

Summary
Multiple sclerosis (MS) is a chronic autoimmune disease of the central nervous system. Lower urinary tract dysfunction due to MS includes a dysfunction of the storage phase or dysfunction of the voiding phase or a detrusor-sphincter dyssynergia. Baseline evaluation includes a voiding chart, an ultrasound scan of the urinary tract, urine culture, and an urodynamic study. For storage symptoms, antimuscarinics are the first-line treatment, and clean intermittent catheterization (CIC) is indicated if there is concomitant incomplete bladder emptying. Intradetrusor injections with botulinum toxin A (BTX-A), are recommended for refractory cases. Urinary diversion is rarely indicated. For patients with voiding symptoms, CIC and alpha-blockers are usually offered. Sexual dysfunction in patients with MS is multifactorial. Phosphodiesterase type 5 inhibitors are first-line therapies for MS-associated erectile dysfunction in both male and female patients. This review summarizes the epidemiology, pathogenesis, risk factors, genetic, clinical manifestations, diagnostic tests, and management of MS. Lastly, the urologic outcomes and therapies are reviewed.
Keywords: multiple sclerosis, urology, lower urinary tract dysfunction, neurogenic bladder
1. Introduction
Multiple sclerosis (MS), the most prevalent neurological disability, is an autoimmune-mediated disorder that affects the central nervous system (CNS) and often leads to severe physical or cognitive incapacitation as well as neurological problems in young adults (1). It is traditionally viewed as a two-stage disease, with early inflammation responsible for relapsing-remitting disease and delayed neurodegeneration causing non-relapsing progression. MS is more common in females. There is a genetic influence on MS susceptibility; about one in eight patients have a family history of MS. The main genetic risk associated with MS resides in HLA -DRB1*15 (2). Approximately, 2.5 million individuals are affected worldwide, and young individuals aged between 20 and 40 years are mainly affected. MS is regarded as a T cell-mediated autoimmune disorder with a predominance of CD8-positive T cells (CD8+) cells compared with other T-cell subsets, B cells or plasma cells (3). The McDonald's diagnostic criteria for MS routinely undergo revisions aligning the criteria with advancements in imaging technologies. Diagnosis is based on parameters such as medical history and neurological exam, as well as paraclinical parameters such as magnetic resonance imaging (MRI), cerebrospinal fluid showing oligoclonal banding, and evoked potentials. MRI remains the most sensitive tool available for determining events that meet diagnostic criteria for dissemination in time and space. The prevalence of MS is highest in North America, Western Europe and Australasia (> 100 cases per 100,000 population), and lowest in countries centered around the equator (< 30 cases per 100,000 population) (4).
Effective management requires a multifaceted approach to control acute attacks, manage progressive worsening, and remediate bothersome or disabling symptoms associated with this illness. The emergence of higher-efficacy drugs requiring less frequent administration has made these preferred options in terms of tolerability and adherence (5). The goals of therapy with disease-modifying agents in patients with MS include shortening the duration of acute exacerbations, decreasing their frequency, and providing symptomatic relief. It is common practice to treat acute relapses of MS with a short course of a corticosteroid (6). For newly diagnosed treatment-naive patients, multiple therapies are indicated and could include the injected medications (interferons (IFN), glatiramer acetate (GA)), oral therapies (fingolimod, dimethyl fumarate (DMF) and teriflunomide), and even monoclonal antibodies (ocrelizumab, natalizumab, and, alemtuzumab). In patients who have ongoing disease activity despite treatment with so-called platform therapies (interferons, GA, or teriflunomide) switching to therapies that may be more effective (fingolimod, DMF, ocrelizumab, natalizumab and alemtuzumab) might result in better control of relapsing disease activity (7). Based on the mechanisms of action and efficacy and safety profiles of these drugs, for most patients, one of the two treatment approaches is normally used. The first approach, which focuses on safety, is escalation and starts with lower risk disease-modifying therapies (DMTs) and shifting to higher risk treatment if disease activity occurs. The second approach, which prioritizes efficacy, is induction, in which a strong immune intervention is used from diagnosis of disease. Several factors have a role in treatment decisions for individual patients with MS, including disease activity, patient characteristics, treatment burden, and cost (8).
Although the genitourinary consequences of MS are rarely life-threatening, they can cause significant morbidity and patient frustration. The majority of patients with MS have symptoms ranging from urgency, urge incontinence, and frequency to urinary retention (9). Most patients with progressive MS will develop voiding dysfunction. Although there are many treatment options for patients with neurogenic bladders, therapy must remain conservative and initially reversible because symptoms from MS tend to wax and wane over time (10). The location of MS plaques will profile unique features of lower urinary tract dysfunction (LUTD). Lesions of the relevant suprapontine or spinal pathways regulating the lower urinary tract functions affect the storage phase, resulting in reduced bladder capacity and detrusor overactivity. The patient might report varying degrees of urinary urgency, frequency, nocturia, and incontinence (overactive bladder (OAB) symptoms). Injury to the suprasacral spinal pathways also results in loss of coordinated activation of the detrusor and inhibition of the urethral sphincter during voiding. Instead, there is a simultaneous contraction of the detrusor and urethral sphincter, known as detrusor-sphincter dyssynergia (DSD). Lesions of the sacral cord or infrasacral pathways result in voiding dysfunction associated with poorly sustained or absent detrusor contractions and/or non-relaxing sphincter (11). Nearly 90% of patients with MS experience some degree of voiding dysfunction and/or incontinence. LUTD rarely presents as the primary MS manifestation and usually appears 6-8 years after the initial diagnosis. There is a paucity of trials that guide treatment of urologic dysfunction in MS patients. Usually, a multidisciplinary team composed of general practitioners, rehabilitation specialists and neurologists, and urologists can properly manage those patients. The management of bladder dysfunction is individually tailored according to the pattern of LUTD (12). Management of LUTD focuses, primarily, on improvement of patients' symptoms and quality of life and, secondarily, on the preservation of the upper urinary tract and avoidance of urological complications. First-line treatments include fluid management, pelvic floor muscle training (PFMT), and medical therapies (antimuscarinic agents), and second-line treatments include Botulinum toxin A (Botox) intradetrusor injections, intravesical therapies, invasive and non-invasive neuromodulation, and catheterization (13).
We performed a narrative review to discuss briefly the epidemiology, pathogenesis, risk factors, genetic contribution, clinical course, diagnosis, and treatment of MS. The urologist had a crucial role in the management of urologic manifestations of patients with MS. We reviewed the current literature regarding the urological outcomes and management of patients with MS.
2. Overview of MS
2.1. Epidemiology of MS
MS is the most frequently demyelinating disease, with a prevalence that varies considerably, from high levels in North America and Europe (> 100/100,000 inhabitants) to low rates in Eastern Asia and sub-Saharan Africa (2/100,000 population) (14). The highest prevalence rates have been estimated for the age group 35-64 years for both sexes and all countries (15). In 2016, there were 2,221,188 prevalent cases of MS globally, which corresponded to a 10.4% (9.1 to 11.8%) increase in age-standardized prevalence since 1990. It was demonstrated that a strong latitude gradient for the prevalence of MS has occurred, with an increase in prevalence of 1.03 times per degree of latitude. A north to south decrease in prevalence by latitude gradient has been recognized in North America and Western Europe (16).
2.2. Pathogenesis of MS
Over the years, MS has been considered to be an autoimmune disorder where myelin-specific T cells initiate an inflammatory process that results in CNS demyelination. These autoreactive T cells are activated in the periphery and upregulate adhesion molecules that allow these T cells to interact with and cross the blood-brain-barrier and finally establish an inflammatory response directed against myelin (17). Within the CNS, these T cells re-encounter specific antigens and set up an inflammatory process that resembles delayed-type hypersensitivity, dominated by lymphocytes and microglia. Various immunological effector mechanisms are initiated, which include cytotoxic T-cell proliferation, antibody production, and activation of microglia. The myelin-oligodendroctye unit is damaged, saltatory conduction breaks down and the symptoms of MS follow (18). In recent years, it has become more evident that axonal damage is the major morphological substrate of permanent clinical disability of MS patients. There was a significant correlation shown between the extent of axon damage and the numbers of CD8-positive cytotoxic T cells and macrophages/ microglia (19). The role of the B-lymphocytes (B cells) in MS pathogenesis is also important. It contributes twofold. First, as autoreactive B cells, they produce autoantibodies, secrete cytokines, clonally replicate memory B cells, and long-living plasma cells, which serve to advance the disease state by their constant production of autoantibodies. Second, as antigen-presenting cells, they activate autoreactive T cells (20).
