

Abstract
Environmental factors such as climate change are now underway, which have substantial impacts on health and well‐being of human kind, but still imprecisely quantified, implications for human health. At present, one of the most significant discussions among scientists worldwide is interdependency of escalating environmental risk factors and the increasing rates of noncommunicable diseases (NCDs), which are the leading cause of death and disability worldwide. Climate change also triggers the occurrence of NCDs through a variety of direct and indirect pathways. Therefore, it is likely that the interdependence of climate change, environmental risk factors, and NCDs as a whole poses great threat to global health. Hence, this paper aims to review the latest evidence on impacts of environmental risk factors on NCDs and methods used in establishing the cause or correlation of environmental risk factors and NCDs. The literature review leveraged online databases such as PubMed and Google Scholar with articles that matched keywords “climate change”, “environmental risk factors,” and “noncommunicable diseases”. This review shows that the burden of NCDs is increasing globally and attribution of environmental risk factors such as climate change is significant. Understanding the nature of the relation between NCDs and the environment is complex and has relied on evidence generated from multiple study designs. This paper reviews eight types of study designs that can be used to identify and measure causal and correlational nature between environment and NCDs. Future projections suggest that increases in temperatures will continue and also increase the public health burden of NCDs.
Keywords: burden of disease, climate change, deaths, environmental change, environmental epidemiology, noncommunicable diseases
1. PLAIN LANGUAGE SUMMARY
Global environmental changes including climate change are now underway, which have huge impacts on health and well‐being of human being. However, its impacts are still not fully quantified and understanding the nexus between environmental changes and human health is very important. At present, one of the most significant discussions among global health communities is interdependency of escalating environmental risk factors including climate change and the increasing rates of noncommunicable diseases (NCDs), which are the leading cause of death and disability worldwide. Hence, this paper aims to review the latest evidence on impacts of global environmental changes on NCDs and methods used in quantifying the impacts of global environmental changes on burden of NCDs. This review shows that the burden of NCDs is increasing globally and attribution of environmental risk factors including climate change is significant.
2. BACKGROUND
Multiple environmental changes, such as climate, threaten the health of present and future generations, damaging health gains achieved over recent decades, and posing additional diseases burden in the future. These global environmental changes are driven by human activities which have deteriorated the Earth's natural system and its function to provide food, clean water, and fresh air and to modulate the global temperature within limits in which humanity has been able to thrive. 1 Environmental changes have direct and indirect impacts on human health, account for a significant burden of disease, and are exacerbating environmental and climate‐sensitive health risks and diseases. It is estimated that 23% of the global deaths in the year 2012 were caused due to environmental risk factors, amounting to 12.6 million deaths. 2 The environment risk factors are defined as a congregation of all the physical, chemical, and biological factors external to a person, and all related behaviors, but excluding those natural environments that cannot reasonably be modified. Moreover, the total and per capita rate of deaths and disease burden linked to the environment tends to be higher in low and middle‐income countries. This in turn can make significant effects towards achieving the sustainable development goals (SDGs), many of which are closely interlinked with the environmental determinants of health. 3 , 4 Climate change is one of the biggest threats to human health and wellbeing. It primarily impacts on social and environmental determinants of health including clean air, safe drinking water, secure food, and shelter and so on. 5 Climate change is projected to have significant adverse impacts on future morbidity and mortality. For example, the World Health Organization (WHO) projects that deaths related to heat exposure will have increased to over 100,000 per year by the 2050 s, with higher mortality rates in low‐ and middle‐income countries and the highest mortality resulting from climate change in South Asia. 6
Environmental hazard is regarded as one of the important causes of disease burden and is associated with the increased risk of exposure to several diseases. Several attempts have been made to identify the association between environmental risk factors and a wide range of infectious diseases. However, effects of climate change on noncommunicable diseases (NCDs) was rarely discussed in the literature. At present, one of the most significant discussions among scientists is the environmental risk factors and its impact on NCDs that are the leading cause of death and disability worldwide. Air pollution has shifted up to the fourth leading risk factors of deaths in 2019 which was in the fifth rank previously. 7 Among all the causes, air pollution is the second major cause contributing to NCDs related deaths globally. 8 Fossil fuels combustion emits various harmful air pollutants; fine particulate matter, ozone, sulfur dioxide, nitrogen dioxide, hydrocarbons, metals, etc. These are the major contributors of disease burden associated with air pollution. The mortality associated with Particulate Matter under 2.5 micrometers (PM2.5) exposure value is attributable to various NCDs; chronic obstructive pulmonary disease (COPD), cerebrovascular disease, ischemic heart disease, respiratory disease, and lung cancer. Similarly, disease burden associated with excess ozone, sulfur, and nitrogen dioxide is attributable to asthma, bronchial, and other lung diseases. 9
The Lancet first commissioned a review on "Managing the health effects of climate change" in 2009, which concluded that climate change is the biggest global health threat of the 21st century. 10 A follow‐up report on "Health and climate change" concluded that tackling climate change could be the greatest global health opportunity of the 21st century. 11 Besides effects on infectious diseases, climate change also triggers the incidence of NCDs through a variety of direct and indirect pathways. 12 The risk factors bridging the way from climate change to NCDs include air pollution, extreme temperature, alteration in food system, increased ozone production in troposphere, increased bushfire, alteration of ambient ultraviolet radiation, increased pests and weeds, extreme weather, and rise in sea level. 12 , 13 Therefore, it is likely that climate change, environmental risk factors, and NCDs collectively pose great threats to global health. If no action is taken, it is estimated that mortality due to ambient air pollution could double by 2050. 14
Despite the linkage, interventions prioritizing climate change and environmental risk factors for NCD prevention are still neglected in different global agenda. 15 This paper aims to review the latest evidence on impacts of environmental risk factors on NCDs, causal pathways, and research methods used in understanding the relationship between environmental risk factors and NCDs.
