

The case
Mr. P is a 45-year-old airplane mechanic with a 5-year history of intermittent neck pain, occipital headaches, bilateral shoulder pain, interscapular pain and left arm pain. His condition has not improved with conservative management consisting of neck support with a soft collar, range of motion and isometric neck exercises, and analgesics. Over the last 12 months, his symptoms have become worse and more persistent. His most recent physical examination revealed decreased lateral flexion of the neck. Neck extension and head compression reproduce his neck, shoulder and interscapular pain. Motor and sensory functions are normal. He has hyperreflexia on the left side and Hoffmann's sign (finger jerk) bilaterally.
Neck pain is a common problem in ambulatory medical practice. Slightly more than 50% of adults experience neck pain at some time. In daily practice, it is useful and practical to deal with every patient with neck pain using an organized approach. I have found that thinking through the following series of points is helpful in organizing the management of patients with neck pain.
In most cases of neck pain, no clear-cut underlying definable pathology can be identified. These patients should be managed conservatively, with the aim of preventing disability and controlling symptoms. In a minority of cases, pain can be the result of varied pathology. It is important to identify the pathology early so that these patients can be managed properly without undue consequence.
The causes of neck pain
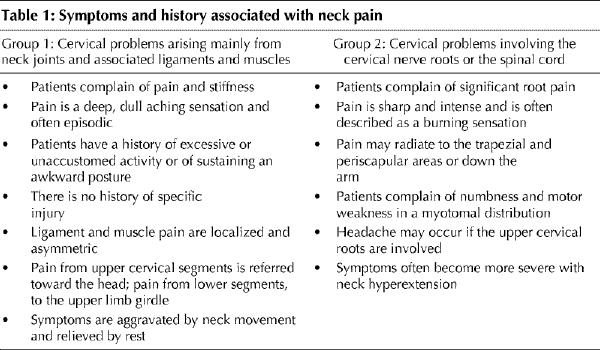
Cervical problems can be divided into 2 main groups: those arising mainly from the joints and associated ligaments and muscles of the neck and those involving the cervical nerve roots or the spinal cord.
The pathologic causes of these problems are
· injury or degeneration affecting muscles or ligaments, soft-tissue strain (the term cervical spondylosis is commonly used for these conditions)
· inflammation, for example, rheumatoid arthritis, ankylosing spondylitis
· infection, for example, discitis, epidural abscess, meningitis
· infiltration, for example, metastatic carcinoma, osteoid osteoma, spinal cord tumours
When confronted with a patient with neck pain, a physician must, first, determine to which of the 2 clinical groups the patient belongs and, second, identify any underlying pathology. Careful history-taking and a proper physical examination are usually sufficient (Table 1), although at times laboratory tests or imaging are needed to establish or confirm a diagnosis.
Table 1
History
In taking the patient's history, the physician should always consider the mode of onset, duration and location of the neck pain; associated symptoms, such as pain elsewhere (especially in other joints); weakness; sensory disturbances; gait disorders; vertigo; visual disturbance; stiffness; deformity; constitutional symptoms such as fever, anorexia and weight loss; and comorbid conditions, such as malignancy and infections.
Group 1: Problems arising mainly from the neck joints and associated ligaments and muscles
Most patients in this group complain of pain and stiffness. They usually have a history of excessive or unaccustomed activity or of sustaining an awkward posture (e.g., as in painting a ceiling). In general, there is no history of a specific injury. Ligament and muscle pain tend to be localized and asymmetric. Pain that arises from joints or discs is usually described as a deep, dull aching sensation. Pain from the upper cervical segments is referred toward the head, and pain from the lower segments is referred to the upper limb girdle (Fig. 1).
