

Abstract
This study proposes that visa status is an important construct that is central to understanding how health selection occurs among immigrants. We used the 2017 baseline survey data of the Health of Philippine Emigrants Study (n = 1,632) to compare the health of nonmigrants remaining in the Philippines and migrants surveyed prior to migration to the United States. Furthermore, we compared migrant health by visa type: limited family reunification, unlimited family reunification, fiancé(e)/marriage, and employment. Migrants reported fewer health conditions than nonmigrants overall. However, health varied among migrants by visa type. Migrants with fiancé(e)/marriage visas were the healthiest, reporting significantly fewer health conditions than the other groups. Limited family reunification migrants reported more health conditions than nonmigrants and unlimited family reunification migrants. We discuss how the immigration visa process reflects broader forms of social and political stratification that cause heterogeneity in immigrant health selection.
Keywords: health selection, immigrant visas, immigrants, Philippines, social stratification
Immigrants tend to be healthier than their nonimmigrant counterparts in the United States—a trend often referred to as the immigrant health advantage (Abraído-Lanza et al. 1999; Acevedo-Garcia and Bates 2008; Markides and Coreil 1986; Palloni and Arias 2004). One explanation for this phenomenon is that healthier individuals select into migrant cohorts (Akresh and Frank 2008; Hamilton, Palermo, and Green 2015; Ro, Fleischer, and Blebu 2016). Evidence supports this selective migration hypothesis, showing that health selection is stronger in migrant cohorts comprised of individuals with higher socioeconomic status (Akresh and Frank 2008; Riosmena, Kuhn, and Jochem 2017). However, a health advantage is also often observed among migrants with lower socioeconomic status (Martinez, Aguayo-Tellez, and Rangel-Gonzalez 2015; Riosmena et al. 2017). Although selection on socioeconomic status is important, it does not fully capture how migrant health selection occurs. Most literature on health selection focuses on immigrants after arrival in a receiving country, although selection begins prior to departure from their home country (Jasso et al. 2005; Téllez, Martínez, and González 2015). Furthermore, much theorizing about migrant health selection emphasizes intrapersonal factors (e.g., motivation, personality, etc.; Dhadda and Greene 2018; Hamilton et al. 2015). Although migrants indeed have a great deal of individual agency (Gong et al. 2011), the ways people migrate are shaped by institutional constraints in both sending and receiving countries (Gee and Ford 2011; Viruell-Fuentes, Miranda, and Abdulrahim 2012).
U.S. immigration policies have the potential to stratify migrants before they step foot on U.S. soil (Jasso 2011; Kato and Sparber 2011; Massey and Taylor 2004). The United States uses immigration visas as a mechanism to limit and control the number and type of people allowed to legally immigrate (U.S. Department of State 2020). The process of applying for and obtaining a U.S. immigration visa creates a system of social stratification abroad that can directly and indirectly influence health differences among people who ultimately obtain visas as well as between migrants and nonmigrants (Jasso 2011, 2016). Migrants may be stratified by their visa type—whether they hold family reunification visas, fiancé(e)/marriage visas, employment visas, and so on—as a consequence of the different kinds of resources needed to secure each specific visa type. For example, for employment visas, applicants with high levels of education are prioritized for entry (U.S. Department of State 2020). Certain visa types are more difficult to obtain because U.S. immigration policy restricts quantity for some (e.g., employment visas) but not for others (e.g., marriage visas; Jasso 2011). Administrative prioritization and backlog can cause some visa application processes to take years, even decades, to complete, whereas other types of visa applications are approved within months (Obinna 2014). These factors can lead to differential experience of stress associated with being in the process of applying for an immigration visa, which can ultimately impact the health status of prospective migrants (Jasso 2011; Jasso et al. 2005). Accordingly, this study considers how visa type stratification reveals heterogeneity in health selection prior to migration.
How immigrant health selection varies by visa status prior to migration is important because if true, it illustrates how U.S. immigration policies influence the circumstances under which people navigate migration, which then shapes health selection of migrants. Although scholars have suggested this might be the case (Akresh and Frank 2008; Jasso et al. 2005; Ro et al. 2016), there is a dearth of empirical research on visas and health. This study investigates how visa status reflects prior life chances and existing resources pertinent to health and just as importantly, examines health prior to migration. Prior research on health selection has conventionally focused on the migrant health trajectory starting with arrival and recognizes declines in the migrant health advantage with greater integration into U.S. society (Gorman, Read, and Krueger 2010; Gubernskaya, Bean, and Van Hook 2013; Hamilton et al. 2015). One study that assessed premigration health using the Mexican Family Life Survey found little evidence of health selection occurring (Rubalcava et al. 2008), although this finding could be due to the lower costs of migration from Mexico to the United States given geographic proximity (Akresh and Frank 2008; Jasso et al. 2004).
In the present study, we analyzed premigration baseline data from the Health of Philippine Emigrants Study (Gee et al. 2018), which compares Filipino migrants destined to the United States with peers who remain in the Philippines, to test migrant health selection and make comparisons by visa type.
BACKGROUND
The Philippine–U.S. Migration Context
The United States is home to the largest number of Filipinos outside of the Philippines. It is important to consider the history of colonization and militarization as context for current migration from the Philippines to the United States. With the annexation of the Philippines by the United States in the late nineteenth century after the Spanish-American War, Filipinos became U.S. nationals and began immigrating in larger numbers, primarily working in low-wage agricultural jobs in the western United States (Le Espiritu and Wolf 2001). The United States took over Spanish naval bases in the Philippines, building its own military presence and leading many Filipinos to work on or around the bases or to serve in the U.S. military (Rodriguez 2010). Since the 1940s, many Filipinos migrated to the United States as agricultural workers, war brides of U.S. servicemen, or health care workers (Lichter, Qian, and Tumin 2015; Liu, Ong, and Rosenstein 1991). Although the Philippines was granted independence in 1944, ties between the United States and Philippine government, military, economy, and education have continued (Boquet 2017).
Philippine emigration to the United States grew in the 1960s with the lifting of national-origin quotas under the 1965 U.S. Immigration Act. Today, 1.9 million Filipinos (accounting for 4% of the U.S. immigrant population) reside in the United States (Zong and Batalova 2018). Filipinos are the third fastest growing immigrant group in the United States, after Chinese and Asian Indians. Current policies in the Philippines promote migration abroad as emigrants typically send remittances that, to date, comprise 11% of the Philippine economy (Zong and Batalova 2018). Migrants are routinely hailed as “New National Heroes,” highlighting their economic importance for the Philippines (Rodriguez 2002).
Employment is a primary channel for migration from the Philippines to the United States. Low wages and few job opportunities in the Philippines combined with health care workforce shortages in other countries create incentives to educate and train health care professionals for export (Boquet 2017; Castro-Palaganas et al. 2017). Migration for family reunification purposes is also common (Medina and Natividad 2012). The long history of migration means that many in the Philippines have family members already living in the United States who can petition for them to immigrate. An under-studied but common means of migration to the United States from the Philippines is through marrying a U.S. citizen. This group of migrants are mostly Filipina women who marry non-Hispanic white men (Kim 2010; Lichter et al. 2015). U.S. military bases in the Philippines have led to many intimate relationships between American servicemen and Filipinas, some resulting in international marriage (Reyes 2017). The Philippines is also popular among U.S. civilian men seeking to marry Asian women. Historically, the Philippines has had a high proportion of mail order brides (Lloyd 2000), a practice that continues today via internet-based dating websites (Tran 2012).
Histories of migration, colonization, militarization, and economic prospect serve as the backdrop against which selective migration occurs. Individuals may make personal decisions about migration, but they are profoundly shaped by historical and sociopolitical forces.
Visa Type and Health Selection
We propose that migrant visa type is a marker of the life chances, resources, and experiences that influence health selection into migration (Jasso 2011, 2016). The process of obtaining a migrant visa may directly select for better health. For example, the United States mandates a medical screening and vaccination for certain illnesses prior to issuing a visa. Some health problems preclude admission (e.g., history of substance abuse), whereas others might be admissible after treatment (e.g., tuberculosis; U.S. Department of State 2020). The process of obtaining a migrant visa may also indirectly select for better health. U.S. Congress places various limits and requirements on who is eligible to apply for visas and how many visas are allocated each year.
Given these market conditions, with more people wanting to migrate than the United States allows, it is likely that only those who are most well resourced are successful in obtaining a visa. Personal resources and traits may be associated with better health among visa holders than those without a visa. Beyond the distinction between those who can obtain a visa (i.e., lawful permanent residents) versus those who cannot or who choose not to seek them (i.e., nonmigrants), the different requirements and restrictions placed on each type of visa can lead to health stratification by specific visa type. In this study, we consider four categories of visas: (1) numerically limited family reunification, (2) numerically unlimited family reunification, (3) fiancé(e)/marriage family reunification, and (4) employment.
