

Abstract
Background: Attention deficit hyperactivity disorder (ADHD) is among the most common neurodevelopmental disorders in children and adolescents. There is a controversy over the true prevalence of ADHD in Iran, the knowledge of which is crucial for allocating health care resources and identifying research priorities. This is an updated systematic review of the prevalence of ADHD in Iranian children and adolescents.
Methods: For this systematic review, PubMed/Medline, Web of Science, Scopus, PsycINFO, IranPsych, IranMedex, Irandoc, Google Scholar, and grey literature were reached for publications between January 1990 and December 2018 that reported prevalence estimates of ADHD in Iran. Parallel independent assessments were conducted. The Quality Assessment Checklist for Prevalence Studies was used to assess the overall quality of studies.
Results: A total of 34 original studies covering 33 621 Iranian children, adolescents, and adults were included. The included studies were mostly conducted on the population of preschool, elementary, middle, and high school-aged children as well as adolescents. Also, 6 studies addressed university students. Prevalence estimates of ADHD reported varied substantially across the studies and offered a range of heterogeneous data.
Conclusion: Overall, making exact comparisons among studies was not easy because the assessment method and the type of sampling could impact prevalence estimates. These factors need to be considered when comparing data from different studies.
Keywords: Attention deficit disorder with hyperactivity, Iran, Prevalence, Review
↑ What is “already known” in this topic:
There is a controversy over the true prevalence of attention deficit hyperactivity disorder (ADHD) in Iran, the knowledge of which is crucial for allocating health care resources and identifying research priorities. To date, several studies have been conducted on children and adolescents in different cities of Iran. However, these studies have mostly been conducted in specific regions in Iran, and thus lack sufficient sample size.
→ What this article adds:
This systematic review is an update of a previous review published in 2010 and aims to summarize the available studies on the prevalence of ADHD in Iran. Prevalence estimates of ADHD reported varied substantially across the studies included in this review. The diverse prevalence estimates could be explained in part by the diagnostic criteria used to define ADHD, number of informants, sampling method, age and nature of the population studied, ADHD screening tools, and requirement of impairment for the diagnosis.
Introduction
Attention deficit hyperactivity disorder (ADHD) is among the most common neurodevelopmental disorders in children and adolescents (1). Inattention, hyperactivity, and impulsivity are the primary features of ADHD (2). As a global health issue, ADHD causes various adverse health outcomes and financial hardship for families and societies (3). Children with ADHD experience substantial functional impairments such as poor school performance, problematic interpersonal relationships, at risk behaviors, as well as comorbid psychiatric disorders (4,5). ADHD symptoms may persist into adulthood (6). ADHD in adults is associated with impairments in social, academic, or occupational functioning (7). Therefore, early diagnosis and treatment of ADHD may assist patients manage their symptoms successfully.
There is a controversy over the true prevalence of ADHD, the knowledge of which is crucial for allocation of health care resources and identification of research priorities (8). Several literature reviews have reported a wide range of prevalence estimates throughout the world, varying from 1% to 20% among school-aged children (9-11). Variability across studies can be explained in part by the diagnostic criteria used to define ADHD, source of information, and requirement of impairment for the diagnosis (12). Geographical and demographic variables are important contributors to the heterogeneity of ADHD prevalence across studies (13). In addition, cultural attitudes can influence physicians’ diagnosis of ADHD; ie, different cultures have various social for acceptable and normal behavior (13,14).
To date, several studies have been conducted on children and adolescents in different cities of Iran. However, these studies have mostly been conducted in specific regions in Iran, and thus lack sufficient sample size. There is no doubt that an estimated ADHD prevalence from one location is not representative of the overall prevalence among Iranian children and adolescents. To our knowledge, in the past decade, only 2 systematic reviews have been conducted on the prevalence estimates of ADHD in Iran (15,16). This systematic review is an update of a previous review published in 2010 and aims to summarize the available studies on the prevalence of ADHD in Iran. Moreover, a better knowledge of the epidemiology of ADHD in Iran can help to establish priorities for the allocation of mental health resources.
Methods
To identify the prevalence of ADHD among Iranians since 1990, a systematic review of the literature was performed. Studies were included if they used validated tools to assess ADHD diagnosis or symptoms and if they reported prevalence estimates of ADHD or attention deficit and/or hyperactivity symptoms in Iran.
Electronic search
PubMed/Medline, Web of Science, Scopus, PsycINFO, IranPsych, IranMedex, Irandoc, and Google Scholar were searched from January 1990 to December 2018 for articles in English and Farsi. Irandoc, Iran Medex, and IranPsych are Iranian databases, of them the last is specifically designed for psychiatric and psychologic literature.
Keywords for search were as follow: (“attention” AND “deficit” AND “disorder” AND “hyperactivity”), “attention deficit disorder with hyperactivity”, “ADD”, “ADHD”, “hyperkinesis”, combining them with “epidemiology”, “prevalence”, “rate”, “Iran”, “Tehran” (and names of other cities which have universities), “Conners rating scale”, “Rutter rating scale”, “Wender Utah rating scale”. The search was performed by a specific strategy for each database.
Hand searching
All Iranian psychiatry and psychology journals were hand-searched to identify published but not indexed articles. All the booklets of Iranian psychiatry, psychology, and epidemiology congress were also hand-searched.
Gray literature: Gray literature review was performed to identify final reports of research projects, dissertations, and nonpublished theses.
Review procedure
Our initial database search yielded 67 articles, and 47 potentially eligible studies were identified after screening the titles and abstracts. The full-texts of eligible studies were then reviewed, and 26 studies were found to fulfill the inclusion criteria and 21 were excluded (the reasons for exclusion are given in Figure 1). Complementary hand searches and gray literature review yielded 10 additional studies. As a result, a total of 36 studies were included.
