

Abstract
Background:
Diagnostic and Statistical Manual of Mental Disorders (DSM-5) included in 2013 Internet gaming disorder (IGD) as a condition for further study, and in 2018, the World Health Organization included gaming disorder (GD) as a mental disorder in the International Classification of Disease (ICD-11). We aim to compare disorders of gaming in both diagnostic systems using a sample of young adults in Mexico.
Methods:
Self-administered survey to estimate the prevalence of DSM-5 IGD and ICD-11 GD in 5 Mexican universities; 7,022 first-year students who participated in the University Project for Healthy Students, part of the World Health Organization World Mental Health International College Student Initiative. Cross-tabulation, logistic regression, and item response theory were used to inform on 12- month prevalence of DSM-5 IGD and ICD-11 GD, without and with impairment.
Results:
The 12-month prevalence of DSM-5 IGD was 5.2% (95% CI, 4.7 to 5.8), almost twice as high as the prevalence using the ICD-11 GD criteria (2.7%; 95% CI, 2.4 to 3.1), and while adding an impairment requirement diminishes both estimates, prevalence remains larger in DSM-5. We found that DSM-5 cases detected and undetected by ICD-11 criteria were similar in demographics, comorbid mental disorders, service use, and impairment variables with the exception that cases detected by ICD-11 had a larger number of symptoms and were more likely to have probable drug dependence than undetected DSM-5 cases.
Conclusion:
DSM-5 cases detected by ICD-11 are mostly similar to cases undetected by ICD-11. By using ICD-11 instead of DSM-5, we may be leaving (similarly) affected people underserved. It is unlikely that purely epidemiological studies can solve this discrepancy and clinical validity studies maybe needed.
Keywords: Mexico, Internet gaming disorder, epidemiology, DSM-5, ICD-11, prevalence
Abstract
Contexte:
En 2013, le DSM-5 a inclus le trouble du jeu sur Internet (TJI) qui nécessitait des études supplémentaires et en 2018, l’Organisation mondiale de la santé a ajouté le trouble du jeu vidéo (TJV) comme trouble mental dans la CIM-11. Nous visons à comparer les troubles de jeu dans les deux systèmes diagnostiques à l’aide d’un échantillon de jeunes adultes du Mexique.
Méthodes:
Un sondage auto-administré visait à estimer la prévalence du TJI-DSM-5 et du TJV-CIM-11 dans 5 universités mexicaines. Des étudiants de première année au nombre de 7 022 ont participé au Projet universitaire pour étudiants en santé (PUERTAS), dans le cadre de l’Initiative mondiale des étudiants du Collège international de la santé mentale de l’Organisation mondiale de la santé (WMH-ICS). La tabulation croisée, la régression logistique et la théorie de la réponse d’item ont servi à nous renseigner sur la prévalence de 12 mois du TJI-DSM-5 et du TJV-CIM-11, avec et sans exigence de dépréciation.
Résultats:
La prévalence de 12 mois du TJI-DSM-5 était de 5,2% (IC à 95% 4,7 à 5,8), presque deux fois aussi élevée que la prévalence utilisant les critères du TJV-CIM-11 [2,7% (IC à 95% 2,4 à 3,1)], et même si l’ajout d’une exigence de dépréciation diminue les deux estimations, la prévalence demeure plus élevée dans le DSM-5. Nous avons constaté que les cas de DSM-5 détectés et non détectés par les critères de la CIM-11 étaient semblables à l’égard des données démographiques, des troubles mentaux comorbides, de l’utilisation des services et des variables de dépréciation, excepté que les cas détectés par la CIM-11 avaient un plus grand nombre de symptômes et étaient plus susceptibles d’avoir une dépendance probable aux drogues que les cas du DSM-5 non détectés.
Conclusion:
Les cas du DSM-5 détectés par la CIM-11 sont pour la plupart semblables aux cas non détectés par la CIM-11. En utilisant la CIM-11 plutôt que le DSM-5, nous pouvons faire en sorte que les personnes (semblablement) affectées soient mal desservies. Il est peu probable que des études purement épidémiologiques puissent résoudre cet écart, et il faudra peut-être des études de validité clinique.
