

Abstract
Introduction
Depression and anxiety are common. Rates are significantly higher in cystic fibrosis (CF), and impact health outcomes. Screening is recommended, but is difficult to implement/sustain annually in a busy CF centre. The aim was to develop an acceptable model for depression and anxiety screening in adolescents/adults with CF and their caregivers that could be sustained and shared.
Methods
Quality improvement methodology with plan-do-study-act cycles, flow diagrams, review of data monthly with our designated ‘Mental Health Team’ and caregiver satisfaction surveys, were used to begin screening in clinics and to improve the process. We then piloted our process at a larger paediatric CF centre.
Results
Prior to 2013, screening was not performed at our CF centre. After the first quarter of depression screening, 88% of adolescents and 69% of adults with CF were screened. The process was refined. By the second year, 99% of patients were screened. Anxiety screening began in year three; 97%–99% of patients were screened for both anxiety and depression in years 3–5. Annual caregiver screening rates were >95%. Screening was changed from Patient Health Questionnaire-2 (PHQ-2) to PHQ-9 due to better sensitivity in caregivers, and expanded to patients. Anxiety screening began in year 3 with the Generalised Anxiety Disorder-7 questionnaire. Patients and caregivers reported acceptance of screening. At the larger paediatric centre used as a pilot, 89.6% of patients were screened in year 1. Feedback included recommendations to improve tracking/follow-up of positive screens.
Conclusions
Development and implementation of a stepwise process for depression and anxiety screening was successful in a paediatric/adult CF clinic, due to constant re-evaluation by an engaged team with feedback from patients via survey. A systematic approach at a busy CF centre can serve as a model to implement screening in a clinic.
Keywords: cystic fibrosis, screening, mental health, quality improvement
Introduction
Background and knowledge
Individuals with cystic fibrosis (CF) have higher rates of depression than the general population. The International Depression/Anxiety Epidemiological Study (TIDES) recruited over 6000 patients with CF and found that symptoms of depression were reported by 10% of adolescents and 19% of adults.1 Studies in CF populations have shown that depression is linked with worse health outcomes such as decreased lung function,2 3 lower body mass index,4 increased exacerbations, hospitalisations, healthcare costs5 6 and lower vitamin D levels.5 Additionally, depression in CF has been associated with challenges in sustaining daily therapies,6 7 diminished quality of life, even after controlling for lung function,3 8 9 and increased mortality.10
The TIDES study found elevated symptoms of depression on the Center for Epidemiologic Studies Depression Scale in 37% of mothers and 31% of fathers, which were 2–3 times the rates in community samples.1 In turn, parental depression was associated with increased rates of depression in youth with CF1, as well as decreased child adherence and negative health outcomes.11
Individuals with CF and their caregivers are also at risk for increased anxiety compared with the general population, with prevalence rates two to three times higher than community samples.1 The TIDES study found elevated symptoms of anxiety in individuals with CF, with rates of anxiety increasing with age (22% of adolescents and 32% of adults). Caregivers also reported elevated symptoms of anxiety, with 48% of female caregivers and 36% of male caregivers experiencing significant anxiety. Similar to depression, parental anxiety is associated with increased risk of anxiety in youths with CF.1 Additionally, individuals with CF frequently face anxiety from healthcare experiences and procedures.12 13 Illness-specific anxiety is associated with impaired functioning, emotional distress and lower quality of life.14
Rationale
Despite knowing that depression and anxiety can adversely affect health outcomes in CF, an organised process and tools for routine annual or ongoing screening in busy CF clinics had not yet been developed or incorporated into CF national or international guidelines. Given the prevalence rates and impact of depression, our centre began depression screening and stepped care treatment as a quality improvement (QI) initiative in 2013, with the addition of screening for anxiety in 2016. Since our programme began, annual depression and anxiety screening is now recommended by the CF Foundation and European CF Society Guidelines Committee on Mental Health for all individuals with CF 12 years and older as well as in the caregivers of all children with CF.15
Specific aims
(1) Develop and implement a depression and anxiety screening and treatment protocol for individuals with CF and their caregivers, (2) Evaluate the prevalence of depression and anxiety and endorsement of suicidal ideation, (3) Provide treatment based on the severity of symptoms, (4) Evaluate patient and caregiver acceptance of screening at CF clinic visits, (5) Use QI methodology to attain and maintain high screening rates and (6) Disseminate the protocol, resources for implementation at another CF centre.
