

Abstract
Introduction:
Psoriasis is a chronic disease. Research shows the emergence of harmful habits such as cigarette smoking and alcohol consumption in people with psoriasis.
Aim:
The aim of this study was to determine the frequency of habits, cigarette smoking and alcohol consumption in patients with psoriasis, sexual distribution, and the relationship of habits with the severity of the disease.
Methods:
The prospective study included 129 subjects with psoriasis, of which 67 or 51,94% were women and 62 or 48,06% were men.
Results:
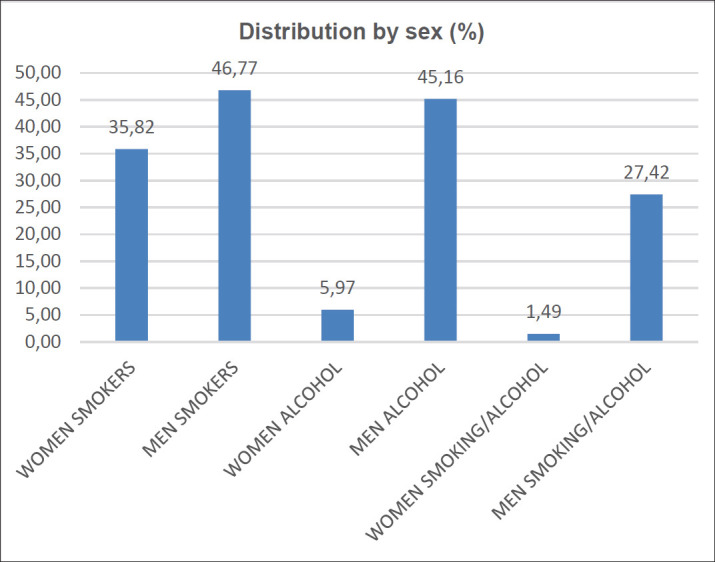
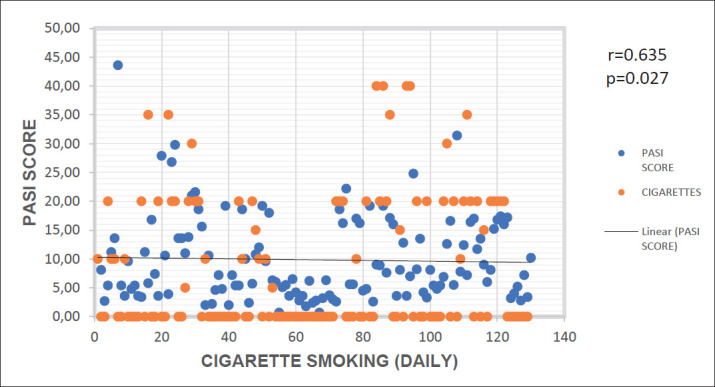
The frequency of cigarette smoking was 41,09%, alcohol consumption 24,80%. The gender distribution of cigarette smoking was: 35,82% of women and 46,77% of men smoked cigarettes. The gender distribution of alcohol consumption is: women 5,97% and men 45,16%. The severity of psoriasis, that is PASI score and cigarette smoking were statistically significantly related (r=0,63), and PASI score and alcohol consumption were not statistically significantly related (r=0,32).
Conclusion:
Cigarette smoking and alcohol consumption are present in psoriasis sufferers, cigarette smoking is associated with disease severity, and alcohol consumption is not. It takes knowledge of the habits of people with psoriasis and a multidisciplinary approach to get rid of harmful habits.
Keywords: Psoriasis, habits, cigarettes, alcohol, PASI score
1. BACKGROUND
Psoriasis is a chronic disease that affects about 2-3% of the world’s population (1). It affects the lifestyle, diet and habits of patients. Studies have shown that in patients with psoriasis, harmful habits such as smoking and alcohol consumption are present, and this is influenced by the chronicity and incurability of psoriasis (2). Cigarette smoking and alcohol consumption have been identified as risk factors for the occurrence of psoriasis, but also exacerbation of existing psoriasis (3, 4). Current and former smokers are more likely to have psoriasis than non-smokers (5, 6).
Increased mortality in psoriasis patients due to smoking and alcohol consumption has been found (7). There are various research results on the connection between the severity of psoriasis and cigarette smoking and alcohol consumption. Some studies have shown an association between cigarette smoking and alcohol consumption with the severity of psoriasis (8, 9) but Sobhan et Farshchian (10) did not find a significant association between cigarette smoking and alcohol consumption with disease severity.
