

Abstract
BACKGROUND
Women are less likely than men to be physically active and more likely to reduce their physical activity as they age. The objective of this research was to understand barriers that might prevent North Carolina women from being physically active after retirement as well as aspects of retirement that might facilitate a more physically active lifestyle to inform intervention strategies applicable to retired women.
METHOD
Semi-structured interviews were conducted with 15 recently retired women living in North Carolina. Interviews were recorded and transcribed. Content analysis was used to identify themes related to barriers and facilitators of physical activity after retirement.
RESULTS
Six themes were identified. One theme was the development of leisure-time physical activity habits over the lifespan. Five other themes described how physical activity after retirement was influenced by prior occupational physical activity, concurrent life transitions (e.g., becoming a caregiver), health, social support, and the community environment.
LIMITATIONS
Women in this study were active participants in community organizations, which might make their experiences unique from those of women who are not engaged with their communities. However, similarities in themes in this and other qualitative studies corroborate the broader transferability of findings.
CONCLUSION
Interventions to promote physical activity among retired North Carolina women should consider emphasizing health benefits of physical activity and improving walking environments and access to physical activity facilities. Local residents should be involved in intervention design to address unique barriers among women who retire from physically demanding jobs or become caregivers.
Regular physical activity reduces the risk of chronic disease, such as cardiovascular disease, diabetes, and cancer, in later life [1, 2]. However, only half of older North Carolinians (aged 65 or older) meet recommendations for engaging in ≥ 150 min/week of moderate or ≥ 5 min/week of vigorous aerobic activity, or a combination of both [2, 3]. As the population of older North Carolinians grows from 1.6 million to 2.6 million by 2035 [4], community-level efforts to support physical activity in later life will be increasingly important.
Retirement might provide an opportunity to promote physical activity among older adults. Retirement might positively impact physical activity through increased free time and prioritization of health [5, 6]. On the other hand, retirement might negatively impact physical activity, for example by reducing access to physical activity resources (e.g., loss of access to employment-based gym facilities) or weakening social networks [7-10].
The Life Course Theory and the Social Ecological Model provide theoretical frameworks for understanding the effect of retirement on physical activity. According to the Life Course Theory, shifts in personal and social identity during retirement might create an opportunity for behavior change, including physical activity [11]. According to the Social Ecological Model (SEM), behavior is influenced by factors at the individual (e.g., self-efficacy), interpersonal (e.g., family), and environmental or community levels (e.g., access to places to be physically active) [12]. Factors that make it easier to be physically active are facilitators, whereas factors that make it more difficult to be physically active are barriers. Retirement might change exposures to factors at multiple levels of SEM. SEM has been used to inform physical activity interventions, which are more likely to be effective when targeting factors from multiple levels [12].
Barriers and facilitators of physical activity among older adults have been studied previously [13-16]. However, few researchers distinguished working persons from retired persons or studied factors that influenced women’s physical activity during the years immediately after retirement [8].
The objective of this qualitative study was to identify barriers and facilitators of physical activity among North Carolina women who were recently retired (< 5 years). We defined physical activity broadly, including activities like walking, gardening, exercise, or playing with grandchildren. We explored barriers and facilitators at the individual, interpersonal, and environmental levels to inform potential intervention strategies applicable to recently retired women.
This study was motivated in part by findings from the Multi-Ethnic Study of Atherosclerosis (MESA), a longitudinal study of 6,814 adults from six US communities [17]. Among MESA participants, retirement was associated with decreased moderate-to-vigorous physical activity, particularly among persons of lower socioeconomic position [18]. This qualitative study was located in one of the MESA communities: Forsyth County, North Carolina, a mid-sized metropolitan region.
We focused on women because women are more likely than men to be insufficiently active and to reduce their physical activity as they age [19]. Evidence further suggests that women are less likely to increase their leisure-time physical activity after retirement than men [20]. Women also are more likely than men to serve in caregiving roles [21], which can limit time for other types of physical activity [22].
Methods
We conducted semi-structured interviews with a purposive sample of 15 retired women living in Forsyth County, North Carolina. This study was reviewed by the Institutional Review Board at the University of North Carolina at Chapel Hill (#16-0002) and all participants provided verbal consent.
Study Location
Forsyth County is the fourth most populous North Carolina county (total population 366,543). One in five residents is aged ≥ 60 [23]. Among older Forsyth County residents, 19% are African American, 79% are non-Hispanic white, and 32% have at least one disease or disability [23]. Eighty-five percent of residents live in census tracts located within a half mile of a park or within one mile (urban areas) or three miles (rural areas) of a recreational facility [24]. However, walkability and public transportation are limited; Winston-Salem, the largest city in the county, has an average Walk Score® of 23, indicating almost complete car dependence.
Participant Recruitment
The first author (Jones) recruited participants in person at four community events (e.g., library book sale, community group meetings); study flyers were posted concurrently in community centers, senior centers, libraries, a senior center e-newsletter, and on a church social media site. Jones selected venues to include events and locations serving diverse women from throughout the Forsyth County community. Interested participants were provided a study information sheet and eligibility criteria. To be eligible, participants had to be female, resident of Forsyth County, aged 55–75, and retired within the past five years. Eligibility was assessed in person or by phone. Recruitment stopped when data saturation was achieved [25].
Study Questionnaire
Prior to interview, women completed a questionnaire about their sociodemographic information, occupation before retirement, and reasons for retirement, and completed the MESA physical activity and neighborhood questionnaires (Appendix 1, available online) [26, 27]. Women who reported physical activity at work prior to retirement were classified as having retired from active occupations.
