

Abstract
Erectile dysfunction is a common symptom among hypertensive patients that impairs quality of life and adherence to antihypertensive pharmacologic therapy. It is also associated with cardiovascular risk factors and disease. The Sexual Health Inventory in Men (SHIM) was administered to 105 ambulatory hypertensive patients, and large and small artery elasticity indices were measured. Each variable was examined in a simple linear regression model or 1‐way analysis of variance model to determine each variable's relationship with the SHIM score. Variables that were significantly associated with the SHIM score in the univariate models included age, duration of hypertension, peripheral vascular disease, and small artery elasticity. Large artery elasticity was not significantly associated with the SHIM score. In the multivariate model, age, hypertension duration, and peripheral vascular disease were associated with a lower SHIM score. This study demonstrates a relationship between erectile dysfunction and reduced artery elasticity.
Sexual dysfunction occurs in 31% of men between the ages of 18 and 59 years and is a marker of atherosclerosis. 1 , 2 , 3 , 4 , 5 Given the importance of normal sexual function in society, it is surprising that North American medical schools do not teach human sexuality well. 6
Untreated normotensive men have a lower rate of erectile dysfunction compared with untreated hypertensive men. 5 Whereas short‐term exposure to antihypertensive drugs from various individual classes over a 6–14‐week period is not associated with self‐reported sexual dysfunction, long‐term exposure is linked to specific drug classes. 7 , 8 , 9 Thus, sexual dysfunction requires the attention of clinicians for its impact on quality of life and adherence to antihypertensive therapy, and because it can be a marker for cardiovascular disease.
Our research objective was to study the relationship between erectile dysfunction and arterial elasticity in treated hypertensive men by administering the Sexual Health Inventory in Men (SHIM) and measuring large and small artery elasticity. Additionally, the relationship of cardiovascular risk factors and target organ damage to SHIM score and arterial elasticity was explored.
METHODS
Study Population Study subjects were 106 hypertensive men older than 18 years with a patent right radial artery. Exclusion criteria included an arteriovenous fistula, acute heart failure, atrial fibrillation, moderate mitral or aortic regurgitation, and weight exceeding 350 lb.
Study Design The Human Assurance Committee of the Medical College of Georgia approved the protocol. Adult hypertensive patients attending an ambulatory outpatient clinic were approached to participate if they met the study inclusion and exclusion criteria. All patients were treated with multiple antihypertensive medications. Informed consent was obtained. On completion, a medical history was taken, which included a history of hypertension duration (self‐reported), treated diabetes mellitus, treated lipid disorder, tobacco use (current, former, or never), myocardial infarction, coronary revascularization, heart failure, stroke or transient ischemic attack, and peripheral vascular disease. No specific information was collected on current antihypertensive drug use since most patients received 2 or more medications of varying duration.
The patients completed the International Index of Erectile Function (IIEF‐5), known commonly as SHIM, which contains 5 questions designed to determine: (1) confidence in obtaining an erection, (2) frequency of penetration during intercourse, (3) maintenance of erection after penetration, (4) difficulty in maintenance of an erection during intercourse, and (5) satisfaction with intercourse. This questionnaire tests for the presence of erectile dysfunction and levels of severity and correlates well with self‐assessed severity of erectile dysfunction. 10 , 11 Scores range from 1 to 25, and severity of erectile dysfunction is classified as follows: 22–25, none; 17–21, mild; 12–16, mild‐to‐moderate; 8–11, moderate; and 1–7, severe. The operating characteristics of the SHIM instrument for the diagnosis of erectile dysfunction are: 98% sensitivity, 88% specificity, 89% positive predictive value, and 98% negative predictive value. 10 For severity of erectile dysfunction, the weighted K value, a measure of agreement, was 0.82 (95% confidence interval [CI], 0.80–0.85). 10 The nonparametric Spearman and Kendall (τ‐b) rank‐order correlations between grades of erectile dysfunction were 0.79 (95% CI, 0.76–0.82) and 0.72 (95% CI, 0.69–0.75). 10
The patients were placed in a supine position for 5 minutes, and arterial elasticity was measured with the CR‐2000 Research CardioVascular Profiling System (Hypertension Diagnostics, Inc, Eagan, MN). 12 A foam‐padded wrist stabilizer was placed on the patient's right wrist to stabilize the radial artery to prevent occlusion of the radial artery and to allow adequate venous return from the hand during waveform collections. The noninvasive arterial pressure wave sensor was positioned on the skin above the radial artery and secured by means of a sensor holding and positioning device that used hook‐and‐loop straps. Three measurements were taken approximately 1 minute apart after 5 minutes of rest in the supine position.
