

Abstract
Caffeine use is widespread, and its consumption increases during periods of stress. Caffeine raises blood pressure by elevating vascular resistance, and this effect is larger and more prolonged in hypertensive patients than in normotensive. The pressor response to caffeine occurs eqully in persons at rest and under stress. The elevated baseline pressures of the hypertensive patient are therefore increased by both caffeine and stress, potentially leading to undesirably high pressures. Such combined effects on blood pressure may potentially confound the evaluation of hypertension, and possibly reduce the effectiveness of antihypertensive therapy. These effects are not abolished by pharmacologic tolerance to caffeine, as tolerance may not be complete with daily intake. The contribution of caffeine's effects to the development of hypertension warrants continued study, and caffeine use by patients merits consideration in terms of assessment and management of this disorder.
Caffeine is the most widely consumed pharmacologic agent. 1 Its beneficial effects 2 , 3 include increased alertness 4 and a mild experience of reward. 5 Its mildly addictive properties may account for the enduring popularity of caffeinated beverages 6 and the increased use of coffee during times of enhanced work stress. 7 About 40% of persons 18–74 years of age in the United States drink coffee or tea three or more times daily, 8 and only 9%–16% report being caffeine abstainers. 9 Intake in the United States averages about 250 mg/day, 1 the equivalent of approximately 3 cups of coffee and 6 cups of tea, and, in Australia, 240 mg/day. 10 Consumption increases up to middle age and then levels off, with similar intake patterns in women and men. 1
Caffeine has attracted attention for its ability to raise blood pressure (BP), 11 , 12 which has led to interest in its relationship to hypertension. 13 Although definitive evidence is lacking that caffeine contributes to sustained hypertension, its central nervous system stimulation and pressor effects merit practical consideration in evaluation and management of the hypertensive patient.
CAFFEINE PHARMACOLOGY
Caffeine is a methylated xanthene that acts on all tissues. 14 It is metabolized in the liver, primarily by the cytochrome P‐450 1A2 enzyme. 15 Its half‐life varies widely among individuals, ranging from 1–10 hours, with a mean of about 4.5 hours. 16
At dietary doses, caffeine's physiologic effects are due to its competitive antagonism of adenosine A1 and A2 receptors. 17 , 18 , 19 , 20 Adenosine is released from all tissues as a byproduct of cellular metabolism, and it then serves as a local regulator of cellular activity. 21 In the cardiovascular system, adenosine lowers the heart rate 22 , 23 , 24 and counteracts myocardial ischemia by antagonizing β‐adrenergic stimulation. 25 Adenosine dilates the blood vessels by reducing norepinephrine release at sympathetic nerve terminals 26 and reducing contraction of smooth muscle cells. 27 Caffeine interferes with the local action of adenosine in the blood vessel wall. Because of the importance of adenosine regulation, caffeine use should be considered in relation to hypertension and stress. 28
Effects of Caffeine on BP
Caffeine acutely elevates BP at rest 12 , 29 and during mental and exercise stress. 30 , 31 , 32 , 33 , 34 , 35 Dietary doses (90–350 mg, corresponding to 1–4 cups of brewed coffee) 36 can elevate BP by as little as 3/4 mm Hg and as much as 14/13 mm Hg. 13 Pressor effects appear in 15–60 minutes and last for 3–4 hours, 12 , 29 , 30 with similar effects in men and women. 37 , 38 The BP rise in response to caffeine increases progressively with doses up to approximately 3 mg/kg of body weight (which is equivalent to about 210 mg, or 2.5 cups of coffee in a 150‐lb man). Higher doses do not produce any increase in this response, 12 suggesting that adenosine receptors are well occupied in the lower dose range. The acute BP effect of coffee is due to its caffeine content and not to other constituents. 13 We have shown that caffeine's pressor effect is caused by a rise in peripheral vascular resistance that begins about 15 minutes after oral intake. 29 , 39 , 40 , 41
The combined BP effects of caffeine and stress, including mental stress 31 , 42 , 43 and isometric 42 , 44 or dynamic exercise, 32 observed in these laboratory studies are usually found to be additive, such that the BP rise in response to a stressor along with caffeine usually equals the sum of the responses to caffeine alone and the stressor alone. Ambulatory and workplace studies also show that caffeine increases BP during daily activities 45 , 46 , 47 , 48 and that caffeine and work stress cause additive increases in BP. 49 , 50
Effects of Caffeine in Hypertension
Caffeine's effect on BP in daily life and during times of stress leads to consideration of its effects in hypertension. Caffeine increases BP in hypertensives, whether or not they are taking antihypertensive medication, 51 , 52 , 53 , 54 and its effect may be greater in older patients. 55 In studies comparing hypertensives with controls, caffeine's effects were greater and more prolonged in hypertensives 53 , 54 , 56 and in high‐risk normotensives 57 (defined as having a positive family history of hypertension and a normal to high‐normal resting BP, according to the Joint National Committee [JNC] VI classifications [130–140/80–90 mm Hg]). 58 We concluded that hypertensives are more sensitive to caffeine's effects than are normotensives. 57 For example, in hypertensives not on medication, a single caffeine dose (equivalent to 2–3 cups of coffee) caused a 10‐mm Hg increase in diastolic BP for 180 minutes of study. In normotensive controls, changes were smaller and briefer, about 6 mm Hg and turning toward baseline within 90 minutes. 54 One cup of coffee has lesser effects.
We recently compared caffeine responses among 182 men in five risk categories based on the JNC VI classification 59 (Figure). Caffeine raised BP in all groups, with increasing effects in high‐normal, stage 1, and treated hypertensives, whose systolic/diastolic BP response was 1.5 times that of the optimal BP group (p<0.0001 and <0.02, respectively). While all subjects in the optimal and normal BP groups remained normotensive after caffeine intake, Bps of 140/90–159/95 mm Hg occurred in 19% of high‐normal, 15% of stage 1, and 89% of men under treatment for hypertension.