Insulin-like growth factor I (IGF-I) promotes myelin production by oligodendrocytes. IGF-I and type 1 IGF receptors (IGF1R) are upregulated at the edges of the demyelinated plaque. It has been shown that oligodendrocytes within MS lesions have reduced IGF1R expression. The ablation of brain IGF1R prevents remyelination in this animal model (21). Immature oligodendroglia in areas of demyelination exhibited increased expression of the IGF-1 receptor during early recovery. Since IGF-1 is an essential factor involved in proper myelinogenesis and neurotrophic effects, this molecule holds potential for applications aimed at repairing tissue in MS (22).
In-depth analysis of spinal cord molecular neuropathology in MS patients was found that areas of incomplete demyelination extend a distance away from plaque borders and are characterized by a TGF-beta 1 (transforming growth factor-beta 1) progliotic signature. Based on the identification of astrocytes vs. oligodendrocyte gene co-expression networks, it was proposed that TGF-beta 1, while preventing acute inflammation, could promote gliosis and alter the translation of myelin genes (23). Also, TGF-β plays a vital role in the development and function of CD4+ regulatory T cells (Tregs). It was found that TGF-β receptor II expression was reduced in MS patients' CD4 T cells. It is well-documented that there is a defect in the Treg population in MS patients, so modulation of TGF-β signaling may be used to correct this defect (24). It is believed that T helper 17 cells (Th17 cells), along with Th1 cells, play a role in MS pathogenesis, which, if not crucial, is at least significant. A majority of CD4+ T cells in acute MS lesions produce IL-17A and hence can be classified as Th17 cells. Certain types of MS, such as opticospinal MS, have a dominant signature of Th17-driven pathology, including a large proportion of granulocytes among CNS-infiltrating cells (25).
Damage to axons is taken as a key factor for disability in MS, but its pathogenesis is largely unknown. Axonal injury is believed to occur as a consequence of demyelination and was recently shown to be a feature even of the early disease stage. Axonal injury is, therefore, at least in part, independent of demyelinating activity, and its pathogenesis may be different from demyelination (26). The factors that contribute to the pathogenesis of MS are summarized in Figure 1.
Figure 1.
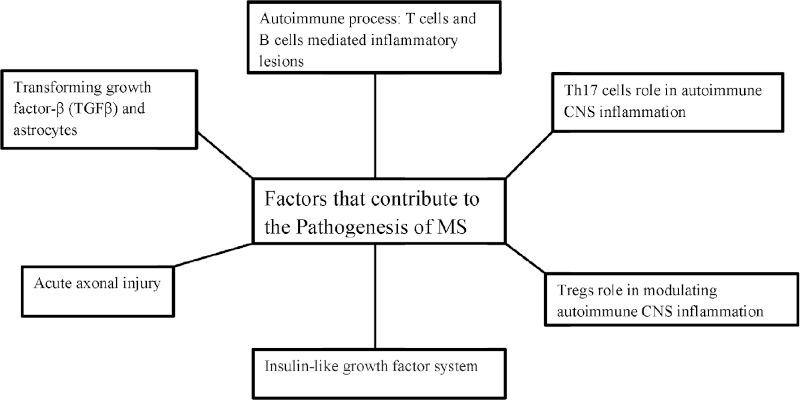
The Pathogenesis of MS. MS, multiple sclerosis; Tregs, Regulatory CD4+ T cells; CNS, central nervous system.
2.3. Risk factors of MS
Vitamin D deficiency, the season of birth, Epstein Barr virus (EBV) infection, and smoking behavior are strongly implicated and able to influence genetic predisposition to MS. Furthermore, these factors appear to act synergistically and the risk of MS in individuals exposed to more than one factor combines (27). The strongest known risk factor for MS is infection with EBV. Compared with uninfected individuals, the hazard of developing MS is approximately 15-fold higher among individuals infected with EBV in childhood and about 30-fold higher among those infected with EBV in adolescence or later in life. There is growing evidence that vitamin D insufficiency is a risk factor for conversion from clinically isolated syndrome to MS and MS progression (28). There is strong evidence that pregnancy does not worsen long-term prognosis despite an increased risk of relapses in the early postpartum period. Exclusive breastfeeding (no supplemental feedings for at least 2 months) reduces this risk of postpartum relapses, whereas nonexclusive breastfeeding appears to have no effect. Obesity or obesity-related comorbidities have been associated with worse outcomes among people with MS (29). It has been suggested that alcohol consumption was associated with mood disorders, disability, and even onset of MS, but a common theme is lacking (30). Physical and emotional stressors continue to be studied as potential MS risk factors. Important issues to be considered are the definitions of stress used, and the period of exposure thought to be relevant. Evidence for the role of emotional stress in MS etiology was weak, but left open the possibility that emotional stressors could be causal factors (31).
2.4. Genetic contribution to MS
The largest and first identified genetic risk factor for MS is an allele from the major histocompatibility complex (MHC) class II HLA-DRB1 gene, HLA-DRB1*15:01, which increases the risk about threefold. The HLA-DRB1 gene is expressed in antigen-presenting cells, and its protein functions in presenting particular types of antigen to CD4 T cells. The HLA-DRB1*15:01 allele is associated with phenotypic features of the disease including female sex and the presence of cerebrospinal fluid-restricted oligoclonal bands (32). As anticipated, the MHC was definitively associated with MS susceptibility; however, beyond the MHC only two other loci were identified. These loci (the first non-MHC loci that were definitely associated with MS risk) encoded genes involved in immune regulation: the interleukin-2 receptor (IL2Ra) and the interleukin-7 receptor (IL7Ra) (33).
Genome-wide association studies (GWAS) have identified more than 150 single nucleotide polymorphisms (SNPs) associated with MS susceptibility. The odds ratio (OR) associated with the majority of these is small, around 1.1-1.2. Many of these SNPs lie close to genes associated with immune function, typically in regulatory rather than coding regions. Functional variants identified include those within IL7R, IL2RA, TNFR1, BAFF, and CYP2R1 (34). Overall, GWAS data support the long-held idea that susceptibility to MS is affected by the action of common (those with a risk allele frequency > 5%) sequence allelic variants in multiple genes. Meta-analysis has now brought the total number of associations to more than 200. The sum of each MS-associated allele (weighted by its effect size) is defined as MS genetic burden and can be calculated for each individual. A similar measure has also been computed to quantify risk at the HLA region; a high HLA-genetic burden is associated with a few demographic (young age at onset) and imaging characteristics. Besides, environmental factors have been shown to interact with genetic risk loci (smoking and HLA), therefore increasing the risk of developing MS (35).
There are significant differences between mild relapsing-remitting MS (mRRMS) and primary progressive MS (PPMS) gene expression. Surprisingly, the differentially expressed genes were mostly involved in immunological and inflammatory pathways, suggesting that the difference in MS phenotypes is caused primarily by a difference in immune responses (36).
2.5. MS stages and clinical progression
MS expresses itself in four clinical forms: relapsing-remitting MS (RRMS), secondary progressive MS (SPMS), primary progressive MS (PPMS), and progressive relapsing MS (PRMS). Approximately 87% of patients present with RRMS, characterized by acute attacks (relapses) followed by partial or full recovery (remission) (37). The earliest clinical presentation of relapsing-remitting MS (RRMS) is the clinically isolated syndrome (CIS). Predicting which CIS patients are at high risk for MS is complicated by the disparity between clinical attacks and the extent of axon pathology (38). With the increased knowledge base of MS pathology, the limitations of purely clinical phenotypes, lacking imaging and biological correlates, became evident. In 2012, the Committee (sponsored by the National Multiple Sclerosis Society (NMSS) and the European Committee for Treatment and Research in MS) reexamined the original clinical phenotypes to provide improved terminology while incorporating imaging, fluid biomarkers, and other assays. The Committee recommended retention of the basics of the original 1996 MS phenotypes but introduced new descriptors of activity and progression. Two new disease courses were added: radiologically isolated syndrome (RIS) and CIS (39).