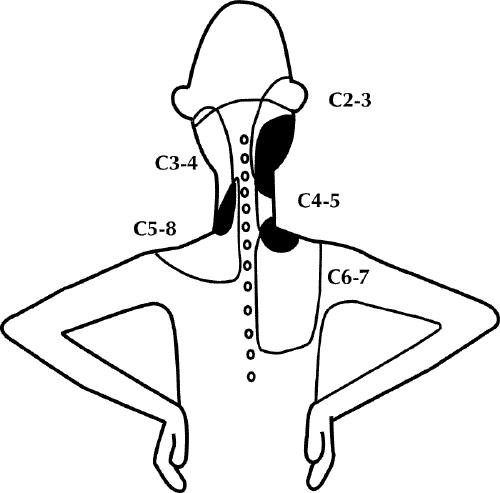
Fig. 1: Pattern of pain referred from the cervical segments. Photo by: Natalia Ng
Symptoms are usually aggravated by neck movement and relieved by rest. The pain is often episodic, which is a reassuring feature, because sinister pathologic processes often produce symptoms that are relentless and progressive.
The C2–3 facet joints may be the source of occipital headache. It is usually dull and may be a referred pain through the occipital nerve. The prevalence of this phenomenon is unclear. The pathology is likely to be a degenerative process.
Group 2: Problems involving the cervical nerve roots or the spinal cord
Patients with nerve root involvement complain of significant root pain, which is usually sharp, intense and often described as a burning sensation. It can radiate out to the trapezial and periscapular areas or down the arm in a dermatomal distribution. Many patients also complain of numbness and motor weakness in a myotomal distribution. Headache may occur if the upper cervical roots are involved. The symptoms often correlate with specific head positions; they become more severe with neck hyperextension, particularly when the head is tilted toward the affected extremity.
Myelopathy is an uncommon complication of cervical spondylosis that is usually not recognized until late in the course of disease. Patients with spinal cord compression may suffer many years of neck, shoulder and arm pain before their condition is diagnosed correctly. It is often accompanied by the gradual onset of shock-like sensation spreading down the spine and possibly into all 4 extremities. There may be lower motor neuron weakness at the level of the lesion. Myelopathy commonly occurs at the level of the fifth cervical vertebra and affects shoulder abduction (deltoid muscle) and external rotation (infraspinous muscle). It may also be associated with Hoffmann's sign (finger jerk), difficulty in walking and clumsiness of hand movement.
Physical examination
The physical examination should begin with a general assessment. Although most neck pain is caused by local mechanical problems, it can be part of a systemic medical problem. The physician should look for evidence of weight loss, pallor suggestive of anemia, adenopathy and abnormalities of the heart, chest and abdomen. Abnormalities of posture, movement, facial expression and gesture should be noted. Finally, cervical problems often require examination of the shoulders, arms and the peripheral nervous system.
Local assessment
Further examination should include careful inspection of the skin and assessment of the position of the head and neck. The physician should palpate the anterior and posterior structures of the neck, especially the spinous processes, facet joints, paraspinal muscles and soft tissues, for tenderness. The temporal artery should be checked for tenderness and induration to ensure that temporal arteritis is not the cause of the neck and shoulder pain. One should also look for tenderness and enlargement of the lymph nodes, thyroid gland and salivary gland, because pathology in these structures could also cause neck or shoulder pain.
The physician should examine neck movement in 3 planes, flexion-extension, left-right rotation and left-right lateral flexion, and should compare active and passive movement. Active movement by the patient may be restricted by pain. Most mechanical neck problems are caused by local injury or wear and tear. Lesions are usually asymmetric, and the range of movement will be asymmetrically painful or limited. Inflammatory or neoplastic disorders, on the other hand, are widespread and more or less symmetric; thus, pain distribution and movement restriction will also be symmetric.
Neurologic assessment
The physician should determine the level of sensory and motor involvement. Hoffmann's and Babinski's signs, gait disorders and spasticity will only occur in patients with spinal cord involvement. Bilateral or multiple-level involvement usually implies serious pathology.
The sensory distribution of C2–4 nerve roots is similar to that illustrated in Fig. 1. There is no clinical motor involvement at these levels:
· C2 — jaw, occipital area
· C3 — occipital area, posterior aspect of neck
· C4 — neck, trapezial area
Fig. 2 illustrates the sensory distribution of C5–8 nerve roots. The motor involvement of C5–8 nerve roots is shown in Fig. 3. Reflex tests for C5–7 nerve roots are depicted in Fig. 4 (there is no reflex test for C8).
