

Abstract
J Clin Hypertens (Greenwich).****;**:**–**. ©2011 Wiley Periodicals, Inc.
Transient ischemic attack (TIA) is currently defined as a transient episode of neurologic dysfunction caused by focal brain, spinal cord, or retinal ischemia without infarction. TIA is an important risk factor for stroke and other major vascular events. Risk factors for TIA or stroke need to be addressed effectively to reduce the risk for stroke in patients who have had a TIA. Aspirin (ASA) significantly reduces the risk for stroke when given after a TIA, stroke, or myocardial infarction in a dose of 50 mg/d to 325 mg/d. The role of ASA in the primary prevention of TIA or stroke, however, is less well‐substantiated. Clopidogrel may be used in the secondary prevention of TIA or stroke, but its antiplatelet effect may be reduced in poor metabolizers of the drug. The combination of ASA and extended‐release dipyridamole is effective in reducing risk for TIA and stroke, and may confer additional risk‐lowering without an increased risk of bleeding compared with ASA alone. ASA monotherapy, clopidogrel alone, or the combination of ASA and extended‐release dypiridamole are all acceptable options for initial therapy in patients with a TIA and stroke, and the combination of ASA plus extended‐release dypiridamole is recommended over ASA alone.
A transient ischemic attack (TIA) has traditionally been defined as an episode of neurologic dysfunction due to ischemia in a vascular territory of the central nervous system (central or retinal) lasting <24 hours, 1 whereas a stroke has been defined as a neurologic deficit that persists for more than 24 hours. With the advent of modern brain imaging methods, this arbitrary time‐based definition of TIA has been overturned, because many patients presenting with symptoms lasting <24 hours were found to have an infarction (Figure 1). 2 In fact, up to one third of patients diagnosed with TIA usually have evidence of infarction as shown by serial magnetic resonance imaging (MRI) studies. 3 In this light, the definition of TIA has been revised to include a tissue‐based diagnosis rather than a time‐based diagnosis. The current definition of TIA is therefore that of a transient episode of neurologic dysfunction caused by focal brain, spinal cord, or retinal ischemia without acute infarction. 2 This tissue‐based definition effectively addresses 3 key concepts of TIA: that TIAs result from reduced cerebral blood flow without infarction of brain tissue, that a brain imaging procedure is required for making a diagnosis of TIA or stroke, and that the clinician should no longer wait for 24 hours to rule in a stroke vs a TIA, as this may lead to inappropriate delays in treatment.
Figure 1.
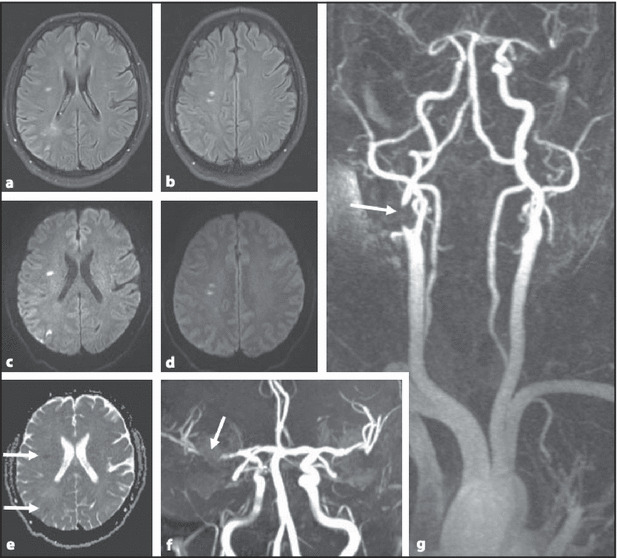
Fluid‐attenuated inversion‐recovery (FLAIR) images (a, b) and diffusion‐weighted magnetic resonance imaging results (c–e) in a 46‐year‐old patient presenting with transient weakness of the arm and leg, from which she had fully recovered after 5 hours. Note the presence of nonspecific white matter lesions on FLAIR imaging, which was seen as restricted diffusion (arrows in e) consistent with acute ischemic damage. Magnetic resonance angiography images (f, g) showed subtotal stenosis at the origin of the right internal carotid artery (arrow) as the likely cause of thromboembolism. Permission from Fazekas F, Niederkorn K, Ebner F, Diez‐Tejedor E. Relevance of neuroimaging in the evaluation of cerebral ischemia. Cerebrovasc Dis. 2009;27(suppl 1):1–8.
TIA has traditionally been regarded as a benign condition relative to stroke that frequently has irreversible or disabling clinical sequelae. Current thinking, however, views TIA as being part of a spectrum of brain ischemia, providing an important therapeutic window where timely intervention may prevent the onset of permanent and often disabling neurologic injury.
Epidemiology
The incidence of TIA is difficult to ascertain because epidemiologic studies have used varying criteria for its definition and many cases are unreported owing to the transient and apparently mild nature of the associated symptoms. Nevertheless, population estimates have determined the incidence of TIA in the United States to be 200,000 to 500,000 annually, 2 with a prevalence of about 2.3%. 4 With the advent of the new TIA definition and the increasing availability of brain imaging, many episodes of transient neurologic deficits that were previously labeled as TIA are expected to be reclassified as stroke, as a result of more accurate diagnosis. This should also allow more reliable comparisons between studies evaluating these conditions.
