

ABSTRACT
The Research Institute for Radiation Biology and Medicine (RIRBM) of Hiroshima University has been conducting a cohort study of atomic bomb survivors (ABS). Cohort members include those who were issued an Atomic Bomb Health Handbook from the Hiroshima local government. A series of dosimetry systems for the ABS were developed at RIRBM to evaluate the health effects associated with radiation exposure. The framework used to estimate individual doses in our dosimetry systems for ABS is mainly based on the Dosimetry System 86, and its revisions developed by the Radiation Effect Research Foundation. This article describes the design and computational principles for the dosimetry systems in RIRBM and the history of the revisions, from the first version of the system, ABS93D, to the most recent version, ABS16D. We then provide a perspective for further improvement and application of the dosimetry system.
Keywords: dosimetry, atomic bomb survivor (ABS), Hiroshima, DS02, DS86
INTRODUCTION
The Research Institute for Radiation Biology and Medicine (RIRBM) of Hiroshima University has conducted a cohort study of atomic bomb survivors in Hiroshima (ABS). The ABS cohort members consist of approximately 290 000 survivors who were officially issued an Atomic Bomb Health Handbook based on the Act for the Support of Atomic Bomb Victims. The cohort members of ABS are classified into four groups: directly exposed survivors, survivors who entered within 2 km of the hypocenter during the first two weeks after the bombing, exposed in utero survivors and other survivors who engaged in rescues and other related activities. Details of the study methods are described elsewhere [1, 2]. Briefly, the cohort members were followed up for mortality by applying vital statistical data. The ABS is not explicitly designed for radiation epidemiological approaches such as Life Span Study (LSS), the most informative study on evaluating the health effects of radiation exposure among atomic bomb survivors in Hiroshima and Nagasaki conducted by the Radiation Effects Research Foundation (RERF). However, the population size of ABS was larger than that of LSS, and it included survivors who were not covered by LSS, such as those who entered the city center within the first two weeks after the bombing. ABS has the potential to reveal the effects of atomic bombs on human health, not only from a radiological perspective but also from the social aspects.
The RIRBM started ABS in 1971 to compile the mortality statistics of all atomic bomb survivors in Hiroshima prefecture as an open cohort approach, which was established mainly based on information from a nationwide survey of atomic bomb survivors carried out by the Ministry of Health and Welfare in 1965 [1]. RIRBM has continued to expand the cohort study by including new receivers each time a handbook was issued. Because the issuance was aimed at relief for the victims in the administrative project, the participants of ABS were not ideally placed to research the relationship between radiation and human health. Initially, information on the exposure status, such as the town and street names at the time of the bombing or when they entered the city center where there was possible exposure to residual radiation from the bombing, was used as a surrogate measure of radiation to evaluate the health effects by combining the information from several surveys of atomic bomb survivors in Hiroshima prefecture and city. For a more detailed and quantitative study, the radiation dose of the individuals was required and a series of dosimetry systems were developed, as described below.
PRINCIPLE OF DOSE ESTIMATION FOR ATOMIC BOMB SURVIVORS IN THE ABS STUDY
How should we estimate the radiation dose for individuals within the ABS? The basic concept of estimating the individual dose in dosimetry systems for the ABS followed that of the dosimetry system established by RERF for LSS. The important points for determining the individual doses are how much radiation occurred in the environment and how it reached the human body. These two points are closely related to the bomb information, particle transport, shielding and geometrical relationship between the explosion and individual locations.
The detailed characteristics of the atomic bomb dropped were essential because the amount of released radiation was determined based on the following parameters: the component and quantity of the fuel used, the materials of the weapon, the weapon structure and how the weapon exploded. However, researchers at RIRBM have been unable to access this information because a large part of such information is long-held military secrets. Information on the locations and shielding conditions of individuals at the time of bombing is also essential for a dose estimation. Such information was collected from the ‘Fact-finding Survey on Atomic Bomb Victims’ conducted in 1965 by the Ministry of Health, Labour and Welfare and the ‘Survey of Atomic Bomb Survivors and Their Families’ carried out by Hiroshima City and Hiroshima Prefecture from 1973 to 1974.