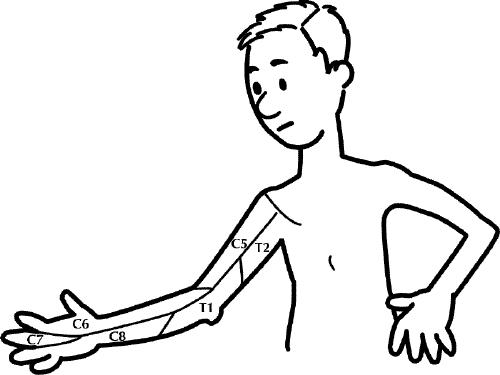
Fig. 2: Sensory distribution of C5–8 nerve roots. Photo by: Natalia Ng
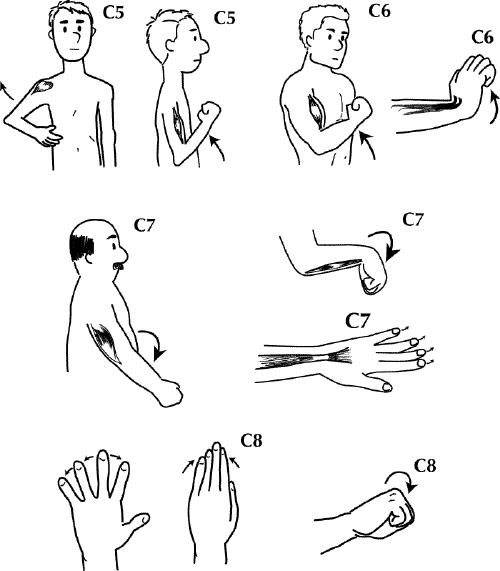
Fig. 3: Motor distribution of C5–8 nerve roots: C5, deltoid and biceps; C6, biceps and wrist extensors; C7, triceps, wrist flexors and finger extensors; C8, interossei muscles and finger flexors. Photo by: Natalia Ng
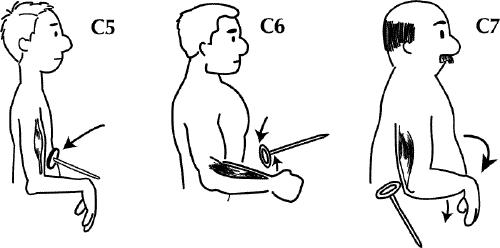
Fig. 4: Reflex tests for C5–7. Photo by: Natalia Ng
Features of spinal cord pressure may occur with lesions at any level. Symptoms usually start with pain in the neck, followed by weakness and a shock-like sensation in the arms or in all 4 extremities. Neck movement, especially cervical flexion (Lhermitte's sign), may provoke paresthesias in the arms or in all 4 extremities. Motor weakness, when present, usually shows features of several cervical levels of involvement and is often asymmetric, affecting one or both arms or the legs. Difficulty in walking may be observed in the presence of pyramidal tract involvement, because compression invariably has some effect on both the posterior and the lateral column of the spinal cord. The legs show spastic weakness with hyperreflexia and Babinski's sign. Vibration and position sensation are often reduced.
Differential diagnosis
After establishing whether the problem is neurologic or is arising from the joints, the physician must identify the cause. A history of injury, recent weight loss and morning stiffness lasting longer than half an hour that involves areas other than the neck should alert the clinician to the possibility of injury, infection or inflammation. A careful general physical examination will confirm these possibilities.
Myelopathy may be a result of rheumatoid arthritis in the C1 and 2 vertebrae. Temporal arteritis may be the cause of occipital or frontal headache. Peripheral nerve entrapment such as carpal tunnel syndrome may mimic C6–7 radiculopathy from the sensory standpoint. Whiplash-associated disorders are cervical hyperextension injuries that are commonly associated with motor vehicle collisions. Although the injury mechanism is unique, patients with whiplash-associated disorders should be treated in the same way as other patients with neck pain. Patients with difficulty swallowing and anterior neck pain immediately after whiplash injury may have more extensive neck injury than patients without these symptoms.
