

ABSTRACT
Background: Previous studies indicate that social support, self-compassion, and posttraumatic growth (PTG) can affect prosocial behaviour and antisocial behaviour, but few studies have examined their combined role in prosocial and antisocial behaviour among adolescents who have experienced traumatic events.
Objective: This study examined the mediating roles of self-compassion and PTG in the relationship between social support and prosocial and antisocial behaviour among Chinese adolescents after the Ya’an earthquake.
Method: Four and a half years after the Ya’an earthquake, 492 students aged 13 to 18 in Lushan County (98.6% of the 499 students surveyed) were assessed using the following system: Measures of Trauma Exposure Questionnaire, Social Support Questionnaire, Self-Compassion Scale, Posttraumatic Growth Inventory, and Child Behaviour Problems Questionnaire.
Results: When we controlled for gender, age, and traumatic exposure, social support had a positive effect on prosocial behaviour. Moreover, social support had an indirect and positive effect on prosocial behaviour via positive self-compassion and PTG, as well as via an indirect path from positive self-compassion to PTG, but social support had a negative effect on antisocial behaviour via PTG, as well as via an indirect path from positive self-compassion to PTG on antisocial behaviour. Social support also had a positive effect on antisocial behaviour via negative self-compassion.
Conclusion: Findings suggest that increased support may be beneficial for prosocial behaviour and reduce antisocial behaviour. Self-compassion and PTG play a significant mediating role between social support, prosocial behaviour, and antisocial behaviour.
KEYWORDS: Social support, self-compassion, PTG, antisocial behaviour, prosocial behaviour
HIGHLIGHTS
• This study examined the mediating roles of self-compassion (positive and negative self-compassion) and PTG in the relationship between social support and prosocial and antisocial behavior among Chinese adolescents after the Ya’an earthquake.
Antecedentes: Estudios previos indican que el apoyo social, la autocompasión y el crecimiento postraumático (PTG en su sigla en inglés) pueden afectar la conducta prosocial y la antisocial, pero pocos estudios han examinado su papel combinado en el comportamiento prosocial y antisocial entre adolescentes que han experimentado eventos traumáticos.
Objetivo: Este estudio examinó los roles mediadores de la autocompasión y el PTG en la relación entre el apoyo social y la conducta prosocial y antisocial en adolescentes chinos después del terremoto de Ya’an.
Método: Cuatro años y medio después del terremoto de Ya’an, 492 estudiantes de 13 a 18 años del condado de Lushan (98.6% de los 499 estudiantes encuestados) fueron evaluados utilizando el siguiente sistema: Cuestionario de Medidas de Exposición a Trauma, Cuestionario de Apoyo Social, Escala de Autocompasión, Inventario de Crecimiento Postraumático y Cuestionario de Problemas de Conducta Infantil.
Resultados: Cuando controlamos el género, la edad y la exposición traumática, el apoyo social tuvo un efecto positivo en el comportamiento prosocial. Más aún, el apoyo social tuvo un efecto indirecto y positivo en la conducta prosocial a través de la autocompasión positiva y el PTG, así como a través de una vía indirecta desde la autocompasión positiva al PTG, pero el apoyo social tuvo un efecto negativo en la conducta antisocial a través del PTG, así como a través de una vía indirecta desde la autocompasión positiva hacia el PTG en la conducta antisocial. El apoyo social también tuvo un efecto positivo en la conducta antisocial a través de la autocompasión negativa.
Conclusión: Los resultados sugieren que un mayor apoyo puede ser beneficioso para la conducta prosocial y reducir la conducta antisocial. La autocompasión y el PTG juegan un papel mediador significativo entre el apoyo social, la conducta prosocial y la conducta antisocial.
Palabras clave: apoyo social, autocompasión, PTG, conducta antisocial, conducta prosocial
背景:先前的研究表明, 社会支持, 自我同情和创伤后成长(PTG)可以影响亲社会行为和反社会行为, 但很少有研究考察它们在经历创伤事件的青少年群体中亲社会行为和反社会行为中的联合作用。
目的: 本研究旨在探讨自我同情与PTG在中国雅安地震后青少年的社会支持, 亲社会行为和反社会行为之间的中介作用。
方法:雅安地震发生四年半后, 采用创伤暴露测量问卷, 社会支持问卷, 自我同情量表, 创伤后成长量表和儿童行为问题问卷对芦山县492名13-18岁的中学生进行了评估。
结果:研究结果表明, 社会支持会促进亲社会行为并降低反社会行为水平。自我同情和PTG在社会支持, 亲社会行为和反社会行为之间发挥中介作用。
关键词: 社会支持, 自我同情, PTG, 反社会行为, 亲社会行为
1. Introduction
Traumatic experiences have a large impact on the physical and mental responses of individuals (Cisler et al., 2011; Ehring, Razik, & Emmelkamp, 2011; Feder et al., 2013). Previous studies have explored many internal psychological factors, such as posttraumatic individual cognition, emotion, and personality (Dunmore, Clark, & Ehlers, 1999; Ehlers & Clark, 2000; Gold et al., 2000), but there are few studies focused on behavioural problems among adolescents who have experienced traumatic events. Adolescence is an important period of individual mental health development (Steinberg, 2005), serious traumatic events may pose a major threat to their mental health, and the negative effects associated may last for a long time (Finkelhor, Ormrod, & Turner, 2007). At the same time, many behavioural responses of individuals are expressed through internal psychological factors, which can affect their academic studies and life overall. For this reason, the behavioural problems of adolescents after trauma have gradually become a focus of research.
Antisocial behaviour is considered to be a typical negative behavioural response after a traumatic event (Ford, Chapman, Connor, & Cruise, 2012). Antisocial behaviour is defined as a pattern of behaviour that ignores and infringes on the interests of others, such as assault, theft, and deception (American Psychiatric Association, 2013), and it is particularly common among adolescents who have experienced traumatic events (Cheng, Zhou, Chen, Zhang, & Wu, 2013). The different manifestations of antisocial behaviour will show different development trends with the physical and mental growth of adolescent (Tremblay, 2004). Previous studies in the field of post-traumatic adolescents have found that after controlling for gender and age, adolescents who experience traumatic events tend to exhibit higher levels of problem behaviour, including aggression, rule-breaking and other maladaptive behaviours (Moylan et al., 2010).
In contrast, some studies have found that traumatic experiences also lead to an increase in prosocial behaviour. Prosocial behaviour refers to the behaviour that individuals consciously do in a social environment that is favourable to others (Eisenberg, 2006). Staub and Vollhardt (2008) described this phenomenon as altruism born of suffering. Previous studies have shown that most survivors who have experienced negative events (Frazier et al., 2013), especially natural disasters (Kaniasty & Norris, 1995; Rao et al., 2011), showed different degrees of enhancement of prosocial behaviours. Further studies have shown that the level of prosocial behaviour changes with age for a specific group of adolescents who have experienced a traumatic event. In recent years, Chinese researchers have studied the prosocial behaviour of adolescents after the Wenchuan earthquake, and found that the prosocial behaviour of adolescents after trauma decreases with age (Qin et al., 2016).
From the previous research results, we know that both prosocial behaviour and antisocial behaviour could occur to adolescents who have experienced traumatic events (Eron & Huesmann, 1984; Gomà-i-Freixanet, 1995), so do they have the same or different influencing factors and internal mechanisms? To explore this issue, we have included prosocial behaviour and antisocial behaviour at the same time.
As an environmental resource, social support has always been the focus of researchers in the field of trauma psychology (Gold et al., 2000; Hyman, Gold, & Cott, 2003; Laffaye, Cavella, Drescher, & Rosen, 2008). Social support is defined as an individual’s perception of the support and help of others (Cobb, 1976). According to the social support resource theory, as an external protective resource, social support can provide an individual with continuous mental energy, so as to maintain them physical and mental health and ultimately affect his behavioural response. (Hobfoll, Freedy, Lane, & Geller, 1990). Based on the above theories, we can speculate that social support may play an important role in influencing prosocial behaviours and antisocial behaviours in posttraumatic adolescents.
