

Abstract
Objective: This study was designed to study the effects of massage and acupuncture on patients with frozen shoulder complicated with cervical spondylosis through range of motion (ROM) and daily living ability. Methods: A total of 164 patients with frozen shoulder treated in our hospital from June 2016 to April 2019 were recruited and divided into a control group and an observation group. There were 100 cases in the observation group, all of whom were treated with massage combined with acupuncture. Another 64 cases were enrolled in the control group, all of whom were treated with acupuncture alone. The recovery of myodynamia, rating scale of the American Shoulder and Elbow Surgeons (ASES), score of American Spinal Injury Association (ASIA), ROM score, vascular cell adhesion molecule 1 (VCAM-1) and intercellular adhesion molecule 1 (ICAM-1), complication rate, total effective rate, and patient satisfaction were assessed. Results: After treatment, patients in the observation group had better recovery of myodynamia than the control group. They also had lower VAS scores, higher life function score and total ASES scores, higher ASIA scores, higher ROM scores, lower VCAM-1 and ICAM-1 expression, lower complication rate, higher total effective rate, and higher patient satisfaction. Conclusion: Massage combined with acupuncture can better improve the ROM of joints and daily living ability of patients with frozen shoulder complicated with cervical spondylosis.
Keywords: Massage, acupuncture, frozen shoulder, cervical spondylosis, range of motion
Introduction
Frozen shoulder is a common orthopedic disease with a prevalence rate of 2% to 5% [1,2]. The etiology of this disease is still unclear and controversial. Primary frozen shoulder is characterized by occult idiopathic attack, while secondary frozen shoulder is associated with many internal factors such as shoulder disease or external trauma. Frozen shoulder related to medical conditions such as diabetes and thyroid diseases is also secondary periarthritis of shoulder, which is generally systemic [3,4]. Another common orthopedic disease, cervical spondylosis, tends to cause pressure on the cervical spinal cord or nerve root, leading to neurological dysfunction. This disease is generally more common among elderly patients. With the further aging of the population, cervical spine disease is becoming more and more important in public health [5-7]. Here, we explored the effects of acupuncture plus massage on the combination of these two diseases.
As a traditional Chinese medicine therapy with a history of more than 2000 years, acupuncture has been widely used in the treatment of numerous diseases [8]. It regulates the Qi (vitality) and blood function of organs and the body’s resistance to diseases by puncturing some meridian points in the body [9]. Among many skin diseases such as eczema [10], urticaria [11,12] and neurodermatitis [13], acupuncture has been proved to have antipruritic effect. Moreover, in the clinical treatment of orthopedics, acupuncture is often used to relieve the symptoms of frozen shoulder. The use of slender needles can significantly relieve the pain caused by frozen shoulder and improve the limited range of motion (ROM) of shoulder joint [14]. Massage therapy is also a traditional Chinese medicine therapy, which involves many technical manipulations, such as swinging, pushing, vibration and joint movement. The doctors use their fingers, hands, elbows, knees, or feet to exert mechanical effects on skin, muscles, meridians, acupoints and joints, thereby relaxing muscles and tendons, improving blood circulation, regulating spinal balance, and relieving edema. It is of great significance in diseases such as osteoarthritis. Therefore, massage and acupuncture are often used in clinical treatment of various orthopedic diseases [15-17]. There are few clinical studies on the effects of massage combined with acupuncture on frozen shoulder complicated with cervical spondylosis. In this experiment, we explored the influence of massage and acupuncture on patients with frozen shoulder combined with cervical spondylosis through the indicators of patients’ ROM and daily living ability.