Short‐Term Prognosis
TIA is an important risk factor for stroke and other major vascular events. Up to 23% of strokes are preceded by TIA, with a 90‐day risk as high as 10.5% and with many occurring during the first week following a TIA. 5 , 6 In a meta‐analysis involving 18 studies of early stroke risk in a total of 10,126 TIA patients, the pooled stroke risk was 3.1% at 2 days and 5.2% at 7 days. 7 Another meta‐analysis of 11 studies reporting early risk of stroke after TIA estimated the pooled risk to be 3.5%, 8%, and 9.2% at 2, 30, and 90 days after TIA, respectively. 8 The pooled risk was higher (9.9%, 13.4%, and 17.3% at 2, 30, and 90 days, respectively) if only the studies that actively ascertained the outcome after the observation period (eg, patient follow‐up in a clinic) were included, as opposed to those that determined stroke after TIA using administrative data (ie, from clinical records or database). In both meta‐analyses, there was significant heterogeneity between the studies included, and weighted regression analysis of this heterogeneity revealed that it was almost fully explained by the study setting and method rather than by chance. The risk of stroke in the first 24 hours after a TIA is particularly impressive. Investigators from the Oxford Vascular Study performed in the United Kingdom have found that of all recurrent strokes that occur during the first week after a TIA, approximately half (52%) occur in the first 24 hours, and that half of these early strokes are disabling or fatal. 9 In this prospective study, the risk of stroke in the first 6, 12, and 24 hours following a first TIA was 1.2%, 2%, and 5.1%, respectively.
These studies likely underestimate stroke incidence (and hence stroke risk) after TIA, given that some patients may not seek consultation for mild or transient symptoms of TIA. In the Oxford Vascular Study, 36% of patients who had a probable TIA prior to a stroke did not seek medical assistance for their TIA symptoms. 9 Another limitation is that the meta‐analyses excluded a larger number of studies owing to differences in TIA definition of variations in observation period (eg, stroke risk at 1 month as opposed to 7 days post‐TIA). Further, the acute event may represent an evolving stroke (ie, stroke progression instead of two distinct events, such as TIA followed by definite ischemic stroke), making it difficult to classify. Nevertheless, the high risk of stroke following TIA reported in these studies highlights the importance of its early recognition and timely management.
Medium‐ and Long‐Term Prognosis
Patients with TIA are a heterogeneous group, presenting with a range of signs and symptoms and differing widely in their burden of concomitant risk factors, comorbid conditions, and underlying vascular and neural pathology. It is generally accepted that the medium‐ and long‐term prognosis after a TIA or stroke is dependent on the individual’s cardiovascular (CV) risk factors, rather than being a function of the event itself (such as the vascular territory of the ischemic event or the presenting signs and symptoms, which is the case for the short‐term prognosis). Age and previous cerebrovascular events are independent predictors of stroke after TIA.
A prospective study conducted in Germany evaluated the medium‐term risk for stroke and mortality in patients who were admitted for a TIA, defined as an acute neurologic deficit of presumably ischemic cause lasting <24 hours regardless of findings on neuroimaging. The study showed that among 1480 consecutively admitted TIA patients (mean age, 68 years; 47.6% women) followed up for a mean of 2 years, 94 (6.5%) had a stroke and 118 died; 21 (1.5% of the total study population) experienced a fatal stroke. 10 Thus, more patients die due to causes other than stroke in the medium‐term after a TIA. Further, the annual stroke risk for this cohort was only 4.4%, and the predictors of stroke on univariate analysis included increasing age, previous cerebrovascular events, coronary artery disease, and atrial fibrillation.
A 10‐year follow‐up of the Oxfordshire Community Stroke Project (OCSP) participants (a study conducted to determine the incidence of first‐ever TIA in Oxfordshire, United Kingdom from 1981 to 1986), attempted to quantify the risk of stroke and other vascular events in patients with a history of TIA who survived the initial “high‐risk” phase after a TIA. Patients were included in the study if they were alive and had not had a stroke at the end of 1998 (7 years after the OCSP started). The median time from most recent TIA to study entry was 3.8 years. In this cohort (mean age, 69 years; 62% male, 48.5% hypertensive, 76.2% exsmokers or current smokers, 14.5% with a history of myocardial infarction [MI]), the risk of first stroke was 19%, whereas the risk of a MI or death from coronary artery disease was higher at 28%. 11 Moreover, the event rates remained constant through time. These studies show that patients who experienced a TIA are at risk for developing stroke as well as other CV events and highlight the need for appropriate management of CV risk factors and concomitant CV disease in order to reduce their risk of these outcomes in the medium‐ and long‐term.
Risk of Cognitive Decline and Dementia
Stroke is associated with increased risk of cognitive decline and dementia, but very few studies have evaluated the risk of developing impaired cognitive function post‐TIA. In a prospective study with a 60,535 person‐year follow‐up, the risk of dementia in patients with focal transient neurologic attacks (defined similarly to TIA) was not greater than in patients without TIA. 12 Given the new definition and more precise imaging criteria for TIA, this issue clearly merits further investigation.
Risk Factors for TIA
Known CV risk factors for TIA and stroke include hypertension, diabetes, dyslipidemia, obesity, cigarette smoking, and heavy alcohol intake. In addition, atrial fibrillation, intracranial atherosclerotic disease, cardiomyopathy, and valvular heart disease increase the risk of TIA or stroke. Management of these risk factors is important in the prevention of stroke in patients who have had a TIA, but correction of these conditions, particularly hypertension and dyslipidemia, is not always achieved. 13 Use of appropriate antihypertensive agents and ≥1 lipid‐lowering agents in patients with hypertension and/or dyslipidemia, achieving glucose control in patients with diabetes, and modifying lifestyle (eg, smoking cessation, limiting alcohol intake, maintaining ideal body weight, and increasing physical activity) are recommended for patients who are at high CV risk who have had a TIA.
