

Abstract
J Clin Hypertens (Greenwich). 2012;14:792–798. ©2012 Wiley Periodicals, Inc.
Heavy alcohol intake increases the risk of hypertension, but the relationship between light to moderate alcohol consumption and incident hypertension remains controversial. The authors sought to analyze the dose‐response relationship between average daily alcohol consumption and the risk of hypertension via systematic review and meta‐analysis. Electronic databases were searched for prospective control studies examining quantitative measurement of alcohol consumption and biological measurement of outcome. The primary endpoint was the risk of developing hypertension based on alcohol consumption. The level of alcohol consumption from each study was assigned to categorical groups based on the midpoint of their alcohol consumption classes to make possible the comparison of heterogeneous classification of alcohol intake. A total of 16 prospective studies (33,904 men and 193,752 women) were included in the analysis. Compared with nondrinkers, men with alcohol consumption with <10 g/d and 11 to 20 g/d had a trend toward increased risk of hypertension (relative risk [RR], 1.03; 95% confidence interval [CI], 0.94–1.13; P=.51) and (RR, 1.15; 95% CI, 0.99–1.33; P=.06), respectively, whereas a significantly increased risk of hypertension was found with heavy alcohol consumption of 31 to 40 g/d (RR, 1.77; 95% CI, 1.39–2.26; P<.001) and >50 g/d (RR, 1.61; 95% CI, 1.38–1.87; P<.001). Among women, the meta‐analysis indicated protective effects at <10 g/d (RR, 0.87; 95% CI, 0.82–0.92; P<.001) and a trend toward decreased risk of hypertension with alcohol consumption 11 to 20 g/d (RR, 0.9; 95% CI, 0.87–1.04; P=.17), whereas a significantly increased risk of hypertension was indicated with heavy alcohol consumption of 21 to 30 g/d (RR, 1.16; 95% CI, 0.91–1.46; P=.23) and 31 to 40 g/d (RR, 1.19; 95% CI, 1.07–1.32; P=.002). In men, heavy alcohol consumption is associated with increased risk of hypertension, whereas there is a trend toward increased risk of hypertension with low and moderate alcohol consumption. The relationship between alcohol consumption and hypertension is J‐shaped in women. Limiting alcohol intake should be advised for both men and women.
Hypertension is a prevalent condition that affects approximately 65 million individuals in the United States based on a preliminary report from the National Health and Nutrition Examination Survey (NHANES) 2005–2006 and coincident US population estimates. 1 Due to its increasing clinical and public health importance, examining the risks or benefits of alcohol consumption in patients with hypertension is needed to assist clinicians in developing appropriate strategies of prevention. In observational studies, moderate alcohol consumption has been associated with lower incidence of cardiovascular diseases such as coronary artery disease, stroke, heart failure, and peripheral vascular disease. 2 , 3 , 4
Epidemiologic evidence suggests that heavy alcohol consumption is strongly associated with increased risk of hypertension. 5 , 6 However, the effects of light to moderate alcohol intake on blood pressure (BP) remain unclear and controversial. Some previous studies have reported a linear association between alcohol intake and BP among men, 7 , 8 while others have reported a threshold only above which there is an association in both men and women, 9 , 10 and still others a J‐ or U‐shaped association among women, 11 , 12 with the nadir among light to moderate alcohol drinkers. These inconclusive results may have resulted in part from ethnic or lifestyle differences in the study populations but also may have been strongly influenced by different methods used to investigate the association between alcohol intake and BP. The objective of the present study was to perform a systematic review and meta‐analysis of the published prospective studies to separately assess the risk of development of hypertension over a long‐term period among men and women based on their levels of alcohol consumption.
Materials and Methods
Search Strategy
We systematically searched the electronic databases MEDLINE, PubMed, Embase, and the Cochrane Library for Central Register of Clinical Trials using the MESH terms “alcohol,”“hypertension,”“blood pressure,” and the names of individual alcoholic beverages. We limited our search to studies in human subjects and English language in peer‐reviewed journals from 1990 to May 2012. Additionally, a manual search of all relevant references from the screened articles and reviews was performed for additional clinical studies (Figure 1).
Figure 1.
