

Abstract
Objective:
To examine perceived academic, social, and athletic competence as potential moderators of the relation between symptoms of irritable bowel syndrome (IBS) and functional disability in adolescents and young adults with a history of recurrent abdominal pain (RAP).
Methods:
We assessed IBS symptoms, competence, and disability by telephone interview in RAP patients five years following their medical evaluation.
Results:
For both male and female subjects, the relation between symptoms and disability was stronger at lower levels of perceived academic competence, Furthermore, among females, the relation between symptoms and disability was stronger at lower levels of perceived social competence; among males, the relation was stronger at lower levels of perceived athletic competence.
Conclusions:
Perceived competence moderated the relation between IBS symptoms and functional disability. Interventions designed to enhance patient competence in various roles may be useful in reducing disability among adolescents and young adults with symptoms of IBS.
Keywords: functional disability, competence, irritable bowel syndrome, recurrent abdominal pain
Recurrent abdominal pain (RAP), the most common recurrent pain complaint of childhood (McGrath, 1990), is characterized by repeated episodes of abdominal pain that occur over a period of at least three months and interfere with a child’s activities, It is estimated that 10% to 15% of school-age children experience RAP (Apley, 1975). The pain rarely has an organic etiology. Nonetheless, many children with RAP continue to complain of abdominal pain when they reach adolescence and adulthood.
Christensen and Mortensen (1975) conducted medical evaluations of adults with a history of RAP and reported that many had a clinical picture consistent with irritable bowel syndrome (IBS). Common among adults, IBS is characterized by abdominal pain related to bowel dysfunction not associated with organic disease (Thompson, Creed, Drossman, Heaton, & Mazzacca, 1994). Christensen and Mortensen’s evaluation of IBS in adults with a history of RAP was limited by the absence of a standardized assessment of IBS symptoms. Recently, a five-year prospective study of RAP patients employed the Manning symptom criteria for IBS and found that a small but significantly greater proportion of RAP patients met the symptom criteria for IBS as adolescents and young adults than did a comparison group of well patients (Walker, Guite, Duke, Barnard, & Greene, 1998). Furthermore, the number of IBS symptoms was significantly correlated with levels of disability and health service utilization in the RAP group but not in the well group. The purpose of this study was to explore the nature of the relation between IBS symptoms and disability in those adolescents and young adults with a history of RAP who participated in the five-year prospective study by Walker et al. (1998).
Irritable bowel syndrome is defined as a “functional” bowel disorder in that it is characterized by symptoms that are “not explained by structural or biochemical abnormalities” (Drossman et al., 1994, p, 1). Possible neurophysiological mechanisms for IBS are not well understood but may include disturbances in colonic motility (e.g., Latimer, 1983; Thompson et al., 1994) or in the perception of visceral pain (Naliboff & Mayer, 1996). The symptoms of IBS include abdominal pain, bloating or distension, and various symptoms of disordered defecation including passage of mucus and altered stool frequency or consistency (Thompson et al., 1994). Female, Caucasian, and middle-aged adults constitute the largest segment of patients with IBS (e.g., Sandler, 1990). However, recent research documents IBS symptoms in children and adolescents as well (e.g., Drossman et al., 1993; Hyams et al., 1995; Thomson & Dancey, 1996).
Studies of patients with IBS indicate that, for the majority of patients, pain interferes with daily activities (van Dulmen, Fennis, Mokkink, van der Velden, & Vleijenberg, 1994) and often results in avoidance of jobs, social interaction, and domestic and leisure activities (Corney & Stanton, 1990). Similarly, many individuals in the community with symptoms of IBS exhibit high levels of disability. In a survey of more than 5,000 U.S. households, individuals with symptoms of IBS reported missing an average of 13.4 days of work or school annually due to illness, while individuals with other functional gastrointestinal disorders averaged only 4,9 days of absence annually (Drossman et al., 1993).
Symptoms of IBS, however, are not necessarily associated with disability. For example, studies of community samples show that many individuals who meet the diagnostic criteria for IBS do not seek treatment for their symptoms (Drossman et al., 1988; Latimer, 1983; Whitehead, Bosmajian, Zonderman, Costa, & Schuster, 1988; Whitehead et al., 1990). Little is known about factors that influence the relation between symptoms of IBS and disability.
A learning theory model of illness behavior suggests that inadequate competence in particular roles may influence the relation between IBS and disability (Wooley, Blackwell, & Winget, 1978). Specifically, individuals who enter the sick role during an episode of illness may subsequently learn to routinely adopt illness behavior if their symptom complaints and disability result in special attention from others and avoidance of activities in which they expect to perform poorly. Thus, among individuals with low competence who tend to experience failure in various activities, a stronger association may develop between symptoms and functional disability than is the case for those with higher competence and expectations of success in their daily activities. This prediction is consistent with evidence that patients whose disability is out of proportion to their medical condition tend to have failed in ordinary activities and to display a lack of social competence (e.g., Whitehead, Fedoravicius, Blackwell, & Wooley, 1979; Wooley et al., 1978). It should be noted that disability may be reinforced by avoidance of potentially aversive activities without any conscious intention by the individual to “use” illness to avoid these activities.
Individuals tend to value competence in some activities more than in others (Harter, 1988). The relevance of a particular domain of competence to the relation between symptoms and functional disability is likely to depend on the subjective importance of that domain of competence to the individual. For example, among individuals who do not value athletics, perceived athletic competence should be irrelevant to the relation between IBS symptoms and disability. In contrast, among individuals who value athletics, the relation between IBS symptoms and disability is likely to be greatest for those with the lowest perceived athletic competence, because they may benefit from avoidance of athletic activities in which they have a high likelihood of failure.