The CR‐2000 Research CardioVascular Profiling System has an oscillometric blood pressure module and a piezoelectric pressure sensor that collects radial artery waveform data for 30 seconds. The oscillometric blood pressure measurements show reasonable agreement with mercury measurements. 13 Using pulse‐wave analysis, a software algorithm computes various hemodynamic parameters. A modified Windkessel model is used to calculate the large (C1) and small artery (C2) elasticity. Invasive measurements support the hemodynamic data collected. 12 There is good immediate test‐retest repeatability and intermediate test‐retest repeatability of blood pressure and hemodynamic measurements and arterial elasticity indices. 12 , 14
Statistical Analyses Descriptive statistics were calculated on all variables collected on all individuals. Because multivariable regression was to be used to examine the effect of large artery elasticity and small artery elasticity on the SHIM score, a complete case analysis was used. Any individual with missing data was eliminated from the regression analyses to ensure that the same sample was used when examining each main independent variable and each covariate in the simple and more comprehensive multiple regression models. Only 1 variable, the duration of hypertension, was found to have missing data (n=11) and these individuals were removed from the regression analyses. Chi‐square tests and t tests were used to examine differences between those removed and those not removed from the regression analyses. There were no statistically significant differences on any variable between those removed and not removed.
All variables were examined in a simple linear regression model or 1‐way analysis of variance (ANOVA) model to determine the variable's relationship with the SHIM score. The main independent variables of interest were large artery elasticity and small artery elasticity. Dichotomous categoric variables that were statistically significant in the simple models were used as dummy variables in the multiple regression models. Two different comprehensive models were constructed for each main independent variable. Other variables that were statistically significant in the simple models were entered into these 2 more comprehensive multiple models, and a stepwise model‐building procedure on each model was used to arrive at the final multiple model. The main independent variables were included in each model regardless of their statistical significance. Statistical significance was assessed using an a level of .05, and all statistical analyses were performed using SAS version 9.1.3 (SAS Institute, Cary, NC).
RESULTS
Descriptive statistics and clinical characteristics are displayed in Table I. The population had a mean age of 59 years and was obese, with a mean body mass index of 31 kg/m2. Seventy percent of the population was Caucasian and 30% African American. The self‐reported duration of hypertension was about 14 years. The average blood pressure was 142/83 mm Hg. The prevalence of current tobacco use, a treated lipid disorder, and diabetes mellitus was 22%, 51%, and 25%, respectively. The rate of target organ involvement was: myocardial infarction, 20%; heart failure, 9%; stroke, 12%; peripheral vascular disease, 7%; and coronary revascularization, 17%. Varying degrees of erectile dysfunction were present in 79% of subjects, and 33% had moderate or severe erectile dysfunction.
Table I.
Descriptive Statistics
| Variable | No. | Mean± SD |
|---|---|---|
| Age, y | 106 | 58.74±11.30 |
| Body mass index, kg/m2 | 106 | 31.16±6.29 |
| Duration of hypertension, y | 95 | 13.78±9.92 |
| Systolic blood pressure, mm Hg | 106 | 141.66±17.36 |
| Diastolic blood pressure, mm Hg | 106 | 83.47±11.28 |
| Large artery elasticity, mL/mm Hg × 10 | 106 | 13.96±4.63 |
| Small artery elasticity, mL/mm Hg × 10 | 106 | 5.33±2.88 |
| Sexual Health Inventory in Men score | 106 | 14.73±7.35 |
The simple linear regression and 1‐way ANOVA model results are given in Table II. Variables that were significantly associated with the SHIM score in the simple models include age (Figure 1), duration of hypertension, peripheral vascular disease (Figure 2), and small artery stiffness. The mean small artery elasticity according to the severity of erectile dysfunction is displayed in Figure 3. The mean small artery elasticity according to the number of risk factors (hypertension, diabetes mellitus, dyslipidemia, current or past smoking history) is displayed in Figure 4. Large artery elasticity was not significantly associated with the SHIM score in the simple model.