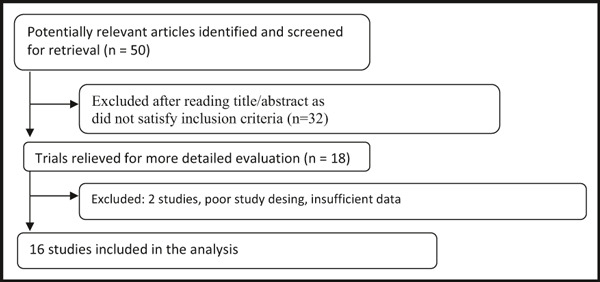
Preferred Reporting Items for Systematic Reviews and Meta‐Analyses (PRISMA) flow diagram of study selection.
Study Selection
Eligible studies included (1) prospective studies assessing the effects of alcohol consumption on long‐term risk of hypertension; (2) studies reporting outcomes of interest, including number of patients who developed hypertension; and (3) at least 3 different nonoverlapping levels of drinking categories to allow estimation of dose‐response relationship; and (4) studies with at least 1 year of follow‐up in each study arm. Exclusion criteria included (1) persons who consumed alcohol used as controls; (2) absence of quantitative description of endpoints; (3) lack of clear and reproducible results; and (4) studies in the abstract form without a published manuscript in a peer‐reviewed journal.
Data Extraction and Quality
The data was independently extracted by two authors (V.A. and A.B.) using standardized protocol, and reporting form disagreements were resolved by arbitration (F.M.) and consensus was reached after discussion. We extracted characteristics of each study (type of design with duration of alcohol consumption and methods), baseline demographics, number of individuals in different drinking categories, number of patients who developed hypertension in different drinking categories for our analysis. Authors of the papers were individually contacted in case the data were unclear.
Outcomes Assessed
Our primary outcome was the effect of different alcohol consumption categories on the long‐term risk of developing hypertension.
Definition of Different Alcohol Consumption Categories
Measurement of alcohol consumption varied among studies. The definition of different categories of alcohol consumption (light, moderate, and heavy) differed substantially among studies. It was based on the amount of alcohol in grams per day (g/d), per week or per month, or the frequency of alcohol consumption per day. Several studies reported alcohol data by using a standard unit of alcohol measurement, called “drinks,” which contained varying amount of alcohol and differed from country to country. Therefore, to obtain meaningful results in terms of risk assessment, it was important to carefully define the categories of alcohol consumption. In order to facilitate direct comparison between studies, alcohol consumption data were converted into the same unit (g/d). If a study did not provide data about the quantity of alcohol equivalent to a standard drink, the average alcohol consumption was assumed to be 12 g per drink in studies performed in the United States, 10 g per drink in studies carried out in the United Kingdom and Europe, and 21.2 g per drink in Japan. 13
Data Analysis and Synthesis
An intention‐to‐treat traditional meta‐analysis was performed in line with recommendations from the Cochrane Collaboration, the Preferred Reporting Items for Systematic Reviews and Meta‐Analyses (PRISMA) Statement, and the Meta‐Analysis of Observational Studies in Epidemiology (MOOSE) guidelines. All analyses were performed by performed by metan command of Stata 10.1 (StataCorp, College Station, TX). Heterogeneity was assessed with the I 2 statistic, with I 2 <25% considered low and I 2 >75% considered high. The association between the risk of development of hypertension and amount of alcohol intake was calculated separately for each alcohol consumption category for men and women separately by treating the nondrinker group as the reference group. Since we expected individual studies to differ in baseline patient characteristics, type and amount of alcohol consumption, and the length of follow‐up, we decided a priori to use a DerSimonian–Laird random‐effects model for relative risk (RR) estimation for all outcomes. Reported values are two‐tailed, and hypothesis testing results were considered statistically significant at P≤.05. Small study effect, including publication bias, was tested using funnel plot and Egger test. We separately analyzed the effects of alcohol consumption on the two sexes.
Based on their daily alcohol intake, men were categorized into 7 drinking categories based on increments of 10 g/d of alcohol consumption: abstainers (nondrinkers), <10 g/d, 10 to 20 g/d, 20 to 30 g/d, 30 to 40 g/d, 40 to 50 g/d, and >50 g/d. Similarly, women were categorized into 5 groups: abstainers (nondrinkers), <10 g/d, 10 to 20 g/d, 20 to 30 g/d, and 30 to 40 g/d. We assigned the level of alcohol consumption from each study to these groups based on the midpoint of the upper and lower boundaries in each category as the average intake. This categorization of alcohol drinking makes possible the comparison of heterogeneous classification of alcohol intake among the different studies and at the same time allows inclusion of data from studies in which precise information on levels of alcohol consumption were not available. When the upper bound of the highest category was not specified, we used the range of the previous reported category. The alcohol habits were assumed to be stable during the follow‐up period.
