

Abstract
Objective:
We undertook a literature review to evaluate the evidence for an association among school-based fitness testing and bullying, weight-based teasing (WBT), and/or gender discrimination.
Methods:
We searched the peer-reviewed literature using PubMed, ERIC and GOOGLE Scholar to identify articles related to school-based physical fitness testing (K-12) on the one hand and bullying, WBT, and/or gender discrimination on the other.
Results:
We identified 12 studies on the impact of school-based physical fitness testing (PFT) on bullying and WBT. These studies do not support the assertion that PFT places students at elevated risk for bullying and/or WBT as compared to other school settings. There is a dearth of studies investigating an association between PFT and gender discrimination.
Conclusions:
The concerns about PFT as a widespread cause of bullying and WBT are not supported by the evidence. It is likely that school climate is a stronger determinant overall of these negative student interactions and that more rigorous teacher training would ameliorate student concerns about fitness testing. Nevertheless, more rigorous research is warranted to determine with confidence that PFT does not elevate students’ risks for bullying and WBT and to examine the risks for students with non-binary gender.
Keywords: physical fitness testing, bullying, weight-based teasing gender discrimination, school-based fitness testing
Epidemiologic data consistently indicate that most United States youth live a physically inactive lifestyle that places them at elevated health risk both during their youth as well as long into their adult years. The most recent data from the Youth Risk Behavior Surveillance System (YRBSS)1 show that fewer than half (ie, 46.5%) of high school students met recommended guidelines, which call for youth to engage in at least 60 minutes per day of moderate-to-vigorous physical activity.2 There are many reasons why these low rates of activity should trigger alarm, including the strong evidence that physical activity is protective against the development of Type 2 diabetes,3–5 promising evidence that higher levels of physical activity are associated with higher executive function and academic achievement,6–8 and the increased risk for chronic disease, (heart disease, hypertension, obesity, certain cancers) that is associated with physical inactivity.9,10
Schools offer an appealing setting for promoting youth physical activity. Schools provide ready access to youth as well as an educational context within which youth can receive programming that will both afford them the opportunity to be active in their formative years and also instill in them the skills and knowledge to remain active throughout their adult lives. Schools have been identified previously as promising and effective settings for promoting youth physical activity.11–13
Among the strategies recommended for leveraging schools to promote youth physical activity is the regular administration of physical fitness testing (PFT), typically comprised of assessments of body composition (eg, body mass index), cardiorespiratory endurance (eg, a progressive shuttle run or timed run), and strength (eg, grip strength or pushups).14 School-based PFT has a long history, with the first national fitness test being developed in 1958.15 Originally motivated by concerns about military readiness, PFT now has been encouraged as a means of monitoring population health,16,17 and has been deployed to illustrate disparities in fitness across socioeconomic status and/or ethnicity.18–20 Large-scale PFT also has the potential to inform policy, although evidence of such utilization of the data is limited.17 School-based PFT is often promoted as a means of educating students about their health and of motivating increased physical activity.14,21,22 Whether school-based PFT is in fact an effective strategy for addressing widespread inactivity among youth has been vigorously debated in both the academic and public policy spheres.15,23,24
Those who argue in favor of continuing to deploy school-based PFT contend that it is imperative to monitor the epidemiology of youth fitness because of the very robust evidence regarding the beneficial health aspects of fitness and the importance of attaching some measure of accountability to physical education (PE) programs.17,25 Moreover, in the absence of school-level data, disparities in youth fitness across school districts, communities, and states may go un-noticed and therefore unaddressed. In a perhaps unique example of the data from PFT being used to inform policy, reporting of fitness survey results led to statewide funding to pay for licensed PE teachers in California elementary schools.17 Proponents of school-based PFT also argue that it has the potential to motivate youth to engage in healthful levels of activity.26 However, there are few studies that have tested this hypothesis, and some evidence that fitness testing is not effective in promoting behavior change.27
There are those who argue that school-based PFT has largely missed the mark in accomplishing its putative goals;28–30 a failure that is often attributed to poor implementation of the fitness testing protocol.31,32 A concrete example of this dynamic is a report recommending modifications to the mandatory school-based body mass index (BMI) screening implemented in Massachusetts,33 which noted that concerns regarding student bullying were likely related to procedures that were insufficiently protective of students’ privacy and confidentiality. An oft-quoted summary of the potential negative impact of PFT on students is that “current programs of field testing of school children are actually antithetical to the goal of promoting physical activity in children. Such tests are demeaning, embarrassing, and uncomfortable to those particular children we are most concerned about-the sedentary lower 10%.”28 More recent criticisms of PFT have raised concerns about whether it carries a risk of exposing students to bullying, weight-based teasing, and/or discrimination against students with non-binary gender. These last 3 concerns were cited by California’s Governor, Gavin Newsom, in a call for a pause on mandatory statewide school-based PFT which he issued in 2020.34,35 To provide context for these concerns, a summary of the literature related to the health consequences of school-based bullying, weight-based teasing, and gender discrimination is presented below.
Bullying
The US Centers for Disease Control and Prevention (CDC) defines bullying as “any unwanted aggressive behavior(s) by another youth or group of youths who are not siblings or current dating partners that involves an observed or perceived power imbalance and is repeated multiple times or is highly likely to be repeated.”36 Bullying can happen in many forms including physical, verbal, or relational/social. Based on the 2017 School Crime Supplement,37 20% of students ages 12–18 experienced bullying during the school year.
Association between bullying and negative health outcomes.
A large body of research supports a negative association between bullying and both mental and physical health.38,39 Among the more rigorous studies on this topic was a prospective study in the Netherlands that followed 1118 9-to-11-year-olds for 6 months and found a reciprocal association between bullying and psychosocial/psychosomatic symptoms.40 Strong evidence also was provided by a prospective, population-based study of 1420 9-to-16-year-olds in western North Carolina, which found that victims of childhood bullying were at increased risk for anxiety disorders, depressive disorders, and panic attacks in adulthood, after controlling for family hardships and childhood psychiatric disorders.41
Association between bullying and physical education (PE).
The possibility that PE may be a setting that places students at risk for bullying has been raised repeatedly in the popular press,42,43 and certainly bullying does occur sometimes to some students in PE;44–46 yet, evidence that PE places students at elevated risk for bullying compared to other settings is weak. In 3 large cross-sectional self-report surveys, PE or gym (where PE typically takes place) was identified as a setting where bullying occurs; yet, none of these studies demonstrated that bullying is more prevalent during PE or in the gym as compared to other school settings. For example, a survey of 15,185 students (grades 4–12) in a diverse Maryland public school district44 found that PE was not a particularly high-risk setting. Twenty percent of middle school students reported being bullied during PE, but more students reporting being bullied in classrooms (29%), hallways/lockers (29%), and the cafeteria (23%). Similar findings emerged from a survey of 11,152 students from 65 schools in Canada46 and a survey of 10,668 middle school students from 20 diverse middle schools in New Jersey and New York.45 Thus, these studies suggest that bullying is no more likely to occur in PE as compared to other school settings.
Body Shaming and Weight-based Teasing (WBT)
Another concern related to PFT is body shaming, which is when someone mocks or criticizes a person for a supposed body imperfection.47 A form of body shaming is weight-based teasing (WBT).48,49 The prevalence of WBT in the US has not been determined with a nationally representative sample, but regional studies of US youth have found the prevalence of WBT ranges from 17.3% to 43%.48,50–52
Association between WBT and negative health outcomes.
WBT is associated with psychosomatic symptoms53 and poor psychological outcomes including anxiety, depressive symptoms, low self-esteem, and self-efficacy.50,51,54–56 Other negative health outcomes associated with WBT include lower self-concept of aerobic fitness, strength, and flexibility,51 disordered eating, and increased BMI.48,49,54,57 There is also some evidence that WBT during physical activity is significantly associated with reduced sports enjoyment, reduced perceived activity compared with peers, and reduced mild-intensity physical activity.58 Overall, the evidence suggests that WBT affects many aspects of mental, emotional, and physical health.
Association between WBT and physical education (PE).
PE classes may offer an opportunity for students to experience WBT. Interviews with students and teachers identified perceived differences, such as body size, as the catalyst for most instances of bullying during PE.59 In a cross-sectional study of 1555 high school students from central Connecticut, approximately 41% of the participants identified being overweight as the primary reason for being victimized and 85% identified WBT occurring among students during physical activity, such as gym class.60 These data suggest that PE could be a setting that places students at risk for WBT.
Gender-based Discrimination
In addition to the concerns about bullying and WBT during PFT, concerns have been expressed about students having to declare their gender as part of the assessment.35,61,62 In society-at-large, there is a growing awareness and acceptance of gender identities other than the binary options of male and female, including transgender, non-binary, and gender nonconforming. In 2019, California put into effect Senate Bill 179 which created a gender category for non-binary that can be used on birth certificates, identity cards, drivers’ licenses, and gender-change court orders.63 In contrast, the norms used to interpret the performance data from PFT are based on binary gender categories, leading some to question whether non-binary gendered youth may be placed in an awkward or uncomfortable position if required to declare a binary gender identity.
