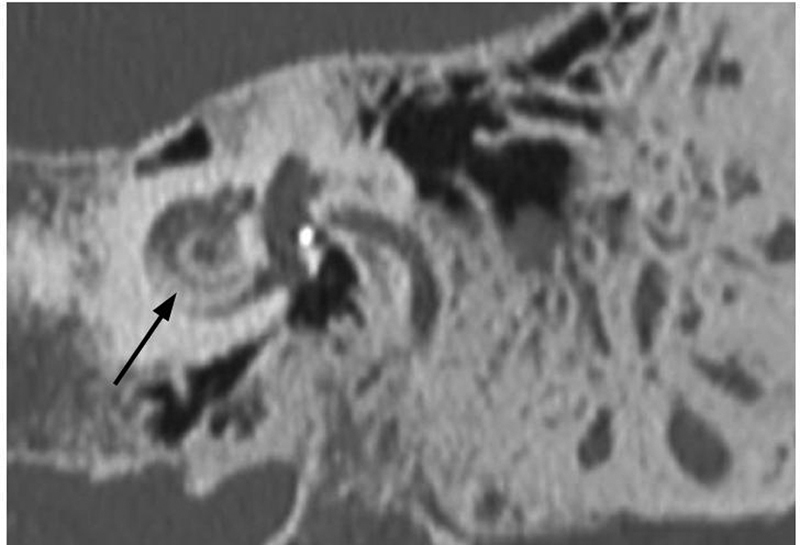
Usually, for the radiological evaluation of suspected otosclerosis, very thin slices are obtained by a scanner with multiple detectors. The imaging data are then reconstructed in the coronal and axial planes, parallel and perpendicular to the plane of the lateral semicircular canal. Other reconstructions, for example, in the direction of the stapes suprastructure plane, might also be necessary. 5 In the otospongiotic phase, the foci are visualized on HRCT as areas of reduced bone density. Thus, they appear as radiolucent areas in the otic capsule - for example, affecting the FAF in the fenestral type ( Fig. 1 ). 1 These foci are best evaluated in the axial view, since the oval window has an anteroposterior orientation. Fenestral foci of ∼ 1mm might already be identified in more widely available HRCTs. 6 7 8 Patients with retrofenestral disease have otherwise perilabyrinthine radiolucent foci, sometimes surrounding the cochlea, which is recognized as the “double ring sign” ( Fig. 2 ). The classic appearance of retrofenestral otosclerosis is rarely mimicked by systemic diseases affecting the temporal bone, such as osteogenesis imperfecta and Paget disease. 6 7 As for the otosclerotic phase, the density of the foci increases, which could hinder the diagnosis and increase false-negative errors. The presence of bone contour irregularities may be key to diagnosis in this context ( Fig. 3 ). 1 However, the accuracy of CT scans in inactive otosclerosis might be better than predicted, since the disease tends to be multifocal, with concomitant active and inactive foci in the same individual. 9
Fig. 1.
Computed tomography scan of temporal bone. Axial view at the level of the oval window, showing a hypodensity focus limited to the fissula ante fenestram (black arrow), typical of otosclerosis. Source: the authors.
Fig. 2.
Computed tomography scan of temporal bone. Axial view at the level of the cochlear basal turn, with a pericochlear hypodensity surrounding the cochlear turns, determining the “double ring sign”, typical of retrofenestral otosclerosis. Source: the authors.
Fig. 3.

Computed tomography scan of temporal bone. Axial view at the level of the oval window, showing the presence of contour irregularities on the surface of the otic capsule (black circle), typical of inactive otosclerosis. Source: the authors.
The use of preoperative imaging evaluation is well-established for some patients with suspected otosclerosis. For example, in cases of isolated sensorineural HL, clinical suspicion in children, especially in boys (to rule out X-linked mixed HL), presence of facial deformities or ear malformations, intermittent HL, associated vestibular impairment, revision cases, history of trauma, and history of chronic otitis media. Alternative diagnoses, such as superior semicircular canal dehiscence (SCCD) syndrome, osteogenesis imperfecta, Paget disease, fibrous dysplasia, malformations or ankylosis of the ossicular chain and otosyphilis should be thoroughly investigated in these situations. 10
High-resolution Computed Tomography in Otosclerosis - Diagnostic Performance
Overall Sensitivity
The sensitivity of HRCT in detecting otosclerosis varies widely across the studies. In the 1980's, Swartz et al identified fenestral otosclerosis on the CT of 74% of the patients suspected of having the disease. 4 Priya et al analyzed the value of HRCT in determining the degree of footplate thickening and the location of the disease in the case of stapedial otosclerosis. When compared with intraoperative findings, CT data showed an 85% of sensitivity in the correct definition of these parameters. The authors argued that the presence of false negatives was justified by an annular fixation of the footplate. 11 This type of fixation found intraoperatively was also consistent with the histological findings of a study by Cherukapally et al. 12 In 2001, Shin et al found a sensitivity of CT scans in the diagnosis of otosclerosis of 91.3%. The false negatives were also attributed to early, “infraradiological” disease. 13 In a radiological, histological and audiometric study, Karosi et al found 28.3% of individuals with nonotosclerotic stapes fixation. Such patients also presented stapediovestibular calcification with an annular aspect on histology, with marked thickening of the footplate. Computed tomography scan showed the lowest diagnostic sensitivity (51.7%) in such cases, even when compared with patients with inactive otosclerosis. The authors stated that audiometry could better tell these two groups apart, since in the nonotosclerotic fixation of the stapes, the occurrence of concomitant sensorineural HL would not be usual. 14 The identification of these cases of nonotosclerotic stapes fixation, perhaps related to early cases of “infraradiological” otosclerosis, might be important for surgical planning. Among them, the intraoperative incidence of footplate-related complications, such as mobilization, fluctuation or fracture, seems higher. 15
There are also data concerning this topic in non-Caucasian individuals. A Korean study of 31 patients (37 ears) with surgically-confirmed otosclerosis indicated a 73% prevalence of patients with suggestive alterations in the preoperative HRCT scans. 16 These results are similar to those published by Naumann et al 17 in patients with clinical suspicion of the disease. The sensitivity of the method in that study increased to 85% after multiplanar reconstructions (MPR). The suspected cases with normal CT even after MPR were those with smaller air-bone gaps (ABGs).