First, we consider a broad category of immigration visas—family reunification visas. These visas are obtained through the U.S. Citizenship and Immigration Services (USCIS) and may be numerically unlimited or numerically limited (Jasso 2011; U.S. Department of State 2020). Numerically unlimited visas have no maximum number of legal permanent residents allowed in those categories, whereas numerically limited visas are those categories where the number of visas granted annually is capped by the State Department.
USCIS gives the highest priority to spouses (married longer than two years), unmarried children (under the age of 21), and parents (21 years or older) of U.S. citizens (U.S. Department of State 2020). These visas are numerically unlimited and require sponsorship from the U.S. citizen relation. This group has the closest existing relation to a U.S. citizen. After showing proof of relation, the process of obtaining a numerically unlimited family visa is relatively quick and straightforward, perhaps lowering visa stress and protecting health (Jasso 2011). On the other hand, numerically limited family reunification migrants include family members with less direct ties to U.S. citizens and family members of lawful permanent residents. Examples include children of U.S. citizens over the age of 21, married children of U.S. citizens and their children, and spouses and children of lawful permanent residents (U.S. Department of State 2020). Due to the numerical limitations placed on these visas, applicants may wait years until a visa becomes available in order to migrate (Jasso 2011). Longer wait times might mean greater experience of visa stress prior to migration, leading to worse health.
There is a special subset of family reunification visa holders that we treat as distinct from the others discussed previously: fiancé(e)s of U.S. citizens or spouses of U.S. citizens who have been married less than two years. These visas are considered “conditional,” meaning that fiancé(e)/marriage visa holders must apply for the conditional status to be removed once living in the United States (U.S. Department of State 2020). For fiancé(e) visas, the couple must marry and apply to have the condition removed within 90 days of the fiancé(e)’s arrival in the United States. For couples married prior to the immigrant spouse’s arrival in the United States, the couple must apply to remove the condition within 90 days of the two-year anniversary of the migrant spouse’s arrival. Although these visas are conditional, they are also numerically unlimited. Therefore, once the U.S. citizen fiancé(e)/spouse agrees to sponsor their partner, the visa is approved quickly. These fiancé(e)/marriage visa holders may have less exposure to premigration visa stress due to fast processing, although they may still experience visa stress until their conditional status is removed once in the United States (Jasso 2011). People who are selected as fiancé(e)/marriage migrants from the Philippines are likely to be younger, female, more English proficient, and more friendly toward non-Filipinos (Lloyd 2000), which may indirectly select for better health. Additionally, a person in visibly poor health is theoretically unlikely to be successful on the international marriage market.
The last group we consider are migrants with employment visas. These visas require an employer or agent sponsor in the United States and approval through the U.S. Department of Labor. All employment visas considered in this study are numerically limited. Within the employment visa category, people with advanced degrees are prioritized for entry, followed by skilled professionals who fill certain labor needs in the United States (U.S. Department of State 2020). Employment visa holders allow the inclusion of spouses and children of the principal person applying for employment in the United States. These are not considered family reunification visas because these visas depend on the spouse or parent gaining approval for lawful permanent residency to work. Much of the past literature on the initiation of migration has focused on employment migrants (Yang 2010), emphasizing differences in labor supply, labor demand, and wages between countries as underlying causes of migration (Lindstrom and López Ramírez 2010; McKenzie, Theoharides, and Yang 2014). In theory, people migrating for work should be in good health to be employable in the United States because they need be able to perform job duties and demands (Rodriguez 2010). Employment migrants who are prioritized to receive a visa because of their advanced degrees demonstrate high educational attainment, which is associated with better health (Mirowsky and Ross 2015). Nevertheless, it may take years of planning for potential employment migrants to obtain a U.S.-based employer sponsor to petition on their behalf, and it may take additional years of waiting for their visas to be approved. This may increase visa stress and lessen health selection.
Research Aims
The aforementioned considerations motivate our study aims to:
categorize and compare visa types among lawful Filipino migrants, describing them regarding type of sponsorship needed, preference level established by the United States, and mean processing time;
determine whether lawful Filipino migrants have a health advantage over nonmigrants remaining in the Philippines prior to emigration to the United States and whether personal characteristics or resources related to health account for this difference;
calculate differences in health by visa type, comparing nonmigrants with limited family reunification, unlimited family reunification, fiancé(e)/marriage, and employment visa holders; and determine whether personal characteristics or resources account for differences in health.
Personal characteristics include those factors migrants might be selected on that are also related to health, including age, gender, English proficiency, region of residence, and access to health care. Personal resources are those that migrants might utilize in order to gain access to a visa and include educational attainment and (lack of) financial strain.
METHODS
Data and Sample
We used data from the Health of Philippine Emigrants Study (HoPES; Gee et al. 2018). HoPES is uniquely structured to examine migration by including a cohort of U.S.-bound migrants (n = 832) from the Philippines and a comparison cohort of nonmigrants (n = 805) who do not have intentions to leave the Philippines. Importantly, HoPES captures baseline data from migrants prior to migration. Participants were recruited from February to October 2017 and will be followed annually until 2020.
Migrants were identified through a partnership with the Commission on Filipinos Overseas, the Philippine federal agency that governs emigration. After Filipinos have clearances to migrate to the United States, they must attend a mandatory predeparture orientation seminar (PDOS) in the cities of Cebu or Manila. Once migrants complete the PDOS, they receive a stamp on their passport. Airport officials prohibit migrants without this stamp to board airline flights departing the Philippines. Thus, the PDOS is the last administrative legal task migrants must undertake before they exit the country. HoPES researchers recruited study participants from people attending the PDOS, allowing for a rare opportunity to sample from the entire universe of lawful permanent migrants bound for the United States. Migrant baseline data were collected within weeks or even days prior to departure to the United States. HoPES migrants are fairly representative of recent (less than two years duration) Filipino immigrants to the United States, as seen in comparisons with American Community Survey (ACS) data (Gee et al. 2018).
Nonmigrants were identified through stratified random sampling of households, with three strata including Metro Manila, Metro Cebu-urban, and Metro Cebu-rural. One person from each household was recruited. Nonmigrants were sampled to match the migrant cohort distribution for age, gender, and education level and are therefore comparable to migrants on these key factors but different in their migration status. One inclusion criterion for the nonmigrant cohort was intention to remain in the Philippines for the next three years.
The present analyses utilized HoPES baseline data for migrants and nonmigrants. The response rates were 36.5% for migrants and 68.6% for nonmigrants (de Castro et al. 2019). A total of 1,637 migrants and nonmigrants completed the baseline assessment in English, Tagalog, or Cebuano. Of these, 1,632 participants had complete data for all variables of interest (<1% missing), and thus, analyses proceeded with complete cases only. Using ACS 2011–2013 data, weights for both migrant and nonmigrant samples were created that adjust the entire sample to be representative of recent Filipino migrants to the United States on age, gender, and education. Using these weights allows for generalizations to be made about the population of Filipino migrants to the United States using the HoPES sample.
Dependent Variable
The main dependent variable was number of health conditions. Participants reported whether they ever had any of the following 10 problems: arthritis/gout/rheumatism, anemia, asthma, cancer, diabetes, high blood pressure, heart disease, hypercholester-olemia, infection from an intestinal parasite, and influenza. These conditions were summed (range 0–10). This measure, adopted from the Medical Outcomes Study, is often used in research as a summary indicator of physical well-being and has been used in prior studies of immigrant health (Gorman et al. 2010; Yoo, Gee, and Takeuchi 2009).
Independent Variables
First, we compared HoPES participants by migrant status—whether participants were in the nonmigrant sample or in the migrant sample. Among migrants, visa type was obtained by asking them to provide the specific visa codes (e.g., IR1, E31) from their documents. These visa codes were then collapsed into the following categories: (1) numerically limited family reunification visa, (2) numerically unlimited family reunification visa, (3) fiancé(e)/marriage visa, or (4) employment visa. Nonmigrants were the reference category in most analyses.
To address Research Aim 1, Table 1 provides detailed information about the visa codes and how they were categorized. Descriptions and details for each visa code were taken from the USCIS website, U.S. Department of State Travel website, and U.S. Department of State Visa Bulletin (U.S. Department of State 2020). For each visa code, we indicate whether the visa holder is a principal (i.e., primary applicant) or derivative (i.e., person receives lawful status through the principal applicant’s status), whether an affidavit of support (i.e., signed contract by U.S.-based sponsor to financially support the intending immigrant) is required, the level of preference for numerically limited visas, and the percentage and frequency in the HoPES migrant sample. We also include a rough estimate of the amount of time it took for the visa to be processed, from the time the applicants filed their last paperwork until they were legally able to migrate. We used the Visa Bulletins for the fiscal year 2017—the year HoPES migrants were recruited—which provides the earliest filing date (i.e., the “date of final action”) for when visa applications are currently being processed for each visa code for a given month (U.S. Department of State 2020). We calculated the visa processing time in years by finding the difference between the year of each migrant’s date of HoPES survey interview and the corresponding year in the date of final action from the given month in the 2017 Visa Bulletin. For example, if a migrant with an F4 visa interviewed for HoPES in March 2017, his or her corresponding date of final action would be August 1, 1993, an approximate processing time of 24 years (i.e., 2017 – 1993). Fiancé(e)/marriage migrants and numerically unlimited family reunification migrants had processing times of zero years because these visas are not subject to numerical limitations.
