

Graphical abstract
Keywords: Importation risk, Entry restriction, Travel quarantine, Web-based tool, Epidemic simulation, Compartmental model
Abstract
Objective
As the potential spread of COVID-19 sparked by imported cases from overseas will pose continuous challenges, it is essential to estimate the effects of control measures on reducing the importation risk of COVID-19. Our objective is to provide a framework of methodology for quantifying the combined effects of entry restrictions and travel quarantine on managing the importation risk of COVID-19 and other pandemics by leveraging different sets of parameters.
Methods
Three major categories of control measures on controlling importation risk were parameterized and modelled by the framework: 1) entry restrictions, 2) travel quarantine, and 3) domestic containment measures. Integrating the parameterized intensity of control measures, a modified SEIR model was developed to simulate the case importation and local epidemic under different scenarios of global epidemic dynamics. A web-based tool was also provided to enable interactive visualization of epidemic simulation.
Results
The simulated number of case importation and local spread modelled by the proposed framework of methods fitted well to the historical epidemic curve of China and Singapore. Based on the simulation results, the total numbers of infected cases when reducing 30% of visitor arrivals would be 88·4 (IQR 87·5–89·6) and 58·8 (IQR 58·3–59·5) times more than those when reducing 99% of visitor arrivals in mainland China and Singapore respectively, assuming actual time-varying Rt and travel quarantine policy. If the number of global daily new infections reached 100,000, 85%–91% of inbound travels should be reduced to keep the daily new infected number below 100 for a country with a similar travel volume as Singapore (daily 52,000 tourist arrivals in 2019). Whereas if the number was lower than 10,000, the daily new infected case would be less than 100 even with no entry restrictions.
Discussions
We proposed a framework that first estimated the intensity of travel restrictions and local containment measures for countries since the first overseas imported case. Our approach then quantified the combined effects of entry restrictions and travel quarantine using a modified SEIR model to simulate the potential epidemic spread under hypothetical intensities of these control measures. We also developed a web-based system that enables interactive simulation, which could serve as a valuable tool for health system administrators to assess policy effects on managing the importation risk. By leveraging different sets of parameters, it could adapt to any specific country and specific type of epidemic.
Conclusions
This framework has provided a valuable tool to parameterize the intensity of control measures, simulate both the case importation and local epidemic, and quantify the combined effects of entry restrictions and travel quarantine on managing the importation risk.
1. Introduction
The Coronavirus disease 2019 (COVID-19) pandemic has posed a significant threat for public health worldwide. As of September 30, COVID-19 has swept to more than 200 countries and territories, reporting 33,785,178 confirmed cases and at least 1,010,147 deaths worldwide [1]. Since countries are in various pandemic phases, the potential spread sparked by imported cases from overseas will continue to pose new challenges for almost every country. In particular, as with the ease of travel restrictions in many countries, the mobility between them and countries with a high incidence of infection may cause successive waves of outbreak [2]. For example, in the early phase of the pandemic, countries such as Thailand, Japan, South Korea and Singapore, which received the highest number of passengers from China, were identified as high-risk countries for case importation [3].
Previous studies suggest that three major types of control measures are effective to contain the severe outbreaks caused by overseas importation: 1) entry restrictions to reduce the number of imported infectious cases, 2) travel quarantine to prevent the imported infectious cases from spreading the virus, and 3) domestic containment to slow down the spread of disease even if imported cases were not isolated [4], [5], [6]. Domestic containment measures, including city lockdown, social distancing, business and school close, etc., have been extensively studied [7], [8], [9], [10]. Several studies assessed the effect of reduced travel at the early stage of the outbreak and concluded that rigorous travel restrictions could delay the outbreak [11], [12], [13]. Other studies suggested that quarantine of inbound travellers is required for reducing the transmission of the virus [14], [2]. However, current studies examined the effects of the three major types of control measures separately, without characterizing the combined effects. In addition, the epidemic spread under different intensities of those control measures was also not investigated in previous studies. Moreover, an integrated framework to measure the combined effects of entry restrictions, quarantine policies and transmissibility of different pandemics, which can offer simulations for the spread of the pandemic under varying combinations of control measures, is lacking.
By implementing aggressive public health measures with rapid response, mainland China and Singapore have achieved promising progress in mitigating the first wave of outbreak [15], [16], [17]. China issued strict measures including city lockdown at the initial stage and international travel restrictions since March 19. The number of daily new confirmed cases was controlled under 100. Singapore was lauded as a success story in the first phase against the coronavirus with proactive measures. However, as the outbreak quickly spread around the world and turned into a global pandemic [18], the imported cases surged since March 5, and later, community outbreaks among migrant workers in local dormitories occurred. This second outbreak led to more proactive strategies such as strict entry restrictions issued by the Singapore government after April 4 [19], [20]. These two real-world cases enabled us to retrospectively evaluate the importance of control measures in preventing a successive outbreak.
