

Abstract
Dentigerous cyst (DC) and ossifying fibroma (OF) are intraosseous lesions of the jaw. Both are varied pathological entities with a wide spectrum of clinical and histological features along with distinct treatment plan and prognosis. While OF comes under fibro-osseous lesions of the jaws, DC is a developmental odontogenic cyst which is formed by the accumulation of fluid between reduced enamel epithelium and enamel or between layers of the enamel organ. This case report presents a rare display of two distinct pathologies synchronously and aims to discuss the possible histogenesis for the same.
Keywords: Dentigerous cyst, fibro-osseous lesion, ossifying fibroma
INTRODUCTION
Amongst many intraosseous lesions of jaws, ossifying fibroma (OF) and dentigerous cyst (DC) are common.[1] DC is a developmental odontogenic cyst that encloses the crown of an unerupted tooth.[2] It is derived from reduced epithelium of the enamel organ, as a result of the accumulation of fluid between this and the crown of the developing tooth.[3] Radiographically, DC presents as unilocular radiolucency with a well-defined sclerotic border, surrounding the crown of an unerupted tooth.[4] On the contrary, OF represents a lesion whereby normal bone is replaced with fibrous tissue containing abnormal bone. The World Health Organization (WHO) in 1972 classified central OF into two types-OF and cementifying fibromas; but in 1992 WHO considered it in one heading as cemento-OF. Further, the term “cementossifying fibroma” was replaced by “ossifying fibroma” in 2005 under the new WHO classification.[1]
The central variant of OF is a relatively rare lesion, is more common in females and has a predilection for the mandible. Radiographically, the lesion manifests as a unilocular, well-demarcated, mixed radiolucent-radiopaque lesion based on the presence of cementum or bone.[5] Although rarely cited in the literature, there is a possibility of two simultaneous lesions at one anatomic site. One of such possibilities has been presented in this case report.
CASE REPORT
A 40-year-old male patient visited the dental outpatient department with the chief complaint of an asymptomatic swelling in right lower front tooth region for 6 months which gradually increased to the present size (~8 cm). The medical and family histories were noncontributory and there was no history of trauma. On extraoral examination, a diffuse swelling was present on the lower anterior region of the jaw extending between right and left commissures of the mouth [Figure 1]. On palpation, the swelling was nontender and hard in consistency. Intraoral examination revealed a bluish colored swelling extending from 31 to 44 region with obliteration of labial vestibule. Orthopantomographic examination revealed a unilocular radiolucent lesion extending from 35 to 44 regions. The radiolucent lesion appeared to encircle and adjoined to the neck of impacted 33. The lesion caused resorption of roots of 31, 32, 41, 42 [Figure 2]. Based on these findings a clinical differential diagnosis of DC, ameloblastoma, glandular odontogenic cyst and ameloblastic fibroma was achieved. Fine-needle aspiration cytology (FNAC) was done and straw-colored fluid was examined histopathologically for the presence of numerous hyperchromatic epithelial cells in the background of the mucoid stroma. The aspirate obtained was also subjected biochemically and the protein estimation was 4.4 gm%. Excisional biopsy was performed and the tissue received was fixed in 10% neutral buffered formalin. On gross examination, one soft tissue (cystic sac) and one hard tissue (33) was received. The tissue was creamish brown in color, soft in consistency, irregular in shape and measured 1.0 cm × 1.2 cm × 1.5 cm in greatest dimensions. The tissue was sectioned and submitted for routine processing. Upon microscopic examination the H&E sections revealed 3–4 cell layered nonkeratinized cystic epithelium overlying moderately dense connective tissue capsule. Numerous odontogenic rests were seen embedded within the otherwise bland stroma containing only few inflammatory cells [Figure 3]. The other end of the section revealed hypercellular stroma with the abundance of plump fibroblasts along with newly formed bone (woven bone) in varying shapes lined by plump osteoblasts encircled with blood vessels of varying caliber. Plump osteoblasts were prominently observed rimming the new bone [Figure 3]. The overall histopathological features were conclusive of concurrent DC and OF. The patient was followed regularly postoperatively for 6 months to check the recurrences, if any and the healing observed was uneventful.