Methods
General data
A total of 164 patients with frozen shoulder treated in The Ninth Hospital of Wuhan from June 2016 to April 2019 were recruited as research objects, and they were divided into a control group and an observation group. One hundred cases of patients were assigned to the observation group to receive massage combined with acupuncture, including 52 males and 48 females, with ages ranging from 47-68 years and an average age of 55.32±5.98 years. Sixty-four cases of patients were assigned to the control group to receive acupuncture alone, including 35 males and 29 females, with ages ranging from 45-67 years and an average age of 55.65±6.01 years. Inclusion criteria: patients had no contraindications related to acupuncture and massage; patients had good compliance and could persist in completing treatment; patients had no mental disorder; patient had no communication disorder. Exclusion criteria: female in gestation period or lactation period; patients had cardiac insufficiency, liver or kidney dysfunction, rheumatoid arthritis, rheumatoid arthritis or other diseases that might affect the results of this study; patients received other treatment measures that might affect the results of this study recently; patients had shoulder contusion or shoulder joint tuberculosis; patients had malignant tumors. This study was conducted with the informed consent of patients and their families, and they had signed the informed consent form. The approval of the hospital ethics committee was also obtained.
Methods
After hospitalization, both groups of patients received routine treatment measures such as anti-inflammatory analgesia, partial closure of pain points and physical therapy. Besides, the medical staff cared for patients before and after treatment, so as to dispel their anxiety and enhance their confidence.
The control group received acupuncture treatment only, and the acupuncture points were Ashi, Jianzhen, Jianqian, Jianjing, Bingfeng, Quchi, Tianzong, Jianliao, Jianyu and so on. Before acupuncture treatment, the medical staff routinely disinfected the acupuncture points of the patient, and then used a 0.3 mm × 30 mm filiform needle (Suzhou Tianyi Acupuncture Equipment Co., Ltd.) to directly stab the Jianjing and Tianzong points of the patient to penetrate 0.5-0.8 inches until the patient felt the sense of acid distention. Then, the medical staff used a 0.3 mm × 30 mm filiform needle (Suzhou Tianyi Acupuncture Equipment Co., Ltd.) to stab the patient’s Jianliao, Jianyu, Quchi and Ashi points for 1.0-1.5 inches until the patient felt the sense of acid distention. The treatment was implemented realistically according to the patient’s condition. For example, the method of lifting, inserting, and reinforcing-reducing method by twirling needle depended on the syndrome of patients. The needles were kept in the body of patient for 30 min since they gained Qi. The acupuncture treatment was performed once a day, and 10 consecutive times was a course of treatment. The treatment lasted for 30 days.
The observation group was treated with massage combined with acupuncture. The acupuncture was also conducted on points of Jianjing, Tianzong, Ashi, Quchi, JianZhen, Jianliao, Jianyu, and so on, in the same way as above, once a day. On the basis of the control group, patients received massage treatment. The patient sat in front of the operator. First of all, the patient was massaged by exercise technique, and his/her shoulder joint was passively moved. Taking the shoulder joint as the center, the patient was rotated and shaken, and the direction was alternately moved clockwise and counterclockwise. The amplitude and intensity of the movement were based on the patient’s tolerance. Secondly, the acupoints Ashi, Jianzhen, Jianqian, Quchi, Tianzong, etc. of the patient were pressed by point-strong stimulus method, and the pressing time of each acupoint was preferably 1.5-3.0 min, and then poking channels manipulation was performed 3-5 times along the vertical direction of muscles. Finally, from the painful part of the patient to the forearm, the muscles were kept in a relaxed state by rubbing repeatedly. The massage treatment was also conducted once a day, and lasted for 30 days.
Detection indexes
(1) Recovery of myodynamia: Myodynamia of patients were observed and compared at admission and 30 d after treatment, and the Lovett score was adopted for assessment [18]. The score ranged from 0 to 5 points. The higher the score, the better the myodynamia recovery.
(2) Scale of the American Shoulder and Surgeons (ASIA): The shoulder joint functions of patients at admission and after treatment were analyzed. The rating scale of ASES [19] was taken as the standard. The content was roughly divided into two parts of pain and life function, each accounted for 50%, with a total score of 100. The score was proportional to the recovery of shoulder joint function. The Visual Analogue Scale (VAS) was adopted [20], and the higher the score of VAS (0-10), the more severe the pain. The assessment of life function adopted life function scale, which included 10 items in daily life such as dressing, combing hair and going to the toilet. The score was proportional to the recovery of life function.
