

Abstract
The concept that preeclampsia is a multisystemic syndrome is appreciated in both research and clinical care. Our understanding of pathophysiology recognizes the role of inflammation, oxidative and endoplasm reticulum stress and angiogenic dysfunction. Yet we have not progressed greatly towards clinically useful prediction nor had substantial success in prevention or treatment. One possibility is that the maternal syndrome may be reached through different pathophysiological pathways, i.e. subtypes of preeclampsia, that in their specificity yield more clinical utility. For example, early and late onset preeclampsia are increasingly acknowledged as different pathophysiological processes leading to a common presentation. Other subtypes of preeclampsia are supported by disparate clinical outcomes, long range prognosis, organ systems involved, and risk factors. These insights have been supplemented by discovery-driven methods, which cluster preeclampsia cases into groups indicating different pathophysiologies. In this presentation we review likely subtypes based on current knowledge and suggest others. We present a consideration of the requirements for a clinically meaningful preeclampsia subtype. A useful subtype should (1) identify a specific pathophysiological pathway or (2) specifically indicate maternal or fetal outcome, (3) be recognizable in a clinically useful time frame and (4) these results should be reproducible and generalizable (but at varying frequency) including in low resource settings. We recommend that the default consideration be that preeclampsia includes several subtypes rather than trying to force all cases into a single pathophysiological pathway. The recognition of subtypes and deciphering their different pathophysiologies will provide specific targets for prevention, prediction and treatment directing personalized care.
Keywords: preeclampsia, syndrome, discovery science, heterogeneity, subtypes, epidemiology, prediction
Introduction
In the past 30 years there has been an explosion in our knowledge of the pathophysiology of preeclampsia. Having abandoned the approach to understanding preeclampsia based on the concept of the disorder as “Pregnancy Induced Hypertension”, preeclampsia is now recognized as a syndrome encompassing far more than simply hypertension and proteinuria. The role of oxidative and endoplasmic reticulum stress, inflammation and secondary endothelial dysfunction and the importance of angiogenic and anti-angiogenic factors have all informed our understanding of the pathophysiology of preeclampsia.1 However, despite this, our ability to prevent and predict the disorder in an actionable timely manner have not achieved a satisfactory level of success. An explanation that is receiving increasing attention is the possibility that there is more than one subtype of preeclampsia, with a variety of pathophysiological pathways leading to maternal and fetal mortality and morbidity.2 (Figure 1)
Figure 1: Multiple Pathophysiological Pathways.
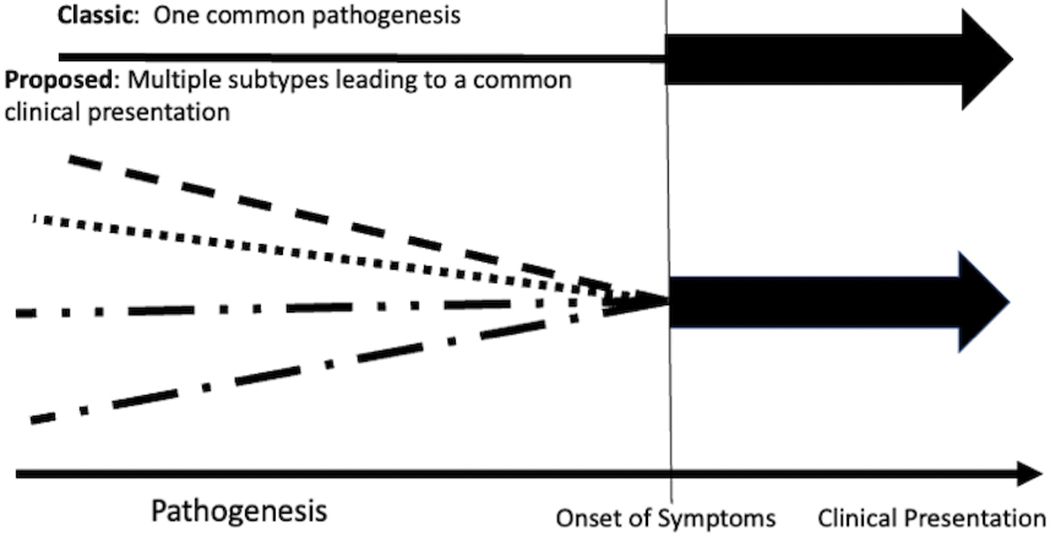
The classic pathway to preeclampsia is considered as a unified pathophysiological pathway resulting in the preeclampsia syndrome. In this presentation we propose that several pathways can result in the common clinical presentation of preeclampsia.
In this presentation we will: 1. consider evidence supporting subtypes, 2. examine impediments to the recognition of subtypes, 3. address the implications of identifying subtypes, 4. review currently postulated subtypes 5. consider how to identify other potential subtypes and 6. present strategies to recognize and test the clinical relevance of subtypes.
Evidence for subtypes of preeclampsia
Several lines of evidence support the consideration that preeclampsia may not be one disorder. One obvious finding supporting this concept is the diversity of the clinical presentation. The syndrome of new onset gestational hypertension and proteinuria or other systemic findings that we term preeclampsia includes women with an indolent disorder changing minimally with progression of pregnancy and women with an “explosive” clinical presentation who on one day exhibit minimal diagnostic findings and the next are critically ill. Although the concepts guiding our understanding of pathophysiology espouse reduced placental perfusion, only about one third of infants of women with preeclampsia manifest fetal growth restriction. Further, the principal organs involved in preeclampsia vary between women, particularly in those having principally hepatic involvement with the HELLP (Hemolysis, Elevated Liver Enzymes, Low Platelets) variant. The laboratory findings associated with preeclampsia, whether clinically or in research studies, vary remarkably.2 This includes the scatter of measurements of findings proposed as causally relevant to the disorder including oxidative stress and angiogenic and antiangiogenic factors. (Figure 2).
Figure 2: PlGF measured longitudinally across pregnancy.
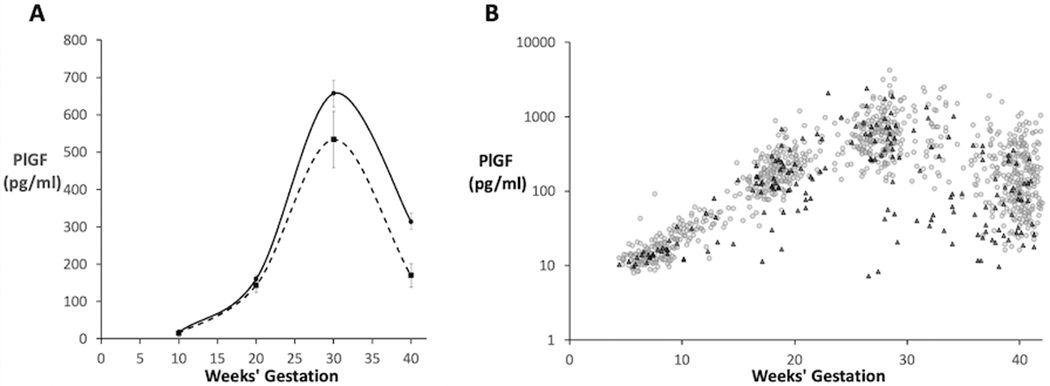
PlGF was measured in 50 women who developed preeclampsia and 300 who did not. The data are arrayed in Panel A as mean and standard error of the mean (square and dashed line preeclampsia, circle and solid line control). In Panel B the same data are arrayed as a scatter plot, (preeclampsia black triangle, control gray circle) clearly indicating the heterogeneity of the data that is not evident in Panel A.