DEVELOPMENT OF ABS93D
In 1993, Hoshi et al. established the first dosimetry system for ABS, i.e. ABS93D [3], using key parameters provided in Dosimetry System 86 (DS86) [4, 5], which is a simulation-based calculation system developed by RERF, which considers all radiation processes generated in a nuclear reaction, transport and shielding until arrival at the human body. The basic concept of how to estimate the individual dose in the revised versions of the dosimetry system for ABS was similar to that of the dosimetry system established in the revision of DS86 by RERF. In developing ABS93D, Hoshi et al. used a set of values for the free-in-air kerma, representative of the shielding factor of Japanese-style wooden houses and the factors for converting the surrounding kerma into the organ dose provided in DS86. Figure 1 summarizes the relationship among free-in-air kerma, shielded kerma, organ dose and their conversion factors.
Fig. 1.
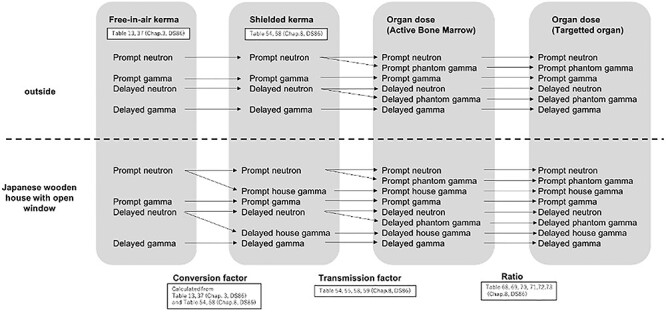
The relationship among free-in-air kerma, shielded kerma, organ dose, and their conversion factors.
In DS86, the free-in-air kerma was calculated for each distance and radiation quality and is summarized in Tables 13 and 37 in Chapter 3 of [5], respectively These values are reflected by the source terms and radiation transport in air, i.e. the location of the bombing, including the height; the energy of the explosion of the bomb, the amounts and components of radionuclides induced through the fission reactions; the neutron reactions with the air, ground and body of the weapon; and the aerodynamics of the explosion.
In free-in air kermas, there are four types of radiation. The fission process in the fuels generates prompt neutrons. The prompt gamma rays consist of primary and secondary gamma rays from the fission products and the activated nuclides by prompt neutrons in the weapons, air and ground, respectively. The term “prompt” implies that such radiation reached the ground within 0.1 s from the time of the bombing. The next two types are “delayed.” The decay of the fission products generated delayed neutrons, which also activated nuclides on their path, resulting in the generation of a part of delayed gamma rays. Of course, the decay of the fission products directly generated delayed gamma rays too. It should be noted that activated nuclides with more than a one minute half-decay time were not considered in the free-in-air kerma, and the individual doses were calculated using DS86 because the main contribution to the accumulated total individual dose was a direct external exposure. The geometrical features of the relationship between the bombing and individual location is essential for direct external exposure. For this reason, the tables show the dependence of distance of the free-in-air kerma in DS86. Using these values, Hoshi et al. comprehensively considered all effects of the source term and the geometrical features in ABS93D without accessing detailed information regarding the bomb.
The framework of DS86 defines the air dose surrounding a target person as “shielded kerma.” The shielded kerma guides the optimization of the calculations. It takes too many computer resources to calculate all paths from the bomb to the individuals using a straightforward Monte Carlo approach. However, a small number of particles reached the individuals, and the remaining number did not contribute to the individual dose. Therefore, in DS86, calculated the particles backward from the individuals to the shielded kerma, and then connected the number to the calculation results from the bomb to the shielded kerma. Six types of shielded kerma were considered: prompt neutrons, prompt gammas, delayed neutrons, delayed gamma, prompt house gamma and delayed house gamma. Two types of house gammas come from the interaction between neutrons and housing materials, contributing to the shielded kerma inside the home. The ABS93D framework incorporates the conversion factor from the free-in-air kerma to the shielded kerma. The conversion factors were calculated by dividing the shielded kerma by the free-in-air kerma 1500 meter from the hypocenter outside and inside the Japanese wooden houses. The shielded kermas from DS86 for outdoors and inside the home with open windows are shown in Tables 54 and 58 in Chapter 8 of [5], respectively. For the calculation of two types of house gamma, the used free-in-air kerma was prompt and delayed neutrons because house gamma rays were induced from neutrons reaching houses.