3. NCD BURDEN ATTRIBUTABLE TO ENVIRONMENTAL RISK
WHO estimated that, globally, 23% of all deaths (around 12.6 million deaths) were associated with the environment and two‐thirds of 12.6 million deaths due to NCDs were attributable to environmental risks. 2 NCD risk factors are strongly associated with environmental exposure and climate change. 16 According to the estimation of the Intergovernmental panel on climate change, the major source of release of environmental pollutants were electricity generation (35%), agriculture, forestry, and other land use (24%), industry (21%), transportation (14%), and buildings (6%). These sources of climate change are responsible for the NCD burden. 17 Air pollution poses the greatest burden in South East Asia and Western Pacific Regions. 18 Globally, air pollution is proved to be the second leading cause of NCDs. 8
Besides these, there are some other environmental factors that might impact on NCDs. Endocrine disruptors are the chemicals that interfere the normal functioning of endocrine system (metabolism, insulin production, sexual development, reproduction, fetal development etc). These substances contaminate the drinking water and food and pollute the air causing adverse effects on human health. 19 Similarly, previous studies have demonstrated the progressive effects of Chernobyl catastrophe on the endocrine system. The accumulation of ionizing radiation on the glands through internal exposure (inhalation, ingestion, injection) or external exposure increases the risk of thyroid as well as breast carcinogenesis. 20 , 21 A recent systematic review and meta‐analysis reports pooled proportion of 14.4% for newly diagnosed diabetes in hospitalized COVID‐19 patients indicating the lethal intersection between communicable diseases and NCDs. 22 Hence, prevention and control of communicable diseases should also consider care of NCDs.
The attribution of overall envrionemntal risks and air pollution on death rate (per 100,000 population) and disasbility adjusted life years (DALYS) from differnet NCDs is provided in Figure 1.
FIGURE 1.
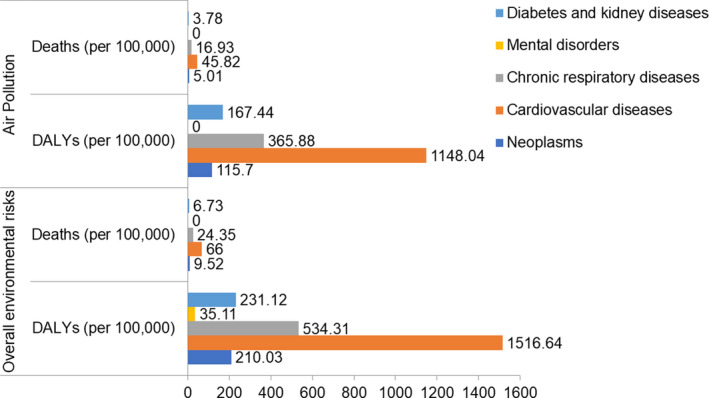
Global Deaths and DALYs attributable to noncommunicable disease burden associated with environmental risk factors. (Source: GBD estimates 2019, IHME)
Similarly, around 7 million deaths were due to air pollution (ambient and household) in 2016 with the 94% deaths in low‐ and middle‐income countries. The cause of premature deaths related to various types of outdoor pollution were Ischemic heart disease (58%), chronic obstructive pulmonary disease (18%), acute lower respiratory infections (18%), and 6% due to lung cancer. 23 Currently, there is also an increasing burden of NCDs in Nepal and two thirds (66%) of deaths are due to NCDs and with an additional 9% due to injuries. 24 According to a population based nationally representative study, the prevalence of chronic obstructive pulmonary disease, diabetes mellitus, chronic kidney disease, and coronary artery diseases is 11.7%, 8.5%, 6%, and 2.9% respectively among Nepalese 20 years old and above. 25 , 26 The NCD STEPS survey shows an increase in prevalence in NCD risk factors in Nepal such as physical inactivity, alcohol consumption, overweight, etc. 27 Among adults aged 40–69, 3.3% have a predicted 30% or more chance of having cardiovascular disease (CVD) in the next ten years. 27 Similarly, population based cancer registries in nine districts of Nepal reported the high prevalence of lung cancer in all the geographic areas of Nepal and higher incidence rate of all types of cancer was found in urban areas compared to semi urban and rural areas. 28 In order to address the increasing burden of Nepal, Government of Nepal has formulated multisectoral NCDs prevention and control plan 2014–2020 and implementing it. 29 Similarly, National health policy 2019 of Government of Nepal has incorpoted NCDs prevention and control polcies and strateiges.