Aspirin in Primary and Secondary Prevention of TIA or Stroke
Aspirin (ASA) significantly reduces the risk of stroke in patients who experience a TIA or stroke. A meta‐analysis of 16 secondary prevention trials involving a total of 17,000 patients showed that there were 100 fewer events in the groups allocated to ASA compared with controls (480 vs 580) during a 43,000 person‐year follow‐up. 14 The proportional risk reduction for stroke from ASA use was 19% (rate ratio, 0.81; 95% confidence interval [CI], 0.71–0.92) compared with controls. In another meta‐analysis, ASA was found to decrease the risk of all‐cause death (odds ratio [OR], 0.91: 95% CI, 0.85–0.98), nonfatal stroke (OR, 0.81; 95% CI, 0.74–0.89), and nonfatal MI (OR, 0.63; 95% CI, 0.48–0.84) compared with placebo in patients with confirmed cerebrovascular disease. 15 For every 1000 patients given ASA within the first 48 hours of an ischemic cerebral event, 13 will avoid death or dependency, with a number needed to treat of 79. 16 In patients with a prior TIA or noncardioembolic ischemic stroke, ASA is an option for initial therapy to reduce the risk of recurrent stroke and other CV events. 17
The value of ASA for primary prevention of ischemic cerebral events is less well‐substantiated. In a large prospective study involving 39,876 initially healthy women 45 years and older, 100 mg of ASA taken on alternating days reduced the risk of stroke by 17% compared with placebo (P=.04), mainly by driving down rates of ischemic stroke (24% risk reduction compared with placebo, P=.009). 18 The benefit was greater in participants 65 years and older, where ASA reduced the risk of ischemic stroke by 30% compared with placebo (P=.05). On the other hand, in a meta‐analysis of 6 primary prevention trials comparing ASA with placebo (which included data from the aforementioned study), the yearly absolute difference of ASA (at a dose range of 100 mg every other day to 500 mg daily) vs placebo in preventing all strokes was only −0.01% (with a net effect of 0.20% for ASA vs 0.21% for placebo per year, P=.4). 14 This was at the expense of increased nonfatal gastrointestinal and extracranial bleeding in the patients who received ASA (0.10% vs 0.07% for placebo, P=.0001). The results suggest that the absolute reduction of CV risk with ASA was only twice the risk associated with bleeding. Further, age, sex, smoking history, body mass index, and the presence of hypertension, diabetes, or dyslipidemia did not significantly alter the decrease in CV risk associated with ASA, suggesting that the absolute risk of vascular events was a function of the individual’s risk factors rather than a benefit derived from ASA. One caveat, however, is that the patients in these primary prevention trials were not taking a statin, which would substantially lower their risk of experiencing a vascular event. To illustrate, a meta‐analysis has shown that for every 1‐mmol/L decrease in low‐density lipoprotein cholesterol there is a 21.1% relative risk (RR) reduction for stroke. 19 Clearly, more studies are needed to identify the role of ASA, if any, in the primary prevention of TIA and ischemic stroke.
The optimal daily ASA dose to reduce CV risk without increasing the risk of bleeding remains unclear. ASA at a dose of as little as 30 mg/d is known to inhibit thromboxane production, but it is given in some instances at a dose that is more than 10 times this amount. The primary and secondary prevention trials used ASA in doses ranging from 30 mg to 1300 mg daily. In a subgroup analysis of 4589 patients in the placebo arm of the Blockage of the Glycoprotein IIb/IIIa Receptor to Avoid Vascular Occlusion (BRAVO) trial, 20 ASA at a dose >165 mg/d was associated with lower all‐cause mortality but without a significant difference in the incidence of nonfatal stroke, compared with ASA dosed at <162 mg/d. The higher ASA dose was associated with a higher risk of any, but not serious, bleeding. In a post hoc analysis of the Clopidogrel for High Antithrombotic Risk and Ischemic Stabilization, Management and Avoidance (CHARISMA) trial, 21 where ASA was given (not randomly assigned) at a dose of 75–162 mg/d, the hazard ratio for the primary efficacy end point (thrombotic events) for doses ≥100 mg/d was the same as for doses <100 mg/d. Further, the risk of bleeding was similar in the two groups. Two older studies have also shown no difference in benefit between various ASA doses. Data from the Dutch TIA Study 22 evaluating the efficacy of ASA 30 mg/d vs 283 mg/d showed that the 30‐mg dose was noninferior and resulted in fewer bleeding events. In the UK‐TIA trial, 23 2435 patients received either ASA at 300 mg/d, ASA at 600 mg twice daily (1200 mg/d), or placebo for a mean of 4 years following a TIA. There was no difference in efficacy between the 300‐ and 1200‐mg daily doses of ASA, and the lower dose had less gastrointestinal toxicity. Current guidelines recommend a dose range of 50 mg to 325 mg of ASA (given as monotherapy) daily in patients who have had a TIA or noncardioembolic ischemic stroke (Table). 17
Table TABLE.