One of the largest prospective cohort studied, conducted by Klatsky colleagues, 14 was not included in our analysis. The authors studied cardiovascular effects of alcohol separately in heavy drinkers (>3 drinks per day), light drinkers (<2 drinks per day), exdrinkers, and abstainers among 127,212 patients for 13.5 years. Although the authors did not report data separately on men and women, they concluded that any drinking level is far from benign and is associated with increased risk of hypertension and adverse cardiovascular outcomes.
Results
Study Selection and Baseline Characteristics
Based on our search strategy, we initially identified 50 potential relevant articles. Based on our inclusion criteria, 33 articles were rejected. Of the 17 remaining articles, the study by Klatsky colleagues was excluded because it did not separately report the effects of alcohol consumption on men and women 14 (Figure 1). This approach enabled us to minimize the bias related to differences other than alcohol consumption between individuals. Of these 16 articles, one included data on hypertension risk in both men and women. We identified 16 prospective cohort studies including 33,904 men and 193,752 women who recorded their drinking habits and evaluated the risk of developing hypertension (I, II). This difference in the overall number of men and women is due to the predominantly female population in the studies by Ascherio colleagues, 15 Sesso colleagues, 16 Thadhani colleagues, 17 and Witteman colleagues. 18 The average follow‐up duration was 7.6 years for women and 9.8 years for men.
Table I.
Characteristics of Included Studies That Examined the Association Between Alcohol Consumption and Hypertension in Men
| Author | Year | Type of Study | Country | Age, y | Participants, No. | Hypertensive Patients, No. | Follow‐up, y |
|---|---|---|---|---|---|---|---|
| Halanych 19 | 2010 | Prospective cohort | United States | 24.8 | 4711 | 941 | 20 |
| Sesso 16 | 2008 | Prospective cohort | United States | 52.2 | 13,455 | 6012 | 17 |
| Stranges 20 | 2004 | Prospective cohort | United States | 56.1 | 2609 | 592 | 6 |
| Ohmori 21 | 2002 | Prospective cohort | Japan | 50 | 413 | 120 | 10 |
| Tsuruta 22 | 2000 | Prospective cohort | Japan | 49.5 | 325 | 93 | 12 |
| Yamada 23 | 1991 | Prospective cohort | Japan | 42.6 | 1393 | 77 | 5 |
| Saremi 24 | 2004 | Prospective cohort | United States | 37 | 1551 | 422 | 14 |
| Curtis 8 | 1997 | Prospective cohort | United States | 34.8 | 488 | 131 | 5 |
| Fuchs 5 | 2001 | Prospective cohort | United States | 53.6 | 3553 | 601 | 6 |
| Nakanishi 25 | 2002 | Prospective cohort | Japan | 23–60 | 5275 | 798 | 4 |
| Nakanishi 26 | 2001 | Prospective cohort | Japan | 43.2 | 1310 | 458 | 9 |
Table II.
Characteristics of Included Studies That Examined the Association Between Alcohol Consumption and Hypertension in Females
| Author | Year | Type of Study | Country | Age, y | Control Patients, No. | Hypertensive Patients, No. | Follow‐up, y |
|---|---|---|---|---|---|---|---|
| Ascherio 15 | 1996 | Prospective cohort | United States | 30–55 | 150,522 | 2526 | 4 |
| Sesso 16 | 2008 | Prospective cohort | United States | 53.4 | 28,848 | 8680 | 9.8 |
| Thadani 17 | 2002 | Prospective cohort | United States | 35.3 | 70,891 | 4188 | 8 |
| Wiiteman 18 | 1989 | Prospective cohort | United States | 30–55 | 58,218 | 3320 | 4 |
| Saremi 24 | 2004 | Prospective cohort | United States | 36.7 | 2240 | 395 | 14 |
| Fuchs 5 | 2001 | Prospective cohort | United States | 52.6 | 4584 | 654 | 6 |
| Klatsky 20 | 2006 | Prospective cohort | United States | 50 | 74,441 | 26,340 | 13.5 |
The study by Klatsky and colleagues included a predominantly female population.