This study was designed to examine the extent to which competence moderates the relation between IBS symptoms and disability in adolescents and young adults with a childhood history of RAP. This sample was selected for study due to evidence that RAP in childhood may be a risk factor for later development of IBS. We examined competence in three domains as a potential moderator of the relation between IBS symptoms and disability. We predicted that, among adolescents and young adults who perceived their academic competence as low, higher levels of IBS symptoms would be associated with higher levels of disability; in contrast, among those who perceived their academic competence as high, higher symptom levels were not expected to be associated with greater disability. We predicted that this finding would pertain regardless of gender because perceived academic competence appears to be valued by both males and females (e.g., Salminen, 1994; Williams & White, 1983).
In addition, we examined the moderating effect of competence in two domains that may differ in their importance to adolescent girls and boys. Girls appear to place great value on social competence (e.g., Ford, 1982; Salminen, 1994; Williams & White, 1983). Thus, we expected that the relation between IBS symptoms and functional disability would be stronger for girls who perceived their social competence as low than for girls who perceived their social competence as high. The moderating effect of social competence on the relation between symptoms and disability was expected to be weaker for boys, because social competence is less important to boys than to girls and thus is less relevant in predicting the extent to which boys’ symptoms will be associated with disability.
Athletic competence, in contrast, tends to be of greater importance to boys than to girls (e.g., Kane, 1988; Salminen, 1994; Williams & White, 1983). Thus, we hypothesized that higher symptom levels would be associated with greater disability among boys who perceived their athletic competence as low but not among boys who rated their athletic competence as high. Among girls, athletic competence was not expected to be a significant moderator of the relation between symptoms and disability.
Method
Participants
Participants were 76 former pediatric patients (25 male, 51 female) who had been referred five years earlier to the Pediatric Gastroenterology Clinic of Vanderbilt University for evaluation of abdominal pain and had participated in a longitudinal study of recurrent abdominal pain (Walker, Garber, & Greene, 1993; Walker et ah, 1998). Subjects for this study met two criteria; (a) they reported abdominal pain for more than three months’ duration at the time of the initial clinic visit, and (b) the medical evaluation yielded no evidence of organic disease, IBS, or constipation. Patients ranged in age from 11 to 23 at the time of the follow-up assessment upon which the present study is based. At the time of the follow-up, participants had a mean age of 15.66 years, SD = 3.23.
Procedure
During the five-year period between the initial evaluation and the follow-up, annual holiday greetings were mailed to study participants, requesting address corrections if the family had moved. Approximately one month before the five-year anniversary of entry into the study, subjects were contacted by telephone and invited to participate in a follow-up interview by telephone. Subjects were assured of the confidentiality of their responses and were told that they would receive $10 for their participation. Of the 90 patients who completed the initial evaluation, 76 (84%) participated in the follow-up. Consent forms were sent to those subjects who agreed to participate. Trained interviewers contacted the subjects to schedule interviews when the conversations could be private. The interviewer read the items to the subjects and recorded their responses. Subjects were instructed to write down the response categories for structured questions prior to the start of the interview, so that these categories could be referenced when responding.
Measures
Symptoms of IBS.
Symptoms of IBS were assessed with eight questions that represent the “a priori descriptive symptoms” for IBS on the Bowel Disease Questionnaire (Talley, Phillips, Wiltgen, Zinsmeister, & Melton, 1990). Three questionnaire items were modified slightly to ensure participants’ understanding. For example, “After finishing a bowel movement do you often feel that there is still stool that needs to be passed?” was modified to “After finishing a bowel movement, do you often feel that there is still more that needs to be passed?” An IBS Symptom Index was computed by summing the number of symptoms endorsed, generating a score from 0 to 8 for each subject. The IBS symptoms assessed included lower or periumbilical pain, pain often relieved by bowel movement, more bowel movements with pain onset, frequent bloating with pain, mucus in stool, frequent feeling of incomplete evacuation; usual bowel pattern in the last year was described as constipation, diarrhea, or alternating constipation and diarrhea.
Functional Disability.
Functional disability (i.e., difficulty in physical and psychosocial functioning due to physical health) was assessed with the self-report form of the Functional Disability Inventory (FDI; Walker & Greene, 1991). The FD1 consists of 15 items referring to disability in the past 2 weeks. Sample items include “In the past two weeks, would you have had any physical trouble or difficulty doing something with a friend (for example, playing a game)?” and “In the past two weeks, would you have had any physical trouble or difficulty doing the activities in gym class or playing sports?” For participants who were working and not currently attending school, item 8 (difficulty being at school all day) was modified to “In the past two weeks, would you have had any physical trouble or difficulty being at your job all day?” Items are rated on a 5-point severity scale (no trouble, a little trouble, some trouble, a lot of trouble, impossible), and total scores are computed by summing the ratings. Walker and Greene (1991) reported high internal consistency for the FDI with coefficient alphas ranging from .85 to .92 and a 2-week test-retest reliability of .80 for pediatric patients with recurrent abdominal pain. In addition, validity of the FDI was demonstrated by moderate correlations with measures of school absence (r = .44, p < .001) and somatic symptoms (r = .45, p < .001).
Competence.
The patient’s perceived academic, social, and athletic competence was assessed with the corresponding subscales of the Self-Perception Profile for Adolescents (SPPA; Harter, 1988). Two statements are presented and the respondent is asked which statement is most like him or her and whether this statement is “sort of true” or “really true” for him or her. Each subscale contains six items; responses to these items are summed to obtain a total score. Sample items include “Some teenagers feel that they are socially accepted BUT other teenagers wish that more people their age accepted them,” and “Some teenagers do very well at all kinds of sports BUT other teenagers don’t feel that they are very good when it comes to sports.” The SPPA was selected because, although it was designed specifically for adolescents, it taps areas of perceived competence likely to be relevant not only for adolescents but also for young adults and thus allowed the use of the same instrument for the entire sample, For the young adults in the sample, interviewers substituted the word “people” for the word “teenagers” in reading the items to respondents, Harter (1988) reported coefficient alphas ranging from .77 to .91 for the academic competence scale, from .77 to .90 for the social competence scale, and from .86 to .92 for the athletic competence scale.
