

Abstract
Objectives:
To evaluate the precision of the virtual occlusal record using the Carestream CS3600 Intraoral Scanner (Carestream Dental, Atlanta, Ga).
Materials and Methods:
A total of 20 participants were recruited for this prospective study using preestablished inclusion/exclusion criteria. A complete intraoral scan and two bite registrations were obtained. The participants were instructed to bite with normal pressure when bite registrations were acquired. Contact locations, size (circumference), and intensity were identified on the maxillary first molars and canines. Agreement between contact size and intensity was assessed with intraclass correlation coefficients. Kappa statistics evaluated agreement in contact locations. Statistical significance was set at P < .05.
Results:
All participant data were included for statistical analysis. Between the two bite registrations, nonstatistically significant differences were observed in the proportion of locations with contacts (P = .7681). A nonstatistically significant difference (−0.25 mm, P = .8416) in mean contact circumference size was observed. A statistically significant difference in mean contact intensity was observed (P = .0448). When evaluating agreement between the bite registrations, a weak correlation for size (intraclass correlation coefficient = 0.35) and intensity (intraclass correlation coefficient = 0.32) was observed as well as a moderate agreement for contact location (κ coefficient = 0.67).
Conclusions:
The findings suggest that the Carestream intraoral scanner software possesses adequate precision when acquiring the location and size of the contacts in bite registrations. The scanner failed to demonstrate adequate precision when acquiring contact intensities in bite registrations. Additional research is warranted to further investigate the precision of virtual occlusal records with currently available software systems.
Keywords: Virtual occlusal record, Precision, Bite registration, Intraoral scanner
INTRODUCTION
Digital impressions made from an intraoral scanning system were introduced in the 1980s.1 They are becoming increasingly popular in dental offices because they are more comfortable for the patient, more time efficient, conserve materials for the dentist, do not require physical storage space, and do not distort over time as seen with impression materials.2
Both the accuracy and the precision of the intraoral scan are important parameters. Accuracy is the closeness of agreement between a test result and the accepted reference value,3 whereas precision is the closeness of agreement between independent test results obtained under stipulated conditions. Precision measures the repeatability or reproducibility of a method or value. A value obtained that is reproducible but not close to the accepted reference value of what is being measured is identified as a precise value, but not accurate.3 Such measures influence the digital model produced, which is used for various purposes including the fabrication of restorations and diagnosis of occlusion. The occlusion, determined by the virtual bite registration, can be used in numerous dental applications, specifically in orthodontics when planning treatment for orthognathic surgery4 and full-arch equilibration.5
There are multiple intraoral scanning systems available on the market, and previous studies have compared different scanners among themselves as well as against one another.6–9 Most of these studies substituted the term truism for accuracy. Imburgia et al.6 compared the precision and trueness of four popular intraoral scanners in oral implantology. They found significant differences in trueness but no differences in precision between the CS3600 (Carestream Dental, Atlanta, Ga), Trios3 (3Shape, Copenehagen, Denmark), Omnicam (Dentsply Sirona, York, Pa) and TrueDefinition (3M OralCare, St Paul, Mn) scanners. Park7 used a phantom model to evaluate the reproducibility of several intraoral scanners including E4D dentist (Planmeca PlanScan-E4D Technologies, Richardson, Tx), Fastscan (Polhemus, Cholchester, Vt), iTero (Align Technology, Inc, San Jose, Ca), Trios (3Shape, Copenehagen, Denmark), and Zfx Intrascan (Zfx, Dachau, Germany). The results suggested that, although all but two intraoral scanners showed high levels of trueness and precision, the level of trueness was dependent on the type of restoration and specific characteristics of each intraoral scanner.7 In a similar study, Mangano et al.8 evaluated the trueness and precision of four intraoral scanners by scanning two stone models with each scanner. Their results demonstrated that the Carestream CS3500 (Carestream Dental, Atlanta, Ga) possessed the best general trueness and precision, followed by the Trios, Zfx Infrascan, and Planscan (Planmeca PlanScan-E4D Technologies, Richardson, Tx).8 In addition, Anh et al.9 investigated the effects of tooth crowding and scanning direction on the precision of three-dimensional images captured by the iTero and Trios digital intraoral scanners. The study showed that the level of precision between the two scanner systems was statistically consistent among models with different amounts of tooth crowding, but was not consistent between scans when scan direction was varied.9 However, both scanners were deemed highly accurate from a clinical perspective.9