2. OBJECTIVE
The aim of this study was to determine the frequency of habits, cigarette smoking and alcohol consumption in patients with psoriasis, sexual distribution, and the relationship with the severity of the disease.
3. METHODS
This is a prospective study, and included 129 subjects with psoriasis over the age of 18, of whom 67 or 51,94% were women and 62 or 48,06% were men. The mean age of the subjects was 48,13 (SD=±14,45) years. The prevalence of psoriasis was: psoriasis vulgaris 82,95%, psoriasis guttata 11,63%, psoriasis pustulosa generalista 3,87%, psoriasis pustulosa palmaris et plantaris 1,55%.
Psoriasis patients older than 18 years participated in the research. Excluded from the study are those subjects who, in addition to psoriasis, also suffer from some other skin disease, suffer from psoriasis for less than a year, use systemic therapy for psoriasis, and pregnant women and mothers. All participants in the research were explained the purpose and manner of conducting the research, and written consent was requested to participate in the research. Then a medical history was taken, including data on habits, cigarette smoking and alcohol consumption, a dermatological examination of the skin and visible mucous membranes was performed, and a PASI score was determined. Smoking data included questions: does he smoke cigarettes, how many cigarettes (per day) and for how many years? Data on alcohol consumption included: do they consume alcohol, how many drinks (daily, weekly or monthly) and for how many years? For determining the severity and outspread of psoriasis, Psoriasis Area and Severity Index (PASI) was used. In four regions body-head, torso, upper and lower extremities. In the four regions of the body-head, torso, upper and lower extremities evaluated the characteristics of the disease, severity of erythema, infiltration and desquamation with the score 1-4, and the affected area of skin psoriatic changes with the score 1-6 (Table 1). In assessing the severity of erythema scales may not be removed. Theoretically PASI can range from 0-72 (11).
Table 1. Measurement of PASI.
| Grade | 0 | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|---|
| Erythema (E) | None | Mild | Medium | Strong | Very Strong | - | - |
| Infiltration (I) | |||||||
| Desquamation (D) | |||||||
| Enveloped area of the skin % (A) | 0 | 1-9 | 10-29 | 30-49 | 50-69 | 70-89 | 90-100 |
By this method we calculate:
Buttocks as a part of lower extremities, that is, region of the leg (l)
Armpits and shoulders as a part of upper extremities, that is, region of the arm (a)
The neck is calculated as a part of the head (h)
Torso (t)
For calculating the PASI, the summation of Erythemas, infiltrations and desquamations of single region is multiplied with the numerical value of the region of the body and with the precentage by which the lesions have spread at a single region. Results obtained for each single region are calculated in PASI.
Form for calculating PASI:
* PASI=0,1x(Eh+Ih+Dh)xAh+0,3x(Et+It+Dt)xAt+0,2x(Ea+Ia+Da)xAa+0,4x(El+Il+Dl)xAl.
Legend :
E- Erythema
a–arm
I – Infiltration
h – head
D – Desqumation
t – torso
A – Area
l–leg
Statistical analysis
For the purposes of statistical calculation and obtaining results, real data were used, which were processed in Microsoft Excel. Measures of central tendency-mean value and measures of dispersion-standard deviation were used. The correlation between the two variables was made by the Pearson correlation coefficient (since they are linear models). The lowest value of the significance level is p<0,05.
3. RESULTS
The smoking frequency was 41,09%, and the frequency of alcohol consumption was 24,80%. The average values of PASI score was 9,85 (SD=±7,27). The average duration of smoking was 21,09 (SD=±12,45) years. The average number of cigarettes smoked was 20,28 per day, and ranged from 5 cigarettes to 40 cigarettes per day.
Graph 1. Distribution by sex of cigarette smoking, alcohol consumption and both.
Graph 2. Correlation between PASI score and cigarette smoking (daily).
Graph 3. Correlation between PASI score and alcohol consupmtion.

The average length of alcohol consumption was 22,031 (SD=±10,88) years. The average number of alcoholic beverages consumed per week was 2,5 and ranged from one beverage per month to two beverages per day.
The correlation value, ie the product-moment coefficient of PASI score and cigarette smoking is r=0,63, which indicates a medium strong correlation, ie the increase in the value of PASI score and cigarette smoking, were statistically related, in a medium strong correlation.
The correlation value, ie the product-moment coefficient of the PASI score and alcohol consumption was r=0,32, which indicates a relatively weak correlation, ie the increase in the value of the PASI score and alcohol consumption were not statistically significantly related.