In this paper, we proposed a novel framework of methodologies that simulates the potential development of the epidemic across different intensities of entry restrictions and quarantine, as well as under different assumptions of the global spread of pandemics. By leveraging different sets of parameters, we assessed the combined effects of control measures on mitigating the risk of COVID-19 importation, providing suggestions on what future control measures could be undertaken under different scenarios of pandemic status. The framework was verified on the subsequent epidemic spread of COVID-19 in mainland China and Singapore.
2. Materials and methods
2.1. Data collection
To illustrate the analytical framework, we collected retrospective data of COVID-19 in mainland China (excluding Hubei province) and Singapore. Daily numbers of local and imported COVID-19 cases in mainland China [21] from February 26 and Singapore [22] from March 5 to May 23, 2020 were collected to estimate the effective reproduction number Rt. Rt is the key measure of epidemic dynamic, defined as the average number of secondary cases caused by one newly infected case at time t. We also collected data of control measures implemented in mainland China and Singapore from the day when the first imported case was reported to May 23 and created a timeline of these policies by their effective dates.
To estimate the number of imported cases in mainland China and Singapore, we collected the data of daily reported cases worldwide from World Health Organization (WHO) [23] and the data of international visitor arrivals in 2019 of the world, mainland China and Singapore [24], [25], [26].
2.2. Integrated framework of methodology
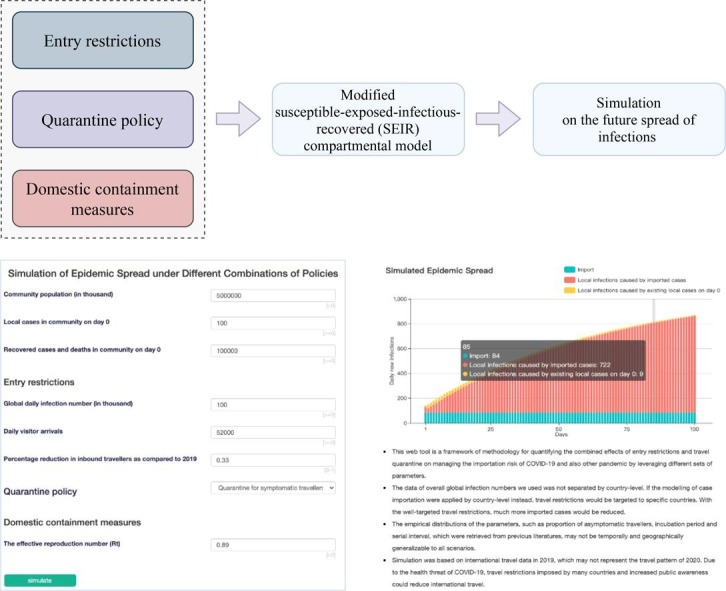
The integrated framework for modelling the combined effects of entry restrictions, travel quarantine and domestic containment measures on managing the importation risk was presented in Fig. 1 .
Fig. 1.

Integrated framework for modelling the combined effects of entry restrictions, travel quarantine and domestic containment measures on managing the importation risk of COVID-19 or other pandemics.
2.2.1. Parameterization of entry restrictions and modelling of case importation
The intensity of entry restrictions will impact the number of inbound travellers, as well as the number of imported cases. We defined “inbound traveller reduction” by the percentage of reduced inbound travellers as compared to the year of 2019. We first estimated the number of imported cases in mainland China and Singapore, assuming no entry restriction was in place, following a previously published approach for modelling case importation based on travel data [2]. The number of imported cases with no entry restriction implemented is assumed to be correlated with the number of global new infected cases, daily probability of travelling for an infected case , the probability of travelling to a certain country (termed as travel weight , which is estimated by the proportion of the total number of inbound travellers of country among the total number of inbound travellers worldwide in 2019). The daily probability of travelling for an infected case was estimated by constructing equations (1, 2, 3) of the expected daily number of imported cases and fitting the predicted number to real reported cases.
| (1) |
| (2) |
| (3) |
where is the expected number of imported cases after time for the subject who was infected on time , is the travel weight of country , is the time from symptom onset to the first medical visit for the subject . is the expected number of imported infected cases after time t for all subjects who were infected on time is the expected number of imported infected cases on time , is the first day of the study period, is the last day of the study period, is the number of infected cases on time .
Reported COVID-19 data of Singapore from March 5 to 13 was used for this estimation, as the travel to mainland China has reduced dramatically due to the early transmission of COVID-19, and no entry restrictions to countries out of China were implemented in Singapore during this period. We excluded new reported cases of Singapore as well as mainland China from the global new infected cases when estimating the daily probability of travelling, as Singapore barred all visitors with recent travel history to mainland China since February 2. We extrapolated the number of true infectious cases from the reported data by sampling from the empirical distribution of the time from symptom onset to reporting [7].