Introduction
In 2013, Internet gaming disorder (IGD) was included in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) as a condition for further study.1 IGD was placed in the section of substance-related and addictive disorders, together with gambling disorder, “reflecting evidence that gambling behaviors activate reward systems similar to those activated by drugs of abuse and produce some behavioral symptoms that appear comparable to those produced by the substance use disorders.”1 Gambling disorder has been included in manuals of psychiatric nosology for quite a number of years. At the time of publication of DSM-5, IGD was the only other behavioral addiction considered for further study, whereas for “sex addiction,” “exercise addiction,” or “shopping addiction,” the DSM-5 working group considered that there was insufficient evidence to include these behaviors as mental disorders.1 In the DSM-5 manual, IGD received a first provisional description; 9 clinical symptoms were identified and a suggestion for cut-off point was made (5 of 9 symptoms for any IGD; mild, moderate, or severe categories were named but not defined). Further, an international consensus led by Nancy Petry2 described in more detail these 9 symptoms put forward by the DSM-5 and formulated the key elements for epidemiological studies on the topic. Since the publication of DSM-5 in 2013, research in this area has tended to be more unified in defining gaming using the 9 symptoms suggested by the DSM-5.2 Recent reviews have shown an increasing number of studies in this area that aim to provide prevalence estimates for DSM-5 IGD and which evaluate different instruments to assess this disorder.3–5
Five years later, the World Health Organization (WHO) included the category of gaming disorder (GD) in the forthcoming International Classification of Disease (ICD-11) manual,6,7 thereby making a diagnosis of GD a real possibility for patients and clinicians.8 In the WHO formulation, GD is characterized by a pattern of persistent or recurrent gaming behavior manifested by only 3 symptoms: impaired control over gaming, increasing priority given to gaming, and continuation or escalation of gaming despite the occurrence of negative consequences. Both, the DSM-5 and ICD-11 included clinically significant impairment or distress for a clinical diagnosis.
Table 1, adapted from,2 provides a glance of DSM-5 and ICD-11 definitions. When initially formulated, the DSM-5 criteria presumably tried to balance criterion from both substance use disorders (5 criteria) and from the gambling tradition (4 criteria). Whether these symptoms from 2 traditions would tend to work together and tap a common latent trait (gaming) was unknown at the time of the DSM-5 formulation. An item response theory (IRT) analysis of DSM-5 in a sample of 1st-year Mexican college students shows that to be the case, with substance and gambling symptoms mixed in the continuum of the IRT latent trait,9 In contrast, the ICD-11 definition emphasized a more unitary substance use approach to define GD as a pure addictive condition consisting of 3 core symptoms (see the parallel definition of alcohol use disorders in10 and the parallel definition of ICD-11-“6C50 Gambling disorder”). We currently do not know whether, by selecting only core substance-like symptoms, ICD-11 gaming cases are, or not, more specific. A simple examination of Table 1 suggests that some (unknown) level of disparity in the diagnosis of DSM-5 IGD and ICD-11 GD is likely. A clinical study among 188 children and adolescents from Korea11 reported that among 73 cases with DSM-5 IGD, only 12 (16.4%) would have an ICD-11 GD diagnosis. Whether similar discordant findings would be present in samples of the general population is currently unknown.
Table 1.
DSM-5 IGD 9 Symptoms from Substance Use (SU) and Gambling (G) Criteria and ICD-11 3 GD Criteria.a
| DSM-5 Symptom | Description |
|---|---|
| S1 | Preoccupation-too much time spent (G) |
| S2 | Withdrawal-feel restless-irritated-angry-anxious-sad (SU) |
| S3 | Tolerance-need more time-excitement (SU) |
| S4 | Unsuccessful attempts to control-cannot reduce gaming (SU)a |
| S5 | Loss of other interests (SU)a |
| S6 | Continued excessive use despite psychosocial problems (SU)a |
| S7 | Deceiving regarding online gaming (G) |
| S8 | Escape-gaming to forget troubles (G) |
| S9 | Negative consequences (G) |
| Impairment requirement | |
| DSM-5: “…leading to clinically significant impairment or distress” | |
| ICD-11: “…result in significant impairment” | |
a DSM-5 symptoms that correspond to ICD-11 criteria.
The goal of this study is, first, to compare the prevalence of DSM-5 IGD and ICD-11 GD, with and without impairment, and the amount of the likely divergence of estimates; second, we aim to study differences, if any, in demographics, symptom severity, comorbidity, impairment, and service use among DSM-5 IGD cases detected by the ICD-11 GD criteria (thereafter IGD+) and undetected by ICD-11 GD criteria (thereafter IGD−), and, third, to identify possible differences in the symptoms profile among IGD+ and IGD− cases.
Methods
Participants
The 2018 to 2019 cohort of the University Project for Healthy Students (PUERTAS; University) Project (for Healthy Students)12 was conducted in 5 Mexican universities from January 2018 to February 2019 and included 7,095 1st-year students out of which 7,022 had completed surveys that included the IGD scale. The description of this sample has been documented elsewhere9 and the IGD scale that we used is freely accessible for the interested readers as a Supplementary Material (https://akjournals.com/view/journals/2006/8/4/article-p714.xml). Briefly, the surveys were administered to a convenience sample of 5 universities chosen based on their interest in early detection of mental health problems. After university approval, we used a census design in which all incoming students for the 2018 to 2019 academic years were invited to participate in a web-based self-report survey. Participation was anonymous and voluntary. Informed consent was obtained from participants through the web platform. While overall procedures were similar across universities, recruitment varied by university. All participants that filled a survey that included the IGD section (n = 7,022) were asked whether they played video games in the past 12 months. Video game users (thereafter called “gamers”) are those who reported playing video games (on a computer, smartphone, console, or any other electronic device) in the past 12 months (yes = 4,262; no = 2,760). To avoid unnecessary respondent burden, the full IGD scale is asked only to those gamers who screened positive to the following: If they played, on average, at least 1 day per week and their duration of gaming (during weekday or weekend) was at least 30 minutes (yes = 2,547—thereafter called “active gamers”; no = 1,715). The overall response rate for all universities in the wider PUERTAS study was 79.3%. Prevalence of DSM-5 IGD and ICD-11 GD is presented for the total sample (n = 7,022), gamers, and active gamers. The IRT analysis was performed among those who are active gamers, and we evaluated differences among IGD+ (n = 178) and IGD− (n = 189) in the subsample of DSM-5-positive respondents (n = 367).