The last parameter of ABS93D introduced herein is the transmission factor from the shielded kerma to the organ dose. For the calculation of the organ dose, two additional types of radiation should be taken into account: prompt and delayed phantom gamma, which come from the interaction between neutrons and the human body. Therefore, in the case of outdoor exposure, there are six transmission factors for four types of shielded kerma in DS86, whereas for inside the house, there are eight transmission factors for six types of shielded kerma, as shown in Tables 54, 55, 58 and 59 in Chapter 8 of [5]. Except for the two types of phantom gammas, the values 1500 meter from the hypocenter were adopted in ABS93D because transmission factors do not depend on the distance. For the phantom gammas, the transmission factors were interpolated corresponding to distances of 500, 1000, 1500 and 2000 meter from the hypocenter. Because the transmission factors were indicated for four orientations, i.e. on the right and left sides and back and front, the averages relative to orientation were applied to ABS93D. These tables show only the case of active bone marrow and breast, and thus the dose in the other organs will be estimated from the active bone marrow dose by multiplying the targeted organ dose ratios with the active bone marrow in Tables 68–73 in Chapter 8 of [5] depending on age.
ABS93D provides the organ dose of the ABSs who were exposed outdoors and inside the Japanese wooden houses when their location at the time of the bombing was accurately recorded. The total number of survivors who were given dose estimates by ABS93D was initially 26 278. After checking the consistency with DS86 at individual doses [6] for 50 318 survivors, including survivors with less than 20 mGy dose exposed at more than 2 km from the hypocenter, Hayakawa et al. concluded that ABS93D was useful for evaluating the health effects among cohort members of ABS, and the risk of cancer mortality was evaluated later in relation to radiation exposure by Matsuura et al. [2] which reported slightly lower, but no marked difference from LSS results for total solid cancers. ABS93D was also applied to the ABS cohort study conducted at Nagasaki University, which considers radiation effects such as monoclonal gammopathy [7]. Finally, ABS93D provided dose estimates for 33 173 individuals exposed within 2 km through an additional investigation up to the year 2004, based on the location of the survivor at the time of the bombing.
DEVELOPMENT OF ABS2000D
In 2000, ABS2000D was developed as the second version of the dosimetry system for ABS with a special focus on improving the free-in-air kerma from DS86, which shows a discrepancy with the measurement data. The free-in-air kerma in DS86, which was used in ABS93D, was checked using measurement data from environmental samples in a retrospective dosimetry, such as thermoluminescence (TL) from bricks and tiles induced from gamma rays [8–13] and residual radionuclides in grass and rocks activated by neutrons, such as 32P, 60Co, 36Cl and 152Eu [14–27]. In addition, after 2000, the fast neutrons that were more influential on individual doses than the thermal neutrons could be directly estimated by measuring 63Ni in Cu using accelerator mass spectroscopy [28, 29].
Although these experimental data were roughly consistent with the values calculated using DS86, systematic inconsistencies were recognized [30, 31]. This tendency was clear in the data measuring the products from the thermal neutron reactions. At nearer the hypocenter, the data of 60Co [16–19, 24],152Eu [16–18, 20, 21] and 36Cl [25, 26] expected lower neutron fluences than DS86, although the tendency was opposite at further than 1.2 km from the hypocenter.
As a theoretical approach, Hoshi et al. proposed a crack model [32] to solve the discrepancy between the experimental data and the values calculated using DS86. In this model, a small crack on the barrel of the bomb near the front nose locknut side was assumed. In the longitudinal direction of the cylindrical bomb body, one assumption was a 3 cm wide parallel space, and the other was a 12 cm wide 90° azimuthal angle crack. The authors assumed the latter because some data related to neutron fluence on the ground showed asymmetry to the hypocenter. In addition, with this model, the height of the neutron emission point, which means the height of the bombing, was elevated by 90 m. Based on this model, the free-in-air kerma was re-calculated using the Monte Carlo source code (MCNP-4B [33]) applied to the survivors in ABS, i.e. ABS2000D. Katayama et al. reassessed the risk of cancer mortality among ABS members based on ABS2000D [34]. It reported no significant change from the results of the ABS using ABS93D.
In the workshops held at RERF for a reassessment of the dosimetry system used to solve the systematic inconsistency with the data starting from 1996, the two key parameters in the source term were identified as having been modified, i.e. from 580 to 600 meter for the height of the bombing, and from 15 to 16 kt for the energy of the explosion.