American Heart Association Recommendations for Antithrombotic Therapy for TIA or Noncardioembolic Ischemic Stroke
| Recommendations | Level of Evidencea |
|---|---|
| For patients with noncardioembolic ischemic stroke or TIA, the use of antiplatelet agents rather than oral anticoagulation is recommended to reduce the risk of recurrent stroke and other cardiovascular events | Class I, level A |
| ASA (50–325 mg/d) monotherapy, the combination of ASA 25 mg and extended‐release dipyridamole 200 mg twice daily and clopidogrel 75 mg monotherapy are all acceptable options for initial therapy. The choice of antiplatelet agent should be individualized on the basis of patient risk factor profiles, cost, tolerance, and other clinical characteristics | ASA monotherapy: class I, level A ASA + dipyridamole: class I, level B Clopidogrel: class IIa, level B |
| The addition of ASA to clopidogrel increases the risk of hemorrhage and is not recommended for routine secondary prevention after ischemic stroke or TIA | Class III, level A |
| For patients allergic to ASA, clopidogrel is reasonable | Class IIa, level C |
| For patients who have an ischemic stroke while taking ASA, there is no evidence that increasing the dose of ASA provides additional benefit. Although alternative antiplatelet agents are often considered, no single agent or combination has been studied in patients who have had an event while receiving ASA | Class IIb, level C |
Abbreviations: ASA, aspirin; TIA, transient ischemic attack. aLevel of evidence: A, data derived from multiple randomized controlled trials; B, data derived from a single randomized trial or nonrandomized studies; C, very limited populations studied, only consensus opinion of experts, case studies, or standard of care. Class I, procedure/treatment should be performed/administered; class IIa, it is reasonable to perform procedure/administer treatment; class IIb, additional studies needed, procedure/treatment may be considered; class III, procedure/treatment should not be performed/administered since it is not helpful and may be harmful. From: Furie KL, Kasner SE, Adams RJ, et al, on behalf of the American Heart Association Stroke Council, Council on Cardiovascular Nursing, Council on Clinical Cardiology, and Interdisciplinary Council on Quality of Care and Outcomes Research. Guidelines for the prevention of stroke in patients with stroke or transient ischemic attack. A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2011;42:227–276.
Other Antiplatelet Agents in the Prevention of Stroke After TIA
Other antiplatelet agents are also effective in lowering stroke risk after TIA (Table). Dipyridamole impedes adenosine uptake into platelets, leading to inhibition of platelet aggregation. It is also a weak inhibitor of phosphodiesterase, thereby enhancing nitric oxide production and resulting in vasodilation. 24 Data from the Second European Stroke Prevention Study (ESPS‐2) 25 showed benefit of adding extended‐release dipyridamole to low‐dose ASA (50 mg/d) for stroke prevention. ESPS‐2 enrolled 7054 patients with a history of TIA or ischemic stroke in the previous 3 months and randomized them to 4 treatment groups: placebo, ASA alone, modified‐release dipyridamole alone, and the combination of ASA and modified‐release dipyridamole. ESPS‐2 showed that the combination of ASA and modified‐release dipyridamole reduced stroke risk significantly by 23.1% compared with ASA alone (P=.006) and by 24.7% compared with dipyridamole alone (P=.002).
These findings were supported by the more recent European/Australasian Stroke Prevention in Reversible Ischemia Trial (ESPRIT). 26 This large trial compared the efficacy of the combination of ASA plus dipyridamole as well as moderate anticoagulation therapy (target international normalized ratio [INR] of 2–3) with that of ASA alone in the secondary prevention of stroke. The ASA and dipyridamole vs ASA arm of the trial randomized 2739 patients within 6 months of a TIA or ischemic stroke to receive ASA (30–325 mg/d, median dose 75 mg/d) with or without dipyridamole (200 mg twice daily; 83% of participants used the extended‐release formulation). Medications were administered open‐label, but the auditing of outcome events was blinded. There were fewer events (vascular death, nonfatal MI, and nonfatal stroke, as well as nonfatal major bleeding complication) in the ASA plus dipyridamole group compared with the ASA‐alone group (13% vs 16%; hazard ratio, 0.80: 95% CI, 0.66–0.98) (Figure 2).
Figure 2.
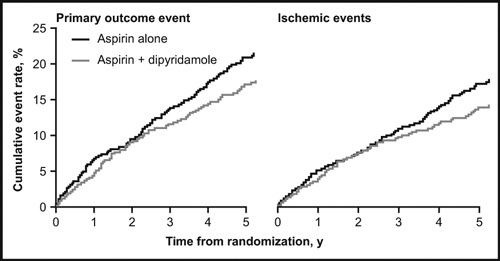
Cumulative event rate during the 5‐year follow‐up for aspirin alone vs aspirin plus dipyridamole in the Aspirin Plus Dipyridamole vs Aspirin Alone After Cerebral Ischemia of Arterial Origin (ESPRIT) trial. Primary outcome event was defined as the composite of death from vascular causes, nonfatal stroke, nonfatal myocardial infarction, and major bleeding (intracerebral, fatal, or requiring hospital admission). Permission from The ESPRIT Study Group. Aspirin plus dipyridamole vs aspirin alone after cerebral ischemia of arterial origin (ESPRIT): randomized controlled trial. Lancet. 2006;367:1665–1673.
In a newer meta‐analysis (which included data from ESPRIT) comparing dipyridamole with or without another antiplatelet agent with control (placebo or antiplatelet drug other than dipyridamole), dipyridamole had no clear benefit in reducing the risk of vascular death (RR, 0.99; 95% CI, 0.87–1.12) but appeared to reduce the risk of vascular events (fatal and nonfatal stroke and MI: RR, 0.88: 95% CI, 0.81–0.95) compared with control, with the effects on cerebral ischemia reaching statistical significance. 27 These data were pooled from studies on patients with arterial vascular disease, including, but not limited to, TIA and stroke. In the light of these findings showing an incremental benefit of the combination of ASA plus extended‐release dipyridamole over ASA monotherapy, this combination is recommended over ASA alone as initial therapy in patients who have had a TIA or ischemic noncardioembolic stroke (Table). 17
Clopidogrel, a thienopyridine derivative, is an inhibitor of platelet activation and aggregation through the irreversible binding of its active metabolite to the P2Y12 class of adenosine diphosphate receptors on platelets. 28 In the trial of Clopidogrel vs Aspirin in Patients at Risk of Ischemic Events (CAPRIE), 29 the ability of clopidogrel 75 mg/d to reduce the risk of a composite of ischemic stroke, MI, or vascular death was compared with that of treatment with ASA 325 mg/d given for 1 to 3 years (mean follow‐up of 1.91 years) in patients with atherosclerotic vascular disease (manifested as recent MI, recent ischemic stroke [not TIA], or symptomatic peripheral arterial disease). An RR reduction of 8.7% was achieved in favor of clopidogrel. In examining the stroke patient subset (involving 6431 patients), the average yearly event rate in the clopidogrel group (n=3233) was 7.15% compared with 7.71% in the ASA group (n=3198), with an RR reduction of 7.3% (95% CI, 5.7–18.7) in favor of clopidogrel (P=.26). In general, the results show that recurrent stroke and stroke deaths were most common in the stroke subgroup, and fatal or nonfatal MIs were most common in the MI group.
