

Abstract
Fibroblast growth factor receptor 1 (FGFR1) has recently been identified as a promising novel therapeutic target and prognostic marker in different types of cancer. In the present study, a meta-analysis was performed to clarify the correlation between FGFR1 and the survival outcomes of head and neck squamous cell carcinoma (HNSCC) patients. PubMed, Embase, and Web of Science were systematically searched for relevant studies in order to explore the prognostic significance of FGFR1 in HNSCC. Hazards ratios (HR) and 95% confidence intervals (CI) were collected to estimate the correlation between overexpression and amplification of FGFR1 and survival outcomes of HNSCC patients. Nine studies including 2708 patients with HNSCC were finally selected for the meta-analysis. The results indicated that FGFR1 predicted poor overall survival (OS) (HR, 1.97; 95% CI, 1.49–2.61, P<0.001) in HNSCC patients. Futhermore, FGFR1 was related to poor OS in human papillomavirus (HPV) negative HNSCC not in HPV positive HNSCC patients. Subgroup analysis stratified by molecular abnormalities, such as overexpression or amplification showed the similar results. The present study demonstrated that HNSCC patients with FGFR1 overexpression and amplification were more likely to exhibit poorer survival.
Introduction
Head and neck squamous cell carcinoma (HNSCC) develop from the mucosal linings of the upper aerodigestive tract, comprising 1) the nasal cavity and paranasal sinuses, 2) the nasopharynx, 3) the hypopharynx, larynx, and trachea, and 4) the oral cavity and oropharynx. Squamous cell carcinoma (SCC) is the most frequent malignant tumor of the head and neck region. Although the group of malignancies arise from different sites of head and neck region, they have similar pathogenesis, staging system, therapeutic strategy, and prognosis. Therefore, it is rational to classify them into one category, HNSCC [1]. HNSCC accounts for approximately 3% of new cancer cases annually and is the fifth most common cancer in the world [2,3]. Despite the successful development of treatment methods, such as surgery, chemotherapy, immunotherapy and radiation, the five-year survival rate of HNSCC patients is estimated to be between 40 and 50% [4]. SCC accounts for more than 95% of these cancers, while their molecular and clinical characteristics are heterogeneous [4–6]. The lack of significant improvement in the survival rates of HNSCC patients with the current treatment methods has led to a search for new prognostic biomarkers and therapeutic targets [7,8].
The fibroblast growth factor receptor (FGFR) family comprises four main receptors (FGFR1-4), which are structurally associated with the corresponding receptor tyrosine kinases. FGFRs are involved in several cellular processes including angiogenesis, wound healing, tissue repair and tumorigenesis [9,10]. Substantial evidence further indicates that genomic driver aberrations, such as mutations, amplifications and translocations may cause a dysregulation in the FGF-FGFR pathway and play an important role in tumor development [11]. Molecular abnormalities and overexpression of FGFR1 have been associated with poor outcomes and have been described in lung carcinomas [12], breast cancer [13], pancreatic cancer [14], oral squamous carcinoma [15] and esophageal squamous cell carcinomas [16]. Moreover, human papillomavirus (HPV) status is known to be associated with both FGFR1 expression/amplification and survival outcomes in HNSCC [17,18].
However, the direct impact of FGFR1 expression and amplification on HNSCC patient survival remains inconclusive due to the variance in the sample size and the experimental design of the studies performed. In the present study, the databases of PubMed, Embase and Web of Science were searched for relevant publications and a meta-analysis was performed. The objective was to assess the association between FGFR1 and the survival outcomes in HNSCC patients.
Materials and methods
Search strategy
We searched for articles published between 2000 and 2020. The complete literature search was conducted in June 2020 in accordance with Dickersin et al [19]. The search was performed throughout specific databases, including PubMed, Web of Science and EMBASE. The search terms included the following: (FGFR1 or fibroblast growth factor receptor 1) and (prognosis OR outcome OR recurrence OR survival OR mortality OR progression) and (head and neck or oral or laryngeal or tonsil or oropharyngeal or oropharynx) and (cancer or squamous cell carcinoma). Furthermore, the reference lists of the retrieved studies were evaluated manually to identify potential pertinent publications.
Selection criteria
The inclusion criteria of the meta-analysis were the following: 1) patients diagnosed with HNSCC; 2) association between the overexpression and amplification of FGFR1 and overall survival (OS); and 3) the language of publications that was confined to English. 4) Sufficient statistical analysis was required, including hazard ratios (HR) and the 95% confidence interval (CI) and HR with prognostic endpoints, or data that could be used to estimate the HR and 95% CI, or other outcomes for OS such as Kaplan- Meier survival curves. The exclusion criteria were the following: 1) studies without sufficient data for meta-analysis; 2) abstracts, reviews, letters and case reports; and 3) studies with non-specific data regarding HNSCC or FGFR1. In case the same cohort was reported by several publications, the most recent publication was included in the meta-analysis.