(3) Nerve function: The recovery of neurological function of patients was detected and compared at admission, 7 days after treatment and 14 days after treatment. The assessment was conducted according to the score established by American Spinal Injury Association (ASIA) [21], and the higher the ASIA score, the better the recovery was.
(4) ROM score: The ROM of shoulder joint of patients at the time of admission and 30 days after treatment was detected and compared. The ROM of shoulder joint score [22] was used as the standard, and the evaluation contents mainly included the ROM of anteflexion, abduction, rear protraction, internal rotation and external rotation. The higher the ROM, the better the function of shoulder joint. A higher score indicated a better recovery.
(5) Inflammatorys: At the time of admission and 30 days after treatment, 5 ml venous blood was collected from the patient. The samples were centrifuged at 1500×g and 4°C for 10 min and then stored at -20°C. The levels of vascular cell adhesion molecule 1 (VCAM-1) and intercellular adhesion molecule 1 (ICAM-1) were measured by enzyme-linked immunosorbent assay (ELISA).
(6) Complication rate: After treatment, the complications of the two groups of patients were counted, and the incidence of complications was calculated. The complications included headache, shoulder pain, shoulder joint movement dysfunction, and muscle atrophy.
(7) Total effective rate: The effective rate was divided into four grades: cured, marked response, effective response and no response. Cured: symptoms such as shoulder joint and neck pain disappeared, all functions recovered, and various symptoms and myodynamia disappeared completely. Marked response: the clinical symptoms such as shoulder joint neck pain were basically relieved, the function was restored, and various symptoms and myodynamia were greatly improved. Effective response: the pain of shoulder joint and neck was relieved, and all kinds of symptoms and myodynamia were improved to a certain extent. No response: the pain of shoulder joint and neck was not improved, and various symptoms and myodynamia were not improved or even worsened. Total effective rate = (number of cured cases + number of cases of marked response + number of cases of effective response)/total number of cases ×100%.
(8) Patients satisfaction: The treatment satisfaction of the two groups of patients was detected and compared using questionnaire, with self-made test content and scoring standard. The total score was 100 points, of which a score of 100-85 points were considered as satisfied, a score of more than 65 points as basically satisfied, and a score of less than 65 points as dissatisfied.
Detection methods
SPSS 19.0 (Asia Analytics Formerly SPSS China) was used for statistical analysis of the data. X2 test was used for counting data. Measurement data were represented by mean ± standard deviation (x̅ ± sd), and t test was adopted. When P < 0.05, the difference was statistically significant.
Results
General data
There was no significant difference between the two groups in terms of general data of gender, age, body mass index (BMI), education years, place of residence, smoking, and employment (P > 0.05), as shown in Table 1.
Table 1.
General data of the two groups
| Classification | Observation group (n = 100) | Control group (n = 64) | t/X2 | P |
|---|---|---|---|---|
| Gender | 0.11 | 0.737 | ||
| Male | 52 (52.00) | 35 (54.69) | ||
| Female | 48 (48.00) | 29 (45.31) | ||
| Age (years) | 55.32±5.98 | 55.65±6.01 | 0.34 | 0.731 |
| BMI (kg/m2) | 24.16±4.39 | 23.98±4.78 | 0.25 | 0.805 |
| Education years (year) | 9.17±2.54 | 9.30±2.33 | 0.33 | 0.742 |
| Place of residence | 0.01 | 0.975 | ||
| Countryside | 44 (44.00) | 28 (43.75) | ||
| Town | 56 (56.00) | 36 (56.25) | ||
| Smoking | 0.49 | 0.485 | ||
| Present | 57 (57.00) | 40 (62.50) | ||
| Absent | 43 (43.00) | 24 (37.50) | ||
| Drinking | 0.39 | 0.531 | ||
| Present | 55 (55.00) | 32 (50.00) | ||
| Absent | 45 (45.00) | 32 (50.00) | ||
| On job | 0.28 | 0.594 | ||
| Yes | 58 (58.00) | 36 (56.25) | ||
| Retired | 42 (42.00) | 28 (43.75) |
Observation group has better recovery of myodynamia than control group
The Lovett score was adopted for assessment, and the score showed little difference between the two groups at admission (P > 0.05). After treatment, both groups showed obvious changes in the score, which was notably higher in the observation group than in the control group (P < 0.05). Such results indicated that the observation group has better recovery of myodynamia than the control group, as shown in Table 2.