Public recognition and acceptance of gender fluidity is a relatively young phenomenon. Research methodology is struggling to catch up and provide useful data. Specifically, the expansion of categories used to describe gender identities has posed a methodological challenge for researchers when trying to ascertain the prevalence of people who identify outside the binary gender system. One study of Minnesota public school students in 9th and 11th grade (N = 80,929) assessed gender identity by asking: “Do you consider yourself transgender, genderqueer, genderfluid, or unsure about your gender identity.” Those who answered yes to this question comprised 2.7% of respondents.64 Another approach used adult data from the CDC’s Behavioral Risk Factor Surveillance System (BRFSS), to estimate prevalence among youth. This survey asked: “Are you transgender?” and yielded a more conservative estimate of 0.7% of youth ages 13 to 17 identifying as transgender.65 Debate continues regarding the best methodology for assessing prevalence of non-binary gender identities among youth, so caution should be exercised in interpreting currently available data. Moreover, the prevalence of non-binary gender individuals appears to be increasing over time,66 although how much of this trend is explained by changing societal attitudes, new research methodologies, or an actual increase in prevalence is unknown at this juncture.
Association between gender discrimination and negative health outcomes.
Transgender and gender non-conforming (TGNC) youth face discrimination and stigma that contribute to mental health problems.67 TGNC youth have an increased risk for anxiety, attention deficit disorder,68 suicidal ideation,69 and depression.70 TGNC youth also experience a significantly higher prevalence of bullying and harassment than cisgender youth.69,71,72
Association between gender discrimination and physical education (PE).
More than 80% of transgender middle and high school students in the Preventing School Harassment Survey (N = 2260) reported hearing negative comments based on gender presentation by other students73 and 44.6% of students in the 2017 National School Climate Survey felt unsafe at school because of their gender expression.74 PE or gym class is a setting within school in which TGNC students may feel particularly unsafe due to the gendered aspects of PE, such as locker rooms, different gender expectations, and division of activities based on gender.75 Based on data from the 2017 National School Climate Survey, 64.1% of transgender students and 41.6% of all genderqueer and other non-binary students avoided PE or gym class because they felt unsafe or uncomfortable. This is significantly higher than their cisgender peers (28.6%),74 suggesting that PE is an environment that is not supportive of gender nonconformity.
Clearly, bullying, WBT, and gender discrimination have negative impacts on physical and mental health, and if school-based PFT places students at elevated risk for these types of interactions this situation should be decisively addressed. The California Governor’s call for pausing school-based PFT has created an opportune moment for evaluating the evidence of unintended negative consequences of school-based PFT. The purpose of this review was to summarize the available evidence that school-based PFT results in bullying, WBT, and/or gender-based discrimination.
METHODS
A search for peer-reviewed publications was conducted using PubMed. ERIC and Google Scholar also were searched but yielded no unique results. Search terms used included terms related to fitness testing (FITNESSGRAM, Timed Mile Run, Physical Fitness Test, Fitness Testing, Body Mass Index, BMI, BMI Screening) paired with at least one term related to the topics of interest (Bullying, Weight Discrimination, Body Shaming, Fat Shaming, Weight-based Teasing, Gender non-conforming, Non-binary, Transgender, Gender bias). If the key word search yielded more than 100 results, the search was refined using the title and abstract only search method in PubMed. Abstracts were screened for articles that were relevant to school-based PFT and focused on students in grades K-12. Backward and forward reference tracing supplemented the key-word search. Only English-language articles were included. Figure 1 shows a flow chart of the search process that followed the PRISMA recommendations.76
Figure 1.
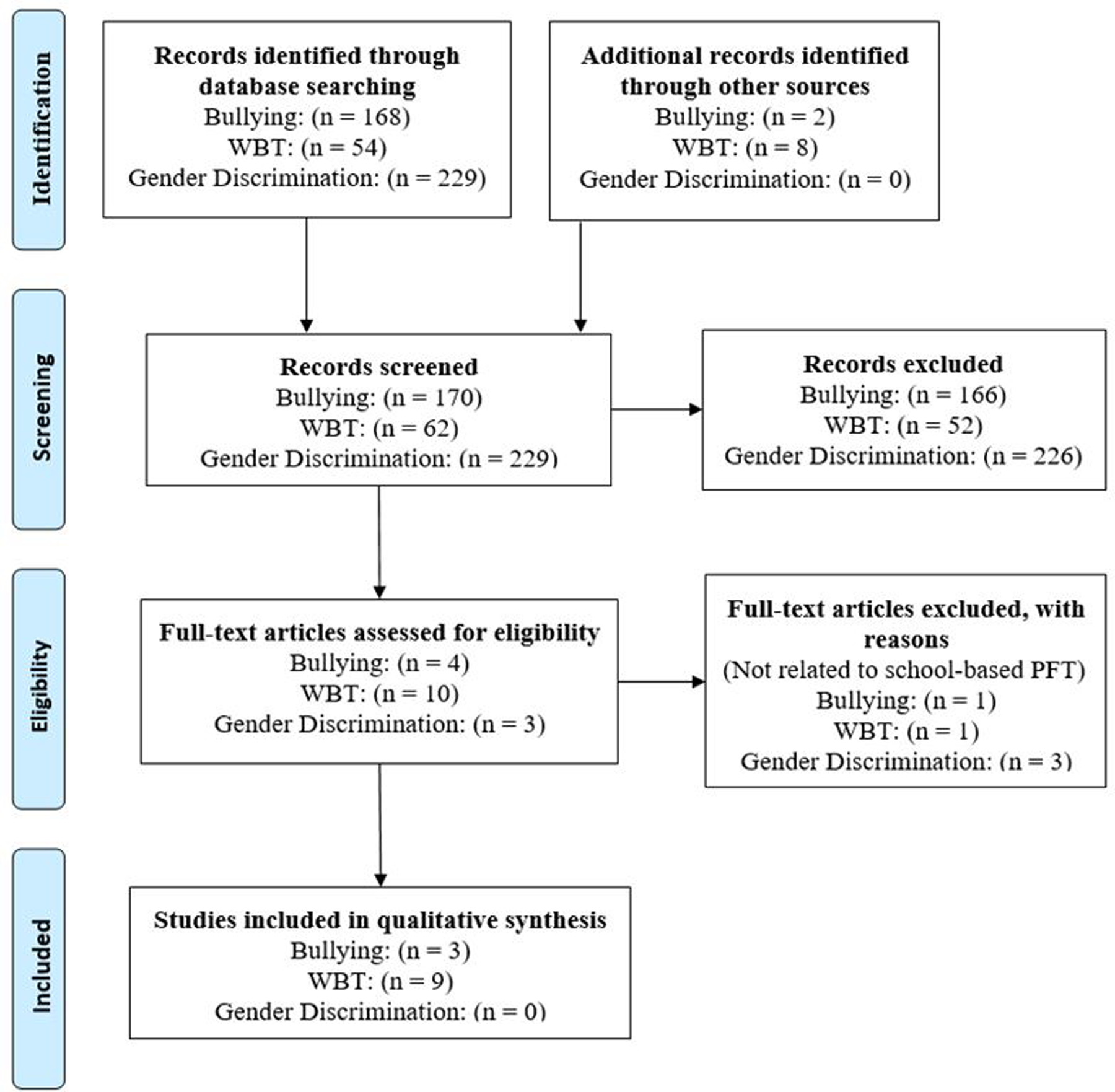
PRISMA Flow Diagram of Literature Search Process
RESULTS
Association between Bullying and Physical Fitness Testing
Weak support for an association between PFT and bullying comes from 3 publications identified by the literature search (Table 1). Two school-based studies were conducted in Texas, where PFT has been mandated, and one survey of pediatricians’ perceptions of mandatory school-based BMI screening was carried out in Massachusetts. One of the Texas studies reported findings from a single focus group of 9 PE teachers. Three of the 9 teachers reported witnessing students teasing other students during PFT.77 This study is of limited utility and generalizability, given the small sample size and the lack of information related to prevalence or severity of the teacher-reported events. Somewhat stronger evidence of an association between PFT and negative peer interactions comes from a large survey of PE teachers in Texas who implemented the mandatory fitness testing. Of the 1505 teachers surveyed, 26.6% reported negative consequences associated with fitness testing.78 Although indicative that some PE teachers perceive PFT to be a setting within which bullying does occur, the conclusions that can be drawn from these 2 Texas studies are limited given that they are not based on students’ own reports and do not place the teachers’ perceptions in the context of how frequently bullying or teasing occurs in the school overall. In the absence of such information, it is not possible to verify whether PFT places students at elevated risk for bullying in the school environment. Finally, 11% of 286 pediatricians surveyed in Massachusetts79 reported that they had delivered counseling to parents about bullying related to school-based BMI screening. Given the low response rate on this survey (18.6%) and the small number of pediatricians who mentioned bullying as an issue raised by parents in the clinical setting, this study provides only a weak indication that school-based PFT may be associated with bullying.
Table 1.