Table II.
Simple Linear Regression or 1‐Way Analysis of Variance Models on Sexual Health Inventory in Men Score (N=95)
| Variable | Slope or Mean | SE or SD | P |
|---|---|---|---|
| Age | −0.27 | 0.06 | <.0001 |
| Race | .9903 | ||
| White | 15.06 | 7.95 | |
| Black | 15.07 | 6.58 | |
| Hispanic | 14.00 | — | |
| Body mass index | −0.07 | 0.12 | .5765 |
| Hypertension duration | −0.25 | 0.07 | .0010 |
| Tobacco use | .3415 | ||
| Yes | 16.53 | 5.37 | |
| No | 14.68 | 7.94 | |
| Myocardial infarction | .1087 | ||
| Yes | 12.58 | 8.48 | |
| No | 15.67 | 7.17 | |
| Heart failure | .0521 | ||
| Yes | 10.70 | 7.13 | |
| No | 15.56 | 7.42 | |
| Stroke | .0687 | ||
| Yes | 11.18 | 8.74 | |
| No | 15.56 | 7.24 | |
| Peripheral vascular disease | .0028 | ||
| Yes | 6.33 | 5.01 | |
| No | 15.54 | 7.30 | |
| Revascularization | .2470 | ||
| Yes | 13.06 | 7.50 | |
| No | 15.46 | 7.49 | |
| Diabetes | .3882 | ||
| Yes | 13.87 | 7.92 | |
| No | 15.43 | 7.39 | |
| Lipid disorder | .0728 | ||
| Yes | 13.71 | 8.17 | |
| No | 16.48 | 6.52 | |
| Systolic blood pressure | −0.0351 | 0.0438 | .4246 |
| Diastolic blood pressure | 0.0270 | 0.0686 | .6942 |
| Large artery elasticity | −0.0371 | 0.1726 | .8304 |
| Small artery elasticity | 0.6256 | 0.2705 | .0229 |
Figure 1.
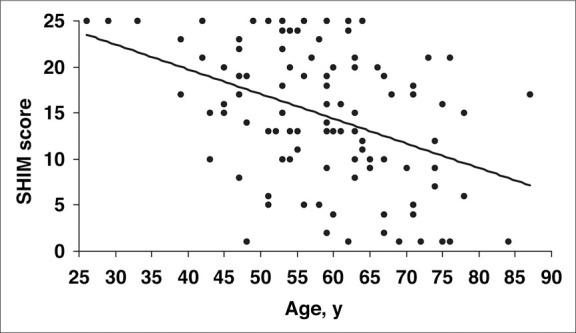
Relationship of age to Sexual Health Inventory in Men (SHIM) score. Increasing age was associated with lower SHIM scores (P<.0001).
Figure 2.
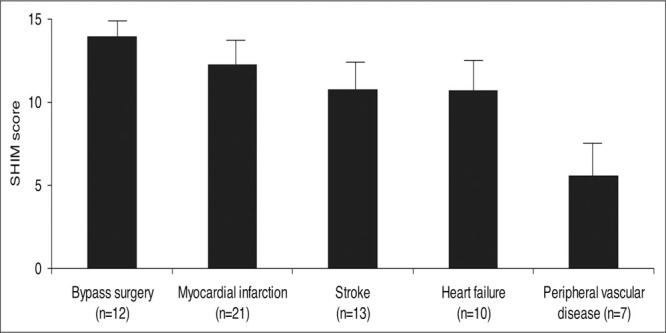
Relationship of target organ damage and Sexual Health Inventory in Men (SHIM) score. Only a history of peripheral vascular disease (P=.0028) was associated with lower SHIM scores. SE is displayed on each bar
Figure 3.