Use of Objective Computed Tomography Scan Parameters
The systematic use of tissue density measurements of specific regions of the temporal bone might be helpful in identifying patients with otosclerosis. Among them, the hypodense otospongiotic foci present reduced density values, measured in Hounsfield Units. 18 19 20 Kutlar et al demonstrated that patients with a clinical-surgical diagnosis of otosclerosis had lower radiological density for the FAF region, but not for other temporal bone areas, in comparison with a control group. 21 Accordingly, Kawase et al and Grayeli et al demonstrated comparatively lower tissue densities in the FAF, but also anterior to the IAO and posterior semicircular canal, respectively. 18 20 It is believed that the use of larger regions of interest (ROIs), of 10 × 10 pixels, placed on the FAF, could increase the reproducibility and confidence of the densitometric evaluation method, even though there is no supporting evidence to date. 19
Otosclerotic foci are generally seen as areas with a lower attenuation coefficient than the surrounding temporal bone. Nevertheless, the absolute values of the coefficient can vary according to the parameters of acquisition and reconstruction, with an important loss of comparability and external validity. 22 The use of relative measures are alternatives that have demonstrated good preliminary results. These measures might include, for example, the density ratio between specific ROIs and control sites or the percentage number of pixels of an area of study below a pre-established density threshold. 19 23
Sanghan et al described the thickness of the otic capsule as another interesting parameter in the CT evaluation of patients with suspected otosclerosis. The presence of a convex contour of the otic capsule anterolateral to the oval window proved to be a good marker of otosclerotic disease. In addition, a distance between the lateral margin of the cochlea and the lateral limit of the contour of the otic capsule in the antefenestral region > 2.3 mm showed an excellent diagnostic accuracy. 24
Techniques for Obtaining and Processing the Computed Tomography Scan
The quality of the assessment of temporal bone CT strongly depends on the examiner. An English study revealed that, when assessing suspected cases of otosclerosis, dedicated neuroradiologists performed significantly better than general radiologists. 25 Another study demonstrated excellent diagnostic accuracy when a tailored protocol for otosclerosis was employed in the CT evaluation. 26
The use of specific image processing techniques can also increase CT sensitivity. Yamashita et al reported that the combined use of a postprocessing method based on reversing the radiological density of the images obtained significantly increased the overall diagnostic accuracy. This improved performance seemed to accrue from an increased contrast between the otosclerotic lesion and the adjacent bone and was especially useful for less experienced radiologists. 23
Results in a Setting Mimicking Clinical Practice
A retrospective English study including 259 clinically-suspected patients showed a high rate (33%) of alternative diagnoses in CT scans negative for otosclerosis. 15 It is interesting to highlight that this study reproduces more accurately the typical scenario observed in many centers worldwide, in which the CT scan is performed in selected patients. In this situation, the radiological study seems to provide useful information for an important portion of the patients. Indeed, the authors stated that performing CT scans prevented many individuals from “exploratory surgeries.” In addition, in this study, the positive predictive value of CT in the diagnosis of otosclerosis was 100%. The authors concluded that clinically-guided CT assessment could be beneficial as it contributed to clinical reasoning in atypical cases and influenced favorably therapeutic decisions. 15
Cone Beam Computed Tomography
Cone beam computed tomography (CBCT) is a relatively new imaging method, widely used in endodontics and orthodontics. The emitted radiation dose is much lower than that of traditional exams, with reduced time for image acquisition and processing. Besides, the diagnostic performance of CBCT has improved at the expense of more accurate scanning techniques and avant-garde image processing software. To date, few studies have evaluated the use of CBCT in otosclerosis. Liktor et al found, in a study with 32 patients, a sensitivity of 65.62% when the radiological evaluation was compared with histopathological findings. The authors noted a strong correlation of the diagnostic performance with the stage of the fenestral disease of the patient: in otospongiosis, the sensitivity of CBCT reached 100%, while in the otosclerotic phase, it decreased to 0%. 27 Redfors et al compared traditional CT and CBCT scans of 20 patients who had undergone stapedectomies 30 years before. For fenestral disease, conventional CT showed greater sensitivity, which was similar for retrofenestral disease. For both methods, the visualization of the prosthesis was deemed satisfactory. 28
Systematic Reviews
A broad 2013 systematic review, which included 37 studies, demonstrated HRCT sensitivity and specificity for the diagnosis of otosclerosis > 90% with the most modern techniques. A grade III level of evidence was found for the correlation between either the results of densitometry or the radiological extension of the disease with the audiometric thresholds. The authors also identified the potential use of CT scans for surgical planning, assessment of complication risks and prediction of postoperative results. 29
Another 2016 review including 7 studies with moderate to high relevance and low to moderate risk of bias demonstrated that the HRCT sensitivity in otosclerosis varied from 60 to 95%. The authors reported better diagnostic performance in more recent studies and in those whose samples had a higher overall prevalence of the disease. As a result, they considered that, in general, the study would not be significantly valuable in typical otosclerosis for diagnostic purposes. However, the use of HRCT could still be useful in determining the extent of the disease and detecting concomitant abnormalities. 30
Radiological Staging of Otosclerosis
Several CT grading scales for otosclerosis have been proposed, but none of them have been universally accepted. 8 31 Perhaps the most adopted staging systems are those proposed by Symons/Fanning ( Table 1a ), 32 Rotteveel ( Table 1b ) 31 and Veillon ( Table 1c ). 33 The first two were described in studies of patients with advanced otosclerosis who underwent cochlear implantation. The Symons/Fanning system is based primarily on the location of the otosclerotic foci, regardless of the type of lesion found. This classification showed a high degree of inter- and intraobserver agreement in another study. 8 The Rotteveel classification, however, is based on the type of lesion and the presence of particular findings, such as the halo effect or “double ring sign” and the narrowing of the basal turn of the cochlea. In the original study, the authors also observed high interobserver agreement and a correlation between the radiological stage of the disease and the age of onset of the HL. 31 The Veillon system takes into account the location of otosclerotic foci within the labyrinthine capsule and stages the disease in four levels, three of which are dedicated to fenestral diseases. 33 A recent study reported that this classification system could predict worse audiometric results in the preoperative period. However, as for the audiometric results after stapedotomy, the Veillon system showed a correlation with improvement of the ABG only in the short-term. 34 Apart from these studies, data on the clinical, therapeutic or prognostic values of these different grading studies in otosclerosis remain scarce.
Table 1. Computed tomography grading systems for otosclerosis.
| A- SYMONS / FANNING CLASSIFICATION | |
|---|---|
| CT Grading | Foci Location |
| Grade 1 | Solely fenestral |
| Grade 2 | Patchy cochlear disease (with or without fenestral involvement) |
| To basal turn (grade 2a) | |
| To middle turn (grade 2b) | |
| Around the lateral aspects of the basal, middle and apical turns (2c) | |
| Grade 3 | Diffuse and confluent cochlear involvement (with or without fenestral involvement) |
| B- ROTTEVEEL CLASSIFICATION | |
| CT Grading | Foci Location |
| Type 1 | Fenestral only (thickened footplate and/or narrowed or enlarged windows) |
| Type 2 | Retrofenestral disease (with or without fenestral involvement) |
| Double ring effect (grade 2a) | |
| Narrowed basal turn (grade 2b) | |
| Double ring effect and narrowed basal turn (2c) | |
| Type 3 | Severe retrofenestral involvement (unrecognizable otic capsule), with or without fenestral involvement |
| C- VEILLON CLASSIFICATION | |
| CT Grading | Foci Location |
| Type 1 | Isolated involvement of the footplate, which is thickened (> 0.6 mm) and hypodense (1a) |
| Anterior fenestral hypodensity ≤ 1 mm (1b) | |
| Type 2 | Anterior fenestral hypodensity > 1 mm, without contact of the focus with the cochlear endosteum |
| Type 3 | Anterior fenestral hypodensity > 1 mm and with contact of the focus with the cochlear endosteum |
| Type 4 | Anterior labyrinthine hypodensities, that is, around the cochlea (4a) |
| Posterior labyrinthine hypodensities, that is, around the semicircular channels or the vestibule (4b) | |
Abbreviation: CT, Computed tomography.