Table 1.
Types of U.S. Visas Categorized into Limited Family Reunification, Unlimited Family Reunification, Fiancé(e)/Marriage, and Employment, Health of Philippine Emigrants Study at Baseline, Migrants Only (n = 831).
| Visa Category | Visa Code | Description of Visa | Numerically Limited? (Yes/No) | Preference Level | Principal or Derivative | Affidavit of Support Needed? (Yes/No/Maybe) | %of Category in HoPES (n) | Estimated Visa Processing Time, in Years (SE) |
|---|---|---|---|---|---|---|---|---|
| Limited family reunification (n = 362) | ||||||||
| F1 | Unmarried child of U.S. citizen | Yes | 1st | Principal | Yes | 1.4 (5) | 18.6 (2.9) | |
| F11 | Certain family member of U.S. citizens | Yes | 1st | Principal | Yes | 7.5 (27) | 13.0 (.9) | |
| F12 | Child of noncitizen classified F11 | Yes | 1st | Principal | Yes | 3.6 (13) | 14.1 (1.5) | |
| F2A/F2 | Certain family members of LPR | Yes | 2nd | Principal | Yes | 13.5 (49) | 2.2 (.2) | |
| F2B | Certain family members of LPR | Yes | 2nd | Principal | Yes | 14.4 (52) | 10.9 (.1) | |
| F21 | Spouse of LPR | Yes | 2nd | Principal | Yes | 3.9 (14) | 2.0 (0) | |
| F22 | Child of LPR | Yes | 2nd | Principal | Yes | 3.0 (11) | 7.0 (1.4) | |
| F22A | Child of LPR | Yes | 2nd | Principal | Yes | .3 (1) | 2.0 (0) | |
| F23 | Child of F21 or F22 | Yes | 2nd | Derivative | Yes | .3 (1) | 11.0 (0) | |
| F24/F2B | Unmarried son/daughter of LPR | Yes | 2nd | Principal | Yes | 14.6 (53) | 10.9 (0) | |
| F25 | Child of F24 | Yes | 2nd | Derivative | Yes | 2.2 (8) | 6.7 (1.6) | |
| FX1a | Spouse of LPR, new arrival | Yes | 2nd | Derivative | Yes | 11.3 (41) | 24.0 (0) | |
| FX2a | Child of LPR, new arrival | Yes | 2nd | Derivative | Yes | 3.0 (11) | 23.0 (.9) | |
| FX3a | Child of FX1 or FX2 | Yes | 2nd | Derivative | Yes | .3 (1) | 24.0 (0) | |
| F3 | Married sons and daughters of U.S. citizens and their spouses and minor children | Yes | 3rd | Principal | Yes | 2.2 (8) | 23.0 (0) | |
| F31 | Married child of U.S. citizen | Yes | 3rd | Principal | Yes | 1.7 (6) | 22.6 (.2) | |
| F32 | Spouse of F31 | Yes | 3rd | Derivative | Yes | 1.4 (5) | 22.6 (.2) | |
| F33 | Child of F31 | Yes | 3rd | Derivative | Yes | 2.2 (8) | 22.9 (.1) | |
| F4 | Brother or sister of U.S. citizens and their spouses and minor children | Yes | 4th | Principal | Yes | 2.8 (10) | 23.7 (.1) | |
| F41/PS | Brother/sister of U.S. citizen, new arrival | Yes | 4th | Principal | Yes | 6.4 (23) | 23.3 (.1) | |
| F42 | Spouse of F41 | Yes | 4th | Derivative | Yes | 1.9 (7) | 23.3 (.2) | |
| F43 | Child of F41 | Yes | 4th | Derivative | Yes | 1.9 (7) | 23.7 (.2) | |
| SE3 | Child of employee of U.S. government abroad | Yes | 4th | Derivative | .3 (1) | 23.0 (0) | ||
| Unlimited family reunification (n = 175) | ||||||||
| AM2 | Spouse/child of AM1 or AM6b | No | N/A | Derivative | Yes | 1.1 (2) | 0 (0) | |
| CR2 | Child of U.S. citizen | No | N/A | Principal | Yes | 1.1 (2) | 0 (0) | |
| K-2 | Child of a K-1 visa holder | No | N/A | Derivative | No | 4.0 (7) | 0 (0) | |
| IB3 | Child of IB-1 (self-petition spouse of U.S. citizen) | No | N/A | Principal | No | .6 (1) | 0 (0) | |
| IR-1 | Spouse of U.S. citizen | No | N/A | Principal | Yes | 13.7 (24) | 0 (0) | |
| IR-2 | Unmarried child of U.S. citizen, under 21 years of age | No | N/A | Principal | Yes | 31.4 (55) | 0 (0) | |
| IR-4 | Orphan to be adopted in the U.S. by a U.S. citizen | No | N/A | Principal | No | .6 (1) | 0 (0) | |
| IR-S | Parent of adult U.S. citizen, new arrival | No | N/A | Principal | Yes | 46.9 (82) | 0 (0) | |
| IWI | Certain spouses of deceased U.S. citizens | No | N/A | Principal | No | .6 (1) | 0 (0) | |
| Fiancé(e)/marriage (n = 232) | ||||||||
| K-1 | Foreign-citizen fiancé(e) of a U.S. citizen | No | N/A | Principal | No | 86.2 (200) | 0 (0) | |
| CRI | Spouse of U.S. citizen (conditional)c | No | N/A | Principal | Yes | 13.79 (32) | 0 (0) | |
| Employment (n = 62) | ||||||||
| E21 | LPR with advanced degree | Yes | 2nd | Principal | Maybed | 8.1 (5) | 0 (0) | |
| E22 | Spouse of E21 | Yes | 2nd | Derivative | Maybe | 1.6 (1) | 0 (0) | |
| E3 | Skilled professional, Australian | Yes | 3rd | Principal | Maybe | 1.6 (1) | 5.0 (0) | |
| E31 | Highly skilled LPR | Yes | 3rd | Principal | Maybe | 19.4 (12) | 3.4 (.4) | |
| E32 | Professional with B.A. degree | Yes | 3rd | Principal | Maybe | 17.7 (11) | 3.8 (.4) | |
| E34 | Spouse of LPR classified E31 or E32 (skilled worker) | Yes | 3rd | Derivative | Maybe | 33.9 (21) | 4.4 (.2) | |
| E3S | Child of LPR classified E31 or E32 | Yes | 3rd | Derivative | Maybe | 3.2 (2) | 5.0 (0) | |
| EB3 | Skilled worker, professional, or other worker | Yes | 3rd | Principal | Maybe | 14.5 (9) | 3.7 (.2) | |
Note: “Numerically Limited” refers to the distinction between visas that are subject to caps on the number of visas issued by the United States each year. “Preference Level” refers to the priority for processing given to “Numerically Limited” visas. “Estimated Visa Processing Time” was calculated by taking the difference in years between the date of interview (month in 2017) from the “date of final action” listed in the U.S. Visa Bulletin for that visa category. The date of final action is the date of the final visa paperwork being filed that was most recently processed by the USCIS for that visa category a given month. HoPES = Health of Philippine Emigrants Study; LPR = lawful permanent resident; N/A = not applicable; SE = standard error; USCIS = U.S. Citizenship and Immigration Services.
FX1–FX3 visas are technically numerically unlimited, but they are tied to (i.e., derivatives of) numerically limited visa holders, making them subject to their principal’s visa’s numerical limitations.
AM1 and AM6 are visa statuses for “Amerasians” who were born in Vietnam after January 1, 1962, and before January 1, 1976, to an Asian mother and a U.S.-citizen military father.
The “conditional” status of CR1 visa holders refers to spouses who have been married for less than two years (as opposed to IR-1 visa holders who have been married for at least two years), who must have their conditional status adjusted after immigrating to the United States.
Employment migrants in this study “maybe” need an affidavit of support because it is unknown from the data whether one is needed or not. Affidavit of support for employment migrants are needed by the U.S. Department of State in the case that either (1) a relative filed the immigration visa petition on the applicant’s behalf or (2) the applicant has a 5% or greater ownership interest in the business that filed the petition.
Covariates
Age, gender, Philippines region of residence, English proficiency, and health care access were included as personal characteristics that may explain the association between visa type and health. They reflect the life chances and individual traits that legal migrants may be selected on to various degrees. For example, if migrants are selected because they are younger, this may account for better health. Migrants might be more likely to be male or female in certain visa categories, which could explain differences in health by visa type. Region of residence, English proficiency, and health care access reflect differential life chances that can affect the likelihood of migration. Philippines region of residence was categorized as Luzon, Visayas, or Mindanao. English proficiency was measured by asking participants how well they could speak English and was coded as very well/well or not very well/not at all.1 Health care access was defined as where respondents sought medical treatment during their last episode of illness or injury. This variable was coded as receiving no treatment, treatment in a hospital, or treatment in a clinic or other source of health care (e.g., pharmacy, medical missions, friends, relatives, traditional healers, etc.).