Effects of Different Alcohol Consumption Categories on Hypertension Risk
In men, the random‐effects model showed a significantly increased risk of hypertension with alcohol consumption of 31 to 40 g/d (RR, 1.77; 95% confidence interval [CI], 1.39–2.26; P<.001) and >50 g/d (RR, 1.61; 95% CI, 1.31–1.87; P<.001). There was a trend towards increased risk of hypertension with alcohol consumption of <10 g/d (RR, 1.03; 95% CI, 0.94–1.13; P=.51), 11 to 20 g/d (RR, 1.15; 95% CI, 0.99–1.33; P=.06), 21 to 30 g/d (RR, 1.07; 95% CI, 0.86–1.34; P=.54), and 41 to 50 g/d (RR, 1.17; 95% CI, 0.84–1.65; P=.34) (2, 3, 4).
Figure 2.
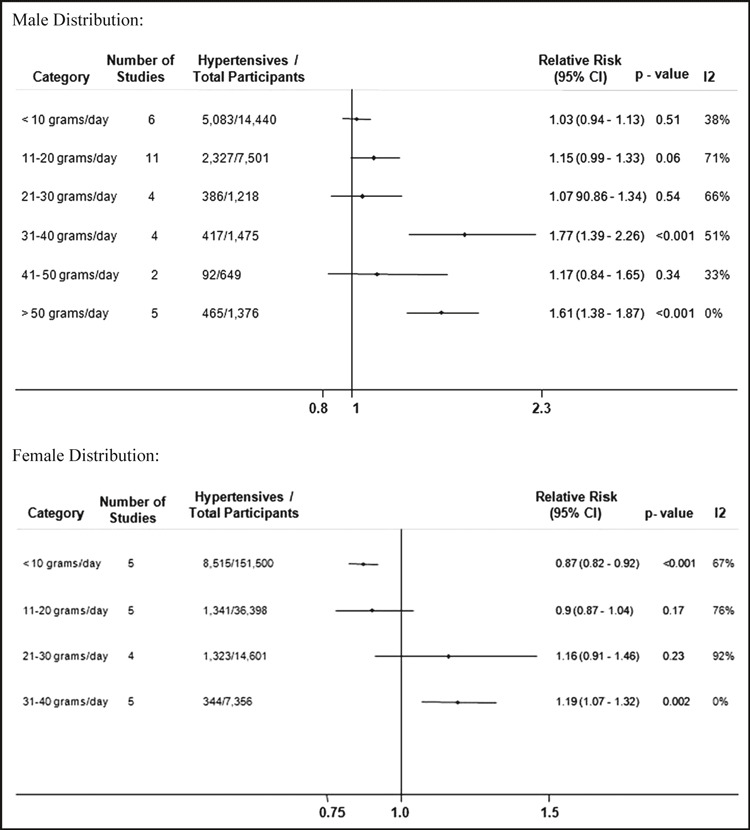
Risk of hypertension in men and women based on different alcohol consumption categories. CI indicates confidence interval.
Figure 3.
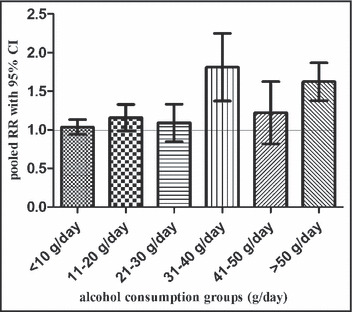
Relationship between average daily alcohol consumption and the risk of hypertension in men. RR indicates relative risk;CI, confidence interval.
Figure 4.
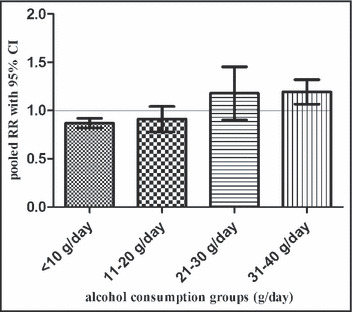
Relationship between average daily alcohol consumption and the risk of hypertension in women. RR indicates relative risk;CI, confidence interval.