Walk Score®
We recorded the Walk Score® (www.walkscore.com) for each participant’s home address. Walk Score® ranges from 0 to 100, with scores below 50 reflecting communities where motorized transport is needed for most or all errands.
Interview Guide
We conducted interviews using a semi-structured interview guide (Appendix 2, available online). The interview guide was developed based on the research objective, the Life Course Theory and SEM, and existing literature [28, 29]. Participants were asked to describe their physical activity and sedentary behavior before and after retirement, barriers and facilitators of physical activity after retirement, and ideas for supporting physical activity among retired women. We defined physical activity for participants as “anything that gets you moving, like walking in your neighborhood or to go somewhere, gardening, doing sports or exercise, or playing with grandchildren.” We defined sedentary behavior as “watching TV, using the computer/phone, reading, or other things you might do sitting down.” Probes were used as indicated in the interview guide (Appendix 2).
Interviews
Jones, a female doctoral student, conducted all interviews. Interviews lasted on average 40 minutes (range 25-75 minutes). Participants received $20 in recognition of their time. Interviews were digitally recorded and transcribed verbatim. Questionnaire responses and transcripts were uploaded to ATLAS.ti version 7 software (Berlin, Germany) for analysis.
Analysis
Descriptive statistics were calculated for sociodemographic and neighborhood characteristics of each study participant using SAS version 9.3 (Cary, North Carolina). Interview transcripts were reviewed using content analysis [30] to identify facilitators and barriers to physical activity after retirement. The first author and a second trained coder used ATLAS.ti to code each transcript independently, then met to resolve discrepancies by consensus discussion. A priori codes based on SEM included codes for barriers and facilitators at the individual, interpersonal, and community levels; the authors inductively derived additional codes based on interview transcripts. Code definitions, clarifications, and example quotations were documented in a detailed codebook. Themes were developed through review and discussion of coded quotations. The team compared similarities and differences in coded quotations between women who retired from physically active and sedentary occupations.
Results
Eighteen women expressed interest in the study, of whom 17 met the eligibility criteria (one did not meet age criteria) and were invited to schedule interviews during April–June 2017. Thirteen women participated in interviews by phone, two in person, and two did not respond to the invitation.
Among 15 participants, seven were African American and eight were non-Hispanic white (Table 1). Participants were on average 68 years old. Sixty percent of participants had completed less than a bachelor’s degree, one-third were married, 40% were widowed, and one-third were caregivers for family members. On average, women had been retired for three years and 53% retired from sedentary occupations. Most women identified multiple reasons for retirement, with family most often identified as a very or moderately important reason. Most women did not live in walkable neighborhoods (average Walk Score® 23). After retirement, 10 participants were active (i.e., participated in some regular physical activity) and five were inactive. Active participants’ physical activities included walking for recreation (n = 7) and for transportation (n = 2), exercise classes (n = 5), gardening (n = 3), and household chores (N = 15) (Table 2).
TABLE 1.
Participant Characteristics, Overall and by Prior Occupational Physical Activity (N = 15)
| Total (N = 15) |
Active Job (n = 7) |
Sedentary Job (n = 8) |
|
|---|---|---|---|
| Characteristic | N (%) or Mean (SD) | N (%) or Mean (SD) | N (%) or Mean (SD) |
| Age, years | 68 (3) | 67 (4) | 70 (2) |
| Race | |||
| African American | 7 (47%) | 4 (57%) | 3 (38%) |
| White | 8 (53%) | 3 (43%) | 5 (63%) |
| Education | |||
| < Bachelor’s degree | 9 (60%) | 4 (57%) | 5 (63%) |
| ≥ Bachelor’s degree | 6 (40%) | 3 (43%) | 3 (38%) |
| Partnership status | |||
| Married | 5 (33%) | 2 (29%) | 3 (38%) |
| Widowed | 6 (40%) | 2 (29%) | 4 (50%) |
| Divorced/single | 4 (27%) | 3 (43%) | 1 (12%) |
| Retirement duration, years | 3 (1) | 3 (1) | 3 (1) |
| Reason for retirementa | |||
| Spend more time with family | 8 (53%) | 3 (43%) | 5 (63%) |
| Wanted to do other things | 5 (33%) | 1 (14%) | 4 (50%) |
| Health | 2 (13%) | 1 (14%) | 1 (12%) |
| Did not enjoy work | 1 (7%) | 0 (0%) | 1 (12%) |
| Caregiverb | 5 (33%) | 2 (29%) | 3 (38%) |
| Neighborhood Walk Score® | 23 (20) | 29 (24) | 17 (15) |
| Physical activities | |||
| Walking | 9 (60%) | 5 (71%) | 4 (50%) |
| Regular non-walking exercisec | 5 (33%) | 0 (0%) | 5 (63%) |
| Television watching, hr/week | 30 (28) | 45 (34) | 17 (13) |
| Prior occupational activityd | |||
| Moderate activity | 3 (20%) | 3 (43%) | - |
| Light activity | 4 (27%) | 4 (57%) | - |
| Sedentary | 8 (53%) | - | 8 (100%) |
Reasons for retirement rated as very or moderately important on a 4-point Likert scale (not at all important, somewhat important, moderately important, very important); women could select multiple reasons
Caregiver defined as reporting providing care for a family member, such as spouse, parent, or grandchild ≥ 150 minutes/week
Regular non-walking exercise defined as reporting participation in non-walking exercise (e.g., aerobics class) at least once per week
Prior occupational physical activity categorized by self-report of usual activity at work prior to retirement: sedentary (light effort while sitting), light activity (light effort while standing/walking), moderate activity (moderate effort while standing/walking, lifting, or pushing)
TABLE 2.