Figure.
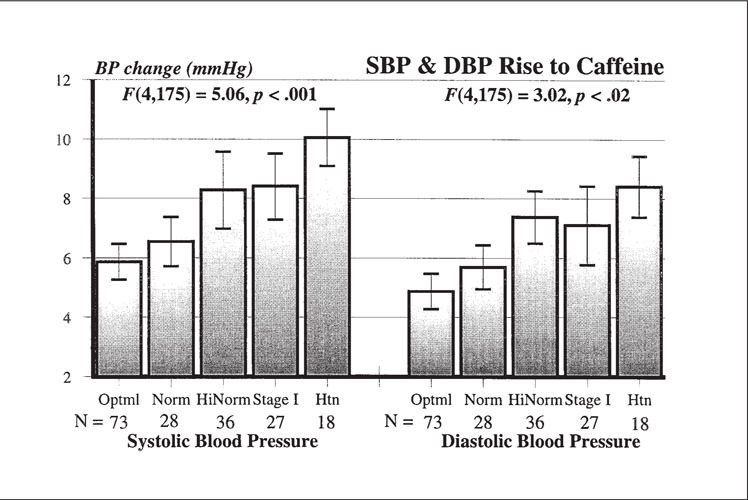
Systolic and diastolic blood pressure (SBP/DBP) increases on oral caffeine intake (3.3 mg/kg, equivalent to about 2.5–3 cups of coffee in a 150–175‐lb man) in five groups stratified by risk for hypertension (Htn) according to Joint National Committee (JNC) VI 58 criteria. There were 73 with optimal (Optml) Bps (<120/80 mm Hg), 28 with normal (Norm) Bps (120/80–129/84 mm Hg), 36 with high‐normal (HiNorm) Bps (130/85–139/89 mm Hg), 27 with stage 1 hypertension (140/90–159/99 mm Hg), and 18 who had been medicated for hypertension and had been withdrawn from medication for 2–4 weeks. Reprinted with permission from Hypertension. 2000;36:137–141. 59
This larger BP increase with caffeine in high‐risk and hypertensive groups is associated with a larger increase in peripheral resistance. 57 After a 3.3‐mg/kg dose of caffeine, stage 1 men had diastolic BP rises and peripheral resistance responses 2–3 times greater than those seen in the optimal BP controls (+8.4 vs. +3.8 mm Hg and +135 vs. +45 dyne·sec·cm−5, respectively). Although all subjects had Bps of <140/85 mm Hg at baseline, 33% of stage 1 men reached these levels after caffeine, while optimal BP controls remained normotensive throughout.
Caffeine, Hypertension, and Stress
Large, prolonged responses to caffeine in hypertensive men suggest that the addition of a stressor could result in still higher Bps. We examined this possibility in the laboratory with 19 optimal BP controls with negative parental histories vs. 20 high‐risk men, as defined above. 39 BP responses to a psychomotor task combined with caffeine were additive and similar in size for both groups. However, the high‐risk group started with higher pressures, and so the combined effects resulted in transient BP elevations into the stage 1–2 range for 50% of high‐risk subjects vs. 26% of controls (p<0.03). In a subsequent study, during 1 hour of psychomotor tasks and mental arithmetic, stage 1 men had larger systolic and diastolic BP increases over all postcaffeine periods than optimal BP controls (p<0.04 and p<0.04) and larger diastolic BP rises in response to the tasks after caffeine (p=0.007). 60 The stage 1 men also had less tendency to return to baseline during a 20‐minute recovery period.
During dynamic exercise, caffeine can cause significant rises in BP and peripheral vascular resistance relative to placebo (p<0.01). 32 These effects may be greater in high‐risk normotensives (positive family history and high‐normal BP), and some of these high‐risk persons may be especially sensitive to caffeine during exercise, experiencing occasional exaggerated Bps (≥230/100 mm Hg). Some have argued that an exaggerated BP response to exercise in normotensives may be a marker of future hypertension. 61 We tested caffeine in 34 normotensives, including 20 high‐risk subjects and 14 low‐risk optimal BP controls. 32 During supine bicycle exercise under placebo, seven high‐risk men, vs. none with low risk, had exaggerated BP. Caffeine given before the bicycle exercise increased the number of exaggerated responders (those with one or more Bps ≥230/100 mm Hg) to 12 in the high‐risk group vs. only three with low risk. The seven high‐risk men with exaggerated responses (one or more exercise Bps ≥230/100 mm Hg) under placebo also had the greatest increases in peripheral resistance in response to caffeine and the greatest BP responses to exercise with caffeine, 33 and the same seven had exaggerated BP rises during a Bruce treadmill protocol on a different day. 62 We speculate that the persons at greatest risk for future hypertension may be those with the greatest responses to stress and to caffeine, although prospective studies need to be done. It might be hypothesized that the habitual use of caffeine reduces the effectiveness of exercise as a nonpharmacologic treatment for hypertension.
In addition, relative to normotensives, we have shown that hypertensives may have prolonged BP increases to caffeine alone 54 and sustained, exaggerated BP responses to exercise following a dose of caffeine. 40 During 30 minutes of bicycle exercise, caffeine (3.3 mg/kg) caused untreated hypertensives to have sustained diastolic BP responses over the entire 30 minutes, whereas diastolic BP of controls returned to baseline after 15 minutes. 40 Seven of 18 hypertensives vs. one of 12 controls had exaggerated BP readings (≥230/100 mm Hg), and hypertensives also maintained a greater rise in the rate‐pressure product (systolic BP × heart rate, an index of myocardial oxygen demand). 63
Collectively, these studies of caffeine, stress, and hypertension suggest that hypertensives and high‐risk normotensives may be sensitive to caffeine, and the addition of mental or exercise stress can lead to sustained and undesirable elevations in BP.