A systematic review showed that the ambient air pollution in cities of 51 countries were due to traffic (25%), industrial activities (15%), domestic fuel burning (20%), natural resources (18%), and other unspecified human sources (22%). These activities contribute to climate change and ultimately impact human health. 30 In a large multicentric study, chronic outdoor exposure to PM2.5 was associated with increased odds of hypertension. 31 Similarly, approximately 3/4 of the chronic kidney disease (CKD) burden attributable to PM2.5 was due to concentration of PM2.5 over 10 µg/m3. 32 Several studies have also described the association between ambient air pollution and diabetes mellitus. 33 , 34 According to WHO air quality guidelines, reducing the PM2.5 concentration to 10 micrograms per cubic meter (µg/m3) could reduce the pollution related deaths by 15%. 9 Previous studies have proved that short term exposure to air pollutants cause headache, nausea, irritation in eye, nose, throat, and skin whereas long term effects exacerbate several respiratory illnesses and can even cause cancer and deaths. 35 Similarly, prolonged exposure to air pollutants and fuel combustion provokes the risk of COPD. 36
In addition to outdoor pollutants, there are some other origins of indoor pollutants. Indoor combustion of fuels, tobacco smoking, benzene, and formaldehyde in furniture are the major sources. Beside this, poor ventilation, air conditioning system, and chimneyless stoves further promote the household air pollution. 36 Previous studies have suggested that indoor air pollution is an important risk factor of hypertension. A systematic review showed that household solid fuel was significantly linked with hypertension. 37 Similarly, a study investigated the association between household air pollution and arthritis in six lower middle‐income countries (China, Ghana, India, Mexico, the Russian Federation, and South Africa). A significant association was observed between using cooking fuels (gas, wood, crops, grass, and animal dung) with the increased odds of arthritis. 38
In the context of COVID‐19 pandemic, comorbidity with NCDs increases individual risk of serious symptoms and death. COVID‐19 has increased mortality of people from CVD, and COPD, which are closely linked to climate change, through effects including extreme heat, ground‐level ozone, wildfire smoke, and increased pollen counts over longer seasons. The recent studies show that impact of COVID‐19 is very high on NCDs causing double epidemic of COVID‐19 and NCDs with highest effect on people suffering from hypertension, respiratory system disease, and CVD as compared with non‐severe diseases 39 , 40 , 41
4. IMPACTS OF CLIMATE CHANGE ON NCDS
Climate change is associated with the increased risk of NCDs through a variety of pathways. Climate change causes the earth's temperature to rise and also alters the rainfall pattern. As a result, the level of environmental air pollutants rise and this leads to increased disease burden associated with CVD. 42 Additionally, the rise in temperature results in severe heat stress which in turn increases the risk of CVD and chronic kidney diseases. 43 , 44 Similarly, the increase in concentration of air pollutants causes an increase in production of troposphere ozone. Exposure to ozone gives rise to mortality and morbidity attributable to several respiratory infections, including lung diseases. 45
A growing body of literature has discussed the impacts of climate change on mental health. Frequent natural disasters and wildfires cause the loss of land and disruption of physical infrastructure, which increases food insecurity. As a result, there is increased risk of mental health consequences such as anxiety, depression, trauma, post‐traumatic stress disorder, and suicidal ideation. 5 Extreme weather events such as floods, landslides, cyclones, and hurricanes also contribute to increased risk of injuries. 46
Climate change alters the behavior of sun exposure, causing change in stratospheric ozone, precipitation and cloud coverage and altering the ambient ultraviolet radiation (UVR). Due to these changes, new kinds of pests and weeds are introduced in the agriculture system. The increased use of herbicides and pesticides contaminates the food and water and their sources leading to Parkinson's diseases and different kinds of cancer like prostate and thyroid cancer. 47 , 48
Figure 2 summarizes the causal pathways of impacts of environmental and climate change on NCDs.