Methods
Context
Our CF centre is a university affiliated, Cystic Fibrosis Foundation (CFF)-accredited CF centre consisting of 180 patients (100 adults and 80 children with 24 adolescents between ages 12–18 years), from eight different counties. Eighty-six per cent of paediatric patients and 40% of adults are seen the recommended four clinic visits per year as per CFF guidelines, with slight variations each year. Centre data are provided by the CFF Registry which was combined data for all individuals with CF at our centre until 2018, when the data were separated into paediatric and adult centres.
Interventions
Plan-Do-Study-Act (PDSA) cycles, flow diagrams, review of data on a monthly basis with our ‘Mental Health Team,’ together with patient and caregiver satisfaction surveys, were used to carry out our specific aims. During the planning phase, we created a multidisciplinary team of individuals to carry out the project, developed a referral network and compiled educational materials. A process for screening in clinic was established. We used paper forms in clinic folders and clinic nurses were integrated into the clinic flow to give a pen and the form to each person. Our medical social worker conducted the assessments, and pulmonary providers served as a backup if the social worker was on leave. The mental health coordinator (MHC) took over for the social worker once the position was available. A process was established for how the treating clinician was made aware of results, how the social worker discussed results with the patient or caregiver, and how the screening scores were tracked. In our clinic, the pulmonary provider is the last person to see each patient, so they were made aware of the scores and discussion prior to entry into the room. The tracking system involved entry of the paper forms into an excel file with scores. Our screening process was expanded and modified in the early years (see figure 1).
Figure 1.

Early Plan-Do-Study-Act cycles. CF, cystic fibrosis.
Screening instruments and interventions
Beginning in 2013, adolescents (12–18 years old) and adults with CF were assessed for symptoms of depression annually during a routine clinic visit using a standardised depression scale (figure 2A). To reduce the burden of applying a full diagnostic instrument to the entire CF clinic population, depression screening involved a two-stage protocol with a two-question screen (the Patient Health Questionnaire-2; PHQ-2), followed by a lengthier instrument, the PHQ-9 if the PHQ-2 score was ≥3. All patients were assessed using the PHQ-2 once a year, more often if there were clinical concerns. The PHQ-2 inquires about the degree to which the individual has experienced depressed mood and anhedonia over the past 2 weeks and does not contain somatic symptoms that overlap with CF physical disease. Further, the PHQ-2 contains two essential features of major depression according to the Diagnostic and Statistical Manual of Mental Disorders 5 (DSM-5).16 The PHQ-2 was used for depression screening because it is in the public domain, takes less than 1 min to administer and score, and is the most well validated two-item screener for depression.17–19 A meta-analysis demonstrated that ultrashort screening instruments such as the PHQ-2 are able to discriminate between depressed versus non-depressed patients in primary care.20
Figure 2.

(A) Patient depression screening algorithm. (B) Parent/caregiver screening algorithm. PHQ, Patient Health Questionnaire. SW, Social Worker.
The PHQ-9 (adults) and the PHQ-9 modified for adolescents (PHQ-A) were used to screen for additional symptoms of depression as defined by the DSM-5,16 and to aide in determining depression severity and thereafter to monitor treatment response. Each contains a question about suicidality. The PHQ-9 is also in the public domain and takes less than 5 min to administer and 1–2 min to score. PHQ-9 scores >10 have a sensitivity of 88% and a specificity of 88% for Major Depressive Disorder.21 PHQ-9 depression severity is calculated by assigning scores of 0, 1, 2 and 3, to the response categories of ‘not at all’, ‘several days’, ‘more than half the days’ and ‘nearly every day’, respectively. The PHQ-9 total score for the nine items ranges from 0 to 27. Scores of 5, 10, 15 and 20 are suggested cut points for mild, moderate, moderately severe and severe depression, respectively.21
A protocol was developed to assess suicidal ideation if this question was endorsed on the PHQ-9 or PHQ-A. All patients who endorsed suicidal ideation were given the Columbia Suicide Severity Rating Scale (C-SSRS), in addition to a follow-up interview to assess risk for suicide and guide intervention, including the development of a safety plan. The C-SSRS is a well-validated scale designed to quantify the severity of suicidal ideation and behaviour.22 The entire CF team was trained in administering the C-SSRS during the planning phase, although the medical social worker was identified as the primary responder to suicidality. Patients with a PHQ-9 or PHQ-A score ≥5 initially or with suicide risk completed an assessment with the team’s social worker, which collected information about psychosocial stressors, previous episodes of depression or anxiety, comorbid psychiatric conditions, psychiatric medication and psychological treatment. Starting in 2016, a psychologist assumed the role of an MHC and completed the clinical assessment for depression and anxiety. Treatment recommendations were tailored to the severity of depressive symptoms (see figure 2A).