Previous studies have confirmed this assumption. First, social support can reduce the possibility of antisocial behaviour. The social support deterioration deterrence model points out that social support can not only alleviate adverse emotional response in posttraumatic individuals, but also can reduce the occurrence of some antisocial behaviours, such as fights, theft, vandalism, etc. (Norris & Kaniasty, 1996). Some Chinese researchers have been found that social support reduces the incidence of antisocial behaviour, such as cheating, discipline violation, and aggression among left-behind children in China (Liu, Fan, & Shen, 2007). Hamama and Ronen-Shenhav (2012) also found that in Israeli teenagers from divorced families, the more social support they felt, the less antisocial behaviours they exhibited.
Social support can also promote, motivate, and reinforce prosocial behaviour. The theory of altruism born of suffering suggests that individuals who have experienced trauma are more likely to exhibit prosocial behaviour in order to return the help they received from others (Vollhardt, 2009). In a study of middle school students, it was found that individuals’ perceived levels of social support positively predicted their prosocial behaviours (Lenzi et al., 2012).
Nevertheless, the underlying mechanisms of the impact of social support on prosocial and antisocial behaviour after natural disasters remains unclear: how does social support improve survivors’ prosocial behaviour and decrease survivors’ antisocial behaviour? Through a literature review, it can be found that PTG is a common psychological reaction of individuals after trauma (Berger & Weiss, 2003), and it may play a role in the relationship between environmental factors and posttraumatic behavioural responses (Joseph, Murphy, & Regel, 2012). From the perspective of the relationship between social support and PTG, a large number of theories and studies have shown that social support can promote PTG. Calhoun and Tedeschi (2004) PTG model suggests that social support can provide a safe and warm environment for individuals who have experienced a traumatic event, in which individuals are more likely to openly express their emotions and feelings. This enables individuals to further reconstruct their cognition of the world and deeply consider the meaning of life in communication with others and self-reflection, thus promoting the development of PTG (Zhou, Wu, & Zhen, 2017). Laceulle, Kleber, and Alisic (2015) analysed the PTG levels of 1290 adolescents from the perspective of adolescent development. The results showed that there was a significant positive correlation between social support and PTG, and PTG decreased with age. In recent years, Chinese researchers have found that social support had a positive effect on PTG among adolescents after the Wenchuan earthquake (Jia, Ying, Zhou, Wu, & Lin, 2015).
In addition, PTG is also a significant factor affecting both prosocial and antisocial behaviours. Most studies on PTG and prosocial behaviour have found that PTG can promote prosocial behaviour (Staub & Vollhardt, 2008). In a study of Chinese middle school students who had experienced the earthquake, PTG was found to have a significantly positive effect on prosocial behaviour (Wang & Wu, 2020). Furthermore, PTG may also be associated with antisocial behaviour. Although there are very few empirical studies on children or adolescents in this field, the relationship between PTG and antisocial behaviour can be found in some theories. According to the social information-processing model (Holtzworth-Munroe, 1992), individuals who have experienced trauma tend to perceive and interpret incoming social stimuli as threatening and hostile, and this irrational belief may be the main cause of antisocial behaviour. A series of positive cognitive changes brought by PTG can effectively guide individuals to objectively evaluate the impact of traumatic events, reduce excessive vigilance and irrational beliefs in regards to the surrounding environment, and thus reduce the incidence of antisocial behaviours (Taft, Creech, & Kachadourian, 2012). Taken together, it is possible that social support can promote prosocial behaviour and reduce antisocial behaviour via PTG in post-disaster circumstances.
In addition, previous studies have shown that self-compassion, as an emotional regulation strategy (Neff, Kirkpatrick, & Rude, 2007), may mediate between social support and an individual’s post-traumatic behavioural response (Dunkel-Schetter, Folkman, & Lazarus, 1987). According to Neff (2003a), Self-compassion is an individual’s tolerance and compassion for himself in suffering. Self-compassion consists of six components: self-kindness, self-judgement, common humanity, isolation, mindfulness, and over-identification. Self-kindness is described as the tendency to be caring and inclusive towards one-self rather than indifference or judgemental. Common humanity refers to seeing one’s experience as a universal experience, rather than seeing one-self as the centre of pain that can lead to feelings of isolation. Mindfulness is supposed to be a clear and calm attitude towards the suffering of the moment rather than exaggerated with them.
In fact, previous studies suggest that self-compassion may not be a unidimensional construct. Instead, it may be constituted by both positive self-compassion (self-kindness, common humanity, and mindfulness) and negative self-compassion (self-judgement, isolation, and over-identification) (Gilbert, McEwan, Matos, & Rivis, 2011; Muris & Petrocchi, 2017; Neff, 2016). Researchers have also found that this two-dimensional structure may have more significance in the study of psychopathological symptoms than the unidimensional structure (Montero-Marin et al., 2016). Specifically, positive self-compassion was more strongly associated with positive mental health, while negative self-compassion was more strongly associated with negative mental outcomes (Gilbert et al., 2011; López et al., 2015). Therefore, in this study, self-compassion is divided into two dimensions: positive self-compassion and negative self-compassion.
From the perspective of the relationship between social support and positive self-compassion, some researchers found that increased social support is associated with increased positive self-compassion (Maheux & Price, 2016). In terms of the relationship between social support and negative self-compassion, Kahn (1965) argued that individuals with negative self-compassion often have a great sense of self-insecurity, while the safe atmosphere created by social support can increase a sense of security and belonging (Laurenceau, Barrett, & Pietromonaco, 1998), thereby reducing negative self-compassion.
Self-compassion may be associated with prosocial behaviour. Some researchers suggest that building the capacity for caring and accepting oneself in suffering can help extend compassion to multiple targets, including the self, others, and all sentient beings (Hofmann, Grossman, & Hinton, 2011). Empirical studies show that positive self-compassion may facilitate prosocial behaviour (Crocker & Canevello, 2008; Longe et al., 2009). However, individuals with higher negative self-compassion may focus on their own painful emotions and interpersonal estrangement from others, which may lead to social withdrawal and loneliness, neither of which are conducive to engaging in prosocial behaviours (Charmaz, 1980; Kahn, 1965).
There is also a correlation between self-compassion and antisocial behaviour. Positive self-compassion relieves negative emotions and reduces antisocial behaviour during setbacks and failures (Leary, Tate, Adams, Batts Allen, & Hancock, 2007). When dealing with interpersonal conflicts, individuals with higher levels of positive self-compassion are more willing to solve relationship problems in a peaceful and non-violent way (Neff & Beretvas, 2013). In a study of 251 male high school students, positive self-compassion among adolescents was found to significantly reduce antisocial behaviour (Barry, Loflin, & Doucette, 2015). On the other hand, individuals with negative self-compassion tend to have higher requirements of others (Kahn, 1965). If other people fail to meet their requirements for a long time, dissatisfaction, anger, and hostility may result, and antisocial behaviours may occur (Kahn, 1965; Milrod, 1972; Wilson, 1985).
While self-compassion and PTG are potential mediators of the relationship between social support, prosocial and antisocial behaviours, there is also a combined relationship among these two mediators. The self in relation model suggests that an individual’s attitude towards oneself is a key factor in promoting posttraumatic recovery and personal growth (Kaplan, 1986). Individuals with positive self-compassion are more likely to acknowledge suffering as part of the common human experience, which can help people gain insight from openly expressing their thoughts and feelings, thereby re-examining the meaning of the disaster and thinking more deeply about life, and thus promoting the development of PTG (Tedeschi & Calhoun, 2004). Indeed, the link between positive self-compassion and PTG has been demonstrated in empirical studies (Wong & Yeung, 2017). As the opposite of positive self-compassion, individuals with high levels of negative self-compassion hold negative and blaming attitudes towards themselves after traumatic events, and previous studies have shown that such negative self-attitudes will hinder PTG (Turner, Bernard, Birchwood, Jackson, & Jones, 2013). Individuals with negative self-compassion tend to regard themselves as the centre of pain after a traumatic event, amplifying negative emotions (Neff, 2003a), which may hinder PTG.
