

TEACHING POINTS
Patient preparation: Standard preoperative staging workup for malignancy in appropriate patients.
Patient position: The patient is placed in the supine position with 5 laparoscopic port sites planned. A left-side-down position is used throughout the laparoscopic dissection.
Critical steps: Intracorporeal ligation and division of the bowel and mesentery followed by specimen withdrawal and extracorporeal anastomosis creation through a right upper quadrant incision.
Technical pearls/tips: The right upper quadrant port site is extended for creation of the off-midline transverse extraction incision, which is associated with a decreased risk of future hernia formation. By performing an intracorporeal division of the bowel and mesentery, the specimen is able to be extracted longitudinally, which minimizes the size of the incision used for extraction.
Potential Areas for Injury/Complication: As with any right hemicolectomy, care is taken to avoid injury to the ureter. Additionally, if the omentum is not adequately dissected off of the transverse colon, the extraction incision may become unnecessarily large.
VIDEO SUMMARY
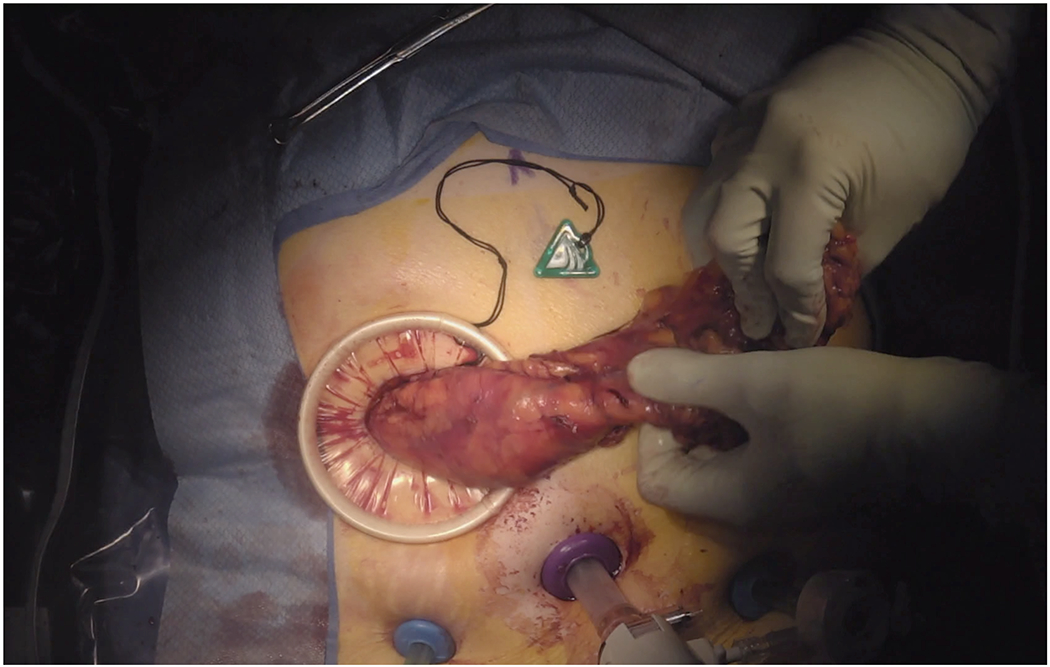
This video demonstrates a laparoscopic right hemicolectomy for malignancy with intracorporeal division of the bowel and mesentery and extracorporeal ileocolic anastomosis. After complete mobilization of the right colon and mesenteric dissection, intracorporeal division of the bowel and mesentery is performed, allowing for longitudinal extraction of the specimen and thus minimization of the extraction site incision size. The right upper quadrant port is extended to create this off-midline site for specimen extraction and anastomosis creation.
KEY IMAGE.
Acknowledgments
Funding/Support: Research reported in this article was supported by award T32CA163177 (Dr. Kane) from the National Institutes of Health. The content is solely the responsibility of the authors and does not necessarily represent the official view of the National Institutes of Health.
Footnotes
Financial Disclosures: None reported.
Proof of Consent: Obtained
See video on DCR YouTube Channel https://youtu.be/a1T8w9-Qc1s