The inbound traveller reduction in mainland China and Singapore was then estimated by applying a dynamic policy weight in the likelihood function of the daily number of imported cases (Equation (4)) and fitting the simulated results to real numbers.
| (4) |
2.2.2. Travel quarantine
We assessed the impact of quarantine by assuming three different scenarios of quarantine policies and varying the input parameters of simulation models accordingly: 1) quarantine all inbound travellers, which has been implemented in mainland China since March 26; 2) quarantine the symptomatic travellers, which was adopted by Singapore since March 5; 3) no quarantine, as applied in most of the countries during the early stage of the epidemic. To simulate the effect of quarantining the symptomatic travellers, we used the proportion of pre-symptomatic cases () [2] and asymptomatic cases () [27] to estimate the potential number of imported cases in the incubation period and asymptomatic cases.
2.2.3. Domestic containment measures
Aggressive domestic containment measures can bring spread under control, and in this situation, Rt will be below 1. However, relaxed interventions may push Rt to rise above 1, and the epidemic spreads. Therefore, the change of Rt can help us understand the effectiveness of domestic containment measures and how these policies affect the spread of the virus. Stratifying the daily new cases into local cases and imported cases from overseas, we estimated time-varying Rt from February 26 to May 23 for mainland China (excluding Hubei province) and from March 5 to May 23 for Singapore, assuming the empirical serial interval [28] (the time period between clinical onset of primary case and onset of symptoms with the secondary case) to be distributed with a mean of 7·5 days and SD of 3·4 days and a reporting delay (the time period between clinical onset and being reported) to be distributed with a mean of 4·9 days and SD of 3·3 days [7], using the R package EpiEstim, version 2.2-1 [29], [30] on weekly time windows.
2.2.4. Simulation model for the epidemic spread under different control measures
Through parameterization of the intensities of the control measures, we were able to integrate them into the following modified susceptible-exposed-infectious-recovered (SEIR) compartmental model to simulate the effect of the above hypothetical control measures on the imported and local infection of COVID-19:
where , , and are the number of susceptible, exposed, infectious and removed cases at time t; is the incubation period, is the infectious period (equals the serial interval minus the mean incubation period); is the effective reproduction number; are the number of imported incubated cases, infectious cases with symptoms and asymptomatic cases at time t who are free of quarantine.
The parameters used in the SEIR model are from previously reported empirical distributions (Table 1 ). Daily value of are estimated from the previous steps.
Table 1.
Distribution of parameters used for simulation.
| Parameters | Value | Distribution | Reference |
|---|---|---|---|
| Proportion of pre-symptomatic travellers, | 0·643 | Beta distribution α = 89·06932, β = 49·45217 |
Empirical distribution [2] |
| Proportion of asymptomatic travellers, | 0·31 | Beta distribution α = 51, β = 115 |
Empirical distribution [27] |
| Travel probability, | 0·0209 | Beta distribution 95% CI: 0·0084-0·0279 |
Estimated by MCMC and bootstrapping |
| Incubation period, | 5·2 | Discrete log-normal (truncated 21 days) Mean: 5·2 SD: 3·91 |
Empirical distribution [2] |
| Serial interval, | 7·5 | Negative binomial distributionMean: 7·5 SD: 3·4 | Empirical distribution [2] |
Through this framework, we input different combinations of , the inbound traveller reduction and quarantine policies and simulate the subsequent epidemic spread of COVID-19. We took mainland China and Singapore as examples to assess the combined effects of control measures with our framework. Based on the estimated time-varying Rt, inbound traveller reduction and quarantine policy, we simulated the daily newly infected cases in mainland China and Singapore. The underreporting cases were adjusted using a recently-developed capture-recapture method, which is a lower bound estimator for the size of partially unobserved populations [31]. A web-based visualization tool (http://101.89.95.81:8260/pic.html) of epidemic spread simulation was developed from this framework, allowing others to obtain simulations easily by varying input parameters based on their situation.
2.2.5. Modelling the uncertainty of parameters
Based on the distributions of parameters in the SEIR model (Table 1), we estimated the cumulative infected cases for mainland China and Singapore under different scenarios using Markov Chain Monte Carlo simulations. For each scenario, we repeated the simulation 1,000 times and reported the confidence intervals of the estimated results. All simulations were performed using R version 3.6.1 (R Foundation for Statistical Computing; Vienna, Austria). The data and code are available at https://github.com/jinyizhu/Importation-Risk-of-COVID-19.