A review of previous literature shows that the relationship between social support, self-compassion, PTG, prosocial behaviour and antisocial behaviour has been verified by a large number of studies, but few studies have explored these factors in combination. More importantly, in previous studies that explored the mechanism of the individual’s post-traumatic behavioural responses, most of the subjects were taken from adults, but less focused on adolescents. To facilitate understanding of the relationship between the above variables, and to elucidate whether prosocial behaviour and antisocial behaviour share the same or different predictive mechanisms, the the present study aimed to: (1) examine the associations between social support and posttraumatic behavioural responses (prosocial and antisocial) in a sample of a middle school in Lushan; (2) investigate the potential mechanisms underlying the associations, including self-compassion and PTG. Based on the results of previous theoretical and empirical studies, a hypothesized model was established for further verification. Figure 1 shows the hypothesized model.
Figure 1.
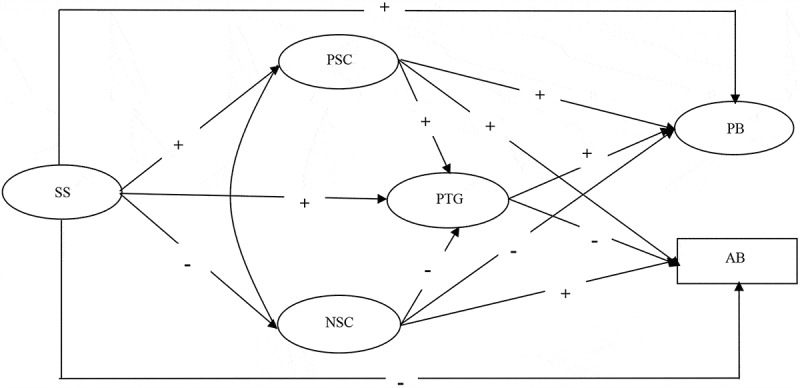
Hypothesized model of the mediating roles of self-compassion and PTG in the relationship between prosocial behaviour and antisocial behaviour. SS, social support; PB, prosocial behaviour; AB, antisocial behaviour; PTG, posttraumatic growth; NSC, negative self-compassion; PSC, positive self-compassion
2. Materials and methods
2.1. Procedure and participants
This study was conducted 4.5 years after the Ya’an earthquake. We focused on the area of Lushan County in Sichuan province, which was most severely affected by the earthquake. Before conducting the investigation, we first contacted the local education department and informed them of the objects, methods, and process of the survey for approval. After getting approval from relevant departments, we selected two middle schools in Lushan County in which to distribute our questionnaire.
With the assistance of the principals and psychology teachers of the two middle schools, we selected first and second grades of both junior high school and senior high school to conduct the investigation. A total of 499 middle school students participated in this survey. In order to accurately present the psychological characteristics of adolescents, we further selected 492 participants aged between 13 and 18 (accounting for 98.5% of the total participants) to be included in the study. All of the students who participated in the survey took a collective test in their own classes on the same day. The mean age of the adolescents at the time of measurement was 14.86 (SD = 1.51) years. Of the 492 students, 229 (46.5%) were male, and 263 (53.5%) were female. All participants had experienced the earthquake.
This study was approved by the Research Ethics Committee of relevant university and conducted with the permission of relevant leaders of participating schools. In the selected classes, all students who arrived at school on the day of the survey were recruited. All students in these classes agreed and were thus recruited to participate. There were no exclusion criteria, and compensation was not provided. The purpose of the study and the voluntary nature of the students’ participation were highlighted before the survey, and written informed consent was obtained from school principals, classroom teachers, and students.
The assessment was conducted under the supervision of the researchers. During the test, we asked the participants to read the instructions carefully and then fill in the questionnaire as required. All questionnaires were recalled immediately after completion. After the questionnaire packets were completed, the participants were told that school psychologists or teachers were available to provide any psychological/counselling services that they might need.
2.2. Measures
2.2.1. Trauma exposure
The trauma exposure questionnaire developed by Wu, Zhang, Lin, and Zang (2013) was used in this study. The questionnaire consisted of 18 items, including whether they had witnessed the trapped injury or death of others, and whether they were informed afterwards of the trapped injury or death of others. Each of the items was rated on a 3-point Likert scale, ranging from 1 (did not experience the situation above) to 3 (saw it myself). Finally, the scores of all subjects were added up as indicators of the degree of trauma exposure. The internal reliability of the questionnaire in this study was acceptable (Cronbach’s α = 0.65).
2.2.2. Social support
Social support was assessed using a modified version of the social net questionnaire (Zhou, Wu, & Zhen, 2017). This questionnaire is a 20-item instrument designed to measure the following forms of perceived social support. The questionnaire contains five components: Emotive support, instrumental support, companion, affirmative evaluation, and intimacy. All the items are rated on a 5-point Likert scale that ranges from 0 (completely disagree) to 4 (completely agree). In this study, the internal reliability of the modified inventory was good (Cronbach’s α = 0.65).
2.2.3. Self-compassion
Participants were given the 26-item Self-Compassion Scale (Neff, 2003b). The scale has six components, divided into positive self-compassion and negative self-compassion. Positive self-compassion includes common humanity, self-kindness, and mindfulness. Negative self-compassion includes feelings of isolation, self-judgement, and over-identification. All the items are rated on a 5-point Likert scale that ranges from 1 (completely disagree) to 5 (completely agree). In this study, the internal reliability of positive self-compassion (Cronbach’s α =.96) and negative self-compassion (α = 0.96) was good.
2.2.4. PTG
This study used a revised version of the posttraumatic growth questionnaire (Zhou et al., 2014). The original Posttraumatic Growth Inventory was developed by Tedeschi and Calhoun (1996). The revised scale adopted in this study includes the following three subscales, with a total of 22 items: Perceived changes in self, a changed sense of relationships with others, and a changed philosophy of life. Each of the 22 items is scored on a 6-point Likert scale that ranges from 0 (no change) to 5 (very great degree of change). The internal reliability of the modified inventory was good (Cronbach’s α = 0.96).
2.2.5. Antisocial behaviour
Antisocial behaviour was measured by the subscale of the Achenbach’s Youth Self–Report (YSR) version of Child Behaviour Checklist (Achenbach, Edelbrock, & Howell, 1987), in which items are reworded in first person and show good test–retest reliability and criterion validity among Chinese adolescents (Lan, Marci, & Moscardino, 2019). This scale contains nine items, all the items are rated on a 3-point Likert scale that ranges from 0 (none) to 2 (frequently). The internal reliability of the modified inventory was good (Cronbach’s α = 0.70).
2.2.6. Prosocial behaviour
This study was measured by the 15-item Prosocial Behaviours Scale, which was developed for Chinese adolescents (Zhang & Kou, 2008). The scale consists of four dimensions: altruism, commonweal-rule, interpersonal relationships, and personality traits. Participants were asked to rate each item from 1 (definitely does not apply to me) to 7 (definitely applies to me) on the Likert scale. In this study, the internal reliability of the modified inventory was good (α = 0.89).
2.3. Data analysis
SPSS 24.0 and Amos 17.0 software were used to analyse the data in this study. We evaluated the missing data before testing the hypothesis. Missing data at the item level were minimal in this study (i.e., less than 1.5% missing on each individual measure). Next, we adopted Little’s Missing Completely at Random test to check missing data pattern. The results revealed that data were missing in a non-random way. Therefore, the full information maximum likelihood (FIML) was used in this study to process the missing data (Schafer & Graham, 2002). Descriptive analysis was performed on all variables, and Pearson correlation analysis was used to test the correlation of main variables.
In order to study the mediating effect of self-compassion and PTG, we established a structural equation model (SEM). The social support latent variable was evaluated in terms of emotive support, instrumental support, companion, affirmative evaluation, and intimacy. Positive self-compassion latent variable was evaluated in terms of common humanity, self-kindness, and mindfulness, whereas the negative self-compassion latent variable was evaluated in terms of isolation, self-judgement, and over-identification. The PTG latent variable was evaluated in terms of perceived changes in the self, a changed sense of relationships with others, and a changed philosophy of life. Finally, the prosocial behaviour latent variable was evaluated in terms of altruism, commonweal-rule, interpersonal relationships, and personality traits.
