

Abstract
Background:
Pleural effusion (PE) is presenting symptoms of many different diseases and is often a diagnostic challenge. Negative cytology in the malignant PE requires more complicated diagnostic procedures, such as closed pleural biopsy or thoracoscopic pleural biopsy. Not all the patients will be fit for such invasive procedures due to high risk. Tumor markers seem to be a promising alternative and have been proposed to aid in the differentiation of the PE etiology.
Objective:
The objective of the study was to evaluate the diagnostic value of pleural fluid carcinoembryonic antigen (CEA) in differentiation between malignant and nonmalignant PEs and to compare adenosine deaminase (ADA) levels with respect to malignant and nonmalignant PE.
Methodology:
It was a prospective observational study. Patients who presented with undiagnosed exudative PE during the time period 2016–2018 were studied. Pleural fluid was subjected to all routine investigations such as sugar, protein, lactate dehydrogenase, ADA, and CEA.
Results:
A total of 100 patients were included in the study. Fifty-one patients had malignancy. Univariate analysis showed that smoker, previous history of cancer, ADA <20, and CEA of >2.15 were variables associated with malignancy. Multivariate analysis showed pleural fluid CEA >2.15 as only independent risk factor associated with malignancy. The sensitivity of 91.5% and 65% and specificity of 92.5% and 81.4%, respectively, were found for CEA 2.15 ng/dl and ADA <16.5 U/L as plotted from receiver operating characteristic curve. The combined CEA and ADA (2.39 ng/ml and 16.5 U/L) values in pleural fluid had higher sensitivity of 100%.
Conclusion:
Our study demonstrated that pleural fluid CEA levels have a sensitivity of 93.5% and specificity of 73% in diagnosing of malignant PE. ADA levels lesser than 16.5 U/L were seen in patients with malignant PE, but less sensitive and specific compared to CEA. Combined ADA and CEA levels had higher sensitivity than CEA alone.
KEY WORDS: Adenosine deaminase, carcino embryonic antigen, lung cancer, pleural effusion
INTRODUCTION
An umpteen number of diseases can masquerade as a pleural effusion (PE) and establishing a definite cause is often a diagnostic challenge.[1,2,3] The first step, however, is determining the nature of PE (exudate or transudate) that allows the physician to narrow down the list of potential causes and point the direction to further investigations. The next step is to ascertain the etiology of effusion whether malignant or benign. Although pleural fluid cytology is a simple and widely used diagnostic tool for differentiating the origin of the pleural fluid, it is limited by a relatively low sensitivity.[2,3,4] The affirmation of the etiology as malignant in the patient with a negative cytological examination requires more arduous diagnostic procedures, such as a closed pleural biopsy or thoracoscopy.[1,5] Tumor markers seem to be an up-and-coming alternative and have been proposed to aid in the differentiation of PE etiology.[4,5] Several studies have revealed that the level of some tumor markers in the pleural fluid and/or serum is a reliable predictor of malignant PE etiology.[6] Other studies show, however, that the sensitivity, specificity, and diagnostic accuracy of different tumor markers are quite low. Our study aimed to evaluate the diagnostic value of pleural fluid carcinoembryonic antigen (CEA) in differentiating malignant from benign PEs. Pleural fluid cytology or thoracoscopic pleural biopsy was used as the gold standard for diagnosis. The secondary objective was to assess the role of adenosine deaminase (ADA) as a discriminative tool between malignant and nonmalignant effusions.
METHODOLOGY
A prospective, cross-Sectional study for 100 patients who were diagnosed with exudative PE in the department of respiratory medicine was conducted during the time interval between 2016 and 2018.
Inclusion criteria
Adults more than 18 years of age with PE were included if they met the Light's criteria (pleural fluid protein/serum protein >0.5 and fluid lactate dehydrogenase (LDH)/serum LDH >0.6) for exudative effusion.
Exclusion criteria
Patients below the age of 18 years were excluded from the study. Patients with transudative and posttraumatic PEs were also excluded from the study.
The study was approved by the hospital's scientific and ethical committee. Informed consent was taken from all the patients.