Identified Peer-reviewed Studies through Literature Search
| Study | Target Population | Sample Size | Methodology |
|---|---|---|---|
| Bullying | |||
| Martin et al., 2010.75 | Secondary physical education teachers from Texas | N = 9 | Focus Group |
| Zhu et al., 2010.76 | Teachers who participated in Texas Youth Education Project | N = 1,505 | Online Self-report survey |
| Bottino et al., 2016.79 | Members of the Massachusetts Chapter of the American Academy of Pediatrics | N = 286 | Online Self-report survey |
| Weight-Based Teasing | |||
| Ikeda et al., 2006.78 | n/a | n/a | Literature Review |
| Soto et al., 2010.79 | n/a | n/a | Literature Review |
| Grimmett et al., 2008.80 | 6–11-year-olds and Parents | N = 358 N = 287 |
Self-report Survey |
| Cash, 1995.85 | Female college students | N = 111 |
Retrospective Survey |
| Hayden-Wade et al., 2005.82 | Overweight and non-overweight children 10–14 years old | N = 70 overweight N = 86 non-overweight |
Survey with BMI Assessment |
| Haines et al., 2007.83 | Students, staff members, and parents | N = 21 student N = 12 staff members N = 21 parents |
Focus Groups and Individual Interviews |
| Cogan et al., 2008.85 | n/a | n/a | Legislative Review and Analysis |
| Janssen et al., 2004.86 | 11–16-year-olds | N = 5,749 | Secondary Analysis of Self-report Survey Data |
| Madsen et al., 2020.90 | California elementary and middle schools (grades 3–8) | N = 79 | Cluster randomized clinical trial |
Association between Weight-based Teasing (WBT) and Physical Fitness Testing (PFT)
Our literature search yielded 9 publications relevant to WBT and PFT – 2 literature reviews, one legislative review, and 6 empirical studies (Table 1). The component of PFT that is typically identified as the culprit for WBT is the assessment of BMI, a weight-to-height ratio used to distinguish weight categories.80 The putative link between BMI assessments and WBT has been called out repeatedly in public forums.34,35,81–84 Yet, the evidence for an association between BMI screening and WBT is sparse. In a comprehensive review of policies and research regarding BMI screening in schools, Ikeda et al81 mentioned concern for labeling students as ‘fat’ and referenced 2 studies as supporting evidence, including a retrospective study of female college students reflecting on their experiences during youth,85 and a cross-sectional study comparing overweight youth’s experience with teasing to non-overweight peers.86 Neither of these studies in fact offers evidence that the BMI assessment is associated with WBT. Similarly, a review by Soto et al82 alluded to a concern about teasing in relation to the BMI assessment and provided a single supporting citation of focus group data from one school in Minnesota in which participants were asked to rate the problem of teasing about weight at the school. Students, staff, and parents reported WBT was a prominent issue at their school,87 but the association with BMI assessment was not evaluated. The concern about WBT being related to BMI screening was again raised in a legislative review arguing against mandatory BMI reporting laws.88 Despite arguing that BMI reporting puts children at risk for bullying and teasing, the only supporting evidence cited was a study that found that children who are overweight/obese experience more bullying compared to normal weight children.89 In sum, the studies referenced in the various reviews on this topic do not provide evidence that PFT is associated with WBT.
Two studies were found that specifically assessed WBT in relationship with BMI screening, and the results of these studies further illustrate that BMI assessments do not appear to be associated with WBT. Grimmett et al83 conducted a descriptive, longitudinal study of 358 children (6–11 years old) from 6 London schools and their parents (N = 287) to examine the potential distress experienced by children in a weight screening program. The children’s height and weight were measured in a screened area at school by trained researchers. Parents and students completed questionnaires 6 weeks prior and 4 weeks after results were sent home. The questionnaire responses provided no evidence that increases in WBT occurred following the BMI assessment. It should be noted that in this study students’ height and weight were recorded in a screened area to ensure the student’s privacy. Such a procedure is consistent with recommended best practices, but may not be widely implemented,77 so the findings of this study may not be widely generalizable.
In a rigorous test of the hypothesis that school-based BMI screening is associated with adverse students outcomes, Madsen et al90 conducted a randomized clinical trial in which 79 elementary and middle schools were randomly assigned to either undergo BMI screening or have no screening for 3 successive years. Students completed a survey each fall and then again 6–9 months after the BMI assessments. A peer weight-based teasing index was included on each survey. Among the 14,318 students studied, WBT did not increase as a function of the BMI assessment. In sum, the available evidence does not provide evidence for an association between school-based PFT and WBT.
Association between Gender Discrimination and Physical Fitness Testing
No peer-reviewed publications related to gender bias and PFT were identified through our literature search. Indirect evidence related to the potential association is reviewed below.
DISCUSSION
The purpose of this review was to examine the available evidence for the assertion that school-based fitness testing places students at risk for bullying, WBT, and/or gender discrimination. This assertion has been voiced repeatedly in the public sphere and is the foundation for a proposal by the Governor of California to place a hold on PFT throughout the state.62 In pursuit of the evidence, we examined the peer-reviewed literature and found little empirical support for an association between school-based PFT and bullying, WBT, or gender discrimination. Whereas a lack of evidence does not demonstrate the absence of an association between PFT and negative student outcomes, it does suggest that the available data are insufficient to justify termination of a statewide fitness testing mandate, given the valuable role that these data play in monitoring youth fitness on a community and population level. As discussed below, actions that can be recommended based on the available evidence include conducting rigorous research to confirm or refute the putative link between fitness testing and negative student impact, making concerted efforts to reduce the occurrence of school-based bullying and WBT by nurturing a positive school climate, establishing universal training and policies to support appropriate execution of fitness testing when implemented, and pursuing investigation of alternative approaches to assess student health.
Only 3 peer-reviewed studies addressing bullying and PFT emerged in our literature search. These studies fail to provide persuasive evidence to suggest that PFT places students at elevated risk for bullying as compared to other school situations. The broader literature on school-based bullying suggests that school climate is the dominant consideration influencing the frequency of bullying,91,92 with factors such as respect for diversity, school engagement, and social support from adults/students setting the stage for reduced incidence of bullying.
Several decades of research have provided compelling evidence that a positive school climate is positively associated with students’ physical and mental well-being and negatively associated with bullying.93 A positive school climate has been defined by the National School Climate Council, in part, as one that “includes norms, values, and expectations that support people feeling socially, emotionally, and physically safe.”94 Bullying has been shown to be more likely to occur when the school climate is unhealthy,92 and bullying can be decreased through schoolwide interventions designed to improve the school climate.95 It is worth noting that the components of a positive school climate closely mirror the components of a PE program that follows established best practices. Major components of a positive school climate include feeling safe, connected, and engaged.96 These components align closely with the standards set forth for PE by the National Board for Professional Teaching Standards (NBPTS),97 which state that: “Accomplished teachers set high expectations and create positive, well-managed classroom environments that engage all students within a safe and respectful culture of learning (Standard V);” and “Accomplished teachers create inclusive and productive learning environments that are safe, fair, and equitable for all students. They promote healthy social interactions within their schools and communities by teaching students to embrace their uniqueness and respect the diversity of others (Standard VI).”
It is also worth noting that there may be a reciprocal relationship between the overall school climate and the climate in the PE program. A positive school climate is cultivated through “setting clear expectations for behavior, promoting mutual respect, consistently enforcing rules, [and] effectively managing classroom transitions.”98 These principles can be effectively established, modeled, and reinforced in the PE program setting, which has been suggested as an ideal platform for addressing students’ social and emotional learning.99 Conversely, PE teachers who operate within a positive school climate are empowered to address directly and decisively any instances of unsupportive behavior exhibited by students.100 In the absence of an overall school climate that prohibits bullying and promotes supportive behavior, bullying is more likely to occur across all school settings.
Weight-based teasing is a particular type of bullying that has been repeatedly called out as likely to be a negative outcome of PFT; yet, our review of the literature revealed no empirical support for this assertion and some evidence in opposition. Unfortunately, several published peer-reviewed articles have promulgated the assumption that students who are overweight or obese are subject to WBT because of PFT, despite the lack of evidence to demonstrate that such an association exists. In fact, the 2 prospective studies that investigated the frequency of WBT before and after students underwent the PFT83,101 found no increase in teasing after the assessments.
Although there is a dearth of evidence that school-based PFT results in WBT, the concern about a link is intuitive, and has been expressed by both students and teachers in qualitative studies.83,87 Recommendations for best practices in carrying out PFT reflect this concern, and include the suggestion that students should be provided with the opportunity to assess their own fitness regularly (with a trusted partner) in informal testing sessions.26 The implication here is that fitness testing should be implemented in such a manner that students feel safe, both in terms of the social context and in terms of their readiness for the assessment. A sense of social and emotional safety is another linchpin of a positive school climate,96 and there is strong evidence to support the efficacy of practices that improve positive peer relationships, positive staff-student relationships, and students’ sense of school connectedness and belonging as a means of improving school climate.98 Thus, the evidence suggests that in a school with a positive school climate the potential for a negative impact of PFT is diminished, and that when PFT is administered using recommended best practices, it may contribute to building a positive school climate.
That PFT is often implemented in a way that is inconsistent with recommended best practices has been documented,77 and may be the underlying reason for widespread concern about the impact of PFT on student well-being. As policymakers and educators continue to wrestle with the question of whether to implement fitness testing in the schools, it is imperative that high-quality studies be conducted to ascertain whether WBT in fact occurs when the assessments are carried out within a positive school climate and using best practices for test administration. One study relevant to this question surveyed 304 elementary school students who completed a BMI screening at school in a private setting by nurses who had received training in sensitive approaches to height and weight assessment.102 Ninety-four percent of the students reported that they were “OK” or “happy” with the experience, suggesting that when implemented using best practices, school-based screening is not likely to lead to negative student reactions. The currently available body of evidence is insufficient to determine whether the benefits of the PFT are outweighed by the putative negative consequences.101,103
Future studies intended to examine the potential link between PFT and negative social interactions should incorporate examination of the experiences of youth with disabilities. Such youth may be especially vulnerable to bullying, especially if they are also obese.104 Calls for inclusive PE programs105,106 point out that students with disabilities tend to score lower on fitness tests compared to youth without disabilities, and that students with disabilities tend to benefit from inclusive physical education programming. Inclusive programming may, however, afford opportunities for students with disabilities to receive unwanted attention during PFT. Thus, best practices for administering PFT among students with disabilities should be identified and incorporated into teacher training.