Next, we applied the SEM approach to assess the following models: (a) a direct effect model with structural paths from social support to prosocial behaviour and antisocial behaviour; (b) an indirect effect model, with the mediators (e.g., positive self-compassion, negative self-compassion, and PTG) inserted between social support and prosocial and antisocial behaviour. Figure 1 shows the hypothesized model.
3. Results
3.1. Descriptive statistics and correlations among main measures
The results of description statistics and correlation analysis of main measures are shown in Table 1. According to Pearson’s correlation analysis, gender was significantly associated with social support, negative self-compassion, prosocial behaviour, and antisocial behaviour. Age was significantly associated with social support. There was no significant correlation between traumatic exposure and other variables, and there was no significant correlation between positive self-compassion and antisocial behaviour. The correlation between other main variables was significant.
Table 1.
Means, standard deviations, and correlations of main variables
| Variable | M | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 Gendera | – | – | – | ||||||||
| 2 Age | 14.86 | 1.516 | −0.10 | – | |||||||
| 3 Trauma exposure | 20.82 | 4.32 | 0.04 | 0.02 | – | ||||||
| 4 Social support | 45.37 | 17.38 | 0.23*** | −0.11* | 0.00 | – | |||||
| 5 PSC | 39.31 | 8.59 | 0.07 | 0.02 | −0.05 | 0.36*** | – | ||||
| 6 NSC | 37.80 | 8.92 | 0.16** | 0.08 | −0.04 | 0.19*** | 0.50*** | – | |||
| 7 PTG | 54.49 | 15.05 | −0.03 | −0.02 | −0.06 | 0.43*** | 0.32*** | 0.12** | – | ||
| 8 Prosocial behaviour | 70.49 | 18.06 | 0.10* | 0.01 | −0.05 | 0.48*** | 0.41*** | 0.21*** | 0.42*** | – | |
| 9 Antisocial behaviour | 2.08 | 2.86 | −0.20*** | −0.07 | −0.01 | −0.11* | −0.01 | 0.11* | −0.13** | −0.17*** | – |
codeda: 1, Male; 2, Female; PSC, positive self-compassion; NSC, negative self-compassion; PTG, posttraumatic growth.
*p <.05. **p <.01. ***p <.001.
3.2. Analysis of mediating effect
In this study, the SEM was used to examine the hypothesized model of the mediating roles of self-compassion and PTG in the relationship between social support and prosocial/antisocial behaviour. (see Figure 1). According to the suggestions of Anderson and Gerbing (1988), we first tested the measurement model (see Figure 2). The measurement model included five latent variable constructs: social support, positive self-compassion, negative self-compassion, PTG, and prosocial behaviour. we found that the model fitting index was acceptable [χ2/df = 4.12, CFI = 0.94, TLI = 0.93, RMSEA(90%CI) = 0.079(0.073 - 0.086)]. Further structural model analysis is possible.
Figure 2.
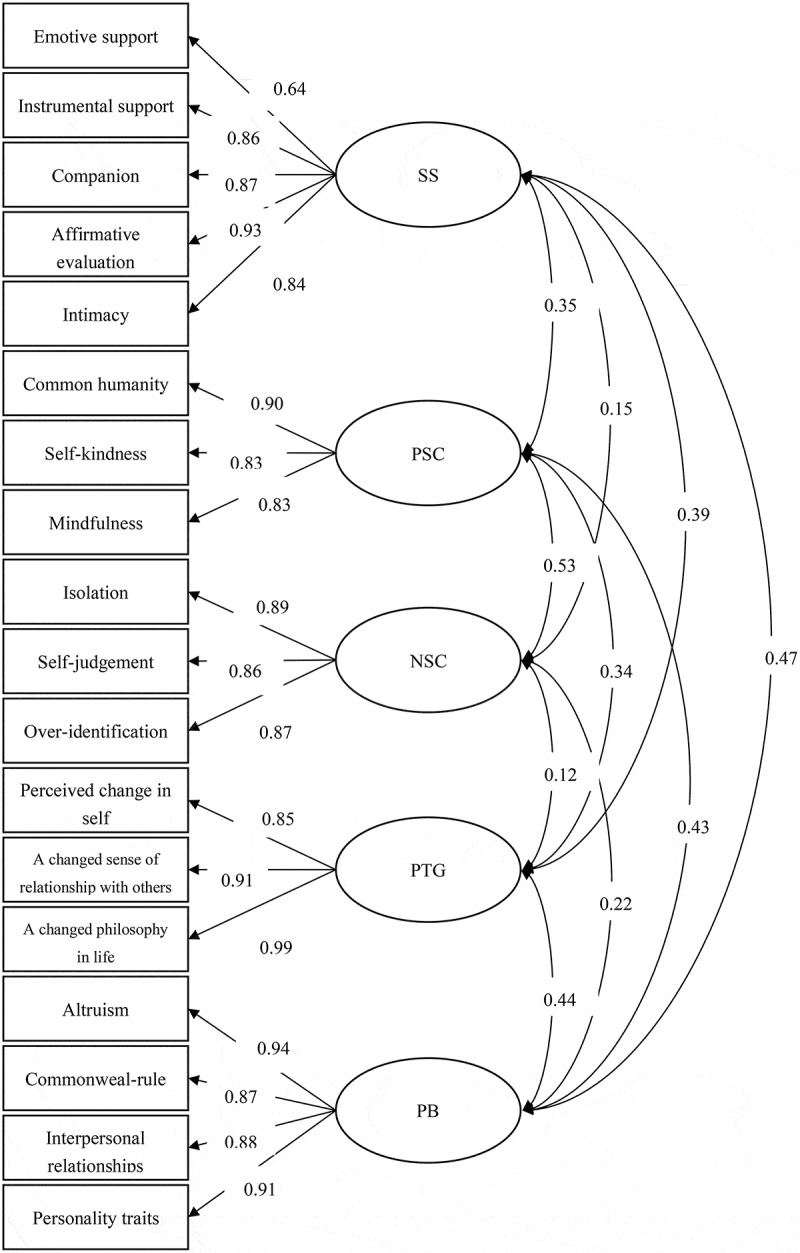
Measurement model. SS, social support; PB, prosocial behaviour; AB, antisocial behaviour; PTG, posttraumatic growth; NSC, negative self-compassion; PSC, positive self-compassion
In the direct effects model, we added gender, age, and trauma exposure as control variables, and established three predictive paths from control variables to social support, prosocial behaviour, and antisocial behaviour. After controlling for trauma exposure, we analysed the direct effects of social support on prosocial behaviours and antisocial behaviour (see Figure 3). Factor loadings for the manifest indicators on their respective latent variables were estimated freely. The results show that the direct effect model fits well [χ2/df = 4.21, CFI = 0.97, TLI = 0.96, RMSEA(90%CI) = 0.078(0.069 - 0.090)]. Direct effect path analysis revealed that social support had a positive effect on prosocial behaviour, but a negative effect on antisocial behaviour.
Figure 3.
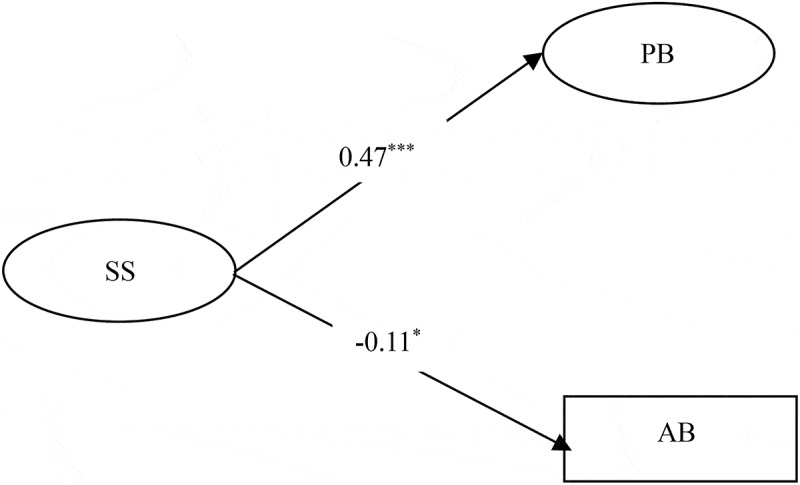
Direct effects model. SS, social support; PB, prosocial behaviour; AB, antisocial behaviour; PTG, posttraumatic growth; NSC, negative self-compassion; PSC, positive self-compassion
*p <.05. **p <.01. ***p <.001.