RRMS can be further characterized as an active or not an active disease, worsening and stable disease. Active disease shows evidence of new relapses, new gadolinium-enhancing lesions, and/or new or enlarging T2lesions on MRI over a specified period. Not active disease is that showing no evidence of disease activity. The worsening state is defined as increased disability confirmed over a specified period following a relapse. Stable disease is defined as no evidence of increasing disability over a specified period following a relapse. PPMS can be further characterized as an active or not an active disease, with progression or without progression. Disease with progression is defined as evidence of disease worsening on an objective measure of change, confirmed over a specified period, with or without relapses. Disease without progression is defined as disease with no evidence of worsening on an objective measure of change over a specified period. SPMS can be further characterized as an active or not an active disease, with progression or without progression. PRMS individuals who were previously diagnosed with progressive relapsing MS would now be considered primary progressive: active (at the time of relapses or new MRI lesions) or not active (40).
If the MRI is typical for MS but there are no clinical symptoms or signs suggestive of a demyelinating disorder, patients are diagnosed as having a radiologically isolated syndrome (RIS). Multiple studies have tried to identify common predictive factors for conversion of RIS to clinical MS, the strongest thus far being an asymptomatic cervical spinal cord lesion (41).
2.6. Diagnostic test for MS
The diagnosis of MS is based on neurological symptoms and signs, alongside evidence of dissemination of CNS lesions in space and time. MRI is often sufficient to confirm the diagnosis when characteristic lesions accompany a typical clinical syndrome, but in some patients, further supportive information is obtained from cerebrospinal fluid examination and neurophysiological testing (42). It is crucial to define the attacks correctly. In a patient presenting with an attack, the most important paraclinical test to confirm the diagnosis is MRI with intravenous contrast agent containing gadolinium. This can both present the nature of the lesions (inflammatory and demyelinating characteristics) for differential diagnosis, and the distribution of the lesions within the CNS (evidence of dissemination in time and space for the latest diagnostic criteria (43).
Since their introduction in 2001 up to the recent 2017 revision, the McDonald diagnostic criteria for MS are based on the number, size, and location of the brain and the spinal cord lesions believed to be typical of MS. Lesion assessment on conventional T2- weighted and post-contrast T1-weighted MRI sequences has allowed the definition of criteria that support the early diagnosis of MS (44). The 2017 revisions of the McDonald diagnostic criteria for MS were agreed on by an international expert panel. One major change is inclusion of cerebrospinal fluid (CSF) oligoclonal bands as evidence of dissemination in time (DIT) in a patient with dissemination in space (DIS) gathered by clinical or magnetic resonance examination. The distinction between asymptomatic and symptomatic lesions in accounting for evidence of dissemination in space or time in supra, infratentorial, and spinal cord syndrome has been abandoned. Finally, cortical lesions can be used to demonstrate dissemination in space (45).
CSF examination remains a valuable diagnostic test, particularly when clinical and MRI evidence is insufficient to confirm the diagnosis of MS. There has been a major change in the most recent MS diagnostic criteria in that oligoclonal bands in the CSF can be used as a surrogate marker of DIT to confirm the diagnosis of RRMS in people with CIS and MRI evidence of DIS. CSF findings are also important when there is a progressive course from onset (PPMS) and when there are any atypical clinical or imaging findings. Evidence of intrathecal antibody synthesis (oligoclonal bands in the CSF but not in a paired serum sample) supports the diagnosis of MS. An elevated CSF protein > 1.0 g/L or significant pleocytosis > 50 cells/mm³ or the presence of neutrophils would suggest an alternative diagnosis (46).
2.7. Management of MS
Intravenous methylprednisolone is an anti-inflammatory glucocorticosteroid that is indicated by the Food and Drug Administration (FDA) for the treatment of MS relapse. Repository corticotropin injection (RCI), is a subcutaneous (SC) or intramuscular (IM) injection of adrenocorticotropic hormone (ACTH) approved by the FDA for use in patients experiencing MS relapse. Plasmapheresis is a medical procedure that has been recommended for steroid-resistant acute MS relapses by the American Academy of Neurology and the American Society for Apheresis. Intravenous immunoglobulin (IVIG) is an administered treatment comprised of pooled immunoglobulin G (IgG) prepared from the fractionation of human plasma and is also used in the treatment of MS relapse despite not having an FDA indication for such use (47).
Seven DMTs are currently approved as first-line therapy in RRMS without any restrictions: (IFN)-beta 1a IM, IFN-beta 1a SC, IFN-beta 1b SC, Peginterferon-beta 1a, GA, teriflunomide, and DMF. In patients with highly active disease (HAD), fingolimod, siponimod, natalizumab, ocrelizumab, or cladribine may be initiated following careful risk stratification (serum anti-JCV antibody, prior immunosuppressant use, cardiac disease, diabetes mellitus, retinal disorders, and malignancies). In patients with rapidly evolving aggressive disease, natalizumab, ocrelizumab, or alemtuzumab are recommended after careful risk stratification. In patients with moderately active disease and suboptimal response to first-line therapies as defined above, treatment escalation to fingolimod, siponimod, natalizumab, ocrelizumab, or cladribine should be considered. In patients with HAD and suboptimal response to DMTs, treatment escalation to natalizumab, ocrelizumab, cladribine or alemtuzumab should be considered (48).
The treatment of both PPMS and SPMS collectively referred to as progressive MS, has proven quite challenging due to the multifactorial and poorly understood pathophysiology of MS in general, specifically that of progressive disease. Ocrelizumab is indicated for patients with early PPMS in terms of disease duration and level of disability, as well as inflammatory activity on MRI. The benefit of ocrelizumab in PPMS patients over age 55 years and more than 10-15 years disease duration is unclear (49). Siponimod is a newer-generation sphingosine 1 phosphate (S1P) receptor modulator that internalizes S1P1 receptors. The results of a phase-III study suggest that siponimod may be beneficial in secondary progressive MS, at least in patients with disease activity (50). Ibudilast slowed brain atrophy in PPMS and SPMS patients in a multicenter phase 2b study. Smaller early phase studies of alpha-lipoic acid and simvastatin each found slowing of the rate of whole-brain atrophy in SPMS patients. Reasons now exist for optimism in the search for DMTs for progressive MS (51). The summary of therapy for MS subtypes is summarized in Table 1.
Table 1. Treatment options according to each subtype of MS.
| Clinical subtype | Therapy |
|---|---|
| Acute MS relapse | Corticosteroids, repository corticotropin injection, plasmapheresis |
| RRMS | (IFN)-beta 1a IM, IFN-beta 1a SC, IFN-beta 1b SC, Peginterferon-beta 1a, GA, Teri-flunomide, DMF |
| RRMS; Highly active disease | Fingolimod, Siponimod, Natalizumab, Ocrelizumab, Cladribine |
| Active SPMS | Ocrelizumab or Siponimod |
| PPMS | Ocrelizumab |
| Refractory rapidly progressive SPMS | Cyclophosphamide, Methotrexate |
MS, multiple sclerosis; RRMS, relapsing-remitting MS; IFN, Interferon; SC, Subcutaneous; IM, Intramuscular injection; GA, glatiramer acetate; DMF, dimethyl fumarate; SPMS, secondary progressive MS; PPMS, primary progressive MS.
3. Urologic outcomes of MS
Urological symptoms often may be present as one of the initial presenting symptoms of MS. It may be the initial presenting complaint in MS in 3-10% of patients. It appears that LUTD occurs secondary to spinal cord involvement and in 50-80% of the patients. This can result in significant morbidity and significant impairment of quality of life. Most patients have storage-phase symptoms (urgency, frequency, nocturia, and urgency urinary incontinence) at some point but many are also affected by voiding-phase symptoms (weak and interrupted stream, straining to urinate, double voiding, and sensation of incomplete bladder emptying after voiding). Storage-phase, OAB affects between 32% and 86% of patients with urgency urinary incontinence reported in 36-72% (52). The lateral and posterior cervical spinal tracts are the most common sites for demyelination from MS and are the exact site of the necessary spinal tract pathways used to coordinate normal voluntary voiding. A patient with progressive and advancing MS loses volitional and synergistic control of the micturition reflex. These patients void only when they experience an involuntary detrusor contraction. Detrusor hyperreflexia due to unmasking of the sacral micturition reflex center or removal of cerebral inhibitory pathways by suprapontine neural plaques (or both) is reported to occur in 50 to 90% of patients with MS. Of the patients with detrusor hyperreflexia, approximately half will also have coexisting external urinary sphincter dyssynergia. Because of the presence of a sacral plaque, approximately 20% of the patients will have detrusor areflexia (53).