A detailed history including symptoms such as cough, pleuritic chest pain, and shortness of breath was elicited from the patients followed by a thorough clinical examination, and necessary investigations were done for all. Diagnostic pleural aspiration was done for all included patients. Pleural fluid was sent for investigations such as ADA, LDH, sugar, protein levels, cytology, and CEA marker. All the patients with an inconclusive cytology report were further subjected to thoracoscopic pleural biopsy for histopathological analysis.
Pleural fluid CEA estimation was done using electrochemiluminescence immunoassay (ECLIA) (Sandwich principle). The total duration of the assay was 18 min.
1st incubation: 10 μL of sample, a biotinylated monoclonal CEA-specific antibody, and a monoclonal CEA-specific antibody labeled with arutheniumcomplex) react to form a sandwich complex
2nd incubation: After addition of streptavidin-coated microparticles, the complex becomes bound to the solid phase via interaction of biotin and streptavidin.
Statistics
Statistical analysis was done using the SPSS Statistics 20 Windows (SPSS Inc., Chicago, USA).
The results are given in mean ± standard deviation for all the continuous variables and in frequency (percentage) for categorical variables. The Pearson's Chi-square test and continuity correction were used for finding the association between two categorical variables. Independent samples t-test was used for comparing the mean protein level between patients with and without cancer. Receiver operating characteristic (ROC) curve for CEA level was plotted for finding the cutoff for discriminating cancer cases, and sensitivity, specificity, and area under the curve were estimated. P < 0.05 was considered statistically significant difference. All tests of statistical significance were two-tailed.
RESULTS
The study included a total of 100 patients, of whom 57 (57%) were male and 43 (43%) were female. Baseline demographics of the patients are shown in Table 1. Our study found the involvement of PE on the left side (49%) to be the most common followed by the right side (41%) and finally bilaterally (10%). As per the chest radiography of patients, effusion was found to be mild in 18%, moderate in 57%, and massive in 25% of patients. The fluid was found to be hemorrhagic in 57% and straw colored in 42% of patients, while one patient was diagnosed to have empyema.
Table 1.
Baseline demographics of the cohort (n=100)
| Baseline demographics | n |
|---|---|
| Gender | |
| Male | 57 |
| Female | 43 |
| Smoking history | |
| Smoker | 44 |
| Nonsmoker | 56 |
| Previous malignancy | |
| Present | 22 |
| Absent | 78 |
| Amount of effusion on chest radiograph | |
| Mild | 18 |
| Moderate | 57 |
| Large | 25 |
| Site of effusion | |
| Left | 49 |
| Right | 41 |
| Bilateral | 10 |
| Color/type of effusion | |
| Straw | 42 |
| Hemorrhagic | 57 |
| Pus | 1 |
| Positive for malignancy | |
| Yes | 59 |
| No | 41 |
Out of 59 patients diagnosed with malignant PE, 52 patients showed ADA levels <20, while in 7 patients, ADA levels were >20. Pleural fluid CEA level was higher in those with cancer (1656.37 [0.452–1207]) than patients without cancer. In our study, the level of CEA was found to be elevated in 33 patients (out of 33) with adenocarcinoma, whereas CEA level was raised in 17 patients (out of 20) with primary carcinoma other than lung and in 5 patients (out of 5) with squamous cell carcinoma. CEA levels were not elevated in patients with neuroendocrine tumors. LDH levels were increased in patients with lung malignancies in this study, but without any statistical significance with P = 0 [Table 2].
Table 2.