Correlation between Computed Tomography and Audiometric Findings in Patients with Otosclerosis
The relationship between otosclerotic foci and audiological features has been studied especially in histopathological studies. However, despite the incomparable value of histological studies in describing otospongiotic and otosclerotic lesions, their ability to correlate structural findings to audiometric data are limited, since there is often a significant and heterogeneous interval between the time of the audiological evaluation and the death of the individual.
On the other hand, CT studies show a better temporal correlation with the audiometric assessment. Even so, the interrelationship between overall CT findings and the degree of HL is still controversial and there is considerable heterogeneity in the disease staging method or radiological parameters used for comparison. 10 Shin et al showed worse audiometric results in patients with pericochlear extension of the disease compared with those whose disease was limited to the FAF on CT scans. 35 A strong correlation between the site of the otosclerotic focus around the cochlea and the audiometric frequency of the sensorineural HL was described in another study. 36 , A study by Marx et al including 200 patients showed worse bone-conduction thresholds in patients with extensive otosclerosis, when compared with those with isolated fenestral disease. The involvement of the pericochlea, of the cochlear endosteum, of the round window or of the internal auditory canal predicted poorer hearing performance. In addition, postoperative audiometric results correlated with CT findings and were worse in extensive otosclerosis. 37 Endosteal extension on CT scans of patients with otosclerosis was also predictive of worse bone-conduction thresholds in a retrospective study that included 259 patients. 15 Another study also demonstrated significantly worse thresholds by both air and bone conduction only for the most advanced cases of the disease, when compared with those that are deemed moderate (with pericochlear foci) or early (fenestral only). 21
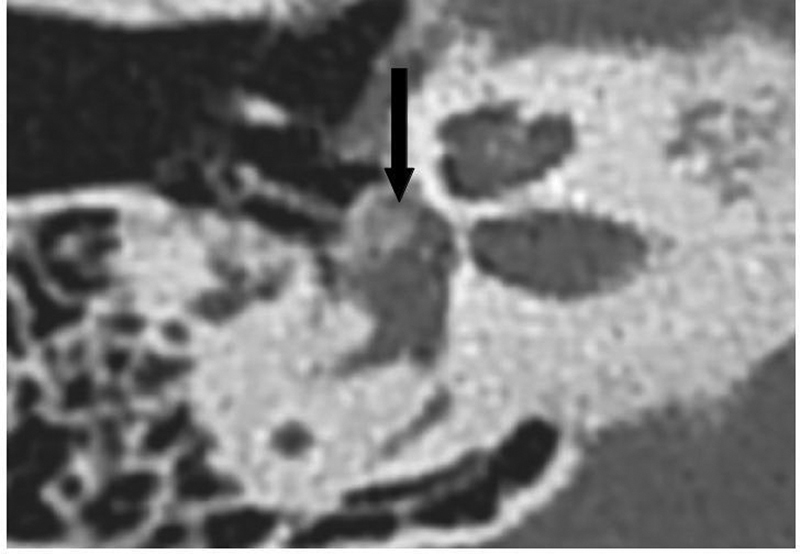
The involvement of the round window seems to implicate in worse bone thresholds in the pre- and postoperative periods, especially when it is obliterated ( Fig. 4 ). 15 34 In these cases, the “single window” effect might impair the transmission of acoustic energy within the cochlea by reducing the compressibility of the intracochlear fluids. Moreover, this phenomenon might also compromise the results of stapedotomy. Nonetheless, involvement of the round window is usually seen in more extensive disease with retrocochlear foci, which might work as an important confounding factor in the analysis of the audiometric parameters. 15
Fig. 4.
Computed tomography scan of temporal bone. Axial view at the level of the facial recess, demonstrating the presence of a hypodense focus causing an increase in volume at the region of the round window (black circle), with apparent continuity with a pericochlear focus (black arrow). Source: the authors.
In contrast, data regarding the audiological implications of more specific characteristics of the foci are conflicting. Min et al could not find a correlation between the existence of hypodensity foci on CT and the degree of HL. They also reported no significant correlation between the density of the foci and the preoperative audiometric thresholds. However, this parameter was significantly related to the postoperative ABG, so that the lower the density of the focus, the higher the ABGs after surgery. 16 Another study also failed to show a correlation between the average density of the fenestral focus and the patients' audiometric performance. 19 In contrast, Kawase et al found a correlation between the density of the region anterior to the oval window and the audiometric thresholds for both air and bone conduction in the frequencies of 500 and 1,000Hz. 18 Grayeli et al also described that antefenestral bone density in patients with otosclerosis would correlate with disease progression and prognosis. 20 Naumann et al demonstrated higher ABGs in patients with larger otosclerotic foci, but could not establish a correlation between bone conduction thresholds and cochlear involvement. 17 A study with Japanese patients also revealed associations between the size of the fenestral focus and the size of the ABG and between the cochlear extent of the disease and the bone conduction thresholds. 38 Finally, Priya et al did not find the radiological correlation between thickness of the footplate and audiometric parameters. 11
In general, location and size of otosclerotic foci seem to be poorer predictors of sensorineural HL than endosteal involvement and injuries to the cochlear integrity. 8 32
Computed Tomography Findings as Predictors of Intraoperative Difficulty and Risks
The CT scan in otosclerosis enables a disease-oriented preoperative evaluation, with special regard to important structures, such as the oval window and the tympanic segment of the facial nerve. A narrow oval window, due to a hypertrophic cochlear promontory or a prolapsed facial nerve, can lead to technical difficulties during the surgical procedure. One study demonstrated that an estimated height of the oval window < 1.4 mm could predict technical difficulties during stapes surgery. 39 Similarly, Parra et al also correlated radiological measurements of the promontory-facial angle and the amplitude of the oval window with the degree of subjective technical intraoperative discomfort. 40 Whether such difficulties incur in worse postoperative results is still unknown.
The overall prevalence of facial nerve dehiscence estimates ranges from 2.7 to 29.5%. Whenever present, this dehiscence leads to decreased oval window size and promontory-facial angle. In addition, it was associated with technical difficulties, probably as a result of a limited access to the footplate and an increased risk of nerve damage. 40
The prevalence of obliterative foci ( Fig. 5 ) was estimated in between 27.5 and 33.9% in CT studies performed in India, with a male preponderance. 11 41 Preferably, the presence of obliterative foci ought to be always ruled out, as it implies an increasing risk of intraoperative complications. Besides, whenever diagnosed, it changes surgical planning, as the surgeon often requires local drilling to place the prosthesis.
Fig. 5.
Computed tomography scan of temporal bone. Axial view at the level of the oval window, showing the presence of an obliterative otosclerotic focus (black arrow). Source: the authors.