The variation in LUTD experienced by patients with MS may be attributable to the variable locations of lesions in the CNS. Understanding this relationship is important to further elucidate the pathophysiological relationship between MS and LUTD (54). Table 2 summarizes the LUTD according to the site of lesion in MS patients. Two factors likely to influence the clinical presentation of LUTD in MS are the MS duration and the severity of the neurological deficiencies and disabilities. There appears to be a significant correlation between the MS duration and the presence and the severity of clinical LUTD but not with their clinical presentation. The prevalence of clinical LUTD appears to be correlated with the severity of the overall deficiencies. The correlation between urinary retention and neurological status is still controversial (55).
Table 2. Lower urinary tract dysfunction according to the site of lesion in MS patients.
| Site of the lesion | Urologic dysfunction on UDS | LUTD type |
|---|---|---|
| Suprapontine | Detrusor overactivity | Mostly storage symp-toms |
| Spinal: Infrapontine, supra-sacral | Detrusor overactivity, detru-sor- sphincter dyssynergia | Storage and voiding symptoms |
| Spinal: Sacral and infrasacral | Detrusor underactivity | Mostly voiding symp-toms |
MS, multiple sclerosis; LUTD, lower urinary tract dysfunction; UDS, urodynamic study.
The presence of LUTD emerges during the visit, either because it is reported by the patient, or because it is found by the neurologist. Initial evaluation consists of several protocols. A consensus of the Italian Multiple Sclerosis Study Group suggest (a) quantification of the neurological deficit using the Functional Systems (FS) Scale and the Expanded Disability Status Scale (EDSS) according to Kurtzke; (b) the use of dedicated psychometric instruments, to best evaluate the possible presence of urinary symptoms; (c) the execution of urine test with urine culture and the possible treatment of urinary tract infections (UTIs) based on the antibiogram; (d) the use of a bladder diary (volume/frequency card) filled out by the patient to obtain information about the frequency of urination and volume voided at each urination; (e) the determination of post-void residual volume (PVR) by ultrasound or bladder catheterization; (f) the performance of an ultrasound of the urinary apparatus (56). A United Kingdom (UK) consensus on the management of the bladder in MS recommends doing an initial assessment with urine testing and measurement of the PVR. Urodynamic study (UDS) with or without additional synchronous fluoroscopic screening (video urodynamics), is used in neuro-urological practice to plan management of refractory symptoms or to identify patients at risk of future complications, particularly upper urinary tract problems. However, it should be noted that upper tract deterioration is much less common in patients with MS than in spinal cord injury (57). The risk of a pathological result in urodynamics is especially high for patients with EDSS > 6.5, use of more than one incontinence pad per day, and an MS that is not of the relapsing-remitting type (58). The ideal moment and context to indicate UDS in MS patients remain controversial. UDS is not indicated in the initial assessment of all MS patients reporting LUTD. Indications to perform UDS in MS patients are one or more of these conditions: evidence for spinal cord disease, increasing degree of disability according to EDSS, hydronephrosis/deterioration of renal function, increased PVR, recurrent UTIs, failure of conservative treatment (59).
UTIs are a major concern for patients with MS and pose a challenge to the treating physician. UTIs are ranked among the top three reasons for hospitalization, being responsible for 30-50% of all in-patient admissions of people with MS. The occurrence of recurrent UTIs in those patients may indicate suboptimal management of underlying LUTD. Known facts are the usefulness of urinalysis using to exclude UTIs and the non-treatment of asymptomatic UTIs except in the context of an acute MS relapse (60). Anatomic upper urinary tract (UUT) abnormalities in MS are reported in 0-25% of patients, most of which are noted at presentation for the evaluation of LUTD. Adverse findings include: pyelonephritis (0- 25%), hydronephrosis (0-25%), vesicoureteral reflux (0-15%) and nephrolithiasis (2-11%). The development of structural UUT changes is low in MS patients. One explanation is that the disease course of MS is marked by relapses and remissions, which may lead to fluctuations in LUTD, leading to less effect on the UUT (61). High EDSS is significantly associated with urodynamic risk factors for UUT damage and allows a risk-dependent stratification in daily neurological clinical practice. An EDSS of ≥ 5.0 identified almost 90% of patients at risk for UUT damage (62). Patients with MS have a high incidence of calcium phosphate stones and struvite stones. The method of bladder management appears to be a risk factor in the development of stone disease (63). Stratifying for sex and age, female patients with MS at the ages of 30 to 39 years and female patients with MS for more than 10 years exhibited an increased risk of bladder cancer, whereas in men the risk of bladder cancer was increased 1 to 9 years after MS diagnosis (64). In a matched cohort study, the incidence rates and mortality rates for bladder cancer were higher in the MS cohort than in the matched cohort, consistent with some, but not all prior studies. The increased risk of bladder cancer in the MS cohort may reflect the more frequent presence of risk factors such as recurrent UTIs or the use of chronic indwelling catheters secondary to the neurogenic bladder (65).
Sexual dysfunctions (SD) are highly prevalent in MS patients and include diminished desire, arousal/erectile dysfunction (ED), and orgasmic/ejaculatory dysfunction. SDs can be caused by damage to the brain, to the spinal cord areas, and the peripheral neurons engaged in sexual response (66). SD may not only be due to lesions affecting the neural pathways involved in physiological function (primary dysfunction) but also result from general physical disabilities (secondary dysfunction) or psychological and emotional issues (tertiary dysfunction) (67). The most common sexual complaint in an MS male is ED, which can be found in 23% to 91% of patients. It is generally known that MS substantially determines a generalized demyelination process that interrupts the continuity of the neural pathways and alters the neural function that is essential for normal erection function (68). As depression occurs very commonly in patients with MS, with a lifetime prevalence of around 50%, this contributes to the very high prevalence of SD in those patients (69). The Multiple Sclerosis Intimacy and Sexuality Questionnaire-19 (MSISQ-19) is a 19- item self-report tool that measures SD stemming from the primary, secondary, or tertiary domains and has been validated in the MS population. An advantage of the MSISQ-19 is that it is quick, taking approximately 2 minutes to complete, and can be done before any patient visit (70).
4. Urologic Management of MS
4.1. Management of the storage symptoms (OAB symptoms) in MS patients
A detailed algorithm for the management of the storage symptoms in MS patients is summarized in Figure 2.
Figure 2.
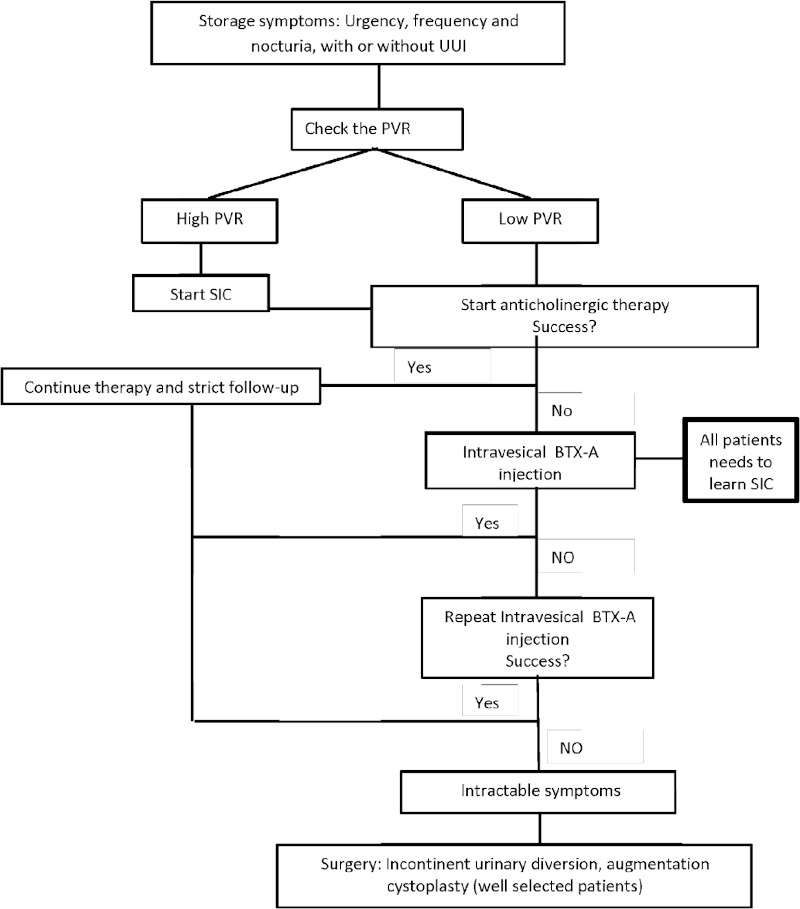
Algorithm for the management of storage symptoms in MS patients. MS, multiple sclerosis; UUI, urge urinary incontinence; SIC, self-intermittent catheterization; PVR, post void residual volume; BTX-A, Botulinum toxin A.