Univariate analysis of variables and its association with malignant effusion
| Variable | Cancer | OR (95% CI) | P | |
|---|---|---|---|---|
| Absent | Present | |||
| Sex | ||||
| Male | 22 | 34 | 0.899 (0.400–2.018) | 0.479 |
| Female | 18 | 25 | ||
| Smoking status | ||||
| Nonsmoker | 28 | 28 | 2.583 (1.107–6.030) | 0.021 |
| Smoker | 12 | 31 | ||
| Previous cancer | ||||
| Present | 03 | 19 | 2.761 (0.944–8.069) | 0.003 |
| Absent | 37 | 40 | ||
| ADA | ||||
| >16.5 | 17 | 07 | 0.182 (0.066–0.499) | 0.001 |
| <16.5 | 23 | 52 | ||
| LDH | ||||
| <485 U/L | 21 | 30 | 1.068 (0.478–2.386) | 0.517 |
| >485 U/L | 19 | 29 | ||
| CEA | ||||
| >2.15 | 3 | 54 | 29.983–591.743 | <0.0001 |
| <2.15 | 37 | 05 | ||
OR: Odd’s ratio, CI: Confidence interval, ADA: Adenosine dehydrogenase, LDH: Lactate dehydrogenase, CEA: Carcinoembryonic antigen
Univariate analysis of different variables and its association with malignancy was done. It showed that history of smoking, previous history of cancer, ADA <20, and CEA of >2.15 were associated with malignancy with P < 0.005, while LDH and male sex did not show any statistically significant association with malignancy.
All the variables with P < 0.05 in univariate analysis were subjected to multivariate analysis [Table 3]. It showed pleural fluid CEA as the only independent risk factor associated with malignant effusion.
Table 3.
Multivariate analysis of variables and its association with malignant effusion
| Variable | Presence of cancer | |
|---|---|---|
| OR (95% CI) | P | |
| Smoker | 3.597 (0.611–21.178) | 0.157 |
| Previous cancer | 5.122 (0.624–42.019) | 0.128 |
| ADA | 0.174 (0.024–1.236) | 0.080 |
| CEA | 202.383 (30.009–1364.903) | <0.0001 |
OR: Odd’s ratio, CI: Confidence interval, ADA: Adenosine dehydrogenase, CEA: Carcinoembryonic antigen
In this study, the cutoff value of CEA was 2.15 ng/dl and that of ADA was 16.5 U/L for malignant effusions as plotted from ROC curve, with sensitivity of 91.5% and 65% and specificity of 92.5% and 81.4%, respectively [Figures 1 and 2].
Figure 1.
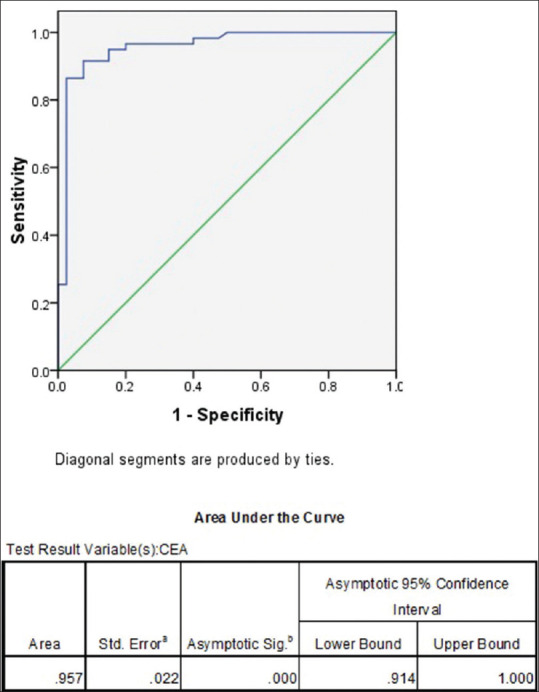
Receiver operating characteristic curve – Pleural fluid carcinoembryonic antigen and malignant effusion
Figure 2.