Depression severity was characterised based on the PHQ-9/PHQ-A severity scores together with diagnostic criteria from DSM-5 and level of functional impairment. Severity of depression was assessed to be mild, moderate, moderately severe or severe based on the number of depression criteria symptoms, the severity of the symptoms and the degree of functional disability and distress associated with the depression. Those with mild depression received education and support; those with a moderate depression received education/support and a referral for evidence-based psychotherapy (EBP); those with moderately severe depression received a referral for EBP and/or antidepressant therapy; and finally those with severe depression receive both a referral for EBP and antidepressant therapy. Patients who screened positive on the PHQ-9/PHQ-A are re-screened at each clinic visit using the PHQ-9/PHQ-A until scores are <5, with stepped care protocols for patients not improving. Additionally, at their next clinic visit we clinically assessed their follow-up to the recommended treatment and referrals.
Caregiver screening was implemented in 2014 (year 2) (figure 2B). The PHQ-2 was initially chosen and offered to all parents/caregivers of children with CF <18 years in Q4, at the same time as patient screening. Similar to the process modifications made to the patient protocol, parent/caregiver screening was also extended to occur during the entire year in 2015. The review of the caregiver screening was completed in privacy when able, and referral for further evaluation was recommended if PHQ-2 was ≥3, with a handout of resources given to all caregivers with elevated screens on the back of the screening form. With only 2% of caregivers screening positive in year 2 for symptoms of depression compared with nearly one-third of caregivers in the TIDES study, in years 3, caregivers were randomised to receive either the PHQ-2 or PHQ-9. The PHQ-9 was more frequently positive (18.6%) vs PHQ-2 (12%), suggesting the PHQ-9 was more sensitive. This was notable despite the higher prevalence of positive PHQ-2 screens in this cohort. In year 4, our screening process was modified so all patients and caregivers were screened with the PHQ-9 or PHQ-9-A (ie, without the stepped screening of the PHQ-2 first). This change was supported by patient satisfaction data and did not affect the clinic flow or efficiency of the screening process as initially conceptualised during our planning cycle.
Measures and analysis
Numbers and percentages of patients and caregivers screened for depression and anxiety were initially tabulated quarterly and subsequently, annually. We also recorded the numbers and percentages of patients who endorsed suicidal ideation or intent on the C-SSRS and had interventions. Patients who screened positive for symptoms of depression or anxiety were divided into categories of mild, moderate, moderately severe or severe. These patients were followed clinically. Assessment of treatment response included readministration of assessment tools (PHQ-9 and/or Generalised Anxiety Disorder-7 (GAD-7 for anxiety) at the next clinical encounter to monitor for reduction or resolution of the symptoms, and if the documented treatment and follow-up plan were adhered to. A stepped-care approach was used and treatment adjusted if there was worsening or no response.
Demographic and clinical variables
All patients screened have a valid consent/assent for the Cystic Fibrosis Patient Registry (CFPR), which is approved by the institutional review board. Demographic and clinical variables were extracted from the medical record at each time of screening to examine potential associations with symptoms of depression or anxiety. Demographic information collected include patient age, gender, marital status, student and employment status (see table 1). Data from 2013 to 2017 (years 1–5) from the CF Registry were reported as combined paediatric and adult programs; 2018 (year 6) and 2019 (year 7) were reported as separate paediatric and adult programmes.
Table 1.
Demographic information for our CF centre
| Year 1 | Year 2 | Year 3 | Year 4 | Year 5 | Year 6 | Year 7 | |
| No of patients screened (≥12 years) | 102 | 108 | 105 | 107 | 118 | 119 | 123 |
| No of screened patients ≥18 years (male, female) |
79 (42M, 37F) |
88 (47M, 41F) | 85 (44M, 41F) | 85 (43M, 42F) | 91 (46M, 45F) | 90 (46M, 43F) | 84 (45M, 39F) |
| No of screened patients 12–17 years old | 23 (10M, 13F) | 20 (10M, 10F) | 20 (11 M, 9F) | 22 (15M, 7F) | 27 (17M, 10 F) | 30 (21M, 9F) | 39 (25M, 14F) |
| % centre female | 49 | 47.2 | 47.6 | 45.8 | 46.6 | 43.6 (peds) | 43 (peds) |
| % centre reported ‘white’ | Not provided | 94.5 | 93.5 | 96.5 | 94.5 | 96.1 (peds) | 96.2 (peds) 98.9 (adult) |
| % centre F508del homozygous | Not provided | Not provided | Not provided | Not provided | Not provided | 50 (peds) 44.2 (adult) |
48.1% (peds) 49.5 (adult) |
CF, cystic fibrosis; F, female; M, male.