Long-term implications of preeclampsia for maternal health also vary, suggesting that different subtypes of preeclampsia may presage different chronic disease risk trajectories after pregnancy. For example, preeclampsia is associated with a doubling of maternal cardiovascular risk in later life.3 However, it would be inaccurate to consider preeclampsia as a homogenous exposure: while preeclampsia at term in the absence of SGA confers a 2-fold increased risk of maternal cardiovascular disease, term preeclampsia with SGA confers over 3-fold risk, and preterm preeclampsia over 5-fold risk of future cardiovascular disease.4 If preeclampsia occurs before 34 weeks that risk may be as high as 10 fold.5
Attempts to prevent preeclampsia share a common evolution. Small early studies are successful6 but subsequent larger studies are not.7,8 One obvious explanation is publication bias with the only small studies considered for publication being those that are successful. An alternative consideration is that small studies are from homogeneous populations while larger, characteristically multicenter studies, are much more heterogeneous in relation to ethnicity, socioeconomic status, age, environmental and other influences. In a disorder with several pathophysiological pathways, a therapy is most likely to be successful if the pathophysiology at which it is directed is present in a homogeneous population. Support for this comes from NIH studies of aspirin (ASA) to prevent preeclampsia in low and high risk women.9,10 Although these multicenter center studies did not support a preventive effect of ASA when data from all centers were combined, in two of the centers ASA was effective in both studies. The effect of ASA at these two centers could have been masked by failure in other centers with subjects that did not share a pathophysiology countered by aspirin therapy.
Impediments to the recognition of subtypes
Despite this substantial variability, the concept of the preeclampsia syndrome as one disorder with a common pathophysiology persists. Part of this is due to the “Occam’s Razor” approach to understanding disease pathophysiology. This concept suggests that the simplest, least complex, explanation for a disease most likely pertains. One can argue that in this age of personalized medicine this may or may not be pertinent for complex diseases, but this most certainly is unlikely for a syndrome such as preeclampsia. The convention that gestational proteinuria and hypertension were diagnostic of preeclampsia was not based on the importance of these findings in the pathophysiology of disorder. Rather they were serendipitous observations in the late nineteenth century of clinical findings which preceded the seizures of eclampsia.11 All of these attitudes led to a thought process that sought to squeeze all of these diversities into a single disorder, ignoring obvious exceptions. This was supported by the use of data presentation which tended to mask variability. Recently, Weissgerber and her colleagues have emphasized that the most common approach to present continuous data in figures as bars with standard deviation or even more so with standard error is very effective at masking variability.12 This has led to the plea, especially pertinent in a syndrome such as preeclampsia, to present data in a manner that reveals, rather than hides, outliers.12 The same objection applies to other data arrays and presentation that do not provide an indicator of variability.(Figure 2)
The importance of subtypes
We will present several suggestions to begin to consider as different kinds of preeclampsia. The search for subtypes within a disease can be classified along a variety of dimensions. These dimensions could include classic epidemiologic variables such as the timing of onset, disease severity, anatomic or pathophysiologic differences in affected organ systems, just to suggest several categories.13 However, the important fact is that these may point us to relevant differences in the pathophysiologic pathways to maternal and infant morbidity and mortality, acute and long term. In other medical disorders this has become the rule. For example, how successful would diabetes therapy be if we did not recognize the existence of different pathological pathways in Type 1 and Type 2 diabetes? In this presentation we present findings to begin to mine potential subtypes for such clinically relevant pathways. The importance of identifying these potential pathophysiological subtypes cannot be overemphasized. The existence of several subtypes of preeclampsia makes it unlikely that one diagnostic or one preventive therapy will be effective. However, the recognition of subtypes and deciphering their different pathophysiologies will provide specific targets for diagnosis and prevention directing personalized care and management.
Currently Suspected Subtypes of Preeclampsia
Several subtypes of preeclampsia have been proposed. We will consider these suspected subtypes as early targets for testing the hypothesis of preeclampsia variants and present information demonstrating the challenges associated with discriminating subtypes.
Early and late onset preeclampsia and severe and mild preeclampsia
Historically, in clinical practice, preeclampsia has been defined as early (<34 weeks’ gestation) or late onset (>34 weeks) (despite the label suggesting onset these would be better described as early and late delivery, since onset is rarely known) or as mild or severe (based on blood pressure, clinical findings and degree of proteinuria). Although severe preeclampsia is primarily a subjective clinical assessment and difficult to clearly differentiate from less severe forms of the disorder, early onset preeclampsia can easily be separated from late onset preeclampsia. It manifests clear differences from the late onset disorder. Early onset preeclampsia is associated with an increase of growth restricted infants14 and pathological evidence of placental malperfusion.15 This is not the case with later onset of the disorder which is also less likely to predict later life cardiovascular disease. Furthermore, available biomarker predictors for preeclampsia are more successful for early than late onset preeclampsia.16 This has led to general agreement that the occurrence of preeclampsia early or late likely indicates distinct variants.
It also seems likely that the diverse risk factors predicting preeclampsia, including previous preeclampsia, chronic hypertension, pre-existing diabetes, multifetal gestation, and obesity would be mediated through different genes, metabolites and pathways to preeclampsia.
However, neither early vs. late onset preeclampsia nor the disorder in women with different risk factors can be discriminated by conventional laboratory assessment of biomarkers such as placental growth factor (PlGF).soluble fms-like tyrosine kinase-1 (sFlt-1), placental protein 13 (PP13), a disintegrin and metalloprotease 12 (ADAM12), pappalysin (PAPP-A ).17 This raises the challenge that there is likely overlap in the several pathways to the preeclampsia syndrome. This should not be considered to diminish the relevance of different routes to the disorder. A principal demonstrated in geriatric medicine is that with disorders of individuals that result from the interaction of several pathways to a common disease effect, normalizing even one of these can reverse the overall disorder.18
Gestational Hypertension
In considering the different suspected subtypes of preeclampsia it is important to consider gestational hypertension. To many and for many years gestational hypertension has been considered as simply the mildest form of preeclampsia. However, Chesley long ago pointed out that, while gestational hypertension might be an early (mildest) form of preeclampsia (as many as 25% of cases proceed to preeclampsia), it was just as likely to be chronic hypertension masked by the normal reduction of blood pressure in early pregnancy.11 Finally, it might be an altogether different form of pregnancy hypertension. Now that other organ system involvement is considered with hypertension to define preeclampsia,19 gestational hypertension is probably best considered as non-syndromic increased blood pressure during pregnancy. This is not to diminish its importance. Blood pressure elevation in pregnancy with hyperuricemia even without proteinuria is as good a predictor of growth restriction or iatrogenic preterm birth as hypertension with proteinuria.20 However, hypertension with neither elevated uric acid nor proteinuria was no different than normal pregnancy in relationship to these outcomes. Nevertheless, despite minimal impact of gestational hypertension on fetal outcome the relationship to increased later life cardiovascular disease is at strong as preeclampsia.4, 21 Thus, gestational hypertension may merit its own subtyping, and should not be considered simply a mild form of preeclampsia.
Other suspected subtypes
Only about one third of the cases of preeclampsia are associated with growth restriction. As mentioned, these tend to be present with early onset preeclampsia. However, even in this setting not all women with preeclampsia have growth restricted infants. It is possible that these pregnancies may differ from those with normal fetal growth.
It is now clearly established that the signs and symptoms of preeclampsia can occur for the first time days to weeks after the termination of pregnancy. In one study 0.5% of delivered women returned with new onset postpartum preeclampsia.22 Almost nothing is known about the pathophysiology or long range prognosis of this condition but conventional pathways such as placental malperfusion are unlikely.
It is also important to compare the route to preeclampsia in high and low resource settings. Although obesity, a leading risk factor for preeclampsia,23 is increasing in many low resource settings, undernutrition is characteristically associated with preeclampsia in these sites. There are few in depth studies of unique preeclampsia pathogenesis in low resource settings. However, it seems reasonable that preeclampsia with under and over nutritional intake might not be similar. Further, different microbiome, qualitative nutritional intake, levels of activity and sexual practices including pregnancy timing could also dictate different pathways to preeclampsia.