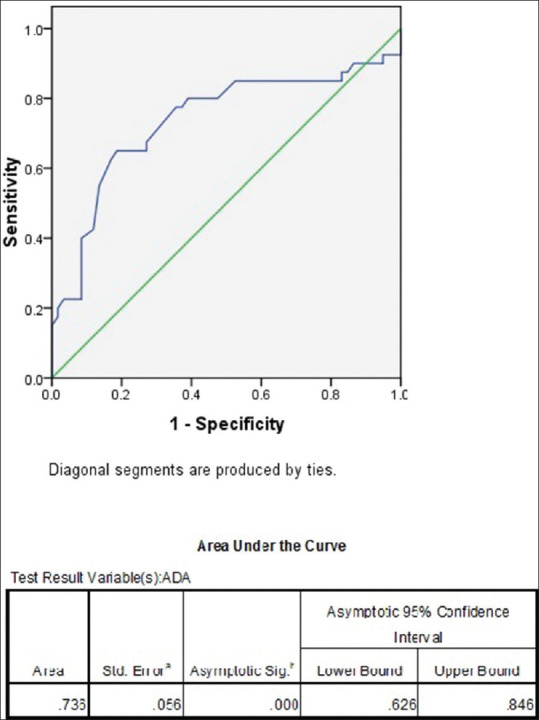
Receiver operating characteristic curve – Pleural fluid adenosine deaminase and malignant effusion
DISCUSSION
Lung cancer is diagnosed in approximately 10 million new cases every year and around 6 million people die from this disease.[7] In cases of malignant effusion, the cytologic examination is important because of its noninvasiveness and the ease of conducting the test. According to reports, repeated thoracentesis can increase the sensitivity of cytology to even 50%–70%.[8] However, repeated cytological examinations can still yield a negative result in those suspected to have a malignant PE. Although thoracoscopy can establish the diagnosis in nearly 90% of patients with malignancy,[9,10,11] this expertise may not be available everywhere and/or may be difficult in patients with a poor performance status.
Approximately 20% of PEs are estimated to be due to malignancy, and around 50% of these are due to primary lung cancer.[6] Several tumor markers in the pleural fluid have been evaluated to distinguish malignant effusion from benign ones. CEA is one such tumor marker that has been studied the most. CEA levels in pleural fluid due to malignancy though shown to be very specific, its sensitivity remains at approximately 29%–77% with variable cutoff values.[12,13,14,15,16,17,18,19,20,21] The assessment of tumor markers in pleural fluid has been proposed as an alternative way of proving a diagnosis of malignant PE. Falling in with this, we evaluated the diagnostic utility of a tumor marker of lung cancer to differentiate malignant from benign effusions.
Previous studies have demonstrated the clinical utility of tumor markers in discriminating various pleural diseases,[10,11,12,13,14,15,16,18] but relying on tumor markers in pleural fluid for diagnosing MPE is still controversial. Regardless, most authors felt that quantification of a panel of tumor markers could improve the cytological diagnosis and should be considered in select cases of indeterminate PEs.
According to the study by Ferrer et al.,[15] CEA was found to be the single best marker in pleural fluid, which was in accordance with previous reports as well. Our study was purported at assessing the diagnostic utility of pleural fluid CEA in patients with exudative PE and its value in differentiating malignant versus nonmalignant PEs. The result was compared with the gold standard of a cytological or histopathological diagnosis using pleural fluid cytology or thoracoscopic pleural biopsy.
Smoking is regarded to be an independent risk factor for developing lung malignancies.[5] Similarly, in this study, 32 patients (72.7%) with cancer had a history of smoking despite that it was not established to be an independent risk factor for association with malignant effusion. The explanation may presumably be due to the small sample size.
This study showed that 19 patients (86.04%) with cancer recorded a previous history of malignancy, which was parallel to the findings by Lee and Chang.[22]
Our study also aimed at assessing the ADA levels, and a cutoff value of <16.5 U/L for suspected malignant PE was obtained using ROC curve. Here, the ADA level showed a specificity of 81.4% and a sensitivity of 65%. Not many studies have been done on evaluating the role of ADA as a tumor marker. In one study done by Mehta et al.,[23] the cutoff for ADA levels in malignancy was taken as 18 U/L and our results were comparable with that of Mehta et al.[23]
When the association of pleural fluid CEA 2.15ng/ml and ADA < 16.5 was checked together for diagnosing malignant pleural effusion, it had specificity of 100% and sensitivity of 74.5%. Accordingly, we report that the specificity for diagnosing the malignant effusion is more when CEA and ADA are combined. Niwa et al.[24] compared CA 19.9, CEA, and ADA for differentiating malignant and benign PE and concluded that combined assays of CA 19.9, CEA, and ADA are useful in differentiating carcinomatous PEs from those of tuberculous origin because of the low incidence of false-negative results (sensitivity 80.5 percent). Similarly, Daniil et al.[25] compared CEA, ADA, and CRP for diagnosing MPE and their results showed that combining tumor markers can improve the accuracy of the diagnosis with a sensitivity of 93%. Since not many studies have been conducted comparing ADA and CEA, the validation of our results requires further studies with a larger sample size. The comparison of the present study CEA with other studies are shown in Table 4.