The third justification used by the Governor of California for wanting to place a hold on PFT revolves around issues of gender identification. Specifically, concerns have been raised that the method for interpreting fitness data requires students to identify as either male or female, and thus, fails to accommodate students with a non-binary gender. Because the potential for gender identification to play a role in the impact of PFT on youth has only newly come to the fore as a concern, there are no published studies that directly address this issue; yet, the data derived from PFT have been normed against a binary gender categorization, leading to concerns about perceived pressure on youth to identify as male or female.34,35,62 As stated by one advocate for youth with non-binary gender identities: “If I’m a transgender boy and nobody knows, and then I don’t meet the standards of a boy physically, I’m put in a difficult situation. Either I don’t meet the standards and take the according grade or I compromise my privacy and tell my teacher I was born as a girl.”61 In other words, a student may be faced with choosing to identify as male, and therefore, be held to a more stringent fitness standard, as boys on average have higher fitness than girls, or choosing to (mis)identify as female so as to be evaluated in comparison to the fitness standards for girls.
Importantly, there are currently no published data that speak to the prevalence or severity of pressure on students to identify their gender during PFT. Data relevant to the prevalence of students with non-binary gendered youth are currently unreliable, yet seem to suggest that between 1%–3% of youth may be uncomfortable if challenged to identify as male or female for the purposes of fitness evaluation. Consistent with California Senate Bill 179, the California Department of Education has adapted to the expansion of gender identities by recognizing a third gender choice of non-binary, which started in the 2018–2019 administration of school-based PFT.107 The gender field is left blank on student score reports for students who identify as non-binary and their scores are not scored or reported.107,108 Whether this approach buffers students who identify as non-binary from potential negative impacts of PFT remains to be demonstrated. More robust information about both the prevalence of non-binary gender identities and how students with non-binary gender experience PFT are needed to describe the scope of the problem and inform possible responses.
Available data suggest that the prevalence of non-binary gender appears to be low,66 but the prevalence of bullying among youth who identify as non-binary gender is high,72 and the consequences can be severe in terms of mental and physical health.67 Theoretically, a student of non-binary gender could be placed in an uncomfortable position if required to state their gender to conform to the needs of the testing. One line of inquiry that would be informative in the current debate over the role of gender identification in PFT is to determine the extent to which the need for gender designation impacts the transgender student’s assessment experience. Quantitatively, certain components of the FITNESSGRAM, the PFT utilized throughout the State of California and several other states, specify different cut-points for boys and girls in the determination of whether a student’s score falls within the Healthy Fitness Zone (HFZ). Boys typically must meet a higher standard to be classified as within the HFZ.109 It is possible to envision that a transgender male experiencing perceived pressure to meet the HFZ criterion might view the classification according to gender as discriminatory. It is important to note, however, that there are no data currently available to demonstrate the prevalence of such experiences or, indeed, the actual impact of the requirement for gender identification on the transgender student’s experience of PFT.
As noted above, research indicates that PFT is frequently implemented in a manner that is inconsistent with established and recommended best practices.77 The California Physical Fitness Test (PFT) Reference Guide for the 2019–2020 school year107 lists under each test component tips for correct implementation. However, these tips rarely address ways to minimize adverse reactions by students. Appropriate and inappropriate uses and administration of PFT have been described, however, in a number of academic publications.26,110–112 These publications highlight important aspects for PE teachers to consider when implementing PFT, such as “respect students privacy wishes. Some students become embarrassed with their mile times. Therefore, teachers should consider staggering start times so that no one knows what lap someone else is on.”110 Another set of recommendations about the appropriate and inappropriate practices in PFT implementation states that: “With physical fitness testing, the actual testing process is often quite public. Appropriate protocol can be used to assure as much privacy as possible (eg, separation of testing stations, screens to avoid observation of measurements, especially body composition measures).”111 Significantly, these published recommendations suggest that PFT should be part of a year-long curriculum,21,112 so that it serves an educational function and is embedded within a coherent series of lesson plans that provide context for fitness testing. The documented shortfall in PE teachers’ utilization of available training materials and implementation of best practices for PFT77 is testament to the need for better targeted training toward putting into practice widely recommended strategies for minimizing potential negative impact of PFT.
It is important to note that PFT can be used to serve 2 independent goals – surveillance and screening. To serve the first goal, surveillance, it is not necessary for students to be informed as to their performance or relative ranking on any of the assessments. Rather, the data can be anonymized and submitted to a centralized database and made available to support setting of policy, distribution of resources, and research. The State of California has posted anonymized and aggregated school fitness data to a publicly accessible website,113 which has enabled a number of policy-relevant publications. One such publication114 used the California PFT data in combination with Census data to demonstrate an association between neighborhood poverty and risk for overweight, and another115 analyzed the California PFT data to show disparities in risk for overweight by race/ethnicity and sex. The data collected by the Texas Youth Evaluation Project,116 in which PFT was implemented among more than 2.6 million students in Texas, were used to highlight the importance of PE teacher training and professional development, which were associated with higher rates of students meeting fitness goals.78 There is a strong rationale, thereby supporting large-scale implementation of PFT as a policy-relevant strategy for improving population health and reducing health disparities.
The second goal that may be served by the PFT is to identify individuals most at risk for health problems associated with poor fitness.82 There are typically certain assumptions made about how individual test results will be utilized and the value that they serve. For example, in a report from the Institute of Medicine released by the Committee on Physical Activity and Physical Education in the School Environment,117(p 210) the text states that PFT “can provide both teacher and student with information about the student’s current fitness level relative to a criterion referenced standard, yield valid information that can serve as the basis for developing a personal fitness or exercise program based on current fitness levels, motivate students to do better to achieve a minimum standard of health-related fitness where deficiencies exist, and possibly assist in the identification of potential future health problems.” Yet, there is little evidence to suggest that any of these potential outcomes of fitness assessments occur on a widespread basis. That is, there are no data to support the expectation that students typically receive constructive fitness testing feedback nor that such information motivates students to “do better.”118 In fact, there is evidence that teachers rarely use fitness test results to craft personal fitness plans for students and that providing students who are low in fitness with a percentile-based categorization of their assessment results may reduce their intrinsic motivation for physical activity.119,120 Moreover, accepted behavior change theory would suggest that merely informing students of their fitness level relative to a standard is a poor strategy to improve fitness, because knowledge of one’s risk status is seldom sufficient to motivate a change in behavior.121
Fitness testing as a means of encouraging individual behavior change has been critiqued on the grounds that “it focuses attention on the outcome or product rather than the underlying behavior that is being promoted (physical activity).”122 This distinction is important for 2 reasons. First, students may score relatively high on tests of fitness without being regularly physically active, as up to 60% of fitness may be genetically determined.123 Because physical activity is associated with many health and psychosocial benefits independent of physical fitness,124–127 relying solely on measures of fitness to provide students with information to inform their lifestyle choices could lead some youth to conclude erroneously that their sedentary behavior is not a cause for concern. A second reason it is important to distinguish between fitness assessment and physical activity assessment is that any recommendations must ultimately be communicated to youth in terms of suggested changes in physical activity. That is, to improve fitness an increase in physical activity is required, and meaningful guidance will be more effective if rooted in information about physical activity levels.
Although the potential utility of physical activity assessment as a component of PE in schools has long been recognized, it often has been assumed to be low in feasibility owing to cost, logistics, and/or lack of reliability of the assessment tools. In the last decade, however, the rapid acceleration in acceptability, ubiquity, and reliability of ambulatory activity monitors has largely removed these barriers to school-based physical activity monitoring. The evidence suggests that consumer-oriented activity monitors are acceptable, even appealing, to youth,128–130 and that the data are of sufficient quality to inform behavioral recommendations.131 Moreover, activity monitors largely do away with the concerns about bullying, WBT, and/or gender discrimination that have been raised in relation to fitness testing. In the current pandemic era, during which many students are not attending school in person and those who are may be asked to maintain physical distance, activity monitoring affords a potential means of remotely evaluating student health. To date, however, activity monitoring has not been widely adopted in the school environment as a method to assess student health, even though there is some evidence to suggest that providing students with data derived from activity monitors may increase their motivation to engage in physical activity.132–135 Future consideration of the role of PFT in schools, therefore, should include a discussion of the potential for physical activity assessment as a possible alternative strategy for identifying students at elevated health risk, generating data that might be used to highlight disparities in health across demographic and regional groups, and promoting individual behavior change conducive to better health.
IMPLICATIONS FOR HEALTH BEHAVIOR OR POLICY
A goal of Healthy People 2030 is to “improve health, fitness, and quality of life through regular physical activity,” which is associated with physical activity objective 6 to “increase the proportion of adolescents who do enough aerobic physical activity.”136 This objective is inherently compatible with the aims of school-based PFT. However, PFT also may afford an opportunity for adolescents to be discouraged from being physically active if the assessments are implemented improperly. On the basis of this literature review, we offer the following recommendations:
Rigorous research should investigate the putative association between PFT on the one hand, and bullying, WBT, and gender discrimination on the other. This research should be designed to compare rates of negative social interactions associated with PFT to those occurring in the school as a whole and to examine the moderating effects of school climate.