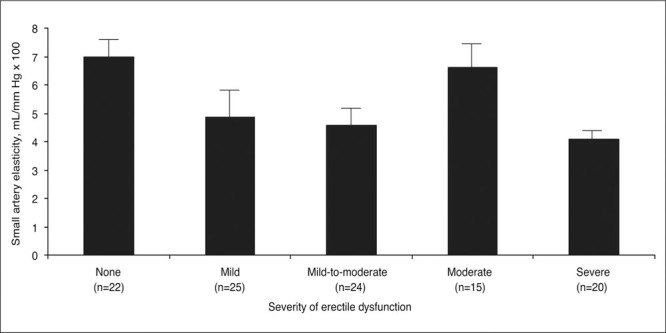
Mean small artery elasticity and severity of erectile dysfunction. As the severity of erectile dysfunction increased, arterial elasticity worsened (P=.0111). SE is displayed on each bar
Figure 4.
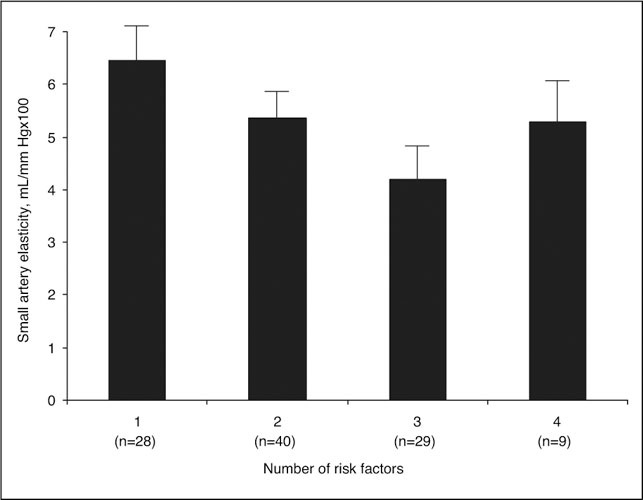
Mean small artery elasticity according to the number of risk factors. Accumulating risk factors were associated, with reduced small artery elasticity. SE is displayed on each bar.
The final multiple regression models are presented in Table III. For large artery elasticity on the SHIM score, the final model consisted of large artery elasticity, age, duration of hypertension, and peripheral vascular disease. Increasing age, longer duration of hypertension, and peripheral vascular disease were associated with declining SHIM scores (ie, more erectile dysfunction). Large artery elasticity remained statistically nonsignificant (P=.1984) in the multivariable model and the estimated coefficient for the slope was in the opposite direction from what was expected. For small artery elasticity on the SHIM score, the final model consisted of small artery elasticity, age, duration of hypertension, and peripheral vascular disease. Small artery elasticity became nonsignificant (P=.O584) in the multivariable model, indicating that there is some potential multicollinearity in the model. The overall multivariable model for small artery elasticity on SHIM score was, however, significant (F4,90=10.95; P<.0001) and the partial R 2 value for small artery elasticity was 0.05. After further investigation of the potential multicollinearity, we found that when age was excluded from the multiple regression models, small artery elasticity was statistically significant. We chose, however, to present the model with both age and small artery elasticity, as both of these variables appear to contribute significantly to the overall R 2 and a larger sample size may reduce the collinearity seen. Thus, the final model for small artery stiffness includes age, hypertension duration, peripheral vascular disease, and small artery elasticity. Increasing age, longer duration of hypertension, peripheral vascular disease, and worsening small artery elasticity (ie, lower small artery elasticity values) were associated with declining SHIM scores (ie, more erectile dysfunction).
Table III.