Table 4.
Comparison of present study with previously published studies
| Studies | PF CEA values used as cut off for malignancy (ng/Ml) | Sensitivity (%) | Specificity (%) |
|---|---|---|---|
| Romero et al.[12] | 3 | 57 | 99 |
| San Jose et al.[13] | 7.2 (1.7*) | 31 (80*) | 93 (48*) |
| Salama et al.[14] | 6 | 64.7 (72.4†) | 95 |
| Ferrer et al.[15] | 40 | 34.9 | 76.7 |
| Miedouge et al.[16] | 6 | 60 (70.5†) | 99 |
| Riantawan et al.[17] | 10 | 77 | 94 |
| Alatas et al.[18] | 3 | 52 | 77 |
| Hernandez et al.[19] | 5.9 | 34 | 97 |
| Villena et al.[20] | 40 | 35 (48†) | 100 |
| Porcel et al.[21] | 50 | 29 | 100 |
| This study | 2.395 | 93.5 | 73 |
*Pleural effusion all neoplasms (PE of pulmonary neoplastic origins), †all Neoplasms(Carcinomas)
In our study, elevated CEA levels in pleural fluid for detecting carcinoma were statistically significant. In the study by Lee et al.[26] to assess the diagnostic value of CEA, neuron-specific enolase, and cytokeratin 19 fragments (CYFRA 21-1) as markers of pleurisy in primary lung cancer, the cutoff value for CEA was taken as 5 ng/ml with a sensitivity of 82% and a specificity of 94%. Nevertheless, in our study, when the cutoff value for CEA level is 2.15 ng/ml as plotted from ROC curve, the sensitivity was 91.5% with a specificity of 92.5%. In a study by Tozzoli et al.,[27] the optimal cutoff for pleural CEA (sensitivity = 71.0%, specificity = 94.7%) was 5 ng/mL. The variation in values can be attributed to the difference in the levels of cutoff values. Comparison of different studies with present study is shown in Table 4.
Strengths and limitations of study
The present study was limited by its small sample size. While our malignant effusion group consisted of not only primary lung but also primary other than lung as well, cases among the major three histologic types were not equal in number. Another limitation was that our study considered only CEA levels and other tumor markers or their combinations were not assessed which may have changed the sensitivity and specificity. Nevertheless, our study was able to detect that ADA levels <16.5 have a specificity of 81% in ruling in malignancy especially in resource-limited settings. In addition, our study stresses that a combination of CEA >2.15 and ADA <16.5, when found in an effusion, potentially identifies patients who warrant further investigations to rule out underlying malignancy.