Table 2.
Lovett scores of the two groups
| Classification | Observation group (n = 100) | Control group (n = 64) | t | P |
|---|---|---|---|---|
| On admission | 1.14±0.29 | 1.16±0.23 | 0.465 | 0.642 |
| 30 d after treatment | 4.01±0.80 | 3.28±0.77 | 5.78 | < 0.001 |
| t | 33.73 | 21.10 | ||
| P | < 0.001 | < 0.001 |
Observation group has better recovery of quality of life than control group
We applied the rating scale of ASES for evaluation, and found little difference in the score of each item between the two groups at admission (P > 0.05), but both groups had reduced VAS score and elevated life function and total scores after treatment. Compared with the control group, the observation group had notably lower VAS score but significantly higher life function and total scores (P < 0.05), as shown in Figure 1.
Figure 1.

ASES scores of the two groups. A. VAS: The VAS score decreased in both groups after treatment, and was significantly lower in the observation group than in the control group (P < 0.05). B. Life function scale: After treatment, the score of life function increased in both groups, and was significantly higher in the observation group than in the control group (P < 0.05). C. Total scores of ASES: After treatment, the total scores of ASES increased in both groups, and were significantly higher in the observation group than in the control group (P < 0.05). Notes: * means comparison with before treatment, P < 0.05. & means comparison with control group, P < 0.05.
Observation group has better recovery of neurological function than control group
The ASIA scores of patients showed little difference between the two groups before treatment (P > 0.05). After treatment, both groups had elevated scores, which was significantly higher in the observation group than in the control group (P < 0.05), suggesting that the observation group had better recovery of neurological functions, as shown in Figure 2.
Figure 2.
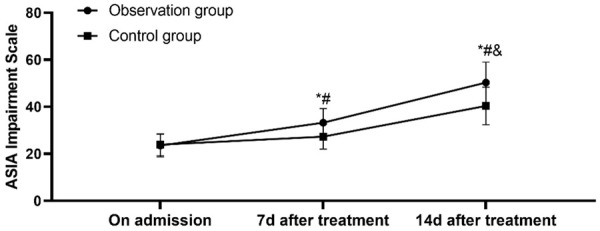
ASIA scores of the two groups. ASIA scores of patients in both groups were improved on 7th and 14th day after treatment, and the score of the observation group was higher than the control group (P < 0.05). Notes: * means comparison with before treatment, P < 0.05. # means comparison with 7 day after treatment, P < 0.05. & means comparison with the control group, P < 0.05.
Observation group has better recovery of shoulder joint function than control group
We investigated the ROM scores of patients, and found little difference between the two groups before treatment (P > 0.05). After treatment, each item of ROM scores was elevated, and those of the observation group were remarkably higher than those of the control group (P < 0.05). Such results indicated that the neurological function recovery in the observation group was better than that in the control group, as shown in Figure 3.
Figure 3.

ROM scores of patients in the two groups. A. Scores of flexion: the score improved in both groups after treatment, and the score of flexion in the observation group was higher than those in the control group (P < 0.05). B. Scores of extension: the score improved in both groups after treatment, and the score of extension in the observation group was higher than those in the control group (P < 0.05). C. Scores of abduction: After treatment, the score improved in both groups, and the abduction score of the observation group was higher than that of the control group (P < 0.05). D. Score of internal rotation: the score improved in both groups after treatment, and the score of internal rotation in the observation group was higher than those in the control group (P < 0.05). E. Scores of external rotation: the score improved in both groups after treatment, and the external rotation score of the observation group was higher than that of the control group. Notes: * means comparison with before treatment, P < 0.05. & means comparison with control group, P < 0.05.