Although the previous studies appraised the trueness and precision of individual maxillary and/or mandibular digital models, they did not evaluate the interarch occlusal relationships. Studies seeking to evaluate the interarch occlusal relationship have only done so using in vitro designs. DeLong et al.10 compared occlusal contacts obtained from virtual maximum intercuspal position records taken from maxillary and mandibular casts and compared them to the following nondigital, “gold standard” techniques: shimstock paper and transillumination. The results demonstrated that nondigital techniques found similar contacts only 81% of the time. The study also found that the virtual interocclusal record and virtual cast methods provided accurate measures of occlusal contacts.10 The study conducted by Mangano et al.8 evaluating the reproducibility of intraoral scans in vitro showed that the stereolithographic and digital models captured by an intraoral scanner were valid and reproducible. An in vivo investigation by Gazit et al.11 analyzed two occlusal marking techniques; however, the techniques used were nondigital. Their results showed that neither technique, the color marking technique nor a novel photo-occlusion technique, was highly reproducible.
No in vivo studies in the literature sought to determine the precision of the occlusal record obtained digitally by an intraoral scanner. Therefore, the aim of this study was to evaluate the precision of the virtual occlusal record using the Carestream CS3600 intraoral scanner (Carestream Dental, Atlanta, Ga).
MATERIALS AND METHODS
Participant Recruitment
This prospective study was assessed and approved by the Indiana University Institutional Review Board (Indianapolis, In) (no. 1802328755). The sample population included 20 participants recruited from the Indiana University School of Dentistry (Indianapolis, In). Eligible individuals met the following inclusion criteria:
Permanent dentition
No functional shift
No full coverage metal restorations
All canines, first molars, and second molars present and in occlusion
A minimum of eight occlusal contacts between the canines and first molars, with at least two contacts on each molar
Contacts were verified, prior to scan acquisition, by drying the teeth with an air-water syringe and marking the teeth with thin blue articulating paper (Henry Schein, Melville, Ny).
Individuals were excluded from participation in the study if they presented with the following exclusion criteria:
Anterior or posterior crossbites
Partially erupted or impacted canines or molars (lack of occlusal contact)
Individuals currently undergoing orthodontic treatment or who finished orthodontic treatment within the previous 3 months
To ensure that each participant met the study inclusion/exclusion criteria, a dental exam was performed and a brief medical history was obtained through an interview. Study involvement was voluntary, and the recruited participants received gift cards as compensation for their participation.
Virtual Data Acquisition
All participants were scanned with the Carestream 3600 intraoral scanner. One scanner within the Indiana University Department of Orthodontics and Oral Facial Genetics (Indianapolis, In) was used for all data collection during the study. To ensure the complete capture of the dentition, an intraoral mirror was used to retract the soft tissue. A single examiner (K.B.) captured one scan and two bite registrations on each participant during a single session under the same clinical settings (same dental unit, with the same chair and head position). The buccal, occlusal, and lingual surfaces of all teeth were captured proceeding from the participant's right side to his or her left. During each participant encounter, the mandibular arch was captured first and then the maxillary arch. Prior to recording the virtual occlusal record, the participants were instructed to bite with normal pressure. Per manufacturer recommendations, three occlusal registrations were obtained. Two occlusal registrations were recorded in the posterior (first molar region) and the third was either in the anterior (incisor region) or posterior (right premolar region) depending on the participant's occlusion.