Next, we inserted the mediators (positive self-compassion, negative self-compassion, and PTG) between social support, prosocial behaviour, and antisocial behaviour. Similarly, in the indirect effects model, we used gender, age, and trauma exposure as control variables and established predictive paths from control variables to social support, self-compassion, PTG, prosocial behaviour, and antisocial behaviour. In addition, we added two predictive paths from positive self-compassion and negative self-compassion to PTG. Because positive self-compassion and negative self-compassion are extracted from self-compassion, we established a correlation path between them. At the same time, we added two predictive paths between positive/negative self-compassion and PTG. We found that this indirect effect model also fit the data well [χ2/df = 2.85, CFI = 0.96, TLI = 0.95, RMSEA(90%CI) = 0.061(0.055 - 0.068)].
In view of the good fitting index of the indirect effect model, we did not modify the path according to the modification indices. The final results of path analyses are shown in Figure 4. Social support had a positive effect on prosocial behaviour, but had no significant effect on antisocial behaviour. Moreover, social support had an indirect and positive effect on prosocial behaviour via positive self-compassion and PTG, as well as via an indirect path from positive self-compassion to PTG. Social support had a negative effect on antisocial behaviour via PTG, as well as via an indirect path from positive self-compassion to PTG on antisocial behaviour. Social support also had a positive effect on antisocial behaviour via negative self-compassion.Figure 4
Figure 4.
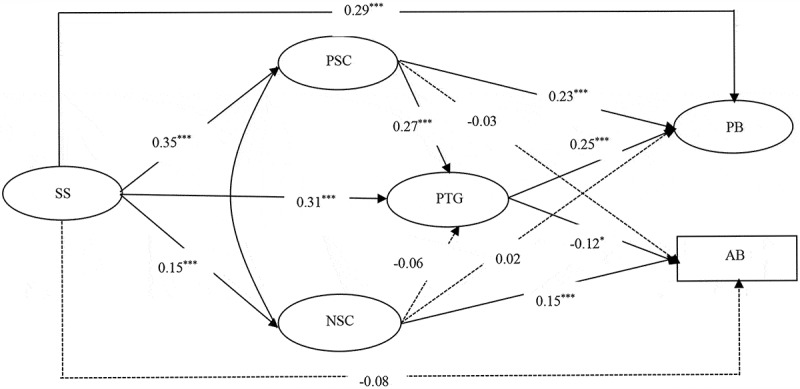
Indirect effects model. Note: SS, social support; PB, prosocial behaviour; AB, antisocial behaviour; PTG, posttraumatic growth; NSC, negative self-compassion; PSC, positive self-compassion
*p <.05. **p <.01. ***p <.001.
Finally, bias-corrected bootstrap tests were performed on the path with significant indirect effect in the path analysis. Table 2 illustrates the results of these tests. The 95% confidence interval of the above mediating effect did not contain 0, and the mediating effect was significant. The indirect effect accounts for 43% of the total effect.
Table 2.
Bias-corrected bootstrap tests of mediating effects
| Path | Standardized β | Standardized 95% CI |
|
|---|---|---|---|
| Low High | |||
| SS-PSC-PB | 0.08*** | 0.06 | 0.31 |
| SS-NSC-AB | 0.02** | 0.01 | 0.06 |
| SS-PTG-PB | 0.08*** | 0.06 | 0.15 |
| SS-PTG-AB | −0.04** | −0.05 | −0.01 |
| SS-PSC-PTG-PB | 0.02** | 0.01 | 0.05 |
| SS-PSC-PTG-AB | −0.01* | −0.01 | −0.01 |
SS, social support; PB, prosocial behaviour; AB, antisocial behaviour; PTG, posttraumatic growth; NSC, negative self-compassion; PSC, positive self-compassion. *p <.05. **p <.01. ***p <.001.
4. Discussion
4.1. Effect of social support on prosocial behaviour and antisocial behaviour
The current study examined the mediating roles of self-compassion and PTG in the relationship between social support and prosocial and antisocial behaviour. After controlling for gender, age, and traumatic exposure, the results revealed that social support had a positive effect on prosocial behaviour, which confirms the altruism born of suffering theory (Vollhardt, 2009) and previous studies (Lenzi et al., 2012). That is to say, individuals with high levels of social support tend to show more interpersonal kindness, and individuals who received kindness and help from others were more likely to exhibit prosocial behaviour in return for support (Twenge, Baumeister, Dewall, Ciarocco, & Bartels, 2007).
The results that social support had a negative effect on antisocial behaviour verified the social support deterioration deterrence model (Norris & Kaniasty, 1996) and previous research (Liu, Fan, & Shen, 2007). Namely, social support can provide a safe and stable environment. In this environment, adolescents can realize a full sense of security, which is not inclined to overestimate potential threats in the environment and redresses the irrational belief that the world is full of hostility and dangers, thus reducing the possibility of antisocial behaviour. However, this study found that the direct path was not significant after inserting PTG and self-compassion. The direct effect of social support on prosocial and antisocial behaviour was explained by mediating variables.
4.2. Mediating effect of self-compassion and PTG
When we controlled for age, gender, and trauma exposure, our study found that social support had a positive effect on prosocial behaviour, but a negative effect on antisocial behaviour via PTG. The role of PTG in social support and prosocial behaviour is supported by Calhoun and Tedeschi’s (2004) PTG model. Social support provides the emotional support for post-earthquake adolescents to rethink themselves, others, and the world (Zhou, Wu, & Zhen, 2017), which helps to promote individual relationships with others and makes the adolescents more willing to engage in emotional communication with others (Rimé, 2009). In communication with others, adolescents rethink the meaning of suffering, gradually realizing PTG (García, Cova, Rincón, Vázquez, & Páez, 2016). The series of positive changes, such as the realization of PTG, interpersonal relationships, and life values, will further encourage adolescents to be ready to help others and actively participate in public welfare activities, promoting prosocial behaviour.
At the same time, the role of PTG in social support and antisocial behaviour supported the social information-processing model (Holtzworth-Munroe, 1992). Improvement in PTG level can help adolescents adjust their cognitive biases effectively and correct their unreasonable beliefs and excessive vigilance and hostility towards the surrounding environment. This enables adolescents to better manage their emotions, thus effectively reducing the occurrence of antisocial behaviours (Taft et al., 2012).
Importantly, we found that adolescents with social support were able to promote prosocial behaviour through positive self-compassion. We believe that social support can provide a safe and stable environment for adolescents so that their needs, beliefs, attitudes, and values can be respected and they can feel more kindness and care (Laurenceau et al., 1998). In this environment, adolescents are more likely to view suffering as an event that all people are likely to experience, thereby increasing the level of individual self-compassion. High levels of positive self-compassion can help adolescents extend compassion and care to others (Hofmann et al., 2011) and gradually show more prosocial behaviour. However, we found that social support did not affect antisocial behaviour through positive self-compassion. The results suggest that positive self-compassion may not have an effect on antisocial behaviour alone, which may require some cognitive factors to be processed.
Our study also found that social support had a positive effect on antisocial behaviours through negative self-compassion. This result suggests that sustained excessive social support may reduce self-efficacy in coping with trauma and increase self-powerlessness long after the occurrence of traumatic events (Bolger & Amarel, 2007). This triggers more negative emotions in adolescents. Individuals with higher levels of negative self-compassion are more immersed in their own painful emotions, and thus isolated from others. In the long run, this may lead to tension and conflict in individual interpersonal relationships, thus increasing the incidence of antisocial behaviours.