3. Results
3.1. Estimating the intensity of control measures and fitting to the historical epidemic curve
We first estimated the actual dynamic inbound traveller reduction in mainland China and Singapore (Fig. 2 A and D). The average intensity since the first imported case was 0·94 in mainland China and 0·86 in Singapore, where approaching 1 indicates the strongest degree of restriction. Based on the estimated inbound traveller reduction, we hypothesized three scenarios for mainland China: 1) 0·31 (corresponding to the scenario with almost no restrictions), 2) 0·85 (corresponding to the average intensity from Jan 26 to March 18, the day before mainland China issued a notice on controlling international flights) and 3) 0·99 (corresponding to the average inbound traveller reduction from Apr 8, when mainland China temporarily closed the land border with Russia, to May 23). The three scenarios for Singapore included: 1) 0·31 (March 5 to March 12, the day before new visitors from Italy, France, Germany and Spain were not allowed entry into Singapore), 2) 0·55 (from March 13 to March 22, the day before all short-term visitors were prohibited from entering or transition through Singapore) and 3) 0·99 (average intensity from March 23 to May 23).
Fig. 2.

Estimation of effective reproduction number Rt, inbound traveller reduction and the actual quarantine policy in mainland China (A, B, C) and Singapore (D, E, F). Rt was presented on sliding weekly windows. Inbound traveller reduction refers to the percentage reduction in inbound travellers as compared to 2019.
We also presented the timeline of actual travel quarantine policies in Fig. 2B and E. For mainland China, no quarantine was required until March 12, when quarantine for symptomatic travellers started, and since March 26, quarantine was required for all inbound travellers. For Singapore, quarantine for symptomatic travellers was required from March 5 to April 9, then mandatory quarantine for all inbound travellers started.
By fitting the daily number of local cases and imported cases from overseas, we estimated the time-varying effective reproduction number (Rt) in mainland China and Singapore (Fig. 2C and F). The average Rt since the first imported case was 0·17 in mainland China and 1·4 in Singapore.
Based on the estimated parameters of intensity of control measures, we retrospectively simulated the epidemic curve by calculating the daily new infected cases in mainland China and Singapore using the modified SEIR model. The simulated results fitted closely to the real numbers (Fig. 3 ), suggesting good validation of the analytical framework.
Fig. 3.

The real and simulated numbers of confirmed cases and timeline of control measures in (A) mainland China (excluding Hubei province) and (B) Singapore. The black dotted line represents the simulated number of newly infected cases based on estimated time-varying Rt, inbound traveller reduction and quarantine policy after adjusting a time lag between infection and reporting. The yellow and blue bars represent daily new confirmed local and imported cases, respectively. (For interpretation of the references to colour in this figure legend, the reader is referred to the web version of this article.)
3.2. Effects of entry restrictions and quarantine policy
For the retrospective evaluation of the effects of control measures, we conducted simulations to assess the potential effects of different inbound traveller reduction and quarantine policies. Based on the estimated inbound traveller reduction in mainland China and Singapore, we hypothesized three scenarios of intensity for mainland China and Singapore respectively under the estimated time-varying Rt and actual quarantine policy. To compare the effects of quarantine policies, we assumed three different scenarios of quarantine policies (quarantine all inbound travellers, quarantine symptomatic travellers, and no quarantine required) with the estimated time-varying Rt and actual inbound traveller reduction.
Fig. 4 shows the entry restrictions and quarantine policy simulations for mainland China and Singapore. For mainland China (Fig. 4A), under the actual Rt and inbound traveller reduction, the total number of simulated imported cases was 1840, and the number of local cases (excluding Hubei province) did not change a lot across different quarantine policies. When quarantine for all inbound travellers was applied, there would be no local cases. If the policy was to quarantine symptomatic travellers, the local case count would be 1833. No quarantine would result in a local case count of 1932, which was similar to the result of quarantine for symptomatic travellers. Assuming actual Rt and quarantine policy (no quarantine until March 12 when quarantine for symptomatic travellers started and quarantined all inbound travellers after March 26) applied, due to a low time-varying Rt, the change of total case count was mainly caused by imported cases under different inbound traveller reduction. The imported and local case count would be 362 and 16, respectively, with the strict entry restrictions; 6979 and 306 when under the moderate level of entry restrictions; 31,998 and 1397 when the most relaxed entry restrictions applied. By applying the capture-recapture method that adjusted for underreporting, the cumulative local cases over the period increased by 889, 1803, 1853, 163, 3638 and 16,828 in the above six scenarios, respectively.
Fig. 4.

Simulation of the disease infection under combinations of control measures for (A) mainland China and (B) Singapore.