In the Management of Atherothrombosis With Clopidogrel in High‐Risk Patients (MATCH) trial, 30 the addition of ASA (75 mg/d) in patients with a recent TIA or ischemic stroke and at least one other CV risk factor who were already receiving clopidogrel did not significantly reduce the incidence of a composite of CV events (which included ischemic stroke, MI, vascular death, rehospitalization for acute ischemia) after an 18‐month follow‐up. This was in a patient population (n=7599) with a mean age of 66 years and with hypertension (78%), diabetes (68%), and dyslipidemia (56%) who were randomized within 30 days of the index event (21% TIA, 79% ischemic stroke).
The efficacy of the combination of ASA plus extended‐release dipyridamole in preventing the first recurrence of stroke in patients 55 years and older with a recent (<90 days prior to randomization) ischemic stroke (no TIA patients were included) was compared with that of clopidogrel in the Prevention Regimen for Effectively Avoiding Second Strokes (PRoFESS) trial. 31 In a 2×2 factorial design, patients (N=20,332) were randomized to receive either a fixed combination of ASA (25 mg) and extended‐release dipyridamole (200 mg) given twice daily (n=10,181) or clopidogrel at 75 mg/d (n=10,151). After a mean follow‐up of 2.5 years, similar rates of recurrence of stroke were observed in the ASA plus extended‐release dipyridamole (9.0%) and clopidogrel (8.8%) groups, with a hazard ratio of 1.01 (95% CI, 0.92–1.11), indicating that neither agent was superior to the other in preventing recurrent stroke; however, the results did not meet prespecified criteria for noninferiority.
Clopidogrel is metabolized to its active form by the CYP2C19 enzyme system in the liver, and in poor metabolizers (found in 2%–14% of the population), the effectiveness of this medication may be reduced, thereby lessening its ability to prevent stroke. 32 Clopidogrel is marketed with a boxed warning that highlights this important finding. Clopidogrel remains to be an acceptable alternative to ASA alone in the secondary prevention of stroke, particularly in patients who have documented ASA allergy (Table). 17
Anticoagulant Therapy in the Secondary Prevention of Stroke
A meta‐analysis of 11 trials comparing anticoagulation (oral coumarin or phenindione, with one trial evaluating low‐dose heparin) with placebo, “usual treatment” (heparin study), or no treatment, in patients with a history of TIA or presumed noncardioembolic ischemic stroke, showed that anticoagulation did not alter the risk of a subsequent ischemic stroke (OR, 0.85; 95% CI, 0.66–1.09), but rather increased the risk of fatal intracranial hemorrhage and major extracranial bleeding. 33 The anticoagulation arm of ESPRIT evaluated the efficacy of moderate‐intensity oral anticoagulation compared with that of ASA in preventing future vascular events (death from vascular causes, nonfatal MI, nonfatal stroke, or major bleeding complication) in patients who had a TIA or a minor stroke of presumed arterial origin. 34 Patients were randomized within 6 months of a TIA or minor stroke to receive oral anticoagulants (target INR 2–3) or ASA at a dose of 30 mg/d to 325 mg/d. ESPRIT was terminated early because ASA combined with dipyridamole was shown to be more effective than ASA alone, but medium‐intensity oral anticoagulation was not more effective than ASA in preventing vascular events. Thus, the possible benefit of oral anticoagulants in patients who had a TIA or ischemic noncardioembolic stroke was offset by an increased incidence of bleeding complications, and its use in secondary prevention of stroke in these patients is not recommended.
On the other hand, oral anticoagulants are indicated for the secondary prevention of stroke in patients with nonvalvular atrial fibrillation (AF). 17 The target INR is between 2 and 3, and protection against stroke is suboptimal when the INR drops below 2. 35 , 36 Warfarin given after TIA or a minor stroke prevents 31 strokes for every 1000 patients treated, and the RR reduction achieved is 68% compared with placebo. 17 In contrast, ASA has an RR reduction of 21% compared with placebo. Pooled evidence from two large trials, the European Atrial Fibrillation Trial (EAFT) involving 455 patients and the Studio Italiano Fibrillazione Atriale (SIFA) trial with 916 patients showed that oral anticoagulation was superior to antiplatelet therapy in the secondary prevention of stroke among patients with nonrheumatic AF, albeit with a higher risk of bleeding. 37 In addition to nonvalvular AF, oral anticoagulants are recommended for secondary prevention of stroke in patients with prosthetic heart valves and valvular heart disease (particularly rheumatic mitral valve disease). 17
Risk of Bleeding
The occurrence of bleeding in patients who are given antithrombotic agents after a TIA or stroke is a major consideration. Bleeding from the gastrointestinal tract, or more seriously, intracranial hemorrhage, may be increased following administration of antithrombotic agents or anticoagulants. Data from a meta‐analysis comparing dual antiplatelet therapy with single‐agent therapy showed that giving two antiplatelet agents is associated with significantly increased risk of major (RR, 1.47; 95% CI, 1.36–1.60) and minor (RR, 1.56; 95% CI, 1.47–1.66) bleeding events compared with single‐agent therapy. 38 The data were pooled from 16 studies of coronary heart disease patients and two studies of ischemic stroke patients (MATCH and ESPS‐2). However, the authors explained that while the risk for bleeding associated with dual antiplatelet therapy was 50% to 60%, this increase in risk was not so different from placebo‐controlled studies involving single agents that show a bleeding risk of about 40% to 50%.