Physical Activity Before (Work and Non-work) and After Retirement Among Participants (N = 15)
| Study ID |
Age | Walk Score®a |
Pre-retirement physical activityb | Post-retirementb physical activity |
Self-perceived Impact of retirementc | |
|---|---|---|---|---|---|---|
| Work | Non-work | |||||
| 1 | 62 | 7 | Standing, walking (light activity) | Walking (occasional), stationary bike | Walking, stationary bike (occasional) | ↓ physical activity, ↑ sedentary behavior due to loss of work activity and not leaving home |
| 2 | 63 | 44 | Standing, walking, lifting (moderate activity) | None | None | ↓ physical activity, ↑ sedentary behavior due to loss of work activity, and increased time/energy for TV/computer |
| 3 | 72 | 42 | Standing, walking (light activity) | Water aerobics | Walking, dancing (occasional) | ↓ physical activity, ↑ sedentary behavior due to loss of work activity and not leaving home |
| 4 | 62 | 57 | Standing, walking, lifting, carrying (moderate activity) | None | Walking for transportation | ↓ physical activity, ↑ sedentary behavior due to loss of work activity and ill-health |
| 5 | 68 | 46 | Walking (light activity) | Walking (dogs) | Walking (dogs), gardening, light swimming (summer) | ↓ physical activity, ↑ sedentary behavior because caring for parents (mostly sedentary) replaced work activity |
| 6 | 69 | 1 | Standing, walking, lifting, carrying (moderate activity) | None | None | ↓ physical activity, ↑ sedentary behavior due to loss of work activity, and increased time/energy for TV/computer |
| 7 | 70 | 6 | Standing, walking (light activity) | Walking | Walking, gardening, gym (occasional) | ↑ physical activity, ↓ sedentary behavior due to increased time/less stress and no longer required to sit at work |
| 8 | 71 | 3 | Sedentary | None | None | No change |
| 9 | 70 | 13 | Sedentary | None | None | ↑ physical activity, ↓ sedentary behavior because always “on the go,” more energy |
| 10 | 72 | 4 | Sedentary | Line dancing, walking (dog) | Walking, water aerobics, Zumba | ↑ physical activity, ↓ sedentary behavior replaced sedentary work with physical activities due to increased time/energy |
| 11 | 71 | 47 | Sedentary | Exercise classes (occasional) | Yoga, cardio class, T’ai Chi, gardening, walking for transportation, biking (occasional) | ↑ physical activity,↓ sedentary behavior due to increased free time and no longer required to sit at work |
| 12 | 68 | 30 | Sedentary | None | None | ↑ physical activity, ↓ sedentary behavior because “on the go” for organizations and no longer required to sit at work |
| 13 | 71 | 10 | Sedentary | Walking (dogs), treadmill | Walking (dogs), exercise class, water aerobics | No change: ↓ physical activity when retired concurrent with remarriage, then ↑ physical activity when widowed 15 months later; ↓ sedentary behavior after retirement because no longer required to sit at work |
| 14 | 69 | 9 | Sedentary | Aerobics (occasional) | Water aerobics (regularly) | Physical activity ↑ briefly after retirement then ↓ when began caring for parents; ↓ sedentary behavior because no longer required to sit at work |
| 15 | 67 | 21 | Sedentary | Aerobics | Walking, yoga, aerobics | ↓ physical activity, ↓ sedentary behavior because caring for parents limited ability to attend exercise classes, but no longer required to sit at work |
Walk Score® from www.WalkScore.com based on participant home address. Neighborhoods with a Walk Score® 0-49 are car dependent (most errands require a car), 50-69 are somewhat walkable (some errands can be accomplished on foot), 70-89 are very walkable (most errands can be accomplished on foot), and 90-100 are ‘walker’s paradise’ (daily errands do not require a car).
Pre- and post-retirement physical activities reported by participants during the qualitative interview and on the self-reported physical activity questionnaire
Participants’ self-perception during the interview of the extent to which their physical activity and sedentary behavior changed after retirement and what accounted for the change.
Barriers and Facilitators of Physical Activity After Retirement
Facilitators and barriers of physical activity after retirement were grouped into six themes. One theme related to development of leisure-time physical activity habits over the lifespan. The other five themes described how physical activity after retirement was influenced by prior occupational physical activity; life transitions concurrent with retirement, health, social interaction and support; and the community environment. Themes are described next with illustrative quotations included in Table 3. Barriers and facilitators are summarized across themes by levels of the Social Ecological Model in Figure 1.
TABLE 3.
