

Abstract
Inhalation therapy is the cornerstone of chronic obstructive pulmonary disease (COPD) management. However, for many COPD patients who are managed at home, nebulization therapy offers an effective alternative treatment and fulfills the gap of catering to the specific population of patients who are unable to use handheld inhaler devices appropriately. The present review highlights key aspects, namely selection of the right beneficiaries for home nebulization, available drugs in nebulized formulations for the treatment of COPD, and the importance of care, cleaning, and maintenance, which are prerequisites for ensuring successful nebulization therapy.
KEY WORDS: Chronic obstructive pulmonary disease, home nebulization, inhalation therapy, maintenance nebulization, nebulization, nebulizer
INTRODUCTION
Inhalation therapy is the cornerstone in the treatment of obstructive airway diseases, especially chronic obstructive pulmonary disease (COPD).[1] Interestingly, with increase in the burden of respiratory diseases, there has also been an increase in the number and types of available inhalation devices for treating these diseases in the past few years.[1] More importantly, what differs in each type of device is the technology used for aerosol generation and hence the technique that a patient needs to employ for optimal drug delivery. Data suggest that all devices are nearly similar in their efficacy when used appropriately.[1,2] However, many real-world studies have highlighted the crucial role of the patient's ability to use the device correctly in governing optimal drug delivery to the lungs and thereby disease control.[3,4,5,6,7]
Of all inhalation devices including pressurized metered-dose inhalers (pMDIs), dry powder inhalers (DPIs), and breath-actuated inhalers, nebulizers are considered the easiest to use, requiring minimal cognitive abilities and virtually no actuation-inhalation coordination, manual dexterity, or hand strength.[1,8] Recent technological advances have made nebulizers more portable and patient-friendly. Moreover, there is a wide availability of different classes of drugs such as long-acting beta2-agonists (LABAs), long-acting muscarinic receptor antagonists, steroids, mucolytics, and antibiotics in nebulized formulations. These factors have expanded the scope for the use of nebulizers from acute settings at clinics or hospitals to the homes of patients. Market analysis data and available literature show that nebulizers are now increasingly being used at home, especially by elderly patients with COPD,[9] thus making it imperative to understand their scope and implications in the current context. Nebulizers, when prescribed for home use, need more careful deliberation and observation as the patients using them are unsupervised unlike when used in the clinics or hospitals. Although there is no dearth of literature available on nebulization therapy in general, a comprehensive review on maintenance home nebulization for patients with COPD is lacking and hence warranted. The term “maintenance nebulization” has been theoretically referred to as chronic use of nebulization therapy at home for more than 3 weeks at home, whereas the term “home nebulization” is an umbrella term that refers to even a short-term use of nebulizers.[10]
The objective of this article is to review key aspects of home nebulization for maintenance therapy in COPD patients, which are as follows: (a) selecting the right patient; (b) perceptions of COPD patients and caregivers on home use of nebulizers; (c) drugs used and approved for nebulization therapy in COPD patients; (d) factors that determine the choice of nebulizers and accessories, and (e) care, cleaning, and maintenance of nebulizers. This review will potentially assist physicians in selecting and guiding COPD patients in the effective long-term management of the disease using the home nebulization strategy.
SELECTING THE RIGHT PATIENT
COPD patients often have age-related or disease-related comorbidities, which make the use of handheld, breath-reliant inhalers such as a pMDI or DPI difficult, resulting in suboptimal drug deposition to lungs. Consequently, disease and symptom control is not achieved.[7]
The 2001 European Respiratory Society (ERS) guidelines by the ERS task force on the use of nebulizers recommend maintenance therapy with nebulizers for home use only after adequately ensuring failure to optimize treatment with handheld inhalers.[11] However, in certain groups of COPD patients, nebulizers can be particularly useful. A review by Dhand et al. describes various clinical scenarios where maintenance therapy with nebulization is the most appropriate choice of treatment for elderly patients with COPD[9] [Table 1].
Table 1.