The presence of outliers should also not be ignored. It is rare for any preeclampsia predictor or component of manifest disease not to be highly scattered with outliers and considerable overlap with findings in women without preeclampsia. It should be considered and if possible tested that the diversity is due to different kinds of preeclampsia. This is demonstrated in Figure 2, in which arraying data as mean and standard error completely mask the diversity of the preeclampsia finding which when examined longitudinally identified subsets of preeclamptic subjects.24
Identification of other Potential Candidate Subtypes
Hypothesis Driven
In addition to the above proposed variants of preeclampsia, available data suggests other subtypes might be successfully explored.
Involvement of Different Maternal Organ Systems: an indicator of Subtypes?
Organs involved in the clinical presentation of preeclampsia are quite variable. While the primary defining feature is maternal hypertension, there is variable involvement of different maternal organ systems including the renal, hepatic, vascular, hemopoietic, coagulation and fibrinolytic systems, the brain, and the immune system. 17,25 Is it possible that the different organs involved might indicate different pathways to preeclampsia?
The variable involvement of differing organ systems suggests that biomarkers affiliated with these systems may identify subtypes; 17,25 However, most of the evidence implicating specific organs is derived from cross-sectional studies of women who present with preeclampsia, making it difficult to decipher cause from effect; this was the reasoning behind longitudinal prediction studies beginning early in gestation.26 While such studies failed to show sufficient predictive power of late first trimester biomarker measurements e.g. PLGF, sFlt-1, they did show increased predictive capacity later in gestation and with serial measurement of biomarkers 27,28 but still not reaching clinical utility. Perhaps carefully collected data from larger populations will indicate different linkages to different organ systems, providing specific targets.
Placental or Maternal Preeclampsia?
The placenta is considered central to the pathophysiology of preeclampsia as delivery of the placenta alleviates the condition. Involvement of defects in extravillous trophoblast invasion and adaptation of spiral arteries in early onset preeclampsia 29 are now generally accepted; however, there is still controversy as to the involvement of this mechanism in late onset preeclampsia. There is a relative dearth of standardized studies of the placental bed in late onset preeclampsia; however, there is evidence that in such cases there is normal trophoblast invasion and adaptation of the vasculature supplying the placenta.30 What then might be the underlying pathophysiology? Redman and Staff15 have suggested that the abnormal placentation of early gestation and the failure of the placenta in late gestation to maintain its own adequate oxygen supply due to increase trophoblast growth results in a common insult, syncytiotrophoblast stress, a common convergence point of two separate insults. These alternative routes to placental dysfunction, one present from early gestation and one not manifest until late gestation should suggest different predictors and preventive strategies.
An alternative explanation is that late onset preeclampsia is largely due to maternal factors. The increased incidence of preeclampsia in women with pre-existing vascular dysfunction (previous preeclampsia, chronic hypertension and pregestational diabetes) is strong evidence that maternal vascular condition is a predisposing factor.31 Additionally, the knowledge that women who have experienced preeclampsia are at increased risk for cardiovascular disease and stroke in later life suggests that vascular stress test of pregnancy may have exposed women with underlying subclinical cardiovascular disease such that they developed preeclampsia. Hence in some women the placenta may be “normal” but the stress of pregnancy interacts with predisposing suboptimal maternal vascular condition to cause preeclampsia17,25,31 However, data do not support the hypothesis that maternal factors are more important with late onset preeclampsia. The effect of prepregnancy maternal risks are indistinguishable for early and late onset preeclampsia, while the relationship to late life cardiovascular is far greater for early than late onset preeclampsia.5
It is simplistic to consider separate maternal and placental variants of preeclampsia. The placenta is always involved but it is likely that maternal genetics, epigenetics, behavior and environment interact with the placental factors modifying the route to placental dysfunction or the response to placental dysfunction. These variable maternal responses raise important questions in our considerations of subtypes and outcomes. It is evident with current observations that two women with similar lab findings, BMI ethnicity etc. may have diverse clinical outcomes. Part of this will be censoring by clinical care (e.g., earlier delivery) but part will be different maternal response to the placental insult. It is quite possible that the several placental syndromes, abruption, early pregnancy loss, stillbirth, fetal growth restriction and preterm birth, may all represent different maternal responses to the same insult.
Different long-range outcomes of preeclampsia as indicators of subtypes
Both preeclampsia and gestational hypertension predict future cardiovascular and cardiometabolic risk in mothers, including chronic hypertension, type 2 diabetes, myocardial infarction, heart failure, and stroke.32,33 Yet, only roughly half of women with preeclampsia develop chronic hypertension by age 50-60.3, 34 There may be differences in the preeclampsia of women who do, and do not, later develop CVD. For example, preterm preeclampsia and recurrent preeclampsia are especially powerful predictors of maternal CVD, suggesting clinically severe preeclampsia is the most likely to predict CVD; yet, to date, studies large enough to examine CVD endpoints have lacked detail on clinical severity of the preeclampsia episode, so this has yet to be confirmed.
As we examine preeclampsia as an ‘exposure’ predicting future maternal health, various preeclampsia subtypes may be revealed; we may even conclude that certain subtypes of preeclampsia might be better grouped with other pregnancy complications predictive of maternal cardiovascular disease. For example, spontaneous preterm delivery and placental abruption,35–38 are also associated with heightened CVD risk. Preeclampsia shares some clinical and histologic features with these pregnancy complications. These observations might prompt us to ‘think outside the hypertensive box’ and consider grouping preeclampsia with other features of pregnancy that result from, or predict, maternal cardiometabolic health.
Furthermore, we may surmise novel preeclampsia subtypes by examining long-term maternal health outcomes other than cardiometabolic disease. For example, in the Nurses’ Health Study 2 (NHS2), women with a history of hypertensive pregnancy had increased risks of respiratory, neurological, and infectious disease mortality than did women with normotensive pregnancies, even after adjustment for factors such as body mass index.
Such later life implications of preeclampsia beg the question of whether chronic disease risk factors predate preeclamptic pregnancy, but go undetected because they are rarely tested in young women, or because the risk factors rarely exceed clinical thresholds in a young population. Subclinical elevations of blood pressure, fasting glucose, abdominal obesity, inflammation, dyslipidemia, markers of poor hemodynamic function, and liver enzymes indicative of endothelial dysfunction are sometimes evident in the years before preeclamptic pregnancy.39–44 Similarly, much – though not all – of the risk of CVD associated with preeclampsia history is accounted for by the emergence of traditional cardiovascular risk factors, such as hypertension, after pregnancy.34, 45 Both the existence and variability in pre-pregnancy and post-pregnancy cardiometabolic risk factors may suggest useful preeclampsia subtypes.
Understanding preeclampsia’s association with later CVD may yield new insights into the vascular and metabolic types of preeclampsia: perhaps preeclampsia can be usefully subcategorized by endothelial dysfunction, insulin resistance, inflammation, or angiogenesis. Some ‘omics’ studies are identifying characteristics of preeclampsia that are familiar to cardiologists, including alterations in specific lipids and carnitines.46 As we interrogate omics studies, it may be fruitful to pursue omic signatures associated with CVD as a priori hypotheses.
Immunologically determined subtypes
During pregnancy the fetal allograft has to be tolerated by the maternal immune system.47 There has long been the thought that preeclampsia, and other disorders of gestation, are associated with a breakdown of this immune tolerance. The major effectors at the maternal fetal interface are uterine natural killer cells (uNK) that are not cytotoxic but regulate trophoblast invasion and spiral artery remodeling. They recognize self-major histocompatibility complexes (MHC) of the mother and non-self-allogenic MHC from the paternal genotype. uNK express killer cell Ig-like receptors (KIR) 48 while extravillous trophoblast express the KIR ligand polymorphic HLA-C. 49 Every pregnancy expresses a unique combination of maternal KIR and fetal HLA-C (has paternal component) which affects the success of placentation and pregnancy.50 Inhibition of uNK responses by MHC-self recognition may lead to defective spiral artery remodeling. Also, certain maternal KIR haplotypes can protect against preeclampsia while others confer risk.50,51 These immunological interactions determine a specific immune subtype which can be predicted by maternal and paternal genes, and which may someday be amenable to intervention.