School-based fitness testing, when implemented, should be supported by rigorous teacher training in best practices not only to ensure adherence to the testing protocol but also to create a safe and learning-oriented context for testing.
In pursuit of the goal of motivating behavior change through providing students with data about themselves, alternatives to PFT, such as physical activity monitoring, should be explored. Behavioral theory would suggest that monitoring the behavior that is amenable to volitional change is more likely to stimulate behavior change as compared to monitoring an outcome of that behavior, such as body composition or cardiorespiratory endurance.
Acknowledgements
The authors thank Truc Trung Nguyen and Jasmin Marao Francisco for their assistance in gathering literature for this review, and Melissa Bittner, PhD for comments on the draft manuscript. This work was supported, in part, by funding from NIH/NCATS (UL1 TR001414).
Footnotes
Human Subjects Approval Statement
This review does not meet the criteria for human subjects research; therefore, institutional review board approval was not applicable.
Conflict of Interest Disclosure Statement
All authors declare they have no conflicts of interest.
References
- 1.US Centers for Disease Control and Prevention. Trends in the Prevalence of Physical Activity and Sedentary Behaviors National YRBS: 1991–2017. https://www.cdc.gov/healthyyouth/data/yrbs/pdf/trends/2017_physical_trend_yrbs.pdf. Published 2019. Accessed June 16, 2020.
- 2.US Department of Health and Human Services, 2018 Physical Activity Guidelines Advisory Committee. 2018 Physical Activity Guidelines Advisory Committee Scientific Report. https://health.gov/our-work/physical-activity/current-guidelines/scientific-report. Published 2018. Accessed June 16, 2020.
- 3.Wahid A, Manek N, Nichols M, Kelly P, Foster C, Webster P, et al. Quantifying the association between physical activity and cardiovascular disease and diabetes: a systematic review and meta-analysis. J Am Heart Assoc. 2016;5(9): e002495. doi: 10.1161/JAHA.115.002495 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hu G, Lakka TA, Kilpelainen TO, Tuomilehto J. Epidemiological studies of exercise in diabetes prevention. Appl Physiol Nutr Metab. 2007;32(3):583–595. doi: 10.1139/H07-030 [DOI] [PubMed] [Google Scholar]
- 5.Gill JM, Cooper AR. Physical activity and prevention of type 2 diabetes mellitus. Sports Med. 2008;38(10):807–824. doi: 10.2165/00007256-200838100-00002 [DOI] [PubMed] [Google Scholar]
- 6.Davis CL, Tomporowski PD, McDowell JE, Austin BP, Miller PH, Yanasak NE, et al. Exercise improves executive function and achievement and alters brain activation in overweight children: a randomized, controlled trial. Health Psychol. 2011;30(1):91–98. doi: 10.1037/a0021766 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Watson A, Timperio A, Brown H, Best K, Hesketh KD. Effect of classroom-based physical activity interventions on academic and physical activity outcomes: a systematic review and meta-analysis. Int J Behav Nutr Phys Act. 2017;14(1):114. doi: 10.1186/s12966-017-0569-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Buscemi J, Kong A, Fitzgibbon ML, Bustamante EE, Davis CL, Pate RR, et al. Society of Behavioral Medicine position statement: elementary school-based physical activity supports academic achievement. Transl Behav Med. 2014;4(4):436–438. doi: 10.1007/s13142-014-0279-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ramires VV, Dumith SC, Goncalves H. Longitudinal association between physical activity and body fat during adolescence: a systematic review. J Phys Act Health. 2015;12(9):1344–1358. doi: 10.1123/jpah.2014-0222 [DOI] [PubMed] [Google Scholar]
- 10.Booth FW, Roberts CK, Thyfault JP, Ruegsegger GN, Toedebusch RG. Role of inactivity in chronic diseases: evolutionary insight and pathophysiological mechanisms. Physiol Rev. 2017;97(4):1351–1402. doi: 10.1152/physrev.00019.2016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.US Centers for Disease Control and Prevention. School health guidelines to promote healthy eating and physical activity. MMWR Recomm Rep. 2011;60(RR-5):1–76. [PubMed] [Google Scholar]
- 12.Pate RR, Davis MG, Robinson TN, Stone EJ, McKenzie TL, Young JC. Promoting physical activity in children and youth: a leadership role for schools: a scientific statement from the American Heart Association Council on Nutrition, Physical Activity, and Metabolism (Physical Activity Committee) in collaboration with the Councils on Cardiovascular Disease in the Young and Cardiovascular Nursing. Circulation. 2006;114(11):1214–1224. doi: 10.1161/circulationaha.106.177052 [DOI] [PubMed] [Google Scholar]
- 13.Pate RR, Flynn JI, Dowda M. Policies for promotion of physical activity and prevention of obesity in adolescence. J Exerc Sci Fit. 2016;14(2):47–53. doi: 10.1016/j.jesf.2016.07.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Pate RR, Oria M, Pillsbury L, eds. Fitness Measures and Health Outcomes in Youth (2012). Washington, DC: The National Academies Press; 2012. [PubMed] [Google Scholar]
- 15.Morrow JR Jr., Ede A. Research Quarterly for Exercise and Sport lecture. Statewide physical fitness testing: a big waist or a big waste? Res Q Exerc Sport. 2009;80(4):696–701. doi: 10.1080/02701367.2009.10599610 [DOI] [PubMed] [Google Scholar]
- 16.Cohen DD, Voss C, Sandercock GR. Fitness testing for children: let’s mount the zebra! J Phys Act Health. 2015;12(5):597–603. doi: 10.1123/jpah.2013-0345 [DOI] [PubMed] [Google Scholar]
- 17.Pate RR, Welk GJ, McIver KL. Large-scale youth physical fitness testing in the United States: a 25-year retrospective review. Pediatr Exerc Sci. 2013;25(4):515–523. doi: 10.1123/pes.25.4.515 [DOI] [PubMed] [Google Scholar]
- 18.Sanchez-Vaznaugh EV, Goldman Rosas L, Fernández-Peña JR, Baek J, Egerter S, Sánchez BN. Physical education policy compliance and Latino children’s fitness: does the association vary by school neighborhood socioeconomic advantage? PLoS One. 2017;12(6):e0178980–e0178980. doi: 10.1371/journal.pone.0178980 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Bai Y School Fitness Assessment and Promotion: State and National Evaluations with FITNESSGRAM [Dissertation]: Department of Kinesiology, Iowa State University; 2016. 10.31274/etd-180810-4746. Accessed April 3, 2021. [DOI] [Google Scholar]
- 20.Lee NE, De AK, Simon PA. School-based physical fitness testing identifies large disparities in childhood overweight in Los Angeles. J Am Diet Assoc. 2006;106(1):118–121. doi: 10.1016/j.jada.2005.09.053 [DOI] [PubMed] [Google Scholar]
- 21.Silverman S, Keating XD, Phillips SR. A lasting impression: a pedagogical perspective on youth fitness testing. Meas Phys Educ Exerc Sci. 2008;12(3):146–166. doi: 10.1080/10913670802216122 [DOI] [Google Scholar]
- 22.Corbin CB. Texas Youth Fitness Study: a commentary. Res Q Exercise Sport. 2010;81(3):S75–S78. doi: 10.1080/02701367.2010.10599696 [DOI] [PubMed] [Google Scholar]
- 23.Cale L, Harris J, Chen MH. More than 10 years after “the horse is dead …”: surely it must be time to “Dismount”?! Pediatr Exerc Sci. 2007;19(2):115–131. doi: 10.1123/pes.19.2.115 [DOI] [PubMed] [Google Scholar]
- 24.Corbin C, Pangrazi R, Welk G. A response to ‘The horse is dead; let’s dismount’. Pediatr Exerc Sci. 1995;7:347–351. doi: 10.1123/pes.7.4.347 [DOI] [Google Scholar]
- 25.Dauenhauer B, Keating X, Stoepker P, Knipe R. State physical education policy changes from 2001 to 2016. J Sch Health. 2019;89(6):485–493. doi: 10.1111/josh.12757 [DOI] [PubMed] [Google Scholar]
- 26.Wiersma L, Sherman C. The responsible use of youth fitness testing to enhance student motivation, enjoyment, and performance. Meas Phys Educ Exerc Sci. 2008;12:167–183. doi: 10.1080/10913670802216148 [DOI] [Google Scholar]
- 27.Hill G, Downing A. Effect of frequent peer-monitored testing and personal goal setting on Fitnessgram scores of Hispanic middle school students. The Physical Eductor. 2015;72(2):193–205. [Google Scholar]
- 28.Rowland TW. The horse is dead; let’s dismount. Pediatr Exerc Sci. 1995;7(2):117. doi: 10.1123/pes.7.2.117 [DOI] [Google Scholar]
- 29.Cale L, Harris J. Fitness testing in physical education – a misdirected effort in promoting healthy lifestyles and physical activity? Phys Educ Sport Pedagogy. 2009;14(1):89–108. doi: 10.1080/17408980701345782 [DOI] [Google Scholar]
- 30.Naughton GA, Carlson JS, Greene DA. A challenge to fitness testing in primary schools. J Sci Med Sport. 2006;9(1):40–45. doi: 10.1016/j.jsams.2006.01.002 [DOI] [PubMed] [Google Scholar]
- 31.Keating XD. The current often implemented fitness tests in physical education programs: problems and future directions. Quest. 2003;55(2):141–160. doi: 10.1080/00336297.2003.10491796 [DOI] [Google Scholar]
- 32.Zhu X, Davis S, Kirk TN, Haegele JA, Knott SE. Innappropriate practices in fitness testing and reporting: alternative strategies. J Phys Educ Recreat Dance. 2018;89(3):46–51. doi: 10.1080/07303084.2017.1417929 [DOI] [Google Scholar]
- 33.Public Health Council. Proposed Amendments to Massachusetts Regulation 105 CMR 200.00. http://blog.mass.gov/publichealth/wp-content/uploads/sites/11/2013/10/BMI-Reg.pdf. Published October 16, 2013. Accessed January 31, 2021.