Although most studies have been done in the laboratory, in one ambulatory study, 64 older hypertensives had significant BP elevations during 2 weeks on a caffeine diet vs. a caffeine‐free diet, although no BP effect was seen in normotensives. In an ambulatory study of male medical students, 50 20 high‐risk (positive family history and high‐normal BP) students had larger BP responses to caffeine (+5/4 vs. +3/3 mm Hg; p<0.05) and to examination stress (+4/1 vs. +7/3 mm Hg; p<0.05) than did the 11 low‐risk controls (negative family history of hypertension and largely optimal BP by JNC VI criteria 58 ). The examination combined with caffeine caused additive increases in BP, such that in the high‐risk men, 46% had average systolic BP of ≥140 mm Hg and 36% had diastolic BP of >90 mm Hg. The finding that stress and caffeine act in concert to raise BP in daily life emphasizes the potential importance of caffeine effects on BP in persons with a hypertensive predisposition.
This BP sensitivity in hypertension risk is parallelled by a tendency to greater stress hormone secretion. Caffeine elevates adrenocorticotropin and cortisol. 65 High‐risk men are more likely than controls to have a cortisol response to caffeine or mental stress alone, and the combined effect of stress and caffeine is greater in high‐risk individuals 66 , 67 and in stage 1 hypertensives. 68 Caffeine also increases cortisol in medical students during low‐ and high‐stress school days, and its effect is additive to the effect of exams. 50
Caffeine Tolerance and Dependence
A significant consideration in evaluating caffeine effects is the widely held view that daily caffeine use leads to complete tolerance within 3–5 days. 16 , 69 The evidence for tolerance includes the following: 1) chronic exposure up‐regulates adenosine receptor density 70 ; 2) habitual caffeine use produces signs of dependence and symptoms of withdrawal, including dysphoria and headache 71 , 72 , 73 ; and 3) withdrawal is relieved by caffeine. 74
However, chronic tolerance to caffeine is only partial, and a degree of response remains even with daily intake. Tolerance to most of caffeine's central nervous system effects is not complete, 75 and our view is that tolerance may vary from system to system and from person to person. Evidence for incomplete tolerance in caffeine's pressor effects comes from several sources. In population screenings, casual Bps are higher in self‐reported users than in nonusers 76 and are also higher in those with higher current blood levels of caffeine. 77 Habitual intake is not inversely related to acute BP response to caffeine. 12 , 41 , 50 , 78 , 79 , 80 In regular consumers, caffeine consistently raises BP, cortisol, and catecholamines after an overnight abstinence. 29 , 54 , 78 , 81 , 82
In controlled trials, caffeine administration can increase BP, even with repeated dosing, 14 , 46 , 47 , 83 and caffeine withdrawal can lower BP 38 over a period of weeks, 37 , 84 , 85 although this effect is not always observed. 86 Two studies examined tolerance more directly. Denaro et al. 87 tested placebo vs. low (4.2 mg/kg) or high (12 mg/kg) doses of caffeine for 5 days each in a randomized crossover design. Some subjects showed complete tolerance, while others had a persistent BP response, with elevations of +10/+10 mm Hg even in the high‐dose condition. Using a rigorous crossover design, James 38 found laboratory and ambulatory Bps still elevated by caffeine (200 mg × 3/day) after 1 week of daily intake. Pharmacokinetic and pharmacodynamic modeling suggests that tolerance develops and diminishes quickly, as with overnight abstinence, and with substantial individual differences. 14 A meta‐analysis of the existing controlled trials 34 indicated that caffeine's effects on BP persist with regular use.
CLINICAL CONSIDERATIONS REGARDING CAFFEINE USE IN HYPERTENSION
Caffeine has not been clearly associated with the development or progression of hypertension in epidemiologic studies, so a possible role for caffeine in the development of hypertension is unproved. Nurminen and colleagues 13 noted that a clear relationship between caffeine and hypertension has been difficult to demonstrate because study designs have allowed for variation in the time between last caffeine intake and BP readings and have not accounted for individual differences in tolerance.
Although caffeine's effect on BP in habitual users appears to be small, on the order of 2–5 mm Hg, its use may not be benign in regard to hypertension. Whelton 88 notes, “A 2–3‐mm Hg average reduction in those with a high‐normal blood pressure should result in a 25%–50% decrease in the incidence of hypertension.”
There is little information on caffeine effects in women and blacks, 89 , 90 a matter of interest because of differences between black and white patients in the prevalence and mechanisms of hypertension 91 and because of the increase in hypertension among women after menopause. 58
Initial Evaluation of Hypertension
The JNC 58 recommends that evaluation of hypertension include BP measurement under standardized conditions, calling for at least two or three readings separated by 2 or more minutes, taken after the patient has been seated for 5 minutes. In the event that BP is above 130/85 mm Hg, evaluation should include identification of known causes of high BP, assessment of target organ damage, and identification of other cardiovascular risk factors. According to the BP level, follow‐up should be undertaken in 1 week to 2 years.
The studies reviewed above show that caffeine can complicate the evaluation of hypertension for several reasons: 1) caffeine may elevate BP over a period of 3–4 hours in the laboratory and in the workplace; 2) repeated caffeine doses will sustain BP elevations for still longer periods; 3) caffeine effects on BP may be larger in hypertensives; 4) caffeine may have larger or more prolonged effects under circumstances that interfere with clearance or metabolism; 5) caffeine tolerance is incomplete, even in habitual users; and 6) persons at greatest risk for hypertension may be especially reactive to clinic BP evaluation—the well known “white coat” effect, 92 and caffeine intake before a clinic visit may further increase BP in these cases. Caffeine use before clinic visits or during home monitoring or 24‐hour ambulatory monitoring may therefore add misleading variability to BP on single visits and across follow‐up visits. Avoidance of caffeine by patients on days of clinic visits and during home monitoring or 24‐hour ambulatory monitoring would eliminate the effect of caffeine as a variable source of BP elevation during patient evaluation.