Figure 1.

Photograph showing diffused swelling in mandibular 34–44 tooth region
Figure 2.

Photograph showing orthopantomogram with unilocular radiolucent lesion (arrow) with well-corticated border involving the left mandible. Extending from 34 to 44 with the impacted tooth (33)
Figure 3.
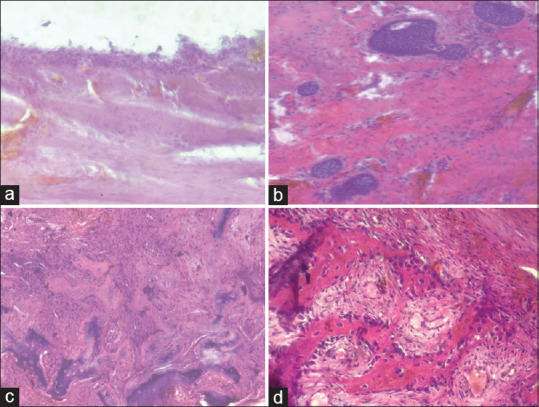
The photomicrograph showing (a). The lining of the dentigerous cyst (b). Odontogenic islands dispersed in moderately dense connective tissue stroma (c). Irregular shaped woven bone formation. (d). Neoplastic bone showing osteoblastic rimming
DISCUSSION
OF and DC are two lesions having entirely diverse clinical courses with varying treatment options and the difference in prognosis. Two distinctively different lesions occurring in the mandible of a patient are exceptionally rare and not reported in the literature.
DC is an epithelial-lined developmental odontogenic cyst that encloses the crown of an unerupted tooth at the cementoenamel junction and accounts for approximately 20%–24% of all epithelial-lined odontogenic cysts. It is believed that DC develops around the crown of an unerupted tooth by the accumulation of fluid either between the reduced enamel epithelium and enamel or in between the layers of the enamel organ.[6,7] In this case, the cyst was seen in association with impacted 33 and in male patient. Histopathologically, it is generally composed of a thin connective tissue wall with a thin layer of stratified squamous epithelium lining. The cyst wall is composed of a very loose fibrous connective tissue or sparsely collagenized myxomatous tissue and may also show varying numbers of inactive odontogenic islands.[7] In the present case, there were 2–3 layers of nonkeratinized stratified squamous epithelium with mature fibrous connective tissue wall with few odontogenic rests. OF on the other hand is one of the most frequent of the 3 fibro-osseous lesions of the jaws. It occurs more frequently in females, with a predilection of 1.75:1 and is predominantly observed in the mandible.[8]
In our case, the lesion was observed in the mandible of a middle-aged male. The concurrent occurrence of these two lesions raises the question of whether it is a collision tumor or their simultaneous occurrence is just a chance finding. A collision tumor is usually composed of two different types of neoplasms derived from clearly different origins of two neoplastic clones that have arisen from different cell types in close proximity to each other.[9] Collision tumors are rare clinical entities wherein two histologically distinct tumor types occur at the same anatomic site, which may occur between tumors originating in the same organ or between metastases from other sites but having originated from the same stem cell.[10]
As reviewed from literature, one possibility for occurrence of OF and DC could be attributed to the fact that first cyst formation may have occurred around the tooth which gradually expanded and stimulated the formation of OF in the surrounding bone which is undergoing remodeling due to expansion and resorption.[11,12] The second possibility of occurrence of both lesions could be stipulated as OF forming first leading to pushing of the impacted canine thereby causing stimulation of dental follicle of the impacted tooth for the formation of DC. However, a mere chance finding of the two distinct pathologies although rare could also be ascertained.