Preoperative CT evaluation can also help identify patients at risk of gusher, which is a rare intraoperative complication of stapedotomy secondary to anomalous communication between the subarachnoid and perilymphatic spaces. Veillon mentioned as potential risk factors: dilatation of the fundus of the internal auditory canal, dilated vestibule, enlarged vestibular aqueduct, enlarged cochlear aqueduct in the most distal portion, cochlear dysplasia, and dilated labyrinthine segment of the facial nerve canal. 42 However, these findings are not always easily individualized in preoperative CT scans and might require extra attention from the examiner. 43
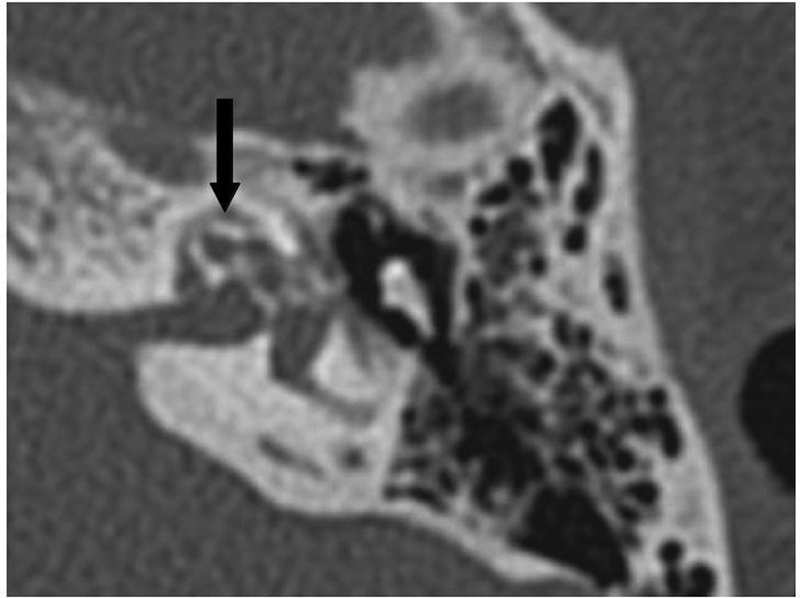
The SSCD syndrome is a condition whose clinical presentation often mimics that of otosclerosis. It is characterized by the absence of bone overlying the superior semicircular canal, facing toward the dura of the middle fossa ( Fig. 6 ). Computed tomography scans might help differentiate SSCD from otosclerosis. In cases in which otosclerosis and SSCD occur simultaneously, the preoperative radiological diagnosis of both conditions can also be beneficial, as this particular situation increases the risk of unsatisfactory surgical outcomes. 44
Fig. 6.
Computed tomography scan of temporal bone. Oblique view at the level of the superior semicircular canal, showing an area of dehiscence (black arrow). Source: the authors.
The presence of diverticula from the internal auditory canal (IAC), usually in the anteroinferior wall, ( Fig. 7 ) is more frequently observed in individuals with otosclerosis. It might indicate localized foci of the disease, but the prognostic value is still controversial and seems to vary according to the time of evaluation, whether pre- or postoperative. The existence of an IAC diverticulum itself did not determine worse preoperative audiometric prognosis in one study. 45 Another group of authors also found no differences between the subgroups of patients with extensive otosclerosis with or without cavity plaques around the IAC on CT in terms of general radiological staging, type of HL, atypical clinical manifestations or incidence of surgical complications during cochlear implantation. 46 On the other hand, a Korean study showed worse postoperative air and bone conduction thresholds, in addition to a greater residual ABG, among patients with retrofenestral disease whose cavitations reached the IAC. According to the authors, the finding could suggest a “third window” effect in this group, similar to that present in patients with SSCD, leading to the dissipation of part of the acoustic energy and, consequently, worse surgical results. 47
Fig. 7.
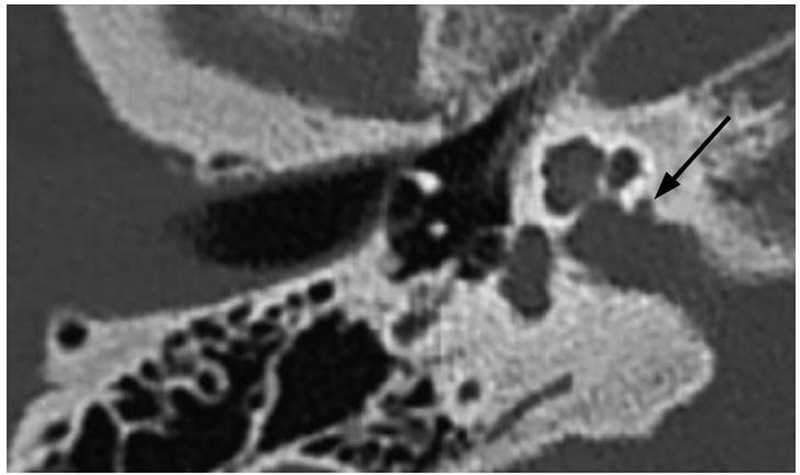
Computed tomography scan of temporal bone. Axial view at the level of the oval window, showing the presence of a diverticulum in the internal auditory canal, also called “nipple sign” (black arrow). Source: the authors.
The presence of a persistent stapedial artery can also be determined by CT scans. In these cases, the foramen spinosum is absent and there is an apparent enlargement of the tympanic segment of the facial nerve. An aberrant internal carotid artery might also be found. The identification of this rare abnormality is critical in ear surgery, due to the intimate relationship with the stapes. 48
Routine Use of Computed Tomography Scans
Some authors believe that the routine use of CT scans in otosclerosis is still not well-established due to the rarity of concomitant malformations of the inner ear, the low predictive value of CT for intraoperative gushers, the absence of surgical contraindication in extensive multifocal disease, the associated costs, and the radiation exposure inherent to the test. 49 In addition, others argue that the body of evidence regarding the diagnostic performance and prognostic value of HRCT in patients with otosclerosis remains limited. 8 16 Furthermore, the routine use of the current radiological staging systems for the comprehensive assessment of otosclerosis in diagnostic, prognostic and therapeutic aspects is not supported by strong research data yet.
Magnetic Resonance Imaging in Otosclerosis
The use of a protocol for endolymphatic hydrops (EH) using magnetic resonance imaging (MRI) before stapes surgery was studied in 16 individuals with otosclerosis. In this study, the patients underwent 3 Tesla MRI 4 hours after intravenous injection of gadolinium. Evidence of EH in the vestibule ( Fig. 8 ) was correlated with the occurrence of prolonged vertigo and decreased hearing gain postoperatively. Cochlear EH, on the other hand, did not interfere with the surgical outcomes. The authors concluded that the method would be effective in identifying patients at high risk for undesirable results. 50
Fig. 8.