4.1.1. General measures and physical treatment
Patients should be encouraged to keep a micturition diary, to drink adequately and regularly throughout the day (1.5-2l/day) but not late at night, and, if a pathological residual volume is present, not to delay micturition in case of urgency (71). Caffeinated fluid intake has a minimal effect on lower urinary tract symptoms in patients with MS. On average, patients with MS do not hydrate excessively and a considerable proportion restricts fluid intake to control urinary symptoms (72). Dietary modifications, with limitation of nighttime fluid intake, voiding before going to bed, and avoidance of caffeine, alcohol, and tea, should also be implemented before any pharmacological treatment for nocturia in patients with MS (73).
Physical therapy interventions can help reduce the negative effects of urge urinary incontinence by decreasing some of the symptoms. Treatment protocols vary, lacking a definitive technique (74). In patients with slight disability and OAB, PFMT may be beneficial. For PFMT to be effective, the neural pathways leading to the pelvic floor must be intact, and patients must be able to contract the pelvic floor muscles. PFMT is thought to strengthen the inhibition exerted on the detrusor by pelvic floor contraction. Several authors have demonstrated the beneficial impacts of PFMT on the course of the disease (75).
4.1.2. Antimuscarinic drugs
The treatment of urine storage problems in patients with MS has been attempted with antimuscarinic drugs such as oxybutynin, trospium chloride, propantheline, imipramine (particularly for nocturia), and solifenacin succinate. Efficacy results were varied but treatment was often associated with significant adverse effects commonly associated with anticholinergic therapies such as dry mouth and constipation and, less frequently, impairment of accommodation with blurred vision (76). One particularly vulnerable population is the neurogenic bladder patients who maintain the ability to void. These patients can void but may have elevated residual urine, difficulty initiating voiding, or have detrusor hypocontractility. These patients can have urgency incontinence that would benefit from antimuscarinics but are at high risk of urinary retention, which is a known side effect (77). The chronic use of classical anticholinergic drugs for bladder symptoms may have a negative impact on cognitive functioning in MS patients. These potential cognitive side effects need to be considered both in clinical practice and research settings (78).
Anatomically and functionally anticholinergics have a potential benefit in MS but an important issue missed in a narrow randomized controlled trials-based assessment is the place of anticholinergics in the management of MS-related urinary symptoms, which has only been addressed thus far in consensus guidelines (79).
4.1.3. Botulinum toxin therapy
When anticholinergic therapy is insufficient or comes with too many side effects, intradetrusor injections with Botulinum toxin A (BTX-A) are recommended. BTX injection is recommended grade A in the European association of urology guidelines to be the most effective minimally invasive treatment to reduce neurogenic detrusor overactivity (NDO). These injections might increase PVR and might introduce the need for intermittent catheterization (80). A study was conducted by Deffontaines-Rufin et al. to assess the safety and efficacy of intravesical BTX-A injection in patients with MS and refractory NDO. Seventy-one patients with MS were included. 77% of the patients had clinical improvement or full success from the treatment with a reduction of their urgency and incontinence. Significant urodynamic improvement after treatment was shown (81). Mehnert et al. concluded in their study that OAB treatment in patients with MS using 100 Units (U) Botox intradetrusor injections seems to be effective and safe. Despite slightly impaired detrusor contractility most patients still voided voluntarily without symptoms (82). The dose of BTX-A commonly used to treat NDO in patients with MS is 200 U, even if in selected patients lower doses can be preferred. To be considered eligible for treatment, all patients should accept and be instructed to perform clean intermittent catheterization (CIC), since the risk of increased PVR volume and/or urinary retention after injection is high, especially with 200 UI of BTX-A (83). Repeated detrusor BTX-A for refractory NDO in patients with MS has a consistent effect on bladder control, resulting in sustained improvement in quality of life (84).
4.1.4. Sacral neuromodulation
Sacral neuromodulation (SNM) has shown promising results in MS patients who presented with DO. Usually, MS patients who are candidates for SNM should have stable disease without an expected requirement for frequent or routine MRI; patients with RPMS typically should not have SNM systems implanted (85).
4.1.5. Surgery
Surgical treatments of LUTD in patients with MS are appropriate in certain situations: when conservative therapies have failed; when intermittent self-catheterization (ISC) through the urethra is not possible; or in patients with serious complications such as sepsis, urethral or perineal fistula, renal failure or severe urinary incontinence. Augmentation cystoplasty can be done in highly-motivated patients. The goal of an augmentation cystoplasty procedure, which involves surgically enlarging the bladder, is to restore a low-pressure and compliant reservoir and, thus, achieve urinary continence. This procedure is often performed using a segment of detubularized ileon to augment the urinary bladder (86). Indications for augmentation cystoplasty include intractable (to conservative management, pharmacological treatment, and neuromodulation) DO or urgency urinary incontinence, and the procedure is performed either to protect renal function or to provide continence. Augmentation ileocystoplasty proved to be effective in neurological patients, including those with MS. Overall, a 77% success rate has been reported using ileum, and the use of ISC varies greatly among different series. Continence rate can be as high as 100%, although anticholinergics, bladder neck reconstruction, or continent diversion may be required to achieve it. Contraindications to augmentation cystoplasty include intrinsic bowel disease and inability to perform ISC. Long term results of augmentation cystoplasty suffer a variable rate of surgical revision (from 5% to 42%), although a 92% success rate has been reported for NDO (87).
Urethral catheters can be uncomfortable and can cause urethral and bladder neck trauma and should therefore only be considered as a temporary measure while waiting for a suprapubic catheter insertion. The patient should be referred to a urology service for suprapubic catheterization, which should be performed under both cystoscopic and ultrasound guidance to minimize the risk of accidental bowel injury. Once inserted, to allow adequate tract epithelialization, the suprapubic catheter should not be changed for up to 8 weeks, after which it can then be changed at intervals of up to 3 months. To minimize the risk of complications associated with long-term urinary catheterization, such as recurrent infections, encrustation, blockages, and bleeding, catheters can be washed out at regular intervals (between changes) and attention can be given to cleanliness (88).
If all previous therapies are insufficient to control LUTD in MS patients and properly prevent complications, or inapplicable because of the disability associated with the disease that does not allow ISC, a surgical approach with non-continent urinary diversion may be an option. Large size studies are lacking to describe outcomes of this strategy and therefore define more accurately the targeted population as well as better inform patients before surgery (89).
4.2. Management of the voiding symptoms in MS patients
4.2.1. Clean intermittent catheterization and long term indwelling catheterization
CIC has been a staple treatment for neurogenic bladder patients with urinary retention and incomplete emptying. In the North American Research Committee on Multiple Sclerosis (NARCOMS) survey of over 9,000 MS patients, 11-15% of people reported currently using or past use of a catheter. Of these patients, over 80% performed intermittent catheterization (90). The frequency of catheterization will depend on factors such as bladder volume, fluid intake, PVR, and some urodynamic parameters. CIC is to be done in cases with persistent urinary retention but indwelling catheters should be avoided. UTI is the most frequent complication in patients performing CIC. Trauma from catheterization can occur but specific data in MS patients are lacking (91).
Indwelling urethral or suprapubic catheters are used by individuals with chronic urinary retention who are unable to perform CIC because of poor hand dexterity, no caregiver assistance, difficulty in using the bathroom, or in select cases of incontinence (92).
4.2.2. Alpha-blockers
Alpha 1-Adrenergic receptors are present at the bladder neck, where increased tone may be responsible for urinary retention and diminished flow rates. O'Riordan et al. conducted a randomized placebo-controlled study to test the hypothesis that blockade of these receptors using the selective alpha 1-adrenergic receptor antagonist would improve bladder emptying in patients with MS. 18 men with MS were included. There was a mean 41% improvement in peak flow rate in the actively treated group compared with a 7.4% deterioration in the placebo group (p < 0.05). Residual volume improved in both groups (93). Alpha-blockers may be effective and safe for treating neurogenic LUTD in female and male patients with MS but the studies were small and the overall quality of evidence was low. To make definitive conclusions, well designed randomized controlled trials are highly warranted (94).