Results
Preliminary Analyses
Table I presents the bivariate correlation matrix for the continuous variables. Higher levels of IBS symptoms were associated with significantly higher levels of functional disability, r = .53, p < .01. Age was associated with significantly higher levels of IBS symptoms, r = .22, p < .05, and significantly higher levels of functional disability, r = .23, p < .05. The correlations between the IBS Symptom Index and measures of competence were negative and ranged in magnitude from −.25 to −.33. Correlations between the measures of competence and functional disability also were negative and ranged in magnitude from −.27 to −.49.
Table I.
Pearson’s Product-Moment Correlations among Variables
| Variable | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|
| 1. Age | – | .22* | .23* | −.23* | −.09 | −.19 |
| 2. IBS symptom index | – | .53** | −.33** | −.30** | −.25* | |
| 3. Functional disability | – | −.41** | −.49** | −.27* | ||
| 4. Academic competence | – | .38** | .29* | |||
| 5. Social competence | – | .44** | ||||
| 6. Athletic competence | – | |||||
p < .05.
p < .01.
T tests for independent samples were conducted to compare males and females on all variables. Results are presented in Table II. The only significant gender difference was for perceived athletic competence. Males reported significantly higher levels of athletic competence than did females, t(74) = 2.76, p < .01.
Table II.
Means and Standard Deviations for Males and Females on All Variables
| Males (n = 25) |
Females (n = 51) |
||||
|---|---|---|---|---|---|
| M | SD | M | SD | p | |
| Age | 15.68 | 3.05 | 15.65 | 3.35 | ns |
| IBS symptom index | 2.28 | 1.77 | 2.20 | 2.07 | ns |
| Functional disability | 5.60 | 9.81 | 7.61 | 8.98 | ns |
| Social competence | 15.16 | 3.63 | 15.00 | 3.09 | ns |
| Athletic competence | 14.08 | 3.74 | 11.57 | 3.72 | .01 |
| Academic competence | 13.92 | 4.16 | 13.47 | 3.59 | ns |
Stem and leaf plots and normal probability plots were examined and indicated that the data were normally distributed.
Overview of Regression Analyses
A series of hierarchical multiple regression analyses was conducted to examine the extent to which academic, social, and athletic competence moderated the relation between IBS symptoms and functional disability in boys and girls. Tests of moderation used the data analytic technique described by Baron and Kenney (1986) and Holmbeck (1997). Scores on the FDI constituted the dependent variable. In the first step of each regression equation, predictor variables included gender (dummy coded “0” for males and “1” for females), IBS symptoms, and a moderator variable (academic competence, social competence, or athletic competence). In the second step, two-way interaction terms were entered, including the interactions between IBS symptoms and gender, between IBS symptoms and a moderator variable, and between gender and a moderator variable. Finally, the three-way interaction among IBS symptoms, gender, and a moderator variable was entered on the third step of each equation. In these analyses evidence of perceived competence moderating the relation between IBS symptoms and functional disability would be obtained by observing significant interactions of the relevant competence variable and the IBS symptom variable in predicting functional disability. For academic competence, which was predicted to moderate the relation equally strongly for boys and girls, the simple two-way interaction of symptoms and competence was expected to obtain. However, for social and athletic competence, where the moderating effect of perceived competence was predicted to be stronger for girls and boys, respectively, a statistically significant three-way interaction, involving competence, IBS symptoms, and gender was expected.
Perceived Academic Competence
The first hierarchical multiple regression analysis investigated the extent to which academic competence moderated the relation between IBS symptoms and functional disability. Gender, IBS symptom scores, and scores on the academic competence subscale of the SPPA were entered in the first step of the equation, followed by two-way interaction terms on the second step, and the three-way interaction term on the third step. The final equation was significant, F(7, 68) = 7.17, p < .0001, R2 = .42. Table III depicts these results, As predicted, a significant two-way interaction emerged between levels of academic competence and levels of IBS symptoms. To examine the nature of the interaction effect, regression lines were plotted for subjects with high (+1 SD) and low (−1 SD) levels of academic competence. This interaction is illustrated in Figure 1. For adolescents and young adults who reported lower levels of academic competence, higher levels of IBS symptoms were associated with higher levels of functional disability. In contrast, for adolescents and young adults reporting higher levels of academic competence, levels of IBS symptoms were not predictive of levels of functional disability. The three-way interaction among academic competence, gender, and IBS symptoms was not significant.
Table III.
Multiple Regression Analysis Examining the Effect of Adolescent-Reported Academic Competence and IBS Symptoms on Functional Disability
| Predictor variable | β | T | R2 change |
|---|---|---|---|
| Step 1: predictor variables | .35** | ||
| Gender | .10 | 1.02 | |
| IBS symptoms | .45 | 4.43** | |
| Academic competence | −.26 | −.258** | |
| Step 2: two-way interactions | .07* | ||
| IBS symptoms × gender | −.29 | 1.19 | |
| Academic competence × IBS symptoms | −.72 | 2.34* | |
| Gender × academic competence | −.46 | 1.14 | |
| Step 3: three-way interaction | .00 | ||
| Academic competence × gender × IBS symptoms | −.07 | .09 | |
p < .05.
p < .001.
Figure 1.