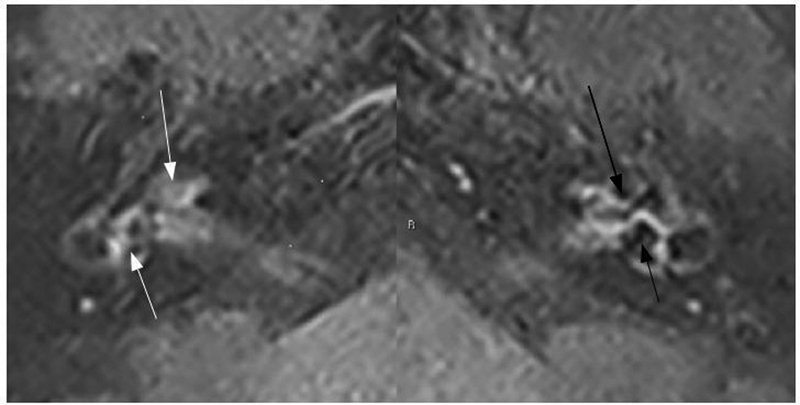
Magnetic resonance imaging of the brain, 4 hours after double injection of gadolinium, at the level of the membranous labyrinth, REAL IR sequence, axial view. Areas with signal voids on the left ear might be observed, corresponding to the cochlea and vestibule, compatible with endolymphatic hydrops (black arrows). The contralateral inner ear has a comparative normal appearance (white arrows). Source: the authors.
Pure cochlear otosclerosis - a rare cause of isolated sensorineural HL, is more usually assessed by MRI in the first instance. A halo of intermediate perilabyrinthic intensity at T1, with slight to moderate enhancement, might be observed in this case. Sometimes, T2 hyperintensity is also noted. 2 In retrofenestral otosclerosis, the use of the 3D-Flair sequence before and after gadolinium seems to effectively evaluate cochlear damage caused by the disease. The presence of hyperintensity and postcontrast enhancement would be good predictors of permeability changes of the blood-labyrinth barrier. 51 52 In different stages of otosclerotic involvement, the aforementioned labyrinthine disturbances might correlate with clinical parameters, such as disease duration and degree of cochlear damage, measured by bone-conduction thresholds. 52
Preliminary studies point toward the utility of imaging in the evaluation of candidates to medical treatment for active otospongiosis. In this context, evidence of demineralization of the cochlear endosteum in HRCT or MRI could support the use of drug therapy to prevent the onset or the progression of the disease, even in cases without audiometric repercussions. 53 Magnetic resonance imaging in particular might be a fair method for objective analysis of medical treatment in otosclerosis. In a controlled study, de Oliveira Vicente et al reported that both subjective and objective measures of signal intensity in the FAF on MRI could serve as parameters of effectiveness during the use of sodium fluoride or sodium alendronate. 54
Imaging in Advanced Otosclerosis
In far advanced otosclerosis with profound HL, both CT and MRI are mandatory prior to cochlear implantation. In this situation, the combination of both methods is able to establish cochlear patency and the extent of cochlear ossification ( Fig. 9 ). Besides, these imaging studies might predict the risk of unintentional electrical stimulation of the facial nerve postoperatively due to the dissipation of the electrical energy amid a dysplastic cochlea. 31
Fig. 9.
Computed tomography scan of temporal bone. Coronal view at the level of the cochlea showing a hyperdense focus on the cochlear endosteum, possibly related to ossifying labyrinthitis (black arrow). Source: the authors.
Use of Computed Tomography and Magnetic Resonance Imaging in the Postoperative Period of Stapes Surgery
The routine use of CT in the postoperative period of stapes surgery is not validated in the literature. A total of 80 patients who had undergone stapes surgery were submitted to CBCT within the first 24 hours of the procedure in a French study. Although the authors found a 15% rate of pneumolabyrinth, they could not correlate this finding with either the incidence of complications or the surgical results. Yet, the length of the prosthesis penetrating into the vestibule was also not a predictor of postoperative outcomes. 55 Similarly, Yehudai et al and Fang et al failed to correlate the depth of penetration of the stapes prosthesis on HRCT with the hearing outcomes or the occurrence of cochleovestibular symptoms after surgery. 56 57 A cadaveric study showed that the material of the prosthesis could have an influence on the CT estimates of the depth of penetration into the vestibule and should therefore be considered whenever a postoperative CT scan is performed. In the case of fluoroplastic prosthesis, the penetration depth could be underestimated by up to 0.5 mm. Metal prostheses, on the other hand, would be better visualized and, when the measurement of their depth reached > 2.2mm, the possibility of otolithic impingement should be appraised. 58
Bajin et al evaluated 20 patients the day after surgery and found pneumolabyrinth in all the CT scans, without any clinical repercussion. Furthermore, the patients no longer presented signs of air within the labyrinth when re-evaluated 7 days after the procedure. 59 Hence, one could state that this transient pneumolabyrinth would be the rule, rather than the exception, after stapes surgery, and would not implicate in postoperative sensorineural HL or vertigo. On the other hand, in the cases of vertigo or sensorineural HL, a pneumolabyrinth after 1 week of surgery suggests a perilymphatic fistula. 60 In this scenario, the postoperative HRCT could also identify cases of protrusion of the stapes prosthesis into the vestibule. 61
The postoperative use of CT scans in cases in which the ABG closure is not achieved also seems beneficial, both in the short- and long-term. High resolution computed tomography might identify, for example, prosthesis displacement, necrosis of the long process of the incus, granulation tissue, unnoticed round window obliteration or ossifying labyrinthitis. 62 Moreover, in some cases, the presence of misdiagnosed or concomitant SSCD might be detected only at this point. In the case of normal postoperative HRCT scans, MRI might be of great value, particularly in the presence of sensorineural deterioration. In these patients, signs of labyrinthitis, inner ear hemorrhage or intralabyrinthine repair granuloma might be found. Such conditions must be promptly diagnosed, as they carry a worse prognosis. 61 Hemorrhages would be suspected by a high signal intensity within the labyrinth in both T1- and T2-weighted images. Hypointense focal T1-weighted contrast-enhanced intralabyrinthine images would indicate repair granulomas. Finally, the obliteration of the labyrinth in T1-weighted images with extensive postcontrast enhancement would be suggestive of labyrinthitis. 61
Discussion
Although the routine use of CT scans might be still a controversial issue, the most recent imaging techniques have enabled important advances in the understanding of otosclerosis. At first glance, for the majority of patients, the diagnosis is set on a clinical basis and diagnostic CT could be redundant and only expose patients to unnecessary radiation. However, the most modern techniques have reached great accuracy and the identification of the few “infraradiological” CT-negative cases might be relevant. Some studies point to the fact that these false-negative cases might occur when the otosclerotic focus is be limited to the annular ligament. Stapes surgery would be perhaps riskier and less successful among these patients.
Computed tomography scan data seem to correlate with audiometric evaluation at some extent, and the use of some CT parameters as predictors of postoperative prognosis seems promising. So far, signs of damages to the cochlear integrity or to the endosteum have more consistently shown better correlation to audiometric thresholds than specific characteristics of the foci such as number, location or size. There remain conflicting results in this field and it might reflect the heterogeneity of the studies regarding the method of imaging acquisition, reconstruction and evaluation. Besides, the already described radiological grading systems need to be supported by increasing evidence of their reproducibility and external validity. They need to prove to be suitable for the appraisal of otosclerosis in the different clinical scenarios the patients might present during follow-up. For example, few studies aimed to assess the usefulness of the radiological classifications preoperatively, and thus we have not reached a consensus of which scale is more appropriate in this situation. Improving the available grading systems might therefore contribute to future studies on the prognostic value of CT scans.