In women, the random‐effects model showed a significantly decreased risk of hypertension with alcohol consumption of <10 g/d (RR, 0.87; 95% CI, 0.82–0.92; P<.001) and a trend toward decreased risk of hypertension with alcohol consumption 11 to 20 g/d (RR, 0.9; 95% CI, 0.87–1.04; P=.17). The meta‐analysis revealed a significantly increased risk of hypertension with alcohol consumption of 31 to 40 g/d (RR, 1.19; 95% CI, 1.07–1.32; P=.002) and a trend toward increased risk of hypertension with alcohol consumption of 21 to 30 g/d (RR, 1.16; 95% CI, 0.91–1.46; P=.23).
Despite the methodologic differences with previous meta‐analysis, the results of the present study are similar to those reported by reported by Taylor and colleagues who also showed a modest protective effect of alcohol consumption in women at low doses. 27
Publication Bias
The funnel plots did not show marked asymmetry and all Egger’s tests were not significant.
Discussion
Our results confirmed that irrespective of sex, heavy alcohol intake increases hypertension risk. In our analysis, however, we found that the association between light to moderate alcohol intake and the risk of developing hypertension differed among women and men. Among women, there is a possible J‐shaped association between amount of alcohol intake and the risk of developing hypertension, in which light to moderate alcohol consumption modestly lowered hypertension risk, whereas heavier consumption of >20 g/d significantly increased hypertension risk. Our analysis results are consistent with the results of previous cross‐sectional studies. 7 , 9 , 11 , 12 Among men, the relationship was more linear up to a dose of 40 g/d, after which the risk of development of hypertension appears to plateau. In the present meta‐analysis we used only prospective studies that explored the longitudinal risk of hypertension after long‐term alcohol consumption. We purposely excluded studies of transient effects of alcohol consumption associated commonly with acute alcohol consumption.
The association between light–moderate drinking and reduced risk of cardiovascular disease mortality is established. 2 , 3 , 4 However, the mechanisms underlying any inverse association between light to moderate alcohol consumption and hypertension may differ from those for coronary heart disease, because only women appear to have a reduced risk of hypertension. In men, light to moderate alcohol consumption continued to be associated with higher risk of hypertension.
In both men and women, heavy alcohol consumption has adverse effects on cardiovascular outcomes; however, it is unclear whether there are significant sex differences in this effect. Chronic exposure to alcohol alters the production of this same set of hormones (ie, estrogen and testosterone), and hence alcohol’s effects on the cardiovascular system could involve an indirect mechanism in which alcohol alters hormone levels and, in turn, the hormones affect BP.
Alternatively, differences in the pattern of drinking, beverage choices, and smoking habits may contribute to the observed sex differences. The health effects of drinking may depend on drinking pattern, and failure to differentiate episodic from regular drinkers may obscure real associations. Previous work has shown that substantially more episodic drinking episodes occur among men. Although some cross‐sectional studies suggest that daily drinking is associated with a stronger alcohol‐BP association than episodic drinking, 13 , 28 others do not. 29 Notably, previous studies suggested that the J‐shaped relationship to hypertension may be the result of previously hypertensive individuals lowering their alcohol intake, 11 leading to a falsely elevated risk of hypertension among those considered nondrinkers. As regards the role of different alcoholic beverages, available data suggest that beverage choice has no important independent roleon BP. 30
Limitations
As with other meta‐analyses of published studies, the present analysis has several limitations. First, its quality is inherited from the validity of the original included studies. There was significant heterogeneity among the studies with respect to the design of the studies, the baseline characteristics of the enrolled patients and their comorbidities, amount of alcohol intake, and duration of follow‐up, among others. The studies had variable BP cut‐offs for the diagnosis of hypertension, with two studies using a cut‐off of 160/95 mm Hg for the diagnosis of hypertension, 8 , 23 resulting in a lower number of cases identified. When interpreting these data it must be remembered that there were a variable number of participants in the various categories of alcohol consumption. Hence, while there may be clearly demarcated results in certain categories of alcohol consumption, there was a trend toward increased or decreased risk of hypertension among other groups. A major concern is that the quality of studies examining the cardiovascular risk related to alcohol consumption relies primarily on the accuracy of assessment of alcohol consumption. To date, there is no available consensus for measuring alcohol consumption. The data on alcohol consumption are based on self‐reporting and the method used is not validated in many of the studies. This can lead to the possibility of misclassification of exposure as a result of under‐reporting. However, past epidemiological community‐based studies have shown that self‐reporting alcohol consumption is reliable. 31 Our alcohol consumption quantification method may lack precision, but it is sufficient to evaluate dose‐related effects on hypertension.