Themes and Subthemes Related to Barriers and Facilitators of Physical Activity After Retirement
| Theme | Subtheme | Illustrative Quotations |
|---|---|---|
| 1. Women’s leisure-time physical activity habits develop over the lifespan | “Well, for the ones [of my retired friends] that are [physically] active [since retiring], they’ve always been active. They’re like me.” (Participant 10) | |
| 2. Women’s perceptions of physical activity differed depending on whether they retired from active versus sedentary jobs | 2.1 Women who retired from active jobs viewed retirement as a time to slow down | “I just wanted to take a nice rest and not do anything because I’ve worked since I was 15 years old. I am going on 70 now. So, I just wanted to take a rest and do nothing for a while.” (Participant 6) “Well, I’m not working. I’m at home so it’s a much more sedate lifestyle. I do a lot more sitting. I just—I mean I don’t have to get up and go all the time like I did.” (Participant 1) |
| 2.2 Women who retired from sedentary jobs viewed retirement as a time to get moving | “I didn’t really do much [when I was working] except go from meeting to meeting and program to program. And, now that I’m retired, I can just sort of focus on like getting in shape… So, there’s a lot more physical activity in retirement than there was when I had a desk job.” (Participant 11) | |
| 3. Women’s opportunities for physical activity after retirement were shaped by concurrent life transitions | “Well, when I first retired, I was very active because I had all my mornings free… And then, my parents became ill… so I had to put the Y and everything on the back burner for a while… I’ll tell you, [caregiving] took up pretty much my whole life for a while.” (Participant 14) “But I really don’t know that many people here. I mean, when I lived in [previous state], I always… [had a] big group of friends so when I did have leisure time there was always somebody to do something with. It’s less so here. I know quite a few less people.” (Participant 5) |
|
| 4. Declining health was a barrier and motivator of physical activity after retirement | 4.1 Physical limitations made it more difficult for women to be physically active | “[Arthritis] is why I don’t do aerobics as much because it seems to feel like it’s, I wouldn’t say injuring me, but it seems to be more difficult. So, I prefer the water aerobics because I don’t feel pain.” (Participant 15) |
| 4.2 Beliefs about physical and mental health benefits of physical activity motivated some women to be active, but inactive women were not motivated to be active despite awareness of potential health benefits | “I tell myself as I’m walking, ‘Well, you’re doing this for this problem. And you’re doing this for the other problem.’ Mentally, it makes me feel as if I have more control over the health conditions I have.” (Participant 7) “It’s everywhere, you read it, it’s on television, your doctor tells you, ‘you need to do this, it’s important, you’ll live longer.’ So, I think the problem [reason I do not do physical activity] is just me: the motivation.” (Participant 8) |
|
| 5. Women’s physical activity was influenced by availability of social support and interaction | 5.1 Family, friends, and church networks provided information and encouragement to be physically active | “We’re both of us [my husband and I] together really trying to keep in shape, stay in shape… So anyway, we sort of both motivate each other.” (Participant 11) “[Physical activity is] also a good way to socialize. You know, you just get out of the house and you’re being with other people. I think that’s really important too.” (Participant 1) |
| 5.2 Opportunities to socialize and make new friends also motivated some women to participate in group exercise but only when they believed they could find companions | “I don’t do much because I don’t have anybody to do it with. You know, maybe if I had a partner or a friend that wanted to get involved in activities and such, then I probably would do more. But by me being by myself, I don’t do anything.” (Participant 2) | |
| 6. Neighborhood environments and community resources supported and constrained physical activity after retirement | 6.1 The neighborhood environment was an important determinant of walking | “[The neighborhood] is pretty, they keep it up and it just makes a nice place to get out and exercise or walk… Well, it’s really pleasant because the atmosphere is nice and the people in the neighborhood are nice.” (Participant 3) “In this neighborhood, there are huge hills… There’s no route around this house that I could take that didn’t require a lot of hills. So, if I was going to walk, I would probably have to go somewhere else.” (Participant 8) |
| 6.2 Community recreational facilities, like senior centers or the Y, provided opportunities for non-walking physical activities | “Anything that we want to do is out there waiting, and most of it is free or minimal cost.” (Participant 8) “Being African American sometimes we feel that ‘Oh, no, that’s for white people.’ I have friends who tell me that all the time when I try to get them to be involved in something. They will tell me, ‘Oh, that’s for white people.’… They feel like it’s not for the African American people, it’s for white people… I’ll hear, ‘They don’t want us around them.’ I say, ‘How do you know until you go and see?’” (Participant 14) |
FIGURE 1.
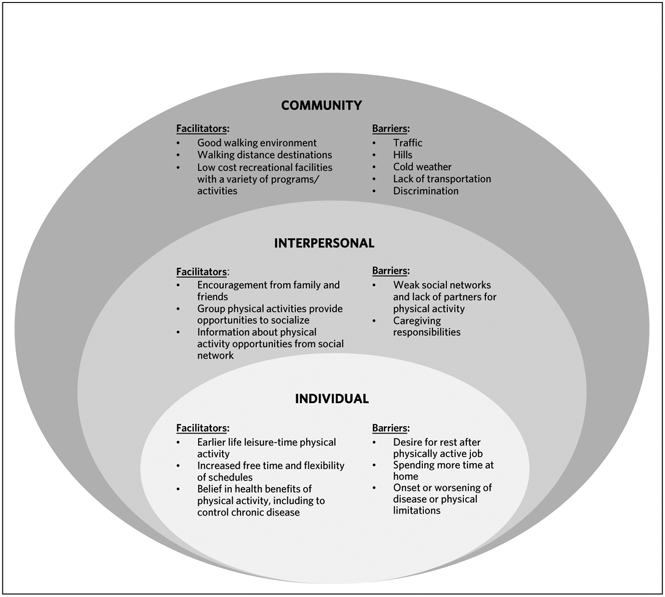
Facilitators and Barriers to Physical Activity After Retirement By Level of the Social Ecological Model
Theme 1: Women’s Leisure-Time Physical Activity Habits Develop Over the Lifespan
All participants who engaged in leisure-time physical activity prior to retirement continued to engage in regular physical activity after retirement (Table 2). These women initiated leisure-time physical activities as children or in early adulthood and continued them into retirement. In contrast, women who were inactive outside of work prior to retiring (including those with active jobs) were inactive during their leisure-time after retirement.