Each participant was assigned a unique identification number. After data acquisition, the scans were deidentified and coded to blind the data prior to conducting study measurements and statistical analysis. All data were stored in an Excel (Microsoft Corporation, Redmond, Wa) spreadsheet within a secured Indiana University Health Box account (Indiana University, Bloomington, In).
The system's associated software, using a proprietary algorithm, was used to determine the location, size, and intensity of occlusal contact points between the maxillary and mandibular arches. These three parameters were used to analyze the occlusal aspect of the virtual bite registration and determine the precision of the digital occlusal contacts recorded by the software (Figure 1). A single examiner (K.B.) collected all selected parameters during data acquisition and assessment. For this study, the heaviest occlusal contacts on the maxillary canines and first molars were selected for analysis (Figure 2). Occlusal contact locations on the maxillary arch were determined visually, and the location was categorized based on the occlusal area on which the contact was located (ie, the mesio-lingual or disto-lingual cusp of the first molar). The location(s) of the heaviest contacts were recorded using the code scheme depicted in Table 1. The mesial, middle, and distal aspects of the canine tooth surface were distinguished by dividing the tooth into equal thirds. If the occlusal contact(s) appeared on multiple areas of a tooth, all areas on the tooth were recorded.
Figure 1.
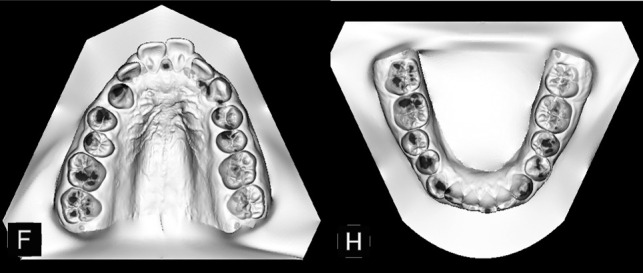
Generated virtual models displaying occlusal contact location, size, and intensity.
Figure 2.
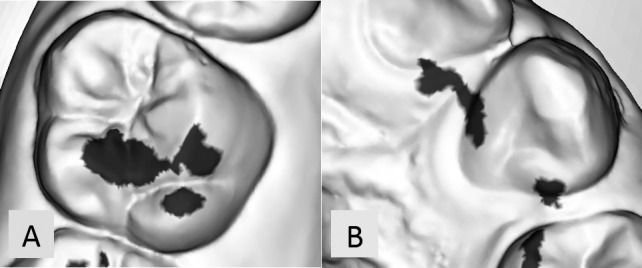
Heaviest occlusal contacts shown on maxillary right first molar (A) and left canine (B).
Table 1.
Occlusal Contact Location and Description
| Tooth |
Contact Location |
Contact Description |
| Molar | MB | Mesio-buccal cusp of tooth |
| ML | Mesio-lingual cusp of tooth | |
| DB | Disto-buccal cusp of tooth | |
| DL | Distal-lingual cusp of tooth | |
| Canine | M | Mesial portion of the tooth surface |
| D | Distal portion of the tooth surface | |
| Middle | Middle portion of the tooth surface |
Contact size was calculated by measuring the contact(s) circumference (Figure 3) using the software's measurement tool. When multiple occlusal contacts existed on the surface of interest, the sum of the total contact circumferences was calculated and utilized. The total circumference for each contact point was recorded using the same computer under similar environmental conditions.
Figure 3.
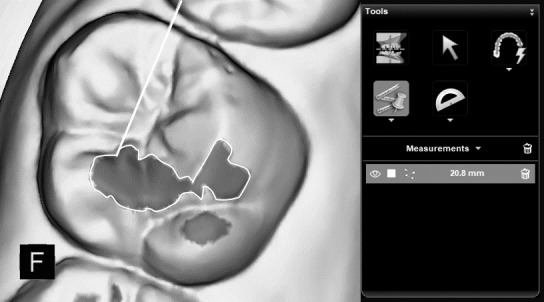
Circumference identification for one of two contacts on a maxillary right molar (contact shown in dark gray, contact circumference outlined by white line).