Clinical scenarios where maintenance treatment with nebulizers is most appropriate in elderly chronic obstructive pulmonary disease patients
| 1. Cognitive impairment of the patient due to age or comorbidity |
| 2. Reduced manual dexterity due to age or comorbidity |
| 3. Patients with muscle weakness or pain due to neuromuscular comorbidity |
| 4. Patients unable to use any handheld inhaler despite repeated instruction and training |
| 5. Patients who cannot generate adequate PIFR, particularly after a debilitating hospitalization |
| 6. Patients who are inadequately controlled by a pMDI or DPI or who need high doses of medication |
PIFR: Peak inspiratory flow rate, pMDI: Pressurized metered-dose inhalers, DPI: Dry powder inhalers
Key patient-related factors include the following.
Suboptimal peak inspiratory flow rate
Normally, forced expiratory volume in 1 s (FEV1) decreases at the rate of 25–30 mL/year from the age of 35–40 years, and the decrease can be up to 60 mL/year after 70 years of age.[12] In COPD, the rate of decline in FEV1 is accelerated and depends on the severity of the disease.[13] Such a decrease in lung function impacts the patient's ability to generate an adequate inspiratory capacity and use inhaler devices efficiently, especially DPIs.
Many studies have correlated suboptimal peak inspiratory flow rates (PIFRs) with increasing age, female gender, exacerbation and postexacerbation condition, and shorter height.[14,15,16,17,18] A recent study performed on 66 outpatients with stable COPD showed that 40% of the patients were unable to achieve optimal inspiratory airflow with his or her own device,[19] underlining the importance of assessing PIFR to optimize therapy in COPD patients.
In a retrospective study done by Loh et al. that examined PIFR in 123 patients admitted with an acute exacerbation of COPD, suboptimal PIFR (PIFR <60 L/min) was present in 52% of patients.[18] Notably, patients with suboptimal PIFR who were discharged on nebulizers had significantly lower rates of COPD readmission as compared with those discharged on DPIs (<30-day readmission, 0 and 50%, respectively; and <90-day readmissions, 17% and 70%, respectively). Given the reduction of PIFR during COPD exacerbations and during hospitalization, it may be prudent to consider transition to non-DPI therapies (such as nebulizers) during and immediately after an exacerbation.
Cognitive impairment
Cognitive impairment is characterized by common signs such as impairment of memory, attentional, and executive functions, which can have detrimental effects on many aspects of patient function, health status, and the quality of life. It has been shown to be related to lower adherence to medical treatment and increased rates of hospitalization and mortality in COPD.[20] Cognitive impairment is highly prevalent in older patients with COPD.[21,22,23,24] It has been estimated that 36% of patients with COPD will present with episodes of cognitive impairment,[25] as compared with 12% of individuals among the general population.[24]
Muscle weakness and impaired dexterity
Reduction in muscle strength and endurance has been reported in COPD patients. In about 40% of patients, the exercise capacity is limited by alterations in skeletal muscle rather than pulmonary problems. Elderly COPD patients also may not have the adequate hand strength required to actuate a pMDI[1] as their handgrip strength is reduced.[26] Inadequate hand strength for inhaler device manipulation may be evident in up to one-third of elderly patients.[27] Gray et al. found that reduced hand strength was a significant predictor of incorrect use of pMDIs in a group of elderly (mean age, 69.7 years) COPD patients.[28]
Recent reports also confirm a strong association between handgrip strength measures with PIFRs,[29] functional capacity,[30] and fatigue[31] seen in COPD patients.
PERCEPTIONS OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE PATIENTS AND CAREGIVERS ON HOME USE OF NEBULIZERS
In a study by Sharafkhaneh et al., most COPD patients and caregivers (89% and 92%, respectively) expressed that they were “generally satisfied with their (or their friend's or family member's) current nebulized treatment.”[32] Up to 80% of both patients and caregivers reported that using a nebulizer was better than using only an inhaler (pMDI/PDI). Both patients (79%) and caregivers (85%) opined that the benefits of nebulization therapy overshadowed the challenges or inconveniences. Patients also reported that their overall quality of life had improved since the adoption of nebulization (75% positive response) and enabled their caregiver to provide care (77% positive response); caregivers reiterated the same sentiment.