Psychosocial or economic factors may play a role in maintaining disability among patients with chronic neck pain. In this setting, it is important to identify these factors and deal with them accordingly. Careful history-taking and a proper physical examination will help to ensure that no organic disease process is overlooked.
Further investigation
In a patient with a 2–3-week history of neck pain, no nerve root or spinal cord involvement and no history of injury, no further investigation is necessary. In all other circumstances, the physician should exclude instability or pathologic changes in the bone by ordering radiographs of the cervical spine in anteroposterior, lateral and oblique views. The oblique view of the cervical spine can show narrowing of the neural foramina. Cervical instability may be visualized on dynamic flexion and extension films. A decrease or reversal of cervical lordosis, revealed by radiography, may be the result of muscle pain or spasm.
Narrowing of disc space and the neural foramina and anterior and posterior osteophyte formation are commonly seen at levels C5–6 and C6–7. These changes take years to develop, but they occur in about 50% of patients over 50 years of age and are not usually the cause of a patient's current symptoms. Patients only develop symptoms when additional factors such as soft-tissue sprain or nerve root irritation occur. The clinician must be careful in explaining the significance of these changes in the current context, because patients are often upset by the use of words such as “degeneration” and “severe osteoarthritis.”
Special imaging techniques, such as CT and MRI of the cervical spine, are indicated for a patient with a neurologic deficit or injury or one who may have some form of disease process in the cervical spine (e.g., infection or rheumatoid arthritis).
A hemogram, measurement of the erythrocyte sedimentation rate and other laboratory investigations, such as liver function tests and serum protein electrophoresis, are indicated when systemic illness is suspected.
Managing the patient
An important feature of management is establishing the prognosis. About two-thirds of patients with neck pain without a neurologic deficit (group 1) or systemic illness will have a favourable long-term outcome. However, one-third will continue to experience pain that will interfere with their lifestyle to some degree. Patients with radicular pain (group 2) often do not achieve complete pain relief.
Neck pain, whether acute or chronic, is commonly treated with physical or manual therapies. These include ultrasonography, ice or hot packs, electrical stimulation, avoidance of activities that produce pain, traction and passive mobilization. These “conventional” interventions may have some short-term effect in reducing pain and improving range of movement of the neck; there are no long-term effects. On the other hand, exercise has been associated with a long-term positive effect.
For group 1 patients, and patients with no clear-cut underlying pathology, management should be conservative. The goal should be to reduce pain, improve the patient's tolerance of activity and work, encourage wellness and prevent deconditioning and the development of illness behaviour, disability and chronicity. The judicious use of analgesics is useful in short-term pain management. The prolonged use of a cervical collar or cervical immobilization should be avoided. A rolled towel around the neck supporting the cervical spine will help the patient rest better at night. The patient should be encouraged to remain active and follow a program of active physiotherapy, such as neck and shoulder girdle exercises. Passive treatments such as the application of heat or cold, acupuncture and massage therapy should be discouraged, unless they are followed in conjunction with exercises.
Physicians should always follow up with their patients regarding the type of physiotherapy they are receiving. Timely visits will serve to reassure patients about their progress, ensure that they are remaining active and allow the physician to watch for the appearance of neurologic signs and systemic illness.
For patients with neurologic involvement (group 2), initial conservative management is appropriate. When the neurologic problem becomes progressive or disabling, it is necessary to conduct further investigations to determine whether any of the pathologic causes listed at the beginning of this article are present. CT and MRI are useful in identifying the causative lesion. Consultation with a specialist may be necessary in order to establish the diagnosis and carry out appropriate treatment.
Treatment for Mr. P
MRI of Mr. P's cervical spine revealed bulging discs at levels C4–5, C5–6 and C6–7, with significant spinal cord compression at these levels indicative of spondylotic myelopathy. He underwent discectomy and, 2 years later, his symptoms were resolved, except for occasional neck pain due to degenerative changes.
Key points .
Slightly more than 50% of adults experience neck pain at some time.