Moreover, the current study also found that social support had a two-mediator indirect effect on antisocial behaviour through positive self-compassion via PTG. The caring and respectful environment provided by social support improves the level of individuals’ positive self-compassion, and high levels of positive self-compassion tend to result in a focus on the present situation with a calm and peaceful attitude and a more objective view of suffering. This can encourage individuals to think clearly about suffering and the meaning of life and generate new thoughts on interpersonal self-cognition and life values, thus promoting the generation and development of PTG. The improvement of PTG brings about a series of positive changes in self-cognition that can further promote prosocial behaviours of adolescents and reduce antisocial behaviours.
Finally, our study found that social support could not affect prosocial behaviour either through negative self-compassion or through both PTG and negative self-compassion. This suggests that positive and negative self-compassion play different roles in social support and prosocial behaviour. Prosocial behaviour is a kind of behaviour which is beneficial to others when individuals devote themselves to social activities (Eisenberg, 2006). But adolescents with negative self-compassion focus on the experience of negative events and exaggerate the fear and pain of disaster events, resulting in loneliness, social withdrawal, and difficulty with active involvement in social activities. Thus, negative self-compassion in relationship between social support and prosocial behaviour was not significant.
There are several limitations of this study that need to be mentioned. First, this study used a self-reported scale, so the results may be affected by common-method variance. Second, our study adopted a cross-sectional study design, in which it is not possible to explore the relationship between variables over time. A longitudinal research design could be adopted in subsequent studies. In addition, adolescents are in important stage of physical and mental development, the cognitive level, ability to cope with trauma, and post-traumatic behavioural response of individuals will change with age. Therefore, exploring the relationship between social support, self-compassion, PTG, prosocial behaviour and antisocial behaviour from a development perspective should be considered in future longitudinal research.
Despite the above limitations, the results of this study not only enrich the current empirical research, but also provide guidance and advice to the psychological workers in the disaster areas. The present study highlights that psychological workers should provide appropriate social support for adolescents when conducting psychological interventions in the behavioural responses of adolescents after disaster. Specifically, it is important to create a warm and safe environment for posttraumatic adolescents, which can improve levels of positive self-compassion, promoting prosocial behaviour. However, excessive attention and support should be avoided, which can increase the level of negative self-compassion in adolescents, thus promoting antisocial behaviour. In addition, while focusing on cultivating adolescents’ positive self-compassion, it is also necessary to guide them to rethink positively about traumatic events, promote the realization of PTG, and thus increase individual prosocial behaviour.
Funding Statement
This work was supported by the National Natural Science Foundation of China [grant number: 32071085].
Disclosure statement
No potential conflict of interest was reported by the authors.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to the containing information that could compromise the privacy of research participants.
References
- Achenbach, T. M., Edelbrock, C., & Howell, C. T. (1987). Empirically based assessment of the behavioral and emotional problems of 2–and 3–year-old children. Journal of Abnormal Child Psychology, 15(4), 629–12. doi: 10.1007/bf00917246 [DOI] [PubMed] [Google Scholar]
- American Psychiatric Association . (2013). Diagnostic and statistical manual of mental disorders. Arlington, VA: Author. [Google Scholar]
- Anderson, J. C., & Gerbing, D. W. (1988). Structural equation modeling in practice: A review and recommended two-step approach. Psychological Bulletin, 103(3), 411–423. doi: 10.1037/0033-2909.103.3.411 [DOI] [Google Scholar]
- Barry, C. T., Loflin, D. C., & Doucette, H. (2015). Adolescent self-compassion: Associations with narcissism, self-esteem, aggression, and internalizing symptoms in at-risk males. Personality and Individual Differences, 77, 118–123. doi: 10.1016/j.paid.2014.12.036 [DOI] [Google Scholar]
- Berger, R., & Weiss, T. (2003). Immigration and posttraumatic growth: A missing link. Journal of Immigrant and Refugee Services, 1(2), 21–39. doi: 10.1300/j191v01n02_02 [DOI] [Google Scholar]
- Bolger, N., & Amarel, D. (2007). Effects of social support visibility on adjustment to stress: Experimental evidence. Journal of Personality and Social Psychology, 92(3), 458–475. [DOI] [PubMed] [Google Scholar]
- Calhoun, L. G., & Tedeschi, R. G. (2004). The foundations of posttraumatic growth: New considerations. Psychological Inquiry, 15(1), 93–102. [Google Scholar]
- Charmaz, K. C. (1980). The social construction of self-pity in the chronically ill. Studies in Symbolic Interaction, 3, 123–145. [Google Scholar]
- Cheng, K., Zhou, X., Chen, Q., Zhang, C., & Wu, X. (2013). The effect of posttraumatic stress disorder on aggressive behavior after the Wenchuan earthquake: The moderating effect of coping style. Psychological Development and Education, 29, 649–656. [Google Scholar]
- Cisler, J. M., Amstadter, A. B., Begle, A. M., Resnick, H. S., Danielson, C. K., Saunders, B. E., & Kilpatrick, D. G. (2011). PTSD symptoms, potentially traumatic event exposure, and binge drinking: A prospective study with a national sample of adolescents. Journal of Anxiety Disorders, 25(7), 978–987. doi: 10.1016/j.janxdis.2011.06.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cobb, S. (1976). Social support as a moderator of life stress. Psychosomatic Medicine, 38(5), 300–314. doi: 10.1097/00006842-197609000-00003 [DOI] [PubMed] [Google Scholar]
- Crocker, J., & Canevello, A. (2008). Creating and undermining social support in communal relationships: The role of compassionate and self–image goals. Journal of Personality and Social Psychology, 95(3), 555–575. doi: 10.1037/0022-3514.95.3.555 [DOI] [PubMed] [Google Scholar]
- Dunkel-Schetter, C., Folkman, S., & Lazarus, R. S. (1987). Correlates of social support receipt. Journal of Personality and Social Psychology, 53(1), 71–80. doi: 10.1037/0022-3514.53.1.71 [DOI] [PubMed] [Google Scholar]
- Dunmore, E., Clark, D. M., & Ehlers, A. (1999). Cognitive factors involved in the onset and maintenance of posttraumatic stress disorder (PTSD) after physical or sexual assault. Behaviour Research and Therapy, 37, 809–829. doi: 10.1016/s0005-7967(98)00181-8 [DOI] [PubMed] [Google Scholar]
- Ehlers, A., & Clark, D. M. (2000). A cognitive model of posttraumatic stress disorder. Behaviour Research and Therapy, 38, 319–345. doi: 10.1016/s0005-7967(01)00123-1 [DOI] [PubMed] [Google Scholar]
- Ehring, T., Razik, S., & Emmelkamp, P. M. (2011). Prevalence and predictors of posttraumatic stress disorder, anxiety, depression, and burnout in Pakistani earthquake recovery workers. Psychiatry Research, 185(1–2), 161–166. doi: 10.1016/j.psychres.2009.10.018 [DOI] [PubMed] [Google Scholar]