Fig. 1.
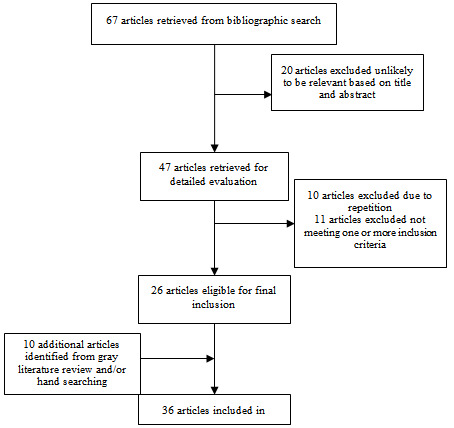
Flow diagram showing selection process of articles included in the systematic review
Data extraction
Parallel independent assessments were conducted to minimize the risk of errors. The extracted data were entered in an electronic data extraction form on Excel.
Quality assessment
We used Quality Assessment Checklist for Prevalence Studies that assesses sampling, measurement, and analysis method of studies with some questions: (1) Does the study design yield a representative sample of respondents to define the target group; (2) Do the survey instruments yield reliable and valid measures of ADHD and other key concepts (the same applies for the translated version); (3) Have the special features of the sampling design been considered in the analysis; and (4) Have subgroups prevalence rates been reported?
Quality Assessment Checklist for Prevalence Studies was performed by 2 scholars from the research team. They conducted a review of each article and reported them independently, and if they both approved the article or the report, we would accept the material; but if either of them rejected the material, a third person reviewed it again.
Statistical analyses
Due to great heterogeneities in the instruments and in the rate of the reported prevalence, we did not conduct analysis but described the results in tables and graphs.
Results
A total of 34 studies (covering 33 621 Iranian children, adolescents, and adults) investigating the prevalence of ADHD in the cities of Iran and 2 reviews of literature on the epidemiology of ADHD in Iran were included. Studies were published from 1999 to 2018. Figure 1 shows the flow diagram of study screening and inclusion process. Characteristics of all included studies are presented in Table 1.
Table 1. Characteristics of the studies included in the systematic review.
| Authors | Year of publication | Sample’s Age | Location | Sample size | Proportion of males (%) | Scale | Prevalence (%) |
| Solaimannigad et al. (17) * | 1999 | 7-11 | Ilam | 2000 | 52 | Child symptom inventory-4 (CSI-4) and clinical interview based on DSM-IV criteria |
Total 4 Male 5.4 Female 2.3 Based on parent report Attention deficit type 7.073 (SD 1.081) Hyperactive/impulsive type 6.607 (SD 0.994) Combined 10.25 (SD 2.329) Based on teacher report Attention deficit type 7.027(SD 1.118) Hyperactive/impulsive type 6.607 (SD 0.994) Combined 10 (SD 1.762) |
| Gelayol et al. (18)* | 2003 | 5 | Tehran | 400 | ? | Child symptom inventory-4 (CSI-4) | Total 11 |
|
Arabgol et al. (19)* |
2004 |
18-32 |
Tehran |
244 |
0 |
Conners' Adult ADHD Rating Scales–Self-Report: Short Version (CAARS–S:S) |
Inattention/Memory problem 2.5 Hyperactivity/Restlessness 7.8 Impulsivity/Emotional lability 4.9 Problems with self-concept 2 ADHD index 3.7 |
|
Tavangar et al. (20)* |
2004 |
7-12 |
Yazd |
1085 |
51.9 |
Child symptom inventory-4 (CSI-4) |
Total 13.4 Attention deficit type 6.8 Hyperactive/impulsive type 9.2 Combined 3.1 |
| Shabani et al. (21)* | 2005 | 7-12 | Zanjan | 428 | ? | Conner’s parent–teacher questionnaire |
Only parent questionnaire 9.1 Only teacher questionnaire 12.2 Both parent and teacher questionnaire 4.9 |
| Hebrani et al. (22) | 2007 | 5-6 | Mashhad | 1083 | 51 | Conner’s parent–teacher questionnaire and clinical interview based on DSM-IV criteria |
Total 12.3(CI95%:10.3 – 14.2) Male 18.1 Female 6.2 |
| Shahim et al. (23)* | 2007 | 7-12 | Shiraz | 1311 | 49 | The SWAN Rating Scale for ADHD | Total 5-8.5 |
| Ghanizadeh (24) | 2008 | 7-12 | Shiraz | 1600 | 50 | Child symptom inventory-4 (CSI-4) |
Total 10.1 Male 13.6 Female 6.5 Attention deficit type Male 5 Female 2.1 Hyperactive-Impulsive type Male 6.1 Female 3.9 Combined Male 2.5 Female 0.5 |
| Akhavan Karbasi et al. (25)* | 2008 | 6 | Yazd | 400 | 50 | Clinical interview based on DSM-IV criteria |
Total 16.3 Male 19.5 Female 13 |
| Moradi et al. (26)* | 2008 | 7-12 | Nishaboor | 722 | 55.7 | Conner’s parent–teacher questionnaire |
Total 12.5(CI95%:10 – 14.8) Male 10.9(CI95%:7.8 – 14) Female 14.3(CI95%:10.5 – 18.2) |
| Najafi et al. (27)* | 2009 | 7-12 | Shiraz | 1205 | 53 |
Child symptom inventory-4 (CSI-4) |
Attention deficit type 6.7 Hyperactive-Impulsive type 6 Combined 5 |
| Amiri et al. (28) | 2010 | 7-15 | Tabriz | 1658 | 52.9 | Conner's teacher rating scale and clinical interview based on DSM-IV-TR criteria |