Scales
DSM-5 and ICD-11 gaming
The section on IGD consisted of 23 items based on the 9 symptoms or domains described in the DSM-5 and formulated by an international consensus led by Nancy Petry that included an English version and a Spanish translation.9,13 Some symptoms/domains were measured by more than 1 question (2 questions each for 7 of the 9 domains; 3 for the domain “negative consequences” and 6 for the domain “continuation”). All 23 questions lead to dichotomous answers (yes/no), and each of the 9 symptoms was considered positive if any of the questions pertaining to a given symptom was positive (yes). As per DSM-5, the presence of 5 of 9 symptoms means that someone has probable IGD. As a working definition of severity, we further split the DSM-5 cases as mild (exactly 5 symptoms), moderate (6 to 7 symptoms) and severe (8 to 9 symptoms). For ICD-11 GD, we required a positive answer to all 3 symptoms (unsuccessful attempts to control-cannot reduce gaming, loss of other interests, and continued excessive use despite psychosocial problems) described by WHO to score positive for a likely GD. Description of the individual symptoms for IGD, together with the psychometric properties of the scale, was reported elsewhere.9
Demographics
Gender, age (those aged 18 to 19 vs. 20+ to compare students who entered university at the expected age vs. those who entered later), and parent’s educational attainment were included in statistical models.
Psychopathology
As described elsewhere,12 scales for screening of alcohol dependence, drug dependence, 12-month major depressive episode, 12-month generalized anxiety disorder, and 12-month suicide ideation were ascertained, using the validated scales of the Alcohol Use Disorders Identification Test and the Composite International Diagnostic Interview Screening Scales.
Other variables
Service use was measured by a series of questions which asked about 12-month and lifetime treatment for an emotional or substance problem, whether the treatment was psychological counseling or medication. Severity of health-related role impairment in the domains of home management/chores, college-related and other work, close personal relationships, and social life during the past 12 months was assessed using an adapted version of the Sheehan Disability Scale.14,15 To be conservative, we required respondents to have severe self-reported role impairment, defined as having a 7 to 10 rating in at least 1 of the 4 areas, for being considered of clinical significance.16
Statistical Analyses
Cross-tabulation was used to inform on 12-month prevalence of DSM-5 IGD and ICD-11 GD, without and with impairment, in the total sample. A binomial exact confidence interval (CI)17 was computed for the prevalence of gaming, and kappa values were computed as a measure of agreement for DSM-5 IGD and ICD-11 GD that were interpreted according to the following values: below 0.0, poor; 0.00 to 0.20, slight; 0.21 to 0.40, fair; 0.41 to 0.60, moderate; 0.61 to 0.80, substantial; and 0.81 to 1.00, almost perfect.17 Associations between IGD+ and IGD− cases with key variables were estimated with cross-tabulation and multivariate logistic regression models, controlling for gender, age, education, and number of IGD symptoms18 which were performed for the subsample of DSM-5 cases. To assess the performance of the IGD+ and IGD− scale, we followed the usual set of steps used in modern nosological work.19 That included the determination of (1) internal consistency, where appropriate internal consistency was assessed with α values between 0.7 and 0.9,20 and (2) dimensionality, assessed through factor analysis with the presence of only one eigenvalue > 1, examination of the scree plot and adequate model fit indices: Comparative Fit Index or Tucker-Lewis Index ≥ 0.95 and root mean square error approximation ≤ 0.06. Once unidimensionality was confirmed, we fit a 2-parameter logistic (2PL) IRT model for dichotomous traits in order to assess difficulty and discrimination of items and to plot their corresponding item information curves (IIC) and item characteristics curves. Akaike and Bayesian information criteria (AIC and BIC), as well as sample-size-corrected BIC are reported as fit indices for this 2PL model.21