Educational attainment and financial strain were included as personal resources that might explain health differences by migrant visa type.2 These socioeconomic resources may be mobilized to gain access to a visa, and they are also commonly associated with health. Educational attainment was measured with four categories: less than high school, high school graduate, some college, or college degree and above. Financial strain was determined by asking respondents to think about the money they have and all their expenses and to respond about the degree of difficulty in meeting those expenses (Kahn and Pearlin 2006). Participants were coded as having high (some to considerable difficulty in meeting expenses), medium (just enough money to pay expenses with no difficulty), or low (enough money with money left over) financial strain.
Statistical Analyses
First, we calculated the sample characteristics of the HoPES baseline sample, comparing migrants with nonmigrants and comparing nonmigrants with migrants disaggregated by visa type (Table 2). Using chi-square tests and bivariate regression models, we calculated p values indicating if differences between groups were statistically significant. We used Stata Version 15 (StataCorp 2017) and applied survey weights.
Table 2.
Descriptive Weighted Statistics for Health of Philippine Emigrants Study Baseline Sample by Migrant Status and Visa Type (n = 1,632).
| % or Mean (SE) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Variable | Total (n = 1,632) | Nonmigrants (n = 801) | All Migrants (n = 831) | Limited Family Visa (n = 362) | Unlimited Family Visa (n = 175) | Fiancé(e)/Marriage Visa (n = 232) | Employment Visa (n = 62) | p Valuea (Nonmigrant, Migrant) | p Valueb (Nonmigrant, 4 Visas) |
| Age (years) | 37.0 (.3) | 37.0 (.4) | 36.9 (.4) | 37.7 (.6) | 41.4 (1.2) | 32.0 (.5) | 36.9 (.9) | ** | |
| Male | 33.5% | 33.6% | 33.5% | 50.3% | 25.9% | 6.6% | 52.5% | *** | |
| Island region | *** | *** | |||||||
| Luzon | 21.6% | .1% | 42.3% | 67.2% | 2.0% | 34.1% | 34.1% | ||
| Visayas | 45.7% | 59.0% | 32.9% | 10.2% | 76.0% | 23.6% | 23.6% | ||
| Mindanao | 32.7% | 40.9% | 24.8% | 22.5% | 22.0% | 42.3% | 42.3% | ||
| English speaking proficiency | |||||||||
| Not at all/not very well | 57.1% | 75.3% | 39.5% | 52.0% | 51.7% | 16.1% | 14.5% | *** | *** |
| Well/very well | 42.9% | 24.7% | 60.5% | 48.0% | 48.3% | 84.0% | 85.5% | ||
| Health care access | *** | *** | |||||||
| No treatment | 42.0% | 34.1% | 49.7% | 43.9% | 46.5% | 60.9% | 53.5% | ||
| Hospital | 33.1% | 34.3% | 32.0% | 35.0% | 29.4% | 28.0% | 35.9% | ||
| Clinic and other | 24.8% | 31.6% | 18.3% | 21.1% | 24.1% | 11.1% | 10.6% | ||
| Educational attainment | *** | *** | |||||||
| Less than high school | 10.3% | 12.8% | 8.0% | 7.0% | 19.4% | 2.9% | 0% | ||
| High school graduate | 18.6% | 16.2% | 20.9% | 21.2% | 20.8% | 25.3% | 3.2% | ||
| Some college | 27.7% | 37.4% | 18.3% | 16.9% | 26.2% | 18.9% | 1.5% | ||
| College degree or more | 43.4% | 33.7% | 52.8% | 54.9% | 33.6% | 53.0% | 95.3% | ||
| Financial strain | *** | *** | |||||||
| High | 30.0% | 42.9% | 17.4% | 23.7% | 15.6% | 10.6% | 9.9% | ||
| Medium | 51.3% | 46.9% | 55.6% | 51.7% | 58.1% | 61.7% | 49.5% | ||
| Low | 18.7% | 10.3% | 27.0% | 24.6% | 26.3% | 27.7% | 40.6% | ||
| Number of health conditionsc | 1.43 (.03) | 1.50 (.05) | 1.37 (.04) | 1.70 (.06) | 1.53 (.10) | .65 (.05) | 1.51 (.15) | * | *** |
Note: Standard errors (SE) for continuous variables provided in parentheses. Significance levels for differences between groups were assessed using chi-square tests and bivariate regression models.
Significance level of difference between nonmigrants and migrants.
Significance level of difference between nonmigrants, limited family visas, unlimited family visas, fiancé(e)/marriage visas, and employment visas.
Range for number of health conditions = 0 to 10.
p < .05,
p < .01,
p < .001.
We examined the associations between migrant status, visa type, and total number of health conditions using Poisson regression (no overdispersion was detected). Table 3 shows our examination of health conditions by migrant status, addressing Research Aim 2 and testing whether migrant health selection is present overall. Table 4 shows our examination of health conditions comparing nonmigrants with migrants by visa type, which addresses Research Aim 3 and tests migrant health selection by specific visa type. For Tables 3 and 4, Model 1 was the bivariate association between migrant status and number of health conditions or between migrant status/visa type and number of health conditions, respectively. Model 2 included personal characteristics: age, gender, region of residence, English proficiency, and health care access. Model 3 additionally included personal resources: educational attainment and financial strain. We conducted pairwise comparisons to indicate differences in health conditions between the different visa types using the postestimation linear combination command (lincom) in Stata (Table 4).
Table 3.
Poisson Regression of Number of Health Conditions on Migrant Status, Health of Philippine Emigrants Study Baseline Sample (n = 1,632).
| Model 1 | Model 2 | Model 3 | ||||
|---|---|---|---|---|---|---|
| Variables | β | 95% CI | β | 95% CI | β | 95% CI |
| Migrant (reference = nonmigrant) | −09* | −.18, −.01 | −.24*** | −.34, −.13 | −.22*** | −.32, −.11 |
| Age | .02*** | .02, .03 | .02*** | .02, .03 | ||
| Male gender (reference = female) | −.00 | −.08, .07 | −.02 | −.09, .06 | ||
| Island region (reference = Luzon) | ||||||
| Visayas | −.59*** | −.71, −.46 | −.60*** | −.72, −.47 | ||
| Mindanao | −.02 | −.13, .09 | −.02 | −.13, −.09 | ||
| English proficiency, speaks very well/well (reference = not very well/not at all) | .11* | .02, .19 | .06 | −.04, .15 | ||
| Health care (reference = no treatment) | ||||||
| Hospital | .34*** | .25, .43 | .34*** | .25, .43 | ||
| Clinic or other | .32*** | .23, .41 | .30*** | .21, .40 | ||
| Educational attainment (reference = less than high school) | ||||||
| High school | −.25*** | −.38, −.12 | ||||
| Some college | −.08 | −.21, .05 | ||||
| College degree and above | .01 | −.12, .14 | ||||
| Financial strain (reference = high) | ||||||
| Medium | −.10* | −.18, −.02 | ||||
| Low | −.05 | −.16, .05 | ||||
| Constant | .41*** | .35, .47 | −.45*** | −.66, −.24 | −.26* | −.50, −.01 |
Note: CI = confidence interval.
p < .05,
p < .001.
Table 4.