Final Multivariate Linear Regression Models on Sexual Health Inventory in Men for Large Artery Elasticity and Small Artery Elasticity (N=95)
| Variable | Slope | SE | P |
|---|---|---|---|
| Large artery elasticity | |||
| Age | −0.2372 | 0.0626 | .0003 |
| Hypertension duration | −0.1694 | 0.0701 | .0177 |
| Peripheral vascular disease | −8.9855 | 2.7029 | .0013 |
| Large artery elasticity | −0.2006 | 0.1548 | .1984 |
| Small artery elasticity | |||
| Age | −0.1824 | 0.0612 | .0037 |
| Hypertension duration | −0.1972 | 0.0680 | .0047 |
| Peripheral vascular disease | −8.8735 | 2.6637 | .0013 |
| Small artery elasticity | 0.4607 | 0.2403 | .0584 |
DISCUSSION
Penile erection involves increased arterial inflow, sinusoidal smooth muscle relaxation, and decreased venous outflow. 15 Cavernous arterial flow decreased with increasing age in 64 patients with erectile dysfuntion. 16 Hypertensive patients with erectile dysfunction undergoing pharmacologic duplex ultrasonography have impairment in penile blood flow after papaverine injection. 17
In the present study, the population consisted of older, obese, treated hypertensive patients with multiple risk factors and target organ damage. The severity of SHIM score was associated with worsening small artery elasticity (P=.0584), after controlling for age (P=.0037), hypertension duration (P=.0047), and the presence of peripheral vascular disease (P=.0013). Other risk factors or target organ damage did not show a statistical relationship, but the sample size was relatively small. Increasing numbers of cardiovascular risk factors were associated with decreasing arterial elasticity. This observation is consistent with previous reports that have shown reduced arterial elasticity individually with hypertension, 18 , 19 smoking, 20 and diabetes mellitus. 21
No attempt was made to catalog the multiple antihypertensive medications used by patients in this study. The relationship of SHIM score to the duration of treatment and the number of drugs used would be difficult to tease out in an analysis. It is well known, however, that certain classes of antihypertensive medications are associated with erectile dysfunction. 7 A double‐blind study was conducted among 557 hypertensive men aged between 45 and 69 years. 9 The subjects received intensive lifestyle counseling and were randomized to placebo, acebutolol, amlodipine, chlorthalidone, doxazosin, or enalapril. The incidence of erectile dysfunction after 2 years without problems at baseline was greatest with chlorthalidone (17.1%; P=.004) and lowest with doxazosin (5.6%). The incidence of erectile dysfunction was similar among all treatments, however, by 48 months. The greatest increase in erectile dysfunction from 2 to 4 years was seen among patients receiving placebo, suggesting the importance of blood pressure control.
The relationship of erectile dysfunction and cardiovascular risk factors and events has been reported in several studies. The Massachusetts Male Aging Study 5 evaluated 513 men (97% Caucasian) between the ages of 40 and 70 years.This cohort included men who did not have erectile dysfunction, diabetes, or heart disease at the baseline visit. The average follow‐up period was 8.9 years. The incidence of erectile dysfunction was higher in smokers (24%) than nonsmokers (14%), and in overweight patients (22%) than patients who were not overweight (13%). Erectile dysfunction was 1.79 times more likely to develop if hypertension was present at baseline. Using a Framingham 10‐year coronary heart disease risk formula, the incidence of erectile dysfunction increased from the lowest quartile (7.6%) to the highest quartile (25.4%). The National Health and Nutrition Examination Survey 22 reported that diabetes mellitus, obesity, current smoking, and hypertension were independently associated with the risk of erectile dysfunction in 3566 men 20 years or older.
Another recent study examined 8063 men 55 years or older without a history of cardiovascular disease. 3 Of these, 4247 men did not have erectile dysfunction at the beginning of the study. After adjustment for covariates, the men who subsequently developed erectile dysfunction were 1.25 times more likely to have a cardiovascular event (P=.04). For the cohort that had or developed erectile dysfunction, the risk of angina, myocardial infarction, stroke, heart failure, or a first cardiovascular event was respectively 1.72 (P=.001), 1.60 (P<.001), 1.79 (P=.01), and 1.45 (P<.001) times higher than in men without erectile dysfunction. Thus, both cardiovascular risk factors and cardiovascular events are linked to erectile dysfunction, probably by generalized alterations in arterial function and structure.
The current study attempted to examine the relationship between various risk factors and cardiovascular target organ damage by studying their effect on SHIM score and arterial elasticity. There was no correlation of SHIM score with tobacco use, diabetes mellitus, or dyslipidemia. Only duration of hypertension and peripheral vascular disease were associated with the SHIM score; however, our study was not powered to examine the relationship of various risk factors and cardiovascular target organ damage with the SHIM score.