Another patient survey conducted by Barta et al. reported similar findings with respect to better control of symptoms, independence in executing most of the chores, better working than inhalers, increased self-confidence, and lesser probability of going to the hospital.[33] However, it also highlighted certain disadvantages such as dependency on the nebulizers, longer time taken for the treatment procedure, practical restrictions to carry the nebulizers around, and feelings of embarrassment. A few patients also reported problems with cleaning and disinfection of the nebulizer parts.
DRUGS USED AND APPROVED FOR NEBULIZATION THERAPY IN CHRONIC OBSTRUCTIVE PULMONARY DISEASE
The nebulized drugs used in COPD fall into the different categories, as listed in Table 2.
Table 2.
Approved nebulized drugs available in India, which can be prescribed for maintenance nebulization in obstructive airway diseases (modified from Ghoshal et al., 2017[10])
| Drug class | Molecules | Recommended use (in adults)* |
|---|---|---|
| SABA | Salbutamol levosalbutamol | As-needed use in OADs |
| LABA | Arformoterol | Long-term maintenance in COPD |
| SAMA | Ipratropium bromide | Long-term maintenance in COPD |
| LAMA | Glycopyrronium bromide | Long-term maintenance in COPD |
| SABA+SAMA | Salbutamol+ipratropium Levosalbutamol+ipratropium | Long-term maintenance in COPD/as-needed use in maintenance regimen in COPD |
| ICS+LABA | Budesonide+formoterol | Long-term maintenance in OAD |
| Mucolytics | N-acetylcysteine ambroxol | Short term adjuvant use in OAD in case of mucus hypersecretion |
*For exact indications, posology, and administration, please refer to the prescribing information available from the manufacturer of the respective products. SABA: Short-acting beta2-agonists, LABA: Long-acting beta2-agonist, SAMA: Short-acting muscarinic antagonist, LAMA: Long-acting muscarinic antagonist, COPD: Chronic obstructive pulmonary disease, OADs: Obstructive airway diseases
Studies comparing drugs administered via a nebulizer versus a pMDI in COPD patients have demonstrated the two routes of administration to be near similar in lung function improvement, symptoms, and quality of life.[34,35] Various studies have also proven the efficacy and safety of nebulized steroids to be comparable with inhaled corticosteroids.[36,37] In the near future, new long-acting bronchodilators and fixed-dose combinations may be made available in nebulized formulations, which will be beneficial to patients who need or prefer nebulized treatments.
FACTORS THAT DETERMINE THE CHOICE OF NEBULIZERS AND ACCESSORIES
There are different types of nebulizers currently available, including jet, ultrasonic, and mesh nebulizers [Figure 1], along with their advanced versions, all of which are based on different principles and have their own advantages and disadvantages [Table 3].
Figure 1.
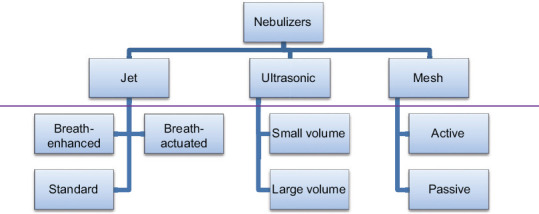
Types of nebulizers
Table 3.