Poisson Regression of Number of Health Conditions on Migrant Status and Visa Type, Health of Philippines Emigrants Baseline Sample (n = 1,632).
| Variables | Model 1 | Model 2 | Model 3 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| β | 95% CI | Sig. | β | 95% CI | Sig. | β | 95% CI | Sig. | |
| Visa type (reference = nonmigrant) | |||||||||
| Limited family reunification | .13** | .04, .21 | c | .01 | −.12, .11 | b, c | .00 | −.12, .12 | b, c |
| Unlimited family reunification | .02 | −.12, .16 | c | −.18* | −.33, −.04 | a, c | −.16* | −.31, −.01 | a, c |
| Fiancé(e)/marriage | −.83*** | −1.00, −.66 | a, b, d | −.60*** | −.77, −.43 | a, b | −.56*** | −.73, −.37 | a, b |
| Employment | .01 | −.20, .21 | c | −.09 | −.30, .11 | c | −.11 | −.32, .10 | c |
| Age | .02*** | .02, .03 | .02*** | .02, .03 | |||||
| Male gender (reference = female) | −.05 | −.13, .02 | −.06 | −.15, −.00 | |||||
| Island region (reference = Luzon) | |||||||||
| Visayas | −.38*** | −.52, −.25 | −.40*** | −.54, −.27 | |||||
| Mindanao | .13* | .02, .25 | .12* | .01, .23 | |||||
| English proficiency, speaks very well/well (reference = not very well/not at all) | .12** | .04, .20 | .08+ | −.01,.17 | |||||
| Health care (reference = no treatment) | |||||||||
| Hospital | .34*** | .25, .43 | .34*** | .25, .43 | |||||
| Clinic or other | .31*** | .22, .40 | .30*** | .21, .39 | |||||
| Educational attainment (reference = less than high school) | |||||||||
| High school | −.24*** | −.37, −.11 | |||||||
| Some college | −.08 | −.20, .05 | |||||||
| College degree and above | −.01 | −.14, .12 | |||||||
| Financial strain (reference = high) | |||||||||
| Medium | −.09* | −.17, −.01 | |||||||
| Low | −.05 | −.16, .06 | |||||||
| Constant | .41*** | .35, .47 | −.59*** | −.80, −.38 | −.39** | −.64, −.15 | |||
| Coefficients for Pairwise Comparisons among Visa Types from Adjusted Models | ||
|---|---|---|
| Comparisons for Model I | β | 95% CI |
| To limited family reunification | ||
| Unlimited family | −.11 | −.25, .04 |
| Fiancé(e)/marriage | −.96*** | −1.13, −.78 |
| Employment | −.12 | −.33, .09 |
| To unlimited family reunification | ||
| Fiancé(e)/marriage | −.85*** | −1.06, −.64 |
| Employment | −.01 | −.25, .22 |
| To fiancé(e)/marriage | ||
| Employment | .84*** | .58, 1.09 |
| Comparisons for Model 2 | ||
| To limited family reunification | ||
| Unlimited family | −.18** | −.31, −.05 |
| Fiancé(e)/marriage | −.59*** | −.78, −.40 |
| Employment | −.09 | −.29, .11 |
| To unlimited family reunification | ||
| Fiancé(e)/marriage | −.41*** | −.62, −.20 |
| Employment | .09 | −.13, .31 |
| To fiancé(e)/marriage | ||
| Employment | .50*** | .26, .75 |
| Comparisons for Model 3 | ||
| To limited family reunification | ||
| Unlimited family | −.16* | −.29, −.03 |
| Fiancé(e)/marriage | −.56*** | −.75, −.37 |
| Employment | −.11 | −.31, .08 |
| To unlimited family reunification | ||
| Fiancé(e)/marriage | −.40*** | −.61, −.19 |
| Employment | .05 | −.18, .27 |
| To fiancé(e)/marriage | ||
| Employment | .45*** | .20, .69 |
Note: CI = confidence interval; Sig. = significance level of test of pairwise differences between visa categories; a = group is different from limited family reunification; b = group is different from unlimited family reunification; c = group is different from fiancé(e)/marriage; d = group is different from employment. Model 1 is unadjusted; Model 2 adjusts for age, gender, island region, English proficiency, and health care access; Model 3 adjusts for all covariates in Model 2 as well as educational attainment and financial strain.
p < .10,
p < .05,
p < .01,
p < .001.
In a supplemental analysis, we examined among migrants only whether the estimated length of time it took for visas to be processed was associated with number of health conditions, accounting for personal characteristics and resources. These results are provided in Supplemental Table A in the online version of the article.
RESULTS
Descriptive Statistics
Table 2 displays descriptive results. Comparing nonmigrants to all migrants, there were no significant differences in age (M = 37) or gender (33.5% male). However, when disaggregating all migrants by visa type, there were significant differences in age, with unlimited family visa holders being the oldest on average (41.4 years) and fiancé(e)/marriage visa holders being the youngest on average (32 years). The visa types also differed greatly in gender distribution. Only 6.6% of fiancé(e)/marriage visa holders and 25.9% of unlimited family visa holders were male, whereas about half of limited family visa and employment visa holders were male. Nonmigrants and migrants differed regarding what region of the Philippines they resided. Although almost all nonmigrants were from either Visayas or Mindanao, 42% of migrants were from Luzon. English speaking proficiency varied across the groups: Migrants overall were much more likely to report speaking English well/very well (60.5%) compared to nonmigrants (24.7%), and this was especially true of fiancé(e)/marriage migrants (84%) and employment migrants (85.5%). Health care access was also significantly different across groups. Although nonmigrants were about equally as likely to not seek treatment, go to a hospital, or go to a clinic/other facility, migrants were more likely to seek no treatment at all (49.7%). Fiancé(e)/marriage and employment migrants were most likely to seek no treatment (60.9% and 53.5%, respectively).
Nonmigrants and migrants differed significantly in their personal resources. Migrants were, overall, more educated than nonmigrants. The highest educational levels were found among employment migrants, 95.3% of whom had a college degree or higher educational attainment. Unlimited family visa holders had similar, if not slightly lower, educational attainment relative to nonmigrants, with 19.4% having less than high school education compared to 12.8% of nonmigrants. Migrants also experienced lower levels of financial strain compared to nonmigrants. The lowest levels were noted among employment migrants (40.6% low financial strain). Notably, all visa categories had lower financial strain than nonmigrants on average.
Number of health conditions varied by migrant status and visa type. Migrants reported significantly (p < .05) fewer health conditions on average than nonmigrants (Ms = 1.37 and 1.50, respectively). Disaggregating migrants by visa type revealed even greater differences in health conditions. Fiancé(e)/marriage migrants reported by far the fewest health conditions (M = .65). Meanwhile, unlimited family migrants and employment migrants reported a similar number of health conditions (Ms = 1.53 and 1.51, respectively) as nonmigrants. Limited family migrants reported a higher number of health conditions (M = 1.70) than nonmigrants.
Table 3 presents the Poisson regression results pre-dicting number of health conditions by migrant status. In Model 1, migrants reported significantly fewer health conditions than nonmigrants (b = −.09, p < .05). This association remained and was greater in magnitude when accounting for age, gender, region of residence, English proficiency, and health care access in Model 2 (b = −.24, p < .001). Older age, being from the region of Luzon (compared to Visayas), greater English proficiency, and accessing health care at a hospital or clinic (compared to no treatment) were all associated with greater number of health conditions. After including educational attainment and financial strain in Model 3, the association between migrant status and health conditions remained (b = −.22, p < .001). High school education (compared with less than high school education) and medium level of financial strain (compared with high financial strain) were associated with fewer health conditions.
Table 4 shows the Poisson regression results pre-dicting number of health conditions by migrant status and specific visa type. In Model 1, limited family reunification migrants had significantly more health conditions than nonmigrants (b = .13, p < .01). Unlimited family reunification migrants did not differ in health conditions compared to nonmigrants, limited family reunification migrants, or employment migrants. Similarly, employment migrants did not differ in health conditions compared to nonmigrants. Fiancé(e)/marriage migrants had significantly fewer health conditions compared to nonmigrants (b = −.83, p < .001) and migrants with all other visa types.
In Table 4, Model 2, the associations between visa type and health conditions are different from Model 1 after accounting for age, gender, region of residence, English proficiency, and health care access. Limited family reunification migrants did not differ in number of health conditions compared to nonmigrants, but they did have more health conditions compared to unlimited family reunification migrants (b = −.18, p < .01; reference = limited family reunification) and fiancé(e)/marriage migrants (b = −.59, p < .001; reference = limited family reunification). Unlimited family reunification migrants had fewer health conditions than nonmigrants (b = −.18, p < .05), but they had more health conditions than fiancé(e)/marriage migrants (b = −.41, p < .001; reference = unlimited family reunification). Fiancé(e)/marriage migrants had significantly fewer health conditions than nonmigrants (b = −.60, p < .001) and migrants of the other three visa types. Employment migrants did not differ from nonmigrants, limited family reunification migrants, or unlimited family reunification migrants, but they had more health conditions than fiancé(e)/marriage migrants (b = .50, p < .001; reference = fiancé(e)/marriage).
In Table 4, Model 3, the associations between visa type and health conditions were similar to Model 2 after additionally accounting for educational attainment and financial strain. In Model 3, older age, region of residence, health care access, education, and financial strain were all independently associated with number of health conditions.
A graphical representation of the differences in number of health conditions by migrant status and visa type, accounting for all covariates, is provided in Figure 1. As seen in this figure, fiancé(e)/marriage migrants have far fewer health conditions than any other group. Unlimited family reunification migrants seem to have fewer health conditions than nonmigrants and limited family reunification migrants on average. Limited family reunification migrants do not differ in health conditions from nonmigrants. Employment migrants seem to have on average fewer health conditions than nonmigrants and limited family migrants, but the confidence interval is too wide for these differences to be statistically significant.
Figure 1.