On the other hand, we have long been aware that pregnancies resulting from the use of assisted reproductive technologies (ART) are at higher risk of developing preeclampsia.52 This is thought to be the result of immunological interactions and of asynchrony between the development of the blastocyst and endometrium at the time of implantation (the seed and the soil hypothesis) 53, 54 due to the use of hormonal regimens to facilitate egg collection. This mismatch may alter placental development and extravillous trophoblast invasion as seen in early onset preeclampsia. It would seem these interactions would provide a profitable area to explore as a source of subtypes with implications for all pregnancies.
Discovery driven candidate subtypes
Another strategy to identify alternative routes to the preeclampsia is to utilize the power of discovery science. (Supplement: Clustering of subtypes1–9) Current powerful analytical strategies have allowed agnostic determination of disease subtypes. The rapid development of the “-omic” technologies has dramatically expanded the number of dimensions that can be added to the more traditional categories with associated increases in both physiologic insight but also analytic complexity. Regardless of the source of the information, however, the underlying assumption will be that individuals sharing a disease subtype will also share similar disease pathophysiologies.55, 62 The search for subtypes then becomes an attempt to identify the presence of these groups, or “clusters”, that represent similar pathophysiological patterns.
Microparticle Associated Protein Clustering in Preeclampsia.
One of our group analyzed plasma microparticle proteomic data gathered at 12 weeks’ gestation from 23 women with early onset preeclampsia of a nature severe enough to require delivery in or before the 35th week of gestation.64 Analysis indicated two sub-groups. Proteins in one cluster were associated with platelet function, while those in the second were associated with complement activity. Interestingly, the second cluster was associated with a more severe clinical course with earlier average gestational age at delivery, higher blood pressures and more severe lab perturbations. This unsupervised search for disease subgroups within women diagnosed with preeclampsia was internally validated by its associated with distinct biological processes and clinically validated by the differences in clinical characteristics and outcome associated with each cluster. At least regarding early preeclampsia with sufficient severity to require delivery during or prior to the 35th week of gestation, these clusters may identify distinct subsets with different pathophysiologies within the disease.
Evidence of subtypes from genomic studies
A bioinformatics approach has been used to extract from the published literature and organize, using cluster analysis and gene ontology, genes and variants associated with different clinical phenotypes of preeclampsia.65 There was distinct segregation of genes by severity and timing of preeclampsia, with associated conditions such as growth restriction and HELLP syndrome and by biological source (maternal, fetal or both). Subsequent placental genomic studies suggest at least three subgroups of preeclampsia. Using the DNA methylation signatures from a mixed group of early onset preeclampsia, late onset preeclampsia and preterm controls Wilson et. al performed hierarchical clustering analysis and found 2 separate clusters.66 Within early onset preeclampsia, they also found evidence of 2 subgroups, however, without strong correlations to clinical phenotypes.
In an attempt to unravel the possible involvement of the placenta in the heterogeneous subtypes of preeclampsia, Leavey et al 67 adopted a genome-wide microarray analysis of gene expression profiles in placental tissue from normotensive vs preeclamptic women. This revealed 5 distinct clusters of placental gene expression: 1. Maternal preeclampsia with placental gene expression profiles similar to healthy pregnancy, 2. “Canonical” preeclampsia with high expression of angiogenic genes, those related to hypoxia and altered hormone secretion, 3. Immunological preeclampsia with an over-representation of immune and proinflammatory genes, 4. Preterm normotensive women with overexpression of genes related to cell proliferation and stress responses and 5. Those with no strong clinical, gene expression or epigenetic associations, probably being chromosomal abnormalities. Subsequently this group performed additional studies 68 and found a 65% concordance between placental gene expression and histopathologic phenotype and strong evidence of 3 distinct forms of placental disease underlying preeclampsia. Cluster 1 developed preeclampsia with very little evidence of placental involvement, Cluster 2 had the most severe placental pathology with evidence of maternal vascular malperfusion, distal villous hypoplasia, infarctions, advanced villous maturation and increased syncytial knots and preponderantly early onset preeclampsia. The immune subtype, cluster 3, again had significant placental pathology with profound immune gene activation e.g. overexpression of TNFa, IFNg, chemokine ligand-10 . Cluster 4 showed the lesions of histologic chorioamnionitis but were normotensive and cluster 5 . (the chromosomal abnormality group)had no enrichment of placental lesion.
Overall, current literature confirms the heterogeneity of preeclampsia at the molecular level. The variable clinical presentation, biomarkers of different organ systems that can be measured and the differing placental gene expression and histologic subtypes point towards at least 2 different subtypes of Canonical or Immune susceptibility, with other possible less prevalent subtypes and the exact number of subtypes are yet to be confirmed by additional large-scale cohort studies at the multi-omics level.70 However, omics approaches are “discovery driven” science, and it has proven clinically insightful in treating other complex diseases, such as cancers. It has become clear that this field will continue to accumulate more data to be organized into databases such as DASH (Data and Specimen Hub) in NICHD. This will ultimately lead to more comprehensive and unbiased identification of molecular subtypes of preeclampsia with corresponding clinical phenotypic differences.
Determining the relevance of candidate subtypes
Clinical relevance
Currently available and emerging data support that the preeclampsia syndrome may be divided into several subtypes. However, which of these are clinically significant? There are features which indicate whether a particular subtype is relevant to management:
-
Subtype identifies a pathway amenable to therapy.
The subtype identifies a specific targetable pathophysiological pathway.
or --The purported subtype predicts radically different outcomes for mother and/or baby. (Figure 3)
-
A subtype must be recognizable:
It must be feasible to identify the subtype in time to direct prediction, prevention and therapy. This is particularly relevant given that many discovery studies are performed on maternal or fetal tissues, including placenta, at the end of pregnancy.
-
Findings must be reproducible and generalizable.
Reproducibility should be tested for the subtype in similar populations. Once reproducibility is established, generalizability should be examined in disparate populations. We suspect most subtypes will be present in most populations but possibly with radically different frequencies. This would explain the difficulty of demonstrating successful prediction or prevention in heterogenous populations. We would urge that assessing generalizability will include low resource settings in which the vast majority of infant and maternal mortality occur.
Figure 3: Increased information on adverse outcome determined by subtype.