Data extraction
First, we inspected the repeatability, and removed the repeated papers. Then, titles and abstracts of the papers were perused carefully. Finally, reading all enrolled full articles carefully again to confirm the exactly appropriate studies. Two investigators independently evaluated the literature against the inclusion and exclusion criteria (LQ Zhou and Y Hu). Discordance in assessments were resolved by discussion with a third investigator (LS Ai). The authors of the studies were contacted by e-mail to request additional information or data for meta-analytic calculations. The Newcastle-Ottawa Scale (NOS) [20,21] was used to assess the qualities of the included publications, which uses a star system (maximum is nine stars) to evaluate a study in the three following domains: selection of participants, comparability of study groups and the ascertainment of outcomes of interest. Scores of NOS of ≥6 were considered as high-quality studies. A detailed description about how we scored each study was shown in S1 Table. The Recommendations for Tumor Marker Prognostic Studies (REMARK) was also used to access the qualities of the included studies [22]. The REMARK checklist consists of 20 items to report for published tumor marker prognostic studies.
The following information was extracted from the studies: author, year, country, cancer type, sample size, age, follow-up, method, cox proportional hazards model, survival analysis, HR, NOS score, REMARK score and OS (OS was detected from the medical treatment until the last follow-up or the time of death of the patient).
Statistical analysis
The HR and the 95% CI were obtained directly from the primary publications or estimated by p values and other published data following Parmer’s methods [23]. Statistical heterogeneity among the included studies was analyzed by the χ2-based Q test and the I2 test [24]. The radom-effect model was applied in our meta—analysis, however, the estimation of between-study variance might not be precise [25,26]. Moreover, subgroup analysis was conducted to explore the source of heterogeneity. Sensitivity analysis was also performed to investigate the influence of each individual study on the overall pooled results. The Begg’s and Egger’s tests were used to evaluate the publication bias. All statistical analyses were performed with STATA statistical software version 12.0 (StataCorp Lp).
Results
Selection and characteristics of the included studies
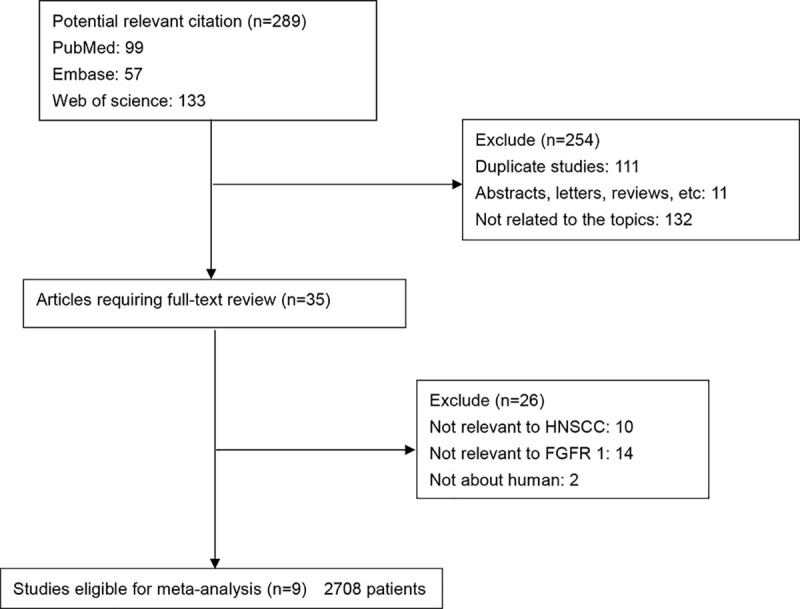
A total of 289 potential records were initially identified by searching the electronic databases (Fig 1). Following exclusion of the duplicates (n = 111), reviews, abstracts and letters (n = 11) and the studies not related to the topics (n = 132), the remaining studies (n = 35) were further evaluated by reading their full texts. A total of 26 studies did not provide specific data regarding HNSCC or FGFR1 and therefore were excluded. Finally, nine studies between 2013 and 2020 with a total 2708 HNSCC patients were included in the present meta-analysis.
Fig 1. Flow diagram of the selection of relevant studies included in the meta-analysis.
The characteristics of the included studies were summarized (Table 1), such as author, year, country, cancer type, sample size, age, follow-up, method, HPV infection, cox proportional hazards model, survival analysis, HR, NOS score and REMARK score. These studies were from France, Netherlands, USA, Australia, Brazil, South Korea and Poland, including three for laryngeal squamous cell carcinoma (LSCC), two for oral tongue squamous cell carcinomas (OTSCC), three for head and neck squamous cell carcinoma (HNSCC), one for oropharyngeal squamous cell carcinoma (OPSCC) and one for oral cavity squamous cell carcinoma (OCSCC), one for hypopharyngeal squamous cell carcinoma (HPSCC). Seven publications included >100 patients and two publications enrolled <100 patients. Nine studies including a total of 2708 patients reported OS. The HR and 95% CI were directly reported in eight studies and were estimated in one study in the original literature. The NOS score was >6 in eight studies. The REMARK score is between 9–16.