For caregiver screening, a similar PDSA cycle was established in year 2 and began with modifying our patient protocol. However, one significant difference was using a one-step screening protocol with the PHQ-2, with caregivers who screen positive referred outside the CF clinic for further evaluation. Due to low positive screen rates compared with the TIDES data (2% vs 31%–37%), in year 3, caregivers were randomised to receive either the PHQ-2 or the PHQ-9. Given the improved sensitivity of the PHQ-9, we decided to employ the PHQ-9/PHQ-A in future cycles for patients and caregivers alike. Ethical considerations were taken into account with caregiver screening given that caregivers are not patients of the CF Centre; caregiver scores were recorded only in locked QI spreadsheets, but were not recorded within the patients’ charts.
A new PDSA cycle was added in year 3 for implementation of anxiety screening with the GAD-7 for patients 12 years and older, as well as caregivers of all CF patients.
Results
We developed and implemented a depression and anxiety screening and treatment protocol for individuals with CF and their caregivers. Key events are presented in table 2. This table includes salient events in the QI process that occurred each year.
Table 2.
QI project timeline
| Year 1: getting started |
Assembled our core QI depression and CF team and developed our screening algorithm and processes |
| Sent letter from our director to all eligible patients and families on depression and CF and inviting them to participate in depression screening | |
| Inclusion of mental health topics in our centre’s quarterly newsletter, Shooting the Breeze | |
| Began annual depression screening for all individuals with CF ≥12 years | |
| Year 2: improving our process |
Added depression screening for caregivers of children with CF <18 years of age |
| Extended screening period for patients, and developed an inpatient screening process for individuals that do not attend outpatient CF clinic visits but present for CF exacerbations and for transplant patients who attend clinic visits annually | |
| Started a monthly multidisciplinary mental health meeting to promote team culture around mental health and involve stakeholders on the CF team | |
| Created a database to track screening | |
| Added mental health to preclinic paediatric and adult team meetings | |
| Developed guide to depression screening at a CF centre to share and disseminate with other centres | |
| Year 3: patient and caregiver satisfaction |
Patient (≥18 years) and caregiver satisfaction surveys |
| Added annual anxiety screening for patients ≥12 years and caregivers | |
| Shared our process with the Ann & Robert H. Lurie Children’s Hospital of Chicago to obtain feedback | |
| Examined the efficiency of our process | |
| CF education night for family members and virtually with people with CF to reinforce importance of mental health screening | |
| Mental Health Corner added to quarterly CF Centre Newsletter for patients and their family members | |
| Year 4: disseminating our work and sustaining our work |
Spreading our QI project:
|
| Began billing for depression screening | |
| Hired a Mental Health Coordinator (MHC) to become the champion of annual screening and follow-up, coordinate treatment, and maintain our referral network. | |
| Year 5: sustaining our improvements |
Expanded the role of the MHC |
| The MHC began to provide evidenced-based psychotherapy (EBP) within the CF centre | |
| Year 6: sustaining our MHC |
Billing efforts for EBP |
| Advocacy with senior leaders | |
| Paediatric grand rounds to disseminate process to other paediatric specialty clinics | |
| Year 7: expanding our efforts |
Adaptation of our algorithms and processes to substance misuse in CF |
| Expanding mental health treatment options within our centre |
CF, cystic fibrosis; QI, quality improvement.
We evaluated our process by determining the number of patients screened (see figure 3). The algorithm we developed provided for treatment based on severity of symptoms, with follow-up screens at the next clinical encounter for all patients in the mild to severe category for depression or anxiety. One of the major goals after implementation of our algorithm was to measure, improve and sustain high depression screening rates. Prior to year 1, 0% of our patients were screened. In the first quarter of implementation, screening for depression was accomplished in 88% of adolescents and 66% of adults. Barriers to screening during the process included: ‘missing’ patients who did not come to clinic during the specified quarter of screening. Therefore, in the second year, we extended the screening period over the entire year to improve our screening rates and ensure all patients who may have missed their quarterly visit were reached.
Figure 3.