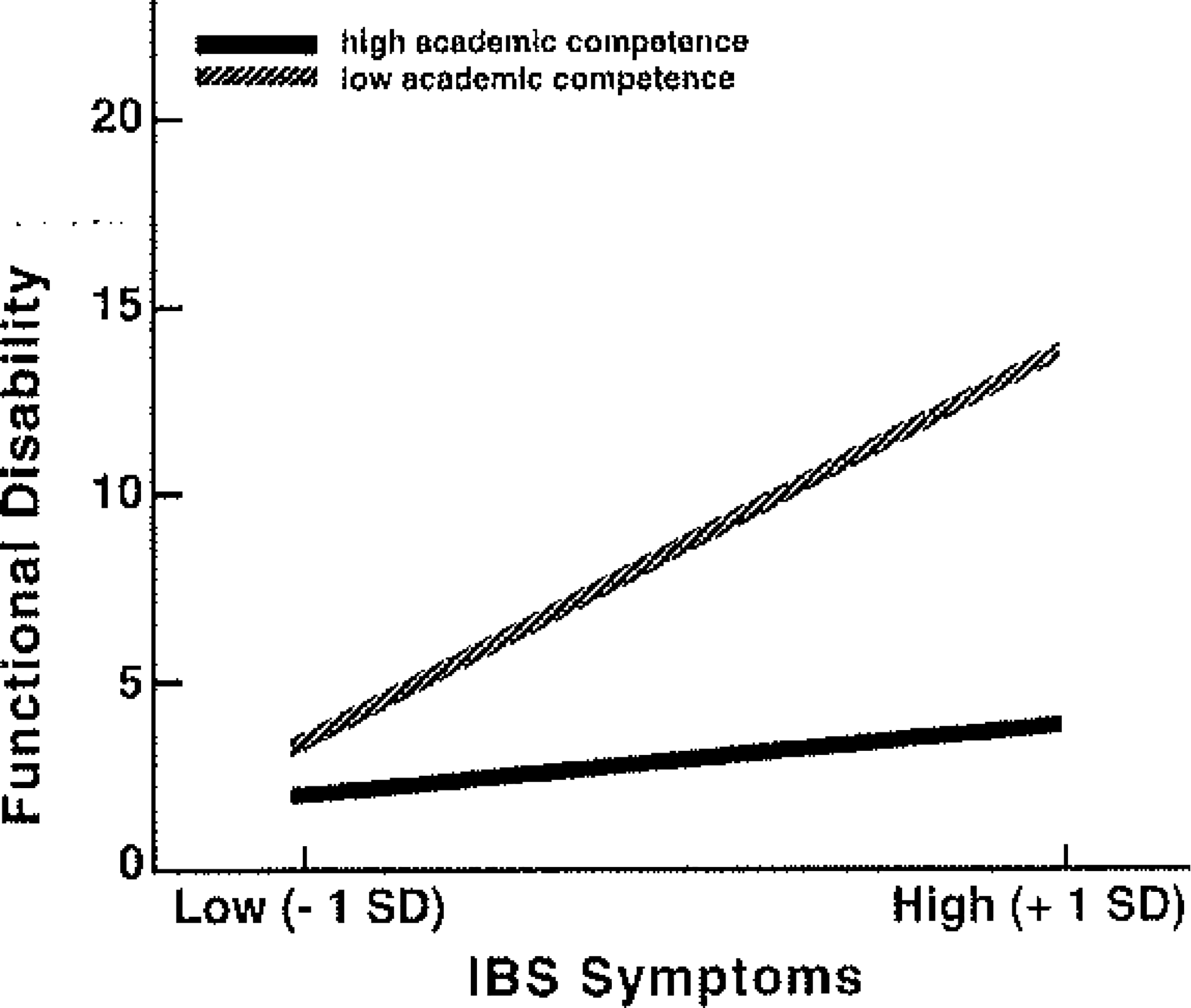
Estimated regression lines showing predicted Functional Disability Inventory (FDI) scores for subjects with low (−1 SD) and high (+1 SD) levels of academic competence on the Self-Perception Profile for Adolescents (SPPA). Graphed lines were plotted by selecting values one standard deviation above and below the mean for academic competence and IBS symptoms; these values were multiplied by their unstandardized regression coefficients to obtain values for plotting the predicted regression lines.
Perceived Social Competence
A second hierarchical multiple regression analysis examined whether social competence moderated the effect of IBS symptoms on functional disability. The resulting equation was significant, F(7, 68) = 10.75, p < .0001, R2 =.53. Table IV presents the results of each step of the analysis. As hypothesized, the three-way interaction among social competence, gender, and IBS symptoms was a significant predictor of functional disability. Regression lines were plotted for subjects with high (+1 SD) and low (−1 SD) levels of social competence to examine the nature of the interaction effect. These plots were done separately for males and females (see Figure 2). Among females with lower levels of social competence, higher levels of IBS symptoms were associated with higher levels of functional disability, hi contrast, for females with higher levels of social competence, the level of IBS symptoms did not significantly influence the level of functional disability, Among males, social competence did not significantly moderate the effect of IBS symptoms on functional disability; instead, males with higher levels of IBS symptoms reported greater functional disability regardless of their level of social competence.
Table IV.
Multiple Regression Analysis Examining the Effect of Adolescent-Reported Social Competence and IBS Symptoms on Functional Disability
| Predictor variable | β | T | R2 change |
|---|---|---|---|
| Step 1: predictor variables | .41** | ||
| Gender | .10 | 1.14 | |
| IBS symptoms | .43 | 4.51** | |
| Social competence | −.36 | −3.78** | |
| Step 2: two-way interactions | .09** | ||
| IBS symptoms × gender | −.02 | −.10 | |
| Social competence × IBS symptoms | −1.21 | −3.43** | |
| Gender × social competence | −.11 | −.26 | |
| Step 3: three-way interaction | .03* | ||
| Social competence × gender × SBS symptoms | −1.73 | −1.97* | |
p < .05.
p < .001.