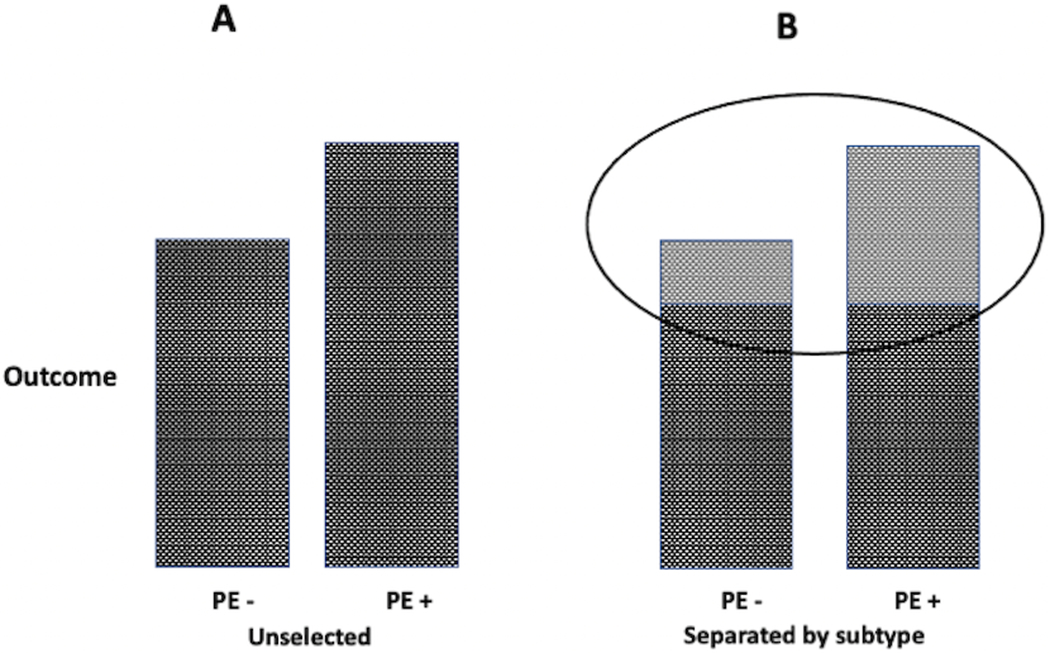
Panel A indicates the overall adverse outcome in women with or without preeclampsia. There is a slight to moderate increase in the adverse outcome in all women with preeclampsia. In panel B the circled area indicates that within these same women those within a specific cluster or subtype ( ) manifest a greater difference in the proportional occurrence of the outcome.
) manifest a greater difference in the proportional occurrence of the outcome.
Evaluation of clinical relevance
Conventional epidemiological relationships may provide evidence for the features cited for subtype relevance.
-
Subtype identifies a pathway amenable to therapy:
If a particular therapy is almost universally effective in a subtype this directs attention to a particular pathway(s).
-
or --The subtype predicts outcome:
The maternal and fetal outcome with the subtype should be compared with that in the general preeclamptic population.(Figure 3)
-
A subtype must be recognizable to predict outcome early enough to direct therapy.
The correlation of the subtype with conventional clinical findings, which in some cases will have identified the subtype (obesity, race, early pregnancy blood pressure etc.) must be sufficiently specific to justify modifying management. Similarly, biomarkers, again which may have been used to identify a particular subtype, must possess similar specificity.
-
Findings must be reproducible and generalizable.
Reproducibility and generalizability should be tested for the subtype in similar and different populations including in subjects from low resource settings
Harnessing the power of big data to draw inference
The use of big data analyses to complement standard epidemiological approaches provides special insights. In addition to being used to identify previously unrecognized subsets, those identified or suspected from clinical findings or hypotheses can be examined to determine the existence and specificity of particular pathways. Given the heterogeneity of this syndrome, we propose that a big data driven approach is much needed in order to draw inference on preeclampsia subtypes.
-
1.
Subtype identifies a pathway amenable to therapy:
Systems analysis of clusters may indicate a specific pathway to the syndrome (e.g. inflammation). If such analysis does not clearly indicate a specific pathway, analyses of risk and response to therapy of women with the cluster can nonetheless provide useful management information. 69
-
2.
or ---The subtype predicts outcome:
Clusters even if not part of a discernable pathway can be related to outcome (Figure 3).69
-
3.
A subtype must be recognizable:
A molecular subtype is credible and potentially useful clinically to direct therapy or indicate outcome if collectively the patients in that cluster are enriched with some clinical phenotypes. For a molecular subtype that is lacking clear phenotypic correspondence, additional pathological findings, biomarkers correlation or association with risk factors (environmental, behavioral or genetic) may provide guidance to its implications for clinical management.
-
5.
Findings must be reproducible and generalizable.
Once the best clusters are identified, one should use additional similar cohorts to validate that indeed these subgroups are reproducible, rather than being specific only to the cohort where the discovery is made. For this purpose, supervised learning methods can be employed. When reproducibility is established the presence and frequency of these clusters in disparate populations including low resource setting should be examined.
Challenges and Solutions
Recognition of subtypes
A major challenge to the recognition of preeclampsia as more than one disorder is the approach of many investigators to studies of preeclampsia. In certain investigative areas, such as cancer, it has become dogma that diseases with phenotypic similarities do not necessarily share common pathogenesis. In 2015, Molin Wang stated, “… it is increasingly necessary to consider pathogenesis and inherent heterogeneity of any given health condition and outcome. As the unique disease principle implies, no single biomarker can perfectly define disease.”70 This has not been the perception of most investigators in preeclampsia. Efforts are made repeatedly to make all cases of preeclampsia fit into to a particular pathogenic pathway (e.g. angiogenesis)71 or some other model of preeclampsia, such that in some cases, it is stated that if the particular marker is not present the disorder is not preeclampsia.71 This approach needs to be modified with the default assumption that there is more than one subtype. In keeping with this, data must be evaluated and presented in a manner that emphasizes rather than hides variability.72
A tremendously valuable addition to our understanding of preeclampsia comes from discovery science, which not only identifies previously unrecognized subsets but also has the capacity to decipher pathways and fine tune risk factors. Given the heterogeneity of the syndrome, it is possible that the same molecular subtype exhibit different profiles at the gene or DNA methylation or metabolite levels, however their commonality is manifested by similarly altered biological functions. Thus, a holistic view for defining molecular subtype needs to be recognized.
High quality data in large quantities
A major challenge to the search for subtypes is the availability of large amounts of high quality data. Electronic medical records would seem to be a readily available source of large amounts of data. Unfortunately, although the amount of data is large and of reasonable quality the data being collected emphasizes billing rather that research and vital information often is not present. Attempts to mine birth certificates and administrative data provide large amounts of data but this often is not high quality and again often lacks adequate detail. A virtually untapped source of high quality data is research studies, however, even very large single studies do not provide adequate numbers of subjects for state of the art analyses. An obvious solution is data sharing; however, this provides its own challenges.73 A major challenge is the mind set of investigators, funding agencies, and academic institution for whom individual credit is the major consideration. In addition, even in well-designed studies, data fields, including outcomes, are not well characterized since there is currently no accepted standardization. Data collection and storage and management present other challenges. Very few databases are designed with the ability to share data as a priority. Trying to combine different databases is expensive and time consuming and again made less valuable because there are no agreed upon standards.
There are some encouraging signs of progress. Funding agencies, (https://www.sciencemag.org/news/2019/11/why-nih-beefing-its-data-sharing-rules-after-16-years ) and academic institutions are increasingly appreciating and encouraging sharing of data. Efforts are also being made to encourage investigators to appreciate the value of sharing as indicated in joint efforts of groups studying Covid.74 The Global Pregnancy Collaboration (CoLab) has provided suggestions to facilitate sharing73 and recommended data fields for the study of preeclampsia,75 and the International Collaboration to Harmonise Outcomes in Pre-eclampsia (iHOPE) has suggested outcomes to be included in preeclampsia studies.76 To attempt to facilitate sharing and merging of data the CoLab has also prepared a preeclampsia database (COLLECT) available to all investigators for a modest cost with no charge to investigators from low resource or beginning investigators who do not have funding. This harmonized database is web based, modular and with data only accessible to the investigator.77 However, when choosing to do so individuals using this database can easily share data with each other.
Conclusions/Recommendations
Conclusions
There is abundant evidence that preeclampsia exists as more than one subtype (e.g. early and late onset preeclampsia). Our current understanding of the variable presentation and prognosis of preeclampsia also directs testing of the hypotheses that some cases of preeclampsia (e.g. with and without obesity, affecting different organ systems, or with or without later life consequences) may also present clinically useful subtypes. These findings are complemented by biomedical informatics techniques enabling new discoveries of preeclampsia subtypes.
Recommendations
We should recognize subtypes of preeclampsia as the default option and celebrate rather than ignore outliers.