Differential item functioning (DIF) analysis for IGD+ and IGD− was performed for 2 key demographic variables: gender (not males vs. males) and age-group (18 to 19 vs. ≥20 years old). DIF analysis allows determining whether subgroups experience differences in item difficulty or discrimination at the same level of the latent trait being measured. In other words, DIF is a procedure to inform if individuals in different subgroups (e.g., males or females) are more likely (or less likely) to endorse different criteria while holding constant underlying trait severity. We performed the IRT assessment of DIF for each of the 9 IGD criteria, and we also computed tests of DIF for all items jointly. IRT-based DIF assessment is considered a more sensitive method for short scales than the classical methods based on observed scores.22 Factor analysis and IRT models were conducted with Mplus 7.4,21 DIF analysis based on IRT models was computed in PARSCALE,22 and all other statistical analyses were conducted using Stata software version 13.1.23
Results
Table 2 provides the 12-month prevalence of DSM-5 and ICD-11 gaming according to both manuals, with and without impairment. Prevalence of DSM-5 IGD was 5.2% (n = 367; 95% CI, 4.7 to 5.8); prevalence of ICD-11 GD was 2.7% (n = 191; 95% CI, 2.4 to 3.1). Among DSM-5 cases (n = 367), ICD detected a total of 178 cases (48.5%; IGD+) and, so, 189 DSM-5 cases (51.5%) would go undetected (IGD−). Kappa was substantial (0.625). Adding the requirement of severe role impairment in the definition of case would greatly reduce the 12-month prevalence in both the DSM-5 condition (0.74% and 95% CI, 0.56 to 0.97; n = 52) and the ICD-11 diagnosis (0.46% and 95% CI, 0.31 to 0.65; n = 32). With impairment, DSM-5 would have less but still an important proportion of undetected cases (42.3%) by the ICD-11 definition, and kappa was increased (0.713). Considering only the active gamers subsample (n = 2,547), the 12-month prevalence of DSM-5 IGD without impairment was 14.4% (95% CI, 13.1 to 15.8) and the correspondent prevalence for ICD-11 GD was 7.5% (95% CI, 6.5 to 8.6; data not shown).
Table 2.
Cross-Tabulation of DSM-5 IGD by ICD-11 GD, without and with Applying Impairment Criteria.
| Without Applying Impairment Criteria | With Application of Impairment Criteria | |||||
|---|---|---|---|---|---|---|
| ICD-11 GD | ICD-11 GD | |||||
| Negative | Positive | Total | Negative | Positive | Totala | |
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |
| DSM-5 IGD | ||||||
| Negative | 6,642 (94.6) | 13 (0.2) | 6,655 (94.8) | 6,934 (99.2) | 2 (0.1) | 6,936 (99.2) |
| Positive | 189 (2.7) | 178 (2.5) | 367 (5.2) | 22 (0.3) | 30 (0.4) | 52 (0.7) |
| Total | 6,831 (97.3) | 191 (2.7) | 7,022 (100) | 6,956 (99.5) | 32 (0.5) | 6,988 (100) |
Source: PUERTAS Study, 2017 to 2018.
a Not all frequencies add up to the total sample size due to missing values.
We compared IGD+ and IGD− for differences in demographics, comorbid psychopathology, the impairment domains of home management/chores, college-related and other work, close personal relationships, and social life and the total Sheehan scale, and service use profiles. In unadjusted cross-tabulations, no statistically significant differences emerged except for a higher probable alcohol dependence (P = 0.035) among IGD+ cases. IGD− cases were more likely to spend more days per week playing video games (P = 0.032), but IGD+ cases showed higher mean number of gaming symptoms (7.2 mean symptoms vs. 5.5 mean symptoms; P < 0.001) and a larger percentage of severe cases (43.8% of IGD+ were severe cases but only 3.2% of IGD− were severe; = 109.2; P < 0.001; data not shown). In Table 3, we present a comparison of IGD+ and IGD− cases on key demographic variables in a multiple logistic regression model that controls for gender, age, maximum parental education, days per week playing video games, and number of gaming symptoms. In these models, both types of cases were similar in severe impairment, lifetime service use, and psychopathology, with the exception that drug abuse/dependence was more present among IGD+ cases (OR = 6.84; 95%CI, 1.20 to 38.79).
Table 3.
Association of Mental Disorders, Suicide Ideation, Impairment, and Treatment, with ICD-11 GD (IGD+) among Those with DSM-5 IGD.
| Main Independent Variablesa | AOR | 95% CI |
|---|---|---|
| Alcohol probable dependence 12-month (ref: no) | 2.01 | (0.74 to 5.48) |
| Drug abuse/dependence 12-month (ref: no) | 6.84* | (1.20 to 38.79) |
| Major depressive episode 12-month (ref: no) | 0.86 | (0.43 to 1.71) |
| Generalized anxiety disorder 12-month (ref: no) | 1.02 | (0.17 to 6.10) |
| Suicidal ideation 12-month (ref: no) | 1.16 | (0.60 to 2.23) |
| Severe disability: Total (ref: no) | 1.17 | (0.55 to 2.49) |
| Lifetime any treatment (ref: no) | 0.84 | (0.44 to 1.60) |
Note. n = 367; AOR = adjusted odds ratio; CI = confidence interval.
Source: Puertas Study, 2018 to 2019.
a Each row from a model that included controls for sex, age (continuous), maximum parental education (categorical), days per week playing video games, and number of DSM symptoms (continuous).