Figure 2.
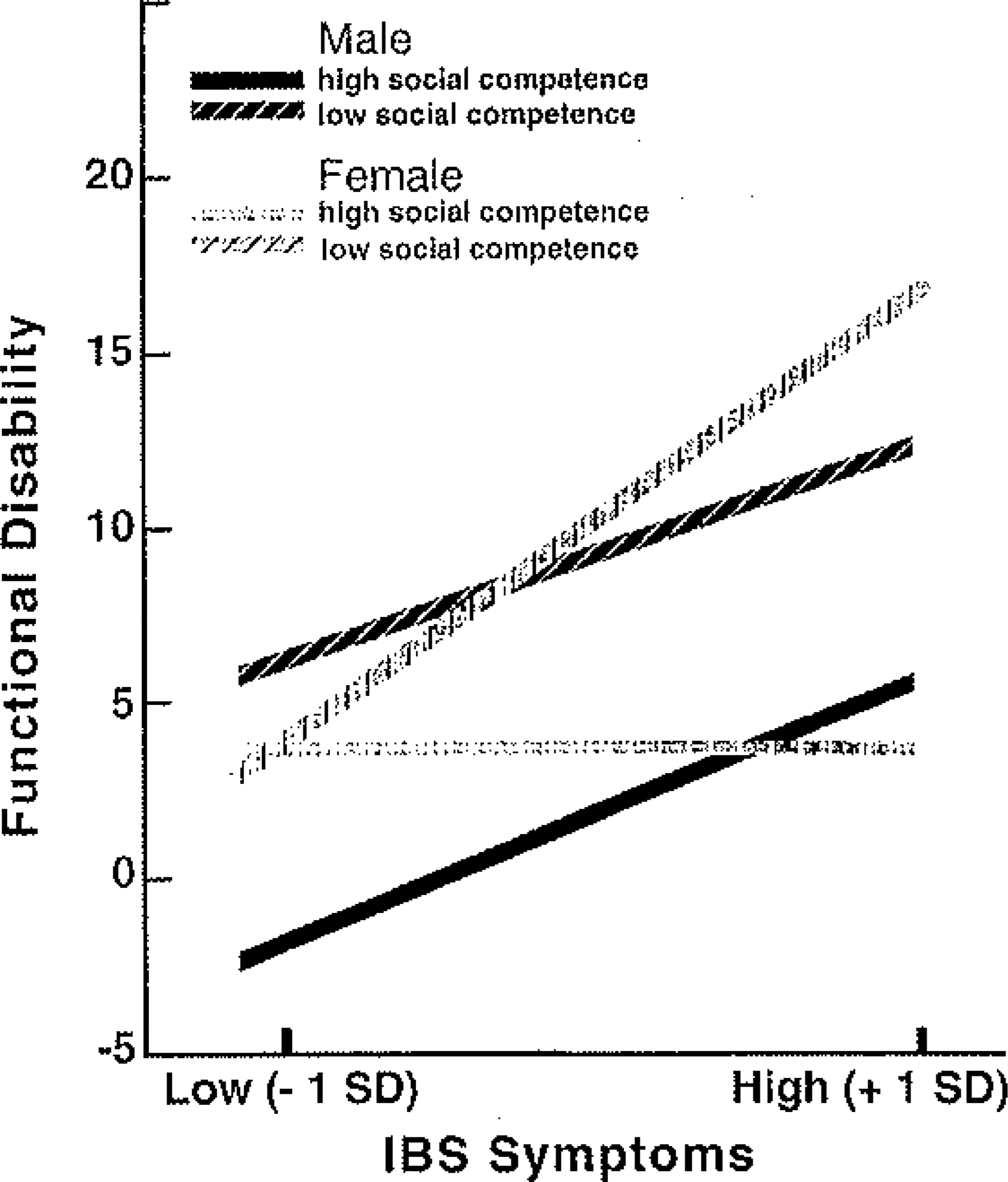
Estimated regression lines showing predicted Functional Disability Inventory (FDI) scores for subjects with low (−1 SD) and high (+1 SD) levels of social competence on the Self-Perception Profile for Adolescents (SPPA). For males and females separately, graphed lines were plotted by selecting values one standard deviation above and below die mean for social competence and IBS symptoms; these values were multiplied by their unstandardized regression coefficients to obtain values for plotting the predicted regression lines.
Perceived Athletic Competence
Finally, another regression analysis evaluated whether athletic competence moderated the relation between IBS symptoms and functional disability. The results indicated significant effects, F(7, 68) = 6.77, p < .0001, R2 = .41, and are presented in Table V, The three-way interaction among athletic competence, gender, and IBS symptoms was significant and is depicted in Figure 3. Among males with lower levels of athletic competence, higher levels of IBS symptoms were associated with higher levels of functional disability. In contrast, among males with higher levels of athletic competence, functional disability tended to be low and was not significantly predicted by level of symptoms, for females, higher levels of IBS symptoms were associated with significantly higher levels of functional disability regardless of level of athletic competence.
Table V.
Multiple Regression Analysis Examining the Effect of Adolescent-Reported Athletic Competence and IBS Symptoms on Functional Disability
| Predictor variable | β | T | R2 change |
|---|---|---|---|
| Step 1: predictor variables | .31** | ||
| Gender | .08 | .73 | |
| IBS symptoms | .50 | 4.92** | |
| Athletic competence | −.12 | −1.15 | |
| Step 2: two-way interactions | .06 | ||
| IBS symptoms × gender | .01 | .04 | |
| Athletic competence × IBS symptoms | .67 | 1.81 | |
| Gender × athletic competence | −.46 | −1.13 | |
| Step 3: three-way interaction | .05* | ||
| Athletic competence × gender × IBS symptoms | 1.72 | 2.35* | |
p < .05.
p < .001.