Comparison between jet, ultrasonic, and mesh nebulizers (modified from Ghoshal et al., 2017[10])
| Parameters | Jet | Ultrasonic | Mesh |
|---|---|---|---|
| Power source | Electric/compressed gas (i.e., oxygen)/battery | Electric/battery | Battery/electric |
| Principle | Compressed air technology | High frequency sound waves | Static/vibrating mesh |
| Treatment time | ~10–15 min | 4–10 min | 1–5 min |
| Output rate | Low | Higher | Highest |
| Cleaning | After every use | After several uses | After every use |
| Cost | Low | High | High |
| Drug formulations | Can nebulize solutions, suspensions, oils | Cannot nebulize suspensions or liquids with high viscosity/surface tension | Some cannot nebulize suspensions with high viscosity/surface tension |
| Portability | Limited | Limited | Portable |
| Sound | Noisy | Silent | Low/silent |
Jet nebulizers are either conventional or breath enhanced or breath actuated.[38] In a conventional jet nebulizer, there is a continuous flow and generation of aerosol, and thus, a large proportion of medication is lost during exhalation, resulting in inefficient aerosol drug delivery and variable dosing. In “breath-actuated' nebulizers and ‘breath-enhanced’ nebulizers, the aerosol is generated during the patient's inspiratory phase, so that the patients do not have to breath coordinate and loss of aerosol to the surrounding is substantially minimized. Both types of nebulizers are modifications of the “conventional” jet nebulizers, specifically designed to improve their efficiency by increasing the amount of aerosol delivered to the patient with less wastage of aerosol during exhalation.
Ultrasonic nebulizers can be small volume or large volume and use the ultrasonic vibrations from piezoelectric crystals to form waves in the liquid medication, which then forms fine droplets at the surface. Ultrasonic nebulizers operate more silently than jet nebulizers but generate heat during operation. Furthermore, ultrasonic nebulizers are unable to aerosolize viscous solutions such as suspensions.[38,39]
Mesh nebulizers can have active mesh or passive mesh, depending on the location of the vibrating element present. Active mesh nebulizers use a piezo element that vibrates a precisely drilled mesh, which is in contact with the medication, to generate an aerosol. Passive mesh nebulizers use a transducer horn that induces passive vibrations, which then traverse through the medication and then to the mesh, and the medication is forced through the mesh to produce an aerosol. Mesh nebulizers have several advantages over other nebulizer systems such as greater efficiency, precision and consistency of drug delivery, silent operation, and generally, portable.[38]
The following characteristics should be reviewed by the physician before advising the patients on buying a nebulizer:[39]
-
Adequate mass median aerodynamic diameter (MMAD) and fine-particle fraction (FPF)/respirable fraction: The MMAD is the median diameter of the aerosol particles that divides the mass of aerosol by half so that 50% mass of the aerosol particles has a bigger diameter and the other 50% mass has a smaller diameter. The MMAD should be in the appropriate range to ensure adequate lung deposition. FPF is the fraction of fine-particle dose that is respirable to the total mass of drug emitted during nebulization
- Preferred: MMAD: ~3 microns; FPF: 75%–80%
-
Nebulizer output/aerosol output (mL/min): Aerosol output is the volume of drug aerosolized by the nebulizer per minute. The greater the aerosol output, the lesser will be the time taken for nebulization
- Preferred: Depends on the type of nebulizer; generally, it is highest for mesh nebulizers, followed by ultrasonic nebulizers, and lowest for jet nebulizers
-
Residual volume: Residual volume, also called as dead volume, is the volume remaining after nebulization is completed. The lower the residual volume, the greater will be the fill volume delivered to the patient
- Preferred: Depends on the type of nebulizer. For mesh nebulizers, the residual volume is 0.1–0.5 mL; for ultrasonic and jet nebulizers, the residual volumes are larger
-
Minimal drug wastage by loss to environment
- Preferred: In jet nebulizers, high-end versions such as breath-enhanced, breath-assisted, or dosimetric options ensure minimal drug wastage. In mesh nebulizers, valved mesh nebulizers or smart nebulizer options minimize drug wastage.
-
Adequate flow rate velocity (velocity of compressed gas in case of jet nebulizer) as a high velocity will increase oropharyngeal drug deposition, and low velocity will result in drug wastage through loss to environment
- Preferred: Generally, a flow rate of 8 L/min is recommended
-
Easy to use
- Preferred: Patient-friendly, easy to carry and use, and less noisy
-
Easy to clean and maintain
- Preferred: Cleaning, disinfection, and maintenance instructions should be clear and easy to execute
Cost to the patient
-
Ergonomically designed patient interface (face mask/mouthpiece).
