

Incidence rates of cervical cancer have declined dramatically in Canada over the last 3 decades, from 19.4 per 100 000 women in 1971 to 8.4 per 100 000 women as estimated in 2000.1 The effectiveness of Papanicolaou smear screening for cervical cancer in reducing morbidity and mortality has been well documented in many countries, including Canada.2,3,4,5,6 Up to 90% of cervical cancers are of the squamous cell type, whereas the majority of the remainder are adenocarcinoma and the less common adenosquamous carcinoma. Recent studies from Sweden,5 the United States7 and Australia8 have reported that the incidence of invasive cervical adenocarcinoma, which used to account for 10%–15% of all cervical cancers, has been steadily increasing in young women,9 even as the overall incidence of cervical cancer has declined. The cause of the increase is unclear, but it is of concern because studies have shown a poorer prognosis for patients with cervical adenocarcinoma than for those with squamous cell carcinoma.9,10 At diagnosis, adenocarcinomas tend to be larger and exhibit a propensity for early lymphatic and hematogenous metastasis.9,11 Few reports are available on the incidence of adenosquamous carcinoma, although a recent study indicated that it was stable.4 No analysis in Canada of incidence trends of cervical cancer by histological subtype has been reported.
Cancer incidence data were obtained from the Canadian Cancer Registry. Because information on the histological classification of cervical cancer was not consistently recorded by all provincial and territorial cancer registries, this analysis only used data for Ontario, Saskatchewan and British Columbia from 1970 through 1996. The 3 provincial cancer registries used the Systematized Nomenclature of Pathology for histological classification until 1978. All those records were subsequently converted to the International Classification of Disease for Oncology (ICD-O) codes. Squamous cell carcinoma of the cervix was coded as 805–808, adenocarcinoma was coded as 814–842, 844–848, 857, 911 and adenosquamous carcinoma as 856 in the ICD-O. Annual population estimates for the 3 provinces were obtained from the Demography Division of Statistics Canada. Age-adjusted rates were calculated by using direct standardization, with the 1991 Canadian population serving as the standard. The temporal trends in the incidence were examined using Poisson regression modelling of annual rates for specific age groups (20–34, 35–49, 50–64 and 65–79 years) as well as for all ages. The average annual percent changes (AAPC) and the 95% confidence intervals were derived from corresponding regression coefficients of these models during the study period.
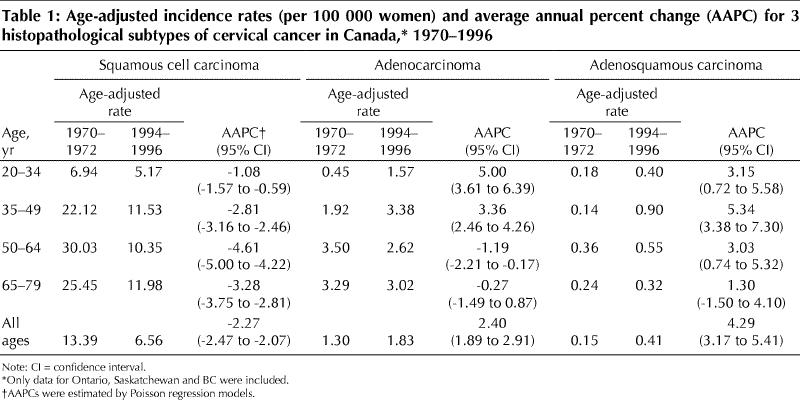
Our results showed that the overall age-adjusted incidence rates of cervical squamous cell carcinoma declined by 51%, from 13.39 per 100 000 women in 1970–1972 to 6.56 per 100 000 women in 1994–1996. Conversely, incidence rates of adenocarcinoma and adenosquamous carcinoma increased considerably, from 1.30 and 0.15 per 100 000 women respectively, in 1970–1972, to 1.83 and 0.41 per 100 000 women respectively, in 1994–1996. Further analysis showed that the observed increase in overall incidence rates of adenocarcinoma and adenosquamous carcinoma was mainly observed in women aged 20–49 years. The risk of developing such invasive carcinomas of the cervix in the 20–34 year and 35–49 year age groups trebled or doubled respectively, over that period. The incidence rates of cervical adenocarcinoma for older women decreased slightly (Table 1).
Table 1
There were no major documented changes in the histological classification of cervical tumours, so the results are unlikely to have been caused by simple shifts of diagnosis between tumour types.9 Well-established risk factors for cervical squamous cell carcinoma, including lower social class or cigarette smoking, do not appear to play a major role in the cause of adenocarcinoma of the cervix.9,10 Earlier studies have suggested an association between several risk factors including oral contraceptive use, human papillomavirus (HPV) type 18 infection and obesity and invasive cervical adenocarcinoma and adenosquamous carcinoma.9,10,12 Current knowledge regarding these factors, however, still cannot entirely explain the recent increase in these specific subtypes of invasive carcinomas of the cervix. As reported from Sweden,5 the United States7 and Australia,8 there is also an increasing trend in the incidence of cervical adenocarcima in younger women, possibly due to changes in sexual habits and increased transmission of HPV. It is uncertain whether such an explanation can be applied to the increase that we observed among younger women in Canada.