The occlusal contact intensities were determined using the “occlusion” menu color scale within the Carestream software. The default scale within the program ranged from violet (overlap) to cyan (very low occlusion). For this study, only the scale range from red (very high/contact) to cyan was used (Figure 4). To facilitate statistical analysis, codes were assigned to the colors on the Carestream contact scale (Table 2).
Figure 4.
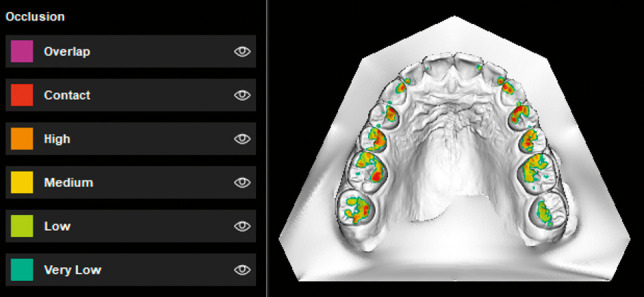
Occlusal contact color scheme provided by scanning software.
Table 2.
Occlusal Contact Intensity Color Scheme Coding
| Contact Intensity |
Assigned Code |
| Cyan (very low) | 1 |
| Green (low) | 2 |
| Yellow (medium) | 3 |
| Orange (high) | 4 |
| Red (very high/contact) | 5 |
Intra- and Interexaminer Reliability
Prior to initiating participant recruitment, intrarater reliability and interrater agreement of contact locations, circumference, and intensity were evaluated. The occlusal registration of five participants were retrieved from the Indiana University School of Dentistry Department of Orthodontics and Oral Facial Genetics intraoral scanner archives and assessed by two examiners (K.S. and K.B.). The same parameters were reevaluated 1 week later by both individuals. Reliability and agreement of the contact circumference and contact intensity were assessed using intraclass correlation coefficients. The reliability and agreement of the heaviest contact points and contact locations were assessed using κ statistics. All correlation values were greater than 0.9.
Statistical Analysis
Intraclass correlation coefficients (ICCs) were used to assess the agreement between contact size and intensity between scans. The ICCs were calculated using the variance components of mixed-model analysis of variance. Contingency tables and kappa statistics were used to assess the agreement between locations of occlusal contacts at different times. Cochran-Mantel-Haenszel chi-square tests were used to examine the differences between locations of occlusal contacts at different times. A power analysis demonstrated that with a sample size of 20 participants, the width of a 95% confidence interval for the ICCs will be at most 0.20, assuming the ICC was at least 0.90.
RESULTS
The data for all 20 recruited participants were used in the statistical analysis (Table 3). Between the two acquired virtual occlusal records, nonstatistically significant differences were observed in the proportion of locations with contacts (P = .7681; Table 4). A minor difference (−0.25 mm) in mean contact circumference size was observed; however, the difference was not statistically significant (P = .8416; Table 5). A statistically significant difference in mean contact intensity was observed (P = .0448; Table 5). When evaluating the agreement between the scans obtained, the two scans demonstrated a weak correlation for size (ICC = 0.35) and intensity (ICC = 0.32). In addition, the kappa coefficient for contact location agreement was found to be 0.67, indicating moderate agreement.
Table 3.