Theme 2: Women’s Perceptions of Physical Activity Differed Depending on Whether They Retired from Active Versus Sedentary Jobs
Women in this study who retired from active jobs viewed retirement as a time to slow down, which meant leaving home less frequently and engaging in less physical activity and more sedentary behavior (subtheme 2.1) (Table 2). Loss of daily routines also was a barrier to physical activity for these participants. In contrast, women who retired from sedentary jobs viewed retirement as a time to get moving and described increased free time, energy, and flexible schedules as facilitators that made physical activity more enjoyable, less rushed, and possible at preferred times of day (e.g., avoid walking after dark) (subtheme 2.2). However, some women who became very active in community organizations and/or underwent other life transitions (discussed further in Theme 3) did not feel that they had more time for physical activity after retirement.
Theme 3: Women’s Opportunities for Physical Activity After Retirement Were Shaped by Concurrent Life Transitions
Women’s control of their post-retirement routines, including physical activity, was constrained by concurrent transitions, such as onset of illness, becoming a caregiver, or moving. Caregiving responsibilities, in particular, disrupted physical activity routines, kept women at home, and led to fatigue and stress that prevented women from being physically active. Women who moved to a new city after retirement found it more difficult to find opportunities and companions for physical activity.
Theme 4: Declining Health was a Barrier and Motivator of Physical Activity After Retirement
Physical limitations made it more difficult for women to be physically active (subtheme 4.1). However, beliefs about physical and mental health benefits of physical activity motivated some women to be active, while inactive women were not motivated to be active despite awareness of potential health benefits (subtheme 4.2). Women with chronic conditions believed that regular physical activity helped manage their conditions or reduced the need for medications or surgery. These beliefs motivated women to remain active despite new physical limitations by adapting the type or intensity of physical activity (e.g., substituting water aerobics for regular aerobics). Active women also believed that regular physical activity would help them to “stay healthy” (participant 2) and “live longer, younger” (participant 8). Staying healthy meant maintaining the ability to do activities they enjoyed (e.g., travel) and “keep up” with family, particularly grandchildren. In addition, women associated physical activity with improved mental health, including feeling better about oneself and releasing stress.
However, awareness of health benefits associated with physical activity did not motivate all women to be active. Inactive women understood that physical activity was good for their health, but perceived retirement as a time when one should be able to do what one wanted and therefore did not participate in physical activity.
Theme 5: Women’s Physical Activity was Influenced by Availability of Social Support and Interaction
Family, friends, and church networks provided information and encouragement to be physically active (subtheme 5.1). Opportunities to socialize and make new friends also motivated some women to participate in group exercise, but only when they believed they could find companions with shared interests (subtheme 5.2).
Theme 6: Neighborhood Environments and Community Resources Supported and Constrained Physical Activity After Retirement.
The neighborhood environment was an important determinant of walking (subtheme 6.1). Pleasant, green, and safe environments facilitated recreational walking whereas access to destinations facilitated transport walking. Hilly terrain, cold or rainy weather, traffic, and fear of crime and falling were barriers to walking. Community recreational facilities, like senior centers or the YMCA, provided opportunities for non-walking physical activities (subtheme 6.2). Women valued facilities that were low-cost, conveniently located, included people of all ages, and where they could adapt the intensity of activities to fit their physical abilities. Five women reported that it was easier to use recreational facilities after they retired because of SilverSneakers®, a program wherein their health insurance company provided free access to any YMCA location. On the other hand, barriers to using recreational facilities included lack of public transportation and discrimination. For some African American women, racism and the legacy of segregation made them feel unwelcome or unsafe, which deterred them from using community recreational facilities.
Discussion
We identified six themes pertaining to facilitators and barriers to women’s physical activity after retirement. These findings may inform the targeting of physical activity interventions to retired women. Women who have no history of leisure-time physical activity, retire from physically active jobs, become caregivers, or move after retirement might be particularly in need of support for physical activity. Intervention strategies include emphasizing the health benefits of physical activity and improving walking environments and access to recreational facilities.
Interventions should emphasize the physical and mental health benefits of physical activity and help women develop strategies to continue physical activity despite physical limitations. Belief in the health benefits of physical activity is a commonly identified facilitator of post-retirement physical activity [6, 9, 22, 31, 32]. However, awareness of health benefits was not sufficient motivation for women to engage in physical activity in this or other studies [9, 31]. Thus, consistent with the Social Ecological Model [12], interventions should also address other factors, including environmental supports for physical activity [31, 33].
Environmental supports for physical activity identified by women in this study included neighborhood attributes and recreational facilities. Improvements to pedestrian infrastructure recommended by the Community Preventive Services Task Force [34], such as adding sidewalks in higher-traffic areas, could facilitate walking among retired US women. However, other barriers to walking (e.g., hills) are difficult to address [31, 35], underscoring the importance of access to recreational facilities (e.g., gym, senior center). In addition, addressing discrimination to create inclusive public spaces is essential to ensuring equitable access to local physical activity resources [13].
