

Abstract
Solar radiation causes acute foveal injury resulting in outer retinal defects. Symptoms often follow an event of unprotected gazing at a solar eclipse or directly viewing the sun. We encountered a series of cases during winter among habitants of high altitudes who complained of visual field scotomas. All of them had a typical history of prolonged sunbathing but denied gazing at the sun directly. Optical coherence tomography showed outer retinal defects involving the ellipsoid zone characteristic of solar retinopathy in all patients. In this case series, we would like to emphasize the role of geographical factors in the causation of solar retinopathy.
Keywords: Altitudinal retinopathy, outer retinal defects, photic retinopathy, solar retinopathy, UV radiation
Introduction
Outer retinal defects are defects in the ellipsoid zone which predominantly involve the foveal cones. They often present with acute central scotoma following unprotected solar eclipse or sun viewing. These defects can also be caused by trauma, acute posterior vitreous detachment, and unprotected welding exposure.1 Eliciting a proper history can point towards the possible etiology and helps in formulating preventive measures. We encountered a series of patients with outer retinal defects who resided at high altitudes. They had no significant risk factors except for the history of prolonged sunbathing, which suggested solar retinopathy as a possible cause of the outer retinal defects.
Case Reports
Case 1
A 42-year-old farmer from the hilly regions of Himachal Pradesh presented with a 1-day history of visual scotoma. He denied a history of trauma, direct sun gazing, or use of medications. His best-corrected visual acuity (BCVA) was 6/9 in both eyes (BE) and BE had central scotoma on the Amsler grid chart. The anterior segment was normal with a clear lens. Indirect ophthalmoscopy showed grossly normal-looking fundus in BE. Spectral domain optical coherence tomography (OCT) through the fovea revealed a cube-shaped outer retinal defect at the fovea in BE (Figure 1a, b). Solar retinopathy was suspected but he denied a history of prolonged direct sun-gazing. On further interrogation, it was learned that he had engaged in long hours of sunbathing the previous 3 days, which was not a typical habit and he did to combat the severe cold.
Figure 1.
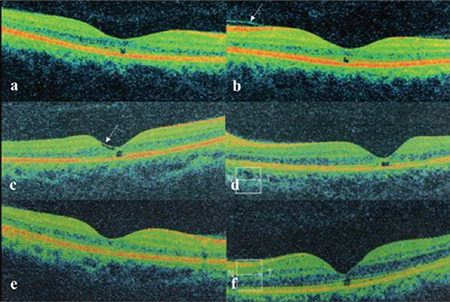
a, b) Optical coherence tomography (OCT) images show outer retinal defects in the right and left eyes of patient 1. Shallow vitreous detachment with normal interface contour is seen in the left eye (arrow). c, d) OCT images of patient 2. Internal limiting membrane draping over the temporal foveal slope is seen in the right eye (arrow). e, f) OCT images of patient 3 with partial discontinuity in the ellipsoid zone in the right eye and full-thickness defect in the outer retinal layers in the left eye
Case 2
A 40-year-old woman from the hilltops was examined for decreased vision in her right eye for 4 days. She was a field supervisor on farmland and had the habit of sunbathing for long hours (lying supine with closed eyes directly under the sun). Her BCVA was 6/12 in the right eye (RE) and 6/6 in the left eye (LE). The anterior segment was normal in BE with clear lenses. Foveal reflex was dull in the RE and normal in the LE. OCT of the RE showed partial inner segment/outer segment (IS/OS) loss at the fovea with internal limiting membrane (ILM) draping (Figure 1c). The LE also showed an outer retinal defect smaller than that in the RE (Figure 1c, d).
Case 3
A 28-year-old man presented to our clinic with complaints of seeing a red spot in his LE for 2 months. He had a history of frequently sunbathing and more so during November and winter. His BCVA was 6/6 in the RE and 6/12 in the LE. The anterior segment was quiet with a clear lens in BE. The fundus was grossly normal in the RE, while the LE showed a dull foveal reflex. OCT of the RE revealed a minimal defect in the IS/OS line and the LE showed focal loss of the outer retinal layers at the fovea with decreased subfield thickness (RE: 236 µm, LE: 206 µm) (Figure 1e, f).
Discussion
Outer retinal defects can be secondary to intrinsic ocular factors like acute posterior vitreous detachment (PVD), macular telangiectasia, Stargardt’s disease, and extrinsic factors like trauma, unprotected direct eclipse/sun-gazing, and welding arc exposure.1,2 Thorough history-taking is paramount to ascertain the etiology, since ultra-structural retinal changes due to all the above causes appear similar on OCT.
Solar retinopathy is an acute injury to foveal structures resulting from staring at the sun during a solar eclipse or during normal daylight hours. Patients often correlate the onset of symptoms with the event of sun-gazing or viewing a solar eclipse without protective glasses. Ultraviolet (UV) light from solar radiation is toxic to photoreceptors as well as the RPE. The major component of damage to the retina by UV radiation is through the photochemical pathway. It causes lipid and protein peroxidation in RPE cells, leading to loss of lysosomal integrity and cell death. Various morphological presentations have been described in OCT secondary to solar retinopathy, namely inner retinal layer hyperreflectivity, outer layer hyperreflectivity, full-thickness retinal hyperreflectivity, outer layer retinal defects, and foveal thinning in long-standing cases.3 In the present case series, all patients had outer retinal layer defects on OCT. None had predisposing factors or history of prolonged gazing at the sun. The common factor among them was repeated sunbathing for a few hours.