FIGURE 2.
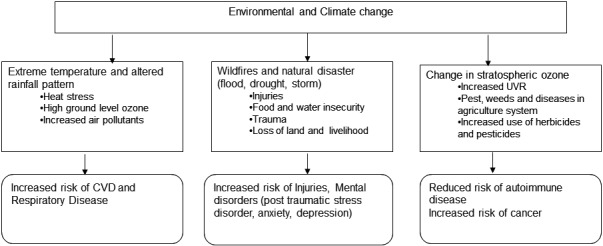
Causal pathways of impacts of environmental and climate change on NCDs
5. RESEARCH METHODS TO ESTABLISH RELATIONSHIPS BETWEEN ENVIRONMENTAL RISK FACTORS AND NCDS
A wide range of research designs are used for understanding the relationship between environmental risk factors and NCDs. 49 This may be done as single method or a combination of mixed methods:
observational studies (descriptive case studies, analytic studies),
experimental or interventional studies,
ecological studies (exploratory or analytic),
time trend studies (exploratory or analytic),
meta‐analyses, and
geo‐spatial models.
An observation study involves observing events for individuals in the study without altering or intervening them which could be a cross‐sectional study if observation be taken at a point of time or longitudinal study if the same subject be studied over time. Similarly, if the study begins with the outcome and considers the risk factors or past exposure is case‐control study and if the study begins with exposure and follows subjects forward in time to evaluate health outcomes that have not yet occurred is cohort study. In an experimental or interventional study, researchers evaluate the effects of an assigned intervention on an outcome.
Descriptive study designs such as case studies and cross‐sectional studies are used for describing the distribution (frequency and pattern) of environmental risk factors or disease outcomes in study populations, and often provide the rationale for pursuing an analytical study. The descriptive study describes distributions of health‐related outcomes (e.g., disease) and events in the population which are useful for formulating research questions and hypotheses.
Analytic study design examines associations with the ultimate goal to establish cause‐effects relationships and such design is useful for identifying the environmental causes of health‐related outcomes (diseases, events, or injury) in specified populations. The unit of analysis is individual and such design can be categorized as observational (case‐control or cohort), experimental or interventional study.
An ecologic study is common in environmental epidemiology which involves making comparisons between populations or groups of people (which is identified according to place such as country, province, city, geographical area, etc.) rather than among individuals which is appropriate in environmental settings. 50 The ecologic study could be exploratory if no specific exposure of interest exists or measured, and analytic if the primary exposure variable of interest is measured and considered in the analysis. The purpose of exploratory ecologic study is to identify the spatial patterns that may indicate an environmental etiology while as the ecologic association between the aggregate exposure level and the rate of health outcome (injury or disease) for various groups. The “ecological fallacy” can occur in that factors that are associated with population or group level disease rates may not be associated with disease in individuals. 51
Similarly, time trend design could be exploratory or analytic. In an exploratory time‐trend (or time series), a comparison of health outcome (injury or disease) rates over time is made for a population in a single geographic area such as age‐period‐cohort analysis. In contrast, in an analytic time‐trend analysis, the focus is on the ecologic association between average exposure change and disease rate change for a population in a single geographic area.