- Eisenberg, N. (2006). Empathy-related responding and prosocial behavior. New Jersey: John Wiley & Sons Press. [Google Scholar]
- Eron, L. D., & Huesmann, L. R. (1984). The relation of prosocial behavior to the development of aggression and psychopathology. Aggressive Behavior, 10(3), 201–211. doi: [DOI] [Google Scholar]
- Feder, A., Ahmad, S., Lee, E. J., Morgan, J. E., Singh, R., Smith, B. W., & Charney, D. S. (2013). Coping and PTSD symptoms in Pakistani earthquake survivors: Purpose in life, religious coping and social support. Journal of Affective Disorders, 147(1–3), 156–163. doi: 10.1016/j.jad.2012.10.027 [DOI] [PubMed] [Google Scholar]
- Finkelhor, D., Ormrod, R. K., & Turner, H. A. (2007). Re-victimization patterns in a national longitudinal sample of children and youth. Child Abuse & Neglect, 31(5), 479–502. doi: 10.1016/j.chiabu.2006.03.012 [DOI] [PubMed] [Google Scholar]
- Ford, J. D., Chapman, J., Connor, D. F., & Cruise, K. R. (2012). Complex trauma and aggression in secure juvenile justice settings. Criminal Justice and Behavior, 39(6), 694–724. doi: 10.1177/0093854812436957 [DOI] [Google Scholar]
- Frazier, P., Greer, C., Gabrielsen, S., Tennen, H., Park, C., & Tomich, P. (2013). The relation between trauma exposure and prosocial behavior. Psychological Trauma: Theory, Research, Practice, and Policy, 5(3), 286–294. doi: 10.1037/a0027255 [DOI] [Google Scholar]
- García, F. E., Cova, F., Rincón, P., Vázquez, C., & Páez, D. (2016). Coping, rumination, and posttraumatic growth in people affected by an earthquake. Psicothema, 28(1), 59–65. doi: 10.1037/a0027255 [DOI] [PubMed] [Google Scholar]
- Gilbert, P., McEwan, K., Matos, M., & Rivis, A. (2011). Fears of compassion: Development of three self-report measures. Psychology and Psychotherapy: Theory, Research and Practice, 84(3), 239–255. doi: 10.1348/147608310x526511 [DOI] [PubMed] [Google Scholar]
- Gold, P. B., Engdahl, B. E., Eberly, R. E., Blake, R. J., Page, W. F., & Frueh, B. C. (2000). Trauma exposure, resilience, social support, and PTSD construct validity among former prisoners of war. Social Psychiatry and Psychiatric Epidemiology, 35, 36–42. doi: 10.1007/s001270050006 [DOI] [PubMed] [Google Scholar]
- Gomà-i-Freixanet, M. (1995). Prosocial and antisocial aspects of personality. Personality and Individual Differences, 19(2), 125–134. doi: 10.1016/s0191-8869(00)00121-5 [DOI] [Google Scholar]
- Hamama, L., & Ronen-Shenhav, A. (2012). Self-control, social support, and aggression among adolescents in divorced and two-parent families. Children and Youth Services Review, 34(5), 1042–1049. doi: 10.1016/j.childyouth.2012.02.009 [DOI] [Google Scholar]
- Hobfoll, S. E., Freedy, J., Lane, C., & Geller, P. (1990). Conservation of social resources: Social support resource theory. Journal of Social and Personal Relationships, 7(4), 465–478. doi: 10.1177/0265407590074004 [DOI] [Google Scholar]
- Hofmann, S. G., Grossman, P., & Hinton, D. E. (2011). Loving-kindness and compassion meditation: Potential for psychological interventions. Clinical Psychology Review, 31(7), 1126–1132. doi: 10.1016/j.cpr.2011.07.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Holtzworth-Munroe, A. (1992). Social skill deficits in maritally violent men: Interpreting the data using a social information processing model. Clinical Psychology Review, 12(6), 605–617. doi: 10.1016/0272-7358(92)90134-T [DOI] [Google Scholar]
- Hyman, S. M., Gold, S. N., & Cott, M. A. (2003). Forms of social support that moderate PTSD in childhood sexual abuse survivors. Journal of Family Violence, 18(5), 295–300. doi: 10.1023/a:1025117311660 [DOI] [Google Scholar]
- Jia, X., Ying, L., Zhou, X., Wu, X., & Lin, C. (2015). The effects of extraversion, social support on the posttraumatic stress disorder and posttraumatic growth of adolescent survivors of the Wenchuan earthquake. PLoS ONE, 10(3), e0121480. doi: 10.1371/journal.pone.0121480 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Joseph, S., Murphy, D., & Regel, S. (2012). An affective–cognitive processing model of post‐traumatic growth. Clinical Psychology & Psychotherapy, 19(4), 316–325. doi: 10.1002/cpp.1798 [DOI] [PubMed] [Google Scholar]
- Kahn, E. (1965). Self-pity. American Journal of Psychiatry, 122(4), 447–451. [DOI] [PubMed] [Google Scholar]
- Kaniasty, K., & Norris, F. H. (1995). Mobilization and deterioration of social support following natural disasters. Current Directions in Psychological Science, 4(3), 94–98. doi: 10.1111/1467-8721.ep10772341 [DOI] [Google Scholar]
- Kaplan, A. (1986). The “self-in-relation”: Implications for depression in women. Psychotherapy: Theory, Research, Practice, Training, 23(2), 234–242. doi: 10.1037/h0085603 [DOI] [Google Scholar]
- Laceulle, O. M., Kleber, R. J., & Alisic, E. (2015). Children’s experience of posttraumatic growth: Distinguishing general from domain-specific correlates. PLoS ONE, 10(12), e0145736. doi: 10.1371/journal.pone.0145736 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Laffaye, C., Cavella, S., Drescher, K., & Rosen, C. (2008). Relationships among PTSD symptoms, social support, and support source in veterans with chronic PTSD. Journal of Traumatic Stress: Official Publication of the International Society for Traumatic Stress Studies, 21(4), 394–401. doi: 10.1002/jts.20348 [DOI] [PubMed] [Google Scholar]
- Lan, X., Marci, T., & Moscardino, U. (2019). Parental autonomy support, grit, and psychological adjustment in Chinese adolescents from divorced families. Journal of Family Psychology, 33(5), 511–520. doi: 10.1037/fam0000514 [DOI] [PubMed] [Google Scholar]
- Laurenceau, J. P., Barrett, L. F., & Pietromonaco, P. R. (1998). Intimacy as an interpersonal process: The importance of self-disclosure, partner disclosure, and perceived partner responsiveness in interpersonal exchanges. Journal of Personality and Social Psychology, 74(5), 1238–1251. doi: 10.1037/0022-3514.74.5.1238 [DOI] [PubMed] [Google Scholar]
- Leary, M. R., Tate, E. B., Adams, C. E., Batts Allen, A., & Hancock, J. (2007). Self-compassion and reactions to unpleasant self-relevant events: The implications of treating oneself kindly. Journal of Personality and Social Psychology, 92(5), 887–904. doi: 10.1037/0022-3514.92.5.887 [DOI] [PubMed] [Google Scholar]
- Lenzi, M., Vieno, A., Perkins, D. D., Pastore, M., Santinello, M., & Mazzardis, S. (2012). Perceived neighborhood social resources as determinants of prosocial behavior in early adolescence. American Journal of Community Psychology, 50(1–2), 37–49. doi: 10.1007/s10464-011-9470-x [DOI] [PubMed] [Google Scholar]
- Liu, X., Fan, X. H., & Shen, J. L. (2007). Relationship between social support and problem behaviors of the left-home-kids in junior middle school. Psychological Development and Education, 23, 98–102. doi: 10.3969/j.issn.1001-4918.2007.03.017 [DOI] [Google Scholar]
- Longe, O., Maratos, F. A., Gilbert, P., Evans, G., Volker, F., Rockliff, H., & Rippon, G. (2009). Having a word with yourself: Neural correlates of self-criticism and self-reassurance. NeuroImage, 49(2), 1849–1856. doi: 10.1016/j.neuroimage.2009.09.019 [DOI] [PubMed] [Google Scholar]
- López, A., Sanderman, R., Smink, A., Zhang, Y., Sonderen, E., Ranchor, A., & Schroevers, M. J. (2015). A reconsideration of the self-compassion scale’s total score: Self-compassion versus self-criticism. PLoS ONE, 10(7), e0132940. doi: 10.1371/journal.pone.0132940 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maheux, A., & Price, M. (2016). The indirect effect of social support on post-trauma psychopathology via self-compassion. Personality and Individual Differences, 88, 102–107. doi: 10.1016/j.paid.2015.08.051 [DOI] [Google Scholar]