Simulation in Singapore (Fig. 4B) with a relatively high time-varying Rt showed a different pattern. Under the actual Rt and inbound traveller reduction, the total count of simulated imported cases was 571, and the local case number varied significantly with different quarantine policies. If the policy was quarantine for all inbound travellers, symptomatic travellers and no quarantine required, the local case count would be none, 66,819 and 87,299, respectively. When actual Rt and quarantine policy (quarantined symptomatic travellers from March 5 to April 9 when quarantine for all inbound travellers started) were applied, the change in cumulative case count was the combined effect of different inbound traveller reduction and high time-varying Rt. The imported and local case count would be 49 and 1960 with the strict entry restrictions; 2614 and 73,484 with the moderate entry restrictions; 4112 and 113,938 with the most relaxed entry restrictions applied. By applying the capture-recapture method, the cumulative local cases over the period increased by 273, 34089, 44461, 988, 38,499 and 59,742 in the above six scenarios, respectively.
Simulation results after adjusting for parameter uncertainty are presented in Table 2 . Assuming actual Rt and quarantine policy, if the most relaxed entry restriction was implemented, the total number of infected cases in mainland China and Singapore would be 88·4 (IQR 87·5-89·6) and 58·8 (IQR 58·3-59·5) times the number with the strict entry restrictions applied, respectively. The simulation results after adjusting for parameter uncertainty (Table 2) indicate that the estimated effects of the control measures are stable over distributions of parameters.
Table 2.
Simulated cumulative cases under combinations of control measures using Markov chain Monte Carlo (MCMC) simulation.
| Control measures | Mainland China | Singapore |
|---|---|---|
| Real number of cumulative cases | 1963 | 30,958 |
| imported | 1713 | 538 |
| local | 250 | 30,420 |
| Actual Rt and inbound traveller reduction | ||
| Quarantine for all travellers | 1840 (1572–2069) | 571 (569–574) |
| Quarantine for symptomatic travellers | 3673 (3479–3829) | 67,391 (51401–83380) |
| No Quarantine | 3773 (3577–3978) | 87,870 (68038–107702) |
| Actual Rt and quarantine policy | ||
| Strict entry restrictions | 378 (330–426) | 2008 (1555–2462) |
| Moderate intensity of entry restrictions | 7285 (6410–8127) | 76,098 (57123–95073) |
| Relaxed entry restrictions | 33,395 (29580–37247) | 118,051 (92504–143597) |
*Data are median (IQR).
3.3. Epidemic simulation under hypothetical global infection
We also simulated the epidemic spread given different global infection numbers to present potential effects of control measures on reducing importation risk under different future scenarios, taking Singapore as an example.
Given global daily new infection number of 10 thousand, 50 thousand and 100 thousand, we estimated the daily number of local infection and imported infection in Singapore under different inbound traveller reduction, while Rt remained to be 0·89 (average Rt of Singapore since April 28, 10 days after the mandatory Stay-Home Notice was issued for work permits) and all symptomatic travellers are quarantined (as shown in Fig. 5 ). We also adjusted for parameter uncertainty of Rt by sampling from its empirical distribution and conducted a Markov Chain Monte Carlo simulation. As presented in Table 3 , given a global daily new infection of 100 thousand, 88% (IQR 85%–91%) of inbound travels should be reduced to keep the daily new infection number below 100; given a global daily new infection of 50 thousand, 76% (IQR 69%-82%) of inbound travels should be reduced to keep the daily new infection number below 100; given a global daily new infection of 10 thousand, the average daily newly infected case would always be less than 100 even if no entry restriction is implemented.
Fig. 5.

Simulation of the effect of different inbound traveller reduction in Singapore under hypothetical global daily new infection number of 10 thousand (top row), 50 thousand (middle row) and 100 thousand (bottom row). In the simulation analysis, Rt remained to be 0·89 (average Rt of Singapore since April 28, 10 days after the mandatory Stay-Home Notice was issued for work permits) and all symptomatic travellers are quarantined.
Table 3.
Simulated number of cumulative cases under hypothetical global infection numbers and different inbound traveller reduction.
| Inbound traveller reduction (%) | Global daily infection |
||
|---|---|---|---|
| 10,000 | 50,000 | 100,000 | |
| 0 | 6184 (8271–11713) | 32,468 (41413–56543) | 65,266 (83828–114715) |
| 10 | 5557 (7435–10533) | 29,218 (37276–50913) | 58,758 (75496–103376) |
| 20 | 4929 (6599–9354) | 25,967 (33136–45275) | 52,243 (67151–92005) |
| 30 | 4301 (5762–8173) | 22,714 (28993–39630) | 45,723 (58792–80603) |
| 40 | 3674 (4926–6993) | 19,459 (24847–33977) | 39,196 (50419–69169) |
| 50 | 3047 (4090–5813) | 16,203 (20697–28316) | 32,662 (42033–57704) |
| 60 | 2420 (3254–4632) | 12,946 (16544–22648) | 26,123 (33634–46207) |
| 70 | 1794 (2419–3452) | 9687 (12388–16972) | 19,576 (25221–34678) |
| 80 | 1171 (1586–2273) | 6427 (8229–11289) | 13,024 (16794–23117) |
| 90 | 553 (758–1099) | 3168 (4069–5600) | 6467 (8354–11524) |
*Data are median (IQR).