In MATCH, the combination of ASA plus clopidogrel, which did not significantly reduce the incidence of the primary end point, resulted in an increased incidence of life‐threatening bleeding compared with clopidogrel plus placebo (2.6% vs 1.3%, P<.0001) without a difference in mortality rates attributed to bleeding. 30 In PRoFESS, the net risk of hemorrhagic stroke or major bleeding event (defined as a hemorrhagic event resulting in significant disability, intraocular bleeding causing loss of vision, symptomatic intracranial bleeding, need for transfusion with ≥2 units of packed red cells or its equivalent, or need for hospitalization) was similar in the ASA plus extended‐release dipyridamole (11.7%) and clopidogrel (11.4%) groups (hazard ratio, 1.03; 95% CI, 0.95–1.11). 31
Usman and colleagues 39 analyzed the comparative risk of bleeding of the different antithrombotic agents (ASA, clopidogrel, ASA plus clopidogrel, ASA plus extended‐release dipyridamole, and vitamin K antagonists) in patients with a history of TIA, cerebral vascular accident, coronary artery disease, peripheral artery disease, or MI. The analysis included 13 trials with a minimum follow‐up of 1 year. The mean incidence of total bleeding (all bleeding episodes) was highest for vitamin K antagonists (16.8%) and lowest for clopidogrel alone, whereas the mean incidence of major bleeding (requiring hospitalization) was highest with anticoagulation (2.5%) and lowest for clopidogrel alone (0.85%). The mean incidence of total bleeding (Figure 3A) and major bleeding (Figure 3B) was lower for the ASA plus extended‐release dipyridamole combination (3.6% and 0.93%, respectively) than for ASA alone (4.8% and 1%, respectively). This phenomenon was attributed by the authors to the ability of dipyridamole to increase vascular nitric oxide production, thereby promoting vasodilation, reduced leukocyte adhesion to the vessel wall, decreased inflammation, and enhanced “platelet sparing,” which leads to increased efficacy without an increased risk of bleeding.
Figure 3.
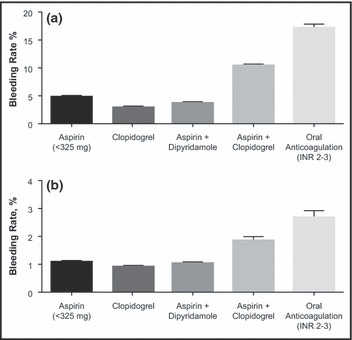
Mean total (A) and mean major (B) bleeding rates per year for the different antithrombotic combinations, aspirin, and oral anticoagulation. INR indicates international normalized ratio. Permission from Usman MHU, Notaro LA, Nagarakant R, et al. Combination antiplatelet therapy for secondary stroke prevention: enhanced efficacy or double trouble? Am J Cardiol. 2009;103:1107–1112.
Conclusions
Although in the presence of an aging population, stroke incidence would be predicted to increase over time, better management of TIA and stroke and modification of premorbid risk factors are expected to counter this trend. Indeed, in the United Kingdom, investigators from the Oxford Vascular Study have found that age‐ and sex‐adjusted incidence of first‐time stroke declined by 29% in the past 2 decades, and there was a decrease in overall stroke mortality and incidence of disabling stroke, without a reduction in case fatality due to incident stroke. 40 There were major reductions in the past 20 years in the proportion of smokers (from 32.6% to 18.1%), mean total cholesterol (from 6.24 to 5.4 mmol/L), mean systolic BP (from 156.3 to 147.6 mm Hg) and diastolic BP (from 88 to 82 mm Hg), and a significant increase in the use of statins, antiplatelet drugs, and antihypertensive agents in these stroke patients. These data show that modification of the various risk factors as well as timely and proper management of cerebral ischemic events can substantially lower the risk for stroke mortality and morbidity.
Use of ASA in the secondary prevention of stroke is supported by very strong data from several large, randomized, placebo‐controlled studies. ASA is inexpensive and widely available, and its use significantly lowers the risk of cerebral ischemic events in patients presenting with a TIA. In recent years, the emergence of newer antiplatelet agents that are comparable to ASA or even confer additional benefit has increased the physician’s options for the secondary prevention of TIA and stroke. Current recommendations regarding antiplatelet therapy are summarized in the Table.
Addition of extended‐release dipyridamole to ASA confers additional benefit without an increased risk of bleeding. 40 Two large randomized clinical trials have demonstrated that the combination is more effective than ASA alone in reducing the risk of subsequent vascular events in patients with a TIA or mild ischemic stroke. 25 , 26 This finding was also shown in a recent meta‐analysis, which revealed that the combination of ASA and dipyridamole had a significant advantage over ASA alone in preventing vascular events, particularly after an ischemic stroke, without a significant difference in reducing the risk of death from vascular causes. The combination of ASA plus extended‐release dypiridamole is an acceptable option in the secondary prevention of stroke.