Many studies did not take into account different drinking patterns. In the majority of studies, lifetime abstainers and former drinkers were combined into one category, “nondrinkers,” thus leading to limited information about risk of hypertension for these two groups separately. Additionally, most studies did not analyze the effect of beverage type (wine, beer, spirits) and, therefore, we cannot answer whether different types of alcoholic beverages are equivalent in their risk on development of hypertension. We also did not compare different ethnicities, including white, black, or Asian, to examine whether a specific race might be at greater risk for the development of hypertension. Also, interpretation is limited by an inability to separate patients with increased BP from alcohol consumption compared with other confounding variables. Associations in observational studies of alcohol intake and BP may be heavily confounded by other factors such as diet, smoking, exercise levels, and socioeconomic status.
Conclusions
Our study confirmed that heavier alcohol consumption >20 g/d is associated with the risk of development of hypertension in both women and men. With regards to light to moderate alcohol consumption (<20 g/d), women had a potentially reduced risk of hypertension, while men had an increased risk of hypertension. Limiting alcohol intake in those with preexisting hypertension is important. Even for light drinkers, vigilant BP monitoring is necessary. The protective effect of alcohol in women is modest and cannot support alcohol consumption as a protective measure. Further studies are required to explore the underlying cause of differential effects of light‐moderate alcohol consumption among men and women.
References
- 1. Egan BM, Zhao Y, Axon RN. US trends in prevalence, awareness, treatment, and control of hypertension, 1988–2008. JAMA. 2010;303:2043–2050. [DOI] [PubMed] [Google Scholar]
- 2. Malinski MK, Sesso HD, Lopez‐Jimenez F, et al. Alcohol consumption and cardiovascular disease mortality in hypertensive men. Arch Intern Med. 2004;164:623–628. [DOI] [PubMed] [Google Scholar]
- 3. Beulens JW, Rimm EB, Ascherio A, et al. Alcohol consumption and risk for coronary heart disease among men with hypertension. Ann Intern Med. 2007;146:10–19. [DOI] [PubMed] [Google Scholar]
- 4. Djousse′ L, Gaziano JM. Alcohol consumption and risk of heart failure in the Physicians’ Health Study I. Circulation. 2007;115:34–39. [DOI] [PubMed] [Google Scholar]
- 5. Fuchs FD, Chambless LE, Whelton PK, et al. Alcohol consumption and the incidence of hypertension: the Atherosclerosis Risk in Communities Study. Hypertension. 2001;37:1242–1250. [DOI] [PubMed] [Google Scholar]
- 6. Potter JF, Beevers DG. Pressor effect of alcohol in hypertension. Lancet. 1984;1:119–122. [DOI] [PubMed] [Google Scholar]
- 7. Dyer AR, Stamler J, Paul O, et al. Alcohol consumption, cardiovascular risk factors and mortality in two Chicago epidemiologic studies. Circulation. 1977;56:1067–1074. [DOI] [PubMed] [Google Scholar]
- 8. Curtis AB, Sherman JA, Strogatz DS, et al. Alcohol consumption and changes in blood pressure among African Americans – the Pitt County study. Am J Epidemiol. 1997;146:727–733. [DOI] [PubMed] [Google Scholar]
- 9. Klatsky AL, Friedman GD, Siegelaub AB, Gerard MJ. Alcohol consumption and blood pressure Kaiser‐Permanente Multiphasic Health Examination data. N Engl J Med. 1977;296:1194–1200. [DOI] [PubMed] [Google Scholar]
- 10. Ford ES, Cooper RS. Risk factors for hypertension in a national cohort study. Hypertension. 1991;18:598–606. [DOI] [PubMed] [Google Scholar]
- 11. Criqui MH, Wallace RB, Mishkel M, et al. Alcohol consumption and blood pressure: the Lipid Research Clinics Prevalence Study. Hypertension. 1981;3:557–565. [DOI] [PubMed] [Google Scholar]
- 12. Gordon T, Kannel WB. Drinking and its relation to smoking, BP, blood lipids and uric acid: the Framingham Study. Arch Intern Med. 1983;143:1366–1374. [PubMed] [Google Scholar]