Descriptive Statisticsa
| Tooth |
Scan Timepoint |
N |
Variable |
N |
Mean |
SD |
Median |
Minimum |
Maximum |
| UL3 | 1 | 20 | Size | 20 | 6.460 | 3.876 | 6.150 | 1.000 | 15.000 |
| Intensity | 20 | 4.150 | 0.875 | 4.000 | 2.000 | 5.000 | |||
| 2 | 20 | Size | 20 | 6.665 | 3.692 | 5.700 | 1.300 | 14.800 | |
| Intensity | 20 | 4.450 | 0.510 | 4.000 | 4.000 | 5.000 | |||
| UL6 | 1 | 20 | Size | 20 | 12.070 | 9.698 | 9.900 | 1.300 | 33.000 |
| Intensity | 20 | 4.450 | 0.826 | 5.000 | 2.000 | 5.000 | |||
| 2 | 20 | Size | 20 | 10.980 | 13.891 | 6.600 | 2.100 | 64.300 | |
| Intensity | 20 | 4.800 | 0.523 | 5.000 | 3.000 | 5.000 | |||
| UR3 | 1 | 20 | Size | 20 | 6.685 | 3.843 | 5.750 | 1.600 | 15.600 |
| Intensity | 20 | 4.150 | 0.933 | 4.000 | 2.000 | 5.000 | |||
| 2 | 20 | Size | 20 | 5.555 | 3.099 | 5.550 | 1.400 | 13.600 | |
| Intensity | 20 | 4.300 | 0.865 | 5.000 | 3.000 | 5.000 | |||
| UR6 | 1 | 20 | Size | 20 | 17.560 | 10.369 | 16.050 | 2.100 | 38.600 |
| Intensity | 20 | 4.800 | 0.523 | 5.000 | 3.000 | 5.000 | |||
| 2 | 20 | Size | 20 | 18.570 | 12.795 | 17.150 | 1.700 | 42.700 | |
| Intensity | 20 | 4.800 | 0.616 | 5.000 | 3.000 | 5.000 |
SD indicates standard deviation; UL3, maxillary left first canine; UL6, maxillary left canine; UR3, maxillary right canine; UR6, maxillary right first molar.
Table 4.
Cochran-Mantel-Haenszel Chi-Square Test Depicting Differences Between Contact Locations at Different Scansa
| Contact in Scan 1 |
|||
| No |
Yes |
||
| Contact in Scan 2 | No | 124 (44.3%) | 24 (8.6%) |
| Yes | 22 (7.9%) | 110 (39.3%) | |
P = .7681.
Table 5.
Mixed-Model Analysis of Variance Comparison Between Scans for Contact Size and Intensity Outcomes
| Effect |
Scan |
Scan |
Difference |
Standard Error |
P Value |
|
| Contact size | Scan | 2 | 1 | −0.2513 | 1.2532 | .8416 |
| Intensity | Scan | 2 | 1 | 0.2000 | 0.0981 | .0448* |
P > .05.
DISCUSSION
The occlusal registration is an important diagnostic source of information for dentists and orthodontists. The aim of this study was to evaluate the precision of the virtual occlusal record using the Carestream CS3600 intraoral scanner. The precision of the virtual occlusal record was evaluated through visual and quantitative comparisons between the two occlusal registrations. Although the results showed nonstatistically significant differences between size and locations of contacts between occlusal registrations, the ICC correlations for contact size and intensity were lower than expected. It is conceivable that the low agreement between contact size and intensity was the result of the method selected to assess these contact parameters. The mean circumference value was relatively small, and the standard deviation for some values varied widely. This trend appeared to negatively impact the correlation values attained. One explanation for the contact intensity variation could be a difference in patient bite force between the acquired bite registrations. In addition, the study demonstrated a significant difference in mean contact intensity (0.2000, P = .0448) between occlusal registrations. This would suggest that there was variability either between the participants' bites or between the occlusal registration scans. Anh et al.9 evaluated the precision of digital records between scans and showed that differences in precision depended on the scanning sequence for both scanners evaluated. In the current study, one scan and two bite registrations were used. The software allowed the user to reopen the data file of a scan and obtain multiple bite registrations. The authors used one scan to eliminate the possibility of potential variabilities in the bite registrations secondary to differences in the acquired maxillary and mandibular arch scans themselves.