Management of Hypertension
Management of hypertension calls for a staged approach. First‐line treatment calls for lifestyle modification, including emphasis on dietary factors and exercise, 58 with the goal of eliminating causes of BP elevation and reducing the risk of atherosclerosis and stroke. Since controllable factors that elevate BP are to be avoided, restriction of caffeine intake may be considered. Caffeine use may potentially reduce the effectiveness of lifestyle modifications, such as exercise, particularly in persons whose responses to caffeine are greater than average. The sensitivity of hypertensive persons to caffeine's pressor effects also calls attention to their use of foods, herbal remedies, and medications that may compete for liver enzyme systems that metabolize caffeine and thereby potentially prolong or increase caffeine's pressor effects. Table I lists common sources of caffeine interactions with prescription medications.
Table I.
| Precipitant Drug | Effect | Description |
| Beta blockers (atenol, propanol) | — | Caffeine effect is similar with and without β blockers. Caffeine reduces the antihypertensive effect of these drugs |
| Cimetidine (Tagamet®, Zantac®) | ↑ | Caffeine hepatic metabolism may be impaired, increasing caffeine |
| Disulfiram (Antabuse®) | ↑ | |
| Fluoroquinolones (Cipro®, norfloxacin) | half‐life and caffeine effect | |
| Terbinafine (Lamisil®) | ↑ | |
| Contraceptives, oral (Ortho‐Cyclen®, Alesse™, Triphasil®) | ↑ | |
| Mexiletine (Mexitil®) | ↑ | Caffeine elimination may be reduced 30%–50% (effect may be greater) |
| Phenylpropanolamine (Accutrim®, Dexatrim®) | ↑ | Serum caffeine levels may be increased Caffeine effects are enhanced |
The next stage of hypertension management calls for continued lifestyle modification with the addition of gradually titrated drug therapy. Caffeine may reduce the effectiveness of some antihypertensive agents, particularly that of β blockers, 93 although it may not affect the response to calcium channel blockers. 94 The potential for caffeine to counteract the antihypertensive actions of some agents is an additional consideration in terms of dietary recommendations for persons undergoing treatment for hypertension.
Although evidence is limited, particularly in certain groups, caffeine abstinence may be a useful, safe, and easily implemented component of the spectrum of lifestyle modifications now in use for hypertension prevention and nonpharmacologic treatment. Table II summarizes these recommendations.
Table II.
Considerations for Evaluation and Management of Hypertension in Caffeine Consumers
| Hypertension Evaluation in Caffeine Consumers | Strength of Evidence |
| Caffeine raises blood pressure acutely: | ++++ |
| For 3–4 hours after intake | +++ |
| After repeated doses | +++ |
| Even in habitual users | +++ |
| During mental and exercise stress | ++ |
| To a larger degree in hypertensives | ++ |
| For a more prolonged time in hypertensives | ++ |
| For a longer time in persons with altered liver metabolism | + |
| Additively with “white coat” blood pressure responses in the clinic | + |
| During home monitoring or 24‐hour ambulatory monitoring | + |
| Hypertension Management in Caffeine Consumers | |
| Caffeine may increase blood pressure: | |
| Differently from clinic visit to clinic visit | + |
| During antihypertensive treatment | ++ |
| During lifestyle interventions, such as exercise | ++ |
| ++++ Strong evidence consistent over a range of studies +++ Consistent evidence over a number of studies ++ Evidence from a limited number of studies or from single sources + Indirect evidence from related studies | |
Additional Clinical Considerations
Caffeine‐induced BP elevation may interact with several conditions that alter the regulation of BP. In postprandial hypotension, caffeine may actually be of benefit through modest BP elevation. 95 However, caffeine's pressor effects may be undesirable in a number of age‐related conditions. The loss of estrogen at menopause lowers the compliance of the blood vessel wall, causing caffeine to have larger pressor effects in postmenopausal women not receiving hormone replacement. 96 Arteriosclerosis and isolated systolic hypertension, two conditions common among the elderly, both elevate cardiac afterload and increase the risk of left ventricular hypertrophy. Because caffeine raises systolic BP, it may potentially compound the increased afterload. Evaluation of chronic congestive heart failure sometimes involves the use of elevated catecholamine levels as a prognostic guide, 97 and caffeine's tendency to increase circulating epinephrine may complicate these assessments. 13 Sleep apnea is considered a risk factor for hypertension, possibly resulting from an endogenous digitalis‐like factor that can increase vascular resistance. 98 Therefore, caffeine's ability to interfere with sound sleep and to raise vascular resistance may potentially contribute to hypertension in sleep apnea, although controlled trials have not yet been performed.
SUMMARY
Caffeine elevates BP and stress hormone secretion. These effects are larger and more prolonged in primary hypertension in persons at high risk of developing hypertension. Stress combined with caffeine exerts additive effects on BP and stress hormones. The combination of caffeine and stress in the workplace can cause elevated BP over a period of hours, with greater effects on persons at risk for hypertension. The combination of caffeine and stress may result in undesirably high Bps during the 2–4‐hour acute phase of the caffeine response, and this effect is not entirely eliminated in regular consumers of caffeine.