[11,12] Based on the histopathological findings, we derived a conclusive diagnosis claiming the pathology to be a case of concurrent DC with OF, since the sequence of aforementioned events could not be ascertained. The present case however is contributory to the existing knowledge of lesions associated with impacted teeth in jaws. The case also invites a debate revolving around the fact that despite appearing as a mere cystic unilocular pathology on radiographic evaluation and initial FNAC, the case presented with a multitude of histopathologic features of two distinct pathologies. Hence, such cases demand a stringent follow-up policy in order to keep a check on relapse/recurrence as the prognosis remains unpredictable.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient (s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initial s will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest
REFERENCES
- 1.Reichart PA, Philipsen HP, Sciubba JJ. The new classification of Head and Neck Tumours (WHO)--any changes? Oral Oncol. 2006;42:757–8. doi: 10.1016/j.oraloncology.2005.10.011. [DOI] [PubMed] [Google Scholar]
- 2.Shear M, Speight PM. Dentigerous Cyst: Cysts of the Oral and Maxillofacial Regions. 4th ed. Singapore: Blackwell Publishers; 2007. pp. 59–75. [Google Scholar]
- 3.Manuel AA, Maria AFS, Jose MHG, Jose LGP, Daniel TL. Case report conservative management of dentigerous cysts in children. J Clin Exp Dent. 2015;7:671–4. doi: 10.4317/jced.52248. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Asián-González E, Pereira-Maestre M, Conde-Fernández D, Vilchez I, Segura-Egea JJ, Gutiérrez-Pérez JL. Dentigerous cyst associated with a formocresol pulpotomized deciduous molar. J Endod. 2007;33:488–92. doi: 10.1016/j.joen.2006.10.011. [DOI] [PubMed] [Google Scholar]
- 5.Swami AN, Kale LM, Mishra SS, Choudhary SH. Central ossifying fibroma of mandible: A case report and review of literature. J Indian Acad Oral Med Radiol. 2015;27:131–5. [Google Scholar]
- 6.Regezi JA, Sciubba JJ. Oral Pathology: Clinico Pathologic Correlations. 3rd ed. Philadelphia: W. B Saunders; 1999. pp. 357–60. [Google Scholar]
- 7.Rajendran R, Sivapathasundhram B. 5th ed. Noida: Elsevier Publishers; 2005. Cysts and Tumours of Odontogenic Origin: Shafer's Textbook of Oral Pathology; pp. 357–424. [Google Scholar]
- 8.Titinchi F, Morkel J. Ossifying fibroma: Analysis of treatment methods and recurrence patterns. J Oral Maxillofac Surg. 2016;74:2409–19. doi: 10.1016/j.joms.2016.05.018. [DOI] [PubMed] [Google Scholar]
- 9.Lyda MH, Fenoglio-Preiser CM. Adenoma-carcinoid tumors of the colon. Arch Pathol Lab Med. 1998;122:262–5. [PubMed] [Google Scholar]
- 10.Murthaiah P, Truskinovsky AM, Shah S, Dudek AZ. Collision tumor versus multiphenotypic differentiation: A case of carcinoma with features of colonic and lung primary tumors. Anticancer Res. 2009;29:1495–7. [PubMed] [Google Scholar]
- 11.Murgod S, Girish HC, Savita JK, Varsha VK. Concurrent central odontogenic fibroma and dentigerous cyst in the maxilla: A rare case report. J Oral Maxillofac Pathol. 2017;21:149–53. doi: 10.4103/jomfp.JOMFP_33_15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Pushpanshu K, Kaushik R, Punyani SR, Jasuja V, Raj V, Seshadri A. Concurrent central odontogenic fibroma (WHO Type) and traumatic bone cyst: Report of a rare case. Quant Imaging Med Surg. 2013;3:341–6. doi: 10.3978/j.issn.2223-4292.2013.12.09. [DOI] [PMC free article] [PubMed] [Google Scholar]