- 34.Jones C Plan to cut PE test - and its body-fat measurement - in California sparks debate. https://edsource.org/2020/newsoms-plan-to-eliminate-p-e-test-sparks-debate-about-body-fat-measurements/624303. Published March 2, 2020. Accessed August 12, 2020.
- 35.Associated Press. California may pause student physical fitness tests due to bullying concerns. Los Angeles Times. https://www.latimes.com/world-nation/story/2020-02-05/california-may-pause-student-fitness-tests-due-to-bullying. February 5, 2020. Accessed August 12, 2020. [Google Scholar]
- 36.Gladden RM, Vivolo-Kantor AM, Hamburger ME, Lumpkin CD. Bullying Surveillance Among Youths: Uniform Definitions for Public Health and Recommended Data Elements, Version 1.0. https://www.cdc.gov/violenceprevention/pdf/bullying-definitions-final-a.pdf. Published 2014. Accessed June 20, 2020.
- 37.National Center for Education Statistics. Student Reports of Bullying Results from the 2017 School Crime Supplement to the National Crime Victimization Survey. https://nces.ed.gov/pubsearch/pubsinfo.asp?pubid=2019054. Published July 2019. Accessed June 20, 2020.
- 38.Hawker DS, Boulton MJ. Twenty years’ research on peer victimization and psychosocial maladjustment: a meta-analytic review of cross-sectional studies. J Child Psychol Psychiatry. 2000;41(4):441–455. doi: 10.1111/1469-7610.00629 [DOI] [PubMed] [Google Scholar]
- 39.Holt MK, Vivolo-Kantor AM, Polanin JR, Holland KM, DeGue S, Matjasko JL, et al. Bullying and suicidal ideation and behaviors: a meta-analysis. Pediatrics. 2015;135(2):e496–e509. doi: 10.1542/peds.2014-1864 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Fekkes M, Pijpers FI, Fredriks AM, Vogels T, Verloove-Vanhorick SP. Do bullied children get ill, or do ill children get bullied? A prospective cohort study on the relationship between bullying and health-related symptoms. Pediatrics. 2006;117(5):1568–1574. doi: 10.1542/peds.2005-0187 [DOI] [PubMed] [Google Scholar]
- 41.Copeland WE, Wolke D, Angold A, Costello EJ. Adult psychiatric outcomes of bullying and being bullied by peers in childhood and adolescence. JAMA Psychiatry. 2013;70(4):419–426. doi: 10.1001/jamapsychiatry.2013.504 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.School Specialty. Bullying in School - Physical Education. https://blog.schoolspecialty.com/bullying-school-physical-education/. Published September 19, 2015. Accessed August 12, 2020.
- 43.Wong A Gym class is so bad, kids are skipping school to avoid it. The Atlantic. https://www.theatlantic.com/education/archive/2019/01/why-pe-is-terrible/581467/.Published January 29, 2019. Accessed July 15, 2020. [Google Scholar]
- 44.Bradshaw CP, Sawyer AL, O’Brennan LM. Bullying and peer victimization at school: perceptual differences between students and school staff. School Psych Rev. 2007;36(3):361–382. doi: 10.1080/02796015.2007.12087929 [DOI] [Google Scholar]
- 45.Perkins HW, Perkins JM, Craig DW. No safe haven: locations of harassment and bullying victimization in middle schools. J Sch Health. 2014;84(12):810–818. doi: 10.1111/josh.12208 [DOI] [PubMed] [Google Scholar]
- 46.Vaillancourt T, Brittain H, Bennett L, Arnocky S, McDougall P, Hymel S, et al. Places to avoid: population-based study of student reports of unsafe and high bullying areas at school. Can J Sch Psychol. 2010;25(1):40–54. doi: 10.1177/0829573509358686 [DOI] [Google Scholar]
- 47.Merriam-Webster. Body-shaming. https://www.merriam-webster.com/dictionary/body-shaming. Accessed August 13, 2020.
- 48.Schvey NA, Marwitz SE, Mi SJ, Galescu OA, Broadney MM, Young-Hyman D, et al. Weight-based teasing is associated with gain in BMI and fat mass among children and adolescents at-risk for obesity: a longitudinal study. Pediatr Obes. 2019;14(10):e12538. doi: 10.1111/ijpo.12538 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Neumark-Sztainer D, Falkner N, Story M, Perry C, Hannan PJ, Mulert S. Weight-teasing among adolescents: correlations with weight status and disordered eating behaviors. Int J Obes Relat Metab Disord. 2002;26(1):123–131. doi: 10.1038/sj.ijo.0801853 [DOI] [PubMed] [Google Scholar]
- 50.Eisenberg ME, Neumark-Sztainer D, Story M. Associations of weight-based teasing and emotional well-being among adolescents. Arch Pediatr Adolesc Med. 2003;157(8):733–738. doi: 10.1001/archpedi.157.8.733 [DOI] [PubMed] [Google Scholar]
- 51.Greenleaf C, Petrie TA, Martin SB. Relationship of weight-based teasing and adolescents’ psychological well-being and physical health. J Sch Health. 2014;84(1):49–55. doi: 10.1111/josh.12118 [DOI] [PubMed] [Google Scholar]
- 52.Puhl RM, Luedicke J. Weight-based victimization among adolescents in the school setting: emotional reactions and coping behaviors. J Youth Adolesc. 2012;41(1):27–40. doi: 10.1007/s10964-011-9713-z [DOI] [PubMed] [Google Scholar]
- 53.Warkentin T, Borghese MM, Janssen I. Associations between weight-related teasing and psychosomatic symptoms by weight status among school-aged youth. Obes Sci Pract. 2017;3(1):44–50. doi: 10.1002/osp4.87 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Goldfield G, Moore C, Henderson K, Buchholz A, Obeid N, Flament M. The relation between weight-based teasing and psychological adjustment in adolescents. Paediatr Child Health. 2010;15(5):283–288. doi: 10.1093/pch/15.5.283 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Losekam S, Goetzky B, Kraeling S, Rief W, Hilbert A. Physical activity in normal-weight and overweight youth: associations with weight teasing and self-efficacy. Obes Facts. 2010;3(4):239–244. doi: 10.1159/000319433 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Goldschmidt AB, Wall M, Choo TH, Becker C, Neumark-Sztainer D. Shared risk factors for mood-, eating-, and weight-related health outcomes. Health Psychol. 2016;35(3):245–252. doi: 10.1037/hea0000283 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Haines J, Neumark-Sztainer D, Eisenberg ME, Hannan PJ. Weight teasing and disordered eating behaviors in adolescents: longitudinal findings from Project EAT (Eating Among Teens). Pediatrics. 2006;117(2):e209–215. doi: 10.1542/peds.2005-1242 [DOI] [PubMed] [Google Scholar]
- 58.Faith MS, Leone MA, Ayers TS, Heo M, Pietrobelli A. Weight criticism during physical activity, coping skills, and reported physical activity in children. Pediatrics. 2002;110(2 Pt 1):e23. doi: 10.1542/peds.110.2.e23 [DOI] [PubMed] [Google Scholar]
- 59.O’Connor JA, Graber KC. Sixth-grade physical education: an acculturation of bullying and fear. Res Q Exerc Sport. 2014;85(3):398–408. doi: 10.1080/02701367.2014.930403 [DOI] [PubMed] [Google Scholar]
- 60.Puhl RM, Luedicke J, Heuer C. Weight-based victimization toward overweight adolescents: observations and reactions of peers. J Sch Health. 2011;81(11):696–703. doi: 10.1111/j.1746-1561.2011.00646.x [DOI] [PubMed] [Google Scholar]
- 61.Lee A California may stop school fitness tests over fears they lead to bullying and body-shaming. CNN. https://www.cnn.com/2020/02/06/us/california-fitness-test-bullying-trnd/index.html. February 6, 2020. Accessed August 27, 2020. [Google Scholar]
- 62.Mays M Newsom wants to halt physical fitness test due to bullying, gender issues. Politico. https://www.politico.com/states/california/story/2020/02/03/newsom-wants-to-halt-physical-fitness-test-due-to-bullying-gender-issues-1258497. February 3, 2020. Accessed August 27, 2020. [Google Scholar]
- 63.Gender Recognition Act, Senate Bill No. 179, (2017). https://leginfo.legislature.ca.gov/faces/billNavClient.xhtml?bill_id=201720180SB179. Published October 10, 2017. Accessed April 3, 2021.