An influence of caffeine on the development or progression of hypertension, or its end points, has not yet been established, although some clinical considerations seem reasonable. Because caffeine is a pressor agent, its daily use may be undesirable in persons likely to develop hypertension. In patients undergoing evaluation for hypertension, unmonitored use of caffeine may have variable effects on BP and compromise the reliability of BP readings in the clinic or home, or on ambulatory monitoring. In persons being treated for hypertension, whether by pharmacologic or nonpharmacologic means, caffeine may elevate blood pressure during a portion of the day, potentially reducing the effectiveness of therapy. Caffeine may also have undesirable BP effects in persons at elevated risk for secondary hypertension, including the elderly, persons with arteriosclerosis, postmenopausal women, and those with sleep apnea. These considerations may call for dietary restriction of caffeine in patients who are under evaluation for hypertension or who are being managed for the disorder.
Acknowledgments: Supported by the Medical Research Service of the Department of Veterans Affairs and by Grants HL 32050 and HL 32050‐S2 from the National Heart, Lung, and Blood Institute, Bethesda, MD.
References
- 1. James JE. Understanding Caffeine. Thousand Oaks, CA: Sage; 1997. [Google Scholar]
- 2. Kawachi I, Willett WC, Colditz GA, et al. A prospective study of coffee drinking and suicide in women. Arch Intern Med. 1996;156:521–525. [PubMed] [Google Scholar]
- 3. Ross GW, Abbott RD, Petrovitch H, et al. Association of coffee and caffeine intake with the risk of Parkinson disease. JAMA. 2000;283:2674–2679. [DOI] [PubMed] [Google Scholar]
- 4. Rainne DG, Grunze HCR, McCarley RW, et al. Adenosine inhibition of mesopontine cholinergic neurons: implications for EEG arousal. Science. 1994;263:689–692. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Daly JW, Fredholm BB. Caffeine—an atypical drug of dependence. Drug Alcohol Depend. 1998;5:199–206. [DOI] [PubMed] [Google Scholar]
- 6. Griffiths RR, Woodson PP. Reinforcing properties of caffeine: studies in humans and laboratory animals. Pharmacol Biochem Behav. 1988;29:419–427. [DOI] [PubMed] [Google Scholar]
- 7. Conway TL, Vickers RR, Ward HW, et al. Occupational Stress and Variation in Cigarette, Coffee, and Alcohol Consumption. Washington, DC: Bureau of Medicine and Surgery, Department of the Navy, Research Work Unit, ZF51.524.002–5020; 1979 (Report No. 79–32). [Google Scholar]
- 8. Dresser CMV. Food Consumption Profiles of White and Black Persons Aged 1–74 Years: United States, 1971–74. Washington, DC: US Government Printing Office; 1979. DHEW Monograph, US Public Health Service publication No. 79‐1658.. [Google Scholar]
- 9. Hughes JR, Oliveto AH. A systematic survey of caffeine intake in Vermont. Exp Clin Psychopharmacol. 1997; 5:393–398. [DOI] [PubMed] [Google Scholar]
- 10. Shirlow MJ. Patterns of caffeine consumption. Hum Nutr Appl Nutr. 1983;37:307–313. [PubMed] [Google Scholar]
- 11. Robertson D, Frolich JC, Carr RK, et al. Effects of caffeine on plasma renin activity, catecholamines and blood pressure. N Engl J Med. 1978;298:181–186. [DOI] [PubMed] [Google Scholar]
- 12. Whitsett TL, Manion CV, Christensen HD. Cardiovascular effects of coffee and caffeine. Am J Cardiol. 1984;53:918–922. [DOI] [PubMed] [Google Scholar]
- 13. Nurminen ML, Niittynen L, Korpela R, et al. Coffee, caffeine and blood pressure: a critical review. Eur J Clin Nutr. 1999;53:831–839. [DOI] [PubMed] [Google Scholar]
- 14. Shi J, Benowitz NL, Denaro CP, et al. Pharmacokinetic‐pharmacodynamic modeling of caffeine: tolerance to pressor effects. Clin Pharmacol Ther. 1993;53:6–14. [DOI] [PubMed] [Google Scholar]
- 15. Berthou F, Flinois JP, Ratanasavanh D, et al. Evidence for the involvement of several cytochromes P‐450 in the first steps of caffeine metabolism by human liver microsomes. Drug Metab Dispos. 1991;19:561–567. [PubMed] [Google Scholar]
- 16. Robertson D, Wade D, Workman R, et al. Tolerance to the humoral and hemodynamic effects of caffeine in man. J Clin Invest. 1981;67:1111–1117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Fredholm BB. Astra Award Lecture. Adenosine, adenosine receptors and the actions of caffeine. Pharmacol Toxicol. 1995;76:93–101. [DOI] [PubMed] [Google Scholar]
- 18. Hoyle CHV. Transmission: Purines. In: Burnstock G, Hoyle CHV, eds. Autonomic Neuroeffector Mechanisms. New York, NY: Harwood Academic Publishers; 1992:367–408. [Google Scholar]
- 19. Biaggioni I, Paul S, Puckett A, et al. Caffeine and theophylline as adenosine receptor antagonists in humans. J Pharmacol Exp Ther. 1991;258:588–593. [PubMed] [Google Scholar]
- 20. Fredholm BB, Sollevi A. Cardiovascular effects of adenosine. Clin Physiol. 1986;6:1–21. [DOI] [PubMed] [Google Scholar]