To enable interactive visualization of the simulation results using our proposed framework, we also provided a web-based visualization tool, which can be accessed through http://101.89.95.81:8260/pic.html. It allows users to obtain simulation results easily by varying input parameters based on their situation. The above analysis could also be replicated by using this online tool.
As shown in Appendix, users are able to input travel data and transmission data, select one of the quarantine policies and enter the corresponding reproduction number to generate the simulation result of epidemic spread. Different diseases can be determined through adjusting the time-varying reproduction number, and different countries and territories can be identified by inputting the current transmission situation and relative travel information. The data visualization module will display simulation results for imported cases and local infections caused by imported cases and by existing local cases under the settings made by users. The importation risk and subsequent epidemic spread for any epidemic disease in any chosen area will be perspicuously illustrated on the page.
4. Discussion
As the COVID-19 pandemic has become a crisis all around the world, it is possible that the pandemic will last for a long time, and the risk of successive outbreaks caused by overseas importation remains high. Management and control of the case importation through leveraging entry restrictions and quarantine policies are therefore crucial. However, an established framework to measure the effects of entry restrictions and quarantine policies, which can offer simulations for the spread of the pandemic under varying combinations of control measures, is lacking. As concerns over the COVID-19 pandemic and even other unknown infectious diseases are still growing, health system administrators should attach importance to importation risks for disease control.
We constructed this novel framework considering the intensity of entry restrictions, quarantine policies, local and global transmissibility of different pandemics. A web-based tool developed from the proposed framework of simulating epidemic spread under hypothetical intensities of such strategies can help visualize the impacts on reducing importation risks, thus serving as informative evidence for policy making.
The simulation of our framework was supported by the real situation of COVID-19 spread in mainland China and Singapore, where we conducted a thorough investigation for the COVID-19 outbreak and the undertaken control measures. Since the first case was detected, containment measures, including locking down the cities, quarantining infected individuals, and social distancing, have been gradually implemented before the Spring Festival in China. Because of the control measures, the Rt in mainland China remained far below 1 (around 0·1) since February 26, and the number of daily new confirmed cases was reduced. However, because of the global outbreak of COVID-19, China reported the first imported case on February 26. The number of imported cases rose sharply ever since, and the Rt increased slightly in the middle of March. Consequently, China implemented a series of entry restrictions and centralized quarantine policies on travellers from overseas since March 15 [32]. As a result, the Rt fell back by the end of March, and the estimated inbound traveller reduction started to rise gradually from 0·75. Then in early April, most of the land border crossings were also closed. Simultaneously, our estimation of the intensity of inbound traveller reduction was reaching close to 1.
The epidemic in Singapore has a different trajectory than in China. There were primarily imported cases from mainland China first, and the cumulative number of cases remained under 100 by the end of February. However, the number of imported cases and community infection cases surged quickly in Singapore after March 5, because of the rapid development of the global epidemic. To prevent imported cases, Singapore implemented entry restrictions to ban all short-term visitors from March 23, and our estimation of the intensity of entry restrictions has increased to 1 since then. Even though Singapore carried out entry restrictions, the local community infection cases began to surge among the migrant worker population after April 3, and the Rt rose steeply over 3 bringing its total to 8014 cases in a population of nearly six million people on April 20. After seeing the second wave, Singapore implemented the ‘circuit breaker’ measures on April 7, including closing schools and non-essential workplaces, social distancing and locking down foreign worker dorms [33], resulting in a drop back of Rt.
Not surprisingly, the simulation results show that a combination of successful domestic containment measures, entry restrictions and individual quarantine policy has the most effective impact on reducing the number of imported and local cases and averting the second local outbreak. Our results also show that when the domestic effective reproduction number Rt is low (as in mainland China), a relaxed quarantine policy does not have a great impact, and relaxed entry restrictions may cause a moderate increase in the number of imported cases. When Rt is relatively high, relaxed entry restrictions or quarantine policies could dramatically increase the number of total infected cases, especially those caused by local transmission. According to our analysis, until the daily global infection drops below ten thousand, it is necessary to implement control measures on reducing inbound travels to keep daily new infected cases below 100 for a country with similar travel volumes as Singapore.
Finally, findings generated by our framework provide reusable methodologies for health system administrators to assess the effects of policy on the spread of infectious disease. Our framework, which can be used to estimate the impact of entry restrictions and quarantine policies to better understand the epidemic spread of different pandemics, is supplementary to the current approach of epidemic studies and will contribute to disease control and public health.