Total 9.7 Male 12.2 Attention deficit 1.2 Hyperactive/impulsive 0.14 Combined 9.5 Female 7.4 Attention deficit 2.1 Hyperactive/impulsive 0.75 Combined 7.8 |
| Talaei et al. (29) | 2010 | 7-9 | Mashhad | 714 | 100 | 10-item Conner’s parent–teacher questionnaire and clinical interview based on DSM-IV-TR criteria |
Total 15.27±2.64 Attention deficit type 4.62 Hyperactive/impulsive type 5.32 Combined 5.32 |
| Alavi et al. (30) | 2010 | 6-11 | Tehran | 799 | 48.9 |
Strengths and Difficulties Questionnaire (SDQ) parent-report KSADS-Present and Lifetime Version (KSADS-PL) |
Total 8.6 |
| Meysamie et al. (31) | 2011 | 3-6 | Tehran | 1403 | 52 | The Preschool Behavior Questionnaire (PBQ) |
Parent evaluation Total 25.8(CI95%: 23.6-28.1%) Male 32.4(CI95%:28.8-36.2) Female 18.1(CI95%:15.3-21.3) Teacher evaluation Total 17(CI95%: 14.1-20.4) Male 23.2(CI95%: 20-27) Female 10.2(CI95%: 7.4-14) |
| Tashakori et al. (32) | 2011 | 5-6 | Ahvaz | 133 | 100 | Conner’s parent–teacher questionnaire |
Total 24.06 Only parent questionnaire 4.51 Only teacher questionnaire 17.29 Both parent and teacher questionnaire 2.25 |
| Namdari et al. (33) | 2012 | 7-12 | Khorramabad | 945 | 49.3 | The Child Symptom Inventories-4 (CSI-4) |
Total 3.17 Attention deficit type 1.26 Hyperactive type 1.05 Combined 0.84 |
| Bakhshani et al. (34) | 2012 | 17-34 | Sistan and Baluchestan | 403 | 50.2 | Adult ADHD Self-Report Scale (ASRS-v1.1) |
Total 25.1 Attention deficit type 11.3 Hyperactive type 10.3 Combined 3.4 |
| Sadeghi Movahed et al. (35)* | 2012 | 18-26 | Ardabil | 582 | 34.7 | Conner’s' Adult ADHD Rating Scales–Self Report |
Total 8.6 Male 10.8 Female 7.3 |
| Salehi et al. (36)* | 2012 | 7-11 | Arak | 2000 | 52 |
Conner’s parent–teacher questionnaire KSADS-Epidemiological (KSADS-E) |
Attention deficit type 2.2 Hyperactive/impulsive type 3.5 Combined 2.7 |
| Mosalanejad et al. (37) | 2013 | 18-44 | Zahedan | 913 | 35.5 | Conner’s' Adult ADHD Rating Scales–Self Report (Screening Version, CAARS-S:SV) |
Attention deficit type 11.7 Hyperactive type 12 Impulsivity 13.2 Self-concept 3.3 |
| Feiz et al. (38) | 2013 | 6-7 | Tehran | 1000 | 38 | Child symptom inventory-4 (CSI-4) |
Attention deficit type Male 2 Female 2.1 Hyperactive-Impulsive type Male 2.5 Female 2.2 Combined Male 1.1 Female 0.6 |
| Jahangard et al. (39) | 2013 | 18-26 | Hamadan | 387 | 34 |
Self-Report Scale Symptom checklist for adult ADHD (ASRS V1.1) Wender Utah Rating Scale Wender- Reimherr Interview |
Based on ASRS 16.5 Based on Wender–Reimherr structured interview (experts’ rating) 13.4 |
| Moayedi et al. (40)* | 2013 | 6-11 | Bandarabbas | 800 | 50 | Child symptom inventory-4 (CSI-4) |
Parent report 12.3 Attention deficit type 5.5 Hyperactive/impulsive type 3.1 Combined 3.6 Teacher report 11.6 Attention deficit type 5 Hyperactive/impulsive type 3.5 Combined 3.1 |
| Shafaat et al. (41)* | 2013 | 14-17 | Sari | 400 | 54.5 | Conner’s parent questionnaire |
Total 14.2 Male 14.3 Female 13.9 |
| Dodangi et al. (42) | 2014 | 6-18 | Paveh | 379 | 52.8 |
Child symptom inventory-4 (CSI-4) Child Behavior Checklist (CBCL) KSADS-Present and Lifetime Version (KSADS-PL) |
Total 11.9 Male 29 Female 15 |
| Bahramabadi et al. (43)* | 2014 | 7-12 | Hamadan | 1938 | 50.98 | Child symptom inventory-4 (CSI-4) and clinical interview based on DSM-IV-TR criteria |
Total 8.62 Male 12.55 Female 4.53 |
| Parvaresh et al. (44)* | 2014 | 18-26 | Kerman | 414 | 38.4 | ADHD self-report scale for adults and clinical interview based on DSM-IV-TR criteria |
Adult ADHD 3.9 Childhood ADHD 8.5 |
| Alizadeh et al. (45) | 2015 | 7-12 | Birjand | 1381 | 52 | Conner’s Rating Scales and clinical interview based on DSM-IV-TR criteria |
Total 7.2 Male 10.2 Female 3.7 Combined 3.16 Attention deficit type 1.22 Hyperactive type 2.73 |
| Bahrami et al. (46)* | 2016 | 7-12 | Kamyaran | 384 | ? | Child symptom inventory-4 (CSI-4) |
Attention deficit type 8.3 Hyperactive-Impulsive type 9.8 Combined 6.7 |
| Abolhassanzadeh et al. (47) | 2016 | 6-11 | Ardabil | 2628 | 47 |
Conners’ Teacher Rating Scale (CTRS) and clinical interview based on DSM-IV-TR criteria |
Total 9.7 Attention deficit type 2 Hyperactive/impulsive type 6.8 Combined 1 |
| Authors | Year of publication | Sample’s Age | Location | Sample size | Proportion of males (%) | Scale | Prevalence (%) |
| Safavi et al. (48) | 2016 | 6-12 | Shahrekord | 631 | 48.8 | Child symptom inventory-4 (CSI-4) |