Table 1. Characteristics of the studies examined in the meta-analysis.
| Author | Year | Country | Cancer type | Sample size | Age | Follow-up(months) | Method | HPV infection | Cox proportional hazards model | Survival analysis | HR | NOS score | REMARK score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Dubot [18] | 2018 | FRANCE | HNSCC | 122 | 56(22–78) | 60 | Targeted NGS | Yes | Multivariate | OS | Reported | 7 | 15 |
| Koole 1 [17] | 2016 | Netherlands | HNSCC | 452 | 56(35–80) | 68 | IHC | Yes | Multivariate | OS,DFS | Reported | 8 | 16 |
| Monico [27] | 2018 | USA | LSCC | 74 | NR | 180 | ddPCR | NR | Multivariate | OS | Reported | 6 | 12 |
| Young [33] | 2013 | Australia | OTSCC | 123 | 59(21–93) | 61.2 | FISH | NR | NO | OS,PFS | Reported | 5 | 9 |
| Koole 2 [32] | 2016 | Netherlands | OCSCC | 512 | 62(24–94) | 78.5 | IHC | Yes | Multivariate | OS | Reported | 6 | 16 |
| Koole 3 [32] | 2016 | Netherlands | OPSCC | 439 | 58(35–59) | 57 | IHC | Yes | Multivariate | OS | Reported | 6 | 16 |
| Mariz [28] | 2019 | Brazil | OTSCC | 85 | 55.5(19–89) | NR | IHC | NR | Multivariate | OS,DFS | Reported | 6 | 11 |
| Starska [29] | 2018 | Poland | LSCC | 137 | 61.9(45–83) | NR | Western blotting | NR | Multivariate | OS,DFS | Reported | 6 | 12 |
| Kim 1 [34] | 2020 | South Korea | LSCC | 155 | 64(30–88) | 38.8 | FISH,IHC | NR | Univariate | OS,DFS | Reported | 7 | 12 |
| Kim 2 [34] | 2020 | South Korea | HPSCC | 54 | 64(30–88) | 38.8 | FISH,IHC | NR | Univariate | OS,DFS | Reported | 7 | 12 |
| Goke [30] | 2013 | USA | HNSCC | 555 | 62 | NR | FISH | YES | NO | OS | Estimated | 6 | 10 |
NR, not reported; NOS, Newcastle-Ottawa Quality Scale; REMARK, Recommendations for Tumor Marker Prognostic Studies; HPV, human papillomavirus; Targeted NGS, targeted next generation sequencing; IHC, immunohistochemistry; ddPCR, droplet digital PCR; FISH, fluorescence in situ hybridization.
Association between FGFR1 and survival of HNSCC patients
Nine studies in the present analysis examined the association between FGFR1 and the survival of patients with HNSCC. The combined results of these studies indicated overexpression and amplification of FGFR1 were associated with poor OS (HR, 1.97; 95% CI, 1.49–2.61, P<0.001). Low heterogeneity was noted (I2 = 34.6%, Pheterogeneity = 0.122) (Fig 2).
Fig 2. Forest plot indicating the association between overexpression/amplification of FGFR1 and OS in HNSCC.
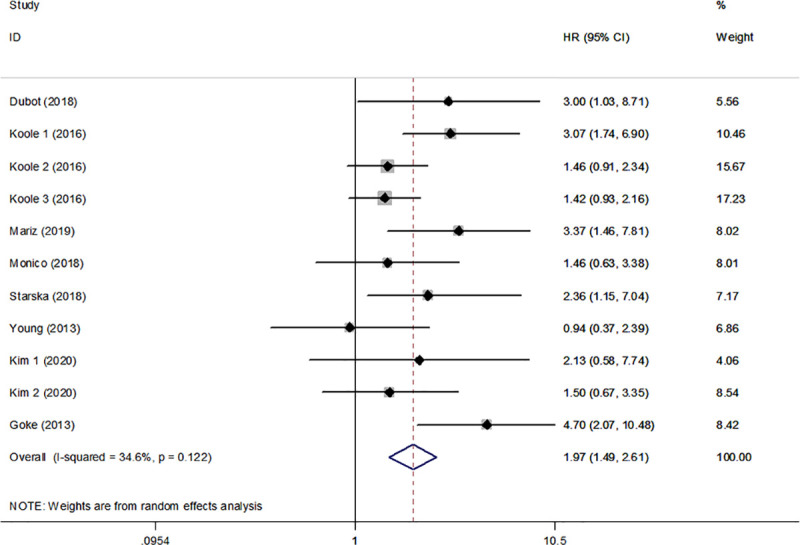
FGFR1, fibroblast growth factor receptor 1; OS, overall survival; HNSCC, head and neck squamous cell carcinoma.
Subgroup analysis for OS was also performed and was stratified according to FGFR1 overexpression and amplification. The summarized HR for FGFR1 overexpression was 1.86 (95% CI, 1.37–2.53, P<0.001) and for the FGFR1 amplification 2.11 (95% CI, 1.16–3.86, P<0.001) (Fig 3). Low heterogeneity was noted between the FGFR1 overexpression and OS, medium heterogeneity was noted between the FGFR1 amplification and OS. (I2 = 28.2%, Pheterogeneity = 0.224; I2 = 48.6%, Pheterogeneity = 0.100, respectively). Furthermore, FGFR1 was related to poorer OS in HPV negative HNSCC (HR, 1.70; 95% CI, 1.16–2.49, P<0.05) (Fig 4).