4. DISCUSSION
A prospective study was conducted to determine the frequency of cigarette smoking and alcohol consumption, sexual distribution, and the association of cigarette smoking and alcohol consumption with the severity of psoriasis. In this study, the smoking frequency was 41,09%. Other studies have also shown an increased incidence of cigarette smoking in psoriasis patients and more frequent cigarette smoking in psoriasis patients than in controls (12-15). This is important because the health status of psoriasis sufferers who smoked was worse than in non-smokers (16), and on the other hand smoking almost doubles the risk of psoriasis (17).The frequency of alcohol consumption was 24,80%. The results of other studies showed that alcohol use was higher in patients with psoriasis than in the control group (18-20). literature, 4 of 5 studies have shown alcohol as a risk factor for psoriasis (21).
The gender distribution of cigarette smoking and alcohol consumption in this study was such that women smoked cigarettes less frequently than men, and in particular consumed less alcohol than men. 35,82% of women smoked cigarettes, 5,97% consumed alcohol, and 46,77% of men smoked cigarettes and 45,16% consumed alcohol. Also, both cigarette smoking and alcohol consumption are significantly less common in women compared to men, 1,49% vs. 27,42%. These findings are consistent with other studies because the prevalence of cigarette smoking and alcohol consumption was higher in men, (22). Another study found that 46,6% of men smoked cigarettes, 39,2% of women, 22,3% of men and 5,5% of women consumed alcohol (9).
In this study, cigarette smoking was statistically significantly associated with psoriasis severity, and alcohol consumption was not statistically significantly associated with psoriasis severity. Other studies have shown different results on the association of psoriasis severity with cigarette smoking and alcohol consumption. Some research has shown that smoking and alcohol consumption are associated with severe forms of psoriasis (13, 23). Also, smoking and alcohol consumption were associated with a PASI score greater than 10 (24). Smoking is associated with an increase in the severity of psoriasis, apropos PASI score (25). And people with psoriasis, with more severe forms of the disease, smoked more compared to milder forms (26). On the other hand, some studies have not found a link between cigarette smoking and alcohol consumption with the severity of psoriasis. Beata et al. (19) found no association between smoking and the severity of psoriasis. Also, smoking was associated with a 70% higher risk of psoriasis, but was not associated with weight or PASI score (27). And there was no association between the severity of psoriasis and alcohol consumption (28). Geographical, ethnic, social and religious norms, as well as their relationship and impact on cigarette smoking and alcohol consumption, should always be taken into account when assessing the frequency of cigarette smoking and alcohol consumption, as well as their gender distribution.
The connection between psoriasis and cigarette smoking and alcohol consumption is quite complex and has not been fully investigated. Cigarette smoking, ie nicotine and alcohol affect many processes in the body, and can affect psoriasis in several ways. Cigarette smoking works by nicotine increasing the production of proinflammatory cytokines, such as TNF-α, IL-12, IL-17, IL-2 (21).
In addition to affecting the production of proinflammatory cytokines, alcohol also affects the proliferation of keratinocytes (29). Alcohol consumption and cigarette smoking affect psoriasis, but psoriasis and everything that accompanies it, stigmatization, prejudice and consequent isolation can affect the habit of smoking cigarettes and consuming alcohol. Caring for habits is part of a comprehensive care for psoriasis. Quitting cigarette smoking and alcohol consumption in psoriasis sufferers should be one of the goals of long-term disease control.
5. CONCLUSION
Cigarette smoking and alcohol consumption are present in psoriasis sufferers, cigarette smoking is associated with the severity of the disease, and alcohol consumption is not. Encourage patients to get used to it, and enable a multidisciplinary approach to this problem.
Author’s contribution:
All authors were involved in the preparation of this article. All authors have read and approved the manuscript.
Conflict of interest:
The authors declare no conflict of interest.
Financial support and sponsorship:
None.