It is hard to establish a causal relationship between environmental risk factors and NCDs using findings of a single study. Hence, meta‐analysis is usually considered in environmental epidemiology because it provides a systematic comparison of studies that results in the aggregation of several studies into one analysis. 52
More recently, geographic information system (GIS) techniques are widely used in environmental epidemiological studies to estimate local burden of diseases and to identify hotspots of NCDs that can be linked with environmental risk factors at different geographical locations. 53 The most commonly used models for establishing relationships between environmental risk factors and NCDs are geostatistical models. 54 , 55 , 56 , 57 Various epidemiological models have been developed to estimate disease burden of NCDs from ambient and household air pollution as well as from lead exposure. 58 , 59 , 60 , 61 Though the health risks of climate change are increasingly observed with more impacts in low‐ and middle‐ income countries, several challenges are reported for conducting climate and health studies in developing countries 62
6. UNANSWERED QUESTIONS
A review has highlighted the importance of Earth observation (EO) technologies that have been used for infectious disease studies but not for NCD research. This technology can provide data on different environmental factors in a cost‐effective way, hence, suitable for measuring the impacts of environmental causes on NCD burden. However, lack of availability of environmental data is hindering the application of this technology for designing the NCD interventions. 63 Similarly, there are methodologies designed for understanding the impacts of climate change on infectious diseases 64 but methods for studying impacts of climate change on NCDs except for impact of climate change on heat related morbidity and mortality. 65 , 66 , 67 It is recommended to address air pollution, climate change, and NCDs in a holistic manner as an important area of research. 68 The campaign against climate change mitigation, such as withdrawal of the USA from the Paris agreement, can also significantly impact global action for climate change mitigation and adaptation and future climate change projections have high uncertainties. 69
7. FUTURE PROJECTIONS
Several studies have estimated heat‐related excess mortality under different climate change scenarios and heat waves are major environmental hazards. 70 , 71 , 72 For example, temperature increases in Beijing are projected to result in an increased CVD related death centered around the years 2050 and 2070 by 3.5% to 10.2%, as compared to its baseline period (2007–2009). 73 Also, chronic diseases are estimated to be highly prevalent in the areas that are vulnerable to environmental changes and food insecurity. 74 The projection of the future public health burden of temperature‐related health effects can provide valuable information to aid public health and environmental authorities in planning and communicating the risks of climate change to the public. 62 However, the uncertainties within such predictions are high and must be considered cautiously in program and policy design. Furthermore, nexus between air pollution, COVID‐19 and global burden of disease is reported 75 which demands further studies how air pollution and COVID‐19 impacts on global burden of diseases inclding of NCDs in future.
8. CONCLUSION
Global environmental change, including climate change, are now underway and have substantial impacts on health and well‐being of humankind, though those impacts are still imprecisely quantified for human health. This review shows that the burden of NCDs is increasing globally and attribution of environmental risk factors, including climate change, is significant. Understanding the nature of the relationship between NCDs and the environment is complex and has relied on evidence generated from multiple study designs. Better understanding the nexus between environmental risk factors and NCDs contributes to better adaptation and planning for prevention and control of NCDs. Future projections suggest that increases in temperatures will continue and also increase the public health burden of NCDs, which reaffirms the urgent need to develop climate resilient health systems worldwide.
This article is part of the Global Voices for Prevention of Noncommunicable Diseases Special Collection
REFERENCES
- 1. Haines A, Harris F, Kasuga F, Machalaba C. Future Earth‐linking research on health and environmental sustainability. BMJ. 2017;357:j2358. [DOI] [PubMed] [Google Scholar]
- 2. Prüss‐Ustün A, Wolf J, Corvalán C, Bos R, Neira M. Preventing disease through healthy environments: A global assessment of the burden of disease from environmental risks. Geneva: World Health Organization (WHO); 2016. [Google Scholar]
- 3. United Nations . The Sustainable Development Goals Report 2017. New York: United Nations; 2017. [Google Scholar]
- 4. Dhimal M, Dhimal M, Karki K, Montag D, Groneberg D, Kuch U. Tracking health‐related Sustainable Development Goals (SDGs) in Nepal. Journal of Health and Social Sciences. 2017;2(2):83‐86. [Google Scholar]