*P < 0.05.
Symptom profiles for cases of DSM-5 IGD and ICD-11 GD among active gamers were further examined within IRT analyses. Firstly, unidimensionality was observed for both types of cases with adequate fit indices, but only for those IGD+, the α value was considered adequate (0.813; see Supplementary Table S1). The two symptoms with higher discrimination among IGD− cases were “continuation” and “tolerance,” while for IGD+ cases, they were “giving up activities” and “negative consequences”; the items with higher difficulty were “negative consequences” and “loss of control” for IGD− cases, and “withdrawal” and “negative consequences” for IGD+ cases (Table 4). Examination of IIC for DSM-5 IGD (Figure 1: upper panel) and ICD-11 GD (Figure 1: lower panel) suggest that in both cases, symptoms from SU and G mix through the IGD continuum, where SU items provide the most information at lower levels of the latent trait, while “negative consequences” provide more information at higher levels. Finally, “continuation” is more informative for IGD+ than for IGD−.
Table 4.
Item Response Theory (IRT) Analysis of DSM-5 IGD and ICD-11 GD among Active Gamers.
| IRT Parameters | ||||
|---|---|---|---|---|
| DSM (n = 2,369)a | ICD (n = 2,358)b | |||
| Discrimination (SE) | Difficulty (SE) | Discrimination (SE) | Difficulty (SE) | |
| Criterion | ||||
| 1. Preoccupation (G) | 1.60 (0.11) | 0.01 (0.04) | 1.50 (0.10) | 0.02 (0.04) |
| 2. Withdrawal | 1.62 (0.15) | 2.24 (0.13) | 2.14 (0.17) | 1.88 (0.08) |
| 3. Tolerance | 2.13 (0.15) | 1.01 (0.05) | 2.02 (0.12) | 1.03 (0.05) |
| 4. Loss of control | 0.90 (0.09) | 2.99 (0.26) | 2.73 (0.21) | 1.27 (0.05) |
| 5. Giving up activities | 1.65 (0.12) | 1.63 (0.08) | 3.05 (0.23) | 1.11 (0.04) |
| 6. Continuation | 2.20 (0.16) | 0.56 (0.04) | 2.52 (0.17) | 0.51 (0.03) |
| 7. Deception (G) | 1.78 (0.15) | 2.07 (0.11) | 2.48 (0.20) | 1.70 (0.07) |
| 8. Escape (G) | 1.70 (0.11) | 1.05 (0.05) | 1.64 (0.10) | 1.07 (0.06) |
| 9. Negative consequences (G) | 1.88 (0.22) | 2.52 (0.17) | 2.95 (0.30) | 1.97 (0.08) |
| Model fit indices | ||||
| AIC | 15,577.3 | 15,286.9 | ||
| BIC | 15,681.1 | 15,390.7 | ||
| SS-BIC | 15,623.9 | 15,333.5 | ||
Note. AIC = Akaike information criterion; BIC = Bayesian information criterion; SS-BIC: sample-size-corrected BIC; SE = standard error; G = item from the DSM-IV Gambling Disorder Criteria.
Source: PUERTAS Study, 2018 to 2019.
a n = 2,369 active gamers from 189 DSM cases (negative to ICD) and 2,180 noncases (see Table 2 for case details).
b n = 2,358 active gamers from 191 ICD cases and 2167 noncases (see Table 2 for case details).
Figure 1.
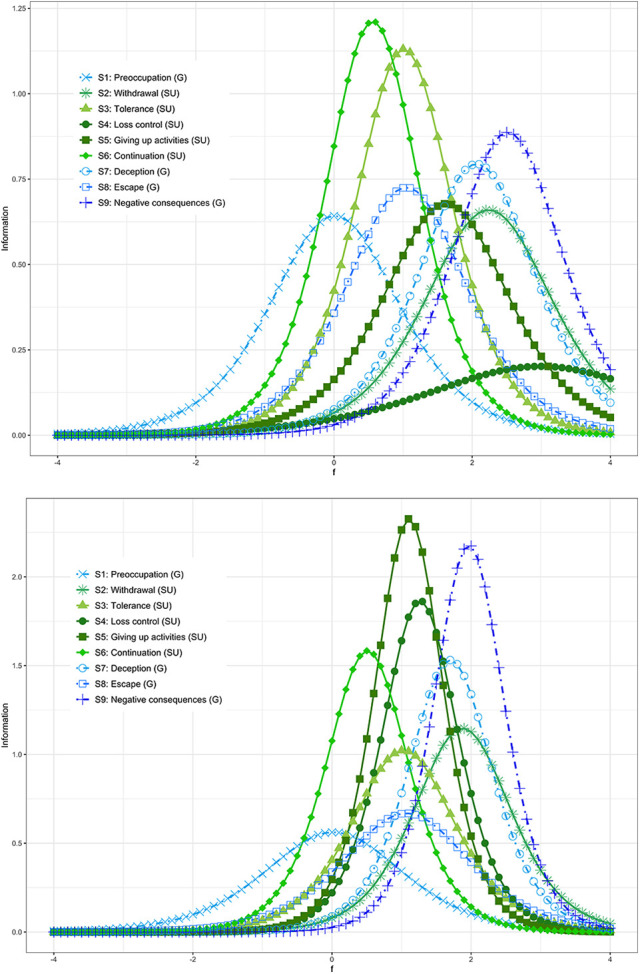
Item information curves (IIC). The upper panel shows DSM-5 IIC, while the lower panel shows ICD-11 IIC.