4.3. Management of the detrusor sphincter dyssynergia in MS patients
Nearly half of the patients with untreated DSD will develop deleterious urologic complications, due to high intravesical pressures, resulting in urolithiasis, UTIs, vesicoureteral reflux, hydronephrosis, obstructive uropathy, and renal failure. The mainstay of treatment is the use of antimuscarinics and catheterization, but in those for whom this is not possible external sphincterotomy has been the last resort option (95). BTX-A injections for DSD have been primarily used in patients who were unable to perform CIC as an alternative to surgical sphincterotomy (96).
4.4. Management of sexual dysfunction in MS patients
The f i r s t - l ine the r api e s f o r ma l e SD ar e phosphodiesterase type 5 inhibitors. Sildenafil and tadalafil are proven effective and well-tolerated therapy for ED in MS patients. Alprostadil (prostaglandin E1) and adrenoceptor antagonists (phentolamine) have been proven useful (97). Women with MS and SD are faced with limited treatment options including sildafenil and possibly estrogen replacement therapy, although more research is needed (98). Sildenafil is unlikely to help all patients with neurogenic female sexual dysfunction. Statistically significant improvement following sildenafil was only reported in the lubrication domain of the sexual function (99).
5. Conclusion
LUTD is common in MS and can be extremely disabling and embarrassing for patients. Depending on disease status and symptoms, MS urinary symptoms may respond to directed behavioral therapy, antimuscarinics, CIC, intravesical BTX injections, sacral neuromodulation, or surgical therapies. Due to the complexity and multifactorial nature of sexual dysfunction in MS patients, a multidisciplinary approach is necessary to provide them the best care. A close urology follow-up can reduce morbidity and improve the quality of life of those patients.
Funding: None.
Conflict of Interest
The authors have no conflicts of interest to disclose.
References
- 1. Ghasemi N, Razavi S, Nikzad E. Multiple sclerosis: pathogenesis, symptoms, diagnoses and cell-based therapy. Cell J. 2017; 19:1-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Dobson R, Giovannoni G. Multiple sclerosis - a review. Eur J Neurol. 2019; 26:27-40. [DOI] [PubMed] [Google Scholar]
- 3. Huang WJ, Chen WW, Zhang X. Multiple sclerosis: pathology, diagnosis and treatments. Exp Ther Med. 2017; 13:3163-3166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Klocke S, Hahn N. Multiple sclerosis. Ment Health Clin. 2019; 9:349-358. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Hauser SL, Cree BAC. Treatment of multiple sclerosis: a review. Am J Med. 2020; 133:1380-1390.e2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Goldenberg MM. Multiple sclerosis review. P T. 2012; 37:175-184. [PMC free article] [PubMed] [Google Scholar]
- 7. Cree BAC, Mares J, Hartung HP. Current therapeutic landscape in multiple sclerosis: an evolving treatment paradigm. Curr Opin Neurol. 2019; 32:365-377. [DOI] [PubMed] [Google Scholar]
- 8. Filippi M, Rocca MA. Rethinking multiple sclerosis treatment strategies. Lancet Neurol. 2020; 19:281-282. [DOI] [PubMed] [Google Scholar]
- 9. Litwiller SE, Frohman EM, Zimmern PE. Multiple sclerosis and the urologist. J Urol. 1999; 161:743-57. [PubMed] [Google Scholar]
- 10. Rashid TM, Hollander JB. Multiple sclerosis and the neurogenic bladder. Phys Med Rehabil Clin N Am. 1998; 9:615-629. [PubMed] [Google Scholar]
- 11. Panicker JN, Fowler CJ, Kessler TM. Lower urinary tract dysfunction in the neurological patient: clinical assessment and management. Lancet Neurol. 2015; 14:720-732. [DOI] [PubMed] [Google Scholar]
- 12. Aharony SM, Lam O, Corcos J. Evaluation of lower urinary tract symptoms in multiple sclerosis patients: Review of the literature and current guidelines. Can Urol Assoc J. 2017; 11:61-64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Tornic J, Panicker JN. The management of lower urinary tract dysfunction in multiple sclerosis. Curr Neurol Neurosci Rep. 2018; 18:54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Leray E, Moreau T, Fromont A, Edan G. Epidemiology of multiple sclerosis. Rev Neurol (Paris). 2016; 172:3-13. [DOI] [PubMed] [Google Scholar]
- 15. Pugliatti M, Rosati G, Carton H, Riise T, Drulovic J, Vécsei L, Milanov I. The epidemiology of multiple sclerosis in Europe. Eur J Neurol. 2006; 13:700-722. [DOI] [PubMed] [Google Scholar]
- 16. GBD 2016 Multiple Sclerosis Collaborators. Global, regional, and national burden of multiple sclerosis 1990- 2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019; 18:269-285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Racke MK. Immunopathogenesis of multiple sclerosis. Ann Indian Acad Neurol. 2009; 12:215-220. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Compston A. The pathogenesis and basis for treatment in multiple sclerosis. Clin Neurol Neurosurg. 2004; 106:246-248. [DOI] [PubMed] [Google Scholar]
- 19. Kuhlmann T, Lingfeld G, Bitsch A, Schuchardt J, Brück W. Acute axonal damage in multiple sclerosis is most extensive in early disease stages and decreases over time. Brain. 2002; 125(Pt 10):2202-2212. [DOI] [PubMed] [Google Scholar]
- 20. Nikbin B, Bonab MM, Khosravi F, Talebian F. Role of B cells in pathogenesis of multiple sclerosis. Int Rev Neurobiol. 2007; 79:13-42. [DOI] [PubMed] [Google Scholar]
- 21. Lewitt MS, Boyd GW. The role of insulin-like growth factors and insulin-like growth factor-binding proteins in the nervous system. Biochem Insights. 2019; 12:1178626419842176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Chesik D, Wilczak N, De Keyser J. The insulin-like growth factor system in multiple sclerosis. Int Rev Neurobiol. 2007; 79:203-226. [DOI] [PubMed] [Google Scholar]
- 23. Nataf S, Guillen M, Pays L. TGFB1-mediated gliosis in multiple sclerosis spinal cords is favored by the regionalized expression of HOXA5 and the age-dependent decline in androgen receptor ligands. Int J Mol Sci. 2019; 20:5934. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Lee PW, Severin ME, Lovett-Racke AE. TGF-β regulation of encephalitogenic and regulatory T cells in multiple sclerosis. Eur J Immunol. 2017; 47:446-453. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Rostami A, Ciric B. Role of Th17 cells in the pathogenesis of CNS inflammatory demyelination. J Neurol Sci. 2013; 333:76-87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Bitsch A, Schuchardt J, Bunkowski S, Kuhlmann T, Brück W. Acute axonal injury in multiple sclerosis. Correlation with demyelination and inflammation. Brain. 2000; 123 (Pt 6):1174-1183. [DOI] [PubMed] [Google Scholar]
- 27. Disanto G, Morahan JM, Ramagopalan SV. Multiple sclerosis: risk factors and their interactions. CNS Neurol Disord Drug Targets. 2012; 11:545-555. [DOI] [PubMed] [Google Scholar]
- 28. Ascherio A. Environmental factors in multiple sclerosis. Expert Rev Neurother. 2013; 13(12 Suppl):3-9. [DOI] [PubMed] [Google Scholar]
- 29. Waubant E, Lucas R, Mowry E, Graves J, Olsson T, Alfredsson L, Langer-Gould A. Environmental and genetic risk factors for MS: an integrated review. Ann Clin Transl Neurol. 2019; 6:1905-1922. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Wang YJ, Li R, Yan JW, Wan YN, Tao JH, Chen B, Huang XL, Yang GJ, Wang J, Ye DQ. The epidemiology of alcohol consumption and multiple sclerosis: a review. Neurol Sci. 2015; 36:189-196. [DOI] [PubMed] [Google Scholar]
- 31. Marrie RA. Environmental risk factors in multiple sclerosis aetiology. Lancet Neurol. 2004; 3:709-718. [DOI] [PubMed] [Google Scholar]