Observation group has better reduced postoperative inflammatory response than control group
The expression levels of ICAM-1 and VCAM-1 after treatment were detected and compared between the two groups. The results showed that there was no difference between the two groups at the time of admission (P > 0.05). After treatment, the expression levels of ICAM-1 and VCAM-1 decreased in both groups, and were lower in the observation group than those in the control group (P < 0.05). The levels of inflammatory cytokines in the observation group were lower, indicating that the relief in the observation group was better than that in the control group, as shown in Figure 4.
Figure 4.
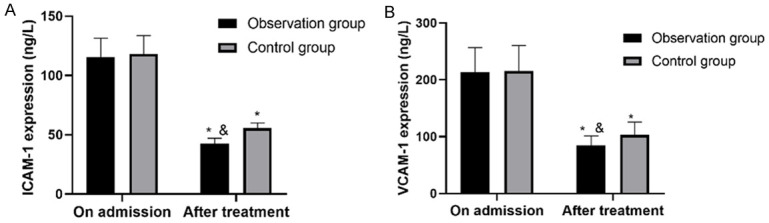
Expression levels of ICAM-1 and VCAM-1 in the two groups. A. ICAM-1: The expression level of ICAM-1 in two groups increased after treatment, and ICAM-1 in the observation group was significantly lower than that in the control group (P < 0.05). B. VCAM-1: The expression level of VCAM-1 in two groups increased after treatment, and VCAM-1 in the observation group was significantly lower than that in the control group (P < 0.05) Notes: & means comparison with before treatment, P < 0.05. & means comparison with control group, P < 0.05.
Observation group has lower incidence of complications than control group
After investigating the incidence of complications of the two groups, it was found that the incidence of the observation group was significantly higher than that of the control group (P < 0.05). The incidence of complications in the observation group was lower than that in the control group, indicating safer treatment in the observation group, as shown in Table 3.
Table 3.
Complication rates in the two groups
| Classification | Observation group (n = 100) | Control group (n = 64) | X2 | P |
|---|---|---|---|---|
| Headache | 2 (2.00) | 6 (9.38) | ||
| Shoulder pain | 1 (1.00) | 4 (6.25) | ||
| Shoulder joint movement dysfunction | 0 (0.00) | 4 (6.25) | ||
| Amyotrophy | 0 (0.00) | 2 (3.12) | ||
| Complication rate (%) | 3 (3.00) | 16 (25.00) | 18.44 | < 0.001 |
Observation group has higher total effective rate than control group
The total effective rate of the observation group was significantly higher than that of the control group (P < 0.05), indicating that the treatment in the observation group was more effective, as shown in Table 4.
Table 4.
Total effective rate of the two groups
| Classification | Observation group (n = 100) | Control group (n = 64) | X2 | P |
|---|---|---|---|---|
| Cured | 64 (64.00) | 24 (37.50) | - | - |
| Markedly effective | 24 (24.00) | 20 (31.25) | - | - |
| Effective | 10 (10.00) | 12 (18.75) | - | - |
| Ineffective | 2 (2.00) | 8 (12.50) | - | - |
| Total effective rate % | 98 (98.00) | 32 (87.50) | 7.86 | 0.006 |
Observation group has higher satisfaction than control group
Our investigation of satisfaction indicated that patients in the observation group had remarkably higher degree of satisfaction than the control group (P < 0.05). More details were shown in Table 5.
Table 5.
Comparison of nursing satisfaction between the two groups
| Classification | Observation group (n = 100) | Control group (n = 64) | X2 | P |
|---|---|---|---|---|
| Satisfied | 70 (70.00) | 40 (62.50) | - | - |
| Basically satisfied | 23 (23.00) | 12 (18.75) | - | - |
| Dissatisfied | 7 (7.00) | 12 (18.75) | - | - |
| Satisfaction (%) | 93 (93.00) | 52 (81.25) | 5.26 | 0.022 |
Discussion
Acupuncture and massage are widely used in the clinical treatment of orthopedic diseases such as cervical spondylosis and frozen shoulder, and can often achieve great results [23,24]. This experiment studied the effects of the combined use of massage and acupuncture on the combination of frozen shoulder and cervical spondylosis. The results revealed that the recovery of joint activities and activities of daily living in the observation group after acupuncture plus massage were better than those of the patients who received acupuncture only. Here, we discussed the impacts from two aspects: the recovery of nerve function and the recovery of limb joint function.