Fig 3. Subgroup analysis for OS was performed following stratification by FGFR1 overexpression and amplification.
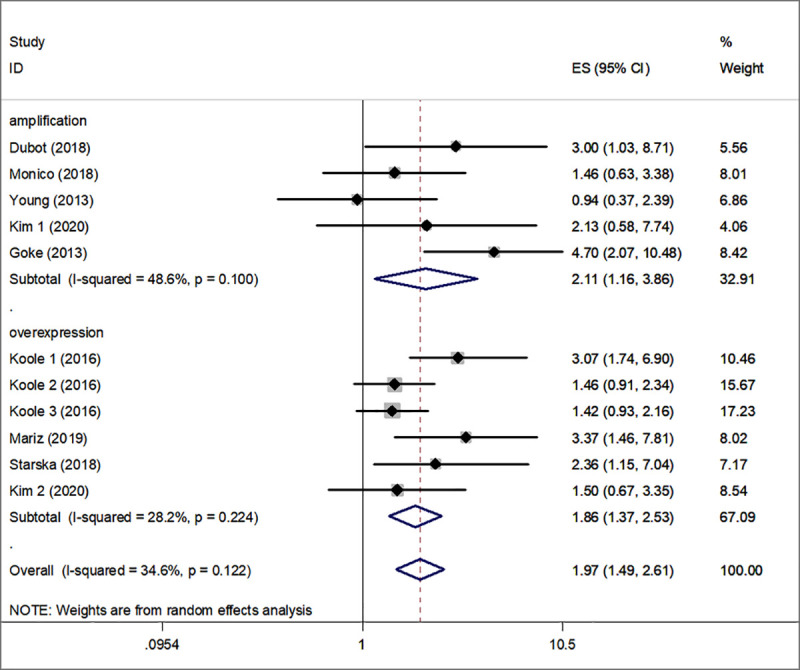
FGFR1, fibroblast growth factor receptor 1; OS, overall survival.
Fig 4. Subgroup analysis for OS was performed following stratification by HPV infection.
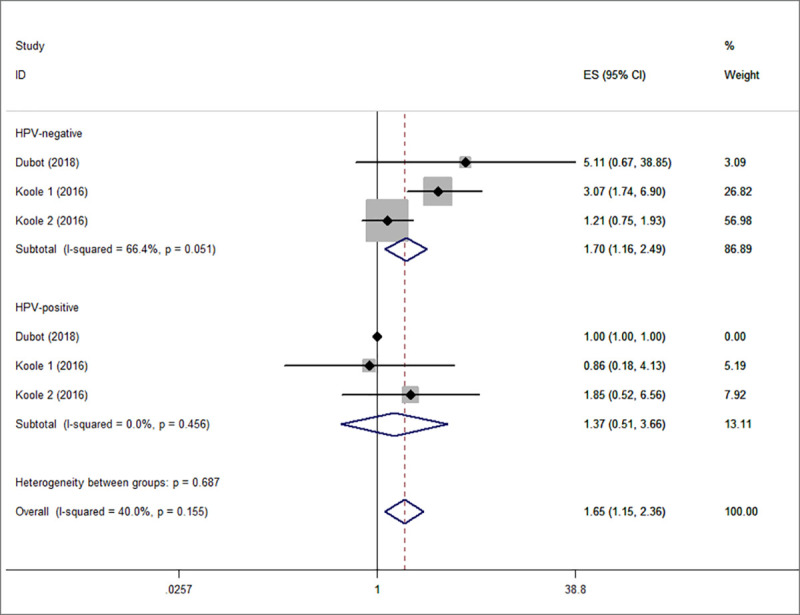
OS, overall survival; HPV, human papillomavirus.
Sensitivity analysis
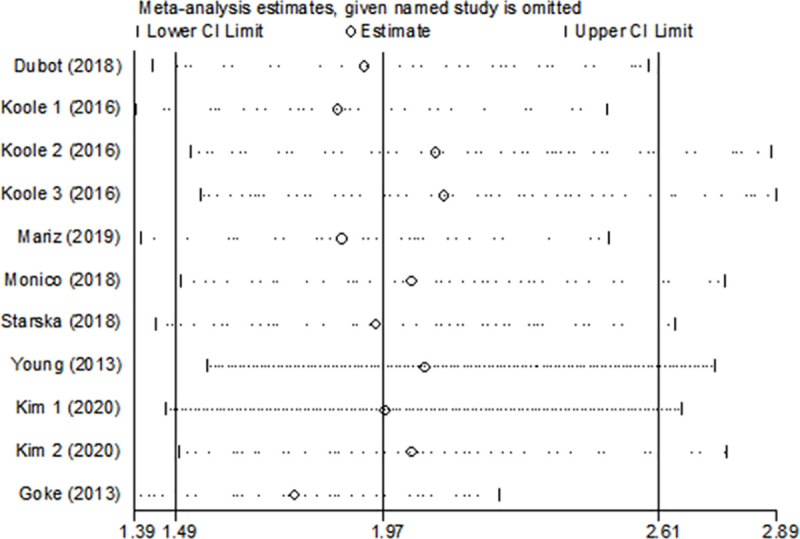
The sensitivity analyses were conducted to evaluate the effects of each single study on the overall effect. The analysis did not detect a study that could alter significantly the combined results (Fig 5). The results of the sensitivity indicated that the pooled effect size of the meta-analysis results was stable and reliable.