- 13. Alkerwi A, Boutsen M, Vaillant M, et al. Alcohol consumption and the prevalence of metabolic syndrome: a meta‐analysis of observational studies. Atherosclerosis. 2009;204:624–635. [DOI] [PubMed] [Google Scholar]
- 14. Klatsky AL, Koplik S, Gunderson E, et al. Sequelae of systemic hypertension in alcohol abstainers, light drinkers, and heavy drinkers. Am J Cardiol. 2006;98:1063–1068. [DOI] [PubMed] [Google Scholar]
- 15. Ascherio A, Hennekens C, Willett WC, et al. Prospective study of nutritional factors, blood pressure, and hypertension among US women. Hypertension. 1996;27:1065–1072. [DOI] [PubMed] [Google Scholar]
- 16. Sesso HD, Cook NR, Buring JE, et al. Alcohol consumption and the risk of hypertension in women and men. Hypertension. 2008;51:1080–1087. [DOI] [PubMed] [Google Scholar]
- 17. Thadhani R, Camargo CA Jr, Stampfer MJ, et al. Prospective study of moderate alcohol consumption and risk of hypertension in young women. Arch Intern Med. 2002;162:569–574. [DOI] [PubMed] [Google Scholar]
- 18. Witteman JC, Willett WC, Stampfer MJ, et al. A prospective study of nutritional factors and hypertension among US women. Circulation. 1989;80:1320–1327. [DOI] [PubMed] [Google Scholar]
- 19. Halanych JH, Safford MM, Kertesz SG, et al. Alcohol consumption in young adults and incident hypertension: 20‐year follow‐up from the Coronary Artery Risk Development in Young Adults Study. Am J Epidemiol. 2010;171:532–539. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Stranges S, Wu T, Dorn JM, et al. Relationship of alcohol drinking pattern to risk of hypertension: a population‐based study. Hypertension. 2004;44:813–819. [DOI] [PubMed] [Google Scholar]
- 21. Ohmori S, Kiyohara Y, Kato I, et al. Alcohol intake and future incidence of hypertension in a general Japanese population: the Hisayama study. Alcohol Clin Exp Res. 2002;26:1010–1016. [DOI] [PubMed] [Google Scholar]
- 22. Tsuruta M, Adachi H, Hirai Y, et al. Association between alcohol intake and development of hypertension in Japanese normotensive men: 12‐year follow‐up study. Am J Hypertens. 2000;13(5 Pt 1):482–487. [DOI] [PubMed] [Google Scholar]
- 23. Yamada Y, Ishizaki M, Kido T, et al. Alcohol, high blood pressure, and serum gamma‐glutamyl transpeptidase level. Hypertension. 1991;18:819–826. [DOI] [PubMed] [Google Scholar]
- 24. Saremi A, Hanson RL, Tulloch‐Reid M, et al. Alcohol consumption predicts hypertension but not diabetes. J Stud Alcohol. 2004;65:184–190. [DOI] [PubMed] [Google Scholar]
- 25. Nakanishi N, Makino K, Nishina K, et al. Relationship of light to moderate alcohol consumption and risk of hypertension in Japanese male office workers. Alcohol Clin Exp Res. 2002;26:988–994. [DOI] [PubMed] [Google Scholar]
- 26. Nakanishi N, Yoshida H, Nakamura K, et al. Alcohol consumption and risk for hypertension in middle‐aged Japanese men. J Hypertens. 2001;19:851–855. [DOI] [PubMed] [Google Scholar]
- 27. Taylor B, Irving HM, Baliunas D, et al. Alcohol and hypertension: gender differences in dose‐response relationships determined through systematic review and meta‐analysis. Addiction. 2009;104:1981–1990. [DOI] [PubMed] [Google Scholar]
- 28. Russell M, Cooper ML, Frone MR, Welte JW. Alcohol drinking patterns and blood pressure. Am J Public Health. 1991;81:452–457. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Puddey IB, Jenner DA, Beilin LJ, Vandongen R. An appraisal of the effects of usual vs recent alcohol intake on blood pressure. Clin Exp Pharmacol Physiol. 1988;15:261–264. [DOI] [PubMed] [Google Scholar]
- 30. Fuchs FD. Vascular effects of alcoholic beverages: is it only alcohol that matters? Hypertension. 2005;45:851–852. [DOI] [PubMed] [Google Scholar]
- 31. Giovannucci E, Colditz G, Stampfer MJ, et al. The assessment of alcohol consumption by a simple self‐administered questionnaire. Am J Epidemiol. 1991;133:810–817. [DOI] [PubMed] [Google Scholar]