The modification of the height had a more substantial impact on the proximal survivors than the distant survivors in terms of the radiation dose; the range between the bomb and the survivors on the ground was altered considerably to be more distant around the hypocenter than a distant location. By contrast, the modification of the energy of the explosion had a common impact regardless of the location. As a result, within the short range, the neutron fluence decreased before the modifications because the modification of the height had a stronger impact than that of the energy of the explosion; within the middle range, both impacts canceled each other out; and in the long-range, the fluence became higher because the modification of the power was dominantly affected. However, the discrepancy within the long-range still remained. At the meeting in 2001, it was agreed that the newly revised dosimetry system, later called DS02, was not applicable to survivors exposed at more than 1.2 km from the hypocenter.
DEVELOPMENT OF ABS16D
Nevertheless, this problem in terms of the dosimetry for distant locations had been resolved within a few years from 2001. In the same year, 2001, Ruehm reported that the re-measurements of 36Cl agreed with the preliminary results from new calculations for locations further than 1.2 km, which was later confirmed and published in 2005 [35]. The consistency in 36Cl triggered the re-measurement of 152Eu up to statistics of an order of magnitude. Finally, agreement between the data for 152Eu and DS02 [36] was confirmed [30].
In addition, the position of the explosion also significantly affected the free-in-air kerma on the ground. In DS02, to improve the precision of the hypocenter, Cullings et al. attempted to correct the distortions of the army map RERF used in DS02 by comparing it with the urban planning map of Hiroshima City using landmarks remaining after the bombing [37].
In addition to these modifications, a precise calculation of the radiation transport in the air was applied to the dosimetry system. RERF then issued DS02, a revision to DS86 [37]. Incidentally, all far-field discrepancies were resolved in 2012 when re-measurements of the 60Co was completed, and an agreement was reported [38].
In response to this revision, Hoshi et al. revised the dose system for ABS2000D by replacing the values of the free-in-air kerma with those in DS02; thus, ABS16D was developed. The organ dose on the active bone marrow summed for all radiation types with RBE = 10 for neutrons is shown in Fig. 2.
Fig. 2.
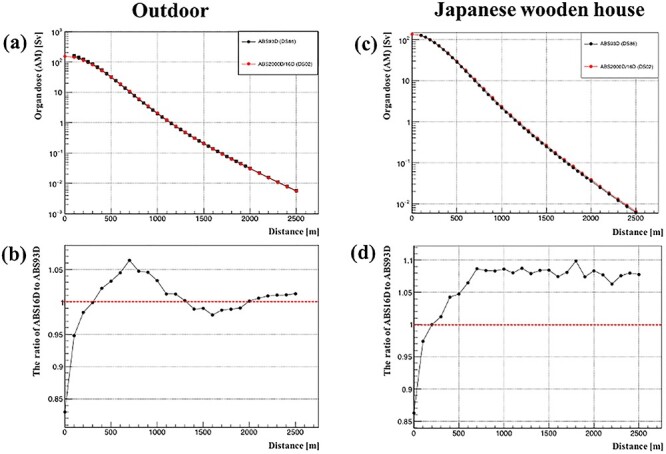
The dose on the active bone marrow in ABS16D relative to the distance (RBE = 10): (a) outdoor case. The black shows ABS93D, and the red shows ABS16D; (b) The ratio of ABS16D to ABS93D outdoors; (c) Inside a Japanese wooden house. The black shows ABS93D, and the red shows ABS16D; and (d) The ratio of ABS16D to ABS93D inside a Japanese wooden house.
At the same time, this revision involves an improvement of the precision of the locations of the survivors, which we will introduce in the next section.
ADDITIONAL FEATURES OF ABS16D AND EXAMPLES OF ITS APPLICATION
In ABS93D and ABS2000D, the original mesh was defined to express the locations of ABSs. It was superimposed on a 100 meter square and concentric circle every 100 meter centered on the hypocenter. The centers of meshes where the survivors were at the time of the bombing had expressed their location used in dose calculation. This implies that the resolution of the position was poor, and the actual position was approximately 70 meter from the center of the mesh at maximum.