In very particular situations, including uncommon differential diagnosis or concomitant anatomical variations, the use of HRCT is already validated. In otologic practice, these situations might occur not so infrequently, so that CT scans have an increasing importance. Besides, if we bear in mind that these situations altogether might correspond to a considerable share of the patients with otosclerosis, the use of imaging would seem more reasonable. Likewise, the use of CT scans is also well-established in cases of surgical failure with residual ABG. In this context, many situations are properly diagnosed, such as prosthesis displacement, a theretofore unrecognized dehiscent superior semicircular canal or a focal granuloma. For each of these situations, the identification of the problem has a major impact on the prognosis and treatment plan.
Magnetic resonance imaging, on the other hand, has a limited – but not negligible – utility in the context of otosclerosis. In fact, in certain cases, the use of this imaging method is not only validated, but essential. It is crucial and accurate in the rare cases of pure cochlear otosclerosis with sensorineural HL. Furthermore, MRI is paramount when evaluating postoperative sensorineural HL and/or vertigo. In this rather dramatic situation, signs of labyrinthitis or hemorrhage have important diagnostic utility. Also, in cochlear implant candidates with far advanced otosclerosis, MRI is probably the most valuable tool in the assessment of cochlear patency and risk of postoperative facial nerve stimulation. Finally, promising contributions of MRI in otosclerosis include the follow-up of patients with active disease submitted to medical treatment and the evaluation of secondary endolymphatic hydrops. Regarding the former, little is known about the criteria to initiate and terminate the therapy and the protocols are widely variable across centers. Thus, the use of MRI might serve as a future guidance to the identification of active foci, which might benefit from the use of bisphosphonates. In cases of patients with otosclerosis presenting with atypical features such as episodic vertigo and aural fullness, avant-garde MRI protocols might accurately determine dilation of the membranous labyrinth compatible with secondary EH. These patients seem to be prone to intraoperative gusher and worse surgical outcomes and are likely to respond to different treatment approaches.
Final Comments
Imaging studies yield valuable data, which might complement the clinical evaluation of patients with otosclerosis in different situations during their follow-up, since the diagnosis up to the investigation of eventual postoperative complications. In many of these scenarios, the use of CT scans and/or MRI is legitimate and yields essential information to guide clinical decisions. The routine use of imaging for diagnosis and preoperative evaluation remains arguable, even though there has been increasing evidence of the value of CT findings in predicting surgical risks and outcomes for a large number of patients.
References
- 1.Vicente AdeO, Yamashita H K, Albernaz P L, Penido NdeO, Penido N DO, Paulo S. Computed tomography in the diagnosis of otosclerosis. Otolaryngol Head Neck Surg. 2006;134(04):685–692. doi: 10.1016/j.otohns.2005.11.030. [DOI] [PubMed] [Google Scholar]
- 2.Goh J PN, Chan L L, Tan T Y. MRI of cochlear otosclerosis. Br J Radiol. 2002;75(894):502–505. doi: 10.1259/bjr.75.894.750502. [DOI] [PubMed] [Google Scholar]
- 3.Glasscock M, Shambaugh G. Philadelphia: WB Saunders; 1990. Surgery of the Ear . 4th ed . [Google Scholar]
- 4.Swartz J D, Faerber E N, Wolfson R J, Marlowe F I. Fenestral otosclerosis: significance of preoperative CT evaluation. Radiology. 1984;151(03):703–707. doi: 10.1148/radiology.151.3.6718730. [DOI] [PubMed] [Google Scholar]
- 5.Purohit B, Hermans R, Op de Beeck K. Imaging in otosclerosis: A pictorial review. Insights Imaging. 2014;5(02):245–252. doi: 10.1007/s13244-014-0313-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Valvassori G E. Imaging of otosclerosis. Otolaryngol Clin North Am. 1993;26(03):359–371. [PubMed] [Google Scholar]
- 7.Schwartz J, Mukherji S. New York: Thieme; 2009. The Inner Ear and Otodystrophies; pp. 298–411. [Google Scholar]
- 8.Lee T C, Aviv R I, Chen J M, Nedzelski J M, Fox A J, Symons S P. CT grading of otosclerosis. AJNR Am J Neuroradiol. 2009;30(07):1435–1439. doi: 10.3174/ajnr.A1558. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Chole R A, McKenna M. Pathophysiology of otosclerosis. Otol Neurotol. 2001;22(02):249–257. doi: 10.1097/00129492-200103000-00023. [DOI] [PubMed] [Google Scholar]
- 10.Wolfovitz A, Luntz M. Impact of Imaging in Management of Otosclerosis. Otolaryngol Clin North Am. 2018;51(02):343–355. doi: 10.1016/j.otc.2017.11.005. [DOI] [PubMed] [Google Scholar]
- 11.Priya S R, Singh P P, Upreti L, Vaid L. High resolution computed tomography in stapedial otosclerosis. Indian J Otolaryngol Head Neck Surg. 2013;65 03:505–511. doi: 10.1007/s12070-011-0412-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Cherukupally S R, Merchant S N, Rosowski J J. Correlations between pathologic changes in the stapes and conductive hearing loss in otosclerosis. Ann Otol Rhinol Laryngol. 1998;107(04):319–326. doi: 10.1177/000348949810700410. [DOI] [PubMed] [Google Scholar]
- 13.Shin Y J, Fraysse B, Deguine O, Cognard C, Charlet J P, Sévely A. Sensorineural hearing loss and otosclerosis: a clinical and radiologic survey of 437 cases. Acta Otolaryngol. 2001;121(02):200–204. doi: 10.1080/000164801300043505. [DOI] [PubMed] [Google Scholar]
- 14.Karosi T, Csomor P, Sziklai I. The value of HRCT in stapes fixations corresponding to hearing thresholds and histologic findings. Otol Neurotol. 2012;33(08):1300–1307. doi: 10.1097/MAO.0b013e31826352ad. [DOI] [PubMed] [Google Scholar]