4.1. Limitation
Several limitations of our study should be noted. First of all, in the estimation of imported cases, we used data of overall global infection numbers rather than separated the calculation by country-level, for the purpose of simplifying the hypothetical scenarios, so that we were able to present potential effects of control measures on reducing importation risk under different dynamics of the global epidemic. If the modelling of case importation were applied by country-level in the future research based on our study, travel restrictions could be targeted to specific countries and the percentage of imported cases reduced would be much more than the percentage of travellers reduced by the well-targeted travel restrictions. Second, we conducted a Markov Chain Monte Carlo simulation by sampling from empirical distributions of these parameters to adjust for parameter uncertainty, yet the distributions of the parameters which were retrieved from previous literature may not be temporally and geographically generalizable to all scenarios. Third, our simulation was based on international travel data in 2019, which may not represent the travel pattern of 2020. Due to the health threat of COVID-19, travel restrictions imposed by many countries and increased public awareness could reduce international travel.
5. Conclusions
Our research has provided a framework to parameterize the intensity of control measures, simulate both the case importation and local epidemic, and quantify the combined effects of entry restrictions and travel quarantine on managing the importation risk. This framework of methodologies is reusable to quantify the impact of policy on the epidemic spread of COVID-19 and other infectious diseases.
CRediT authorship contribution statement
Tiange Chen: Conceptualization, Methodology, Data curation, Software, Formal analysis, Writing - original draft. Siwan Huang: Conceptualization, Methodology, Data curation, Software, Formal analysis, Writing - original draft. Guanqiao Li: Conceptualization, Methodology, Data curation, Formal analysis, Writing - original draft. Yuan Zhang: Data curation, Visualization, Writing - original draft. Ye Li: Data curation, Writing - original draft. Jinyi Zhu: Writing - review & editing. Xuanling Shi: Conceptualization, Methodology, Supervision, Writing - review & editing. Xiang Li: Conceptualization, Methodology, Supervision, Writing - review & editing. Guotong Xie: Conceptualization, Methodology, Supervision, Writing - review & editing. Linqi Zhang: Conceptualization, Methodology, Supervision, Writing - review & editing.
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Footnotes
Supplementary data to this article can be found online at https://doi.org/10.1016/j.jbi.2021.103800.
Appendix A. Supplementary material
The following are the Supplementary data to this article:
References
- 1.WHO. Coronavirus Disease (COVID-19) Dashboard. https://covid19.who.int/?gclid=CjwKCAjwtqj2BRBYEiwAqfzurx7uyKiD1EnoqsDrJ6RFFDbVK5PPcghY18uFoGn4chuRPGisF9d94RoCtCAQAvD_BwE (accessed May 23 2020).
- 2.Wells C.R., Sah P., Moghadas S.M., et al. Impact of international travel and border control measures on the global spread of the novel 2019 coronavirus outbreak. Proc Natl Acad Sci U S A. 2020;117(13):7504–7509. doi: 10.1073/pnas.2002616117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bogoch I.I., Watts A., Thomas-Bachli A., Huber C., Kraemer M.U.G., Khan K. Potential for global spread of a novel coronavirus from China. J Travel Med. 2020;27(2) doi: 10.1093/jtm/taaa011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Chinazzi M., Davis J.T., Ajelli M., et al. The effect of travel restrictions on the spread of the 2019 novel coronavirus (COVID-19) outbreak. Science. 2020;368(6489):395–400. doi: 10.1126/science.aba9757. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.N. Ferguson, D. Laydon, G. Nedjati Gilani, et al., Report 9: Impact of non-pharmaceutical interventions (NPIs) to reduce COVID19 mortality and healthcare demand, 2020. [DOI] [PMC free article] [PubMed]
- 6.Nussbaumer-Streit B., Mayr V., Dobrescu A.I., et al. Quarantine alone or in combination with other public health measures to control COVID-19: a rapid review. Cochrane Database Syst. Rev. 2020;4 doi: 10.1002/14651858.CD013574. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Leung K., Wu J.T., Liu D., Leung G.M. First-wave COVID-19 transmissibility and severity in China outside Hubei after control measures, and second-wave scenario planning: a modelling impact assessment. Lancet. 2020 doi: 10.1016/S0140-6736(20)30746-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Maier B.F., Brockmann D. Effective containment explains subexponential growth in recent confirmed COVID-19 cases in China. Science. 2020;368(6492):742–746. doi: 10.1126/science.abb4557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Cowling B.J., Ali S.T., Ng T.W., et al. Impact assessment of non-pharmaceutical interventions against coronavirus disease 2019 and influenza in Hong Kong: an observational study. Lancet Public Health. 