- Preferred: Mouthpiece should be preferred over a face mask. A face mask reduces the available drug for deposition in the lungs.
The use of the mouthpiece has been shown to result in higher aerosol delivery and better clinical outcomes versus a face mask in terms of significant improvement in lung function and reduced incidence of adverse events.[40,41,42] Moreover, significant facial and eye deposition of aerosol can occur with a face mask, especially when it is not snug fitting, which can lead to side effects.[43] Hence, a mouthpiece should be preferred over a face mask when administering inhaled steroids, antibiotics, or anticholinergics. However, a face mask should be reserved for situations in which the patient is too sick or finds it very difficult to coordinate breathing using a mouthpiece.[44]
CARE, CLEANING, AND MAINTENANCE OF NEBULIZERS
Cleaning and maintenance of the nebulizer is integral to the success of home maintenance therapy of COPD. The importance of cleaning, disinfection, and correct maintenance of the nebulizer should be communicated to the patients and the caregivers. If the nebulizer accessories are not cleaned and disinfected regularly, it leads to increase in the chances of infections, which can have a profound impact on the health and lung function of the COPD patient.[45] A study performed by Della Zuana et al. demonstrated that a one-time educational intervention (with oral and written instructions) to the patients and caregivers who were using nebulizers at home had a significant positive impact on the daily maintenance and significant reduction in the proportion of contaminated nebulizers by 43%.[46] It is also recommended to perform a regular check and review of COPD patients (at least every 6 months) who are on nebulization therapy so as to monitor the efficacy and safety of the ongoing medication.[10]
CONCLUSION
Prescribing the appropriate inhalation therapy to COPD patients should be based on various factors such as the patient's ability to use the device, patient's lung function, physical and cognitive skills, and individual preference. It is common in routine practice to encounter COPD patients who are unable to optimally use handheld inhalers because of physical or cognitive impairments and/or with poor lung condition. Treatment options such as nebulization, which do not require coordination of actuation and inhalation or an inspiratory flow threshold, represent a promising suitable alternative in such patients. Benefits of nebulization therapy can be optimized through careful patient selection, prescribing the appropriate drug regimen and nebulizer, counseling the patient and caregivers on the disease, and regular assessment and follow-up checks.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Barrons R, Pegram A, Borries A. Inhaler device selection: Special considerations in elderly patients with chronic obstructive pulmonary disease. Am J Health Syst Pharm. 2011;68:1221–32. doi: 10.2146/ajhp100452. [DOI] [PubMed] [Google Scholar]
- 2.Chapman KR, Voshaar TH, Virchow JC. Inhaler choice in primary practice. Eur Respir Rev. 2005;14:117–22. [Google Scholar]
- 3.Melani AS, Bonavia M, Cilenti V, Cinti C, Lodi M, Martucci P, et al. Inhaler mishandling remains common in real life and is associated with reduced disease control. Respir Med. 2011;105:930–8. doi: 10.1016/j.rmed.2011.01.005. [DOI] [PubMed] [Google Scholar]
- 4.Melani AS, Canessa P, Coloretti I, DeAngelis G, DeTullio R, Del Donno M, et al. Inhaler mishandling is very common in patients with chronic airflow obstruction and long-term home nebuliser use. Respir Med. 2012;106:668–76. doi: 10.1016/j.rmed.2011.11.016. [DOI] [PubMed] [Google Scholar]