- 5. Hayes K, Blashki G, Wiseman J, Burke S, Reifels L. Climate change and mental health: risks, impacts and priority actions. International Journal of Mental Health Systems. 2018;12(1):1‐12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. World Health Organization . Quantitative risk assessment of the effects of climate change on selected causes of death, 2030s and 2050s. Geneva: World Health Organization; 2014. [Google Scholar]
- 7. Health Effects Institute . State of Global Air 2020. Special Report. Boston, MA: Health Effects Institute; 2020. [Google Scholar]
- 8. Prüss‐Ustün A, van Deventer E, Mudu P, et al. Environmental risks and non‐communicable diseases. BMJ. 2019;364:l265. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. World Health Organization . Ambient (outdoor) air pollution; 2018. https://www.who.int/news‐room/fact‐sheets/detail/ambient‐(outdoor)‐air‐quality‐and‐health
- 10. Costello A, Abbas M, Allen A, et al. Managing the health effects of climate change. The Lancet. 2009;373(9676):1693‐1733. [DOI] [PubMed] [Google Scholar]
- 11. Watts N, Adger WN, Agnolucci P, et al. Health and climate change: policy responses to protect public health. Lancet. 2015;386(10006):1861‐1914. [DOI] [PubMed] [Google Scholar]
- 12. Friel S, Bowen K, Campbell‐Lendrum D, Frumkin H, McMichael AJ, Rasanathan K. Climate change, noncommunicable diseases, and development: the relationships and common policy opportunities. Annu Rev Public Health. 2011;32:133‐147. [DOI] [PubMed] [Google Scholar]
- 13. Colagiuri R, Boylan S, Morrice E. Research priorities for NCD prevention and climate change: An international Delphi survey. International journal of environmental research and public health. 2015;12(10):12941‐12957. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Lelieveld J, Evans JS, Fnais M, Giannadaki D, Pozzer A. The contribution of outdoor air pollution sources to premature mortality on a global scale. Nature. 2015;525(7569):367‐371. [DOI] [PubMed] [Google Scholar]
- 15. Landrigan PJ, Fuller R, Acosta NJR, et al. The Lancet Commission on pollution and health. The lancet. 2018;391(10119):462‐512. [DOI] [PubMed] [Google Scholar]
- 16. Campbell‐Lendrum D, Prüss‐Ustün A. Climate change, air pollution and noncommunicable diseases. Bull World Health Organ. 2019;97(2):160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Clarke LE, Jiang K, Akimoto K, et al. Assessing Transformation Pathways. In: Climate Change 2014: Mitigation of Climate Change. Contribution of Working Group III to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change. Pacific Northwest National Lab. (PNNL), Richland, WA (United States); 2015. [Google Scholar]
- 18. World Health Organization . Burden of disease from the joint effects of household and ambient air pollution for 2016. Social and Environmental Determinants of Health Department: Geneva, Switzerland. 2016;2018:7. [Google Scholar]
- 19. Kabir ER, Rahman MS, Rahman I. A review on endocrine disruptors and their possible impacts on human health. Environ Toxicol Pharmacol. 2015;40(1):241‐258. [DOI] [PubMed] [Google Scholar]
- 20. Foley TP Jr, Límanová Z, Potluková E. Medical consequences of Chernobyl with focus on the endocrine system: Part 1. Casopis lekaru ceskych. 2015;154(5):227‐231. [PubMed] [Google Scholar]
- 21. Foley TP, Límanová Z, Potluková E. Medical Consequences of Chernobyl with Focus on the Endocrine System‐Part 2. Casopis lekaru ceskych. 2015;154(6):287‐291. [PubMed] [Google Scholar]
- 22. Sathish T, Kapoor N, Cao Y, Tapp RJ, Zimmet P. Proportion of newly diagnosed diabetes in COVID‐19 patients: a systematic review and meta‐analysis. Diabetes Obes Metab. 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. World Health Organization . Ambient (outdoor) air quality and health. Fact sheet. WHO. 2018.
- 24. Nepal Health Research Council . MEOR Burden of disease 2017: a country report based on the global burden of disease 2017 study. Kathmandu, Nepal Nepal health research Council (NHRC). Ministry of health and population (MoHP) and monitoring evaluation and operational research (MEOR Nepal, 2019[Google Scholar].
- 25. Nepal Health Research Council . Population Based Prevalence of Selected Non‐Communicable Diseases in Nepal. Kathmandu: Nepal Health Research Council, Government of Nepal; 2019. [DOI] [PubMed] [Google Scholar]
- 26. Dhimal M, Karki KB, Sharma SK, et al. Prevalence of selected chronic non‐communicable diseases in Nepal. Journal of Nepal Health Research Council. 2019;17(3):394‐401. [DOI] [PubMed] [Google Scholar]
- 27. Dhimal M, Bista B, Bhattarai S, et al. Report of Non Communicable Disease Risk Factors: STEPS Survey Nepal 2019. Kathmandu: Nepal Health Research Council; 2020. [Google Scholar]
- 28. Jha AK, Chapagain S, Dhimal M, et al. Population Based Cancer Registries at Kathmandu, Bhaktapur, Lalitpur, Siraha, Saptari, Dhanusha, Mohattari, West Rukum and East Rukum Districts, Nepal, 2018. Government of Nepal: Nepal Health Research Council; 2020. [Google Scholar]
- 29. Government of Nepal and the World Health Organization . Multisectoral Action Plan for the Prevention and Control of Non Communicable Diseases (2014–2020).