According to our studies on the recovery of patients’ neurological function, the scores of ASIA and ROM of patients were improved after treatment, and the scores were higher in the observation group. Acupuncture was defined as a treatment method used to stimulate body tissues. When the needle is inserted into the acupoint, the skin, muscle and nerve components, connective tissue, and chemical signal transmission will be affected, because the acupuncture signal caused by the change of acupuncture depth may be transmitted through different signal pathways [25]. Therefore, the neurological function scores of the two groups were improved after treatment, indicating effectively restored neurological function. The VAS score in the ASES scores of the two groups decreased after treatment, which also showed that acupuncture played a role in nerve conduction. Massage is beneficial to increase blood flow, and has an obvious recovery effect on muscle spasm. Besides, massage can cause the body to release β-endorphin to suppress the pain in the affected part, and has a good effect on anxiety and depression caused by cervical nerve root neuralgia [26]. As such, massage can effectively restore the neurological function of patients. This is also the reason why patients in the observation group had better neurological function recovery. The effects of massage on relieving muscle spasm can facilitate the recovery of myodynamia of patients, so the myodynamia of patients in the control group was better recovered. Massage promotes the release of β-endorphin in the treatment process, which can effectively relieve the pain of patients. Therefore, the VAS score of the observation group was lower. It has been proved from theory and clinical practice that acupuncture and massage can down-regulate some inflammatory cytokines and have therapeutic effect on inflammation [27,28]. The results of this experiment proved this down-regulation, and acupuncture and massage can reduce the level of inflammatory cytokines more quickly. Generally speaking, both massage and acupuncture can play a role in the recovery of neurological function after treatment, and the combination of the two can not only promote the recovery of neurological function, but also reduce the pain and inflammation reaction, and help better recover myodynamia.
We then investigated patient’s ROM and its influence on the recovery of the patient’s ability of daily living. It was reported that severe nervous system injury and inflammatory reaction caused by upper limbs will lead to complete or partial motor paralysis, thus affecting various functions of upper limbs [29,30]. The use of acupuncture is helpful to the recovery of patients’ neurological function, and the use of massage reduces the pain and inflammation of related parts of patients, contributing to faster recovery of the myodynamia. With acupuncture, the ROM of the joints was restored in both groups. The combination of the two can effectively restore the joint function of patients after better recovery of nerve function, and the recovery of joint function will enable patients to perform daily activities of dressing, combing hair and going to the toilet with less discomfort and therefore more smoothly.
In the future experiments, we will examine the relationship between acupuncture and massage on specific neural signal pathway molecules, which was not studied due to the technical limitations. Besides, in the future research, we will also pay attention to the patients’ negative emotions such as anxiety and depression, so as to continuously improve the treatment plan and promote the recovery of patients.
To sum up, the combined treatment of massage and acupuncture can better improve the ROM of patients with frozen shoulder and cervical spondylosis, and improve their life function, which is worthy of clinical promotion.
Disclosure of conflict of interest
None.