This study found that women who were the most active after retirement had participated in leisure-time physical activity in childhood or earlier adulthood, similar to previous studies [9, 22, 28]. This finding is consistent with the Life Course Theory principle of lifespan development, which links later life behavior (e.g., leisure-time physical activity) to the formative years of life course development [11]. Intervention strategies can address barriers associated with earlier life physical activity habits by providing opportunities for utilitarian physical activity (e.g., community service rather than exercise) for women who do not enjoy or value leisure-time physical activities [36] and by fostering a structured physical activity routine outside of the home [9, 31].
This study is one of the first to find that women who retired from physically active occupations reported being less physically active after retirement whereas women who retired from sedentary occupations frequently reported being more active after retirement. Although other studies identified loss of work routines as a barrier [29, 31, 32] and increased free time as a facilitator [10, 29, 37], none linked these factors to prior occupational physical activity.
Concurrent transitions during retirement also are important considerations for targeting interventions [33]. Experiencing multiple transitions was associated with decreased physical activity among adults in a systematic review [38]. For participants in this study, becoming a caregiver and moving posed unique barriers to physical activity after retirement. Women who were caregivers faced disruption of leisure-time physical activity routines, inability to leave home, fatigue, and stress, similar to a sample of retired British women [22]. Caregiving was associated with decreased physical activity among US retirees in one prior study [39], but not two others [37, 40]. Differences in the type and intensity of caregiving could contribute to varied findings across studies. For retired women facing caregiving-related barriers, incorporating physical activity into caregiver support groups or respite services could reduce stress and provide opportunities for physical activity.
Whereas becoming a caregiver limited time and energy for physical activity, moving after retirement disrupted women’s social networks. Social support and companionship facilitate physical activity among retired women [5, 8]. In the future, greater geographic movement and rising rates of divorce and childlessness might increase the number of women entering retirement with weak social networks [41]. Thus, interventions that provide opportunities for social interaction are likely of increasing importance.
Strengths and Limitations
There were two primary strengths of this study. First, participants were socioeconomically diverse and included African American and non-Hispanic white women. Including the perspectives of retirees from minority racial/ethnic and lower socioeconomic status groups is essential for reducing persistent health disparities. We explored but did not identify differences in themes by race in this sample. Second, we focused on facilitators and barriers of physical activity from multiple levels, including the community environment. Interventions targeting multiple levels are more likely to be effective [12], and community-level changes have a potential for broad public health benefit [34].
Limitations include that the findings from this research are particular to the place and time of data collection: Forsyth County, North Carolina in 2017. Forsyth County has a growing and diverse older adult population, many resources from local universities, and a large network of parks, but is geographically dispersed with limited public transportation. Women in this study were active participants in community organizations, making their experiences unique from those of women who might be more isolated from their communities. The study findings are most relevant to communities with similar geographic and demographic characteristics, although the identification of similar themes in this and other qualitative studies (e.g., importance of social support) corroborates the broader transferability of findings. There were also some limitations to the data collected; for instance, women were asked to describe but not to quantify changes in physical activity and sedentary behavior after retirement, and the definition of sedentary behavior used in this study included behaviors that might have health benefits, such as reading [42]. In addition, few women offered specific recommendations for intervention strategies; a focus group format might be more effective than one-on-one interviews to facilitate brainstorming of intervention ideas.
Conclusions
Promoting physical activity among retired women likely will require multiple intervention strategies. This study identified barriers and facilitators that should be considered for intervention design. Next steps could include assessing the needs of women who might be at greatest risk for physical inactivity, including those who retire from physically active jobs, become caregivers, or move after retirement, and the feasibility of incorporating physical activities into existing programs such as caregiver support groups. Findings also underscore the value of investing in environmental supports for walking and improving public transportation to recreational centers. Such interventions are of increasing public health importance given the rapid growth of older adult populations and high burden of preventable disease associated with aging.
Supplementary Material
Acknowledgments
The authors thank the participants of this study for sharing their experiences, enthusiasm, and ideas. The authors also thank Susan Meny for her assistance with this project. The authors acknowledge Megan Peters, Michael Plante, and Deanna Caruso for their role in coding interview transcripts.
This work was supported by funding from the University of North Carolina at Chapel Hill Gillings Dissertation Award, the Royster Society of Fellows, and the National Institutes of Health National Heart Lung and Blood Institute [NRSA #T32-HL007055-38].
Footnotes
Potential conflicts of interest. The authors report no relevant conflicts of interest.
Contributor Information
Sydney A. Jones, Department of Epidemiology, Gillings School of Global Public Health, University of North Carolina, Chapel Hill, North Carolina..
Jennifer Leeman, School of Nursing, University of North Carolina, Chapel Hill, North Carolina..
Kelly R. Evenson, Department of Epidemiology, Gillings School of Global Public Health, University of North Carolina, Chapel Hill, North Carolina..