Fig 5. The sensitivity analyses were conducted to evaluate the effects of each single study on the overall effect.
Publication bias
The publication bias was assessed by the Begg’s funnel plots and the Egger’s test in the present study. The results were quite symmetric, indicating that the analysis did not include publication bias among the studies (P = 0.187) (Fig 6).
Fig 6. Publication bias of the enrolled analysis.
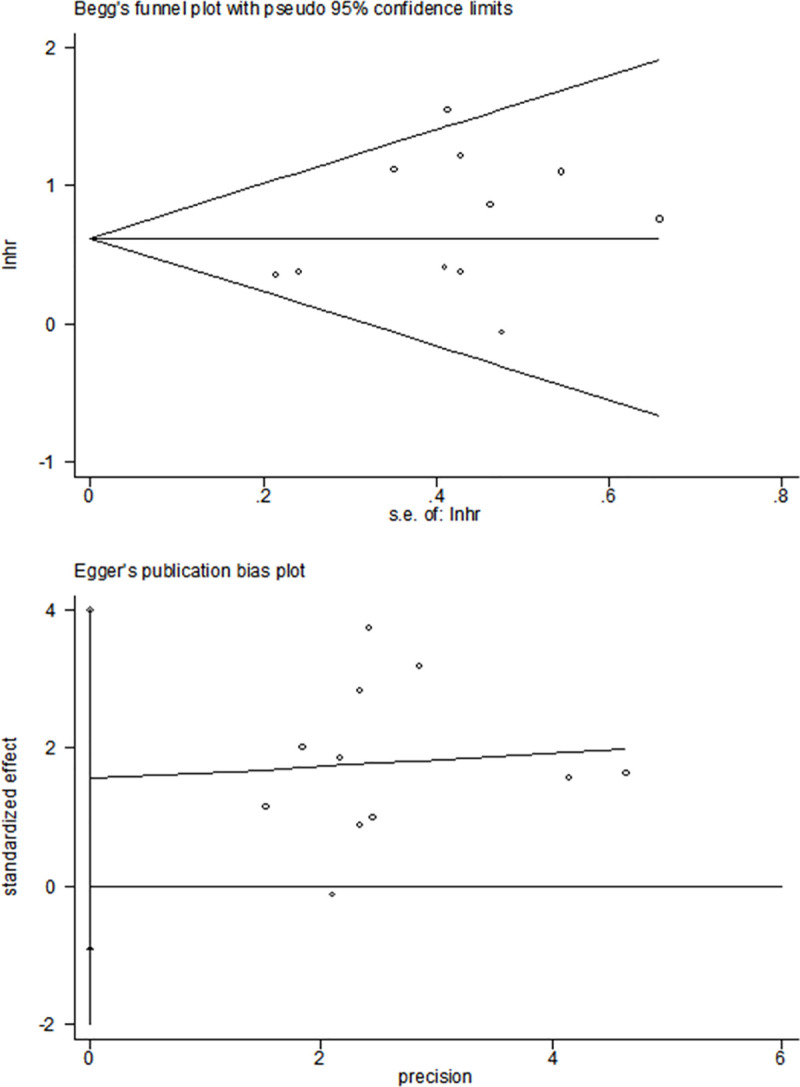
The publication bias was accessed using the Begg’s funnel plots and the Egger’s test.
Discussion
Numerous studies have focused on the identification of new prognostic markers that can be used for cancer monitoring and detection. An association between FGFR1 and poor prognosis has been shown in various types of HNSCC [27–29]. Goke et al reported that FGFR1 amplification was a frequent event in primary and metastatic HNSCC and that it could be used as a poor prognostic indicator [30]. Dubot et al demonstrated that FGFR1 amplification was associated with lower survival and that it could be used as a prognostic biomarker for patients with HNSCC [18]. Hase et al, Young et al and Koole et al reported that FGFR1 was associated with poor outcome of HNSCC [17,31–33]. Kim et al recently found that FGFR1 amplification may serve as an independent prognostic factor for DFS in hypopharyngeal and laryngeal squamous cell carcinoma [34]. Our results are consistent with these results. However, Ipenburg et al reported FGFR1 gene amplification and FGFR1 protein expression are not of value as prognostic biomarkers in HNSCC in a review, [35]. The results are contrast with ours, but the evidence on FGFR1 in HNSCC is limited to only very few studies in Ipenburg’s study. These results are not comparable, due to the patient population and heterogeneous designs. The present study is the first meta-analysis including nine published studies with 2708 patients to provide useful information for clinical decision-making in HNSCC. The results indicated that overexpression and amplification of FGFR1 significantly predicted poor OS in HPV negative HNSCC patients.