Efforts should be directed at testing the clinical usefulness of purported subtypes and ultimately design subtype-specific prediction, prevention and therapy.
Discovery science should be exploited to identify and refine subtypes, pathways, risk factors and outcome. Since several different subtypes based on different omics (e.g. gene expression, DNA methylation) are proposed, it is important to consolidate these conclusions aided by advanced bioinformatics algorithms that can integrate multiple types of data.
It is critical to establish consistent and standard protocols for sample collection, sample processing, data generation and data analysis pipelines. Equally importantly, data harmonization and sharing is urgently needed to enable the “Big Data” approach. The pregnancy research community, similar to other biomedical domains, needs to rapidly adopt to the “data sharing” and “open data” mind-set in order to allow knowledge discovery and re-discovery. 78
We should modify data collection, sharing, and analysis to support future “perfect” studies but should also begin now, as best possible with materials available, to discriminate preeclampsia subtypes.
Analytical strategies directed at characterizing and utilizing heterogeneity that have become part of the armamentarium of investigators in other areas should begin to be applied to the study of preeclampsia. Tools are available to identify clinically useful subtypes. The importance of recognizing and using these subtypes cannot be overemphasized. With these approaches we will identify rational, individualized approaches to prediction, prevention and perhaps even therapy.
Supplementary Material
Acknowledgements
This presentation is based upon presentations and discussions at the Global Pregnancy Collaboration Workshop, Subtypes of Preeclampsia: A Strategy for Recognizing and Deciphering Pathophysiology, Sept 2 – 3, 2019 Oxford, England. Speakers contributing, in addition to listed authors, included: Ira Bernstein, University of Vermont; Kent Thornburg and Leslie Myatt, Oregon Health Sciences University; Titia Lely, UMC Ultrecht; Robin Tuytten, Metabolomics ; Chris Redman and William Cooke, University of Oxford; Katie Gray, David Cantonwine, Chelsea Messinger and Tom McElrath, Harvard University; Gordon Smith, Cambridge University
Sources of Funding
Lana Garmire was supported by R01 LM012373 and LM012907 awarded by NLM, and R01 HD084633 awarded by NICHD.
Contributor Information
James M. Roberts, Investigator Magee-Womens Research Institute, Professor Obstetrics Gynecology and Reproductive Sciences, Epidemiology and Clinical and Translational Research, University of Pittsburgh.
Janet W. Rich-Edwards, Associate Professor, Department of Epidemiology, Harvard T. H. Chan School of Public Health, Harvard University, Boston, Massachusetts, Division of Women’s Health, Department of Medicine, Brigham and Women’s Hospital and Harvard Medical School, Boston, Massachusetts
Thomas F. McElrath, Associate Professor, Division of Maternal-Fetal Medicine, Brigham & Women’s Hospital, Harvard Medical School, Boston, MA
Lana Garmire, Associate Professor (with tenure), Department of Computational Medicine and Bioinformatics, Medical School, University of Michigan.
Leslie Myatt, Professor Obstetrics and Gynecology, Bob and Charlee Moore Endowed Professor, Moore Institute of Nutrition and Wellness, Oregon Health & Science University.
References
- 1.Burton GJ, Redman CW, Roberts JM, Moffett A. Pre-eclampsia: pathophysiology and clinical implications. BMJ. 2019; 366:l2381. [DOI] [PubMed] [Google Scholar]
- 2.Roberts JM, Bell MJ. If we know so much about preeclampsia, why haven’t we cured the disease? J Reprod Immunol. 2013; 99:1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bellamy L, Casas JP, Hingorani AD, Williams DJ. Pre-eclampsia and risk of cardiovascular disease and cancer in later life: systematic review and meta-analysis. BMJ. 2007; 335:974. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Riise HKR, Sulo G, Tell GS, Igland J, Nygard O, Iversen A- C, Daltveit AK. Association Between Gestational Hypertension and Risk of Cardiovascular Disease Among 617 589 Norwegian Women. Journal of the American Heart Association. 2018; 7:13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Mongraw-Chaffin ML, Cirillo PM, Cohn BA. Preeclampsia and cardiovascular disease death: prospective evidence from the child health and development studies cohort. Hypertension. 2010; 56:166–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Chappell LC, Seed PT, Briley AL, Kelly FJ, Lee R, Hunt BJ, Parmar K, Bewley SJ, Shennan AH, Steer PJ, Poston L. Effect of antioxidants on the occurrence of pre-eclampsia in women at increased risk: a randomised trial. Lancet. 1999; 354:810–6. [DOI] [PubMed] [Google Scholar]
- 7.Poston L, Briley AL, Seed PT, Kelly FJ, Shennan AH, Vitamins in Pre-eclampsia Trial C. Vitamin C and vitamin E in pregnant women at risk for pre-eclampsia (VIP trial): randomised placebo-controlled trial.[see comment]. Lancet. 2006; 367:1145–54. [DOI] [PubMed] [Google Scholar]
- 8.Roberts JM, Myatt L, Spong CY, et al. Vitamins C and E to Prevent Complications of Pregnancy-Associated Hypertension. N Engl J Med. 2010; 362:1282–91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Sibai BM, Caritis SN, Thom E, Klebanoff M, McNellis D, Rocco L, Paul RH, Romero R, Witter F, Rosen M, et al. Prevention of preeclampsia with low-dose aspirin in healthy, nulliparous pregnant women. The National Institute of Child Health and Human Development Network of Maternal-Fetal Medicine Units. N Engl J Med. 1993; 329:1213–8. [DOI] [PubMed] [Google Scholar]
- 10.Caritis S, Sibai B, Hauth J, Lindheimer MD, Klebanoff M, Thom E, VanDorsten P, Landon M, Paul R, Miodovnik M, Meis P, Thurnau G. Low-dose aspirin to prevent preeclampsia in women at high risk. National Institute of Child Health and Human Development Network of Maternal-Fetal Medicine Units [see comments]. N Engl J Med. 1998; 338:701–5. [DOI] [PubMed] [Google Scholar]
- 11.Chesley L Hypertensive Disorders in Pregnancy. New York: Appleton-Century-Crofts; 1978. [Google Scholar]
- 12.Weissgerber TL, Winham SJ, Heinzen EP, Milin-Lazovic JS, Garcia-Valencia O, Bukumiric Z, Savic MD, Garovic VD, Milic NM. Reveal, Don’t Conceal: Transforming Data Visualization to Improve Transparency. Circulation. 2019; 140:1506–18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Staff AC, Benton SJ, von Dadelszen P, Roberts JM, Taylor RN, Powers RW, Charnock-Jones DS, Redman CWG. Redefining preeclampsia using placenta-derived biomarkers. Hypertension. 2013; 61:932–42. [DOI] [PubMed] [Google Scholar]
- 14.Xiong X, Fraser WD. Impact of pregnancy-induced hypertension on birthweight by gestational age. Paediatr Perinat Epidemiol. 2004; 18:186–91. [DOI] [PubMed] [Google Scholar]
- 15.Redman CW, Staff AC. Preeclampsia, biomarkers, syncytiotrophoblast stress, and placental capacity. Am J Obstet Gynecol. 2015; 213:S9.e1, S9–11. [DOI] [PubMed] [Google Scholar]
- 16.Rolnik DL, Wright D, Poon LC, et al. Aspirin versus Placebo in Pregnancies at High Risk for Preterm Preeclampsia. N Engl J Med. 2017:28. [DOI] [PubMed] [Google Scholar]
- 17.Myatt L, Miodovnik M. Prediction of preeclampsia. Semin Perinatol. 1999; 23:45–57. [DOI] [PubMed] [Google Scholar]