Sato et al. tried to improve the accuracy of the locations of the survivors using GIS [39]. They used an urban planning map and detailed residential map in Hiroshima City from approximately 1928 and 1930 for GIS, respectively. The former map is based on survey results but does not include house numbers, whereas the latter map includes house numbers, but no survey was conducted. By combining the two, a map surveyed with house numbers was created and used as a base. This base map was modified geometrically by comparison with other maps, and the aviation photograph taken in 1945 by the US army.
The questionnaire survey conducted from 1968 to 1970 provided detailed information on the location of each survivor, which aimed to collect many testimonies of the damage caused by the explosion in every house around the city center to reconstruct the state of the hypocenter. Based on these results, the addresses of the survivors present during the bombing were fixed. Sato et al. newly defined the center of the house in each address to coordinate the survivors at the time of the bombing, which improved the distance between the bomb and survivors. Owing to this endeavor, the accuracy of the distance improved for approximately 6000 of the survivors and the revised distance shifted an additional 0.2 meter on average from the previous value. The standard deviation of the differences between the original and revised distances was 32 meter, which reflects both the improvement of location and modification of the map [40].
ABS16D adopted these improvements in the same way as the revision of the free-in-air kerma from DS86 to DS02. The most significant contribution to the individual dose was the revision of the free-in-air kerma. Sato et al. compared the risk of cancer mortality in an ABS cohort using ABS93D and ABS16D. They found a similar decrease in the point estimate of the excess relative risk (ERR) per Gy as shown in LSS through the revision from DS86 to DS02 [40]. ABS16D was recently used to evaluate the relative biological effectiveness (RBE) of the neutrons. Based on the linear ERR model, which was applied to the LSS and ABS data, Sato K et al. found that the best estimate of the RBE for LSS or ABS was much higher than 10, which is widely used in atomic bomb survivor studies, although there were no statistically significant differences among the estimated values [41].
FUTURE PROSPECTS OF THE DOSIMETRY SYSTEM FOR STUDY ON ABS
One of the remaining issues for ABS16D is the comparison of the individual doses for the same person between LSS and ABS, which is under planning (as of 2021). In addition, we should evaluate the uncertainty in the dose estimates and its potential impact on the risk evaluation in epidemiological studies. In DS86, the magnitude of uncertainty in the individual doses is generally assumed to range from 30–45%, and allowance for such uncertainty typically increases the risk estimates by 10%–15% [4]. In the dosimetry systems for ABS, we should consider the Berkson-type error owing to the application of a typical coefficient from DS86 to the target survivors who were exposed, as well as the original random error associated with DS86. The situations for each survivor were assumed to be more diverse and detailed in DS86 than in the dosimetry systems for ABS, and typical coefficients for every shielding category that the dosimetry systems for the ABS adopted were calculated by averaging these detailed situations. Although we should confirm this, we believe this type of uncertainty is not significant because the survivors having these coefficients applied for the calculation are limited in only shielding categories DS86 validated that considered variety of details. For evaluating uncertainty, we can apply coefficients in detailed situations before taking the average in DS86 and verify the range of radiation dose caused by changing coefficients. Additionally, the way to collect the information of position at the bombing and shielding situation was slightly different between ABS and LSS.
The information was gathered by questionnaire, but only in LSS, RERF interviewed cohort members at the beginning. We should make the comparison of the distance and shielding categories in the same individuals.
It would be better to expand the dose estimation for survivors with no dose assigned to take advantage of the ABS study because the total cohort size is approximately 290 000 individuals. Based on the testimonies, various types of shielding at the bombing were reported, but only ‘outdoor (no shielding)’ and ‘Japanese wooden houses’ were considered for ABS because only these shield types were calculated in DS86. A new type of building, i.e. a wooden school building, was introduced in DS02 and should be applied to our dosimetry systems. In addition, it will be possible to conduct a Monte Carlo simulation to calculate other shielding factors for concrete, tin, brick, stone and storehouses.
To improve the accuracy of the dose estimation, we need to update the transmission factor from shielded kerma to organ dose by reflecting the development [42, 43] and considering studies [44] on a more detailed Japanese phantom. In addition, we should also consider the elevation of the individual survivors during the bombing; Cullings et al. indicated in the newest version, DS02R1, that the height of the position of the survivor affected the angle of elevation to the explosion point and the thickness of the terrestrial shielding [45].