REFERENCES
- 1.Madden SK, Flanagan KL, Jones G. How Lifestyle Factors and Their Associated Pathogenetic Mechanisms Impact Psoriasis. Clin Nutr. 2020 Apr;39(4):1026–1040. doi: 10.1016/j.clnu.2019.05.006. [DOI] [PubMed] [Google Scholar]
- 2.Gupta MA, Gupta AK. Psychodermatology: An update. J Am Acad Dermatol. 1996 Jun;34(6):1030–1046. doi: 10.1016/s0190-9622(96)90284-4. [DOI] [PubMed] [Google Scholar]
- 3.Albaghdadi A. Current and Under Development Treatment Modalities of Psoriasis: A Review. Endocr Metab Immune Disord Drug Targets. 2017;17(3):189–199. doi: 10.2174/1871530317666170804153751. [DOI] [PubMed] [Google Scholar]
- 4.Akay A, Pekcanlar A, Bozdag KE, Altintas L, Karaman A. Assessment of depression in subjects with psoriasis vulgaris and lichen planus. J Eur Acad Dermatol Venereol. 2002 Jul;16(4):347–352. doi: 10.1046/j.1468-3083.2002.00467.x. [DOI] [PubMed] [Google Scholar]
- 5.Bø K, Thoresen M, Dalgard F. Smokers Report More Psoriasis, but Not Atopic Dermatitis or Hand Eczema: Results From a Norwegian Population Survey Among Adults. Dermatology. 2008;216(1):40–45. doi: 10.1159/000109357. [DOI] [PubMed] [Google Scholar]
- 6.Dai XY, Wang SC, Chou YJ, Chang YT, Chen TJ, Li CP, et al. Smoking, but Not Alcohol, Is Associated With Risk of Psoriasis in a Taiwanese Population-Based Cohort Study. J Am Acad Dermatol. 2019 Mar;80(3):727–734. doi: 10.1016/j.jaad.2018.11.015. [DOI] [PubMed] [Google Scholar]
- 7.Poikolainen K, Karvonen J, Pukkala E. Excess Mortality Related to Alcohol and Smoking Among Hospital-Treated Patients With Psoriasis. Arch Dermatol. 1999 Dec;135(12):1490–1493. doi: 10.1001/archderm.135.12.1490. [DOI] [PubMed] [Google Scholar]
- 8.Ma L, Li M, Wang H, Li Y, Bai B. High Prevalence of Cardiovascular Risk Factors in Patients With Moderate or Severe Psoriasis in Northern China. Arch Dermatol Res. 2014 Apr;306(3):247–251. doi: 10.1007/s00403-013-1437-3. [DOI] [PubMed] [Google Scholar]
- 9.Gerdes S, Zahl VA, Weichenthal M, Mrowietz U. Smoking and Alcohol Intake in Severely Affected Patients With Psoriasis in Germany. Dermatology. 2010;220(1):38–43. doi: 10.1159/000265557. [DOI] [PubMed] [Google Scholar]
- 10.Sobhan M, Farshchian M. Associations Between Body Mass Index and Severity of Psoriasis. Clin Cosmet Investig Dermatol. 2017 Nov;24(10):493–498. doi: 10.2147/CCID.S147236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Fredriksson T, Pettersson U. Severe psoriasis-oral therapy with new retinoid. Dermatologica. 1978;157:238–244. doi: 10.1159/000250839. [DOI] [PubMed] [Google Scholar]
- 12.Menegon DB, Pereira AG, Camerin AC, Cestari T. Psoriasis and Comorbidities in a Southern Brazilian Population: A Case-Control Study. Int J Dermatol. 2014 Nov;53(11):e518–525. doi: 10.1111/ijd.12186. [DOI] [PubMed] [Google Scholar]
- 13.Adisen E, Uzun E, Erduran F, Gürer MA. Prevalence of Smoking, Alcohol Consumption and Metabolic Syndrome in Patients With Psoriasis. An Bras Dermatol. 2018 Mar;93(2):205–211. doi: 10.1590/abd1806-4841.20186168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Farshchian M, Ansar A, Sobhan M. Associations Between Cardiovascular Risk Factors and Psoriasis in Iran. Clin Cosmet Investig Dermatol. 2015 Aug;10(8):437–442. doi: 10.2147/CCID.S86418. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ferdinando LB, Fukumoto PK, Sanches S, Fabricio LHZ, Skare TL. Metabolic Syndrome and Psoriasis: A Study in 97 Patients. Rev Assoc Med Bras (1992) 2018 Apr;64(4):368–373. doi: 10.1590/1806-9282.64.04.368. [DOI] [PubMed] [Google Scholar]