We examined the possible presence of DIF, in the discrimination and difficulty parameters, for age and gender in both types of cases. DIF was present for both types of cases for gender (P < 0.001). For age-group, in the case of IGD−, DIF was not present in the discrimination estimate, but it was present in the difficulty estimates (= 28.8; P = 0.001); among IGD+, DIF was present in the discrimination parameters ( = 60; P < 0.001; Supplementary Table 2).
Discussion
In this report, we provide novel information for understanding the empirical differences and similarities between the newly introduced DSM and ICD conceptualizations of a GD and how this might impact case detection and by extension treatment eligibility. In summary, we found that the 12-month prevalence of gaming is almost twice as high when determined by DSM-5 criteria than ICD-11 criteria, and while adding an impairment requirement diminishes both estimates, prevalence remains larger in DSM-5. It is noteworthy that while almost all of ICD-11 GD cases are detected by the DSM-5 IGD criteria, less than half of DSM-5 IGD cases are detected by ICD-11 GD criteria. We found that DSM-5 cases detected and undetected by the ICD-11 GD definition were similar in most variables with the exception that detected cases were more severe in number of symptoms and more likely to have probable drug abuse/dependence. Symptom profiles of detected and undetected cases were also similar, with substance use symptoms providing information at lower levels of the latent trait, while the negative consequences symptom provides the most information at higher levels. We found evidence of DIF for gender in both classifications, suggesting that psychometric work is further needed on the performance of questionnaires for GD among males and females, a matter much neglected in the field.5
This is the first study, of which we are aware, that provides 12-month prevalence estimates for ICD-11 GD in a nonclinical or online self-selected population. In this sample of college students, the ICD-11 almost halves the corresponding DSM-5 IGD prevalences. Lower detection rates when using ICD-11 for GDs were also reported for a clinical sample of children and adolescents in Korea.11 The reason for this reduction is that ICD-11 focus exclusively on 3 main core addictive symptoms that are the same symptoms used to describe alcohol use disorders10 and gambling disorders.24 It could be that by adapting a definition in accordance with other addictive disorders, cases of ICD-11 GD turn out to be more comorbid with probable drug abuse/dependence cases than undetected cases. No other excess in mental comorbidities was found. By focusing exclusively on a core group of symptoms from substance use disorders, the ICD may be missing some additional information by not measuring negative consequences and some of the gambling items. Further research in this area is sorely needed. The good news (glass half full) is that while IGD+ cases tend to have more DSM-5 symptoms than IGD− cases, detected and undetected cases are very similar in sociodemographics characteristics, comorbid psychopathology (with the exception drug use disorders previously mentioned), impairment, and service use. So, in general, by applying ICD-11 criteria, we are not missing more severe DSM-5 cases. On the other hand, the bad news (glass half empty) is that since IGD+ and IGD− cases are so similar, by using ICD-11 instead of DSM-5, we may be leaving (similarly) affected people underserved. As a recent discussion on the different estimates of prevalence of alcohol use disorders by using DSM-5 and ICD-11 shows,25,26 it is unlikely that purely epidemiological studies can solve this discrepancy.
Limitations
Prevalence estimates are based on a convenience sample of Mexican colleges where students participated on a voluntary basis, limiting generalizability of results, and were obtained using a self-report web-based survey rather than a comprehensive clinical diagnostic interview and therefore should be considered a screening of possible cases rather than a confirmed diagnosis of gaming for both the DSM-5 and the ICD-11. The universities included were both public and private, but they were not randomly selected and therefore the study participants are not representative of all university students in Mexico. They are nevertheless representative of 1st-year students of the participating universities. Also, Mexicans youth not attending universities and without access to Internet or devices to play video games were beyond our sample frame. While these findings are also not generalizable to other populations, they are of interest globally given the large migration of Mexicans to other countries such as Canada and the lack of data in nonclinical samples. In addition, the IGD and GD scales were not validated by a clinical interview for Mexican youth specifically. The severity levels for DSM-5 IGD were based exclusively on symptom count and have not been validated previously. Finally, impairment in the survey was measured using the Sheehan Disability Scale that is not anchored to any specific mental disorder (including gaming).