Screening for cervical cancer was introduced throughout Canada in the late 1960s. Our results show that there were large reductions in the incidence of cervical squamous cell carcinoma in the population, especially in older women, between 1970 and 1996. The observation that temporal trends in adenocarcinoma and adenosquamous carcinoma of the cervix appear to be in contrast to those of squamous cell carcinoma may reflect the effects of screening practices for cervical cancer in Canada. It could be that Pap smear screening is less efficient, or even of no benefit, for adenocarcinomas and adenosquamous carcinomas of the cervix7,11 or that the risk factors are more pertinent to younger women,5,10,12 or both. We suggest that well-designed epidemiological studies concerning the causes of adenocarcinoma and adenosquamous carcinoma are warranted, as is the development of newer and more sensitive screening methods for these 2 particular forms of cervical carcinoma. Furthermore, the changing patterns of histology-specific cervical cancer incidence may emphasize the importance of cancer surveillance according to histopathological subtype.
Footnotes
This article has been peer reviewed.
Acknowledgement: The authors gratefully acknowledge the provincial cancer registries for providing the cancer incidence data to the Canadian Cancer Registry at Statistics Canada.
Competing interests: None declared.
Reprint requests to: Dr. Yang Mao, Cancer Bureau, LCDC Building #6, Tunney's Pasture, AL 0601C1, Ottawa ON K1A 0L2; fax 613 941-2057; yang_mao@hc-sc.gc.ca
References
- 1.National Cancer Institute of Canada. Canadian Cancer Statistics 2000. Toronto: The Institute; 2000. p. 17-38.
- 2.Pettersson F, Björkholm E, Näslund I. Evaluation of screening for cervical cancer in Sweden: trends in incidence and mortality 1958–1980. Int J Epidemiol 1985;14:521-7. [DOI] [PubMed]
- 3.Anderson GH, Boyes DA, Benedet JL, Le Riche JC, Matisie JP, Suen KC, et al. Organisation and results of the cervical cytology screening programme in British Columbia, 1955–85. BMJ 1988;296:975-8. [DOI] [PMC free article] [PubMed]
- 4.Quinn M, Babb P, Jones J, Allen E, on behalf of the United Kingdom Association of Cancer Registries. Effect of screening on incidence of and mortality from cancer of the cervix in England: evaluation based on routinely collected statistics. BMJ 1999;318:904-7. [DOI] [PMC free article] [PubMed]
- 5.Bergstrom R, Sparen P, Adami HO. Trends in cancer of the cervix uteri in Sweden following cytological screening. Br J Cancer 1999;81:159-66. [DOI] [PMC free article] [PubMed]
- 6.Miller AB, Lindsay J, Hill GB. Mortality from cancer of the uterus in Canada and its relationship to screening for cancer of the cervix. Int J Cancer 1976; 17:602-12. [DOI] [PubMed]
- 7.Zheng T, Holford TR, Ma Z, Chen Y, Liu W, Ward BA, et al. The continuing increase in adenocarcinoma of the uterine cervix: a birth cohort phenomenon. Int J Epidemiol 1996;25:252-8. [DOI] [PubMed]
- 8.Armstrong B, Holman D. Increasing mortality from cancer of the cervix in young Australian women. Med J Aust 1981;9:460-2. [DOI] [PubMed]
- 9.Wharton V. Neoplasms of the cervix. In: Holland JF, Frei E III, Bast RC Jr, Kufe DW, Morton DL, Weichselbaum RR, editors. Cancer medicine. Vol. II. 4th ed. Toronto: Williams & Wilkins; 1995. p. 2227-61.
- 10.Kjaer SK, Brinton LA. Adenocarcinomas of the uterine cervix: the epidemiology of an increasing problem. Epidemiol Rev 1993;15:486-98. [DOI] [PubMed]
- 11.Mitchell H, Medley G, Gordon I, Giles G. Cervical cytology reported as negative and risk of adenocarcinoma of the cervix: no strong evidence of benefit. Br J Cancer 1995;71:894-7. [DOI] [PMC free article] [PubMed]
- 12.Gordon AN, Bornstein J, Kaufman RH. Human papillomavirus associated with adenocarcinoma and adenosquamous carcinoma of the cervix: analysis by in situ hybridization. Gynecol Oncol 1989;35:345-8. [DOI] [PubMed]