- 16.Bremander A, Jacobsson LTH, Bergman S, Haglund E, Löfvendahl S, Petersson IF. Smoking Is Associated With a Worse Self-Reported Health Status in Patients With Psoriatic Arthritis: Data From a Swedish Population-Based Cohort. Clin Rheumatol. 2015 Mar;34(3):579–583. doi: 10.1007/s10067-014-2742-8. [DOI] [PubMed] [Google Scholar]
- 17.Sarkar R, Chugh S, Bansal S. General Measures and Quality of Life Issues in Psoriasis. Indian Dermatol Online J. 2016 Nov-Dec;7(6):481–488. doi: 10.4103/2229-5178.193908. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Gonzaga HFS, Chaves MD, Gonzaga LHS, Picciani BLS, Jorge MA, Dias EP, et al. Environmental Factors in Benign Migratory Glossitis and Psoriasis: Retrospective Study of the Association of Emotional Stress and Alcohol and Tobacco Consumption With Benign Migratory Glossitis and Cutaneous Psoriasis. J Eur Acad Dermatol Venereol. 2015 Mar;29(3):533–536. doi: 10.1111/jdv.12616. [DOI] [PubMed] [Google Scholar]
- 19.Baeta IGR, Bittencourt VF, Gontijo B, Goulart EMA. Comorbidities and Cardiovascular Risk Factors in Patients With Psoriasis. An Bras Dermatol. 2014 Sep-Oct;89(5):735–744. doi: 10.1590/abd1806-4841.20142874. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Aounallah A, Mernissi FZ, Dahmani B, Bougmiza I, Houria S, Bouadjar B, et al. Addictive Behaviors, Cardiovascular and Metabolic Comorbidities in North African Psoriatic Patients: Case-Control Study. Pan Afr Med J. 2019 Dec;34:205. doi: 10.11604/pamj.2019.34.205.12883. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Brenaut E, Horreau C, Pouplard C, Barnetche T, Paul C, Richard MA, et al. Alcohol consumption and psoriasis: A systematic literature review. J Eur Acad Dermatol Venereol. 2013 Aug;27(3):30–35. doi: 10.1111/jdv.12164. [DOI] [PubMed] [Google Scholar]
- 22.Bayaraa B, Imafuku S. Relationship Between Environmental Factors, Age of Onset and Familial History in Japanese Patients With Psoriasis. J Dermatol. 2018 Jun;45(6):715–718. doi: 10.1111/1346-8138.14321. [DOI] [PubMed] [Google Scholar]
- 23.Zhu KJ, Liu Z, Liu H, Li SJ, Zhu CY, Li KS, et al. An Association Study on the CHRNA5/A3/B4 Gene Cluster, Smoking and Psoriasis Vulgaris. Arch Dermatol Res. 2014 Dec;306(10):939–944. doi: 10.1007/s00403-014-1510-6. [DOI] [PubMed] [Google Scholar]
- 24.Jiamton S, Suthipinittharm P, Kulthanan K, Chularojanamontri L, Wongpraparut C, Slipa-Archa N, et al. Clinical Characteristics of Thai Patients With Psoriasis. J Med Assoc Thai. 2012 Jun;95(6):795–801. [PubMed] [Google Scholar]
- 25.Ahdout J, Kotlerman J, Elashoff D, Kim J, Chiu MW. Modifiable Lifestyle Factor Associated With Metabolic Syndrome in Patients With Psoriasis. Clin Exp Dermatol. 2012 Jul;37(5):477–483. doi: 10.1111/j.1365-2230.2012.04360.x. [DOI] [PubMed] [Google Scholar]
- 26.Curco N, Barriendos N, Barahona MJ, Arteaga C, Garcia M, Yordanov S, et al. Factors Influencing Cardiometabolic Risk Profile in Patients With Psoriasis. Australas J Dermatol. 2018 May;59(2):e93–e98. doi: 10.1111/ajd.12577. [DOI] [PubMed] [Google Scholar]
- 27.Wolk K, Mallbris L, Larsson P, Rosenblad A, Vingard E, Stahle M. Excessive Body Weight and Smoking Associates With a High Risk of Onset of Plaque Psoriasis. Acta Derm Venereol. 2009;89(5):492–497. doi: 10.2340/00015555-0711. [DOI] [PubMed] [Google Scholar]
- 28.Asokan N, Prathap P, Rejani P. Severity of Psoriasis Among Adult Males Is Associated With Smoking, Not With Alcohol Use. Indian J Dermatol. 2014 May;59(3):237–240. doi: 10.4103/0019-5154.131382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Farkas A, Kemeny L. Alcohol, liver, systemic inflammation and skin: a focus on patients with psoriasis. Skin Pharmacol Physiol. 2013;26(3):119–126. doi: 10.1159/000348865. [DOI] [PubMed] [Google Scholar]