In studying the effects of exposure to lower doses of radiation, it may be worthwhile establishing a dosimetry system that accounts for internal exposure and residual radiation within a short period for the survivors in the ABS cohort study, which was once considered in DS86 but was found to have little contribution. Research on the physiological and chemical dynamics of radioactive nuclides has progressed compared to the time required to establish DS86.
ACKNOWLEDGEMENTS
The authors would like to thank Emeritus Professor Masaharu Hoshi for the helpful comments on the article. He contributed as the leading member establishing the dose systems for the ABS study. We also thank all the staff members who engaged at RIRBM for developing the dose systems. We would like to thank Editage (www.editage.com) for English language editing.
SUPPLEMENT FUNDING
This supplement has been funded by the Program of the Network-type Joint Usage/Research Center for Radiation Disaster Medical Science of Hiroshima University, Nagasaki University, and Fukushima Medical University.
CONFLICT OF INTEREST
The authors report no conflict of interest.
REFERENCES
- 1. Kurihara M, Munaka M, Hayakawa N et al. Mortality statistics among atomic bomb survivors in Hiroshima prefecture, 1968–1972. J Radiat Res 1981;22:456–71. [DOI] [PubMed] [Google Scholar]
- 2. Matsuura M, Hoshi M, Hayakawa N et al. Analysis of cancer mortality among atomic bomb survivors registered at Hiroshima University. Int J Radiat Biol 1997;71:603–11. [DOI] [PubMed] [Google Scholar]
- 3. Hoshi M, Matsuura M, Hayakawa N et al. Estimation of radiation doses for atomic-bomb survivors in the Hiroshima University registry. Health Phys 1996;70:735–40. [DOI] [PubMed] [Google Scholar]
- 4. Cullings HM, Fujita S, Funamoto S et al. Dose estimation for atomic bomb survivor studies: its evolution and present status. Radiat Res 2006;166Pt 2:219–54. [DOI] [PubMed] [Google Scholar]
- 5. Roesch WC (ed). US-Japan Joint Reassessment of Atomic Bomb Radiation Dosimetry in Hiroshima and Nagasaki. Final Report Vols. 1 and 2. Hiroshima, Japan: Radiation Effects Research Foundation, 1987. [Google Scholar]
- 6. Hayakawa N, Hoshi M, Matsuura M et al. Comparison between DS86 and ABS93D. Studies on radiation effect for atomic bomb survivors. Proceedings of the cooperative Committee of Atomic Bomb Causalities. Shigematsu Group. Radiation Effect Research Foundation 1994;119–23. [Google Scholar]
- 7. Iwanaga M, Tagawa M, Tsukasaki K et al. Relationship between monoclonal gammopathy of undetermined significance and radiation exposure in Nagasaki atomic bomb survivors. Blood 2009;113:1639–50. [DOI] [PubMed] [Google Scholar]
- 8. Nagatomo T, Ichikawa Y, Ishii H et al. Thermoluminescence dosimetry of γ rays from the atomic bomb at Hiroshima using the predose technique. Radiat Res 1988;113:227–34. [PubMed] [Google Scholar]
- 9. Nagatomo T, Ichikawa Y, Hoshi M. Thermoluminescence dosimetry of gamma rays using ceramic samples from Hiroshima and Nagasaki: a comparison with DS86 estimates. J Radiat Res 1991;32:48–57. [DOI] [PubMed] [Google Scholar]