- 64.Rider GN, McMorris BJ, Gower AL, Coleman E, Eisenberg ME. Health and care utilization of transgender and gender nonconforming youth: a population-based study. Pediatrics. 2018;141(3):e20171683. doi: 10.1542/peds.2017-1683 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Herman JL, Flores AR, Brown TNT, Wilson BDM, Conron KJ. Age of Individuals who Identify as Transgender in the United States. https://williamsinstitute.law.ucla.edu/wp-content/uploads/Age-Trans-Individuals-Jan-2017.pdf. Published 2017. Accessed July 22, 2020.
- 66.Meerwijk EL, Sevelius JM. Transgender population size in the United States: a meta-regression of population-based probability samples. Am J Public Health. 2017;107(2):e1–e8. doi: 10.2105/AJPH.2016.303578 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Valentine SE, Shipherd JC. A systematic review of social stress and mental health among transgender and gender non-conforming people in the United States. Clin Psychol Rev. 2018;66:24–38. doi: 10.1016/j.cpr.2018.03.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Becerra-Culqui TA, Liu Y, Nash R, Cromwell L, Flanders WD, Getahun D, et al. Mental health of transgender and gender nonconforming youth compared with their peers. Pediatrics. 2018;141(5):e20173845. doi: 10.1542/peds.2017-3845 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Eisenberg ME, Gower AL, McMorris BJ, Rider GN, Shea G, Coleman E. Risk and protective factors in the lives of transgender/gender nonconforming adolescents. J Adolesc Health. 2017;61(4):521–526. doi: 10.1016/j.jado-health.2017.04.014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Roberts AL, Rosario M, Slopen N, Calzo JP, Austin SB. Childhood gender nonconformity, bullying victimization, and depressive symptoms across adolescence and early adulthood: an 11-year longitudinal study. J Am Acad Child Adolesc Psychiatry. 2013;52(2):143–152. doi: 10.1016/j.jaac.2012.11.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Reisner SL, Greytak EA, Parsons JT, Ybarra ML. Gender minority social stress in adolescence: disparities in adolescent bullying and substance use by gender identity. J Sex Res. 2015;52(3):243–256. doi: 10.1080/00224499.2014.886321 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Gordon AR, Conron KJ, Calzo JP, White MT, Reisner SL, Austin SB. Gender expression, violence, and bullying victimization: findings from probability samples of high school students in 4 US school districts. J Sch Health. 2018;88(4):306–314. doi: 10.1111/josh.12606 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.McGuire JK, Anderson CR, Toomey RB, Russell ST. School climate for transgender youth: a mixed method investigation of student experiences and school responses. J Youth Adolesc. 2010;39(10):1175–1188. doi: 10.1007/s10964-010-9540-7 [DOI] [PubMed] [Google Scholar]
- 74.Kosciw JG, Greytak EA, Zongrone AD, Clark CM, Truong NL. The 2017 National School Climate Survey: The Experiences of Lesbian, Gay, Bisexual, Transgender, and Queer Youth in Our Nation’s Schools. https://www.glsen.org/sites/default/files/2019-10/GLSEN-2017-National-School-Climate-Survey-NSCS-Full-Report.pdf. Published 2018. Accessed July 21, 2020.
- 75.Devís-Devís J, Pereira-García S, López-Cañada E, Pérez-Samaniego V, Fuentes-Miguel J. Looking back into trans persons’ experiences in heteronormative secondary physical education contexts. Phys Educ Sport Pedagogy. 2018;23(1):103–116. doi: 10.1080/17408989.2017.1341477 [DOI] [Google Scholar]
- 76.Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. doi: 10.1371/journal.pmed.1000097 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Martin SB, Ede A, Morrow JR Jr., Jackson AW. Statewide physical fitness testing: perspectives from the gym. Res Q Exerc Sport. 2010;81(3 Suppl):S31–S41. doi: 10.1080/02701367.2010.10599692 [DOI] [PubMed] [Google Scholar]
- 78.Zhu W, Welk GJ, Meredith MD, Boiarskaia EA. A survey of physical education programs and policies in Texas schools. Res Q Exerc Sport. 2010;81(3 Suppl):S42–S52. doi: 10.1080/02701367.2010.10599693 [DOI] [PubMed] [Google Scholar]
- 79.Bottino CJ, de Ferranti SD, Meyers AF, Rhodes ET. Massachusetts pediatricians’ views toward body mass index screening in schools: continued controversy. Clin Pediatr (Phila). 2016;55(9):844–850. doi: 10.1177/0009922815618487 [DOI] [PubMed] [Google Scholar]
- 80.US Centers for Disease Control and Prevention. Body Mass Index (BMI). https://www.cdc.gov/healthyweight/assessing/bmi/index.html. Published 2020. Accessed August 12, 2020.
- 81.Ikeda JP, Crawford PB, Woodward-Lopez G. BMI screening in schools: helpful or harmful. Health Educ Res. 2006;21(6):761–769. doi: 10.1093/her/cyl144 [DOI] [PubMed] [Google Scholar]
- 82.Soto C, White JH. School health initiatives and childhood obesity: BMI screening and reporting. Policy Polit Nurs Pract. 2010;11(2):108–114. doi: 10.1177/1527154410374218 [DOI] [PubMed] [Google Scholar]
- 83.Grimmett C, Croker H, Carnell S, Wardle J. Telling parents their child’s weight status: psychological impact of a weight-screening program. Pediatrics. 2008;122(3):e682–e688. doi: 10.1542/peds.2007-3526 [DOI] [PubMed] [Google Scholar]
- 84.Crawford PB, Hinson J, Madsen KA, Neumark-Sztainer D. An update on the use and value of school BMI screening, surveillance, and reporting. Child Obes. 2011;7(6):441–449. doi: 10.1089/chi.2011.0600.roun [DOI] [Google Scholar]
- 85.Cash TF. Developmental teasing about physical appearance: retrospective descriptions and relationships with body image. Soc Behav Pers. 1995;23(2):123–129. doi: 10.2224/sbp.1995.23.2.123 [DOI] [Google Scholar]
- 86.Hayden-Wade HA, Stein RI, Ghaderi A, Saelens BE, Zabinski MF, Wilfley DE. Prevalence, characteristics, and correlates of teasing experiences among overweight children vs. non-overweight peers. Obes Res. 2005;13(8):1381–1392. doi: 10.1038/oby.2005.167 [DOI] [PubMed] [Google Scholar]
- 87.Haines J, Neumark-Sztainer D, Thiel L. Addressing weight-related issues in an elementary school: what do students, parents, and school staff recommend? Eat Disord. 2007;15(1):5–21. doi: 10.1080/10640260601044428 [DOI] [PubMed] [Google Scholar]
- 88.Cogan JC, Smith JP, Maine MD. The risks of a quick fix: a case against mandatory body mass index reporting laws. Eat Disord. 2008;16(1):2–13. doi: 10.1080/10640260701771664 [DOI] [PubMed] [Google Scholar]
- 89.Janssen I, Craig WM, Boyce WF, Pickett W. Associations between overweight and obesity with bullying behaviors in school-aged children. Pediatrics. 2004;113(5):1187–1194. doi: 10.1542/peds.113.5.1187 [DOI] [PubMed] [Google Scholar]
- 90.Madsen KA, Thompson HR, Linchey J, Ritchie LD, Gupta S, Neumark-Sztainer D, et al. Effect of school-based body mass index reporting in California public schools: a randomized clinical trial [published online ahead of print, 2020 Nov 16]. JAMA Pediatr. 2021;175(3):251–259. doi: 10.1001/jamapediatrics.2020.4768 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Espelage DL, Swearer SM, eds. Bullying in American Schools: A Social-Ecological Perspective on Prevention and Intervention. Mahwah, NJ: Lawrence Erlbaum Associates Inc; 2004. [Google Scholar]
- 92.Wang CX, Berry B, Swearer SM. The critical role of school climate in effective bullying prevention. Theor Pract. 2013;52(4):296–302. doi: 10.1080/00405841.2013.829735 [DOI] [Google Scholar]
- 93.Thapa A, Cohen J, Guffey S, Higgins-D’Alessandro A. A review of school climate research. Rev Educ Res. 2013;83(3):357–385. doi: 10.3102/0034654313483907 [DOI] [Google Scholar]
- 94.National School Climate Center. What is School Climate? https://www.schoolclimate.org/about/our-approach/what-is-school-climate. Published 2007. Accessed September 16, 2020.
- 95.Bradshaw CP, Waasdorp TE, Leaf PJ. Effects of school-wide positive behavioral interventions and supports on child behavior problems. Pediatrics. 2012;130(5):E1136–E1145. doi: 10.1542/peds.2012-0243 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Hong J, Espelage DL, Lee J. School climate and bullying prevention programs. In Shapiro H, ed. The Wiley Handbook on Violence in Education: Forms, Factors, and Preventions. Hoboken, NJ: John Wiley & Sons Inc; 2012:359–374. [Google Scholar]
- 97.National Board for Professional Teaching Standards. Physical Education Standards. http://nbpts.org/wp-content/uploads/ECYA-PE.pdf. Published 2014. Accessed August 27, 2020.