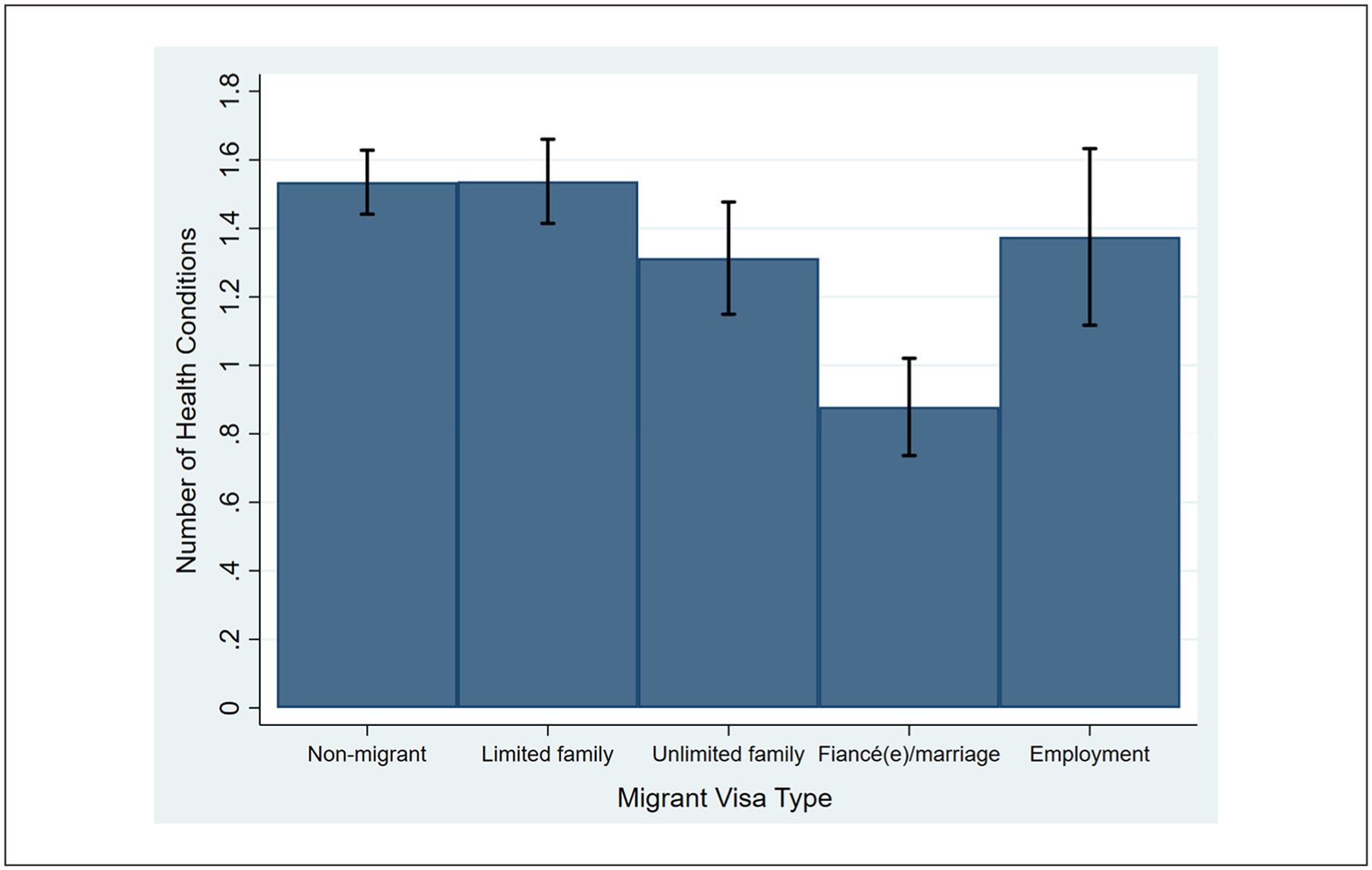
Number of Health Conditions by Visa Type, Health of Philippines Emigrants Baseline Sample (n = 1,632).
Note: Adjusted for age, gender, island region, English proficiency, health care access, educational attainment, and financial strain. Black vertical bars represent 95% confidence intervals.
Supplemental Table A in the online version of the article shows that among migrants only, longer visa processing times are associated with more health conditions even after accounting for personal characteristics and resources (b = .01, p < .001). However, becaise the visa processing time variable is a rough estimate, these findings are preliminary and should be interpreted with some caution.
DISCUSSION
This study advances our understanding of how migrant health is shaped by U.S. immigration policy, adding to the growing body of literature stressing the importance of contextualizing immigrant selectivity within sending and receiving countries (Feliciano 2020). Immigrant visas are sociopolitical constructs that shape how health selectivity occurs. Our results imply that visas reflect life chances and premigration processes that affect health selection (Jasso 2011, 2016).
Consistent with prior research, we found evidence of health selection occurring for migrants compared to nonmigrants (Akresh and Frank 2008; Hamilton et al. 2015; Ro et al. 2016). Our study is novel through the use of premigration data, comparing a representative sample of Filipino migrants to Filipinos of similar age, gender, and education who do not migrate (Feliciano 2020). Migrants reported fewer health conditions than nonmigrants overall, showing that health selection is evident among migrants from the Philippines prior to leaving for the United States. Also consistent with research on immigrant selectivity, we found migrants generally had greater socioeconomic resources compared to nonmigrants. Low financial strain was associated with migrant status.
Moreover, our examination of visa types adds greater nuance to our understanding of health selectivity. We examined four visa categories: numerically limited family reunification, numerically unlimited family reunification, fiancé(e)/marriage, and employment. Our analysis revealed that fiancé(e)/marriage was the only visa category that showed strong health selection. These visa holders tended to be younger women with high levels of English proficiency. Interestingly, controls for these characteristics and socioeconomic resources did not explain away the health advantage of migrants in this category. We speculate on several other reasons that may explain this selection. First, there may be other socioeconomic factors that were unmeasured, such as wealth, that drive selection. Second, there might be factors such as physical attractiveness that simultaneously select for marriage and health (Rhodes et al. 2007; Singh et al. 2010). Third, perhaps the prospect of being married and reunited with their spouse fosters optimism and reduces stress, thus improving health.
In contrast, we did not find strong evidence of health selection among numerically unlimited family reunification and employment migrants: The health of these two groups was no different than the health of nonmigrants prior to migration. Unlimited family visa migrants had similar levels of education but lower levels of financial strain than nonmigrants. This low financial strain may be indicative of their close family relation to a U.S. citizen, who likely supported the visa holder prior to migration through remittances. After accounting for personal characteristics and resources, numerically unlimited family reunification migrants had a slight health advantage over nonmigrants, indicating some positive health selection unattributed to finances. As expected, employment visa holders were relatively young with high English proficiency, low financial strain, and high levels of education. Surprisingly, this did not equate to strong positive health selection for employment migrants; they showed little evidence of health selection before or after accounting for these factors. However, the findings for employment migrants should be interpreted with some caution given the small sample for this visa type (n = 62).
Our examination of numerically limited family reunification migrants as a separate category of visa holders found no evidence of health selection for this group. In fact, they reported worse health than nonmigrants despite having higher education and lower financial strain compared to nonmigrants. This health disadvantage was mitigated after accounting for age, gender, region of residence, English proficiency, and health care access. This result mirrors previous studies that found health selection to be weakest or nonexistent among groups of limited family reunification visa holders (Akresh and Frank 2008; Riosmena et al. 2017; Ro et al. 2016). Taken together, these findings demonstrate heterogeneity in health selection by visa type—which can differentially stratify both health and social advantages among migrants from the same country.
We additionally explored the possibility that health selection by visa type may be explained by differential experience of visa stress during the process of applying for and obtaining legal permanent residency (Jasso 2011; Jasso et al. 2005). Our examination of the visa categories in Table 1 revealed drastic differences in the estimated amount of time it took to process the visas. Numerically unlimited family reunification migrants and fiancé(e)/marriage migrants only waited weeks or at most months for their visas to be approved once submitted. These were the same migrants who showed the greatest evidence of positive health selection. Meanwhile, numerically limited family reunification migrants waited, on average, 14 years (range = 2–24 years) and employment migrants waited, on average, 3.6 years (range = 0–4.4 years) for their visas to be processed. The group that had the longest average wait time—numerically limited family reunification migrations—showed lack of health selection in our main analysis. In a supplemental analysis among migrants only, we found that longer visa processing time was significantly associated with a higher number of health conditions even after accounting for personal characteristics (including age) and resources. We did not include a model with both visa type and visa processing times because the two constructs are highly related to one another. It is also important to keep in mind that our visa processing time variable was only an estimate based on extrapolation from an external data source (2017 Visa Bulletin), and these estimates likely underestimate the amount of time that migrants experienced visa stress (from the time they started the visa application process to the time their visas were ultimately approved; U.S. Department of State 2020). Nevertheless, this analysis suggests that longer visa processing times, which are determined by U.S. policy and affected by bureaucratic backlog, may explain worse health and lack of health selection among legal migrants whose visas took much longer to be approved.