2020 doi: 10.1016/S2468-2667(20)30090-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Islam N., Sharp S.J., Chowell G., et al. Physical distancing interventions and incidence of coronavirus disease 2019: natural experiment in 149 countries. BMJ. 2020;370 doi: 10.1136/bmj.m2743. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Linka K., Peirlinck M., Sahli Costabal F., Kuhl E. Outbreak dynamics of COVID-19 in Europe and the effect of travel restrictions. Comput. Methods Biomech. Biomed. Eng. 2020:1–8. doi: 10.1080/10255842.2020.1759560. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Anzai A., Kobayashi T., Linton N.M., et al. Assessing the impact of reduced travel on exportation dynamics of novel coronavirus infection (COVID-19) J. Clin. Med. 2020;9(2):601. doi: 10.3390/jcm9020601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Lai S., Ruktanonchai N.W., Zhou L., et al. Effect of non-pharmaceutical interventions to contain COVID-19 in China. Nature. 2020 doi: 10.1038/s41586-020-2293-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Peak C.M., Kahn R., Grad Y.H., et al. Individual quarantine versus active monitoring of contacts for the mitigation of COVID-19: a modelling study. Lancet Infect. Dis. 2020 doi: 10.1016/S1473-3099(20)30361-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Zhang J., Litvinova M., Wang W., et al. Evolving epidemiology and transmission dynamics of coronavirus disease 2019 outside Hubei province, China: a descriptive and modelling study. Lancet. Infect. Dis. 2020 doi: 10.1016/S1473-3099(20)30230-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Koo J.R., Cook A.R., Park M., et al. Interventions to mitigate early spread of SARS-CoV-2 in Singapore: a modelling study. Lancet. Infect. Dis. 2020 doi: 10.1016/S1473-3099(20)30162-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Peck K.R. Early diagnosis and rapid isolation: response to COVID-19 outbreak in Korea. Clin. Microbiol. Infect. 2020 doi: 10.1016/j.cmi.2020.04.025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Soo R.J., Chiew C.J., Ma S., Pung R., Lee V. Decreased Influenza Incidence under COVID-19 Control Measures Singapore. Emerging Infect. Dis. 2020;26(8) doi: 10.3201/eid2608.201229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.https://www.gov.sg/article/covid-19-cases-in-singapore (accessed May 26 2020).
- 20.Cattani M. Global coalition to accelerate COVID-19 clinical research in resource-limited settings. Lancet. 2020 doi: 10.1016/S0140-6736(20)30798-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.China NHCotPsRo. Outbreak Report. http://www.nhc.gov. cn/xcs/yqtb/list_gzbd.shtml. (accessed May 23 2020).
- 22.Singapore MoH. Situation Report. https://www.moh.gov.sg/covid-19/situation-report (accessed May 23 2020).
- 23.Organization WH. Situation Report. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed May 23 2020).
- 24.Organization UNWT. International Tourism and COVID-19. https://www.unwto.org/international-tourism-and-covid-19 (accessed May 23 2020).
- 25.China MoCaTotPsRo. Tourism statistics in 2019. https://www.mct.gov.cn/whzx/whyw/202003/t20200310_851786.html (in Chinese) (accessed May 23 2020).
- 26.Board ST. Tourism Statistics: Monthly Visitor Arrivals. https://stan.stb.gov.sg/portal/tourism-statistics.html (accessed May 23 2020).
- 27.Quilty B.J., Clifford S., Hellewell J., et al. Quarantine and testing strategies in contact tracing for SARS-CoV-2: a modelling study. Lancet. Public Health. 2021 doi: 10.1016/S2468-2667(20)30308-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Li Q., Guan X., Wu P., et al. Early transmission dynamics in Wuhan, China, of novel coronavirus–infected pneumonia. N. Engl. J. Med. 2020 doi: 10.1056/NEJMoa2001316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Cori A., Ferguson N.M., Fraser C., Cauchemez S. A new framework and software to estimate time-varying reproduction numbers during epidemics. Am. J. Epidemiol. 2013;178(9):1505–1512. doi: 10.1093/aje/kwt133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Thompson R., Stockwin J., van Gaalen R., et al. Improved inference of time-varying reproduction numbers during infectious disease outbreaks. Epidemics. 2019;29 doi: 10.1016/j.epidem.2019.100356. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Bohning D., Rocchetti I., Maruotti A., Holling H. Estimating the undetected infections in the Covid-19 outbreak by harnessing capture-recapture methods. Int J Infect Dis. 2020;97:197–201. doi: 10.1016/j.ijid.2020.06.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.International travellers to Beijing to pay for 14 days of coronavirus quarantine. https://www.scmp.com/news/china/society/article/3075288/international-travellers-beijing-pay-14-days-coronavirus.
- 33.Coronavirus: Singapore reports 120 new cases, locks down two foreign worker dorms. https://www.scmp.com/week-asia/health-environment/article/3078515/coronavirus-singapore-reports-120-new-cases-locks-down (accessed May 11 2020).
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.