In cases of neck pain, a physician must first determine whether it arises from the joints, ligaments and muscles of the neck (group 1) or from the cervical nerve roots and the spinal cord (group 2).
The second step is to identify the underlying pathology, which may include injury or degeneration, inflammation, infection or infiltration. This step is important, even though in the majority of cases no definable underlying pathology can be identified.
Physical examination should include a general assessment, because neck pain may be part of a systemic medical problem.
Further examination should include assessment of the position of the head and neck, checking for tenderness, and investigation of active and passive neck movement.
When the problem is neurologic, the physician should determine the level of the spine from which it originates.
A history of injury, recent weight loss and prolonged or extensive morning stiffness will alert the clinician to the possibility of injury, infection or inflammation.
Rheumatoid arthritis, temporal arteritis, carpal tunnel syndrome and whiplash-associated disorders must be considered in the differential diagnosis.
When patients have neck pain that lasts for more than a few weeks, nerve root or spinal cord involvement, or a history of injury, the physician should order radiographs to check for instability or pathologic changes in the cervical spine.
Although degeneration in the spine is common in individuals over 50 years of age, such changes become symptomatic only when additional factors such as soft-tissue sprain or nerve root irritation occur.
About two-thirds of group 1 patients with neck pain will have a favourable long-term outcome; group 2 patients often do not achieve complete pain relief.
Acute or chronic neck pain is commonly treated with physical or manual therapies, including ultrasonography, ice or hot packs, electrical stimulation, avoidance of activities that produce pain, traction and passive mobilization.
The physician should continue to see patients who are receiving physiotherapy to reassure them about their progress, ensure that they are remaining active and watch for neurologic signs and systemic illness.
Articles to date in the rheumatology series .
Esdaile JM. Rheumatology: introduction to the series. CMAJ 2000;162(7):1007.
Ensworth S. Rheumatology: 1. Is it arthritis? CMAJ 2000; 162(7):1011-6.
Shojania K. Rheumatology: 2. What laboratory tests are needed? CMAJ 2000;162(8):1157-63.
Reid G, Esdaile JM. Rheumatology: 3. Getting the most out of radiology. CMAJ 2000;162(9):1318-25.
Cibere J. Rheumatology: 4. Acute monoarthritis. CMAJ 2000;162(11):1577-83.
Klinkhoff A. Rheumatology: 5. Diagnosis and management of inflammatory polyarthritis. CMAJ 2000; 162(13):1833-8.
Price GE. Rheumatology: 6. Localized therapy. CMAJ 2000;163(2):176-83.
Huang SHK. Rheumatology: 7. Basics of therapy. CMAJ 2000;163(4):417-23.
Lacaille D. Rheumatology: 8. Advanced therapy. CMAJ 2000;163(6):721-8.
Clark BM. Rheumatology: 9. Physical and occupational therapy in the management of arthitis. CMAJ 2000; 163(8):999-1005.
Brady OH, Masri BA, Garbuz DS, Duncan CP. Rheumatology: 10. Joint replacement of the hip and knee — when to refer and what to expect. CMAJ 2000;163(10):1285-91.
Puttick MPE. Rheumatology: 11. Evaluation of the patient with pain all over. CMAJ 2001;164(2):223-7.
Recommended reading
Mathews JA. Neck pain. In: Klippel JH, Dieppe PA, editors. Practical rheumatology. St. Louis (MO): Mosby; 1995. p. 41-52.
Sweaey RL. Chronic neck pain. Rheum Dis Clin North Am 1996;22:411-39.
Bogduk N. The neck. Baillieres Clin Rheumatol 1999;13:261-85.
Footnotes
This series has been reviewed and endorsed by the Canadian Rheumatology Association.
The Arthritis Society salutes CMAJ for its extensive series of articles on arthritis. The Society believes that this kind of information is crucial to educating physicians about this devastating disease.
This article has been peer reviewed.
Competing interests: None declared.
Reprint requests to: Dr. Ian Tsang, 240-575 West 8th Ave., Vancouver BC V5Z 1C6; fax 604 875-5944