Figure 3.
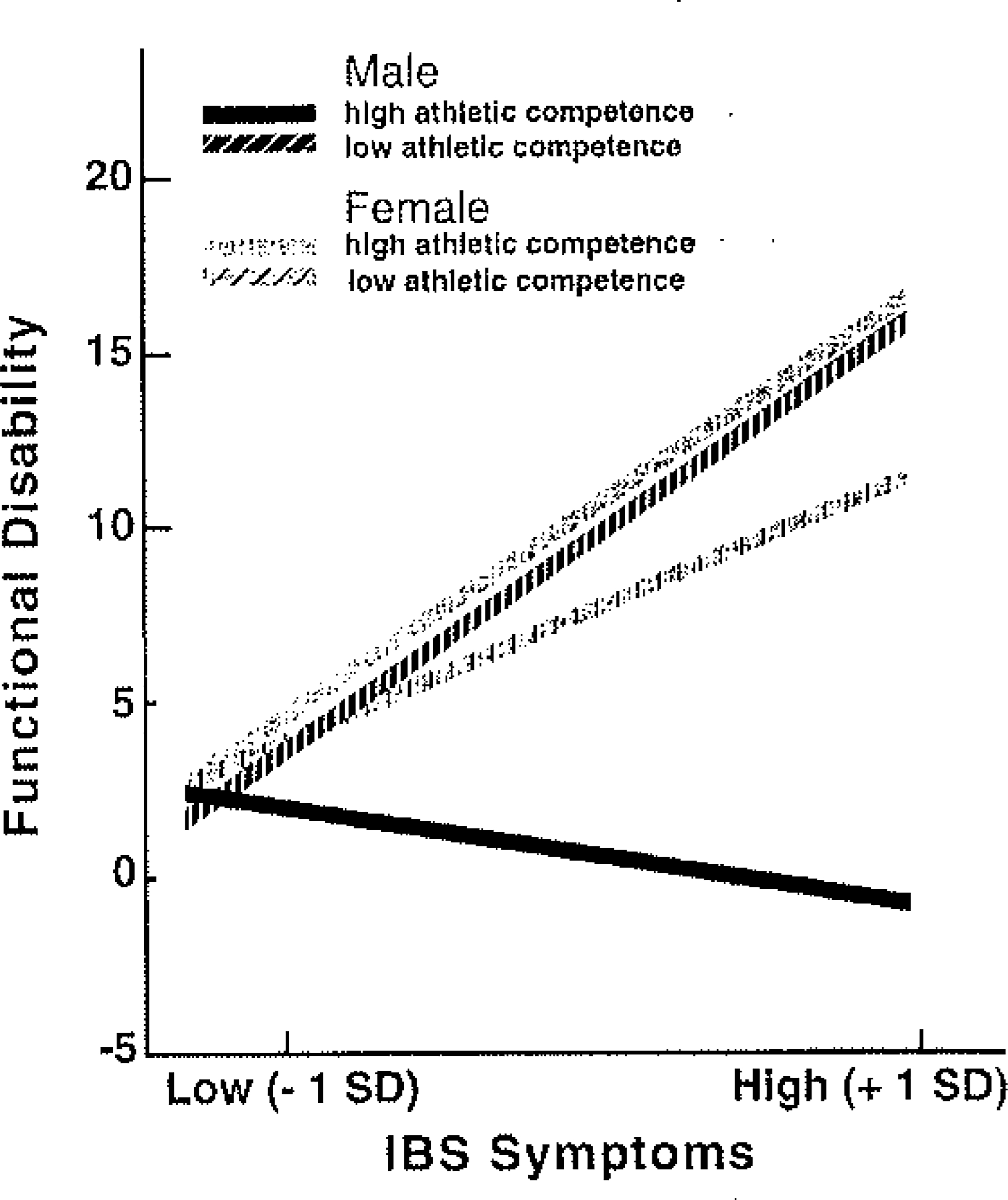
Estimated regression lines showing predicted Functional Disability Inventory (FDI) scores for subjects with low (−1 SD) and high (+1 SD) levels of athletic competence on the Self-Percept ion Profile for Adolescents (SPPA). For males and females separately, graphed lines were plotted by selecting values one standard deviation above and below the mean for athletic competence and IBS symptoms; these values were multiplied by their unstandardized regression coefficients to obtain values for plotting the predicted regression lines.
Discussion
A learning theory model of illness behavior (e.g., Wooley et al., 1978) suggests that illness behavior may be reinforced if it results in avoidance of activities in which the patient expects to fail. Individuals with low competence are likely to have greater prior experience of failure and higher current expectations for failure; thus, they may benefit from illness- related disability in that it results in avoidance of failure. In contrast, among individuals who perceive themselves as more competent, inability to participate in activities may be a punishing consequence of illness because it deprives them of opportunities for success. Thus, in comparison to less competent individuals, more competent individuals may exert greater effort to continue their activities despite illness. Consequently, the association between illness and sick role behavior such as functional disability should be greater among individuals with lower competence.
This hypothesis was examined in a sample of adolescents and young adults who, because of their childhood history of recurrent abdominal pain, were considered at risk for symptoms of irritable bowel syndrome as they reached adolescence and young adulthood. Results indicated that the relation between symptoms and disability was stronger for boys and girls with lower perceived academic competence than for those with higher perceived academic competence. Furthermore, among girls the relation between IBS symptoms and functional disability was stronger for those with lower perceived social competence than for those with higher perceived social competence. Finally, among boys, the relation between symptoms and disability was stronger for those with lower perceived athletic competence than for those with higher perceived athletic competence.