- 18.Resnick NM, Marcantonio ER. How should clinical care of the aged differ? Lancet. 1997; 350:1157–8. [DOI] [PubMed] [Google Scholar]
- 19.Roberts JM, August PA, Bakris G, et al. Hypertension in Pregnancy Report of the American College of Obstetricians and Gynecologists’ Task Force on Hypertension in Pregnancy. Obstet Gynecol. 2013; 122:1122–31. [DOI] [PubMed] [Google Scholar]
- 20.Schmella MJ, Clifton RG, Althouse AD, Roberts JM. Uric Acid Determination in Gestational Hypertension: Is it as Effective a Delineator of Risk as Proteinuria in High-Risk Women? Reproductive Sciences. 2015; 22:1212–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Tooher J, Thornton C, Makris A, Ogle R, Korda A, Hennessy A. All Hypertensive Disorders of Pregnancy Increase the Risk of Future Cardiovascular Disease. Hypertension. 2017; 70:798–803. [DOI] [PubMed] [Google Scholar]
- 22.Redman EK, Hauspurg A, Hubel CA, Roberts JM, Jeyabalan A. Clinical Course, Associated Factors, and Blood Pressure Profile of Delayed-Onset Postpartum Preeclampsia. Obstet Gynecol. 2019; 134:995–1001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Roberts JM, Bodnar LM, Patrick TE, Powers RW. The role of obesity in preeclampsia. Pregnacy Hypertension. 2011; Jan 1;1:6–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Powers RW, Roberts JM, Plymire DA, Pucci D, Datwyler SA, Laird DM, Sogin DC, Jeyabalan A, Hubel CA, Gandley RE. Low Placental Growth Factor Across Pregnancy Identifies a Subset of Women With Preterm Preeclampsia Type 1 Versus Type 2 Preeclampsia? Hypertension. 2012; 60:239–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Myatt L, Carpenter L. Prediction of Preeclampsia. In: F L MB, eds. Preeclampsia Etiology and Clinincal Practice. Cambridge: Cambridge University Press; 2007. [Google Scholar]
- 26.Myatt L, Clifton RG, Roberts JM, et al. First-Trimester Prediction of Preeclampsia in Nulliparous Women at Low Risk. Obstet Gynecol. 2012; 119:1234–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Myatt L, Clifton RG, Roberts JM, et al. The utility of uterine artery Doppler velocimetry in prediction of preeclampsia in a low-risk population. Obstet Gynecol. 2012; 120:815–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Myatt L, Clifton RG, Roberts JM, et al. Can changes in angiogenic biomarkers between the first and second trimesters of pregnancy predict development of pre-eclampsia in a low-risk nulliparous patient population? BJOG. 2013; 120:1183–91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Brosens IA, Robertson WB, Dixon HG. The role of the spiral arteries in the pathogenesis of preeclampsia. Obstet Gynecol Annu. 1972; 1:177–91. [PubMed] [Google Scholar]
- 30.Brosens I The uteroplacental vessels at term - the distribution and extent of physiological changes. Trophoblast Research. 1988; 3:61–7. [Google Scholar]
- 31.Myatt L, Roberts JM. Preeclampsia: Syndrome or Disease? Curr Hypertens Rep. 2015; 17:83. [DOI] [PubMed] [Google Scholar]
- 32.Grandi SM, Filion KB, Yoon S, Ayele HT, Doyle CM, Hutcheon JA, Smith GN, Gore GC, Ray JG, Nerenberg K, Platt RW. Cardiovascular Disease-Related Morbidity and Mortality in Women With a History of Pregnancy Complications. Circulation. 2019; 139:1069–79. [DOI] [PubMed] [Google Scholar]
- 33.Wu P, Haththotuwa R, Kwok CS, Babu A, Kotronias RA, Rushton C, Zaman A, Fryer AA, Kadam U, Chew-Graham CA, Mamas MA. Preeclampsia and Future Cardiovascular Health: A Systematic Review and Meta-Analysis. Circulation Cardiovascular Quality & Outcomes. 2017; 10. [DOI] [PubMed] [Google Scholar]
- 34.Stuart JJ, Tanz LJ, Missmer SA, Rimm EB, Spiegelman D, James-Todd TM, Rich-Edwards JW. Hypertensive Disorders of Pregnancy and Maternal Cardiovascular Disease Risk Factor Development: An Observational Cohort Study. Ann Intern Med. 2018; 169:224–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Ananth CV, Hansen AV, Elkind MSV, Williams MA, Rich-Edwards JW, Nybo Andersen AM. Cerebrovascular disease after placental abruption: A population-based prospective cohort study. Neurology. 2019; 93:e1148–e58. [DOI] [PubMed] [Google Scholar]
- 36.Catov JM, Wu CS, Olsen J, Sutton-Tyrrell K, Li J, Nohr EA. Early or recurrent preterm birth and maternal cardiovascular disease risk. Ann Epidemiol. 2010; 20:604–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Wu P, Gulati M, Kwok CS, Wong CW, Narain A, O’Brien S, Chew-Graham CA, Verma G, Kadam UT, Mamas MA. Preterm Delivery and Future Risk of Maternal Cardiovascular Disease: A Systematic Review and Meta-Analysis. J Am Heart Assoc. 2018; 7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Tanz LJ, Stuart JJ, Williams PL, Rimm EB, Missmer SA, Rexrode KM, Mukamal KJ, Rich-Edwards JW. Preterm Delivery and Maternal Cardiovascular Disease in Young and Middle-Aged Adult Women. Circulation. 2017; 135:578–89. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Foo FL, Mahendru AA, Masini G, Fraser A, Cacciatore S, MacIntyre DA, McEniery CM, Wilkinson IB, Bennett PR, Lees CC. Association Between Prepregnancy Cardiovascular Function and Subsequent Preeclampsia or Fetal Growth Restriction. Hypertension. 2018; 72:442–50. [DOI] [PubMed] [Google Scholar]
- 40.Haug EB, Horn J, Markovitz AR, Fraser A, Klykken B, Dalen H, Vatten LJ, Romundstad PR, Rich-Edwards JW, Asvold BO. Association of Conventional Cardiovascular Risk Factors With Cardiovascular Disease After Hypertensive Disorders of Pregnancy: Analysis of the Nord-Trondelag Health Study. JAMA Cardiology. 2019; 4:628–35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Cho GJ, Park JH, Shin SA, Oh MJ, Seo HS. Metabolic syndrome in the non-pregnant state is associated with the development of preeclampsia. Int J Cardiol. 2016; 203:982–6. [DOI] [PubMed] [Google Scholar]
- 42.Hedderson MM, Darbinian JA, Sridhar SB, Quesenberry CP. Prepregnancy cardiometabolic and inflammatory risk factors and subsequent risk of hypertensive disorders of pregnancy. Am J Obstet Gynecol. 2012; 207:68.e1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Magnussen EB, Vatten LJ, Lund-Nilsen TI, Salvesen KA, Davey Smith G, Romundstad PR. Prepregnancy cardiovascular risk factors as predictors of pre-eclampsia: population based cohort study.[see comment]. BMJ. 2007; 335:978. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Cho GJ, Kim HY, Park JH, Ahn KH, Hong SC, Oh MJ, Kim HJ. Prepregnancy liver enzyme levels and risk of preeclampsia in a subsequent pregnancy: A population-based cohort study. Liver Int. 2018; 38:949–54. [DOI] [PubMed] [Google Scholar]
- 45.Markovitz AR, Haug EB, Horn J, Fraser A, Tilling KM, Rimm EB, Missmer SA, Williams PL, Romunstad PR, Åsvold BO, Rich-Edwards JW. Normotensive preterm delivery and maternal cardiovascular risk factor trajectories across the life course: The HUNT Study, Norway. Acta Obstet Gynecol Scand. 2020;00:1–11. 10.1111/aogs.14016 [DOI] [PubMed] [Google Scholar]
- 46.Kelly RS, Croteau-Chonka DC, Dahlin A, et al. Integration of metabolomic and transcriptomic networks in pregnant women reveals biological pathways and predictive signatures associated with preeclampsia. Metabolomics. 2017; 13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Moffett A, Loke YW. The immunological paradox of pregnancy: a reappraisal. Placenta. 2004; 25:1–8. [DOI] [PubMed] [Google Scholar]