Limitations
Some limitations should be acknowledged. Although the response rate for the migrant cohort was some-what low (36.5%), reflecting the busy lives of migrants prior to departure, the HoPES migrant sample was representative of recent Filipino immigrants in the ACS (Gee et al. 2018). Additionally, nonmigrants were sampled from two regions but not the entire country. Thus, some caution is warranted regarding selection bias. In addition, although respondents were assured that their responses were confidential and would not influence the visa process, it is possible that migrants may still undercount their health conditions. If this is the case, HoPES migrants could be less healthy than the survey would suggest, perhaps inflating any health selection findings. Lastly, given our focus on legal migration from a single country, the Philippines, certain immigrant groups were naturally left out, including humanitarian migrants (e.g., refugees), diversity visa holders, and undocumented immigrants. Future work should examine these other visa types, including undocumented persons applying for lawful status, and how their health is stratified by the visa process in other countries.
CONCLUSION
Our study provides a novel look at what underlies discrepancies in health selection among migrant cohorts by examining health stratification based on an important sociopolitical construct: immigrant visas. Visas reflect historical and contemporary immigration policies that fundamentally shape who is deemed eligible to migrate. These policies influence how potential migrants navigate the path toward lawful permanent residency. Therefore, how restrictive U.S. immigration policies become along with lengths of processing times may contribute to differences in immigrant selectivity in the future. If our findings are any indication, it is possible that greater administrative backlogs will lead to longer experiences of visa stress, thereby negatively affecting health and negating health selection among migrants with the most restrictive visas. Disparities among migrants will emerge even as people applying for less restrictive and faster visa types, such fiancé(e)/marriage visas, experience high levels of positive health selection.
The natural extension of this research is to examine how visa type shapes health as immigrants integrate into their destination country. Do initial health advantages, especially among fiancé(e)/marriage migrants, decline with time after integration into the United States? If so, how long does this process take, and in what ways does this manifest? How do prior life circumstances, including experiencing visa stress in the premigration context, contribute to later health trajectories in the United States? How do parents’ migrant visa types affect the health of their children born in the United States? Furthermore, do these ideas generalize to other countries? These are all areas for future inquiry. Our study highlights the importance of considering visa category as a social determinant of immigrant health.
Supplementary Material
ACKNOWLEDGMENTS
We thank the Commission on Filipinos Overseas and their staff, especially Regina Galias, Ivy Miravalles, Golda Myra Roma, and Paul Vincent Avecilla, without whom this research would not be possible. We also thank Nanette Lee Mayol, Midea Kabamalan, Anna Vivas, Karen Llave, Elma P. Laguna, Christian Joy Cruz, Lorna Perez, Delia Carba, Klarrines Tanalago, Vanessa Medina, and Larry Tagalog for their insights and assistance with this project. A special thanks to Emily María Migliore for lending her legal expertise to check the accuracy of our visa classifications. An earlier version of this research was presented at the annual meeting of the American Public Health Association in 2019. Thank you to the anonymous reviewers and editor for their valuable feedback and critiques.
FUNDING
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by funding from the U.S. National Institutes of Health (1R01HD083574–01A1). We are grateful to the California Center for Population Research at UCLA (CCPR) for general support. CCPR receives population research infrastructure funding (P2C-HD041022) from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD). Brittany N. Morey received support from the University of California, Riverside Chancellor’s Postdoctoral Fellowship.
Author Biographies
Brittany N. Morey is an assistant professor in the Program of Public Health at the University of California-Irvine. Her research focuses on how structural inequity shapes racial and ethnic health inequities, especially for Asian Americans, Pacific Islanders, and other immigrant groups in the United States. Previously, she was a Chancellor’s Postdoctoral Fellow at the University of California-Riverside. She is currently receiving support through the National Cancer Institute to examine how ethnic enclaves contribute to breast cancer outcomes among Asian Americans and Latinxs.
Adrian Matias Bacong is a doctoral student in the Department of Community Health Sciences at the University of California-Los Angeles Fielding School of Public Health. His research focuses on health inequities attributed to race, ethnicity, immigration status, and the racialization of immigrant legal status.
Anna K. Hing is a doctoral candidate at the University of California-Los Angeles Fielding School of Public Health. Her research examines how structural inequity, especially in relation to racism, voting rights, and immigration, creates health disparities for people of color.
A. B. de Castro is a professor and associate dean for diversity, equity, and inclusion at the University of Washington School of Nursing. His research focuses on immigrant health, emphasizing how employment opportunities, job conditions, and work organization contribute to disparities in chronic stress and occupational-related injury and illness. He is co-principal investigator on the Health of Philippine Migrants Study, funded by the National Institutes of Health.
Gilbert C. Gee is a professor in the Department of Community Health Sciences at the University of California-Los Angeles Fielding School of Public Health. His research focuses on the social determinants of health inequities of racial, ethnic, and immigrant minority populations using a multilevel and life course perspective. A primary line of his research focuses on conceptualizing and measuring racial discrimination and in understanding how discrimination may be related to illness. He is co-principal investigator on the Health of Philippine Migrants Study, funded by the National Institutes of Health.
Footnotes
SUPPLEMENTAL MATERIAL
Table A is available in the online version of the article.
Although English proficiency is typically seen as a marker of immigrant assimilation postmigration, it does not have that same meaning premigration, especially in a country like the Philippines where English is an official language. Many Filipino phrases include English words, such as “diabetes or mataas na blood sugar,” which means “diabetes or high blood sugar.” Therefore, English proficiency in this context accounts for artifacts in language and comprehension.
We also considered occupational title, employment, and income as additional covariates. However, these factors were excluded because many migrants terminate their jobs prior to exiting the country.
REFERENCES
- Abraído-Lanza Ana F., Dohrenwend Bruce P., Ng-Mak Daisy S., and Turner J. Blake. 1999. “The Latino Mortality Paradox: A Test of the ‘Salmon Bias’ and Healthy Migrant Hypotheses.” American Journal of Public Health 89(10):1543–48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Acevedo-Garcia Dolores, and Bates Lisa M.. 2008. “Latino Health Paradoxes: Empirical Evidence, Explanations, Future Research, and Implications.” Pp. 101–13 in Latinas/os in the United States: Changing the Face of América, edited by Rodríguez H, Sáenz R, and Menjívar C. Boston: Springer US. [Google Scholar]
- Akresh Ilana Redstone, and Frank Reanne. 2008. “Health Selection among New Immigrants.” American Journal of Public Health 98(11):2058–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boquet Yves. 2017. The Philippine Archipelago. Cham, Switzerland: Springer. [Google Scholar]
- Castro-Palaganas Erlinda, Spitzer Denise L., Kabamalan Maria Midea M., Sanchez Marian C., Caricativo Ruel, Runnels Vivien, Labonté Ronald, Murphy Gail Tomblin, and Bourgeault Ivy Lynn. 2017. “An Examination of the Causes, Consequences, and Policy Responses to the Migration of Highly Trained Health Personnel from the Philippines: The High Cost of Living/Leaving—a Mixed Method Study.” Human Resources for Health 15(1):25. doi: 10.1186/s12960-017-0198-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- de Castro AB, Hing Anna K., Lee Nanette R., Kabamalan Maria Midea M., Llave Karen, Crespi Catherine M., Wang May, and Gee Gilbert. 2019. “Cohort Profile: The Health of Philippine Emigrants Study (HoPES) to Examine the Health Impacts of International Migration from the Philippines to the USA.” BMJ Open 9(11):e032966. doi: 10.1136/bmjopen-2019-032966. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dhadda Amrit, and Greene Giles. 2018. “‘The Healthy Migrant Effect’ for Mental Health in England: Propensity-Score Matched Analysis Using the Empiric Survey.” Journal of Immigrant and Minority Health 20(4):799–808. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Feliciano Cynthia. 2020. “Immigrant Selectivity Effects on Health, Labor Market, and Educational Outcomes.” Annual Review of Sociology 46(1):25.1–25.20. [Google Scholar]