- 32. Parnell GP, Booth DR. The multiple sclerosis (MS) genetic risk factors indicate both acquired and innate immune cell subsets contribute to MS pathogenesis and identify novel therapeutic opportunities. Front Immunol. 2017; 8:425. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Cree BA. Multiple sclerosis genetics. Handb Clin Neurol. 2014; 122:193-209. [DOI] [PubMed] [Google Scholar]
- 34. Dobson R, Giovannoni G. Multiple sclerosis - a review. Eur J Neurol. 2019; 26:27-40. [DOI] [PubMed] [Google Scholar]
- 35. Koch MW, Ilnytskyy Y, Golubov A, Metz LM, Yong VW, Kovalchuk O. Global transcriptome profiling of mild relapsing-remitting versus primary progressive multiple sclerosis. Eur J Neurol. 2018; 25:651-658. [DOI] [PubMed] [Google Scholar]
- 36. Thompson AJ, Baranzini SE, Geurts J, Hemmer B, Ciccarelli O. Multiple sclerosis. Lancet. 2018; 391:1622-1636. [DOI] [PubMed] [Google Scholar]
- 37. Loma I, Heyman R. Multiple sclerosis: pathogenesis and treatment. Curr Neuropharmacol. 2011; 9:409-416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Thrower BW. Clinically isolated syndromes: predicting and delaying multiple sclerosis. Neurology. 2007; 68:S12-S15. [DOI] [PubMed] [Google Scholar]
- 39. Lublin FD, Reingold SC, Cohen JA, et al. Defining the clinical course of multiple sclerosis: the 2013 revisions. Neurology. 2014; 83:278-286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Klineova S, Lublin FD. Clinical course of multiple sclerosis. Cold Spring Harb Perspect Med. 2018; 8:a028928. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Alshamrani F, Alnajashi H, Freedman M. Radiologically isolated syndrome: watchful waiting vs. active treatment. Expert Rev Neurother. 2017; 17:441-447. [DOI] [PubMed] [Google Scholar]
- 42. Brownlee WJ, Hardy TA, Fazekas F, Miller DH. Diagnosis of multiple sclerosis: progress and challenges. Lancet. 2017; 389:1336-1346. [DOI] [PubMed] [Google Scholar]
- 43. Ömerhoca S, Akkaş SY, İçen NK. Multiple sclerosis: diagnosis and differential diagnosis. Noro Psikiyatr Ars. 2018; 55:S1-S9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Filippi M, Preziosa P, Banwell BL, et al. Assessment of lesions on magnetic resonance imaging in multiple sclerosis: practical guidelines. Brain. 2019; 142:1858-1875. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Hartung HP, Graf J, Aktas O, Mares J, Barnett MH. Diagnosis of multiple sclerosis: revisions of the McDonald criteria 2017 - continuity and change. Curr Opin Neurol. 2019; 32:327-337. [DOI] [PubMed] [Google Scholar]
- 46. Ford H. Clinical presentation and diagnosis of multiple sclerosis. Clin Med (Lond). 2020; 20:380-383. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Costello J, Njue A, Lyall M, Heyes A, Mahler N, Philbin M, Nazareth T. Efficacy, safety, and quality-of-life of treatments for acute relapses of multiple sclerosis: results from a literature review of randomized controlled trials. Degener Neurol Neuromuscul Dis. 2019; 9:55-78. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Yamout B, Sahraian M, Bohlega S, et al. Consensus recommendations for the diagnosis and treatment of multiple sclerosis: 2019 revisions to the MENACTRIMS guidelines. Mult Scler Relat Disord. 2020; 37:101459. [DOI] [PubMed] [Google Scholar]
- 49. Baldassari LE, Fox RJ. Therapeutic Advances and Challenges in the Treatment of Progressive Multiple Sclerosis. Drugs. 2018; 78:1549-1566. [DOI] [PubMed] [Google Scholar]
- 50. Goodman AD, Anadani N, Gerwitz L. Siponimod in the treatment of multiple sclerosis. Expert Opin Investig Drugs. 2019; 28:1051-1057. [DOI] [PubMed] [Google Scholar]
- 51. Ciotti JR, Cross AH. Disease-modifying treatment in progressive multiple sclerosis. Curr Treat Options Neurol. 2018; 20:12. [DOI] [PubMed] [Google Scholar]
- 52. Sand PK, Sand RI. The diagnosis and management of lower urinary tract symptoms in multiple sclerosis patients. Dis Mon. 2013; 59:261-268. [DOI] [PubMed] [Google Scholar]
- 53. Andrews KL, Husmann DA. Bladder dysfunction and management in multiple sclerosis. Mayo Clin Proc. 1997; 72:1176-1183. [DOI] [PubMed] [Google Scholar]
- 54. Weissbart SJ, Pechersky D, Malykhina A, Bavaria T, Parrillo L, Arya LA, Bilello M, Wein AJ, Smith AL. The impact of pontine disease on lower urinary tract symptoms in patients with multiple sclerosis. Neurourol Urodyn. 2017; 36:453-456. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. de Sèze M, Ruffion A, Denys P, Joseph PA, Perrouin- Verbe B; GENULF. The neurogenic bladder in multiple sclerosis: review of the literature and proposal of management guidelines. Mult Scler. 2007; 13:915-928. [DOI] [PubMed] [Google Scholar]
- 56. G h e z z i A, C a r o n e R, D e l P o p o l o G, e t a l. Recommendations for the management of urinary disorders in multiple sclerosis: a consensus of the Italian Multiple Sclerosis Study Group. Neurol Sci. 2011; 32:1223-1231. [DOI] [PubMed] [Google Scholar]
- 57. Fowler CJ, Panicker JN, Drake M, Harris C, Harrison SC, Kirby M, Lucas M, Macleod N, Mangnall J, North A, Porter B, Reid S, Russell N, Watkiss K, Wells M. A UK consensus on the management of the bladder in multiple sclerosis. J Neurol Neurosurg Psychiatry. 2009; 80:470-477. [DOI] [PubMed] [Google Scholar]
- 58. Wiedemann A, Kaeder M, Greulich W, Lax H, Priebel J, Kirschner-Hermanns R, Füsgen I. Which clinical risk factors determine a pathological urodynamic evaluation in patients with multiple sclerosis? an analysis of 100 prospective cases. World J Urol. 2013; 31:229-233. [DOI] [PubMed] [Google Scholar]
- 59. Averbeck MA, Iacovelli V, Panicker J, Schurch B, Finazzi Agrò E. Urodynamics in patients with multiple sclerosis: A consensus statement from a urodynamic experts working group. Neurourol Urodyn. 2020; 39:73-82. [DOI] [PubMed] [Google Scholar]
- 60. Phé V, Pakzad M, Curtis C, Porter B, Haslam C, Chataway J, Panicker JN. Urinary tract infections in multiple sclerosis. Mult Scler. 2016; 22:855-861. [DOI] [PubMed] [Google Scholar]
- 61. Fletcher SG, Dillon BE, Gilchrist AS, Haverkorn RM, Yan J, Frohman EM, Lemack GE. Renal deterioration in multiple sclerosis patients with neurovesical dysfunction. Mult Scler. 2013; 19:1169-1174. [DOI] [PubMed] [Google Scholar]
- 62. Ineichen BV, Schneider MP, Hlavica M, Hagenbuch N, Linnebank M, Kessler TM. High EDSS can predict risk for upper urinary tract damage in patients with multiple sclerosis. Mult Scler. 2018; 24:529-534. [DOI] [PubMed] [Google Scholar]
- 63. Ganesan V, Chen WM, Jain R, De S, Monga M. Multiple sclerosis and nephrolithiasis: a matched-case comparative study. BJU Int. 2017; 119:919-925. [DOI] [PubMed] [Google Scholar]
- 64. D'Amico E, Chisari CG, Arena S, Zanghì A, Toscano S, Lo Fermo S, Maimone D, Castaing M, Sciacca S, Zappia M, Patti F. Cancer risk and multiple sclerosis: evidence from a large Italian cohort. Front Neurol. 2019; 10:337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65. Marrie RA, Maxwell C, Mahar A, Ekuma O, McClintock C, Seitz D, Webber C, Groome PA. Cancer incidence and mortality rates in multiple sclerosis: a matched cohort study. Neurology. 2021; 96:e501-e512. [DOI] [PubMed] [Google Scholar]
- 66. Lew-Starowicz M, Gianotten WL. Sexual dysfunction in patients with multiple sclerosis. Handb Clin Neurol. 2015; 130:357-370. [DOI] [PubMed] [Google Scholar]
- 67. Kessler TM, Fowler CJ, Panicker JN. Sexual dysfunction in multiple sclerosis. Expert Rev Neurother. 2009; 9:341-350. [DOI] [PubMed] [Google Scholar]