- 5.Jarvis S, Ind PW, Shiner RJ. Inhaled therapy in elderly COPD patients; time for re-evaluation? Age Ageing. 2007;36:213–8. doi: 10.1093/ageing/afl174. [DOI] [PubMed] [Google Scholar]
- 6.Khassawneh BY, Al-Ali MK, Alzoubi KH, Batarseh MZ, Al-Safi SA, Sharara AM, et al. Handling of inhaler devices in actual pulmonary practice: Metered-dose inhaler versus dry powder inhalers. Respir Care. 2008;53:324–8. [PubMed] [Google Scholar]
- 7.Gregoriano C, Dieterle T, Breitenstein AL, Dürr S, Baum A, Maier S, et al. Use and inhalation technique of inhaled medication in patients with asthma and COPD: Data from a randomized controlled trial. Respir Res. 2018;19:237. doi: 10.1186/s12931-018-0936-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Geller DE. Comparing clinical features of the nebulizer, metered-dose inhaler, and dry powder inhaler. Respir Care. 2005;50:1313–21. [PubMed] [Google Scholar]
- 9.Dhand R, Dolovich M, Chipps B, Myers TR, Restrepo R, Farrar JR. The role of nebulized therapy in the management of COPD: Evidence and recommendations. COPD. 2012;9:58–72. doi: 10.3109/15412555.2011.630047. [DOI] [PubMed] [Google Scholar]
- 10.Ghoshal AG, Salvi S, Dhar R, Guleria R, Mahashur A, Mukhopadhyay A, et al. Consensus Document on home nebulization for maintenance treatment of obstructive airway Diseases: A joint initiative by the national allergy asthma bronchitis institute (NAABI) and chest research foundation (CRF) J Assoc Physicians India. 2017;65:60–73. [PubMed] [Google Scholar]
- 11.Boe J, Dennis JH, O'Driscoll BR, Bauer TT, Carone M, Dautzenberg B, et al. European Respiratory Society guidelines on the use of nebulizers. Eur Respir J. 2001;18:228–42. doi: 10.1183/09031936.01.00220001. [DOI] [PubMed] [Google Scholar]
- 12.Sharma G, Goodwin J. Effect of aging on respiratory system physiology and immunology. Clin Interv Aging. 2006;1:253–60. doi: 10.2147/ciia.2006.1.3.253. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Tantucci C, Modina D. Lung function decline in COPD. Int J Chron Obstruct Pulmon Dis. 2012;7:95–9. doi: 10.2147/COPD.S27480. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Janssens W, VandenBrande P, Hardeman E, De Langhe E, Philps T, Troosters T, et al. Inspiratory flow rates at different levels of resistance in elderly COPD patients. Eur Respir J. 2008;31:78–83. doi: 10.1183/09031936.00024807. [DOI] [PubMed] [Google Scholar]
- 15.Mahler DA, Waterman LA, Gifford AH. Prevalence and COPD phenotype for a suboptimal peak inspiratory flow rate against the simulated resistance of the Diskus® dry powder inhaler. J Aerosol Med Pulm Drug Deliv. 2013;26:174–9. doi: 10.1089/jamp.2012.0987. [DOI] [PubMed] [Google Scholar]
- 16.Malmberg LP, Rytilä P, Happonen P, Haahtela T. Inspiratory flows through dry powder inhaler in chronic obstructive pulmonary disease: Age and gender rather than severity matters. Int J Chron Obstruct Pulmon Dis. 2010;5:257–62. doi: 10.2147/copd.s11474. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Sharma G, Mahler DA, Mayorga VM, Deering KL, Harshaw O, Ganapathy V. Prevalence of low peak inspiratory flow rate at discharge in patients hospitalized for COPD exacerbation. Chronic Obstr Pulm Dis. 2017;4:217–24. doi: 10.15326/jcopdf.4.3.2017.0183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Loh CH, Peters SP, Lovings TM, Ohar JA. Suboptimal inspiratory flow rates are associated with chronic obstructive pulmonary disease and all-cause readmissions. Ann Am Thorac Soc. 2017;14:1305–11. doi: 10.1513/AnnalsATS.201611-903OC. [DOI] [PubMed] [Google Scholar]