Total 17.3 Male 10 Female 7.3 Attention deficit type 5.9 Hyperactive/impulsive type 5.9 Combined 5 |
| Mohammadi et al. (49) | 2016 | 6-18 | Tehran, Shiraz, Isfahan, Tabriz and Mashhad | 2051 | 52 |
Strengths and Difficulties Questionnaire (SDQ) KSADS-Present and Lifetime Version (KSADS-PL) |
Total 3.96 Male 5.03 Female 2.79 |
| Faraji-Goodarzi et al. (50) | 2017 | 6-11 | Khorramabad | 1200 | 50 | Questionnaires using ADHD scale-IV |
Total 5.6 Male 6.8 Female 4.3 |
| Total sample size: 33621 | |||||||
| Shooshtary et al. (systematic review) (15) | 2010 | 4-32 | All cities of Iran | ||||
|
Yadegari et al. (Systematic review and Meta-analysis) (16) |
2018 |
6-14 |
All cities of Iran |
15124 |
Prevalence of ADHD Based on parents and teachers' consensus: 12% (CI 95%: 9.0 - 15) From parents' perspective 15.6% (CI 95%: 9.8 - 21.5) From teachers' perspective 17.2% (CI 95%: 12.7 - 21.8) Subgroups' prevalence rates Attention deficit 4.2 hyperactive impulsive 4.1 Combined type 3.5% |
*Studies published in Persian
The included studies were mostly conducted on the population of preschool, elementary, middle, and high school-aged children as well as adolescents. Six studies addressed university students. Of the 36 studies included, all except 3 involved both male and female participants.
Overall prevalence of ADHD
Prevalence estimates of ADHD reported varied substantially across the studies and offered a range of heterogeneous data.
Prevalence of ADHD in preschool children
Five studies evaluated the prevalence of ADHD in preschoolers (18,22,25,31,32).These studies were conducted in Tehran, Mashhad, Yazd, and Ahvaz. Collectively, these studies included 3419 children. Data collection tools used were Child symptom inventory-4 (CSI-4), Conners' Parent & Teacher Rating Scale (CTRS), Preschool Behavior Questionnaire (PBQ), and clinical interviews based on DSM-IV and DSM-IV-TR criteria. Total prevalence of ADHD ranged between 11% in the study of Gelayol et al (18) and 25.8% in the study of Meysamie et al (31). Figures were higher in boys (18.1% to 32.4%) (22,31) than in girls (6.2% to 18.1%) (22,31).
Prevalence of ADHD in school-aged children
Twenty-three studies assessed the prevalence of ADHD in school-aged children and adolescents, most of whom addressed elementary school students. These studies were conducted in Tehran, Khorramabad, Shiraz, Isfahan, Tabriz, Mashhad, Shahrekord, Ardabil, Kamyaran, Birjand, Hamadan, Nishaboor, Paveh, Sari, Arak, Bandarabbas, Yazd, and Ilam. As a whole, these studies included 27,259 children and adolescents. Data collection tools used were Conners' Parent & Teacher Rating Scale (CTRS), teacher and parent versions of Child Symptom Inventory-4 (CSI-4) , the SWAN Rating Scale for ADHD, Strengths and Difficulties Questionnaire (SDQ), KSADS-Present and Lifetime Version (KSADS-PL), KSADS-Epidemiological (KSADS-E), Child Behavior Checklist (CBCL), and clinical interviews based on DSM-IV and DSM-IV-TR criteria. Total prevalence of ADHD ranged between 3.17% in the study of Namdari et al (33) and 17.3% in the study of Safavi et al (48). Overall, figures were higher in boys (5.03% to 29%)(42,49) than in girls (2.3% to 15%) (17,42), except in the study of Nishaboor (26) in which girls had higher figures than boys (14.35 versus 10.9%). The prevalence of the subtypes of ADHD varied significantly across the studies.
Prevalence of ADHD in adults
Six studies evaluated the prevalence of ADHD in university students (19,34,35,37,39,44). The studies were performed in Kerman, Hamadan, Sistan and Baluchestan, Zahedan, Ardabil, and Tehran. Together these studies included 2943 university students. Data were collected using Conners' Adult ADHD Rating Scales (CAARS-S:S), Adult ADHD Self-Report Scale (ASRS-v1.1), Wender Utah Rating Scale, Wender–Reimherr structured interview, and clinical interviews based on DSM-IV and DSM-IV-TR criteria. Total prevalence of ADHD ranged between 3.9% in the study of Parvaresh et al (44) and 25.1% in that of Bakhshani et al (34). Only 3 studies reported the prevalence rates based on gender. In the studies published by Sadeghi Movahed et al (35) and Bakhshani et al (34) ADHD was more common in males than in females and in the study of Jahangard et al (39) the prevalence estimates for ADHD in adults did not differ significantly between genders.