- 10. Ichikawa Y, Nagatomo T, Hoshi M et al. Thermoluminescence dosimetry of gamma rays from the Hiroshima atomic bomb at distances of 1.27 to 1.46 kilometers from the hypocenter. Health Phys 1987;52:443–51. [DOI] [PubMed] [Google Scholar]
- 11. Hoshi M, Sawada S, Ichikawa Y et al. Thermoluminescence dosimetry of γ-rays from the Hiroshima atomic bomb at distances 1.91–2.05 km from the hypocenter. Health Phys 1989;57:1003–8. [PubMed] [Google Scholar]
- 12. Nagatomo T, Hoshi M, Ichikawa Y. Thermoluminescence dosimetry of the Hiroshima atomic-bomb gamma rays between 1.59 km and 1.63 km from the hypocenter. Health Phys 1995;69:556–9. [DOI] [PubMed] [Google Scholar]
- 13. Nagatomo T, Hoshi M, Ichikawa Y. Comparison of the measured gamma ray dose and the DS86 estimate at 2.05 km ground distance in Hiroshima. J Radiat Res 1992;33:211–7. [DOI] [PubMed] [Google Scholar]
- 14. Hoshi M, Kato K. Data on neutrons in Hiroshima. In: Roesch WC (ed). US–Japan Joint Reassessment of Atomic Bomb Radiation Dosimetry in Hiroshima and Nagasaki. Hiroshima: Radiation Effects Research Foundation, 1987, 252–5. [Google Scholar]
- 15. Hoshi M, Hasai H, Yokoro K. Studies of radioactivity produced by the Hiroshima atomic bomb: 1. neutron-induced radioactivity measurements for dose evaluation. J Radiat Res 1991;32:20–31. [DOI] [PubMed] [Google Scholar]
- 16. Hoshi M, Yokoro K, Sawada S et al. Europium-152 activity induced by Hiroshima atomic bomb neutrons: comparison with the 32P, 60Co, and 152Eu activities in dosimetry system 1986 (DS86). Health Phys 1989;57:831–7. [PubMed] [Google Scholar]
- 17. Shizuma K, Iwatani K, Hashi H et al. Specific activities of 60Co and 152Eu in samples collected from the atomic-bomb dome in Hiroshima. J Radiat Res 1992;33:151–62. [DOI] [PubMed] [Google Scholar]
- 18. Shizuma K, Iwatani K, Hasai H et al. Residual 152Eu and 60Co activities induced by neutrons from the Hiroshima atomic bomb. Health Phys 1993;65:272–82. [DOI] [PubMed] [Google Scholar]
- 19. Shizuma K, Iwatani K, Hasai H et al. Identification of 63Ni and 60Co produced in a steel sample by thermal neutrons from the Hiroshima atomic bomb. Nucl Instrum Meth Phys Res A 1997;384:375–9. [Google Scholar]
- 20. Shizuma K, Iwatani K, Hasai H et al. 152Eu depth profiles in granite and concrete cores exposed to the Hiroshima atomic bomb. Health Phys 1997;72:848–55. [DOI] [PubMed] [Google Scholar]
- 21. Imura T, Nakanishi T, Komura K et al. Europium-152 in sample exposed to the nuclear explosions at Hiroshima and Nagasaki. Nature 1983;302:132–4. [Google Scholar]
- 22. Nakanishi T, Ohtani H, Mizuochi R et al. Residual neutron-induced radionuclides in samples exposed to the nuclear explosion over Hiroshima: comparison of the measured values with calculated values. J Radiat Res 1991;32:69–82. [DOI] [PubMed] [Google Scholar]
- 23. Hashizume T, Maruyama T, Shiragai A, et al. Estimation of the air dose from the atomic bombs in Hiroshima and Nagasaki. Health Phys; 1967;13:149–61. [DOI] [PubMed] [Google Scholar]
- 24. Kerr GD, Dyer FF, Emery JF et al. Activation of Cobalt by Neutrons from the Hiroshima Bomb. US: Oak Ridge National Laboratory Report No. ORNL-6590. 1990.