The relationship of erectile dysfunction with cardiovascular risk factors and local penile hemodynamics is established. As documented by previous studies, erectile dysfunction was common in our population of treated hypertensives with concomitant risk factors and target organ damage. The present study expands the information to document a reduction in small artery elasticity in hypertensive patients with worsening erectile dysfunction that is a function of age and duration of hypertension.
One could simply take the view that there are modern therapies to treat erectile dysfunction, and not be concerned about it. The phosphodiesterase type 5 inhibitors sildenafil, vardenafil, and tadalafil are effective therapies in many hypertensive patients with erectile dysfunction. 23 , 24 , 25 , 26 There is some evidence that aortic stiffness and pulse wave reflection from the periphery may decrease after sildenafil 50 mg. This was reported in a small, randomized, placebo‐controlled, doubleblind study of 24 patients with coronary artery disease. 27 Nonetheless, while it is important to treat erectile dysfunction to enhance quality of life and ensure adherence to pharmacologic antihypertensive therapy to reach treatment goals, it is critically important that we not ignore the other cardiovascular risk factors and diseases that may be present with erectile dysfunction.
CONCLUSIONS
This study observed decreasing small artery elasticity with worsening erectile dysfunction in hypertensive patients.
Disclosure: Pfizer, Inc provided a grant to Helen Fain, RN, for this study. The design of the study, the statistical analysis, and the content of the manuscript were not influenced by the sponsor.
References
- 1. Laumann EO, Paik A, Rosen RC. Sexual dysfunction in the United States: prevalence and predictors. JAMA. 1999;281:537–544. [DOI] [PubMed] [Google Scholar]
- 2. Prisant LM. Sexual dysfunction and hypertension. In: Izzo JL, Black HR, eds. Hypertension Primer. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2003:470–472. [Google Scholar]
- 3. Thompson IM, Tangen CM, Goodman PJ, et al. Erectile dysfunction and subsequent cardiovascular disease. JAMA. 2005;294:2996–3002. [DOI] [PubMed] [Google Scholar]
- 4. Feldman HA, Goldstein I, Hatzichristou DG, et al. Impotence and its medical and psychosocial correlates: results of the Massachusetts Male Aging study. J Urol. 1994;151:54–61. [DOI] [PubMed] [Google Scholar]
- 5. Feldman HA, Johannes CB, Derby CA, et al. Erectile dysfunction and coronary risk factors: prospective results from the Massachusetts Male Aging study. Prev Med. 2000;30:328–338. [DOI] [PubMed] [Google Scholar]
- 6. Solursh DS, Ernst JL, Lewis RW, et al. The human sexuality education of physicians in North American medical schools. Int J Impot Res. 2003;15:S41–S45. [DOI] [PubMed] [Google Scholar]
- 7. Prisant LM, Carr AA, Bottini PB, et al. Sexual dysfunction with antihypertensive drugs. Arch Intern Med. 1994;154:730–736. [PubMed] [Google Scholar]
- 8. Prisant LM, Weir MR, Frishman WH, et al. Self‐reported sexual dysfunction in men and women treated with bisoprolol, hydrochlorothiazide, enalapril, amlodipine, placebo, or bisoprolol/hydrochlorothiazide. J Clin Hypertens (Greenwich). 1999;1:22–26. [PubMed] [Google Scholar]
- 9. Grimm RH Jr, Grandits GA, Prineas RJ, et al. Long‐term effects on sexual function of five antihypertensive drugs and nutritional hygienic treatment in hypertensive men and women. Treatment of Mild Hypertension Study (TOMHS). Hypertension. 1997;29:8–14. [DOI] [PubMed] [Google Scholar]
- 10. Rosen RC, Cappelleri JC, Smith MD, et al. Development and evaluation of an abridged, 5‐item version of the International Index of Erectile Function (IIEF‐5) as a diagnostic tool for erectile dysfunction. Int J Impot Res. 1999;11:319–326. [DOI] [PubMed] [Google Scholar]