Discussion
We conducted a comprehensive systematic review of studies addressing prevalence rates of ADHD in Iran. Methodological characteristics were coded for each study, including the size of sample, rate of response, source of information, and whether the diagnosis followed the DSM criteria. These data must be interpreted with caution because of the high variability present in the conducted analyses. Perhaps the diverse prevalence estimates reported in the studies could be explained in part by the diagnostic criteria used to define ADHD, number of informants, sampling method, age, and nature of the population studied, ADHD screening tools, and requirement of impairment for the diagnosis.
Most of the Iranian studies included in our review only used rating scales to diagnose ADHD. Previous studies have shown screening with questionnaires identifies higher rates of the population as affected, while studies focused on ADHD using definitions based on DSM report lower prevalence rates (51). Furthermore, different rating scales such as Conners, Rutter and CSI-4 have been used in the included studies. These assessment tools have different diagnostic performance in sensitivity, specificity, and diagnostic odds ratios. It seems when diagnosis was made based on DSM criteria, the heterogeneity dropped. Additional differences in the prevalence estimates can be attributed to the differences in the study populations.
No representative community sample was present in the studies included in our review. This affects the reported prevalence rate. A number of studies have found that parents and teachers’ ratings of ADHD symptoms are only weakly to moderately correlated (52,53). An American epidemiological analysis found that community samples showed higher prevalence rates than school samples (mean prevalence: 10.3% for community samples as compared with 6.9% for school samples) (54).
Another important finding is that the rate of combined type is the least in all studies except the studies conducted in Tabriz and Ilam, and in few studies inattentive type is more frequent than hyperactive-impulsive type (8,12,17,18,24). In line with our results, several studies have reported a lower prevalence of combined subtype symptoms than other ADHD subtypes. However, other studies have found the combined type to be the most prevalent for both boys and girls (55,56).
The diverse prevalence estimates reported in the studies may be partly due to differences in the sex ratio and age range of study subjects. It is often believed that the prevalence of ADHD in boys is considerably higher than in girls, particularly in children. Likewise, the prevalence of ADHD varies with age. The intensity and number of ADHD symptoms decrease with age, suggesting lower rates of ADHD detection in adults. Previous studies have shown a decline in the ADHD prevalence with increasing age over the age range of 10-20 (57), 8-15 (58), and 6-14 years (59). Therefore, even within studies conducted on children, the age range of participants can potentially influence the apparent prevalence. Most of the studies in Iran have been performed on school-aged children. Although the respective analyses were conducted in similar age groups, the heterogeneity did not decrease. Dramatic differences exist among rates in the studies conducted in adults. The lowest rates were obtained in Kerman (3.9%) (44), Tehran (3.7%) (19), and Ardabil (8.6%) (35), which used ADHD self-report scale for adults and clinical interview based on DSM-IV-TR criteria, Conner’s' Adult ADHD Rating Scales–Self Report, and Conner’s' Adult ADHD Rating Scales–Self Report, respectively. The highest rates were obtained in Hamadan (16.5%) (39), Zahedan (12%) (37) and Sistan and Baluchestan (25.1%) (34), which used Self-Report Scale Symptom checklist for adult ADHD, Conner’s' Adult ADHD Rating Scales–Self Report, and Adult ADHD Self-Report Scale, respectively. It seems such differences are not plausible based on biological context, so cultural explanation would explain them better. There are, however, other possible explanations. First, there are not enough psychiatric services in the areas with high rates of ADHD adults. Second, there is higher stigma to see a psychiatrist in these areas. It brings a question whether they have higher rates of adult ADHD because they did not get any treatment at their childhood. Another possible explanation for the higher prevalence of ADHD in these regions is that people may be from linguistically diverse backgrounds, and language barriers contribute to poorer understanding of questionnaires, and eventually inaccurate patient assessment.
The diagnosis of ADHD is influenced by cultural factors, meaning that tolerance of hyperactive behavior may differ across cultures. Therefore, ADHD would not be as noticeable by adults in some cultures (60). Cultural attitudes also influence the type of care patients prefer, accessibility of health care services, and level of trust in health care systems (61).
Study limitations
The findings in this report are subject to at least 2 limitations. First, most studies included in this systematic review have used rating scales rather than diagnostic interviews. In contrast to the rating scale methods, the interview-based assessments more closely mirror the diagnostic evaluation done by experienced clinicians and might well incorporate the DSM criteria for ADHD diagnosis. Second, a number of studies have only reported the mean scale scores, which need to be interpreted cautiously, because it is not clear how many individuals scored above the diagnostic cut-off point.
Conclusion
Overall, making exact comparisons among studies was not easy because the assessment method and type of sampling may impact prevalence estimates. These factors need to be considered when comparing data from different studies.
Acknowledgment
The authors appreciate the valuable comments of unknown reviewers.
Conflict of Interests
The authors declare that they have no competing interests.