- 30. Karagulian F, Belis CA, Dora CFC, et al. Contributions to cities’ ambient particulate matter (PM): A systematic review of local source contributions at global level. Atmos Environ. 2015;120:475‐483. [Google Scholar]
- 31. Arku RE, Brauer M, Ahmed SH, et al. Long‐term exposure to outdoor and household air pollution and blood pressure in the Prospective Urban and Rural Epidemiological (PURE) study. Environ Pollut. 2020;114197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Bowe B, Artimovich E, Xie Y, Yan Y, Cai M, Al‐Aly Z. The global and national burden of chronic kidney disease attributable to ambient fine particulate matter air pollution: a modelling study. BMJ Global Health. 2020;5(3):e002063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. He D, Wu S, Zhao H, et al. Association between particulate matter 2.5 and diabetes mellitus: A meta‐analysis of cohort studies. Journal of diabetes investigation. 2017;8(5):687‐696. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Bowe B, Xie Y, Li T, Yan Y, Xian H, Al‐Aly Z. The 2016 global and national burden of diabetes mellitus attributable to PM2· 5 air pollution. The Lancet Planetary Health. 2018;2(7):e301‐e312. [DOI] [PubMed] [Google Scholar]
- 35. Manisalidis I, Stavropoulou E, Stavropoulos A, Bezirtzoglou E. Environmental and health impacts of air pollution: A review. Frontiers in public health; 2020:8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Jiang X‐Q, Mei X‐D, Feng D. Air pollution and chronic airway diseases: what should people know and do? J Thorac Dis. 2016;8(1):E31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Li L, Yang A, He X, et al. Indoor air pollution from solid fuels and hypertension: A systematic review and meta‐analysis. Environ Pollut. 2020;259(113914):7. [DOI] [PubMed] [Google Scholar]
- 38. Yamamoto SS, Yacyshyn E, Jhangri GS, Chopra A, Parmar D, Jones CA. Household air pollution and arthritis in low‐and middle‐income countries: Cross‐sectional evidence from the World Health Organization’s study on Global Ageing and Adult Health. PLoS One. 2019;14(12):e0226738. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Azarpazhooh MR, Morovatdar N, Avan A, et al. Covid‐19 pandemic and burden of non‐communicable diseases: An ecological study on data of 185 countries. Journal of Stroke and Cerebrovascular Diseases. 2020;29(9):105089. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. World Health Organization . The impact of the COVID‐19 pandemic on noncommunicable disease resources and services: results of a rapid assessment. 2020.
- 41. Pal R, Bhadada SK. COVID‐19 and non‐communicable diseases. Postgrad Med J. 2020;96(1137):429‐430. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Daiber A, Lelieveld J, Steven S, et al. The “exposome” concept–how environmental risk factors influence cardiovascular health. Acta Biochim Pol. 2019;66(3):269‐283. [DOI] [PubMed] [Google Scholar]
- 43. Pradhan B, Kjellstrom T, Atar D, et al. Heat stress impacts on cardiac mortality in Nepali migrant workers in Qatar. Cardiology. 2019;143(1):37‐48. [DOI] [PubMed] [Google Scholar]
- 44. Glaser J, Lemery J, Rajagopalan B, et al. Climate change and the emergent epidemic of CKD from heat stress in rural communities: the case for heat stress nephropathy. Clin J Am Soc Nephrol. 2016;11(8):1472‐1483. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Khaniabadi YO, Hopke PK, Goudarzi G, Daryanoosh SM, Jourvand M, Basiri H. Cardiopulmonary mortality and COPD attributed to ambient ozone. Environ Res. 2017;152:336‐341. [DOI] [PubMed] [Google Scholar]
- 46. Ahmed S, Hasan MZ, Pongsiri MJ, Ahmed MW, Szabo S. Effect of extreme weather events on injury, disability, and death in Bangladesh. Climate Dev. 2020;1–12. [Google Scholar]
- 47. Silva JF, Mattos IE, Luz LL, Carmo CN, Aydos RD. Exposure to pesticides and prostate cancer: systematic review of the literature. Rev Environ Health. 2016;31(3):311‐327. [DOI] [PubMed] [Google Scholar]
- 48. Han MA, Kim JH, Song HS. Persistent organic pollutants, pesticides, and the risk of thyroid cancer: systematic review and meta‐analysis. Eur J Cancer Prev. 2019;28(4):344‐349. [DOI] [PubMed] [Google Scholar]
- 49. Pearce N. Classification of epidemiological study designs. Int J Epidemiol. 2012;41(2):393‐397. [DOI] [PubMed] [Google Scholar]
- 50. Morgenstern H. Ecologic studies in epidemiology: concepts, principles, and methods. Annu Rev Public Health. 1995;16(1):61‐81. [DOI] [PubMed] [Google Scholar]
- 51. Greenland S, Robins J, Piantadosi S, Cohen B. Ecologic studies‐biases, misconceptions, and counterexamples. Invited commentaries. Authors replies. Am J Epidemiol. 1994;139(8):747‐771. [DOI] [PubMed] [Google Scholar]
- 52. Stroup DF, Berlin JA, Morton SC, et al. Meta‐analysis of observational studies in epidemiology: a proposal for reporting. JAMA. 2000;283(15):2008‐2012. [DOI] [PubMed] [Google Scholar]