References
- 1.Akbar M, McLean M, Garcia-Melchor E, Crowe LA, McMillan P, Fazzi UG, Martin D, Arthur A, Reilly JH, McInnes IB, Millar NL. Fibroblast activation and inflammation in frozen shoulder. PLoS One. 2019;14:e0215301. doi: 10.1371/journal.pone.0215301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kelley MJ, Shaffer MA, Kuhn JE, Michener LA, Seitz AL, Uhl TL, Godges JJ, McClure PW. Shoulder pain and mobility deficits: adhesive capsulitis. J Orthop Sports Phys Ther. 2013;43:A1–31. doi: 10.2519/jospt.2013.0302. [DOI] [PubMed] [Google Scholar]
- 3.Ando A, Hamada J, Hagiwara Y, Sekiguchi T, Koide M, Itoi E. Short-term clinical results of manipulation under ultrasound-guided brachial plexus block in patients with idiopathic frozen shoulder and diabetic secondary frozen shoulder. Open Orthop J. 2018;12:99–104. doi: 10.2174/1874325001812010099. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ryan V, Brown H, Minns Lowe CJ, Lewis JS. The pathophysiology associated with primary (idiopathic) frozen shoulder: a systematic review. BMC Musculoskelet Disord. 2016;17:340. doi: 10.1186/s12891-016-1190-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ryan V, Brown H, Minns Lowe CJ, Lewis JS. The pathophysiology associated with primary (idiopathic) frozen shoulder: a systematic review. BMC Musculoskelet Disord. 2016;17:340. doi: 10.1186/s12891-016-1190-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Karadimas SK, Gatzounis G, Fehlings MG. Pathobiology of cervical spondylotic myelopathy. Eur Spine J. 2015;24(Suppl 2):132–138. doi: 10.1007/s00586-014-3264-4. [DOI] [PubMed] [Google Scholar]
- 7.Murphy RK, Sun P, Xu J, Wang Y, Sullivan S, Gamble P, Wagner J, Wright NN, Dorward IG, Riew D, Santiago P, Kelly MP, Trinkaus K, Ray WZ, Song SK. Magnetic resonance imaging biomarker of axon loss reflects cervical spondylotic myelopathy severity. Spine (Phila Pa 1976) 2016;41:751–756. doi: 10.1097/BRS.0000000000001337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Zhao Y, Yu J, Liu S, Zhou J, Wang J, Wang Z, Liu Z. Ecchymosis combined with postinflammatory hyperpigmentation associated with acupuncture therapy: an observational study of 167 subjects. Medicine (Baltimore) 2020;99:e18721. doi: 10.1097/MD.0000000000018721. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Zhang YJ, Cao HJ, Li XL, Yang XY, Lai BY, Yang GY, Liu JP. Cupping therapy versus acupuncture for pain-related conditions: a systematic review of randomized controlled trials and trial sequential analysis. Chin Med. 2017;12:21. doi: 10.1186/s13020-017-0142-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Xie Y. A review of clinical research on acupuncture therapy for eczema. J Clin Med Lit. 2018;5:192. [Google Scholar]
- 11.Bai T, Fan B. A review of traditional Chinese medicine for chronic urticaria. Chin J Ethnomed Ethnopharm. 2017;26:75–77. 80. [Google Scholar]
- 12.Wei W. Clinical progress of Chinese medicine for chronic urticaria. J New Chin Med. 2018;50:24–27. [Google Scholar]
- 13.Ma T, Liu G, Li Q. A review of traditional Chinese medicine for neurodermatitis. Acta Chin Med Pharmacol. 2014;42:91–94. [Google Scholar]
- 14.Yang C, Lv T, Yu T, Wong S, Lu M, Li Y. Acupuncture at Tiaokou (ST38) for shoulder adhesive capsulitis: what strengths does it have? A systematic review and meta-analysis of randomized controlled trials. Evid Based Complement Alternat Med. 2018;2018:4197659. doi: 10.1155/2018/4197659. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Tang S, Qian X, Zhang Y, Liu Y. Treating low back pain resulted from lumbar degenerative instability using Chinese Tuina combined with core stability exercises: a randomized controlled trial. Complement Ther Med. 2016;25:45–50. doi: 10.1016/j.ctim.2016.01.001. [DOI] [PubMed] [Google Scholar]