Another possible explanation could be the differences in the acquisition of the bite registration, such as the tilting of the intraoral scanner. Edher et al.12 evaluated the interocclusal records of subjects obtained from mounted zirconia master models. Both quadrants and complete arches were scanned, and it was concluded that different occlusal contacts were obtained from interocclusal registration scans in different segments of the dental arch. A more pronounced difference was seen in complete arch scans, where a tilting effect toward the site of the interocclusal registration was observed. Standardization of the scanner wand during image acquisition was not included in the current study because this is not regulated during typical clinical use. However, variations in scanner tilt may have occurred and could explain the lower contact size and intensity agreement observed. In addition, it is possible that the tilt of the scanner was different when capturing different bite registration areas in the mouth, making this explanation plausible but impractical for a clinical setting. Wong et al.13 evaluated the accuracy of digital static interocclusal registration. They observed interocclusal distortions in two of the three scanners tested. In that study, the authors credited these differences to potential flaws in the scanner software algorithm, which serves to match the maxillary and mandibular arches together. In addition, they noted that the interocclusal distortion could also be a result of software inaccuracies in the whole process of image capturing, stitching, and postprocessing capabilities.13 This software-based phenomenon could also help explain the reduced agreement seen.
Along with the provided explanations, the variations observed in the bite registrations could be attributed to variations in a participant's bite. No studies were found that used an in vivo design to evaluate successive virtual occlusal records in one session as with the current study. However, Jaschouz and Mehl14 used an in vivo design to investigate the reproducibility of habitual intercuspation in different instances. The participants of that study were seen in the morning and afternoon for occlusal registration acquisition. During both sessions, the participants were asked to lay horizontally and sit upright during intraoral scan acquisition. Four digital occlusal registrations were captured per participant, and these registrations were compared among each other. The study found no significant differences in habitual intercuspation based on session time or participant positioning. These findings were in agreement with the results of the current study, which showed no statistically significant differences in contact size or location. However, the study by Jaschouz and Mehl14 did not include an assessment of contact intensity and thus provided no evidence to help explain the significant difference noted for this parameter. Although the participants in the current study were instructed to bite in their normal maximal intercuspal position for both records, the bite force that they exerted could not be confirmed quantitatively. Bite force variation could be a confounding factor for occlusal contact intensity readings despite the guidance given to participants during the study. The decision to conduct an in vivo study with participants made the study findings more clinically relevant but more difficult to ensure complete standardization of participant bite force.
Although there were no statistically significant differences in the location or size of occlusal contacts, statistically significant differences in contact intensity of the occlusal bite registration were observed. Thus, the proposed hypothesis was confirmed; however, the difference observed is likely not clinically significant. When considering all of the obtained data, it may be suggested that the Carestream 3600 scanner software contains sufficient clinical precision to identify malocclusions and dentition relationships. The virtual records produced from the dental and occlusal scans provide clinicians with an adequate notion of where occlusal contacts exist within an individual's bite. However, the intensity of the occlusal contacts appeared less precise, and this aspect of the virtual occlusal record should be used with caution.
The present study had several potential limitations. The study design included the use of only a single scanner, making it more challenging to compare the results from this study with other studies using different scanners. In addition, the occlusal color scale used by the Carestream software was not linked with numerical values, making it difficult to provide quantitative data for some of the parameters of interest. Finally, the current study did not attempt to link the participants' digital occlusal registration with their actual occlusion (accuracy assessment). No current technique/technology exists to overlay the digital and actual bite registrations accurately. In lieu of these observed limitations, this study provided important foundational information that will help ascertain the level of precision present in intraoral scanners, such as the Carestream 3600, in an in vivo setting.
CONCLUSIONS
The scanner software possesses clinically adequate precision when acquiring contact size and location in virtual bite registrations.
The scanner software failed to demonstrate adequate precision when acquiring the different grades of occlusion in bite registrations.
Additional research is warranted to investigate further the precision of virtual occlusal records with currently available software systems.