- 53. Nuckols JR, Ward MH, Jarup L. Using geographic information systems for exposure assessment in environmental epidemiology studies. Environ Health Perspect. 2004;112(9):1007‐1015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Blangiardo M, Boulieri A, Diggle P, Piel FB, Shaddick G, Elliott P. Advances in spatiotemporal models for non‐communicable disease surveillance. Int J Epidemiol. 2020;49(Supplement_1):i26‐i37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. NCD Risk Factor Collaboration . Rising rural body‐mass index is the main driver of the global obesity epidemic in adults. Nature. 2019;569(7755):260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Double Burden of Malnutrition Collaborators . Mapping local patterns of childhood overweight and wasting in low‐and middle‐income countries between 2000 and 2017. Nat Med. 2020;26(5):750. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57. Taddei C, Zhou B, Bixby H, et al. Repositioning of the global epicentre of non‐optimal cholesterol. Nature. 2020;582:73‐77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58. Brauer M, Freedman G, Frostad J, et al. Ambient air pollution exposure estimation for the global burden of disease 2013. Environ Sci Technol. 2016;50(1):79‐88. [DOI] [PubMed] [Google Scholar]
- 59. Burnett RT, Pope CA, Ezzati M, et al. An integrated risk function for estimating the global burden of disease attributable to ambient fine particulate matter exposure. Environ Health Perspect. 2014;122(4):397‐403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60. Fewtrell L, Kaufman R, Prüss‐Üstün A. Lead: assessing the environmental burden of diseases at national and local levels. Geneva. 2003. [Google Scholar]
- 61. Fewtrell L, Prüss‐Üstün A, Landrigan P, Ayuso‐Mateos J. Estimating the global burden of disease of mild mental retardation and cardiovascular diseases from environmental lead exposure. Environ Res. 2004;94(2):120‐133. [DOI] [PubMed] [Google Scholar]
- 62. Dhimal M. Climate change and health: research challenges in vulnerable mountainous countries like Nepal. Global Forum for Health Research. 2008. [Google Scholar]
- 63. Jia P, Stein A, James P, et al. Earth observation: investigating noncommunicable diseases from space. Annu Rev Public Health. 2019;40:85‐104. [DOI] [PubMed] [Google Scholar]
- 64. Campbell‐Lendrum DH, Woodruff R, Prüss‐Üstün A, Corvalán CF, Organization WH. Climate change: quantifying the health impact at national and local levels: World Health. Organization. 2007. [Google Scholar]
- 65. Chen K, Horton RM, Bader DA, et al. Impact of climate change on heat‐related mortality in Jiangsu Province, China. Environ Pollut. 2017;224:317‐325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66. Kinney PL, O’Neill MS, Bell ML, Schwartz J. Approaches for estimating effects of climate change on heat‐related deaths: challenges and opportunities. Environ Sci Policy. 2008;11(1):87‐96. [Google Scholar]
- 67. Luber G, McGeehin M. Climate change and extreme heat events. Am J Prev Med. 2008;35(5):429‐435. [DOI] [PubMed] [Google Scholar]
- 68. Figueres C, Landrigan PJ, Fuller R. Tackling air pollution, climate change, and NCDs: time to pull together. Lancet. 2018;392(10157):1502‐1503. [DOI] [PubMed] [Google Scholar]
- 69. Ward B, Bowen A. An analysis of the Trump Administration’s economic and policy arguments for withdrawal of the United States from the Paris Agreement on climate change. 2020.
- 70. Honda Y, Kondo M, McGregor G, et al. Heat‐related mortality risk model for climate change impact projection. Environ Health Prev Med. 2014;19(1):56‐63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71. Huang C, Barnett AG, Wang X, Vaneckova P, FitzGerald G, Tong S. Projecting future heat‐related mortality under climate change scenarios: a systematic review. Environ Health Perspect. 2011;119(12):1681‐1690. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72. Guo Y, Li S, Li Liu D, Chen D, Williams G, Tong S. Projecting future temperature‐related mortality in three largest Australian cities. Environ Pollut. 2016;208:66‐73. [DOI] [PubMed] [Google Scholar]
- 73. Zhang B, Li G, Ma Y, Pan X. Projection of temperature‐related mortality due to cardiovascular disease in Beijing under different climate change, population, and adaptation scenarios. Environ Res. 2018;162:152‐159. [DOI] [PubMed] [Google Scholar]
- 74. Scheelbeek PF, Tuomisto HL, Bird FA, Haines A, Dangour AD. Effect of environmental change on yield and quality of fruits and vegetables: two systematic reviews and projections of possible health effects. The Lancet Global Health. 2017;5:S21. [Google Scholar]
- 75. Dhimal M, Shrestha R. Global Burden of Disease, Air Pollution and COVID‐19. Kathmandu University Medical Journal. 2020;18(71):214–216. [PubMed] [Google Scholar]