- 15.Dudau C, Salim F, Jiang D, Connor S EJ. Diagnostic efficacy and therapeutic impact of computed tomography in the evaluation of clinically suspected otosclerosis. Eur Radiol. 2017;27(03):1195–1201. doi: 10.1007/s00330-016-4446-8. [DOI] [PubMed] [Google Scholar]
- 16.Min J Y, Chung W H, Lee W Y. Otosclerosis: incidence of positive findings on temporal bone computed tomography (TBCT) and audiometric correlation in Korean patients. Auris Nasus Larynx. 2010;37(01):23–28. doi: 10.1016/j.anl.2009.04.010. [DOI] [PubMed] [Google Scholar]
- 17.Naumann I C, Porcellini B, Fisch U. Otosclerosis: incidence of positive findings on high-resolution computed tomography and their correlation to audiological test data. Ann Otol Rhinol Laryngol. 2005;114(09):709–716. doi: 10.1177/000348940511400910. [DOI] [PubMed] [Google Scholar]
- 18.Kawase S, Naganawa S, Sone M, Ikeda M, Ishigaki T. Relationship between CT densitometry with a slice thickness of 0.5 mm and audiometry in otosclerosis. Eur Radiol. 2006;16(06):1367–1373. doi: 10.1007/s00330-005-0128-7. [DOI] [PubMed] [Google Scholar]
- 19.Yamashita K, Yoshiura T, Hiwatashi A. The radiological diagnosis of fenestral otosclerosis: the utility of histogram analysis using multidetector row CT. Eur Arch Otorhinolaryngol. 2014;271(12):3277–3282. doi: 10.1007/s00405-014-2933-6. [DOI] [PubMed] [Google Scholar]
- 20.Grayeli A B, Yrieix C S, Imauchi Y, Cyna-Gorse F, Ferrary E, Sterkers O. Temporal bone density measurements using CT in otosclerosis. Acta Otolaryngol. 2004;124(10):1136–1140. doi: 10.1080/00016480410018188. [DOI] [PubMed] [Google Scholar]
- 21.Kutlar G, Koyuncu M, Elmali M, Basar F, Atmaca S. Are computed tomography and densitometric measurements useful in otosclerosis with mixed hearing loss? A retrospective clinical study. Eur Arch Otorhinolaryngol. 2014;271(09):2421–2425. doi: 10.1007/s00405-013-2729-0. [DOI] [PubMed] [Google Scholar]
- 22.Levi C, Gray J E, McCullough E C, Hattery R R. The unreliability of CT numbers as absolute values. AJR Am J Roentgenol. 1982;139(03):443–447. doi: 10.2214/ajr.139.3.443. [DOI] [PubMed] [Google Scholar]
- 23.Yamashita K, Hiwatashi A, Togao O. Additive value of “otosclerosis-weighted” images for the CT diagnosis of fenestral otosclerosis. Acta Radiol. 2017;58(10):1215–1221. doi: 10.1177/0284185116687172. [DOI] [PubMed] [Google Scholar]
- 24.Sanghan N, Chansakul T, Kozin E D, Juliano A F, Curtin H D, Reinshagen K L. Retrospective Review of Otic Capsule Contour and Thickness in Patients with Otosclerosis and Individuals with Normal Hearing on CT. AJNR Am J Neuroradiol. 2018;39(12):2350–2355. doi: 10.3174/ajnr.A5892. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Kanona H, Rana I, Offiah C, Patel N. Importance of a dedicated neuroradiologist in reporting high-resolution computed tomography for otosclerosis: a retrospective comparison study of 40 patients. J Laryngol Otol. 2017;131(06):492–496. doi: 10.1017/S0022215117000561. [DOI] [PubMed] [Google Scholar]
- 26.Brown L A, Mocan B O, Redleaf M I. Diagnostic Protocol for Detecting Otosclerosis on High-Resolution Temporal Bone CT. Ann Otol Rhinol Laryngol. 2019;128(11):1054–1060. doi: 10.1177/0003489419859036. [DOI] [PubMed] [Google Scholar]
- 27.Liktor B, Révész P, Csomor P, Gerlinger I, Sziklai I, Karosi T. Diagnostic value of cone-beam CT in histologically confirmed otosclerosis. Eur Arch Otorhinolaryngol. 2014;271(08):2131–2138. doi: 10.1007/s00405-013-2702-y. [DOI] [PubMed] [Google Scholar]
- 28.Redfors Y D, Gröndahl H G, Hellgren J, Lindfors N, Nilsson I, Möller C. Otosclerosis: anatomy and pathology in the temporal bone assessed by multi-slice and cone-beam CT. Otol Neurotol. 2012;33(06):922–927. doi: 10.1097/MAO.0b013e318259b38c. [DOI] [PubMed] [Google Scholar]
- 29.Virk J S, Singh A, Lingam R K. The role of imaging in the diagnosis and management of otosclerosis. Otol Neurotol. 2013;34(07):e55–e60. doi: 10.1097/MAO.0b013e318298ac96. [DOI] [PubMed] [Google Scholar]
- 30.Wegner I, van Waes A MA, Bittermann A J. A Systematic Review of the Diagnostic Value of CT Imaging in Diagnosing Otosclerosis. Otol Neurotol. 2016;37(01):9–15. doi: 10.1097/MAO.0000000000000924. [DOI] [PubMed] [Google Scholar]
- 31.Rotteveel L J, Proops D W, Ramsden R T, Saeed S R, van Olphen A F, Mylanus E A. Cochlear implantation in 53 patients with otosclerosis: demographics, computed tomographic scanning, surgery, and complications. Otol Neurotol. 2004;25(06):943–952. doi: 10.1097/00129492-200411000-00014. [DOI] [PubMed] [Google Scholar]
- 32.Marshall A H, Fanning N, Symons S, Shipp D, Chen J M, Nedzelski J M. Cochlear implantation in cochlear otosclerosis. Laryngoscope. 2005;115(10):1728–1733. doi: 10.1097/01.mlg.0000171052.34196.ef. [DOI] [PubMed] [Google Scholar]
- 33.Veillon F, Stierle J-L, Dussaix J, Ramos-Taboada L, Riehm S.Imagerie de l'otospongiose: confrontation clinique et imagerie J Radiol 200687(11 Pt 2):1756–1764. [DOI] [PubMed] [Google Scholar]
- 34.Meranger A, David A, Beigner B M, Charpiot A, Tavernier L. Audiometric Results of Stapedotomy Surgery for Otoscelorsis: Influence of the Radiological Stage. Otol Neurotol. 2019;40(02):e75–e81. doi: 10.1097/MAO.0000000000002109. [DOI] [PubMed] [Google Scholar]
- 35.Shin Y J, Deguine O, Cognard C, Sévely A, Manelfe C, Fraysse B. [Reliability of CT scan in the diagnosis of conductive hearing loss with normal tympanic membrane] Rev Laryngol Otol Rhinol (Bord) 2001;122(02):81–84. [PubMed] [Google Scholar]
- 36.Güneri E A, Ada E, Ceryan K, Güneri A. High-resolution computed tomographic evaluation of the cochlear capsule in otosclerosis: relationship between densitometry and sensorineural hearing loss. Ann Otol Rhinol Laryngol. 1996;105(08):659–664. doi: 10.1177/000348949610500813. [DOI] [PubMed] [Google Scholar]
- 37.Marx M, Lagleyre S, Escudé B. Correlations between CT scan findings and hearing thresholds in otosclerosis. Acta Otolaryngol. 2011;131(04):351–357. doi: 10.3109/00016489.2010.549841. [DOI] [PubMed] [Google Scholar]