A recent study reported that 7.1% of all tumor types exhibited genetic alterations and that FGFR1 was involved in almost 50% of these alterations [36,37]. A significant association between disease prognosis and FGFR1 expression was noted in various cancer patients and the studies suggested that FGFR1 was an independent prognostic factor [13,38]. The exact mechanism underlying the association of FGFR1 with cancer incidence has not been clearly elucidated. Recently, numerous studies have shown that FGFR1 can promote tumour progression and development by regulating signaling pathways and inducing cancer cell survival, proliferation and tumour angiogenesis [39,40]. Therefore, FGFR1 overexpression may be used as a marker of tumorigenesis and inflammation and as a poor prognostic indicator of cancer patients.
Targeted therapies have produced striking benefits for patients with cancer. FGFRs are not constitutively active in nonmalignant cells due to their transmembrane proteins that contain intrinsic enzymatic activities. Therefore, FGFRs are preferable targets of other therapeutic modalities and small-molecule inhibitors, such as ligand traps and antibody-based agents can inhibit FGFR signaling with therapeutic efficacy in cancer patients [41,42]. Certain types of cancers, such as endometrial uterine cancer, breast cancer [13], urothelial carcinoma [43] and lung cancer [44] have been shown to be responsive to FGFR-mediated tumour therapy. Clinical trials have provided proof that FGFR kinase inhibitors are effective therapeutic agents used in specific cancer types. According to the results of the present study, the FGFR inhibitors may hold a therapeutic potential against HNSCC.
However, the present meta-analysis contains several limitations. First, the numbers of articles used for assessing the association between FGFR1 and the prognosis of HNSCC were limited in the present meta-analysis. Therefore, additional studies are required to produce accurate conclusions. In addition, according to Begg’s funnel plots and the Egger’s test, the publication bias was not significant. Second, studies containing languages other than English and the inclusion of unpublished data may contribute to additional bias. Third, the results may be heterogeneous due to the utilization of different methods and statistical analysis. Forth, our results may be an overestimate of the prognostic significance of FGFR1 to some extent due to the majority of the included studies reporting positive results. Finally, one of the records included in the systematic review did not report the HR directly. Therefore, the extrapolated HR might be less reliable compared with reported statistics.
In summary, the present meta-analysis included electronic databases and a total of 2708 patients from nine studies. The results demonstrated that patients with overexpression and amplification of FGFR1 were more likely to exhibit poor prognosis. Taken together, the meta-analysis results suggest that FGFR1 possesses a prognostic value for HNSCC. However, additional studies with larger sample sizes are required to acquire more representative and precise findings.
Supporting information
(DOC)
(DOCX)
(DOCX)
Data Availability
All relevant data are within the manuscript and its Supporting Information files.
Funding Statement
The authors received no specific funding for this work.
References
- 1.Stransky N., et al., The mutational landscape of head and neck squamous cell carcinoma. Science, 2011. 333(6046): p. 1157–60. 10.1126/science.1208130 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Audet N., et al., Lymphatic vessel density, nodal metastases, and prognosis in patients with head and neck cancer. Arch Otolaryngol Head Neck Surg, 2005. 131(12): p. 1065–70. 10.1001/archotol.131.12.1065 [DOI] [PubMed] [Google Scholar]
- 3.Hussey D.H., Latourette H.B., and Panje W.R., Head and neck cancer: an analysis of the incidence, patterns of treatment, and survival at the University of Iowa. Ann Otol Rhinol Laryngol Suppl, 1991. 152: p. 2–16. 10.1177/00034894911000s401 [DOI] [PubMed] [Google Scholar]
- 4.Leemans C.R., Braakhuis B.J., and Brakenhoff R.H., The molecular biology of head and neck cancer. Nat Rev Cancer, 2011. 11(1): p. 9–22. 10.1038/nrc2982 [DOI] [PubMed] [Google Scholar]