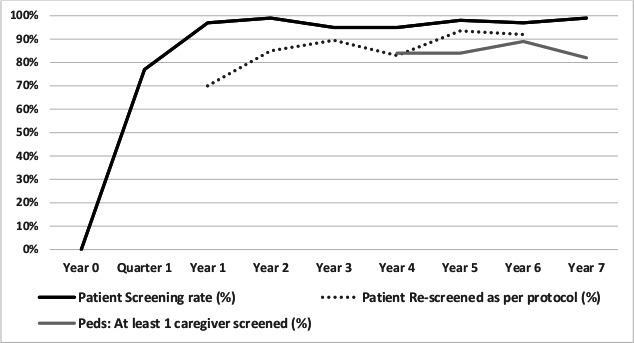
Run chart of screening and rescreening rates for patient depression (years 1–4) and patient depression/anxiety (years 5–7) and caregivers depression/anxiety (years 4–7).
Another barrier to screening was missing screens in patients who were frequently hospitalised, while still acknowledging that hospitalisation itself could affect the levels of depression and anxiety reported by the patients. To address these hospitalisation concerns, in year 2, we expanded depression screening to the inpatient setting during the second week of hospitalisation, to reach those non-adherent to outpatient clinic visits while minimising the impact of the acute stress hospitalisation on screening results.
Another barrier to screening was that lung transplant patients are only seen at the local CF centre once per year, and may ‘miss’ screening if it only occurs during one quarter or time period. The solution to this at our centre was to screen patients who previously received a lung transplant at any clinic visit during the year.
With these modifications, we addressed multiple barriers and improved our screening rates in year 2 (2014) to 99% of adolescents and adults. Due to a slight drop in screening success in years 3 and 4, in year 5 (2017) we changed the start of the annual mental health screening period to quarter 3 (Q3) of the year to increase those who would have screening in case they missed their Q4 visit but came to their Q3. As a result, our screening rates increased to 97% and have ranged from 95% to 99% since 2013 (see figure 3). It is notable that we were able to sustain our process despite a major change in the clinic space in year 5, and a change in personnel including the MHC who performed the process in year 6.
Suicide assessment was an essential part of our depression screening process. At the end of the first year of screening the C-SSRS was only completed 60% (n=5) of the time, despite endorsement of suicidality on the PHQ-9/PHQ-A. The protocol was modified so all screening responses were to be reviewed before a patient was discharged from clinic, and thereafter between year 2 to year 6, 80–85% of C-SSRS screens were completed. Further efforts by our CF psychologist were made to bring this critical assessment tool to 100% of all patients endorsing suicidality on the PHQ-9 or PHQ-A being assessed for suicidal ideation and intent in year 7.
Consequences of screening for depression and anxiety include detection of symptoms of depression and anxiety that required treatment and follow-up and the need to ensure patient safety in the clinic and prior to discharge home. On average, there were high rates of symptoms of depression and anxiety, screenings scores >5 (14%–41% in adults and 10%–25% in adolescents); however, the rates of moderate or severe depression and anxiety requiring referral to treatment and reassessments were in the 5%–10% range. After the first year of screening, 70% of patients that needed to be rescreened for elevated PHQ-9 were rescreened (see figure 3). Subsequently in years 2 through 6 on average 83%–93.5% of our patients that needed to be rescreened for elevated PHQ-9 or GAD-7 scores were rescreened (figure 3). Year 7 data are still being analysed. On average five adults and five adolescents per year had positive suicidal ideation, but only one adult and one adolescent per year had a suicide plan.
Through a satisfaction survey, we evaluated patient and caregiver acceptance of screening at CF clinic visits. Satisfaction data provided helpful feedback to our screening process and assured that the process was not too cumbersome for patients. Feedback was obtained through a telephone satisfaction survey to assess the patient and caregiver perspectives on the depression screening process in years 3–4. Feedback was obtained from 29 individuals with CF (11 adolescents and 18 adults) and 16 caregivers of adolescent patients with CF. None of those surveyed disagreed with this statement ‘The CF centre should be responsible for identifying, treating and referring for child/adolescent/adult CF patient depression’; 66% agreed and 33% were neutral. Fifty-six per cent agreed, 38% neutral and only 6% disagreed with the statement that ‘The CF centre should be responsible for caregiver depression assessment and treatment.’ Ninety-one per cent felt that the screening process was efficient, 7% felt it was not and 2% could not comment. In terms of the usefulness of screening, 76% of those surveyed felt it was at least somewhat helpful. The satisfaction survey also assessed barriers for follow-up for treatment of depression or anxiety, which included finding a mental health provider. Later, our CF psychologist was able to provide evidence based practice within the centre as a solution. The psychologist also began contacting mental health providers for patients outside of the centre, after signed consent forms were completed. Screening caregivers for depression and anxiety was generally well accepted, but there were a few families who declined screening. Data were collected for years 4–6 (see figure 3).