- 38.Kiyomizu K, Tono T, Yang D, Haruta A, Kodama T, Komune S. Correlation of CT analysis and audiometry in Japanese otosclerosis. Auris Nasus Larynx. 2004;31(02):125–129. doi: 10.1016/j.anl.2004.01.006. [DOI] [PubMed] [Google Scholar]
- 39.Ukkola-Pons E, Ayache D, Pons Y, Ratajczak M, Nioche C, Williams M. Oval window niche height: quantitative evaluation with CT before stapes surgery for otosclerosis. AJNR Am J Neuroradiol. 2013;34(05):1082–1085. doi: 10.3174/ajnr.A3354. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Parra C, Trunet S, Granger B. Imaging Criteria to Predict Surgical Difficulties During Stapes Surgery. Otol Neurotol. 2017;38(06):815–821. doi: 10.1097/MAO.0000000000001417. [DOI] [PubMed] [Google Scholar]
- 41.Raman R, Mathew J, Idikula J. Obliterative otosclerosis. J Laryngol Otol. 1991;105(11):899–900. doi: 10.1017/s0022215100117773. [DOI] [PubMed] [Google Scholar]
- 42.Veillon F. Paris: Médecine - Sciences Flammarion; 1991. Imagerie de l'oreille. [Google Scholar]
- 43.Krouchi L, Callonnec F, Bouchetemblé P, Tollard E, Dehesdin D, Marie J P. Preoperative computed tomography scan may fail to predict perilymphatic gusher. Ann Otol Rhinol Laryngol. 2013;122(06):374–377. doi: 10.1177/000348941312200605. [DOI] [PubMed] [Google Scholar]
- 44.Ungar O J, Handzel O, Cavel O, Oron Y. Superior semicircular canal dehiscence with concomitant otosclerosis-A literature review and case discussion. Clin Case Rep. 2018;6(12):2364–2370. doi: 10.1002/ccr3.1822. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Wang F, Yoshida T, Shimono M. Significance of internal auditory canal diverticula in ears with otosclerosis. Acta Otolaryngol. 2018;138(12):1066–1069. doi: 10.1080/00016489.2018.1521526. [DOI] [PubMed] [Google Scholar]
- 46.Puac P, Rodríguez A, Lin H C. Cavitary plaques in otospongiosis: CT findings and clinical implications. AJNR Am J Neuroradiol. 2018;39(06):1135–1139. doi: 10.3174/ajnr.A5613. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Shim Y J, Bae Y J, An G S. Involvement of the Internal Auditory Canal in Subjects With Cochlear Otosclerosis: A Less Acknowledged Third Window That Affects Surgical Outcome. Otol Neurotol. 2019;40(03):e186–e190. doi: 10.1097/MAO.0000000000002144. [DOI] [PubMed] [Google Scholar]
- 48.Silbergleit R, Quint D J, Mehta B A, Patel S C, Metes J J, Noujaim S E. The persistent stapedial artery. AJNR Am J Neuroradiol. 2000;21(03):572–577. doi: 10.1097/00129492-200111000-00044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.McElveen J T, Jr, Kutz J W., Jr Controversies in the Evaluation and Management of Otosclerosis. Otolaryngol Clin North Am. 2018;51(02):487–499. doi: 10.1016/j.otc.2017.11.017. [DOI] [PubMed] [Google Scholar]
- 50.Sone M, Yoshida T, Sugimoto S. Magnetic resonance imaging evaluation of endolymphatic hydrops andpost-operative findings in cases with otosclerosis. Acta Otolaryngol. 2017;137(03):242–245. doi: 10.1080/00016489.2016.1232862. [DOI] [PubMed] [Google Scholar]
- 51.Lombardo F, De Cori S, Aghakhanyan G. 3D-Flair sequence at 3T in cochlear otosclerosis. Eur Radiol. 2016;26(10):3744–3751. doi: 10.1007/s00330-015-4170-9. [DOI] [PubMed] [Google Scholar]
- 52.Berrettini S, Lombardo F, Bruschini L. 3D fluid attenuated inversion recovery (FLAIR) magnetic resonance imaging at different stages of otosclerosis. Eur Arch Otorhinolaryngol. 2018;275(11):2643–2652. doi: 10.1007/s00405-018-5093-2. [DOI] [PubMed] [Google Scholar]
- 53.Vicente A de O, Yamashita H K, Cruz O LM, Suzuki F B, Penido N de O. The effectiveness of audiometric evaluation in drug treatment for otospongiosis. Rev Bras Otorrinolaringol (Engl Ed) 2012;78(02):73–79. doi: 10.1590/S1808-86942012000200012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.de Oliveira Vicente A, Chandrasekhar S S, Yamashita H K, Cruz O LM, Barros F A, Penido N O. Magnetic resonance imaging in the evaluation of clinical treatment of otospongiosis: a pilot study. Otolaryngol Head Neck Surg. 2015;152(06):1119–1126. doi: 10.1177/0194599815574698. [DOI] [PubMed] [Google Scholar]
- 55.Vandevoorde A, Williams M T, Ukkola-Pons E, Daval M, Ayache D. Early Postoperative Imaging of the Labyrinth by Cone Beam CT After Stapes Surgery for Otosclerosis With Correlation to Audiovestibular Outcome. Otol Neurotol. 2017;38(02):168–172. doi: 10.1097/MAO.0000000000001306. [DOI] [PubMed] [Google Scholar]
- 56.Yehudai N, Masoud S, Most T, Luntz M. Depth of stapes prosthesis in the vestibule: baseline values and correlation with stapedectomy outcome. Acta Otolaryngol. 2010;130(08):904–908. doi: 10.3109/00016480903555424. [DOI] [PubMed] [Google Scholar]
- 57.Fang Y, Wang B, Galvin J J., III MPR-CT Imaging for Stapes Prosthesis: Accuracy and Clinical Significance. Otol Neurotol. 2016;37(04):321–323. doi: 10.1097/MAO.0000000000000987. [DOI] [PubMed] [Google Scholar]
- 58.Warren F M, Riggs S, Wiggins R H., III Computed tomographic imaging of stapes implants. Otol Neurotol. 2008;29(05):586–592. doi: 10.1097/MAO.0b013e3181758e96. [DOI] [PubMed] [Google Scholar]
- 59.Bajin M D, Mocan BÖ, Saraç S, Sennaroğlu L. Early computed tomography findings of the inner ear after stapes surgery and its clinical correlations. Otol Neurotol. 2013;34(04):639–643. doi: 10.1097/MAO.0b013e31828be1ab. [DOI] [PubMed] [Google Scholar]
- 60.Williams M T, Ayache D. Imaging of the postoperative middle ear. Eur Radiol. 2004;14(03):482–495. doi: 10.1007/s00330-003-2198-8. [DOI] [PubMed] [Google Scholar]
- 61.Ayache D, Lejeune D, Williams M T. Imaging of postoperative sensorineural complications of stapes surgery: a pictorial essay. Adv Otorhinolaryngol. 2007;65:308–313. doi: 10.1159/000098850. [DOI] [PubMed] [Google Scholar]
- 62.Whetstone J, Nguyen A, Nguyen-Huynh A, Hamilton B E. Surgical and clinical confirmation of temporal bone CT findings in patients with otosclerosis with failed stapes surgery. AJNR Am J Neuroradiol. 2014;35(06):1195–1201. doi: 10.3174/ajnr.A3829. [DOI] [PMC free article] [PubMed] [Google Scholar]