- Gee Gilbert C., de Castro AB, Crespi Catherine M., Wang May C., Llave Karen, Brindle Eleanor, Lee Nanette R., Kabamalan Maria Midea M., and Hing Anna K.. 2018. “Health of Philippine Emigrants Study (HoPES): Study Design and Rationale.” BMC Public Health 18(1):771. doi: 10.1186/s12889-018-5670-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gee Gilbert C., and Ford Chandra L.. 2011. “Structural Racism and Health Inequities.” Du Bois Review: Social Science Research on Race 8(1):115–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gong Fang, Xu Jun, Fujishiro Kaori, and Takeuchi David T.. 2011. “A Life Course Perspective on Migration and Mental Health among Asian Immigrants: The Role of Human Agency.” Social Science & Medicine 73(11):1618–26. [DOI] [PubMed] [Google Scholar]
- Gorman Bridget K., Read Jen’nan Ghazal, and Krueger Patrick M.. 2010. “Gender, Acculturation, and Health among Mexican Americans.” Journal of Health and Social Behavior 51(4):440–57. [DOI] [PubMed] [Google Scholar]
- Gubernskaya Zoya, Bean Frank D., and Van Hook Jennifer. 2013. “(Un)Healthy Immigrant Citizens: Naturalization and Activity Limitations in Older Age.” Journal of Health and Social Behavior 54(4):427–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hamilton Tod G., Palermo Tia, and Green Tiffany L.. 2015. “Health Assimilation among Hispanic Immigrants in the United States: The Impact of Ignoring Arrival-Cohort Effects.” Journal of Health and Social Behavior 56(4):460–77. [DOI] [PubMed] [Google Scholar]
- Jasso Guillermina. 2011. “Migration and Stratification.” Social Science Research 40(5):1292–336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jasso Guillermina. 2016. “Migration, Human Development, and the Life Course.” Pp. 331–64 in Handbook of the Life Course.Vol. II, edited by Shanahan MJ, Mortimer JT, and Johnson M. Kirkpatrick. Cham, Switzerland: Sprinter International Publishing. [Google Scholar]
- Jasso Guillermina, Massey Douglas S., Rosenzweig Mark R., and Smith James P.. 2004. “Immigrant Health: Selectivity and Acculturation.” Pp. 227–66 in Critical Perspectives on Racial and Ethnic Differences in Health in Late Life, edited by Anderson NB, Bulatao RA, and Cohen B. Washington, DC: National Academies Press. [PubMed] [Google Scholar]
- Jasso Guillermina, Massey Douglas S., Rosenzweig Mark, and Smith James. 2005. “Immigration, Health, and New York City: Early Results Based on the U.S. New Immigrant Cohort of 2003.” Economic Policy Review (Dec):127–51. [Google Scholar]
- Kahn Joan R., and Pearlin Leonard I.. 2006. “Financial Strain over the Life Course and Health among Older Adults.” Journal of Health and Social Behavior 47(1):17–31. [DOI] [PubMed] [Google Scholar]
- Kato Takao, and Sparber Chad. 2011. “Quotas and Quality: The Effect of H-1b Visa Restrictions on the Pool of Prospective Undergraduate Students from Abroad.” The Review of Economics and Statistics 95(1):109–26. [Google Scholar]
- Kim Minjeong. 2010. “Gender and International Marriage Migration.” Sociology Compass 4(9):718–31. [Google Scholar]
- Espiritu Yen Le, and Wolf Diane L.. 2001. “The Paradox of Assimilation: Children of Filipino Immigrants in San Diego.” Pp. 157–86 in Ethnicities: Children of Immigrants in America, edited by Rumbaut RG and Portes A. Berkeley and Los Angeles: University of California Press. [Google Scholar]
- Lichter Daniel T., Qian Zhenchao, and Tumin Dmitry. 2015. “Whom Do Immigrants Marry? Emerging Patterns of Intermarriage and Integration in the United States.” The ANNALS of the American Academy of Political and Social Science 662(1):57–78. [Google Scholar]
- Lindstrom David P., and Ramírez Adriana López. 2010. “Pioneers and Followers: Migrant Selectivity and the Development of U.S. Migration Streams in Latin America.” The ANNALS of the American Academy of Political and Social Science 630(1):53–77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liu John M., Ong Paul M., and Rosenstein Carolyn. 1991. “Dual Chain Migration: Post-1965 Filipino Immigration to the United States.” International Migration Review 25(3):487–513. [PubMed] [Google Scholar]
- Lloyd Kathryn A. 2000. “Wives for Sale: The Modern International Mail-Order Bride Industry.” North-western Journal of International Law & Business 20(2): 341–68. [Google Scholar]
- Markides Kyriakos S., and Coreil Jeannine. 1986. “The Health of Hispanics in the Southwestern United States: An Epidemiologic Paradox.” Public Health Reports 101(3):253–65. [PMC free article] [PubMed] [Google Scholar]
- Martinez Jose N., Aguayo-Tellez Ernesto, and Rangel-Gonzalez Erick. 2015. “Explaining the Mexican-American Health Paradox Using Selectivity Effects.” International Migration Review 49(4):878–906. [Google Scholar]
- Massey Douglas S., and Taylor J. Edward. 2004. International Migration: Prospects and Policies in a Global Market. New York: OUP Oxford. [Google Scholar]
- McKenzie David, Caroline Theoharides, and Dean Yang. 2014. “Distortions in the International Migrant Labor Market: Evidence from Filipino Migration and Wage Responses to Destination Country Economic Shocks.” American Economic Journal: Applied Economics 6(2):49–75. [Google Scholar]
- Medina Belen, and Natividad Josefina. 2012. “Filipino Chain Migration to the United States.” Philippine Population Journal 1(4):67–94. [Google Scholar]
- Mirowsky John, and Ross Catherine E.. 2015. “Education, Health, and the Default American Lifestyle.” Journal of Health and Social Behavior 56(3):297–306. [DOI] [PubMed] [Google Scholar]
- Obinna Denise N. 2014. “The Challenges of American Legal Permanent Residency for Family- and Employment-Based Petitioners.” Migration and Development 3(2): 272–84. [Google Scholar]
- Palloni Alberto, and Arias Elizabeth. 2004. “Paradox Lost: Explaining the Hispanic Adult Mortality Advantage.” Demography 41(3):385–415. [DOI] [PubMed] [Google Scholar]
- Reyes Victoria. 2017. “Stigmatized Love, Boundary-Making, and the Heroic Love Myth: Filipina Women Constructing Their Relationships with U.S. Military Men within and Beyond the Legal Framework.” Pp. 140–57 in International Marriages and Marital Citizenship: Southeast Asian Women on the Move, edited by Fresnoza-Flot A and Ricordeau G. Abingdon, UK: Routledge. [Google Scholar]
- Rhodes Gillian, Yoshikawa Sakiko, Palermo Romina, Simmons Leigh W., Peters Marianne, Lee Kieran, Halberstadt Jamin, and Crawford John R.. 2007. “Perceived Health Contributes to the Attractiveness of Facial Symmetry, Averageness, and Sexual Dimorphism.” Perception 36(8):1244–52. [DOI] [PubMed] [Google Scholar]
- Riosmena Fernando, Kuhn Randall, and Jochem Warren C.. 2017. “Explaining the Immigrant Health Advantage: Self-Selection and Protection in Health-Related Factors among Five Major National-Origin Immigrant Groups in the United States.” Demography 54(1):175–200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ro Annie, Fleischer Nancy L., and Blebu Bridgette. 2016. “An Examination of Health Selection among U.S. Immigrants Using Multi-national Data.” Social Science & Medicine 158:114–21. [DOI] [PubMed] [Google Scholar]
- Rodriguez Robyn M. 2002. “Migrant Heroes: Nationalism, Citizenship and the Politics of Filipino Migrant Labor.” Citizenship Studies 6(3):341–56. [Google Scholar]
- Rodriguez Robyn Magalit. 2010. Migrants for Export: How the Philippine State Brokers Labor to the World. Minneapolis: University of Minnesota Press. [Google Scholar]
- Rubalcava Luis N., Teruel Graciela M., Thomas Duncan, and Goldman Noreen. 2008. “The Healthy Migrant Effect: New Findings from the Mexican Family Life Survey.” American Journal of Public Health 98(1):78–84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Singh Devendra, Dixson Barnaby J., Jessop Tim S., Morgan Bethan, and Dixson Alan F.. 2010. “Cross-Cultural Consensus for Waist–Hip Ratio and Women’s Attractiveness.” Evolution and Human Behavior 31(3):176–81. [Google Scholar]
- StataCorp. 2017. “Stata Statistical Software: Release 15.” College Station, TX: StataCorp LLC. [Google Scholar]
- Téllez Ernesto Aguayo, Martínez José N., and González Erick Rangel. 2015. “Explaining the Mexican-American Health Paradox Using Selectivity Effects.” International Migration Review 49(4):878–906. [Google Scholar]
- Tran Trinh. 2012. “Mis-matched: Taking a State Approach to Enforcing the Growing International Matchmaking Industry.” Family Court Review 50(1):159–74. [Google Scholar]
- U.S. Department of State. 2020. “U.S. Department of State Webpage.” https://www.state.gov/.
- Viruell-Fuentes Edna A., Miranda Patricia Y., and Abdulrahim Sawsan. 2012. “More Than Culture: Structural Racism, Intersectionality Theory, and Immigrant Health.” Social Science & Medicine 75(12):2099–106. [DOI] [PubMed] [Google Scholar]
- Yang Philip Q. 2010. “A Theory of Asian Immigration to the United States.” Journal of Asian American Studies 13(1):1–34. [Google Scholar]
- Yoo Hyung Chol, Gee Gilbert C., and Takeuchi David. 2009. “Discrimination and Health among Asian American Immigrants: Disentangling Racial from Language Discrimination.” Social Science & Medicine 68(4):726–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zong Jie, and Batalova Jeanne. 2018. Filipino Immigrants in the United States. Washington, DC: Migration Policy Institute. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.