- 19.Ghosh S, Pleasants RA, Ohar JA, Donohue JF, Drummond MB. Prevalence and factors associated with suboptimal peak inspiratory flow rates in COPD. Int J Chron Obstruct Pulmon Dis. 2019;14:585–95. doi: 10.2147/COPD.S195438. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Bourbeau J, Bartlett SJ. Patient adherence in COPD. Thorax. 2008;63:831–8. doi: 10.1136/thx.2007.086041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Andrianopoulos V, Gloeckl R, Vogiatzis I, Kenn K. Cognitive impairment in COPD: Should cognitive evaluation be part of respiratory assessment? Breathe (Sheff) 2017;13:e1–9. doi: 10.1183/20734735.001417. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Chang SS, Chen S, McAvay GJ, Tinetti ME. Effect of coexisting chronic obstructive pulmonary disease and cognitive impairment on health outcomes in older adults. J Am Geriatr Soc. 2012;60:1839–46. doi: 10.1111/j.1532-5415.2012.04171.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Charbek E, Huynh K, Kim E, Nayak RP. Assessment of cognitive impairment in patients with chronic obstructive pulmonary disease using the rapid cognitive screen. J Nutr Health Aging. 2019;23:102–4. doi: 10.1007/s12603-018-1146-x. [DOI] [PubMed] [Google Scholar]
- 24.Villeneuve S, Pepin V, Rahayel S, Bertrand JA, de Lorimier M, Rizk A, et al. Mild cognitive impairment in moderate to severe COPD: A preliminary study. Chest. 2012;142:1516–23. doi: 10.1378/chest.11-3035. [DOI] [PubMed] [Google Scholar]
- 25.Torres-Sánchez I, Rodríguez-Alzueta E, Cabrera-Martos I, López-Torres I, Moreno-Ramírez MP, Valenza MC. Cognitive impairment in COPD: A systematic review. J Bras Pneumol. 2015;41:182–90. doi: 10.1590/S1806-37132015000004424. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Kovarik M, Joskova V, Patkova A, Koblizek V, Zadak Z, Hronek M. Hand grip endurance test relates to clinical state and prognosis in COPD patients better than 6-minute walk test distance. Int J Chron Obstruct Pulmon Dis. 2017;12:3429–35. doi: 10.2147/COPD.S144566. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Armitage JM, Williams SJ. Inhaler technique in the elderly. Age Ageing. 1988;17:275–8. doi: 10.1093/ageing/17.4.275. [DOI] [PubMed] [Google Scholar]
- 28.Gray SL, Williams DM, Pulliam CC, Sirgo MA, Bishop AL, Donohue JF. Characteristics predicting incorrect metered-dose inhaler technique in older subjects. Arch Intern Med. 1996;156:984–8. [PubMed] [Google Scholar]
- 29.Frohnhofen H, Hagen O. Handgrip strength measurement as a predictor for successful dry powder inhaler treatment application in older individuals with COPD. Gerontol Geriat. 2011;44:245–9. doi: 10.1007/s00391-011-0222-1. [DOI] [PubMed] [Google Scholar]
- 30.Strandkvist V, Andersson M, Backman H, Larsson A, Stridsman C, Lindberg A. Hand grip strength is associated with fatigue among men with COPD: Epidemiological data from northern Sweden. Physiother Theory Pract. 2020;36:408–16. doi: 10.1080/09593985.2018.1486490. [DOI] [PubMed] [Google Scholar]
- 31.Gonçalves da Silva AL, Garmatz E, Goulart C, Carvalho L, Cardoso D, Paiva DN. Handgrip and functional capacity in chronic obstructive pulmonary disease patients. Fisioter Mov Curitiba. 2017;30:501–7. [Google Scholar]
- 32.Sharafkhaneh A, Wolf RA, Goodnight S, Hanania NA, Make BJ, Tashkin DP. Perceptions and attitudes toward the use of nebulized therapy for COPD: Patient and caregiver perspectives. COPD. 2013;10:482–92. doi: 10.3109/15412555.2013.773302. [DOI] [PubMed] [Google Scholar]
