

Abstract
Supplemental Digital Content is available in the text.
A 51-year-old female with a history of hypertension and tobacco use was admitted to our unit due to recent onset of fever (38.5°C), cough, and respiratory distress. SARS-CoV-2 infection was confirmed by real-time polymerase chain reaction (RT-PCR) assays performed on nasopharyngeal swabs. We administered oxygen via a high-flow-nasal-cannula, ribavirin/interferon beta-1b, low-dose dexamethasone, and prophylactic anticoagulation (enoxaparin 40 mg subcutaneously twice daily). On day-3, the patient developed precordial chest pain after intense cough. Electrocardiography revealed normal sinus rhythm and mild ST-segment elevation/biphasic T waves in precordial leads V2 and V3. Cardiac enzymes (including troponin-I <0.01 ng/ml) and echocardiography were inconclusive for myocardial ischemia. However, coronary angiography depicted a type-two (diffuse smooth stenosis) spontaneous coronary artery dissection (SCAD) at the distal left anterior descending (LAD) artery (Fig. 1a, Supplemental Video1, Supplemental digital content 1, http://links.lww.com/MCA/A404).
Fig. 1.
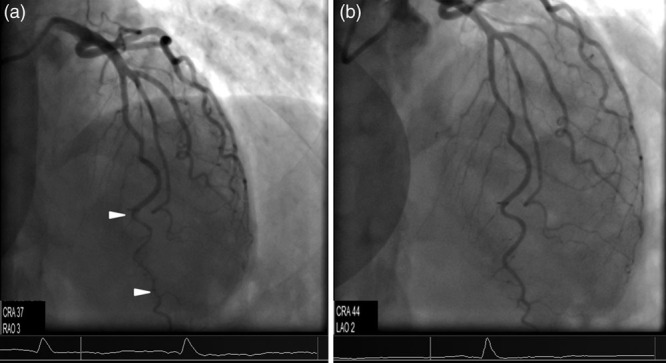
(a) A cranial (37°) coronary angiographic view illustrating a typical type-two coronary artery dissection at the distal left anterior descending artery (region between the two arrowheads). (b) Follow-up coronary angiography [projection approximately same to (a)] demonstrating total restoration of the patency of the affected vessel. CRA, cranial; LAO, left anterior oblique.
The patient had a single-vessel SCAD and no signs of refractory ischemia or hemodynamic instability. Hence, conservative treatment integrating dual antiplatelet, anticoagulation, and statin therapy was administered based on current recommendations [1]. Chest pain was relieved, while no ischemic or other complications occurred. RT-PCR test for COVID-19 was negative on day-18, and the patient was discharged to home isolation. Coronary angiography after 1 month (Fig. 1b, Supplemental Video2, Supplemental digital content 2, http://links.lww.com/MCA/A405) showed restored LAD anatomy and patency.
Scarce data exist regarding the pathogenesis and treatment of SCAD in COVID-19 [2]. In our patient, no conditions associated with the development of SCAD (i.e., fibromuscular dysplasia, hormonal therapy, systemic inflammatory disease, or connective tissue disorder) were identified [1]. However, COVID-19-associated thromboinflammation might have been implicated in the pathobiology of SCAD [3]. In addition, the role of intense cough as a precipitating factor in the development of SCAD was clearly highlighted in our COVID-19 patient [1].
Acknowledgements
IRB information: The study was approved by the Institutional Review Board of King Saud Medical City, Riyadh, Saudi Arabia [H-01-R-053, IORG0010374, H1RI-22-20-03]. Written informed consent was obtained from the patient.
Conflicts of interest
There are no conflicts of interest.
Footnotes
Supplemental Digital Content is available for this article. Direct URL citations appear in the printed text and are provided in the HTML and PDF versions of this article on the journal's website, www.coronary-artery.com.
References
- 1.Hayes SN, Kim ESH, Saw J, Adlam D, Arslanian-Engoren C, Economy KE, et al. ; American Heart Association Council on Peripheral Vascular Disease; Council on Clinical Cardiology; Council on Cardiovascular and Stroke Nursing; Council on Genomic and Precision Medicine; and Stroke Council. Spontaneous coronary artery dissection: current state of the science: a scientific statement from the American heart association. Circulation. 2018; 137:e523–e557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Courand PY, Harbaoui B, Bonnet M, Lantelme P. Spontaneous coronary artery dissection in a patient with COVID-19. JACC Cardiovasc Interv. 2020; 13:e107–e108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Price LC, McCabe C, Garfield B, Wort SJ. Thrombosis and COVID-19 pneumonia: the clot thickens! EurRespir J. 2020; 56:2001608. [DOI] [PMC free article] [PubMed] [Google Scholar]