Future studies on the clinical validity of epidemiological instruments such as the one reported here, with both DSM-5 and ICD-11 criteria, and longitudinal responses to key risk factors, to treatment and reducing disability are areas for further improvement. There is a need to replicate our findings, particularly among younger adolescents and those living in high-income countries, such as Canada, where the availability of Internet gaming is pervasive. Furthermore, the study of GD must continually adapt to changes in technology as these changes may well impact the diagnostic construct. The introduction of GD in ICD-11 brings the possibility of treating a considerable number of affected persons, and more research is needed on treatment options.27
Conclusion
Despite these limitations, our data have important implications for public health policy and treatment as they suggest large differences in prevalence of gaming depending upon whether the DSM-5 or the ICD-11 criteria are used, with the first one detecting twice as many cases. Because the DSM-5 cases that are undetected by ICD-11 are so similar to the detected cases, there seems to be little clinical justification for treating one group over the other and thus the DSM-5 cases that would go undetected by using ICD-11 definition may go underserved.
Supplemental Material
Supplementary_material for (Internet) Gaming Disorder in DSM-5 and ICD-11: A Case of the Glass Half Empty or Half Full: (Internet) Le trouble du jeu dans le DSM-5 et la CIM-11: Un cas de verre à moitié vide et à moitié plein by Guilherme Borges, Ricardo Orozco, Corina Benjet, Kalina I. Mart´ınez Mart´ınez, Eunice Vargas Contreras, Ana Lucia Jim´enez P´erez, Alvaro Julio Pel´aez Cedr´es, Praxedis Cristina Hern´andez Uribe, Mar´ıa Anabell Covarrubias D´ıaz Couder, Ra´ ul A. Gutierrez-Garcia, Guillermo E. Quevedo Ch´avez, Yesica Albor, Enrique Mendez, Maria Elena Medina-Mora, Philippe Mortier and Jos´e Luis Ayuso-Mateos in The Canadian Journal of Psychiatry
Acknowledgments
The survey was carried out in conjunction with the WHO World Mental Health International College Surveys Initiative (WHO WMH-ICS). The authors thank the WHO WMH-ICS collaborators and staff for assistance with instrumentation.
Authors’ Note: The initial draft of this article was prepared by GB in cooperation with RO and CB. CB was responsible for obtaining funding. GB, CB, MEMM, RAGG, YA, JLA, and PM participated in the study concept and design. YA and RAGG coordinated the universities and supervised the study implementation. KIMM, EVC, ALJP, AJPC, PCHU, GEQC, and ACD implemented the study in their universities. GB, RO, and EM participated in the analysis and interpretation of data. All authors reviewed and approved the final version of the article. The Research Ethics Committee of the National Institute of Psychiatry approved the research protocol. Participation was anonymous and voluntary. Informed consent was obtained from participants through the web platform. Only those aged 18 or above were eligible to participate. For all participants who answered affirmatively to depressive symptomatology, alcohol or drug problems, any and all suicidal behavior or nonsuicidal self-injury and those experiencing an extremely stressful event in the prior year, an automatic message was displayed providing them with information of where they could obtain professional help. University-based, community-based and online options were provided.
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Benjet received support from the National Council on Science and Technology (CONACyT; CB 285548) and the Fundación Miguel Alemán A.C. Philippe Mortier has a Sara Borrell contract awarded by the ISCIII (CD18/00049), and received funding from the Generalitat de Catalunya (2017 SGR 452) and the Belgian Fund for Scientific Research (11N0514N/11N0516 N).
ORCID iD: Guilherme Borges  https://orcid.org/0000-0002-3269-0507
https://orcid.org/0000-0002-3269-0507
Ricardo Orozco
https://orcid.org/0000-0002-6580-585X
Supplemental Material: The supplemental material for this article is available online.
References
- 1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5 1 ed. American Psychiatric Publishing; 2013. [Google Scholar]
- 2. Petry N, Rehbein F, Douglas A, et al. An international consensus for assessing internet gaming disorder using the new DSM-5 approach. Addiction. 2014;109(9):1399–1406. [DOI] [PubMed] [Google Scholar]
- 3. Feng W, Ramo DE, Chan SR, Bourgeois J. Internet gaming disorder: trends in prevalence 1998-2016. Addict Behav. 2017;75:17–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Fam J. Prevalence of internet gaming disorder in adolescents: a meta-analysis across three decades. Scand J Psychol. 2018;59(5):524–531. [DOI] [PubMed] [Google Scholar]
- 5. King D, Chamberlain S, Carragher N, et al. Screening and assessment tools for gaming disorder: a comprehensive systematic review. Clin Psychol Rev. 2020;77:711–720. [DOI] [PubMed] [Google Scholar]
- 6. WHO | Gaming disorder. 2018. [accessed 2019 Dec 14]. https://www.who.int/features/qa/gaming-disorder/en.