Staff at our site received education about mental health in CF at team meetings and were key stakeholders in this initiative. Gaining their support and comfort with mental health screening and engagement of our entire team was critical. For example, our entire CF multidisciplinary team participated in C-SSRS training to assess suicide risk and we made sure the screening process was easily integrated into the clinic flow without affecting other staff’s ability to complete their functions. An additional factor that helped sustain our process included the hiring of a psychologist to fill the role of a MHC in year 4 (2016) to oversee screening, treatment and referrals.
Our screening process was piloted at another paediatric CF centre at the Ann & Robert H. Lurie Children’s Hospital of Chicago in year 3 (2015). The team in Chicago followed the process outlined above, and used modifications due to Medicaid issues and access to mental health resources. Their main concern about the process was ‘having a mental health professional be available to talk with these patients at that time.’ In their initial year of screening, 77 paediatric patients ≥12 years were screened between November 2014 and April 2015. A total of 89.6% of their population was successfully screened, 9.2% refused and 1% were excluded. They began the process at their main clinic and 1 month later expanded to a satellite clinic. The feedback and screening data from the Ann & Robert H. Lurie Children’s Hospital of Chicago showed that the process could be replicated in a larger clinical cohort, but that other sites might have different barriers to implementing referrals or follow-up for mental health screening. The feedback we obtained also emphasised our need to have proper tracking of our information, which is done in an excel file. At around the same time, the CFF recognised these barriers and began work on how all sites can have a smooth referral process. At our site, we also used our new MHC to ensure follow-up of positive screens, especially for those with suicidal ideation.
Discussion
We designed a systematic outpatient depression and anxiety screening process with a treatment protocol that could be successfully implemented in a busy, moderately sized CF centre. QI methodology was used to define our protocol, integrate it into the existing clinic workflow, and track screening rates and adherence to our protocol. Screening rates increased significantly in the first year, and were sustained. The prevalence of depression and anxiety was higher in our study than reported in the literature. The prevalence of suicidality was 5%–10% depending on the year, so having all providers trained in assessment for safety was important. The training was easily accomplished even by those without a mental health background, but knowing what to do for referral in an emergency situation was paramount. Through the use of our screening protocols, we were able to assess these patients appropriately, and develop safety plans and provide referrals. High numbers of patients were appropriately rescreened as indicated by the protocol. Fortunately, those requiring treatment referral were in the 5%–10% range, and these patients are in the focus of our MHC and even involved in other cognitive behavioural therapy treatment studies or referrals to treatment.
Our process did not affect the efficiency of clinical care. We learnt that patients with CF and families are accepting of, and even expect, screening for depression and anxiety within the CF clinics. Screening of caregivers might be met with relatively more resistance, given that parents/caregivers are not our identified patients. Based on our survey data this may be overcome by educating families on the importance of the mental health of the entire CF family unit, by screening caregivers separately from their child and having an acceptable process for recording and storing their data. In addition, we began to learn in later years about coproduction with patient and family partners of the CF care centre in order to improve care. Thus, an area for improvement for our study would have been the inclusion of people with CF and their families in all phases of our QI effort. This is something we hope to do in the future.
Based on our data and processes, we created a manual of procedures, which was informed by use of QI methodology to improve our screening success.23 In order to support their dissemination across the care centre network, we modified our processes based on feedback from a collaborating paediatric CF centre in Chicago. A Dropbox, a shareable electronic file, of mental health resources was also created. Additional resources have been added based on feedback and is now open access internationally,15 with over 350 individuals accessing the materials. Further, our toolkit and resources have been disseminated on a listserv for CF mental health providers which is open to anyone with an interest in mental health in CF and consists of nearly 400 individuals from 12 countries. Our team helps to moderate communications on the CF Mental Health Listserv. The activity on this listserv indicates that screening has been implemented in many centres across the USA. Additionally, depression and anxiety screening is now a part of the data recorded by the CFF for accredited CF centres. According to the 2018 Patient Registry, 73% of adolescents and 80% of adults in the CF registry received a screening for depression and anxiety that year, although with a wide variation across centres.24
The success of our programme in depression and anxiety screening has been influenced by CFF grants providing funding for an MHC to join the multidisciplinary CF care team. Screening could be provided by other members of the care team if an MHC is not available. Limitations to generalisability could be the strong integration of our adult and paediatric CF centres; many CF centres are completely separate in terms of location and leadership. Barriers to replication of these processes could also be hindered by lack of personnel (such as those who are designated to survey the patients or track data) or lack of buy-in by the CF teams, families or hospital administration. Another limitation to generalisability could include our centre size, as larger centres and very small satellites may have more difficulty implementing screening procedures across all sites. However, the algorithm and processes were tested and successfully implemented in a larger paediatric centre at the Ann & Robert H. Lurie Children’s Hospital in Chicago, which also has multiple clinic sites, thus mitigating this potential limitation.