All of the patients resided in the Solan district of Himachal Pradesh, India. This area is at an altitude of approximately 1,300-1,500 m above sea level and often has snowfall in winters. It is well known that high altitudes above 1,350 m can cause deleterious health effects. The quantity of UV light increases with altitude at a rate of 4% for each 300 m ascent. A combination of high altitude and snow at 2,000 m results in twice the amount of UV light compared to sea level.4
UVB (280-340 nm) waves can cause a wide range of pathologies from snow blindness to skin cancer. UVB rays increase with high altitude, and high surface reflectivity (sand, watery snow, glass, metal) can increase the net solar irradiance.5 Yannuzzi et al.6 observed a similar series of cases with foveal pseudocyst presenting with an acute central scotoma. They had no history of prolonged sun gazing but had sunbathed and exercised under the sun for long hours. The author extensively analyzed the geophysical factors and attributed the occurrence of solar retinopathy to clear sky, exposure to solar noon, and possibly UVB radiation due to relatively lower ozone layers. Age-related lenticular changes reduce the transmission of radiant energy and protect the retina.7,8 In this series, all had a clear lens and were emmetropic, putting them at risk of damage by UV radiation.
The impact of altitude on the retina is secondary to a hypoxic environment. They present with engorged retinal vessels, retinal hemorrhages, and disc edema.9 The patients in this series were habitants of high altitudes. Though changes of altitudinal retinopathy were not seen, its deleterious effects might have added to the insult apart from sunbathing.
The other causes of outer retinal defects in this series were ruled out with good history taking and imaging. None of the patients’ OCT images showed PVD (except patient 1, Figure 1b) or gross vitreoretinal anomalies. The second patient exhibited ILM drape sign (Figure 1a) but the fundus had no parafoveal telangiectatic vessel or grey hue reflex suggestive of macular telangiectasia. No history of any intraocular procedure, topical or systemic medication, or previous hospitalization ruled out other causes of outer retinal defects.
To conclude, the present case series documents the occurrence of outer retinal defects as a presenting feature of solar retinopathy in individuals living at high altitudes who reported prolonged sunbathing under the direct sun to combat the cold climate but denied direct sun-gazing. This series adds additional evidence to the existing literature about the harmful effects of prolonged unprotected sun exposure at high altitudes.
Acknowledgments
We are grateful to Dr. Pratyusha Ganne (consultant, AIIMS Mangalagiri, India) for reviewing the manuscript for grammatical aspects.
Footnotes
Ethics
Peer-review: Externally peer reviewed.
Authorship Contributions
Surgical and Medical Practices: R.S., Concept: R.S., R.G., Rav. G., Design: R.S., N.C.K., Data Collection or Processing: R.S., N.C.K., Analysis or Interpretation: R.S., N.C.K., Literature Search:R.S., N.C.K., R.G., Rav.G., Writing: R.S., N.C.K., R.G., Rav.G.
Conflict of Interest: No conflict of interest was declared by the authors.
Financial Disclosure: The authors declared that this study received no financial support.
References
- 1.Zambarakji HJ, Schlottmann P, Tanner V, Assi A, Gregor ZJ. Macular microholes: pathogenesis and natural history. Br J Ophthalmol. 2005;89:189–193. doi: 10.1136/bjo.2004.052084. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Commander J, Gardiner M, Loewenstein J. High-resolution optical coherence tomography findings in solar maculopathy and the differential diagnosis of outer retinal holes. Am J Ophthalmol. 2011;152:413–419. doi: 10.1016/j.ajo.2011.02.012. [DOI] [PubMed] [Google Scholar]
- 3.Begaj T, Schaal S. Sunlight and ultraviolet radiation-pertinent retinal implications and current management. Surv Ophthalmol. 2018;63:174–192. doi: 10.1016/j.survophthal.2017.09.002. [DOI] [PubMed] [Google Scholar]
- 4.Karaküçük S, Mirza GE. Ophthalmological effects of high altitude. Ophthalmic Res. 2000;32:30–40. doi: 10.1159/000055584. [DOI] [PubMed] [Google Scholar]
- 5.Taylor HR. The biological effects of UV-B on the eye. Photochem Photobiol. 1989;50:489–492. doi: 10.1111/j.1751-1097.1989.tb05553.x. [DOI] [PubMed] [Google Scholar]
- 6.Yannuzzi LA, Fisher YL, Slakter JS, Krueger A. Solar retinopathy: a photobiologic and geophysical analysis. 1989. Retina. 2012;32(Suppl 1):28–43. doi: 10.1097/iae.0b013e31823f9b65. [DOI] [PubMed] [Google Scholar]
- 7.Youssef PN, Sheibani N, Albert DM. Retinal light toxicity. Eye (Lond) 2011;25:1–14. doi: 10.1038/eye.2010.149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Cruickshanks KJ, Klein R, Klein BE. Sunlight and age-related macular degeneration. Arch Ophthalmol. 1993;111:514–518. doi: 10.1001/archopht.1993.01090040106042. [DOI] [PubMed] [Google Scholar]
- 9.McFadden DM, Houston CS, Sutton JR, Powles AC, Gray GW, Roberts RS. High-altitude retinopathy. JAMA. 1981;245:581–586. [PubMed] [Google Scholar]