- 16.Smith CA, Levett KM, Collins CT, Dahlen HG, Ee CC, Suganuma M. Massage, reflexology and other manual methods for pain management in labour. Cochrane Database Syst Rev. 2018;3:CD009290. doi: 10.1002/14651858.CD009290.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Mo Z, Li D, Zhang R, Chang M, Yang B, Tang S. Comparisons of the effectiveness and safety of tuina, acupuncture, traction, and chinese herbs for lumbar disc herniation: a systematic review and network meta-analysis. Evid Based Complement Alternat Med. 2019;2019:6821310. doi: 10.1155/2019/6821310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Hidayat AA, Arief Z, Happyanto DC. LOVETT scaling with flex sensor and MYO armband for monitoring finger muscles therapy of post-stroke people. EMITTER Int J of Engine Techn. 2015;3:60–76. [Google Scholar]
- 19.Tashjian RZ, Hung M, Keener JD, Bowen RC, McAllister J, Chen W, Ebersole G, Granger EK, Chamberlain AM. Determining the minimal clinically important difference for the American shoulder and elbow surgeons score, simple shoulder test, and visual analog scale (VAS) measuring pain after shoulder arthroplasty. J Shoulder Elbow Surg. 2017;26:144–148. doi: 10.1016/j.jse.2016.06.007. [DOI] [PubMed] [Google Scholar]
- 20.Heller GZ, Manuguerra M, Chow R. How to analyze the visual analogue scale: myths, truths and clinical relevance? Scand J Pain. 2016;13:67–75. doi: 10.1016/j.sjpain.2016.06.012. [DOI] [PubMed] [Google Scholar]
- 21.Roberts TT, Leonard GR, Cepela DJ. Classifications in brief: American Spinal Injury Association (ASIA) impairment scale. Clin Orthop Relat Res. 2017;475:1499–1504. doi: 10.1007/s11999-016-5133-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Kim SG, Kim WS. Effect of Ankle Range of Motion (ROM) and lower-extremity muscle strength on static balance control ability in young adults: a regression analysis. Med Sci Monit. 2018;24:3168–3175. doi: 10.12659/MSM.908260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Gu CL, Yan Y, Zhang D, Li P. An evaluation of the effectiveness of acupuncture with seven acupoint-penetrating needles on cervical spondylosis. J Pain Res. 2019;12:1441–1445. doi: 10.2147/JPR.S199798. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Asheghan M, Aghda AK, Hashemi E, Hollisaz M. Investigation of the effectiveness of acupuncture in the treatment of frozen shoulder. Mater Sociomed. 2016;28:253–257. doi: 10.5455/msm.2016.28.253-257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Ju ZY, Wang K, Cui HS, Yao Y, Liu SM, Zhou J, Chen TY, Xia J. Acupuncture for neuropathic pain in adults. Cochrane Database Syst Rev. 2017;12:CD012057. doi: 10.1002/14651858.CD012057.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Wei X, Wang S, Li L, Zhu L. Clinical evidence of Chinese massage therapy (Tui Na) for cervical radiculopathy: a systematic review and meta-analysis. Evid Based Complement Alternat Med. 2017;2017:9519285. doi: 10.1155/2017/9519285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Jiang S, Zhang H, Fang M, Zhang Y, Lu N, Zhu Q, Cheng Y, Ai J, Zhou N, Li J, Fang L, Yao F. Analgesic effects of Chinese Tuina massage in a rat model of pain. Exp Ther Med. 2016;11:1367–1374. doi: 10.3892/etm.2016.3055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.McDonald JL, Cripps AW, Smith PK, Smith CA, Xue CC, Golianu B. The anti-inflammatory effects of acupuncture and their relevance to allergic rhinitis: a narrative review and proposed model. Evid Based Complement Alternat Med. 2013;2013:591796. doi: 10.1155/2013/591796. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Hao GL, Zhang TY, Zhang Q, Gu MY, Chen C, Zou L, Cao XC, Zhang GC. Partial recovery of limb function following end-to-side screw anastomosis of phrenic nerve in rats with brachial plexus injury. Med Sci Monit. 2018;24:4832–4840. doi: 10.12659/MSM.908379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Merola A, Rosso M, Romagnolo A, Peci E, Cocito D. Peripheral nerve ultrasonography in chronic inflammatory demyelinating polyradiculoneuropathy and multifocal motor neuropathy: correlations with clinical and neurophysiological data. Neurol Res Int. 2016;2016:9478593. doi: 10.1155/2016/9478593. [DOI] [PMC free article] [PubMed] [Google Scholar]