CONCLUSION
According to previous reports, CEA was found to be the best single screening tumor marker in pleural fluid. Our study demonstrated that pleural fluid CEA of >2.15 had a sensitivity of 93.5% and a specificity of 73% in diagnosing malignant PEs. Likewise, ADA levels lesser than 16.5U/L were observed in patients with malignant PE, but this was less sensitive and specific compared to CEA. Whereas, a combined ADA and CEA levels had a higher specificity than CEA alone for effusions due to cancer. Patients found having pleural fluid CEA >2.15 should strongly be recommended further evaluation with pleural biopsy for confirming the diagnosis.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Sahn SA. The pleura. Am Rev Respir Dis. 1988;138:184–234. doi: 10.1164/ajrccm/138.1.184. [DOI] [PubMed] [Google Scholar]
- 2.Miserocchi G, Agostoni E. Contents of the pleural space. J Appl Physiol. 1971;30:208–13. doi: 10.1152/jappl.1971.30.2.208. [DOI] [PubMed] [Google Scholar]
- 3.Light RW. Lippincott Williams and Wilkins. 4th ed. 2001. Physiology of pleural space. In: Pleural Disease; pp. 8–16. [Google Scholar]
- 4.Light RW. Clinical practice.Pleural effusion. N Engl J Med. 2002;346:1971–7. doi: 10.1056/NEJMcp010731. [DOI] [PubMed] [Google Scholar]
- 5.Sahn SA, Huggins JT. Malignant Pleural effusions, Fishman's Pulmonary Diseases and Disorders. Mc Graw Hill Medical, New York. (5th Edition) 2015:1505–1516. [Google Scholar]
- 6.Marel M, Stastny B, Melínová L, Svandová E, Light RW. Diagnosis of pleural effusions.Experience with clinical studies, 1986 to 1990. Chest. 1995;107:1598–603. doi: 10.1378/chest.107.6.1598. [DOI] [PubMed] [Google Scholar]
- 7.Fenton KN, Richardson JD. Diagnosis and management of malignant pleural effusions. Am J Surg. 1995;170:69–74. doi: 10.1016/s0002-9610(99)80257-8. [DOI] [PubMed] [Google Scholar]
- 8.Nance KV, Shermer RW, Askin FB. Diagnostic efficacy of pleural biopsy as compared with that of pleural fluid examination. Mod Pathol. 1991;4:320–4. [PubMed] [Google Scholar]
- 9.Prakash UB, Reiman HM. Comparison of needle biopsy with cytologic analysis for the evaluation of pleural effusion: analysis of 414 cases. Mayo Clin Proc. 1985;60:158–64. doi: 10.1016/s0025-6196(12)60212-2. [DOI] [PubMed] [Google Scholar]
- 10.Edmondstone WM. Investigation of pleural effusion: comparison between fibreoptic thoracoscopy, needle biopsy and cytology. Respir Med. 1990;84:23–6. doi: 10.1016/s0954-6111(08)80089-3. [DOI] [PubMed] [Google Scholar]
- 11.Light RW. Pleural effusions related to metastatic malignancies. In: Light RW, editor. Pleural Diseases. 4th ed. Philadelphia, PA: Lippincott, Williams & Wilkins; 2001. pp. 108–34. [Google Scholar]
- 12.Romero S, Fernández C, Arriero JM, Espasa A, Candela A, Martín C, et al. CEA, CA 15-3 and CYFRA 21-1 in serum and pleural fluid of patients with pleural effusions. Eur Respir J. 1996;9:17–23. doi: 10.1183/09031936.96.09010017. [DOI] [PubMed] [Google Scholar]
- 13.San Jose ME, Alvarez D, Valdes L, Sarandeses A, Valle JM, Penela P. Utility of tumour markers in the diagnosis of neoplastic pleural effusion. Clin Chim Acta. 1997;265:193–205. doi: 10.1016/s0009-8981(97)00120-4. [DOI] [PubMed] [Google Scholar]
- 14.Salama G, Miédougé M, Rouzaud P, Mauduyt MA, Pujazon MC, Vincent C, et al. Evaluation of pleural CYFRA 21-1 and carcinoembryonic antigen in the diagnosis of malignant pleural effusions. Br J Cancer. 1998;77:472–6. doi: 10.1038/bjc.1998.75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ferrer J, Villarino MA, Encabo G, Felip E, Bermejo B, Vilà S, et al. Diagnostic utility of CYFRA 21-1, carcinoembryonic antigen, CA 125, neuron specific enolase, and squamous cell antigen level determinations in the serum and pleural fluid of patients with pleural effusions. Cancer. 1999;86:1488–95. doi: 10.1002/(sici)1097-0142(19991015)86:8<1488::aid-cncr15>3.0.co;2-y. [DOI] [PubMed] [Google Scholar]