- 21. Worku Y, Newby AC. The mechanism of adenosine production in rat polymorphonuclear leukocytes. Biochem J. 1983;214:325–330. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Freilich A, Tepper D. Adenosine and its cardiovascular effects. Am Heart J. 1992;123:1324–1328. [DOI] [PubMed] [Google Scholar]
- 23. Mosqueda‐Garcia R, Robertson D, Robertson RM. The cardiovascular effects of caffeine. In: Garattini S., ed. Coffee, Caffeine, and Health. New York, NY: Raven Press; 1993:157–193. [Google Scholar]
- 24. Belardinelli L, Linden J, Berne R. The cardiac effects of adenosine. Prog Cardiovasc Dis. 1989;32:73–97. [DOI] [PubMed] [Google Scholar]
- 25. Sato H, Masatsug UH, Kitakaze M, et al. Endogenous adenosine blunts beta‐adrenoceptor‐mediated response in hypoperfused canine myocardium. Circulation. 1992;85:1594–1603. [DOI] [PubMed] [Google Scholar]
- 26. Su C. Purinergic inhibition of adrenergic transmission in rabbit blood vessels. J Pharmacol Exp Ther. 1978;205:351–361. [PubMed] [Google Scholar]
- 27. Costa F, Sulur P, Angel M, et al. Intravascular source of adenosine during forearm ischemia in humans: implications for reactive hyperemia. Hypertension. 1999;33:1453–1457. [DOI] [PubMed] [Google Scholar]
- 28. Yamada K, Goto A, Ishii M, et al. Plasma adenosine concentrations are elevated in conscious spontaneously hypertensive rats. Clin Exp Pharmacol Physiol. 1992;19:563–567. [DOI] [PubMed] [Google Scholar]
- 29. Pincomb GA, Lovallo WR, Passey RL, et al. Effects of caffeine on vascular resistance, cardiac output, and myocardial contractility in young men. Am J Cardiol. 1985;56:119–122. [DOI] [PubMed] [Google Scholar]
- 30. Horst K, Jenkins WL. The effect of caffeine, coffee and decaffeinated coffee upon blood pressure, pulse rate and simple reaction time of men of various ages. J Pharmacol. 1935;50:385–395. [Google Scholar]
- 31. Lane JD. Caffeine and cardiovascular responses to stress. Psychosom Med. 1983;51:373–380. [DOI] [PubMed] [Google Scholar]
- 32. Sung BH, Lovallo WR, Pincomb GA, et al. Effects of caffeine on blood pressure response during exercise in normotensive healthy young men. Am J Cardiol. 1990;65:909–913. [DOI] [PubMed] [Google Scholar]
- 33. Pincomb GA, Wilson MF, Sung BH, et al. Effects of caffeine and exercise on pressure regulation in men at risk for hypertension. Am Heart J. 1991;122:1107–1115. [DOI] [PubMed] [Google Scholar]
- 34. Jee SH, He J, Whelton PK II, et al. The effect of chronic coffee drinking on blood pressure: a meta‐analysis of controlled clinical trials. Hypertension. 1999;33:647–652. [DOI] [PubMed] [Google Scholar]
- 35. Piha SJ. Effect of acute dose of caffeine on cardiovascular autonomic responses in healthy subjects. Clin Physiol. 1994; 14:411–417. [DOI] [PubMed] [Google Scholar]
- 36. Barone JJ, Roberts HR. Caffeine consumption. Food Chem Toxicol. 1996;34:119–129. [DOI] [PubMed] [Google Scholar]
- 37. Bak AA, Grobbee DE. A randomized study on coffee and blood pressure. J Hum Hypertens. 1990;4:259–264. [PubMed] [Google Scholar]
- 38. James JE. Chronic effects of habitual caffeine consumption on laboratory and ambulatory blood pressure. J Cardiovasc Risk. 1994;1:159–164. [DOI] [PubMed] [Google Scholar]
- 39. Lovallo WR, Pincomb GA, Sung BH, et al. Hypertension risk and caffeine's effect on cardiovascular activity during mental stress. Health Psychol. 1991;10:236–243. [DOI] [PubMed] [Google Scholar]
- 40. Sung BH, Lovallo WR, Whitsett T, et al. Caffeine elevates blood pressure response to exercise in mild hypertensive men. Am J Hypertens. 1995;8:1184–1188. [DOI] [PubMed] [Google Scholar]
- 41. Pincomb G, Sung B, Sausen K, et al. Consistency of cardiovascular response pattern to caffeine across multiple studies using impedance and nuclear cardiography. Biol Psychol. 1993;36:131–138. [DOI] [PubMed] [Google Scholar]
- 42. France C, Ditto B. Cardiovascular responses to the combination of caffeine and mental arithmetic, cold pressor, and static exercise stressors. Psychophysiology. 1992;29:272–282. [DOI] [PubMed] [Google Scholar]
- 43. Pincomb GA, Lovallo WR, Passey RB, et al. Effect of behavior state on caffeine's ability to alter blood pressure. Am J Cardiol. 1988;61:798–802. [DOI] [PubMed] [Google Scholar]
- 44. Pincomb GA, Lovallo WR, Wilson MF. The interactive effects of caffeine and isometric handgrip exercise. Psychophysiology. 1985;22:608–609. [Google Scholar]
- 45. France C, Ditto B. Cardiovascular responses to occupational stress and caffeine in telemarketing employees. Psychosom Med. 1989;51:145–151. [DOI] [PubMed] [Google Scholar]
- 46. Green PJ, Suls J. The effects of caffeine on ambulatory blood pressure, heart rate, and mood in coffee drinkers. J Behav Med. 1996;19:111–128. [DOI] [PubMed] [Google Scholar]
- 47. Jeong DU, Dimsdale JE. The effects of caffeine on blood pressure in the work environment. Am J Hypertens. 1990; 3:749–753. [DOI] [PubMed] [Google Scholar]
- 48. Myers MG, Reeves RA. The effect of caffeine on daytime ambulatory blood pressures. Am J Hypertens. 1991;4:427–431. [DOI] [PubMed] [Google Scholar]