Cite this article as: Hakim Shooshtari M, Shariati B, Kamalzadeh L, Naserbakht M, Tayefi B, Taban M. The prevalence of attention deficit hyperactivity disorder in Iran: An updated systematic review. Med J Islam Repub Iran. 2021 (14 Jan);35:8. https://doi.org/10.47176/mjiri.35.8
References
- 1.Thapar A, Cooper M. Attention deficit hyperactivity disorder. Lancet (London, England) 2016;387(10024):1240–50. doi: 10.1016/S0140-6736(15)00238-X. [DOI] [PubMed] [Google Scholar]
- 2. Association AP. Diagnostic and statistical manual of mental disorders (DSM-5®): American Psychiatric Pub; 2013. [DOI] [PubMed]
- 3.Asherson P, Buitelaar J, Faraone SV, Rohde LA. Adult attention-deficit hyperactivity disorder: key conceptual issues. Lancet Psychiatry. 2016;3(6):568–78. doi: 10.1016/S2215-0366(16)30032-3. [DOI] [PubMed] [Google Scholar]
- 4.Harpin V, Mazzone L, Raynaud JP, Kahle J, Hodgkins P. Long-Term Outcomes of ADHD: A Systematic Review of Self-Esteem and Social Function. J Atten Disord. 2016;20(4):295–305. doi: 10.1177/1087054713486516. [DOI] [PubMed] [Google Scholar]
- 5.Shaw M, Hodgkins P, Caci H, Young S, Kahle J, Woods AG. et al. A systematic review and analysis of long-term outcomes in attention deficit hyperactivity disorder: effects of treatment and non-treatment. BMC Med. 2012;10:99. doi: 10.1186/1741-7015-10-99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Barkley RA, Fischer M, Smallish L, Fletcher K. The persistence of attention-deficit/hyperactivity disorder into young adulthood as a function of reporting source and definition of disorder. J Abnorm Psychol. 2002;111(2):279–89. [PubMed] [Google Scholar]
- 7.Ramos-Quiroga JA, Montoya A, Kutzelnigg A, Deberdt W, Sobanski E. Attention deficit hyperactivity disorder in the European adult population: prevalence, disease awareness, and treatment guidelines. Curr Med Res Opin. 2013;29(9):1093–104. doi: 10.1185/03007995.2013.812961. [DOI] [PubMed] [Google Scholar]
- 8.Singh I. Beyond polemics: science and ethics of ADHD. Nat Rev Neurosci. 2008;9(12):957–64. doi: 10.1038/nrn2514. [DOI] [PubMed] [Google Scholar]
- 9.Thomas R, Sanders S, Doust J, Beller E, Glasziou P. Prevalence of attention-deficit/hyperactivity Disorder: A systematic review and meta-analysis. Pediatrics. 2015;135(4):e994–e1001. doi: 10.1542/peds.2014-3482. [DOI] [PubMed] [Google Scholar]
- 10.Guilherme P, Lessa Horta B, Biederman J, Augusto Rohde L. The worldwide prevalence of ADHD: A systematic review and metaregression analysis. Am J Psychiatry. 2007;164(6):942–8. doi: 10.1176/ajp.2007.164.6.942. [DOI] [PubMed] [Google Scholar]
- 11.Liu A, Xu Y, Yan Q, Tong L. The prevalence of attention deficit/hyperactivity disorder among Chinese children and adolescents. Sci Rep. 2018;8(1):11169. doi: 10.1038/s41598-018-29488-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Willcutt EG. The prevalence of DSM-IV attention-deficit/hyperactivity disorder: a meta-analytic review. Neurotherapeutics. 2012;9(3):490–9. doi: 10.1007/s13311-012-0135-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Miyasaka M, Kajimura S, Nomura M. Biases in understanding attention deficit hyperactivity disorder and autism spectrum disorder in Japan. Front Psychol. 2018;9:244. doi: 10.3389/fpsyg.2018.00244. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Polanczyk G, de Lima MS, Horta BL, Biederman J, Rohde LA. The worldwide prevalence of ADHD: a systematic review and metaregression analysis. Am J Psychiatry. 2007;164(6):942–8. doi: 10.1176/ajp.2007.164.6.942. [DOI] [PubMed] [Google Scholar]
- 15.Shooshtary MH, Chimeh N, Najafi M, Mohamadi MR, Yousefi-Nouraie R, Rahimi-Mvaghar A. The prevalence of attention deficit hyperactivity disorder in Iran: a systematic review. Iran J Psychiatry. 2010;5(3):88–92. [PMC free article] [PubMed] [Google Scholar]
- 16.Yadegari N, Sayehmiri K, Azodi MZ, Sayehmiri F, Modara F. The prevalence of attention deficient hyperactivity disorder among Iranian children: A meta-analysis. Iran J Psychiatry Behav Sci. 2018;12(4) [Google Scholar]
- 17.Solaiman Nigad H, Kalantai M, Ahmadi S. Epidemiologic study of attention deficit hyperactivity disorder among students of 7-11 years old at pimary schools of Ilam. J Ilam Univ Med Sci. 1999;9(31):30–5. [Google Scholar]
- 18.Gelayol A, Farhud D, Shahmohammadi D. Hyperactivity, attention and concentration deficit in preschool children. Iran J Pediatr. 2003;12(4):53–7. [Google Scholar]
- 19.Arabgol F, Hayati M, Hadid M. Prevalence of attention - deficit/hyperactivity disorder in a group of university students. iricss. 2004;6(1):73–87. [Google Scholar]
- 20.Tavangar H, Morowati Sharifabad MA, Pourmovahed Z, Dehghani K. Prevalence and related factors of attention deficit hyperactivity disorder in students of Yazd primary schools (2004) J Qazvin Univ Med Sci. 2008;12(2):20–25. [Google Scholar]