- 16.Miédougé M, Rouzaud P, Salama G, Pujazon MC, Vincent C, Mauduyt MA, et al. Evaluation of seven tumour markers in pleural fluid for the diagnosis of malignant effusions. Br J Cancer. 1999;81:1059–65. doi: 10.1038/sj.bjc.6690807. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Riantawan P, Sangsayan P, Bangpattanasiri K, Rojanaraweewong P. Limited additive value of pleural fluid carcinoembryonic antigen level in malignant pleural effusion. Respiration. 2000;67:24–9. doi: 10.1159/000029458. [DOI] [PubMed] [Google Scholar]
- 18.Alataş F, Alataş O, Metintaş M, Colak O, Harmanci E, Demir S. Diagnostic value of CEA, CA 15-3, CA 19-9, CYFRA 21-1, NSE and TSA assay in pleural effusions. Lung Cancer. 2001;31:9–16. doi: 10.1016/s0169-5002(00)00153-7. [DOI] [PubMed] [Google Scholar]
- 19.Hernández L, Espasa A, Fernández C, Candela A, Martín C, Romero S. CEA and CA 549 in serum and pleural fluid of patients with pleural effusion. Lung Cancer. 2002;36:83–9. doi: 10.1016/s0169-5002(01)00474-3. [DOI] [PubMed] [Google Scholar]
- 20.Villena V, López-Encuentra A, Echave-Sustaeta J, Martín-Escribano P, Ortuño-de-Solo B, Estenoz-Alfaro J. Diagnostic value of CA 549 in pleural fluid. Comparison with CEA, CA 15.3 and CA 72.4. Lung Cancer. 2003;40:289–94. doi: 10.1016/s0169-5002(03)00120-x. [DOI] [PubMed] [Google Scholar]
- 21.Porcel JM, Vives M, Esquerda A, Salud A, Pérez B, Rodríguez-Panadero F. Use of a panel of tumor markers (carcinoembryonic antigen, cancer antigen 125, carbohydrate antigen 15-3, and cytokeratin 19 fragments) in pleural fluid for the differential diagnosis of benign and malignant effusions. Chest. 2004;126:1757–63. doi: 10.1378/chest.126.6.1757. [DOI] [PubMed] [Google Scholar]
- 22.Lee JH, Chang JH. Diagnostic utility of serum and pleural fluid carcinoembryonic antigen, neuron-specific enolase, and cytokeratin 19 fragments in patients with effusions from primary lung cancer. Chest. 2005;128:2298–303. doi: 10.1378/chest.128.4.2298. [DOI] [PubMed] [Google Scholar]
- 23.Mehta AA, Gupta AS, Ahmed S, Rajesh V. Diagnostic utility of adenosine deaminase in exudative pleural effusions. Lung India. 2014;31:142–4. doi: 10.4103/0970-2113.129842. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Niwa Y, Kishimoto H, Shimokata K. Carcinomatous and tu- berculous pleural effusions.Comparison of tumor markers. Chest. 1985;87:351–5. doi: 10.1378/chest.87.3.351. [DOI] [PubMed] [Google Scholar]
- 25.Daniil ZD, Zintzaras E, Kiropoulos T, Papaioannou A, Koutsokera A. Discrimination of exudative pleural effusions based on multiple biological parameters. Eur Respir J. 2007;30:957–64. doi: 10.1183/09031936.00126306. [DOI] [PubMed] [Google Scholar]
- 26.Lee HJ, Chang HJ. Diagnostic utility of serum and pleural fluid carcinoembryonic antigen, neuron-specific enolase, and cytokeratin 19 fragments in patients with effusions from primary lung cancer. Chest. 2005;128:2298–303. doi: 10.1378/chest.128.4.2298. [DOI] [PubMed] [Google Scholar]
- 27.Tozzoli R, Basso SM, D’Aurizio F, Metus P, Lumachi F. Evaluation of predictive value of pleural CEA in patients with pleural effusions and histological findings: A prospective study and literature review. Clin Biochem. 2016;49:1227–31. doi: 10.1016/j.clinbiochem.2016.08.006. [DOI] [PubMed] [Google Scholar]