- 49. Pincomb GA, Lovallo WR, Passey RB, et al. Caffeine enhances the physiological response to occupational stress in medical students. Health Psychol. 1987;62:101–112. [DOI] [PubMed] [Google Scholar]
- 50. Shepard JD, Al'Absi M, Whitsett TL, et al. Additive pressor effects of caffeine and stress in male medical students at risk for hypertension. Am J Hypertens. 2000;13:475–481. [DOI] [PubMed] [Google Scholar]
- 51. Freestone S, Ramsay LE. Effect of coffee and cigarette smoking on the blood pressure of untreated and diuretic‐treated hypertensive patients. Am J Med. 1982;73:348–353. [PubMed] [Google Scholar]
- 52. Goldstein IB, Shapiro D. The effects of stress and caffeine on hypertensives. Psychosom Med. 1987;49:226–235. [DOI] [PubMed] [Google Scholar]
- 53. Smits P, Pieters G, Thien T. The role of epinephrine in the circulatory effects of coffee. Clin Pharmacol Ther. 1986;40:431–437. [DOI] [PubMed] [Google Scholar]
- 54. Sung BH, Whitsett TL, Lovallo, WR , et al. Prolonged increase in blood pressure by a single oral dose of caffeine in mild hypertensive men. Am J Hypertens. 1994;7:755–758. [DOI] [PubMed] [Google Scholar]
- 55. Rachima‐Maoz C, Peleg E, Rosenthal T. The effect of caffeine on ambulatory blood pressure in hypertensive patients. Am J Hypertens. 1998;11:1426–1432. [DOI] [PubMed] [Google Scholar]
- 56. Greenstadt L, Yang L, Shapiro D. Caffeine, mental stress, and risk for hypertension: a cross‐cultural replication. Psychosom Med. 1988;50:15–22. [DOI] [PubMed] [Google Scholar]
- 57. Pincomb GA, Lovallo WR, McKey BS, et al. Acute blood pressure effects of caffeine in men with borderline to mild hypertension. Am J Cardiol. 1996;75:270–274. [DOI] [PubMed] [Google Scholar]
- 58. Joint National Committee . The Sixth Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Arch Intern Med. 1997;157:2413–2446. [DOI] [PubMed] [Google Scholar]
- 59. Hartley TR, Sung BH, Pincomb GA, et al. Hypertension risk status and caffeine's effect on blood pressure. Hypertension. 2000;36:137–141. [DOI] [PubMed] [Google Scholar]
- 60. Lovallo WR, Al'Absi M, Pincomb GA, et al. Caffeine raises blood pressure during extended mental stress in borderline hypertensive men. Int J Behav Med. 2000;7:183–188. [DOI] [PubMed] [Google Scholar]
- 61. Wilson NV, Meyer BM. Early prediction of hypertension using exercise blood pressure. Prev Med. 1981;10:62–68. [DOI] [PubMed] [Google Scholar]
- 62. Wilson MF, Sung BH, Pincomb GA. Exaggerated response to exercise in men at risk for systemic hypertension. Am J Cardiol. 1990;66:731–736. [DOI] [PubMed] [Google Scholar]
- 63. Gobel FL, Nordstrom LA, Nelson RR, et al. The rate‐pressure product as an index of myocardial oxygen consumption during exercise in patients with angina pectoris. Circulation. 1978;57:549–556. [DOI] [PubMed] [Google Scholar]
- 64. Rakic V, Burke V, Beilin LJ. Effects of coffee on ambulatory blood pressure in older men and women: a randomized controlled trial. Hypertension. 1999;33:869–873. [DOI] [PubMed] [Google Scholar]
- 65. Lovallo WR, Al'Absi M, Blick K, et al. Stress‐like adrenocorticotropin responses to caffeine in young healthy men. Pharmacol Biochem Behav. 1996;55:365–369. [DOI] [PubMed] [Google Scholar]
- 66. Al'Absi M, Lovallo WR, McKey B, et al. Hypothalamic‐pituitary‐adrenocortical responses to psychological stress and caffeine in men at high risk for hypertension. Psychosom Med. 1998;60:521–527. [DOI] [PubMed] [Google Scholar]
- 67. Lovallo WR, Pincomb GA, Sung BH, et al. Caffeine may potentiate adrenocortical stress responses in hypertension‐prone men. Hypertension. 1989;14:170–176. [DOI] [PubMed] [Google Scholar]
- 68. Al'Absi M, Everson SA, Lovallo WR. Hypertension risk factors and cardiovascular reactivity to mental stress in young men. Int J Psychophysiol. 1995;20:155–160. [DOI] [PubMed] [Google Scholar]
- 69. Myers MG. Effects of caffeine on blood pressure. Arch Intern Med. 1988;148:1189–1193. [PubMed] [Google Scholar]
- 70. Paul S, Kurunwune B, Biaggioni I. Caffeine withdrawal: apparent heterologous sensitization to adenosine and prostacyclin actions in human platelets. J Pharmacol Exp Ther. 1993;267:838–843. [PubMed] [Google Scholar]
- 71. Lane JD. Effects of brief caffeine beverage deprivation on mood, symptoms, and psychomotor performance. Pharmacol Biochem Behav. 1997;58:203–208. [DOI] [PubMed] [Google Scholar]
- 72. Lane JD, Phillips‐Bute BG. Caffeine deprivation affects vigilance performance and mood. Physiol Behav. 1998;65:171–175. [DOI] [PubMed] [Google Scholar]
- 73. Silverman K, Evans SM, Strain EC, et al. Withdrawal syndrome after the double‐blind cessation of caffeine consumption. N Engl J Med. 1992;327:1109–1114. [DOI] [PubMed] [Google Scholar]
- 74. Evans SM, Griffiths RR. Caffeine withdrawal: a parametric analysis of caffeine dosing conditions. J Pharmacol Exp Ther. 1999;289:285–294. [PubMed] [Google Scholar]