- 98.Voight A, Nation M. Practices for improving secondary school climate: a systematic review of the research literature. Am J Community Psychol. 2016;58(1–2):174–191. doi: 10.1002/ajcp.12074 [DOI] [PubMed] [Google Scholar]
- 99.Jacobs J, Wright P. Social and emotional learning policies and physical education. Strategies. 2014;27:42–44. doi: 10.1080/08924562.2014.960292 [DOI] [Google Scholar]
- 100.Rukavina P, Doolittle S, Li W, Beale-Tawfeeq A, Manson M. Teachers’ perspectives on creating an inclusive climate in middle school physical education for overweight students. J Sch Health. 2019;89(6):476–484. doi: 10.1111/josh.12760 [DOI] [PubMed] [Google Scholar]
- 101.Madsen KA, Linchey J. School-based BMI and body composition screening and parent notification in California: methods and messages. J Sch Health. 2012;82(6):294–300. doi: 10.1111/j.1746-1561.2012.00700.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Johnston JC, McNeil DA, Best M, MacLeod C. A growth status measurement pilot in four Calgary area schools: perceptions of grade 5 students and their parents. J Sch Nurs. 2011;27(1):61–69. doi: 10.1177/1059840510394188 [DOI] [PubMed] [Google Scholar]
- 103.Thompson HR, Madsen KA. The report card on BMI report cards. Curr Obes Rep. 2017;6(2):163–167. doi: 10.1007/s13679-017-0259-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Haegele JA, Aigner C, Healy S. Impact of weight and disability status on bullying victimisation and perpetration among youth. J Paediatr Child Health. 2021;57(3):383–387. doi: 10.1111/jpc.15230. [DOI] [PubMed] [Google Scholar]
- 105.Gilbert E Designing inclusive physical education with universal design for learning. J Phys Educ Recreat. 2019;90(7):15–21. doi: 10.1080/07303084.2019.1637305 [DOI] [Google Scholar]
- 106.Wilhelmsen T, Sorensen M. Inclusion of children with disabilities in physical education: a systematic review of literature from 2009 to 2015. Adapt Phys Act Q. 2017;34(3):311–337. doi: 10.1123/apaq.2016-0017 [DOI] [PubMed] [Google Scholar]
- 107.California Department of Education. Physial Fitness Test Reference Guide. https://www.cde.ca.gov/TA/tg/pf/index.asp. Published 2020. Accessed September 19, 2020.
- 108.California Department of Education. PFT Frequently Asked Questions and Answers. https://www.cde.ca.gov/TA/tg/pf/pft11fasqa.asp. Published 2019. Accessed September 19, 2020.
- 109.California Department of Education. FITNESSGRAM: Healthy Fitness Zone Charts. https://www.cde.ca.gov/ta/tg/pf/healthfitzones.asp#:~:text=Standards%20established%20by%20The%20Cooper,organized%20by%20gender%20and%20age. Published 2020. Accessed September 9, 2020.
- 110.Stewart A, Annboyce B, Boyce BA, Block ME. Effective teaching practices during physical fitness testing. J Phys Educ Recreat. 2005;76(1):21–24. doi: 10.1080/07303084.2005.10607314 [DOI] [Google Scholar]
- 111.Ernst M, Corbin CB, Beighle A, Pangrazi R. Appropriate and inappropriate uses of FITNESSGRAM: a commentary. J Phys Act Health. 2006;3(s2):S90–S100. doi: 10.1123/jpah.3.s2.s90 [DOI] [Google Scholar]
- 112.Phillips SR, Marttinen R, Mercier K. Fitness assessment: recommendations for an enjoyable student experience. Strategies. 2017;30(5):19–24. doi: 10.1080/08924562.2017.1344168 [DOI] [Google Scholar]
- 113.California Department of Education. PFT Results. https://www.cde.ca.gov/ta/tg/pf/pftresults.asp. Published 2020. Accessed October 2, 2020.
- 114.Drewnowski A, Rehm C, Kao C, Goldstein H. Poverty and childhood overweight in California Assembly districts. Health Place. 2009;15(2):631–635. doi: 10.1016/j.healthplace.2008.09.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Madsen KA, Weedn AE, Crawford PB. Disparities in peaks, plateaus, and declines in prevalence of high BMI among adolescents. Pediatrics. 2010;126(3):434–442. doi: 10.1542/peds.2009-3411 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116.Cooper KH. Reflections on the Texas Youth Evaluation Project and implications for the future. Res Q Exerc Sport. 2010;81(3 Suppl):S79–S83. doi: 10.1080/02701367.2010.10599697 [DOI] [PubMed] [Google Scholar]
- 117.Kohl H, Cook H, Committee on Physical Activity and Physical Education in the School Environment, Food and Nutrition Board, Institute of Medicine, eds. Educating the Student Body: Taking Physical Activity and Physical Education to School. Washington, DC: The National Academies Press; 2013. [PubMed] [Google Scholar]
- 118.Keating X, Silverman S. Teachers’ use of fitness tests in school-based physical education programs. Meas Phys Educ Exerc Sci. 2004;8(3):145–165. doi: 10.1207/s15327841mpee0803_2 [DOI] [Google Scholar]
- 119.Whitehead JR, Corbin CB. Youth fitness testing: the effect of percentile-based evaluative feedback on intrinsic motivation. Res Q Exerc Sport. 1991;62(2):225–231. doi: 10.1080/02701367.1991.10608714 [DOI] [PubMed] [Google Scholar]
- 120.Mercier K, Phillips SR, Silverman S. High school physical education teachers’ attitudes and use of fitness tests. High Sch J. 2016;99(2):179–190. doi: 10.1353/hsj.2016.0001 [DOI] [Google Scholar]
- 121.Rutkowski EM, Connelly CD. Obesity risk knowledge and physical activity in families of adolescents. J Pediatr Nurs. 2011;26(1):51–57. doi: 10.1016/j.pedn.2009.12.069 [DOI] [PubMed] [Google Scholar]
- 122.Welk GJ. The role of physical activity assessments for school-based physical activity promotion. Meas Phys Educ Exerc Sci. 2008;12(3):184–206. doi: 10.1080/10913670802216130 [DOI] [Google Scholar]
- 123.Bouchard C, Rankinen T, Timmons JA. Genomics and genetics in the biology of adaptation to exercise. Compr Physiol. 2011;1(3):1603–1648. doi: 10.1002/cphy.c100059 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124.Ozemek C, Laddu DR, Lavie CJ, Claeys H, Kaminsky LA, Ross R, et al. An update on the role of cardiorespiratory fitness, structured exercise and lifestyle physical activity in preventing cardiovascular disease and health risk. Prog Cardiovasc Dis. 2018;61(5–6):484–490. doi: 10.1016/j.pcad.2018.11.005 [DOI] [PubMed] [Google Scholar]
- 125.Farren GL, Zhang T, Gu X, Thomas KT. Sedentary behavior and physical activity predicting depressive symptoms in adolescents beyond attributes of health-related physical fitness. J Sport Health Sci. 2018;7(4):489–496. doi: 10.1016/j.jshs.2017.03.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126.Myers J, Kokkinos P, Nyelin E. Physical activity, cardiorespiratory fitness, and the metabolic syndrome. Nutrients. 2019;11(7):1652. doi: 10.3390/nu11071652 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 127.Hu MX, Turner D, Generaal E, Bos D, Ikram MK, Ikram MA, et al. Exercise interventions for the prevention of depression: a systematic review of meta-analyses. BMC Public Health. 2020;20(1):1255. doi: 10.1186/s12889-020-09323-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128.Schneider M, Chau L. Validation of the Fitbit Zip for monitoring physical activity among free-living adolescents. BMC Res Notes. 2016;9(1):448. doi: 10.1186/s13104-016-2253-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 129.Schaefer SE, Van Loan M, German JB. A feasibility study of wearable activity monitors for pre-adolescent school-age children. Prev Chronic Dis. 2014;11:E85. doi: 10.5888/pcd11.130262 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130.Muller J, Hoch AM, Zoller V, Oberhoffer R. Feasibility of physical activity assessment with wearable devices in children aged 4–10 years-a pilot study. Front Pediatr. 2018;6:5. doi: 10.3389/fped.2018.00005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 131.Yang X, Jago R, Zhang Q, Wang YY, Zhang J, Zhao WH. Validity and reliability of the wristband activity monitor in free-living children aged 10–17 years. Biomed Environ Sci. 2019;32(11):812–822. doi: 10.3967/bes2019.103 [DOI] [PubMed] [Google Scholar]
- 132.Suchert V, Steinvoord K, Schwarz J, Isensee B, Krieger C. Motivational aspects and critical issues of a pedometer intervention in adolescents. Health Promot Pract. 2018;19(1):60–67. doi: 10.1177/1524839916667273 [DOI] [PubMed] [Google Scholar]
- 133.Isensee B, Suchert V, Hansen J, Weisser B, Hanewinkel R. Effects of a school-based pedometer intervention in adolescents: 1-year follow-up of a cluster-randomized controlled trial. J Sch Health. 2018;88(10):717–724. doi: 10.1111/josh.12676 [DOI] [PubMed] [Google Scholar]
- 134.Chen JL, Guedes CM, Cooper BA, Lung AE. Short-term efficacy of an innovative mobile phone technology-based intervention for weight management for overweight and obese adolescents: pilot study. Interact J Med Res. 2017;6(2):e12. doi: 10.2196/ijmr.7860 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 135.Nation-Grainger S “It’s just PE’ till “It felt like a computer game’: using technology to improve motivation in physical education. Res Pap Educ. 2017;32(4):463–480. doi: 10.1080/02671522.2017.1319590 [DOI] [Google Scholar]
- 136.Office of Disease Prevention and Health Promotion. Healthy People 2030. https://health.gov/our-work/healthy-people-2030. Published 2020. Accessed October 31, 2020.