- 11. Cappelleri JC, Siegel RL, Glasser DB, et al. Relationship between patient self‐assessment of erectile dysfunction and the sexual health inventory for men. Clin Ther. 2001;23:1707–1719. [DOI] [PubMed] [Google Scholar]
- 12. Prisant LM, Pasi M, Jupin D, et al. Assessment of repeatability and correlates of arterial compliance. Blood Press Monit. 2002;7:231–235. [DOI] [PubMed] [Google Scholar]
- 13. Prisant LM, Resnick LM, Hollenberg SM. Assessment of sequential same arm agreement of blood pressure measurements by a CVProfilor DO‐2020 versus a Baumanometer mercury sphygmomanometer. Blood Press Monit. 2001;6:149–152. [DOI] [PubMed] [Google Scholar]
- 14. Zimlichman R, Shargorodsky M, Boaz M, et al. Determination of arterial compliance using blood pressure waveform analysis with the CR‐2000 system: reliability, repeatability, and establishment of normal values for healthy European population‐the Seven European Sites Study (SESS). Am J Hypertens. 2005;18:65–71. [DOI] [PubMed] [Google Scholar]
- 15. Wespes E. Smooth muscle pathology and erectile dysfunction. Int J Impot Res. 2002;14(suppl 1):S17–S21. [DOI] [PubMed] [Google Scholar]
- 16. Chung WS, Park YY, Kwon SW. The impact of aging on penile hemodynamics in normal responders to pharmacological injection: a Doppler sonographic study. J Urol. 1997;157:2129–2131. [PubMed] [Google Scholar]
- 17. Muller SC, El‐Damanhoury H, Ruth J, et al. Hypertension and impotence. Eur Urol. 1991;19:29–34. [DOI] [PubMed] [Google Scholar]
- 18. McVeigh GE, Burns DE, Finkelstein SM, et al. Reduced vascular compliance as a marker for essential hypertension. Am J Hypertens. 1991;4:245–251. [DOI] [PubMed] [Google Scholar]
- 19. Prisant LM, Resnick LM, Hollenberg SM. Arterial elasticity among normotensive subjects and treated and untreated hypertensive subjects. Blood Press Monit. 2001;6:233–237. [DOI] [PubMed] [Google Scholar]
- 20. McVeigh GE, Morgan DJ, Finkelstein SM, et al. Vascular abnormalities associated with long‐term cigarette smoking identified by arterial waveform analysis. Am J Med. 1997;102:227–231. [DOI] [PubMed] [Google Scholar]
- 21. McVeigh GE, Morgan DR, Allen P, et al. Early vascular abnormalities and de novo nitrate tolerance in diabetes mellitus. Diabetes Obes Metab. 2002;4:336–341. [DOI] [PubMed] [Google Scholar]
- 22. Saigal CS, Wessells H, Pace J, et al. Predictors and prevalence of erectile dysfunction in a racially diverse population. Arch Intern Med. 2006;166:207–212. [DOI] [PubMed] [Google Scholar]
- 23. Kloner RA, Brown M, Prisant LM, et al. Effect of sildenafil in patients with erectile dysfunction taking antihypertensive therapy. Sildenafil Study Group . Am J Hypertens. 2001;14:70–73. [DOI] [PubMed] [Google Scholar]
- 24. Zusman RM, Prisant LM, Brown MJ. Effect of sildenafil citrate on blood pressure and heart rate in men with erectile dysfunction taking concomitant antihypertensive medication. Sildenafil Study Group . J Hypertens. 2000;18:1865–1869. [DOI] [PubMed] [Google Scholar]
- 25. van Ahlen H, Wahle K, Kupper W, et al. Safety and efficacy of vardenafil, a selective phosphodiesterase 5 inhibitor, in patients with erectile dysfunction and arterial hypertension treated with multiple antihypertensives. J Sex Med. 2005;2:856–864. [DOI] [PubMed] [Google Scholar]
- 26. Kloner RA, Mitchell M, Emmick JT. Cardiovascular effects of tadalafil in patients on common antihypertensive therapies. Am J Cardiol. 2003;92:47M–57M. [DOI] [PubMed] [Google Scholar]
- 27. Vlachopoulos C, Hirata K, O'Rourke ME. Effect of sildenafil on arterial stiffness and wave reflection. Vase Med. 2003;8:243–248. [DOI] [PubMed] [Google Scholar]