- 75. Nehlig A. Are we dependent upon coffee and caffeine? A review on human and animal data. Neurosci Biobehav Rev. 1999;23:563–576. [DOI] [PubMed] [Google Scholar]
- 76. McCubbin JA, Wilson JF, Bruehl S, et al. Gender effects on blood pressures obtained during on‐campus screening. Psychosom Med. 1991;53:90–100. [DOI] [PubMed] [Google Scholar]
- 77. Sharp DS, Benowitz NL. Pharmacoepidemiology of the effect of caffeine on blood pressure. Clin Pharmacol Ther. 1990;47:57–60. [DOI] [PubMed] [Google Scholar]
- 78. Izzo JL Jr, Ghosal A, Kwong T, et al. Age and prior caffeine use alter the cardiovascular and adreno—medullary responses to oral caffeine. Am J Cardiol. 1983;52:769–773. [DOI] [PubMed] [Google Scholar]
- 79. Lane JD, Adcock RA, Williams RB, et al. Caffeine effects on cardiovascular and neuroendocrine responses to acute psychosocial stress and their relationship to level of habitual caffeine consumption. Psychosom Med. 1990;52:320–336. [DOI] [PubMed] [Google Scholar]
- 80. Ratliff‐Crain J, O'Keeffe MK, Baum A. Cardiovascular reactivity, mood, and task performance in deprived and non‐deprived coffee drinkers. Health Psychol. 1989;8:427–447. [DOI] [PubMed] [Google Scholar]
- 81. Lane JD, Kuhn CM, Williams RB. Habitual caffeine use does not reduce caffeine's potentiation of cardiovascular and neuroendocrine stress reactivity [abstract]. Psychophysiology. 1989;26:S41. [Google Scholar]
- 82. Lovallo WR, Al'Absi M, Pincomb GA, et al. Caffeine and behavioral stress effects on blood pressure in borderline hypertensive caucasian men. Health Psychol. 1996;15:11–17. [DOI] [PubMed] [Google Scholar]
- 83. Burr ML, Gallacher JE, Butland BK, et al. Coffee, blood pressure and plasma lipids: a randomized controlled trial. Eur J Clin Nutr. 1989;43:477–483. [PubMed] [Google Scholar]
- 84. Van Dusseldorp M, Smits P, Thien T, et al. Effect of decaffeinated versus regular coffee on blood pressure. A 12‐week double‐blind trial. Hypertension. 1989;14:563–569. [DOI] [PubMed] [Google Scholar]
- 85. Superko HR, Hyll J, DiRicco C, et al. Effects of cessation of caffeinated‐coffee consumption on ambulatory and resting blood pressure in men. Am J Cardiol. 1994;73:780–784. [DOI] [PubMed] [Google Scholar]
- 86. MacDonald TM, Sharpe K, Fowler G, et al. Caffeine restriction: effect on mild hypertension. BMJ. 1991;303:1235–1238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87. Denaro CP, Brown CR, Jacob P III, et al. Effects of caffeine with repeated dosing. Eur J Clin Pharmacol. 1991;40:273–278. [DOI] [PubMed] [Google Scholar]
- 88. Whelton PK. Epidemiology of hypertension. Lancet. 1994; 344:101–106. [DOI] [PubMed] [Google Scholar]
- 89. Strickland TL, Myers HF, Lahey BB. Cardiovascular reactivity with caffeine and stress in black and white normotensive females. Psychosom Med. 1989;51:381–389. [DOI] [PubMed] [Google Scholar]
- 90. Sharp DS, Benowitz NL, Osterloh JD, et al. Influence of race, tobacco use, and caffeine use on the relation between blood pressure and blood lead concentration. Am J Epidemiol. 1990;131:845–854. [DOI] [PubMed] [Google Scholar]
- 91. Frohlich ED. Hemodynamic differences between black patients and white patients with essential hypertension. Hypertension. 1990;15(6 pt 2):675–680. [DOI] [PubMed] [Google Scholar]
- 92. Mancia G, Sega R, Milesi C, et al. Blood‐pressure control in the hyptertensive population. Lancet. 1997;349:454–457. [DOI] [PubMed] [Google Scholar]
- 93. Smits P, Hoffmann H, Thien T, et al. Hemodynamic and humoral effects of coffee after β1‐selective and nonselective β‐blockade. Clin Pharmacol Ther. 1983;34:153–158. [DOI] [PubMed] [Google Scholar]
- 94. Van Nguyen P, Myers MG. Cardiovascular effects of caffeine and nifedipine. Clin Pharmacol Ther. 1988;44:315–319. [DOI] [PubMed] [Google Scholar]
- 95. Rakic V, Beilin LJ, Burke V. Effect of coffee and tea drinking on postprandial hypotension in older men and women. Clin Exp Pharmacol Physiol. 1996;23:559–563. [DOI] [PubMed] [Google Scholar]
- 96. Massengill JS, Hartley TR, Sung BH, et al. Caffeine's Effects on Blood Pressure in Middle Aged Persons. Paper presented at: Annual meeting of the Society of Behavioral Medicine, April, 2000. Nashville, TN. [Google Scholar]
- 97. Cohn JN, Levine TB, Olivari MT, et al. Plasma norepinephrine as a guide to prognosis in patients with chronic congestive heart failure. N Engl J Med. 1984;311:819–823. [DOI] [PubMed] [Google Scholar]
- 98. Paci A, Marrone O, Lenzi S, et al. Endogenous digitalis‐like factors in obstructive sleep apnea. Hypertens Res. 2000; 23(suppl):S87–S91. [DOI] [PubMed] [Google Scholar]
- 99. Hebel SK, ed. Drug Facts and Comparisons. St. Louis, MO: Facts and Comparisons, Wolters Kluwer Company; 2000. Available at: www.fandc.com/efactsintro.asp. Accessed October 15,2001. [Google Scholar]
- 100. Tatro DS, ed. Drug Interaction Facts. St. Louis, MO: Facts and Comparisons, Wolters Kluwer Company; 2000. Available at: www.fandc.com/efactsintro.asp. Accessed October 15,2000. [Google Scholar]