- 5.Seiwert T.Y., et al., Integrative and comparative genomic analysis of HPV-positive and HPV-negative head and neck squamous cell carcinomas. Clin Cancer Res, 2015. 21(3): p. 632–41. 10.1158/1078-0432.CCR-13-3310 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.van Kempen P.M., et al., Differences in methylation profiles between HPV-positive and HPV-negative oropharynx squamous cell carcinoma: a systematic review. Epigenetics, 2014. 9(2): p. 194–203. 10.4161/epi.26881 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Conley B.A., Treatment of advanced head and neck cancer: what lessons have we learned? J Clin Oncol, 2006. 24(7): p. 1023–5. 10.1200/JCO.2005.05.0682 [DOI] [PubMed] [Google Scholar]
- 8.Noorlag R., et al., Nodal metastasis and survival in oral cancer: Association with protein expression of SLPI, not with LCN2, TACSTD2, or THBS2. Head Neck, 2015. 37(8): p. 1130–6. 10.1002/hed.23716 [DOI] [PubMed] [Google Scholar]
- 9.Powers C.J., McLeskey S.W., and Wellstein A., Fibroblast growth factors, their receptors and signaling. Endocr Relat Cancer, 2000. 7(3): p. 165–97. 10.1677/erc.0.0070165 [DOI] [PubMed] [Google Scholar]
- 10.Hughes S.E., Differential expression of the fibroblast growth factor receptor (FGFR) multigene family in normal human adult tissues. J Histochem Cytochem, 1997. 45(7): p. 1005–19. 10.1177/002215549704500710 [DOI] [PubMed] [Google Scholar]
- 11.Dieci M.V., et al., Fibroblast growth factor receptor inhibitors as a cancer treatment: from a biologic rationale to medical perspectives. Cancer Discov, 2013. 3(3): p. 264–79. 10.1158/2159-8290.CD-12-0362 [DOI] [PubMed] [Google Scholar]
- 12.Miao J.L., et al., Fibroblast Growth Factor Receptor 1 Gene Amplification in Nonsmall Cell Lung Cancer. Chin Med J (Engl), 2016. 129(23): p. 2868–2872. 10.4103/0366-6999.194649 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Andre F., et al., Targeting FGFR with dovitinib (TKI258): preclinical and clinical data in breast cancer. Clin Cancer Res, 2013. 19(13): p. 3693–702. 10.1158/1078-0432.CCR-13-0190 [DOI] [PubMed] [Google Scholar]
- 14.Lehnen N.C., et al., Fibroblast growth factor receptor 1 gene amplification in pancreatic ductal adenocarcinoma. Histopathology, 2013. 63(2): p. 157–66. 10.1111/his.12115 [DOI] [PubMed] [Google Scholar]
- 15.Freier K., et al., Recurrent FGFR1 amplification and high FGFR1 protein expression in oral squamous cell carcinoma (OSCC). Oral Oncol, 2007. 43(1): p. 60–6. 10.1016/j.oraloncology.2006.01.005 [DOI] [PubMed] [Google Scholar]
- 16.Wang D., et al., Association of fibroblast growth factor receptor 1 gene amplification with poor survival in patients with esophageal squamous cell carcinoma. Oncotarget, 2017. 8(51): p. 88857–88869. 10.18632/oncotarget.21486 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Koole K., et al., FGFR1 Is a Potential Prognostic Biomarker and Therapeutic Target in Head and Neck Squamous Cell Carcinoma. Clin Cancer Res, 2016. 22(15): p. 3884–93. 10.1158/1078-0432.CCR-15-1874 [DOI] [PubMed] [Google Scholar]
- 18.Dubot C., et al., Comprehensive genomic profiling of head and neck squamous cell carcinoma reveals FGFR1 amplifications and tumour genomic alterations burden as prognostic biomarkers of survival. Eur J Cancer, 2018. 91: p. 47–55. 10.1016/j.ejca.2017.12.016 [DOI] [PubMed] [Google Scholar]
- 19.Dickersin K., Scherer R., and Lefebvre C., Identifying relevant studies for systematic reviews. Bmj, 1994. 309(6964): p. 1286–91. 10.1136/bmj.309.6964.1286 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Stang A., Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol, 2010. 25(9): p. 603–5. 10.1007/s10654-010-9491-z [DOI] [PubMed] [Google Scholar]
- 21.Gláucia F.C., et al., The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomized studies. 2013. [Google Scholar]
- 22.Sauerbrei W., et al., Reporting Recommendations for Tumor Marker Prognostic Studies (REMARK): An Abridged Explanation and Elaboration. J Natl Cancer Inst, 2018. 110(8): p. 803–811. 10.1093/jnci/djy088 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Parmar M.K., Torri V., and Stewart L., Extracting summary statistics to perform meta-analyses of the published literature for survival endpoints. Stat Med, 1998. 17(24): p. 2815–34. [DOI] [PubMed] [Google Scholar]
- 24.Higgins J.P., et al., Measuring inconsistency in meta-analyses. Bmj, 2003. 327(7414): p. 557–60. 10.1136/bmj.327.7414.557 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Borenstein M., et al., A basic introduction to fixed-effect and random-effects models for meta-analysis. Res Synth Methods, 2010. 1(2): p. 97–111. 10.1002/jrsm.12 [DOI] [PubMed] [Google Scholar]
- 26.Tufanaru C., et al., Fixed or random effects meta-analysis? Common methodological issues in systematic reviews of effectiveness. Int J Evid Based Healthc, 2015. 13(3): p. 196–207. 10.1097/XEB.0000000000000065 [DOI] [PubMed] [Google Scholar]