These findings are consistent with the hypothesis that illness behavior, such as functional disability, maybe reinforced among those whose disability permits avoidance of valued activities in which they perceive their competence to be inadequate. However, there are alternative ways in which symptoms, competence, and disability could be related that are consistent with these data. For example, individuals with more severe symptoms and disability may be limited in their ability to participate in academic, social, and athletic activities as a result of their pain and thus may become less competent or may develop perceptions of lower competence in these domains. Reductions in actual or perceived competence also might represent a stressor that further exacerbates symptoms. Thus, IBS symptoms, disability, and competence may influence each other in a reciprocal fashion. The nature of the relation among these variables could be further explored by intervention studies that improve functioning in one area, for example, competence, and examine the impact in other areas, such as symptoms and disability.
In future research on the relation between illness and disability, it will be important to expand the assessment of competence, In this study, the importance of each domain of competence was inferred from subjects’ gender, in keeping with previous research demonstrating that the importance of social and athletic competence varies by gender among adolescents (e.g., Ford, 1982; Salminen, 1994; Williams & White, 1983). This approach did not allow for the possibility that individuals within each gender may have differed in the extent to which a particular domain of competence was important; for example, for some girls athletic competence may have been quite important, and for some boys, social competence may have been particularly important. Another approach would be to have each subject rate the personal importance of each domain of competence.1 In addition, inclusion of observational as well as self-report measures of competence would allow evaluation of the extent to which both observed and perceived deficits in competence may influence illness-related functional disability.
Sample characteristics must be kept in mind when interpreting the results of this study. Participants had a childhood history of RAP and had previously sought medical treatment for their symptoms, Lowman, Drossman, Cramer, and McKee (1987) found that individuals who reported more medical visits for bowel symptoms as children were more likely to seek medical treatment for IBS symptoms in adulthood, They hypothesized that a history of abdominal pain and reinforcement of illness behavior in childhood may lead these individuals to respond to abdominal pain with increased symptom complaints and disability during adulthood, Thus, the former RAP patients who comprised the sample for this study may have been more likely than those without such a history to report functional disability in association with IBS symptoms, In addition, participants in the study tended to have low levels of IBS symptoms and were not available for medical evaluations; the observed relation among symptoms, disability, and competence may not extend to individuals with higher levels of symptomatology or to individuals with a medical diagnosis of IBS.
Furthermore, these results are based on a general rather than illness-specific measure of functional disability. The levels of functional disability reported on the Functional Disability inventory may include activity limitations due to symptoms other than IBS. In addition, the Functional Disability Inventory assesses disability in various domains but does not have separate subscales for academic, social, and athletic disability, it is possible that competence in each domain protects against disability specific to that domain, that is, disability particular to functioning in academic, social, and athletic arenas. Future work might use a more differentiated measure that assesses functional disability in these arenas. However, disability may overlap across domains, making it difficult to differentiate among academic, social, and athletic disability.
It has been suggested that physicians address psychosocial factors in addition to medical factors in order to enhance adaptation to IBS (e.g., Drossman, 1996; Drossman et al., 1988; van Dulmen et al., 1994). This study suggests that competence is one psychosocial factor that may warrant attention, as it may influence the extent to which IBS symptoms are associated with disability. Intervention studies might explore whether interventions to enhance patient competence in domains of personal importance would reduce the level of disability associated with IBS symptoms and whether interventions to reduce disability would enhance competence. Such interventions might be a useful adjunct to medical treatment. Future research also might be extended to an examination of the extent to which lower competence is linked with higher disability in illnesses ranging in severity from colds to chronic conditions such as asthma or diabetes. There are tremendous individual differences in the expression of illnesses (e.g., Mechanic, 1986). Our findings suggest that competence may be important in understanding these differences.
Acknowledgments
This study was based on Robyn E. Lewis’s master’s thesis. The research was supported by a grant from the National institute of Child Health and Human Development (HD23264).
Footnotes
The Self-Perception Profile for Adolescents (Harter, 1988) includes a form for respondents to rate the personal importance of each domain. We did not use this form, but it would be a useful addition to future research.
References
- Apley J (1975). The child with abdominal pains. Oxford: Basil Blackwell. [Google Scholar]
- Baron RM, & Kenny DA (1986). The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology, 51, 1173–1182. [DOI] [PubMed] [Google Scholar]
- Christensen MF, & Mortensen O (1975). Long-term prognosis in children with recurrent abdominal pain. Archives of Disease in Childhood, 50, 110–114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Corney RH, & Stanton R (1990). Physical symptom severity, psychology and social dysfunction in a series of outpatients with irritable bowel syndrome. Journal of Psychosomatic Research, 34, 483–491. [DOI] [PubMed] [Google Scholar]