References
- 1.Blair SN, Morris JN. Healthy hearts--and the universal benefits of being physically active: physical activity and health. Ann Epidemiol. 2009;19(4):253–256. doi: 10.1016/j.annepidem.2009.01.019 [DOI] [PubMed] [Google Scholar]
- 2.US Department of Health and Human Services. Physical Activity Guidelines for Americans, 2nd edition. Washington, DC: U.S. Department of Health and Human Services; 2018. https://health.gov/sites/default/files/2019-09/Physical_Activity_Guidelines_2nd_edition.pdf/. Published 2018. Accessed April 21, 2019. [Google Scholar]
- 3.North Carolina State Center for Health Statistics. 2017 BRFSS Survey Results: North Carolina. North Carolina State Center for Health Statistics; website. https://schs.dph.ncdhhs.gov/data/brfss/2017/nc/all/_PA150R2.html. Published 2018. Accessed April 4, 2019. [Google Scholar]
- 4.Division of Aging and Adult Services. North Carolina is Aging! Raleigh, NC: North Carolina Department of Health and Human Services; 2017. https://files.nc.gov/ncdhhs/documents/files/NC%20State%20Aging%20Profile%202017_0.pdf. Published 2017. Accessed April 4, 2019. [Google Scholar]
- 5.Barnett I, Guell C, Ogilvie D. The experience of physical activity and the transition to retirement: a systematic review and integrative synthesis of qualitative and quantitative evidence. Int J Behav Nutr Phys Act. 2012;9:97. doi: 10.1186/1479-5868-9-97 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Berg J, Levin L, Abramsson M, Hagberg J-E. Mobility in the transition to retirement - the intertwining of transportation and everyday projects. J Transp Geogr. 2014;38:48–54. 10.1016/j.jtrangeo.2014.05.014 [DOI] [Google Scholar]
- 7.Perras MG, Strachan SM, Fortier MS. Possible selves and physical activity in retirees: The mediating role of identity. Res Aging. 2016;38(8):819–841. doi: 10.1177/0164027515606191 [DOI] [PubMed] [Google Scholar]
- 8.Baxter S, Blank L, Johnson M, et al. Interventions to promote or maintain physical activity during and after the transition to retirement: An evidence synthesis. Public Health Research. 2016;4(4). PMID: 27148615. [PubMed] [Google Scholar]
- 9.Beck F, Gillison F, Standage M. A theoretical investigation of the development of physical activity habits in retirement. Br J Health Psychol. 2010;15(Pt 3):663–679. doi: 10.1348/135910709X479096 [DOI] [PubMed] [Google Scholar]
- 10.Smeaton D, Barnes H, Vegeris S. Does retirement offer a “window of opportunity” for lifestyle change? Views from English workers on the cusp of retirement. J Aging Health. 2016;29(1):25–44. doi: 10.1177/0898264315624903 [DOI] [PubMed] [Google Scholar]
- 11.Elder GJ, Kirkpatrick Johnson M, Crosnoe R. The emergence and development of life course theory. In: Mortimer JT, Shanahan MJ, eds. Handbook of the life course. New York, NH: Kluwer Academic/Plenum Publishers; 20013:3–19. [Google Scholar]
- 12.Sallis J, Owen N, Fisher E. Ecological models of health behavior. In: Glanz K, Rimer BK, Viswanath K, eds. Health Behavior and Health Education: Theory, Research, and Practice. San Francisco, CA: Jossey-Bass; 2008:465–485. [Google Scholar]
- 13.Kosma M, Buchanan D, Hondzinski J. Complexity of exercise behavior among older African American women. J Aging Phys Act. 2017;25(3):333–344. doi: 10.1123/japa.2016-0032 [DOI] [PubMed] [Google Scholar]
- 14.Siddiqi Z, Tiro JA, Shuval K. Understanding impediments and enablers to physical activity among African American adults: A systematic review of qualitative studies. Health Educ Res. 2011;26(6):1010–1024. doi: 10.1093/her/cyr068 [DOI] [PubMed] [Google Scholar]
- 15.Yen IH, Fandel Flood J, Thompson H, Anderson LA, Wong G. How design of places promotes or inhibits mobility of older adults: Realist synthesis of 20 years of research. J Aging Health. 2014;26(8):1340–1372. doi: 10.1177/0898264314527610 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Moran M, Van Cauwenberg J, Hercky-Linnewiel R, Cerin E, Deforche B, Plaut P. Understanding the relationships between the physical environment and physical activity in older adults: a systematic review of qualitative studies. Int J Behav Nutr Phys Act. 2014;11:79. doi: 10.1186/1479-5868-11-79 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Bild DE, Bluemke DA, Burke GL, et al. Multi-ethnic study of atherosclerosis: Objectives and design. Am J Epidemiol. 2002;156(9):871–881. [DOI] [PubMed] [Google Scholar]
- 18.Jones SA, Li Q, Aiello AE, O’Rand AM, Evenson KR. Physical activity, sedentary behavior, and retirement: The Multi-Ethnic Study of Atherosclerosis. Am J Prev Med. 2018;54(6):786–794. doi: 10.1016/j.amepre.2018.02.022 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Shaw BA, Liang J, Krause N, Gallant M, McGeever K. Age differences and social stratification in the long-term trajectories of leisure-time physical activity. J Gerontol B Psychol Sci Soc Sci. 2010;65(6):756–766. doi: 10.1093/geronb/gbq073 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Barnett I, van Sluijs EM, Ogilvie D. Physical activity and transitioning to retirement: a systematic review. Am J Prev Med. 2012;43(3):329–336. doi: 10.1016/j.amepre.2012.05.026 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Muller C, Volkov O. Older women: Work and caregiving in conflict? A study of four countries. Soc Work Health Care. 2009;48(7):665–695. doi: 10.1080/00981380902921732 [DOI] [PubMed] [Google Scholar]