- 27.Monico J., et al., Fibroblast growth factor receptor 1 amplification in laryngeal squamous cell carcinoma. PLoS One, 2018. 13(1): p. e0186185. 10.1371/journal.pone.0186185 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Mariz B., et al., FGF-2 and FGFR-1 might be independent prognostic factors in oral tongue squamous cell carcinoma. Histopathology, 2019. 74(2): p. 311–320. 10.1111/his.13739 [DOI] [PubMed] [Google Scholar]
- 29.Starska K., et al., Fibroblast growth factor receptor 1 and 3 expression is associated with regulatory PI3K/AKT kinase activity, as well as invasion and prognosis, in human laryngeal cancer. Cell Oncol (Dordr), 2018. 41(3): p. 253–268. 10.1007/s13402-017-0367-z [DOI] [PubMed] [Google Scholar]
- 30.Goke F., et al., Fibroblast growth factor receptor 1 amplification is a common event in squamous cell carcinoma of the head and neck. Mod Pathol, 2013. 26(10): p. 1298–306. 10.1038/modpathol.2013.58 [DOI] [PubMed] [Google Scholar]
- 31.Hase T., et al., Correlation of basic fibroblast growth factor expression with the invasion and the prognosis of oral squamous cell carcinoma. J Oral Pathol Med, 2006. 35(3): p. 136–9. 10.1111/j.1600-0714.2006.00397.x [DOI] [PubMed] [Google Scholar]
- 32.Koole K., et al., FGFR Family Members Protein Expression as Prognostic Markers in Oral Cavity and Oropharyngeal Squamous Cell Carcinoma. Mol Diagn Ther, 2016. 20(4): p. 363–74. 10.1007/s40291-016-0204-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Young R.J., et al., Frequency of fibroblast growth factor receptor 1 gene amplification in oral tongue squamous cell carcinomas and associations with clinical features and patient outcome. Oral Oncol, 2013. 49(6): p. 576–81. 10.1016/j.oraloncology.2013.01.006 [DOI] [PubMed] [Google Scholar]
- 34.Kim E.K., et al., Prognostic implications of Fibroblast growth factor receptor 1 (FGFR1) gene amplification and protein overexpression in hypopharyngeal and laryngeal squamous cell carcinoma. BMC Cancer, 2020. 20(1): p. 348. 10.1186/s12885-020-06792-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Ipenburg N.A., et al., Fibroblast Growth Factor Receptor Family Members as Prognostic Biomarkers in Head and Neck Squamous Cell Carcinoma: A Systematic Review. Target Oncol, 2016. 11(1): p. 17–27. 10.1007/s11523-015-0374-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Harding M.J. and Nechiporuk A.V., Fgfr-Ras-MAPK signaling is required for apical constriction via apical positioning of Rho-associated kinase during mechanosensory organ formation. Development, 2012. 139(17): p. 3130–5. 10.1242/dev.082271 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Helsten T., et al., The FGFR Landscape in Cancer: Analysis of 4,853 Tumors by Next-Generation Sequencing. Clin Cancer Res, 2016. 22(1): p. 259–67. 10.1158/1078-0432.CCR-14-3212 [DOI] [PubMed] [Google Scholar]
- 38.Konecny G.E., et al., Second-line dovitinib (TKI258) in patients with FGFR2-mutated or FGFR2-non-mutated advanced or metastatic endometrial cancer: a non-randomised, open-label, two-group, two-stage, phase 2 study. Lancet Oncol, 2015. 16(6): p. 686–94. 10.1016/S1470-2045(15)70159-2 [DOI] [PubMed] [Google Scholar]
- 39.Jiao J., et al., FGF1-FGFR1 axis promotes tongue squamous cell carcinoma (TSCC) metastasis through epithelial-mesenchymal transition (EMT). Biochem Biophys Res Commun, 2015. 466(3): p. 327–32. 10.1016/j.bbrc.2015.09.021 [DOI] [PubMed] [Google Scholar]
- 40.Turner N. and Grose R., Fibroblast growth factor signalling: from development to cancer. Nat Rev Cancer, 2010. 10(2): p. 116–29. 10.1038/nrc2780 [DOI] [PubMed] [Google Scholar]
- 41.Touat M., et al., Targeting FGFR Signaling in Cancer. Clin Cancer Res, 2015. 21(12): p. 2684–94. 10.1158/1078-0432.CCR-14-2329 [DOI] [PubMed] [Google Scholar]
- 42.Katoh M., Therapeutics Targeting FGF Signaling Network in Human Diseases. Trends Pharmacol Sci, 2016. 37(12): p. 1081–1096. 10.1016/j.tips.2016.10.003 [DOI] [PubMed] [Google Scholar]
- 43.Hahn N.M., et al., A Phase II Trial of Dovitinib in BCG-Unresponsive Urothelial Carcinoma with FGFR3 Mutations or Overexpression: Hoosier Cancer Research Network Trial HCRN 12–157. Clin Cancer Res, 2017. 23(12): p. 3003–3011. 10.1158/1078-0432.CCR-16-2267 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Lim S.H., et al., Efficacy and safety of dovitinib in pretreated patients with advanced squamous non-small cell lung cancer with FGFR1 amplification: A single-arm, phase 2 study. Cancer, 2016. 122(19): p. 3024–31. 10.1002/cncr.30135 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
(DOC)
(DOCX)
(DOCX)
Data Availability Statement
All relevant data are within the manuscript and its Supporting Information files.