- 7. Saunders J, Hao W, Long J, et al. Gaming disorder: its delineation as an important condition for diagnosis, management, and prevention. J Behav Addict. 2017;20(3):271–279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Rumpf H, Achab S, Billieux J, et al. Including gaming disorder in the ICD-11: the need to do so from a clinical and public health perspective. J Behav Addict. 2018;7(3):556–561. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Borges G, Orozco R, Benjet C, et al. DSM-5 Internet gaming disorder among a sample of Mexican first-year college students. J Behav Addict. 2019;8(4):131–211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Saunders J, Degenhardt L, Geoffrey M, Vladimir P. Alcohol use disorders in ICD-11: past, present, and future. Alcohol Clin Exp Res. 2019;43(8):1617–1631. [DOI] [PubMed] [Google Scholar]
- 11. Jo Y, Bhang S, Choi J, Hae Kook L, Seung YL, Yong Sil K. Clinical characteristics of diagnosis for internet gaming disorder: comparison of DSM-5 IGD and ICD-11 GD diagnosis. J Clin Med. 2019;8(7):945. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Benjet C, Gutiérrez-García R, Abrego-Ramírez A, et al. Psychopathology and self-harm among incoming first-year students in six Mexican universities. Salud Publica Mex. 2019;61(1):16–26. [DOI] [PubMed] [Google Scholar]
- 13. Petry N, Rehbein F, Ko C, O’Brien CP. Internet gaming disorder in the DSM-5. Curr Psychiatry Rep. 2015;17(9):72. [DOI] [PubMed] [Google Scholar]
- 14. Leon A, Olfson M, Portera L, Farber L, Sheehan DV. Assessing psychiatric impairment in primary care with the Sheehan disability scale. Int J Psychiatry Med. 1997;27(2):93–105. [DOI] [PubMed] [Google Scholar]
- 15. Ormel J, Petukhova M, Chatterji S, et al. Disability and treatment of specific mental and physical disorders across the world. Br J psychiatry. 2008;192(5):368–375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Alonso J, Vilagut G, Mortier P, et al. The role impairment associated with mental disorder risk profiles in the WHO world mental health international college student initiative. Int J Methods Psychiatr Res. 2018;28(2):3–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Stata Corp. Stata 13: Base Reference Manual [Computer software]. [Google Scholar]
- 18. Hosmer D, Lemeshow S. Applied logistic regression. 2nd ed. Hoboken (NJ): Wiley & Sons; 2000. [Google Scholar]
- 19. Shmulewitz D, Keyes KM, Wall MM, et al. Nicotine dependence, abuse and craving: dimensionality in an Israeli sample. Addiction. 2011;106(9):1675–1686. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Streiner D, Geoffrey R. Health measurement scales: a practical guide to their development and use. 2nd ed. Oxford University Press; 1995: p. 399. [Google Scholar]
- 21. Muthén L, Muthén B. MPlus: statistical analysis with latent variables: user’s guide. 7 ed. Los Ángeles, California: Muthén & Muthén; 2015. [Google Scholar]
- 22. Du Toit M. (editor). IRT from SSI: Bilog-MG, multilog, parscale, testfact. Lincolnwood, Illinois: Scientific Software International; 2003. [Google Scholar]
- 23. Stata Corp. Stata Statistical Software. Release 13.1 [Computer software]; 2014. [Google Scholar]
- 24. ICD-11—Mortality and Morbidity Statistics. 2019. [accessed 2019 Dec 14]. https://icd.who.int/browse11/l-m/en#/http%3A%2F%2Fid.who.int%2Ficd%2Fentity%2F1041487064.
- 25. Degenhardt L, Bharat C, Bruno R, et al. Concordance between the diagnostic guidelines for alcohol and cannabis use disorders in the draft ICD-11 and other classification systems: analysis of data from the WHO’s world mental health surveys. Addiction. 2019;114(3):534–552. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Room R, Rehm J. Harm to others does matter in substance use disorders, and so does discordance between the diagnostic systems. Addiction. 2019;114(3):553–554. [DOI] [PubMed] [Google Scholar]
- 27. King D, Delfabbro P. Video game addiction. In: Press A, editor. Video game addiction, in principles addiction: comprehensive addictive behaviors and disorders. San Diego, California: Elsevier Inc; 2018:1–294. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary_material for (Internet) Gaming Disorder in DSM-5 and ICD-11: A Case of the Glass Half Empty or Half Full: (Internet) Le trouble du jeu dans le DSM-5 et la CIM-11: Un cas de verre à moitié vide et à moitié plein by Guilherme Borges, Ricardo Orozco, Corina Benjet, Kalina I. Mart´ınez Mart´ınez, Eunice Vargas Contreras, Ana Lucia Jim´enez P´erez, Alvaro Julio Pel´aez Cedr´es, Praxedis Cristina Hern´andez Uribe, Mar´ıa Anabell Covarrubias D´ıaz Couder, Ra´ ul A. Gutierrez-Garcia, Guillermo E. Quevedo Ch´avez, Yesica Albor, Enrique Mendez, Maria Elena Medina-Mora, Philippe Mortier and Jos´e Luis Ayuso-Mateos in The Canadian Journal of Psychiatry