- 22.Carmichael F, Duberley J, Szmigin I. Older women and their participation in exercise and leisure-time physical activity: The double edged sword of work. Sport in Society. 2015;18(1):42–60. 10.1080/17430437.2014.919261 [DOI] [Google Scholar]
- 23.North Carolina Department of Health and Human Services. Forsyth County Aging Profile, 2015. Raleigh, NC: North Carolina Department of Health and Human Services; 2015. https://files.nc.gov/ncdhhs/documents/files/County%20aging%20profiles%202015.pdf. Published 2015. Access October 5, 2017. [Google Scholar]
- 24.County Health Rankings & Roadmaps. County Health Rankings: Forsyth County, NC. CountyHealthRankings.org. http://www.countyhealthrankings.org/app/north-carolina/2017/rankings/forsyth/county/outcomes/overall/snapshot. Published 2017. Accessed October 23, 2017. [Google Scholar]
- 25.Francis JJ, Johnston M, Robertson C, et al. What is an adequate sample size? Operationalising data saturation for theory-based interview studies. Psychol Health. 2010;25(10):1229–1245. doi: 10.1080/08870440903194015 [DOI] [PubMed] [Google Scholar]
- 26.Echeverria SE, Diez-Roux AV, Link BG. Reliability of self-reported neighborhood characteristics. J Urban Health. 2004;81(4):682–701. doi: 10.1093/jurban/jth151 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Ainsworth BE, Irwin ML, Addy CL, Whitt MC, Stolarczyk M. Moderate physical activity patterns of minority women: The Cross-Cultural Activity Participation Study. J Womens Health Gend Based Med. 1999;8(6):805–813. [DOI] [PubMed] [Google Scholar]
- 28.Barnett I, Guell C, Ogilvie D. How do couples influence each other’s physical activity behaviours in retirement? An exploratory qualitative study. BMC Public Health. 2013;13:1197. doi: 10.1186/1471-245813-1197 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.McDonald S, O’Brien N, White M, Sniehotta FF. Changes in physical activity during the retirement transition: A theory-based, qualitative interview study. Int J Behav Nutr Phys Act. 2015;12:25. doi: 10.1186/s12966-015-0186-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Savin-Baden M, Major CH. Qualitative Research: The essential guide to theory and practice. New York, NY: Routledge; 2018. [Google Scholar]
- 31.Kosteli MC, Williams SE, Cumming J. Investigating the psychosocial determinants of physical activity in older adults: A qualitative approach. Psychol Health. 2016;31(6):730–749. doi: 10.1080/08870446.2016.1143943 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Liechty T, Genoe MR, Marston HR. Physically active leisure and the transition to retirement: The value of context. Annals of Leisure Research. 2017;20(1):23–38. doi: 10.1080/11745398.2016.1187570 [DOI] [Google Scholar]
- 33.Heaven B, O’Brien N, Evans EH, et al. Mobilizing resources for wellbeing: Implications for developing interventions in the retirement transition. Gerontologist. 2016;56(4):615–629. doi: 10.1093/geront/gnu159 [DOI] [PubMed] [Google Scholar]
- 34.US Community Preventive Services Task Force. Physical Activity: Built Environment Approaches Combining Transportation System Interventions with Land Use and Environmental Design. Atlanta, GA: The Community Guide; 2017. https://www.thecommunityguide.org/sites/default/files/assets/PA-Built-Environments.pdf. Published 2017. Accessed July 31, 2019. [Google Scholar]
- 35.Van Dyck D, Mertens L, Cardon G, De Cocker K, De Bourdeaudhuij I. Opinions toward physical activity, sedentary behavior, and interventions to stimulate active living during early retirement: A qualitative study in recently retired adults. J Aging Phys Act. 2017;25(2):277–286. doi: 10.1123/japa.2015-0295 [DOI] [PubMed] [Google Scholar]
- 36.Witcher CS, Holt NL, Spense JC, Cousins SO. A case study of physical activity among older adults in rural Newfoundland, Canada. J Aging Phys Act. 2007;15(2):166–183. [DOI] [PubMed] [Google Scholar]
- 37.Scanlon-Mogel J, Roberto K. Older adults’ beliefs about physical activity and exercise: Life course influences and transitions. Quality Ageing Older Adults. 2004;5(3):33–44. 10.1108/14717794200400017 [DOI] [Google Scholar]
- 38.Engberg E, Alen M, Kukkonen-Harjula K, Peltonen JE, Tikkanen HO, Pekkarinen H. Life events and change in leisure time physical activity: A systematic review. Sports Med. 2012;42(5)433–447. doi: 10.2165/11597610-000000000-00000 [DOI] [PubMed] [Google Scholar]
- 39.Queen TL, Butner J, Berg CA, Smith J. Activity engagement among older adult spousal caregivers. J Gerontol B Psychol Sci Soc Sci. 2019;74(7):1278–1282. 10.1093/geronb/gbx106 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Jones SA, Li Q, Aiello AE, O’Rand AM, Evenson KR. Correlates of changes in walking during the retirement transition: The multiethnic study of atherosclerosis. Prev Med Rep. 2018;11:221–230. doi: 10.1016/j.pmedr.2018.07.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Strobl H, Brehm W, Tittlbach S. Physical activity during the transition period between occupation and retirement. Z Gerontol Geriatr. 2010;43(5):297–302. doi: 10.1007/s00391-010-0103-z [DOI] [PubMed] [Google Scholar]
- 42.Tremblay MS, Aubert S, Barnes JD, et al. Sedentary Behavior Research Network (SBRN) - Terminology Consensus Project process and outcome. Int J Behav Nutr Phys Act. 2017;14(1):75. doi: 10.1186/s12966-017-0525-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.