Another antiplatelet agent, clopidogrel, has been shown to be effective in reducing the incidence of vascular events compared with ASA, but the results for the stroke subset did not reach statistical significance. Direct comparison between clopidogrel and the combination of ASA and extended‐release dipyridamole failed to demonstrate noninferiority and showed that the two agents achieved comparable event rates. Further, genetic testing is recommended to identify poor metabolizers of clopidogrel in order to determine whether clopidogrel or alternative antiplatelet regimen should be used in them. Current guidelines recommended ASA, the combination of ASA and extended‐release dipyridamole, and clopidogrel monotherapy as acceptable options for initial therapy in patients with TIA or ischemic stroke (Table). 17 Each patient’s risk factors and clinical profile, medication costs, and tolerability should be made in choosing the appropriate antiplatelet agent for any given patient.
Disclosures: This work was supported by Boehringer Ingleheim Pharmaceuticals, Inc (BIPI). Editorial assistance was provided by Christina Peterson, MD, of Publication CONNEXION (Newtown, PA), which was contracted by BIPI for these services. The authors meet criteria for authorship as recommended by the International Committee of Medical Journal Editors (ICMJE), were fully responsible for all content and editorial decisions, and were involved at all stages of manuscript development. The authors received no compensation related to the development of the manuscript.
References
- 1. Special report from the National Institute of Neurological Disorders and Stroke . Classification of cerebrovascular diseases III. Stroke. 1990;21:637–676. [DOI] [PubMed] [Google Scholar]
- 2. Easton JD, Saver JL, Albers GW, et al. Definition and evaluation of transient ischemic attack. A scientific statement for healthcare professionals from the American Heart Association/American Stroke Association Stroke Council; Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; and the Interdisciplinary Council on Peripheral Vascular Disease. Stroke. 2009;40:2276–2293. [DOI] [PubMed] [Google Scholar]
- 3. Shah SH, Saver JL, Kidwell CS, et al. A multicenter, pooled, patient‐level data analysis of diffusion‐weighted MRI in TIA patients. Stroke. 2007;38:463. [Google Scholar]
- 4. Johnston SC, Fayad PB, Gorelick PB, et al. Prevalence and knowledge of transient ischemic attack among US adults. Neurology. 2003;60:1429–1434. [DOI] [PubMed] [Google Scholar]
- 5. Rothwell PM, Warlow CP. Timing of TIAs preceding stroke: time window for prevention is very short. Neurology. 2005;64:817–820. [DOI] [PubMed] [Google Scholar]
- 6. Johnston SC, Gress DR, Browner WS, Sidney S. Short‐term prognosis after emergency department diagnosis of TIA. JAMA. 2000;284:2901–2906. [DOI] [PubMed] [Google Scholar]
- 7. Giles MF, Rothwell PM. Risk of stroke early after transient ischemic attack: a systematic review and meta‐analysis. Lancet Neurol. 2007;6:1063–1072. [DOI] [PubMed] [Google Scholar]
- 8. Wu CM, McLaughlin K, Lorenzetti DL, et al. Early risk of stroke after transient ischemic attack. A systematic review and meta‐analysis. Arch Intern Med. 2007;167:2417–2422. [DOI] [PubMed] [Google Scholar]
- 9. Chandratheva A, Meta Z, Geraghty OZ, et al. Population‐based study of risk and predictors of stroke in the first few hours after a TIA. Neurology. 2009;72:1941–1947. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Weimar C, Benemann J, Huber R, et al. Long‐term mortality and risk of stroke after transient ischemic attack. J Neurol. 2009;256:639–644. [DOI] [PubMed] [Google Scholar]
- 11. Clark TG, Murphy MFG, Rothwell PM. Long‐term risks of stroke, myocardial infarction, and vascular death in “low risk” patients with a non‐recent transient ischemic attack. J Neurol Neurosurg Psychiatry. 2003;74:577–580. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Bos MJ, van Rijn MJE, Witteman JCM, et al. Incidence and prognosis of transient neurological attacks. JAMA. 2007;298:2877–2885. [DOI] [PubMed] [Google Scholar]
- 13. Johnson P, Rosewell M, James MA. How good is the management of vascular risk after stroke, transient ischemic attack or carotid endarterectomy? Cerebrovasc Dis. 2007;23:156–161. [DOI] [PubMed] [Google Scholar]
- 14. Antithrombotic Trialists’ Collaboration . Aspirin in the primary and secondary prevention of vascular disease: collaborative meta‐analysis of individual participant data from randomized trials. Lancet. 2009;373:1849–1860. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Lievre M, Cucherat M. Aspirin in the secondary prevention of cardiovascular disease: an update of the APTC meta‐analysis. Fundam Clin Pharmacol. 2010;24(3):385–391. [DOI] [PubMed] [Google Scholar]
- 16. Sandercock PAG, Counsell C, Gubitz GJ, Tseng MC. Antiplatelet therapy for acute ischemic stroke. Cochrane Database Syst Rev. 2008:CD000029. doi: 10.1002/14651858.CD000029.pub2. [DOI] [PubMed] [Google Scholar]
- 17. Furie KL, Kasner SE, Adams RJ, et al. Guidelines for the prevention of stroke in patients with stroke or transient ischemic attack. A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2011;42:227–276. [DOI] [PubMed] [Google Scholar]
- 18. Ridker PM, Cook NR, Lee I, et al. A randomized trial of low‐dose aspirin in the primary prevention of cardiovascular disease in women. N Engl J Med. 2005;352:1293–1304. [DOI] [PubMed] [Google Scholar]
