

Abstract
Untreated systemic hypertension is associated with retinopathy, optic neuropathy, and choroidopathy. Hypertensive choroidopathy is less common than retinal hemorrhages and infarcts seen with accelerated hypertension. The manifestations of choroidopathy include serous retinal detachment, Elschnig spots, and Siegrist streaks. Elschnig spots are yellow demarcated lesions in the perimacular region that leak fluorescein after occlusion of the choriocapillaris. When the Elschnig spot heals, a pigment spot is left surrounded by a depigmented pale halo. Siegrist streaks are linear hyperpigment‐ed streaks over choroidal arteries. Hypertensive choroidopathy has been reported in toxemia of pregnancy, renal disease, pheochromocytoma, and malignant hypertension.
The target organ involvement of the eye is more complex than is commonly appreciated, affecting retinal vessels, choroid, and the optic nerve. Although the retinal vascular changes and optic neuropathy are well known, hypertensive choroidopathy usually does not receive as much attention. Hypertensive choroidopathy (Figure 1 and Figure 2) occurs later than the retinal vascular changes of arteriolar narrowing and arteriovenous crossing changes. 1 These advanced abnormalities are observed more commonly in younger patients with acute increases in blood pressure and are associated with a poor prognosis in the untreated hypertensive patient. Hypertensive choroidopathy has been reported in toxemia of pregnancy, renal disease, pheochromocytoma, and malignant hypertension. 2 The location of these changes is commonly observed in the macular region.
Figure 1.
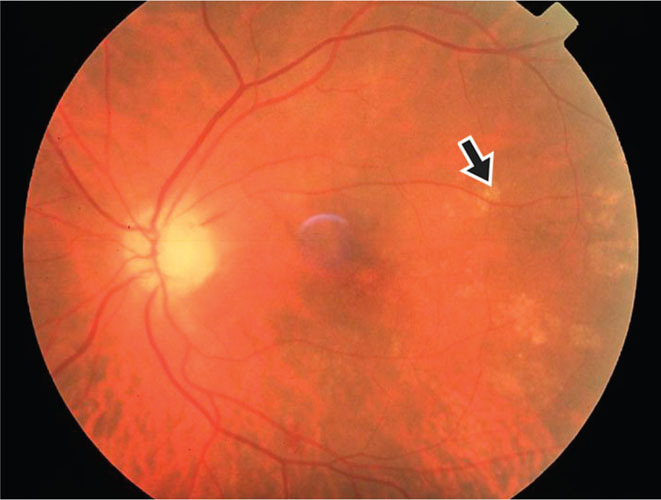
Elschnig spots (arrow) are the changes in the retinal pigment epithelium from nonperfused areas of the choriocapillaris. Photographed by Michael S. Stanley, ophthalmic photographer.
Figure 2.
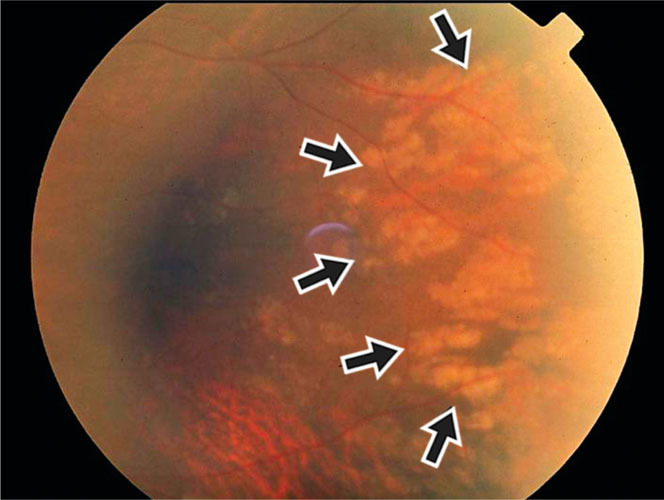
Siegrist streaks (arrows) are linear hyper‐pigmented streaks over choroidal arteries, and they denote ischemia of the choroidal lobules. These streaks observed in the temporal midperipheral retina are more hypopigmented as they are acute and will become pigmented. Photographed by Michael S. Stanley, ophthalmic photographer.
CIRCULATION
The ophthalmic artery branch of the internal carotid artery supplies the optic nerve and retina, extra‐ocular muscles, and eyelids. Branches of ophthalmic artery include the central retinal artery and short and long posterior ciliary arteries. The central retinal artery and vein supply the inner (anterior) two thirds of the retina. 3
The choroid lies between the retinal pigment epithelium and sclera. 4 The choroidal circulation receives blood primarily from the short and long posterior ciliary arteries and delivers blood to the retinal pigment epithelium, optic nerve, and outer (posterior) one third of the retina. The retinal photoreceptors and pigment epithelium are nourished by an inner layer of the choroid which is called the choriocapillaris.
CLINICAL MANIFESTATIONS
Accelerated hypertension and/or ophthalmic/ciliary artery occlusion may result in choroidal ischemia. With complete ophthalmic artery occlusion, both the retinal and choroidal circulations are compromised. Compromise of ciliary arteries may occur without retinal artery involvement, leading to choroidal ischemia, which causes hypertensive choroidopathy (Table I) with or without optic neuropathy. The retinal pigment epithelium becomes necrotic; this may result in areas of serous retinal detachment. Two manifestations of hypertensive choroidopathy are: 1) Elschnig spots (Figure 1) and Figure 2) Siegrist streaks (Figure 2). 5 Elschnig spots are the changes in the retinal pigment epithelium from nonperfused areas of the choriocapillaris. 6 Their appearance is pale or yellow and tends to have defined margins. Once a scar develops, a central pigment is seen within the atrophic region. Siegrist streaks are linear hyperpigmented streaks over choroidal arteries. 4 , 6 These changes are different from the more superficial (anterior) retinal infarcts ("cotton wool spots") and retinal hard exudates observed in accelerated and chronic hypertension. Fluorescein angiography is used to confirm ophthalmoscopic suspicion of hypertensive choroidopathy. In addition to hypertension control and management, carotid ischemia and temporal arte‐ritis need to be considered.
Table.
Pathogenesis of Hypertensive Choroidopathy
| Marked elevation in systemic blood pressure |
| ↓ |
| Autonomic regulatory capacity exceeded |
| ↓ |
| Fibrin‐platelet obstruction |
| ↓ |
| Obstruction of choroid arteries and choriocapillaries |
| ↓ |
| Necrosis of overlying retinal pigment epithelium |
| ↓ |
| Fibrinous exudation |
References
- 1. Wolffsohn JS, Hurcomb PG. Hypertension and the eye. Curr Hypertens Rep. 2002;4:471–476. [DOI] [PubMed] [Google Scholar]
- 2. Tso MO, Jampol LM. Pathophysiology of hypertensive retinopathy. Ophthalmology. 1982;89:1132–1145. [DOI] [PubMed] [Google Scholar]
- 3. Frank RN. The eye in hypertension. In: Izzo JL Jr, Black HR, eds. Hypertension Primer. Dallas , TX : Lippincott Williams & Wilkins; 2003:209–211. [Google Scholar]
- 4. McMahon TT, Maino JH. Hypertensive choroidopathy. J Am Optom Assoc. 1982;53:713–717. [PubMed] [Google Scholar]
- 5. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension. 2003;42:1206–1252. [DOI] [PubMed] [Google Scholar]
- 6. Murphy RP, Chew EY. Hypertension. In: Ryan SJ, ed. Retina. Vol. 2. St. Louis : The CV Mosby Company; 1989:449–455. [Google Scholar]