- 21.Shabani M, Yadegari A. prevalence of attention deficit hyperactivity disorder (ADHD) in elementary school children in Zanjan 2004 - 2005. J Zanjan Univ Med Sci. 2005;13(51):42–8. [Google Scholar]
- 22.Hebrani P, Abdolahian E, Behdani F, Vosoogh I, Javanbakht A. The prevalence of attention deficit hyperactivity disorder in preschool-age children in Mashhad, North-East of Iran. Arch Iran Med. 2007;10(2):147–51. [PubMed] [Google Scholar]
- 23.Shahim S, Mehrangiz L, Yousefi F. Prevalence of attention deficit hyperactivity disorder in a group of elementary school children. Iran J Pediatr. 2007;17(2) [Google Scholar]
- 24.Ghanizadeh A. Distribution of symptoms of attention deficit-hyperactivity disorder in schoolchildren of Shiraz, South of Iran. Arch Iran Med. 2008;11(6):618–24. [PubMed] [Google Scholar]
- 25.Akhavan Karbasi S, Golestan M, Fallah R, Sadr Bafghi M. Prevalence of Attention Deficit Hyperactivity Disorder in 6 Year Olds of Yazd City. J Shahid Sadoughi Univ Med Sci. 2008;15(4):29–34. [Google Scholar]
- 26.Moradi A, Khabazkhoob M, Agah T, Javaherforoushzadeh A, Rezvan B, Haeri Kermani Z. et al. The prevalence of attention deficit hyperactivity disorder (ADHD) among school children of Nishaboor – Iran during 2006. J Gorgan Univ Med Sci. 2008;10(2):37–42. [Google Scholar]
- 27.Najafi M, Foladchang M, Alizadeh H, Mohammadifar M. Prevalence of attention deficit hyperactivity disorder, conduct disorder and oppositional defiant disorder. J Except Child. 2009;9(3):239–54. [Google Scholar]
- 28.Amiri S, Fakhari A, Maheri M, Mohammadpoor Asl A. Attention deficit/hyperactivity disorder in primary school children of Tabriz, North-West Iran. Paediatr Perinat Epidemiol. 2010;24(6):597–601. doi: 10.1111/j.1365-3016.2010.01145.x. [DOI] [PubMed] [Google Scholar]
- 29.Talaei A, Mokhber N, Abdollahian E, Bordbar MRF, Salari E. Attention deficit/hyperactivity disorder: A survey on prevalence rate among male subjects in elementary school (7 to 9 years old) in Iran. J Atten Disord. 2010;13(4):386–90. doi: 10.1177/1087054708329886. [DOI] [PubMed] [Google Scholar]
- 30.Alavi A, Mohammadi MR, Joshaghani N, Mahmoudi-Gharaei J. Frequency of psychological disorders amongst children in urban areas of Tehran. Iran J Psychiatry. 2010;5(2):55. [PMC free article] [PubMed] [Google Scholar]
- 31.Meysamie A, Fard MD, Mohammadi MR. Prevalence of attention-deficit/hyperactivity disorder symptoms in preschool-aged Iranian children. Iran J Pediatr. 2011;21(4):467–72. [PMC free article] [PubMed] [Google Scholar]
- 32.Tashakori A, Afkandeh R. Prevalence of ADHD symptoms amonge male preschoolers based on different informants in Ahvas city of Iran. ISRN pediatrics. 2011;2011:709653. doi: 10.5402/2011/709653. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Namdari P, Nzari H, Pournia Y. Epidemiologic feature of attention deficit and hyperactivity disorder (ADHD) in elementary school children. Hong Kong J Paediatr. 2012;17:162–6. [Google Scholar]
- 34.Bakhshani NM, Babaei S, Raghibi M. Self-reported ADHD symptoms prevalence in a university student population: Using adult self-report-V11 screener. Mod Appl Sci. 2012;6(8):63–7. [Google Scholar]
- 35.Sadeghi Movahed F, Molavi P, Samadzadeh M, Shahbazzadegan B, Askari Moghadam R. Prevalence of ADHD among the students residing in dormitory of Ardabil university of medical sciences. J Ardabil Univ Med Sci. 2012;12(5):87–94. [Google Scholar]
- 36.Salehi B, Ebrahimi S, Moradi S. The relationship between attention deficit hyperactivity disorder and comorbid disorders among primary students in one Arak area. J Hormozgan Univ Med Sci. 2012;16(1):49–59. [Google Scholar]
- 37.Mosalanejad M, Mosalanejad L, Lashkarpour K. Prevalence of ADHD among students of zahedan university of medical science in iran. Iran J Psychiatry Behav Sci. 2013;7(2):83–90. [PMC free article] [PubMed] [Google Scholar]
- 38.Feiz P, Emamipour S. A survey on prevalence rate of attention-deficit hyperactivity disorder among elementary school students (6-7 years old) in Tehran. Procedia Soc Behav Sci. 2013;84:1732–5. [Google Scholar]
- 39.Jahangard L, Haghighi M, Bajoghli H, Holsboer-Trachsler E, Brand S. Among a sample of Iranian students, adult attention deficit hyperactivity disorder is related to childhood ADHD, but not to age, gender, socioeconomic status, or birth order--an exploratory study. Int J Psychiatry Clin Pract. 2013;17(4):273–8. doi: 10.3109/13651501.2013.800555. [DOI] [PubMed] [Google Scholar]
- 40.Moayedi F, Moayedi A, Goli G, Hemedi Y. Prevalence of attention deficit hyperactivity disorder in Bandarabbas primary school students in 2010. Hormozgan Univ Med Sci. 2013;17(3):241–7. [Google Scholar]
- 41.Shafaat A, Tirgari-Seraj A, Daneshpoor SMM, Hajian M, Khademloo M. Prevalence of attention deficit hyper activity disorder in High-School Students of Sari, Iran. J Mazandaran Univ Med Sci. 2013;23(104) [Google Scholar]