- 68. Balsamo R, Arcaniolo D, Stizzo M, Illiano E, Autorino R, Natale F, Costantini E, Damiano R, De Sio M. Increased risk of erectile dysfunction in men with multiple sclerosis: an Italian cross-sectional study. Cent European J Urol. 2017; 70:289-295. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69. Marck CH, Jelinek PL, Weiland TJ, Hocking JS, De Livera AM, Taylor KL, Neate SL, Pereira NG, Jelinek GA. Sexual function in multiple sclerosis and associations with demographic, disease and lifestyle characteristics: an international cross-sectional study. BMC Neurol. 2016; 16:210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70. Domingo S, Kinzy T, Thompson N, Gales S, Stone L, Sullivan A. Factors associated with sexual dysfunction in individuals with multiple sclerosis: implications for assessment and treatment. Int J MS Care. 2018; 20:191-197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71. Henze T, Rieckmann P, Toyka KV; Multiple Sclerosis Therapy Consensus Group of the German Multiple Sclerosis Society. Symptomatic treatment of multiple sclerosis. Multiple Sclerosis Therapy Consensus Group (MSTCG) of the German Multiple Sclerosis Society. Eur Neurol. 2006; 56:78-105. [DOI] [PubMed] [Google Scholar]
- 72. Tam J, Gross MD, Cheung A, Melville PM, Kim JM, Weissbart SJ. Fluid intake and urinary symptoms in patients with multiple sclerosis. J Urol. 2020; 204:1284-1289. [DOI] [PubMed] [Google Scholar]
- 73. Peyronnet B, Krupp LB, Reynolds WS, Gamé X, Amarenco G, Cornu JN, Ryerson LZ, Sammarco CL, Howard JE, Charlson RW, Dmochowski RR, Brucker BM. Nocturia in Patients With Multiple Sclerosis. Rev Urol. 2019; 21:63-73. [PMC free article] [PubMed] [Google Scholar]
- 74. Block V, Rivera M, Melnick M, Allen DD. Do physical therapy interventions affect urinary incontinence and quality of life in people with multiple sclerosis?: an evidence-based review. Int J MS Care. 2015; 17:172-180. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75. Bientinesi R, Gandi C, Bassi P. Managing urological disorders in multiple sclerosis patients: a review of available and emerging therapies. Int Neurourol J. 2020; 24:118-126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76. de Sa JC, Airas L, Bartholome E, Grigoriadis N, Mattle H, Oreja-Guevara C, O'Riordan J, Sellebjerg F, Stankoff B, Vass K, Walczak A, Wiendl H, Kieseier BC. Symptomatic therapy in multiple sclerosis: a review for a multimodal approach in clinical practice. Ther Adv Neurol Disord. 2011; 4:139-168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77. Cameron AP. Medical management of neurogenic bladder with oral therapy. Transl Androl Urol. 2016; 5:51-62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78. Cruce R, Vosoughi R, Freedman MS. Cognitive impact of anticholinergic medication in MS: Adding insult to injury? Mult Scler Relat Disord. 2012; 1:156-161. [DOI] [PubMed] [Google Scholar]
- 79. Nicholas R, Young C, Friede T. Bladder symptoms in multiple sclerosis: a review of pathophysiology and management. Expert Opin Drug Saf. 2010; 9:905-915. [DOI] [PubMed] [Google Scholar]
- 80. Weckx F, Tutolo M, De Ridder D, Van der Aa F. The role of botulinum toxin A in treating neurogenic bladder. Transl Androl Urol. 2016; 5:63-71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81. Deffontaines-Rufin S, Weil M, Verollet D, Peyrat L, Amarenco G. Botulinum toxin A for the treatment of neurogenic detrusor overactivity in multiple sclerosis patients. Int Braz J Urol. 2011; 37:642-648. [DOI] [PubMed] [Google Scholar]
- 82. Mehnert U, Birzele J, Reuter K, Schurch B. The effect of botulinum toxin type a on overactive bladder symptoms in patients with multiple sclerosis: a pilot study. J Urol. 2010; 184:1011-1016. [DOI] [PubMed] [Google Scholar]
- 83. Schurch B, Carda S. OnabotulinumtoxinA and multiple sclerosis. Ann Phys Rehabil Med. 2014; 57:302-314. [DOI] [PubMed] [Google Scholar]
- 84. Khan S, Game X, Kalsi V, Gonzales G, Panicker J, Elneil S, Apostolidis A, Hamid R, Dasgupta P, Kessler TM, Fowler CJ. Long-term effect on quality of life of repeat detrusor injections of botulinum neurotoxin-A for detrusor overactivity in patients with multiple sclerosis. J Urol. 2011; 185:1344-1349. [DOI] [PubMed] [Google Scholar]
- 85. Averbeck MA, Moreno-Palacios J, Aparicio A. Is there a role for sacral neuromodulation in patients with neurogenic lower urinary tract dysfunction? Int Braz J Urol. 2020; 46:891-901. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86. Phé V, Chartier-Kastler E, Panicker JN. Management of neurogenic bladder in patients with multiple sclerosis. Nat Rev Urol. 2016; 13:275-288. [DOI] [PubMed] [Google Scholar]
- 87. Tubaro A, Puccini F, De Nunzio C, Digesu GA, Elneil S, Gobbi C, Khullar V. The treatment of lower urinary tract symptoms in patients with multiple sclerosis: a systematic review. Curr Urol Rep. 2012; 13:335-342. [DOI] [PubMed] [Google Scholar]
- 88. Seth JH, Sahai A, Panicker JN. Lower urinary tract dysfunction in multiple sclerosis. Curr Bladder Dysfunct Rep. 2012; 7:97-104. [Google Scholar]
- 89. Akakpo W, Chartier-Kastler E, Joussain C, Denys P, Lubetzki C, Phé V. Outcomes of ileal conduit urinary diversion in patients with multiple sclerosis. Neurourol Urodyn. 2020; 39:771-777. [DOI] [PubMed] [Google Scholar]
- 90. Tracey JM, Stoffel JT. Secondary and tertiary treatments for multiple sclerosis patients with urinary symptoms. Investig Clin Urol. 2016; 57:377-383. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91. Wyndaele JJ. Self-intermittent catheterization in multiple sclerosis. Ann Phys Rehabil Med. 2014; 57:315-320. [DOI] [PubMed] [Google Scholar]
- 92. Wilde MH, McMahon JM, McDonald MV, Tang W, Wang W, Brasch J, Fairbanks E, Shah S, Zhang F, Chen DG. Self-management intervention for long-term indwelling urinary catheter users: randomized clinical trial. Nurs Res. 2015; 64:24-34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93. O'Riordan JI, Doherty C, Javed M, Brophy D, Hutchinson M, Quinlan D. Do alpha-blockers have a role in lower urinary tract dysfunction in multiple sclerosis? J Urol. 1995; 153:1114-1116. [PubMed] [Google Scholar]
- 94. Schneider MP, Tornic J, Sýkora R, Abo Youssef N, Mordasini L, Krhut J, Chartier-Kastler E, Davies M, Gajewski J, Schurch B, Bachmann LM, Kessler TM. Alpha-blockers for treating neurogenic lower urinary tract dysfunction in patients with multiple sclerosis: A systematic review and meta-analysis. A report from the Neuro-Urology Promotion Committee of the International Continence Society (ICS). Neurourol Urodyn. 2019; 38:1482-1491. [DOI] [PubMed] [Google Scholar]
- 95. Mahfouz W, Corcos J. Management of detrusor external sphincter dyssynergia in neurogenic bladder. Eur J Phys Rehabil Med. 2011; 47:639-650. [PubMed] [Google Scholar]
- 96. Eldred-Evans D, Dasgupta P. Use of botulinum toxin for voiding dysfunction. Transl Androl Urol. 2017; 6:234-251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97. Guo ZN, He SY, Zhang HL, Wu J, Yang Y. Multiple sclerosis and sexual dysfunction. Asian J Androl. 2012; 14:530-535. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98. Pöttgen J, Rose A, van de Vis W, Engelbrecht J, Pirard M, Lau S, Heesen C, Köpke S; RiMS Special Interest Group Psychology and Neuropsychology. Sexual dysfunctions in MS in relation to neuropsychiatric aspects and its psychological treatment: A scoping review. PLoS One. 2018; 13:e0193381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99. Dasgupta R, Wiseman OJ, Kanabar G, Fowler CJ, Mikol D. Efficacy of sildenafil in the treatment of female sexual dysfunction due to multiple sclerosis. J Urol. 2004; 171:1189-1193; discussion 1193. [DOI] [PubMed] [Google Scholar]