- 25. Straume T, Finkel RC, Eddy D et al. Use of accelerator mass spectrometry in the dosimetry of Hiroshima neutrons. Nucl Instrum Methods Phys Res, Sect B 1990;52:552–6. [Google Scholar]
- 26. Straume T, Egbert SD, Woolson WA et al. Neutron discrepancies in the DS86 Hiroshima dosimetry system. Health Phys 1992;63:421–6. [DOI] [PubMed] [Google Scholar]
- 27. Yamasaki F, Sugimoto A. Radioactive 32P produced in sulfur in Hiroshima. US–Japan joint reassessment of atomic bomb radiation dosimetry in Hiroshima and Nagasaki. Final report. DS86. Dosim Syst 1986;2:246–47 (appendix to vol. 1). [Google Scholar]
- 28. Straume T, Rugel G, Marchetti AA et al. Measuring fast neutrons in Hiroshima at distances relevant to atomic-bomb survivors. Nature 2003;424:539–42. [DOI] [PubMed] [Google Scholar]
- 29. Rühm W, Carroll KL, Egbert SD et al. Neutron-induced 63 Ni in copper samples from Hiroshima and Nagasaki: a comprehensive presentation of results obtained at the Munich Maier-Leibnitz laboratory. Radiat Environ Biophys 2007;46:327–38. [DOI] [PubMed] [Google Scholar]
- 30. Hoshi M, Endo S, Tanaka K et al. Intercomparison study on (152)Eu gamma ray and (36)cl AMS measurements for development of the new Hiroshima–Nagasaki atomic bomb dosimetry system 2002 (DS02). Radiat Environ Biophys 2008;47:313–22. [DOI] [PubMed] [Google Scholar]
- 31. Hoshi M, Takada J, Oka T. A possible explanation for the DS86 discrepancy between the data and calculation in Hiroshima. Nagasaki Symposium: Radiation and Human health, Proposal from Nagasaki. UK: Excerpta Medica, 1996, 175–91. [Google Scholar]
- 32. Hoshi M, Endo S, Takada J et al. A crack model of the Hiroshima atomic bomb: explanation of the contradiction of “dosimetry system 1986”. J Radiat Res 1999;40:145–54. [DOI] [PubMed] [Google Scholar]
- 33. Briesmeister JF. General MCNP-A. Monte Carlo N-particle transport code version 4. In: A. Los Alamos National Laboratory. Report LA-12625-M. US, Oak Ridge: the Radiation Safety Information Computational Center, 1993. [Google Scholar]
- 34. Katayama H, Matsuura M, Endo S et al. Reassessment of the cancer mortality risk among Hiroshima atomic-bomb survivors using a new dosimetry system, ABS2000D, compared with ABS93D. J Radiat Res 2004;43:53–64. [DOI] [PubMed] [Google Scholar]
- 35. Huber T, Rühm W, Kato K et al. The Hiroshima thermal-neutron discrepancy for (36)cl at large distances. Part I: New (36)cl measurements in granite samples exposed to A-bomb neutrons. Radiat Environ Biophys 2005;44:75–86. [DOI] [PubMed] [Google Scholar]
- 36. Hoshi M. New dosimetry system for atomic bombs: DS02. J Hiroshima Med Ass 2004;57:314–8. [DOI] [PubMed] [Google Scholar]
- 37. Young RW, Kerr GD. Reassessment of the Atomic Bomb Radiation Dosimetry for Hiroshima and Nagasaki – Dosimetry System 2002 (DS02). Hiroshima, Japan: Radiation Effects Research Foundation, 2002. [Google Scholar]
- 38. Gasparro J, Hult M, Marissens G et al. Measurements of (60)co in massive steel samples exposed to the Hiroshima atomic bomb explosion. Health Phys 2012;102:400–9. [DOI] [PubMed] [Google Scholar]
- 39. Sato Y, Hoshi M, Otaki M et al. Using geographic information system (GIS) for improvement of Hibakusha location accuracy. J Hiroshima Ass 2010;63:261–4. [Google Scholar]
- 40. Sato K, Tomita T, Otani K. Implementation of DS02-compliant atomic bomb dosimetry system. Nagasaki J at Hiroshima University 2016;91:197–201 (abs.16D). [Google Scholar]
- 41. Satoh K, Yasuda H, Kawakami H et al. Relative biological effectiveness of neutrons derived from the excess relative risk model with the atomic bomb survivors data managed by Hiroshima University. Radiat Prot Dosimetry 2018;180:346–50. [DOI] [PubMed] [Google Scholar]
- 42. Griffin K, Paulbeck C, Bolch W et al. Dosimetric impact of a new computational voxel phantom series for the Japanese atomic bomb survivors: children and adults. Radiat Res 2019;191:369–79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Paulbeck C, Griffin K, Lee C et al. Dosimetric impact of a new computational voxel phantom series for the Japanese atomic bomb survivors: pregnant females. Radiat Res 2019;192:538–61. [DOI] [PubMed] [Google Scholar]
- 44. Sato T, Funamoto S, Paulbeck C et al. Dosimetric impact of a new computational voxel phantom series for the Japanese atomic bomb survivors: methodological improvements and organ dose response functions. Radiat Res 2020;194:390–402. [DOI] [PubMed] [Google Scholar]
- 45. Cullings HM, Grant EJ, Egbert SD et al. DS02R1: improvements to atomic bomb survivors’ input data and implementation of dosimetry system 2002 (DS02) and resulting changes in estimated doses. Health Phys 2017;112:56–97. [DOI] [PubMed] [Google Scholar]