In addition, the COVID-19 pandemic surfaced the need to convert many processes to telehealth in 2020. A timely publication from Ireland showed that online and paper-based screening for depression and anxiety in adult patients with CF yield comparable findings on prevalence rates and scores,25 lending credence to application of electronic screening methods not yet tested in our QI project. We are in the process of making electronic screening more feasible in our clinic for telehealth visits; right now the visits are conducted by our social worker or MHC verbally.
Conclusion
A stepwise process for depression and anxiety screening and intervention was successful in our paediatric and adult CF centre. We improved the effectiveness of our process uniformity utilising a QI infrastructure. We modified our screening protocol and resources to create a toolkit based on patient, caregiver, staff and another CF centre’s feedback, enabling us to disseminate this screening and intervention to other centres. This process can be a model for integrating depression and anxiety screening and intervention in other CF centres and can serve as a template for a similar programme for those with other chronic illness and their family members.
Acknowledgments
We would like to extend our deepest appreciation to the individuals with CF and their families. We are grateful for the additional Buffalo Mental Health Team members including Carolyn Pardee, PhD and Kimberly Rand LMSW, and the support of patient advocate, Anne Clark. We would like to express our thanks to the patients, parents, psychiatry and psychology colleagues in both Buffalo and Chicago.
Footnotes
Contributors: The authors confirm contribution to the paper as follows: conception and design: DMG, CF, AS, AC, LF, CR, NS, DB and BS; data analysis/interpretation: DMG, CF, AS, AC, LF, CR, NS, DB and BS; draft manuscript preparation: DMG, CF, AS, AC, LF, CR, NS, DB, BS; draft manuscript revision: DMG; all authors approved the final version of the manuscript and are accountable for accuracy.
Funding: This work was supported by the Cystic Fibrosis Foundation Therapeutics (Smith14Q10).
Competing interests: None declared.
Patient and public involvement: Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review: Not commissioned; externally peer reviewed.
Data availability statement
Data are available upon request.
Ethics statements
Patient consent for publication
Not required.
Ethics approval
The project was reviewed by the State University of New York at Buffalo IRB (UBIRB), who found that the activity is not research involving human subjects as defined by DHHS and FDA regulations. This project was undertaken as a quality improvement project.
References
- 1. Quittner AL, Goldbeck L, Abbott J, et al. Prevalence of depression and anxiety in patients with cystic fibrosis and parent caregivers: results of the International depression epidemiological study across nine countries. Thorax 2014;69:1090–7. 10.1136/thoraxjnl-2014-205983 [DOI] [PubMed] [Google Scholar]
- 2. Ploessl C, Pettit RS, Donaldson J. Prevalence of depression and antidepressant therapy use in a pediatric cystic fibrosis population. Ann Pharmacother 2014;48:488–93. 10.1177/1060028013514846 [DOI] [PubMed] [Google Scholar]
- 3. Riekert KA, Bartlett SJ, Boyle MP, et al. The association between depression, lung function, and health-related quality of life among adults with cystic fibrosis. Chest 2007;132:231–7. 10.1378/chest.06-2474 [DOI] [PubMed] [Google Scholar]
- 4. Snell C, Fernandes S, Bujoreanu IS, et al. Depression, illness severity, and healthcare utilization in cystic fibrosis. Pediatr Pulmonol 2014;49:1177–81. 10.1002/ppul.22990 [DOI] [PubMed] [Google Scholar]
- 5. Smith BA, Cogswell A, Garcia G. Vitamin D and depressive symptoms in children with cystic fibrosis. Psychosomatics 2014;55:76–81. 10.1016/j.psym.2013.01.012 [DOI] [PubMed] [Google Scholar]
- 6. Hilliard ME, Eakin MN, Borrelli B, et al. Medication beliefs mediate between depressive symptoms and medication adherence in cystic fibrosis. Health Psychol 2015;34:496–504. 10.1037/hea0000136 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Smith BA, Modi AC, Quittner AL, et al. Depressive symptoms in children with cystic fibrosis and parents and its effects on adherence to airway clearance. Pediatr Pulmonol 2010;45:756–63. 10.1002/ppul.21238 [DOI] [PubMed] [Google Scholar]
- 8. Cronly JA, Duff AJ, Riekert KA, et al. Health-related quality of life in adolescents and adults with cystic fibrosis: physical and mental health predictors. Respir Care 2019;64:406–15. 10.4187/respcare.06356 [DOI] [PubMed] [Google Scholar]
- 9. Yohannes AM, Willgoss TG, Fatoye FA, et al. Relationship between anxiety, depression, and quality of life in adult patients with cystic fibrosis. Respir Care 2012;57:550–6. 10.4187/respcare.01328 [DOI] [PubMed] [Google Scholar]
- 10. Schechter MS, Ostrenga J, Fink A, et al. Five year survival is decreased in CF patients screening positive for depression. Pediatr Pulmonol 2017;52:404–5. [Google Scholar]
- 11. Barker DH, Quittner AL. Parental depression and pancreatic enzymes adherence in children with cystic fibrosis. Pediatrics 2016;137:e20152296. 10.1542/peds.2015-2296 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Procedural anxiety. Available: https://www.cff.org/Life-With-CF/Daily-Life/Emotional-Wellness/Procedural-Anxiety/ [Accessed 06 Apr 2020].