- 19. Amarenco P, Labreuche J. Lipid management in the prevention of stroke: review and updated meta‐analysis of statins for stroke prevention. Lancet Neurol. 2009;8:453–463. [DOI] [PubMed] [Google Scholar]
- 20. Aronow HD, Califf RM, Harrington RA, et al. Relation between aspirin dose, all‐cause mortality, and bleeding in patients with recent cerebrovascular or coronary ischemic events (from the BRAVO trial). Am J Cardiol. 2008;102:1285–1290. [DOI] [PubMed] [Google Scholar]
- 21. Steinhubl SR, Bhatt DL, Brennan DM, et al. Aspirin to prevent cardiovascular disease: the association of aspirin dose with clopidogrel with thrombosis and bleeding. Ann Intern Med. 2009;150:379–386. [DOI] [PubMed] [Google Scholar]
- 22. The Dutch TIA Trial Study Group . A comparison of two doses of aspirin (30 mg vs. 283 mg a day) in patients after a transient ischemic attack or minor ischemic stroke. N Engl J Med. 1991;325:1261–1266. [DOI] [PubMed] [Google Scholar]
- 23. Farrell B, Godwin J, Richards S, Warlow C. The United Kingdom transient ischemic attack (UK‐TIA) aspirin trial: final results. J Neurol Neurosurg Psychiatry. 1991;54:1044–1054. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Antithrombotic Trialists’ Collaboration . Collaborative meta‐analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction and stroke in high‐risk patients. BMJ. 2002;324:71–86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Diener HC, Cunha L, Forbes C, et al. European Stroke Prevention Study 2. Dipyridamole and acetylsalicylic acid in the secondary prevention of stroke. J Neurol Sci. 1996;143:1–13. [DOI] [PubMed] [Google Scholar]
- 26. The ESPRIT Study Group . Aspirin plus dipyridamole versus aspirin alone after cerebral ischemia of arterial origin (ESPRIT): randomised controlled trial. Lancet. 2006;367:1665–1673. [DOI] [PubMed] [Google Scholar]
- 27. DeSchryver E, Algra A, van Gijn J. Dipyridamole for preventing stroke and other vascular events in patients with vascular disease. Cochrane Database Syst Rev. 2007;18:CD001820. doi: 10.1002/14651858.CD001820.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Bristol‐Myers Squibb/Sanofi Pharmaceuticals . Plavix [package insert]. Bridgewater, NJ: Bristol‐Myers Squibb/Sanofi Pharmaceuticals; 2009. [Google Scholar]
- 29. CAPRIE Steering Committee . A randomized, blinded trial of clopidogrel versus aspirin in patients at risk of ischemic events (CAPRIE). Lancet. 1996;348:1329–1339. [DOI] [PubMed] [Google Scholar]
- 30. Diener HC, Bogousslavsky J, Brass LM, et al. Aspirin and clopidogrel compared with clopidogrel alone after recent ischaemic stroke or transient ischaemic attack in high‐risk patient (MATCH): randomised, double‐blind placebo‐controlled trial. Lancet. 2004;364:331–367. [DOI] [PubMed] [Google Scholar]
- 31. Sacco RL, Diener HC, Yusuf S, et al. Aspirin and extended‐release dipyridamole versus clopidogrel for recurrent stroke. N Engl J Med. 2008;359:1238–1251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. FDA Drug Safety Communication . Reduced effectiveness of Plavix (clopidogrel) in patients who are poor metabolizers of the drug. http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm/203888.htm#ds. Accessed April 1, 2010.
- 33. Sandercock PAG, Gibson LM, Liu M. Anticoagulants for preventing recurrence following presumed non‐cardioembolicischaemic stroke or transient ischaemic attack. Cochrane Database Syst Rev. 2009;15:CD000248. doi: 10.1002/14651858.CD000248.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. The ESPRIT Study Group . Medium‐intensity oral anticoagulants versus aspirin after cerebral ischemia of arterial origin (ESPRIT): a randomized controlled trial. Lancet Neurol. 2007;6:115–124. [DOI] [PubMed] [Google Scholar]
- 35. European Atrial Fibrillation Trial (EAFT) Study Group . Secondary prevention in non‐rheumatic atrial fibrillation after transient ischaemic attack or minor stroke. Lancet. 1993;342:1255–1262. [PubMed] [Google Scholar]
- 36. Blackshear JL, Halperin JL, Hart RG, et al. Adjusted‐dose warfarin versus low‐intensity, fixed‐dose warfarin plus aspirin for high‐risk patients with atrial fibrillation: stroke Prevention in Atrial Fibrillation III randomized clinical trial. Lancet. 1996;348:633–638. [PubMed] [Google Scholar]
- 37. Saxena R, Kuodstaal P. Anticoagulants versus antiplatelet therapy for preventing stroke in patients with nonrheumatic atrial fibrillation and a history of stroke or transient ischemic attack. Cochrane Database Syst Rev. 2004;18:CD000187. doi: 10.1002/14651858.CD000187.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Serebruany VL, Malinin AI, Ferguson JJ. Bleeding risks of combination vs. single antiplatelet therapy: a meta‐analysis of 18 randomized trials comprising 129,314 patients. Fundam Clin Pharmacol. 2008;22:315–321. [DOI] [PubMed] [Google Scholar]
- 39. Usman MHU, Notaro LA, Nagarakanti R, et al. Combination antiplatelet therapy for secondary stroke prevention: enhanced efficacy or double trouble? Am J Cardiol. 2009;103:1107–1112. [DOI] [PubMed] [Google Scholar]
- 40. Rothwell PM, Coull AJ, Giles MF, et al. Change in stroke incidence, mortality, case‐fatality, severity, and risk factors in Oxfordshire, UK from 1981 (Oxford Vascular Study). Lancet. 2004;363:925–933. [DOI] [PubMed] [Google Scholar]