- Drossman DA (1996). Editorial: Gastrointestinal illness and the biopsychosocial model. Journal of Clinical Gastroenterology, 22, 252–254. [DOI] [PubMed] [Google Scholar]
- Drossman DA, Li Z, Andruzzi E, Temple RD, Talley NJ, Thompson WG, Whitehead WE, Janssens J, Funch-Jensen P, Corazziari E, Richter JE, & Koch GG (1993). U.S, householder survey of functional gastrointestinal disorders: Prevalence, sociodemography and health impact. Digestive Diseases and Sciences, 38, 1569–1580. [DOI] [PubMed] [Google Scholar]
- Drossman DA, McKee DC, Sandler RS, Mitchell CM, Cramer EM, Lowman BC, & Burger AL (1988). Psychosocial factors in the irritable bowel syndrome. A multivariate study of patients and nonpatients with irritable bowel syndrome, Gastroenterology, 95, 701–708. [DOI] [PubMed] [Google Scholar]
- Drossman DA, Richter JE, Nicholas J, Talley W, Thompson G, Corazziari E, & Whitehead WE (1994). The functional gastrointestinal disorders and their diagnosis: A coming of age. In Drossman DA (Ed.), The functional gastrointestinal disorders: Diagnosis, pathophysiology, and treatment-A multinational consensus (pp. 1–23). Boston: Little, Brown. [Google Scholar]
- Ford ME (1982). Social cognition and social competence in adolescence. Developmental Psychology, 18, 323–340. [Google Scholar]
- Harter S (1988). Manual for the Self-Perception Profile for Adolescents. Denver, CO: University of Denver. [Google Scholar]
- Holmbeck GN (1997). Toward terminological, conceptual, and statistical clarity in the study of mediators and moderators: Examples from the child-clinical and pediatric psychology literatures. Journal of Consulting and Clinical Psychology, 65, 599–610. [DOI] [PubMed] [Google Scholar]
- Hyams JS, Treem WR, Justinich CJ, Davis P, Shoup M, & Burke G (1995). Characterization of symptoms in children with recurrent abdominal pain: Resemblance to irritable bowel syndrome. Journal of Pediatric Gastroenterology and Nutrition, 20, 209–214. [DOI] [PubMed] [Google Scholar]
- Kane MJ (1988). The female athletic role as a status determinant within the social systems of high school adolescents. Adolescence, 23, 253–264. [PubMed] [Google Scholar]
- Latimer PR (1983). Functional gastrointestinal disorders: A behavioral medicine approach. New York: Springer. [Google Scholar]
- Lowman BC, Drossman DA, Cramer EM, & McKee DC (1987). Recollection of childhood events in adults with irritable bowel syndrome. Journal of Clinical Gastroenterology, 9, 324–330. [DOI] [PubMed] [Google Scholar]
- McGrath PA (1990). Pain in children: Nature, assessment, treatment. New York: Guilford Press. [Google Scholar]
- Mechanic D (1986). The concept of illness behavior: Culture, situation, and personal predisposition. Psychological Medicine, 16, 1–7. [DOI] [PubMed] [Google Scholar]
- Naliboff B, & Mayer EA (1996). Sensational developments in the irritable bowel. Gut, 39, 770–771. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Salminen S (1994). Sex-roles and values of school children using self-esteem as a moderating factor. Adolescence, 29, 875–884. [PubMed] [Google Scholar]
- Sandler RS (1990). Epidemiology of irritable bowel syndrome in the United States. Gastroenterology, 99, 409–415. [DOI] [PubMed] [Google Scholar]
- Talley NJ, Phillips SE, Wiltgen CM, Zinsmeister AR, & Melton LJ (1990). Assessment of functional gastrointestinal disease: The Bowel Disease Questionnaire. Mayo Clinic Procedures, 65, 1456–1479. [DOI] [PubMed] [Google Scholar]
- Thompson WG, Creed F, Drossman DA, Heaton K, & Mazzacca G (1994). Functional bowel disorders and functional abdominal pain. In Drossman DA (Ed.), The functional gastrointestinal disorders: Diagnosis, pathophysiology, and treatment-A multinational consensus (pp, 115–173). Boston: Little, Brown. [Google Scholar]
- Thomson S, & Dancey CP (1996). Symptoms of irritable bowel in school children: Prevalence and psychosocial effects, Journal of Pediatric Health Care, 10, 280–285. [DOI] [PubMed] [Google Scholar]
- van Dulmen AM, Fennis JFM, Mokkink HGA, van der Velden HGM, & Vleijenberg G (1994). Doctors’ perception of patients’ cognitions and complaints in irritable bowel syndrome at an out-patient clinic, Journal of Psychosomatic Research, 38, 581–590. [DOI] [PubMed] [Google Scholar]
- Walker LS, Garber J, & Greene JW (1993). Psychosocial correlates of recurrent childhood pain: A comparison of pediatric patients with recurrent abdominal pain, organic illness, and psychiatric disorders, Journal of Abnormal Psychology, 102, 248–258. [DOI] [PubMed] [Google Scholar]
- Walker LS, & Greene JW (1991). The Functional Disability Inventory: Measuring a neglected dimension of child health status, Journal of Pediatric Psychology, 16, 39–58. [DOI] [PubMed] [Google Scholar]
- Walker LS, Guite JW, Duke M, Barnard JA, & Greene JW (1998). Recurrent abdominal pain: A potential precursor of irritable bowel syndrome in adolescents and young adults, Journal of Pediatrics, 132,. 1010–1015. [DOI] [PubMed] [Google Scholar]
- Whitehead WE, Bosmajian L, Zonderman AB, Costa PT Jr., & Schuster MM (1988). Symptoms of psychologic distress associated with irritable bowel syndrome. Comparison of community and medical clinic samples. Gastroenterology, 95, 709–714. [DOI] [PubMed] [Google Scholar]
- Whitehead WE, Crowell MD, Bosmajian L, Zonderman A, Costa PT Jr., Benjamin C, Robinson JC, Heller BR, & Schuster MM (1990). Existence of irritable bowel syndrome supported by factor analysis of symptoms in two community samples. Gastroenterology, 98, 336–340, [DOI] [PubMed] [Google Scholar]
- Whitehead WE, Fedoravicius AS, Blackwell B, & Wooley S (1979). A behavioral conceptualization of psychosomatic illness: Psychosomatic symptoms as learned responses. In McNamara JR (Ed), Behavioral approaches to medicine: Application and analysis New York: Plenum. [Google Scholar]
- Williams JM, & White KA (1983). Adolescent status systems for males and females at three age levels. Adolescence, 70, 381–389. [Google Scholar]
- Wooley SC, Blackwell B, & Winget C (1978). A learning theory model of chronic illness behavior: Theory, treatment, and research. Psychosomatic Medicine, 40, 379–401. [DOI] [PubMed] [Google Scholar]