- 42.Dodangi N, Habibi Ashtiani N, Valadbeigi B. Prevalence of DSM-IV TR psychiatric disorders in children and adolescents of Paveh, a Western City of Iran. Iran Red Crescent Med J. 2014;16(7) doi: 10.5812/ircmj.16743. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Bahramabadi M, Ganji K. The study of prevalence of attention deficit / hyperactivity disorder (ADHD) and it’s comorbidity with learning disorder (LD) in primary school’s students. J Learn Disabil. 2014;3(4):25–43. [Google Scholar]
- 44.Parvaresh N, Ziaadini H, Erfani R, Shokoohi M. Prevalence of attention deficit hyperactivity disorder and its relation with depression. J Gorgan Univ Med Sci. 2014;16(1):94–9. [Google Scholar]
- 45.Alizadeh H, Armion E, Coolidge F, D D. Flores Z, E Sutton C The Prevalence of attention-deficit/ hyperactivity disorder among primary school students in an Iranian rural region. Psychology. 2015;06(03):263–268. [Google Scholar]
- 46.Bahrami M, Yousefi F, Bahrami A, Farazi E, Bahrami A. The prevalence of attention deficit – hyperactivity disorder and related factors, among elementary school student in Kamyaran city in 2014-2015. Shenakht J Psychol Psychiatry. 2016;3(3):1–11. [Google Scholar]
- 47.Abolhassanzadeh M, Shafiee-Kandjani AR, Vaziri Z, Molavi P, Sadeghi-movahhed F, Noorazar G. et al. The prevalence and risk factors of attention deficit hyperactivity disorder among the elementary school students in Ardabil, Iran, in 2011-2012. J Anal Res Clin Med. 2016;4(3):146–52. [Google Scholar]
- 48.Safavi P, Ganji F, Bidad A. Prevalence of attention-deficit hyperactivity disorder in students and needs modification of mental health services in Shahrekord, Iran in 2013. J Clin Diagn Res : JCDR. 2016;10(4):Lc25–8. doi: 10.7860/JCDR/2016/14481.7671. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Mohammadi MR, Ahmadi N, Salmanian M, Asadian-Koohestani F, Ghanizadeh A, Alavi A. et al. Psychiatric disorders in Iranian children and adolescents. Iran J Psychiatry. 2016;11(2):87–98. [PMC free article] [PubMed] [Google Scholar]
- 50.Faraji-Goodarzi M, Taee N, Gharib-zadeh F. Prevalence of attention deficit hyperactivity disorder of primary school students in Khorramabad. Early Child Dev Care. 2018:1–8. [Google Scholar]
- 51.Papageorgiou V, Kalyva E, Dafoulis V, Vostanis P. Differences in parents' and teachers' ratings of ADHD symptoms and other mental health problems. Eur J Psychiatry. 2008;22(4):200–10. [Google Scholar]
- 52.Narad ME, Garner AA, Peugh JL, Tamm L, Antonini TN, Kingery KM. et al. Parent–teacher agreement on ADHD symptoms across development. Psychol Assess. 2015;27(1):239–48. doi: 10.1037/a0037864. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Sollie H, Larsson B, Mørch W-T. Comparison of mother, father, and teacher reports of ADHD core symptoms in a sample of child psychiatric outpatients. J Atten Disord. 2012;17(8):699–710. doi: 10.1177/1087054711436010. [DOI] [PubMed] [Google Scholar]
- 54.Brown RT, Freeman WS, Perrin JM, Stein MT, Amler RW, Feldman HM. et al. Prevalence and assessment of attention-deficit/hyperactivity disorder in primary care settings. Pediatrics. 2001;107(3):e43–e. doi: 10.1542/peds.107.3.e43. [DOI] [PubMed] [Google Scholar]
- 55.Cardo E, Servera M, Llobera J. Estimation of the prevalence of attention deficit hyperactivity disorder among the standard population on the island of Majorca. Rev Neurol. 2007;44(1):10–4. [PubMed] [Google Scholar]
- 56.Montiel-Nava C, Pena JA, Lopez M, Salas M, Zurga JR, Montiel-Barbero I. et al. Estimations of the prevalence of attention deficit hyperactivity disorder in Marabino children. Rev Neurol. 2002;35(11):1019–24. [PubMed] [Google Scholar]
- 57.Cohen P, Cohen J, Kasen S, Velez CN, Hartmark C, Johnson J. et al. An epidemiological study of disorders in late childhood and adolescence--I Age- and gender-specific prevalence. J Child Psychol Psychiatry. 1993;34(6):851–67. doi: 10.1111/j.1469-7610.1993.tb01094.x. [DOI] [PubMed] [Google Scholar]
- 58.Gomez-Beneyto M, Bonet A, Catala MA, Puche E, Vila V. Prevalence of mental disorders among children in Valencia, Spain. Acta Psychiatr Scand. 1994;89(5):352–7. doi: 10.1111/j.1600-0447.1994.tb01528.x. [DOI] [PubMed] [Google Scholar]
- 59.Breton JJ, Bergeron L, Valla JP, Berthiaume C, Gaudet N, Lambert J. et al. Quebec child mental health survey: prevalence of DSM-III-R mental health disorders. J Child Psychol Psychiatry. 1999;40(3):375–84. [PubMed] [Google Scholar]
- 60.Gómez-Benito J, Van de Vijver FJR, Balluerka N, Caterino L. Cross-Cultural and Gender Differences in ADHD Among Young Adults. J Atten Disord. 2015;23(1):22–31. doi: 10.1177/1087054715611748. [DOI] [PubMed] [Google Scholar]
- 61.Livingston R. Cultural Issues in Diagnosis and Treatment of ADHD. J Am Acad Child Adolesc Psychiatry. 1999;38(12):1591–4. doi: 10.1097/00004583-199912000-00021. [DOI] [PubMed] [Google Scholar]