- 13. Nusbaum K, Filigno SS, Feldstein J, et al. Assessing and responding to stress related to pulmonary function testing in cystic fibrosis through quality improvement. Pediatr Pulmonol 2020;55:1139–46. 10.1002/ppul.24673 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Trask PC, Paterson AG, Wang C, et al. Cancer-specific worry interference in women attending a breast and ovarian cancer risk evaluation program: impact on emotional distress and health functioning. Psychooncology 2001;10:349–60. 10.1002/pon.510 [DOI] [PubMed] [Google Scholar]
- 15. Quittner AL, Abbott J, Georgiopoulos AM, et al. International Committee on mental health in cystic fibrosis: cystic fibrosis Foundation and European cystic fibrosis Society consensus statements for screening and treating depression and anxiety. Thorax 2016;71:26–34. 10.1136/thoraxjnl-2015-207488 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. American Psychiatric Association (APA) . Diagnostic and statistical manual of mental disorders. 5th edn. Arlington, VA: American Psychiatric Publishing, 2013. [Google Scholar]
- 17. Kroenke K, Spitzer RL, Williams JBW. The patient health Questionnaire-2: validity of a two-item depression screener. Med Care 2003;41:1284–92. 10.1097/01.MLR.0000093487.78664.3C [DOI] [PubMed] [Google Scholar]
- 18. Löwe B, Kroenke K, Gräfe K. Detecting and monitoring depression with a two-item questionnaire (PHQ-2). J Psychosom Res 2005;58:163–71. 10.1016/j.jpsychores.2004.09.006 [DOI] [PubMed] [Google Scholar]
- 19. Löwe B, Wahl I, Rose M, et al. A 4-item measure of depression and anxiety: validation and standardization of the patient health Questionnaire-4 (PHQ-4) in the general population. J Affect Disord 2010;122:86–95. 10.1016/j.jad.2009.06.019 [DOI] [PubMed] [Google Scholar]
- 20. Mitchell AJ, Coyne JC. Do ultra-short screening instruments accurately detect depression in primary care? A pooled analysis and meta-analysis of 22 studies. Br J Gen Pract 2007;57:144–51. [PMC free article] [PubMed] [Google Scholar]
- 21. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med 2001;16:606–13. 10.1046/j.1525-1497.2001.016009606.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Posner K, Brown GK, Stanley B, et al. The Columbia-Suicide severity rating scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am J Psychiatry 2011;168:1266–77. 10.1176/appi.ajp.2011.10111704 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Goetz DM, Frederick C, Cogswell A, et al. Developing and Sustaining a Model for Depression and Anxiety Screening & Stepped Care Treatment: Year Four of the Buffalo Quality Improvement Initiative. Pediatr Pulmonol 2017:519. [Google Scholar]
- 24. Cystic Fibrosis Foundation Patient Registry . Annual data report. ©2019 cystic fibrosis Foundation. Bethesda, Maryland, 2018. [Google Scholar]
- 25. Cronly J, Duff AJ, Riekert KA, et al. Online versus paper-based screening for depression and anxiety in adults with cystic fibrosis in Ireland: a cross-sectional exploratory study. BMJ Open 2018;8:e019305. 10.1136/bmjopen-2017-019305 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data are available upon request.