- Milrod, D. (1972). Self-pity, self-comforting, and the superego. The Psychoanalytic Study of the Child, 27(1), 505–528. doi: 10.1080/00797308.1972.11822726 [DOI] [Google Scholar]
- Montero-Marín, J., Gaete, J., Demarzo, M., Rodero, B., Lopez, L. C. S., & García-Campayo, J. (2016). Self-criticism: A measure of uncompassionate behaviors toward the self, based on the negative components of the self-compassion scale. Frontiers in Psychology, 7, 1281. doi: 10.3389/fpsyg.2016.01281 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moylan, C. A., Herrenkohl, T. I., Sousa, C., Tajima, E. A., Herrenkohl, R. C., & Russo, M. J. (2010). The effects of child abuse and exposure to domestic violence on adolescent internalizing and externalizing behavior problems. Journal of Family Violence, 25(1), 53–63. doi: 10.1007/s10896-009-9269-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muris, P., & Petrocchi, N. (2017). Protection or vulnerability? A meta‐analysis of the relations between the positive and negative components of self‐compassion and psychopathology. Clinical Psychology & Psychotherapy, 24(2), 373–383. doi: 10.1002/cpp.2005 [DOI] [PubMed] [Google Scholar]
- Neff, K. D. (2003a). Self-compassion: An alternative conceptualization of a healthy attitude towards oneself. Self and Identity, 2(2), 85–101. doi: 10.1080/15298860309032 [DOI] [Google Scholar]
- Neff, K. D. (2003b). The development and validation of a scale to measure self-compassion. Self and Identity, 2(3), 223–250. doi: 10.1080/15298860309027 [DOI] [Google Scholar]
- Neff, K. D. (2016). Does self-compassion entail reduced self-judgment, isolation, and over-identification? A response to Muris, Otgaar, and Petrocchi (2016). Mindfulness, 7(3), 791–797. doi: 10.1007/s12671-016-0531-y. [DOI] [Google Scholar]
- Neff, K. D., & Beretvas, S. N. (2013). The role of self-compassion in romantic relationships. Self and Identity, 12(1), 78–98. doi: 10.1080/15298868.2011.639548 [DOI] [Google Scholar]
- Neff, K. D., Kirkpatrick, K. L., & Rude, S. S. (2007). Self-compassion and adaptive psychological functioning. Journal of Research in Personality, 41(1), 139–154. doi: 10.1016/j.jrp.2006.03.004 [DOI] [Google Scholar]
- Norris, F. H., & Kaniasty, K. (1996). Received and perceived social support in times of stress: A test of the social support deterioration deterrence model. Journal of Personality and Social Psychology, 71(3), 498–511. doi: 10.1037/0022-3514.71.3.498 [DOI] [PubMed] [Google Scholar]
- Qin, Y., Zhou, Y., Fan, F., Chen, S., Huang, R., Cai, R., & Peng, T. (2016). Developmental trajectories and predictors of prosocial behavior among adolescents exposed to the 2008 Wenchuan earthquake. Journal of Traumatic Stress, 29(1), 80–87. doi: 10.1007/s10964-017-0786-1 [DOI] [PubMed] [Google Scholar]
- Rao, L. L., Han, R., Ren, X. P., Bai, X. W., Zheng, R., Liu, H., & Li, S. (2011). Disadvantage and prosocial behavior: The effects of the Wenchuan earthquake. Evolution and Human Behavior, 32(1), 63–69. doi: 10.1016/j.evolhumbehav.2010.07.002 [DOI] [Google Scholar]
- Rimé, B. (2009). Emotion elicits the social sharing of emotion: Theory and empirical review. Emotion Review, 1(1), 60–85. doi: 10.1177/1754073908097189 [DOI] [Google Scholar]
- Schafer, J. L., & Graham, J. W. (2002). Missing data: Our view of the state of the art. Psychological Methods, 7(2), 147–177. doi: 10.1037/1082-989X.7.2.147 [DOI] [PubMed] [Google Scholar]
- Staub, E., & Vollhardt, J. (2008). Altruism born of suffering: The roots of caring and helping after victimization and other trauma. American Journal of Orthopsychiatry, 78(3), 267–280. doi: 10.1037/a0014223 [DOI] [PubMed] [Google Scholar]
- Steinberg, L. (2005). Cognitive and affective development in adolescence. Trends in Cognitive Sciences, 9(2), 69–74. doi: 10.1037/a0014223 [DOI] [PubMed] [Google Scholar]
- Taft, C. T., Creech, S. K., & Kachadourian, L. (2012). Assessment and treatment of posttraumatic anger and aggression: A review. The Journal of Rehabilitation Research and Development, 49(5), 777–788. doi: 10.1682/jrrd.2011.09.0156 [DOI] [PubMed] [Google Scholar]
- Tedeschi, R. G., & Calhoun, L. G. (1996). The posttraumatic growth inventory: Measuring the positive legacy of trauma. Journal of Traumatic Stress, 9(3), 455–471. [DOI] [PubMed] [Google Scholar]
- Tedeschi, R. G., & Calhoun, L. G. (2004). Posttraumatic growth: Conceptual foundations and empirical evidence. Psychological Inquiry, 15(1), 1–18. doi: 10.1207/s15327965pli1501_01 [DOI] [Google Scholar]
- Tremblay, R. E. (2004). Decade of behavior distinguished lecture: Development of physical aggression during infancy. Infant Mental Health Journal: Official Publication of The World Association for Infant Mental Health, 25(5), 399–407. [Google Scholar]
- Turner, M. H., Bernard, M., Birchwood, M., Jackson, C., & Jones, C. (2013). The contribution of shame to post-psychotic trauma. British Journal of Clinical Psychology, 52(2), 162–182. doi: 10.1111/bjc.12007 [DOI] [PubMed] [Google Scholar]
- Twenge, J. M., Baumeister, R. F., Dewall, C. N., Ciarocco, N. J., & Bartels, J. M. (2007). Social exclusion decreases prosocial behavior. Journal of Personality and Social Psychology, 92(1), 55–56. doi: 10.1037/0022-3514.92.1.56 [DOI] [PubMed] [Google Scholar]
- Vollhardt, J. R. (2009). Altruism born of suffering and prosocial behavior following adverse life events: A review and conceptualization. Social Justice Research, 22(1), 53–97. doi: 10.1007/s11211-009-0088-1 [DOI] [Google Scholar]
- Wang, W. C., & Wu, X. C. (2020). Mediating roles of gratitude, social support and posttraumatic growth in the relation between empathy and prosocial behavior among adolescents after the Ya’an earthquake. Acta Psychologica Sinica, 52, 307–316. doi: 10.3724/SP.J.1041.2020.00307 [DOI] [Google Scholar]
- Wilson, S. L. (1985). The self-pity response: A reconsideration. Progress in Self-Psychology, 1, 178–190. [Google Scholar]
- Wong, C. C. Y., & Yeung, N. C. Y. (2017). Self-compassion and posttraumatic growth: Cognitive processes as mediators. Mindfulness, 8(4), 1078–1087. doi: 10.1111/j.1540-4560.1972.tb00029.x [DOI] [Google Scholar]
- Wu, X., Zhang, Y., Lin, D., & Zang, W. (2013). The effect of disaster exposure on PTSD of primary and secondary students Mediating and moderating effects. Psychological Development and Education, 29(6), 641–648. [Google Scholar]
- Zhang, Q. P., & Kou, Y. (2008). A confirmative research on prototype concept structure of prosocial behavior endorsed by adolescents. Sociological Study, 4, 182–202. [Google Scholar]
- Zhou, X., Wu, X., & Zhen, R. (2017). Understanding the relationship between social support and posttraumatic stress disorder/posttraumatic growth among adolescents after Ya’an earthquake: The role of emotion regulation. Psychological Trauma: Theory, Research Practice, and Policy, 9(2), 214–221. doi: 10.1037/tra0000213 [DOI] [PubMed] [Google Scholar]
- Zhou, X., Wu, X. C., An, Y. Y., & Chen, J. L. (2014). The roles of rumination and social support in the associations between core belief challenge and post-traumatic growth among adolescent survivors after the Wenchuan earthquake. Acta Psychologica Sinica, 46(10), 1509–1520. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to the containing information that could compromise the privacy of research participants.