- 33.Barta SK, Crawford A, Roberts C. Survey of patients' views of domiciliary nebulizer treatment for chronic lung disease. Respi Med. 2002;96:375–81. doi: 10.1053/rmed.2001.1292. [DOI] [PubMed] [Google Scholar]
- 34.Tashkin DP, Klein GL, Colman SS, Zayed H, Schonfeld WH. Comparing COPD treatment: Nebulizer, metered dose inhaler, and concomitant therapy. Am J Med. 2007;120:435–41. doi: 10.1016/j.amjmed.2006.07.043. [DOI] [PubMed] [Google Scholar]
- 35.Gogtay J, Salvi S, Pandya H, Ghosal A, Dhar R, Walanj S, et al. Efficacy and safety of nebulized formoterol/budesonide (FB Neb) compared with formoterol/budesonide pMDI (FB pMDI) in patients with severe to very severe COPD. Respirology. 2014;19:63–253. [Google Scholar]
- 36.Bisgaard H, Nikander K, Munch E. Comparative study of budesonide as a nebulized suspension vs. pressurized metered-dose inhaler in adult asthmatics. Respir Med. 1998;92:44–9. doi: 10.1016/s0954-6111(98)90031-2. [DOI] [PubMed] [Google Scholar]
- 37.Murphy K, Noonan M, Silkoff PE, Uryniak T. A 12-week, multicenter, randomized, partially blinded, active-controlled, parallel-group study of budesonide inhalation suspension in adolescents and adults with moderate to severe persistent asthma previously receiving inhaled corticosteroids with a metered-dose or dry powder inhaler. Clin Ther. 2007;29:1013–26. doi: 10.1016/j.clinthera.2007.06.005. [DOI] [PubMed] [Google Scholar]
- 38.Lavorini F, Fontana GA, Usmani OS. New inhaler devices-the good, the bad and the ugly respiration. Thematic Rev Ser. 2014;88:3–15. doi: 10.1159/000363390. [DOI] [PubMed] [Google Scholar]
- 39.Gardenhire DS, Brunett D, Strickland S, Myres T. Guide to Aerosol Delivery Devices for Respiratory Therapist. American Association for Respiratory Care. 4th ed. 2017. [Last accessed on 2020 Sep 26]. https://www.aarc.org/wp-content/uploads/2015/04/aerosol_guide_rt.pdf .
- 40.Mellon M, Leflein J, Walton-Bowen K, Cruz-Rivera M, Fitzpatrick S, Smith JA. Comparable efficacy of administration with face mask or mouthpiece of nebulized budesonide inhalation suspension for infants and young children with persistent asthma. Am J Respir Crit Care Med. 2000;162:593–8. doi: 10.1164/ajrccm.162.2.9909030. [DOI] [PubMed] [Google Scholar]
- 41.Hess DR. Aerosol delivery devices in the treatment of asthma. Respir Care. 2008;53:699–723. [PubMed] [Google Scholar]
- 42.Everard ML, Clark AR, Milner AD. Drug delivery from jet nebulisers. Arch Dis Child. 1992;67:586–91. doi: 10.1136/adc.67.5.586. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Gupta P, O'Mahony MS. Potential adverse effects of bronchodilators in the treatment of airways obstruction in older people: Recommendations for prescribing. Drugs Aging. 2008;25:415–43. doi: 10.2165/00002512-200825050-00005. [DOI] [PubMed] [Google Scholar]
- 44.Kishida M, Suzuki I, Kabayama H, Koshibu T, Izawa M, Takeshita Y, et al. Mouthpiece versus facemask for delivery of nebulized salbutamol in exacerbated childhood asthma. J Asthma. 2002;39:337–9. doi: 10.1081/jas-120002291. [DOI] [PubMed] [Google Scholar]
- 45.Ari A, Restrepo RD. American Association for Respiratory Care. Aerosol delivery device selection for spontaneously breathing patients: 2012. Respir Care. 2012;57:613–26. doi: 10.4187/respcare.01756. [DOI] [PubMed] [Google Scholar]
- 46.Della Zuana A, Garcia Dde O, Juliani RC, Silva Filho LV. Effect that an educational program for cystic fibrosis patients and caregivers has on the contamination of home nebulizers. J Bras Pneumol. 2014;40:119–27. doi: 10.1590/S1806-37132014000200004. [DOI] [PMC free article] [PubMed] [Google Scholar]