ACKNOWLEDGMENTS
The authors would like to thank George Eckert, the Indiana University School of Dentistry Orthodontic Department staff, and the Indiana University School of Dentistry Kishibay-Eteson Research in Orthodontics fund for their support with this study.
REFERENCES
- 1.Birnbaum NS, Aaronson HB. Dental impressions using 3D digital scanners: virtual becomes reality. Compend Contin Educ Dent. 2008;29:494–496. 498–505. [PubMed] [Google Scholar]
- 2.Yuzbasioglu E, Kurt H, Turunc R, Bilir H. Comparison of digital and conventional impression techniques: evaluation of patients' perception, treatment comfort, effectiveness and clinical outcomes. BMC Oral Health. 2014;14:10. doi: 10.1186/1472-6831-14-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.International Organization for Standardization. Accuracy (trueness and precision) of measurement methods and results—Part 1: General principles and definitions. https://www.iso.org/standard/11833.html Accessed September 15, 2018.
- 4.Nilsson J, Richards RG, Thor A, Kamer L. Virtual bite registration using intraoral digital scanning, CT and CBCT: in vitro evaluation of a new method and its implication for orthognathic surgery. J Craniomaxillofac Surg. 2016;44:1194–1200. doi: 10.1016/j.jcms.2016.06.013. [DOI] [PubMed] [Google Scholar]
- 5.Kerstein RA, Grundset K. Obtaining measurable bilateral simultaneous occlusal contacts with computer-analyzed and guided occlusal adjustments. Quintessence Int. 2001;32:7–18. [Google Scholar]
- 6.Imburgia M, Logozzo S, Hauschild U, Veronesi G, Mangano C, Mangano FG. Accuracy of four intraoral scanners in oral implantology: a comparative in vitro study. BMC Oral Health. 2017;17:92. doi: 10.1186/s12903-017-0383-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Park JM. Comparative analysis on reproducibility among 5 intraoral scanners: sectional analysis according to restoration type and preparation outline form. J Adv Prosthodont. 2016;8:354–362. doi: 10.4047/jap.2016.8.5.354. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Mangano FG, Veronesi G, Hauschild U, Mijiritsky E, Mangano C. Trueness and precision of four intraoral scanners in oral implantology: a comparative in vitro study. PLoS One. 2016;11(9):e0163107. doi: 10.1371/journal.pone.0163107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Anh JW, Park JM, Chun YS, Kim M, Kim M. A comparison of the precision of three-dimensional images acquired by 2 digital intraoral scanners: effects of tooth irregularity and scanning direction. Korean J Orthod. 2016;46:3–12. doi: 10.4041/kjod.2016.46.1.3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.DeLong R, Knorr S, Anderson GC, Hodges J, Pintado MR. Accuracy of contacts calculated from 3D images of occlusal surfaces. J Dent. 2007;35:528–534. doi: 10.1016/j.jdent.2007.02.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Gazit E, Fitzig S, Lieberman MA. Reproducibility of occlusal marking techniques. J Prosthet Dent. 1986;55:505–509. doi: 10.1016/0022-3913(86)90188-5. [DOI] [PubMed] [Google Scholar]
- 12.Edher F, Hannam AG, Tobias DL, Wyatt CCL. The accuracy of virtual interocclusal registration during intraoral scanning. J Prosthet Dent. 2018;120:904–912. doi: 10.1016/j.prosdent.2018.01.024. [DOI] [PubMed] [Google Scholar]
- 13.Wong KY, Esguerra RJ, Chia VAP, Tan YH, Tan KBC. Three-dimensional accuracy of digital static interocclusal registration by three intraoral scanner systems. J Prosthodont. 2018;27:120–128. doi: 10.1111/jopr.12714. [DOI] [PubMed] [Google Scholar]
- 14.Jaschouz S, Mehl A. Reproducibility of habitual intercuspation in vivo. J Dent. 2014;42:210–218. doi: 10.1016/j.jdent.2013.09.010. [DOI] [PubMed] [Google Scholar]