- 48.Parham P, Moffett A. Variable NK cell receptors and their MHC class I ligands in immunity, reproduction and human evolution. Nat Rev Immunol. 2013; 13:133–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Apps R, Murphy SP, Fernando R, Gardner L, Ahad T, Moffett A. Human leucocyte antigen (HLA) expression of primary trophoblast cells and placental cell lines, determined using single antigen beads to characterize allotype specificities of anti-HLA antibodies. Immunology. 2009; 127:26–39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Moffett A, Colucci F. Uterine NK cells: active regulators at the maternal-fetal interface. J Clin Invest. 2014; 124:1872–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Hiby SE, Walker JJ, O’Shaughnessy K M, Redman CW, Carrington M, Trowsdale J, Moffett A. Combinations of maternal KIR and fetal HLA-C genes influence the risk of preeclampsia and reproductive success. J Exp Med. 2004; 200:957–65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Conrad KP, Baker VL. Corpus luteal contribution to maternal pregnancy physiology and outcomes in assisted reproductive technologies. Am J Physiol Regul Integr Comp Physiol. 2013; 304:R69–72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Conrad KP. Evidence for Corpus Luteal and Endometrial Origins of Adverse Pregnancy Outcomes in Women Conceiving with or Without Assisted Reproduction. Obstet Gynecol Clin North Am. 2020; 47:163–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.von Versen-Hoynck F, Hackl S, Selamet Tierney ES, Conrad KP, Baker VL, Winn VD. Maternal Vascular Health in Pregnancy and Postpartum After Assisted Reproduction. Hypertension. 2020; 75:549–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Begg CB, Zabor EC, Bernstein JL, Bernstein L, Press MF, Seshan VE. A conceptual and methodological framework for investigating etiologic heterogeneity. Stat Med. 2013; 32:5039–2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Bhattacherjee V, Mukhopadhyay P, Singh S, Johnson C, Philipose JT, Warner CP, Greene RM, Pisano MM. Neural crest and mesoderm lineage-dependent gene expression in orofacial development. Differentiation. 2007; 75:463–77. [DOI] [PubMed] [Google Scholar]
- 57.Brock G, Pihur V, Datta S, Datta S. ClValid: An R package for cluster validation. Journal of Statistical Software. 2008; 25:1–22. [Google Scholar]
- 58.Chu S, DeRisi J, Eisen M, Mulholland J, Botstein D, Brown PO, Herskowitz I. The transcriptional program of sporulation in budding yeast. Science. 1998; 282:699–705. [DOI] [PubMed] [Google Scholar]
- 59.DeRisi JL, Iyer VR, Brown PO. Exploring the metabolic and genetic control of gene expression on a genomic scale. Science. 1997; 278:680–6. [DOI] [PubMed] [Google Scholar]
- 60.Eisen MB, Spellman PT, Brown PO, Botstein D. Cluster analysis and display of genome-wide expression patterns. Proc Natl Acad Sci U S A. 1998; 95:14863–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.MacQueen J Some methods for classification and analysis of multivariate observations. Proc fifth Berkeley Symp Math Stat Probab Stat; 1967. 1967. p. 281–97. [Google Scholar]
- 62.Ogino S, Chan AT, Fuchs CS, Giovannucci E. Molecular pathological epidemiology of colorectal neoplasia: an emerging transdisciplinary and interdisciplinary field. Gut. 2011; 60:397–411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Pihur V, Brock GN, Datta S. Cluster Validation for Microarray Data: An Appraisal. Stat Sci Interdiscip Res Adv Multivar Stat Methods: World Scientific; 2009; 2009:195–206. [Google Scholar]
- 64.McElrath TF, Cantonwine DE, Jeyabalan A, Doss RC, Page G, Roberts JM, Brohman B, Zhang Z, Rosenblatt KP. Circulating Microparticle Proteins Obtained in the Late First Trimester Predict Spontaneous Preterm Birth at Less than 35 Weeks Gestation: A Panel Validation with Specific Characterization by Parity. Am J Obstet Gynecol. 2019; 25:25. [DOI] [PubMed] [Google Scholar]
- 65.Triche EW, Uzun A, DeWan AT, Kurihara I, Liu J, Occhiogrosso R, Shen B, Parker J, Padbury JF. Bioinformatic approach to the genetics of preeclampsia. Obstet Gynecol. 2014; 123:1155–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Wilson SL, Leavey K, Cox BJ, Robinson WP. Mining DNA methylation alterations towards a classification of placental pathologies. Hum Mol Genet. 2018; 27:135–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Leavey K, Benton SJ, Grynspan D, Kingdom JC, Bainbridge SA, Cox BJ. Unsupervised Placental Gene Expression Profiling Identifies Clinically Relevant Subclasses of Human Preeclampsia. Hypertension. 2016; 68:137–47. [DOI] [PubMed] [Google Scholar]
- 68.Benton SJ, Leavey K, Grynspan D, Cox BJ, Bainbridge SA. The clinical heterogeneity of preeclampsia is related to both placental gene expression and placental histopathology. Am J Obstet Gynecol. 2018; 219:604 e1–e25. [DOI] [PubMed] [Google Scholar]
- 69.Hamada T, Keum N, Nishihara R, Ogino S. Molecular pathological epidemiology: new developing frontiers of big data science to study etiologies and pathogenesis. J Gastroenterol. 2017; 52:265–75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Wang M, Kuchiba A, Ogino S. A Meta-Regression Method for Studying Etiological Heterogeneity Across Disease Subtypes Classified by Multiple Biomarkers. Am J Epidemiol. 2015; 182:263–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Rana S, Karumanchi SA, Lindheimer MD, Rana S, Karumanchi SA, Lindheimer MD. Angiogenic factors in diagnosis, management, and research in preeclampsia. Hypertension. 2014; 63:198–202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Weissgerber TL, Milic NM, Winham SJ, Garovic VD. Beyond Bar and Line Graphs: Time for a New Data Presentation Paradigm. Plos Biology. 2015; 13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Roberts JM, Mascalzoni D, Ness RB, Poston L, Global Pregnancy C. Collaboration to Understand Complex Diseases: Preeclampsia and Adverse Pregnancy Outcomes. Hypertension. 2016; 67:681–7. [DOI] [PubMed] [Google Scholar]
- 74.Moorthy V, Henao Restrepo AM, Preziosi MP, Swaminathan S. Data sharing for novel coronavirus (COVID-19). Bull World Health Organ. 2020; 98:150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Myatt L, Redman CW, Staff AC, Hansson S, Wilson ML, Laivuori H, Poston L, Roberts JM, Global Pregnancy C. Strategy for standardization of preeclampsia research study design. Hypertension. 2014; 63:1293–301. [DOI] [PubMed] [Google Scholar]
- 76.Duffy J, Cairns AE, Richards-Doran D, et al. A core outcome set for pre-eclampsia research: an international consensus development study. BJOG: An International Journal of Obstetrics & Gynaecology. 2020; 127:1516–26. [DOI] [PubMed] [Google Scholar]
- 77.Myers JE, Myatt L, Roberts JM, Redman C, Global Pregnancy C. COLLECT, a collaborative database for pregnancy and placental research studies worldwide. BJOG: An International Journal of Obstetrics & Gynaecology. 2019; 126:8–10. [DOI] [PubMed] [Google Scholar]
- 78.Brito JJ, Li J, Moore JH, Greene CS, Nogoy NA, Garmire LX, Mangul S. Recommendations to enhance rigor and reproducibility in biomedical research. GigaScience. 2020; 9:01. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.